Introduction to Transitions of Care
|
|
|
- Jeffrey Warren
- 5 years ago
- Views:
Transcription
1 Introduction to Transitions of Care Margie McLaughlin Director of Education Development This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. CMSQIN_C2_201505_0030
2 What s a LAN? Learning Action Network Community of people connected through education, dissemination and sharing ideas and best practices Dynamic! Community of sharers Share shamelessly! Rhythm Prepare > Deploy > Pollinate > Review
3 What s Pollination Education? Method for spreading information Small learning modules with corresponding activities and engagement How far and wide can you pollinate? Pollination happens all throughout your organization Collaborative-interdisciplinary (all the other teams!) Everyone becomes involved and aware of the work that is being done Families, residents too!
4 How do we Pollinate? Creatively!! Table tents in the break room Posters, bulletin boards Resident/Family Council meetings Progress boards How many staff have (filled out the survey, watched the video, attempted the homework assignment Create awareness, transparency energy Make it fun and worthwhile
5 What will the Series 1 topics include? Introduction to Transitions Integrating QAPI into Transitions Preventing Adverse Events Interact Training Reducing Healthcare Acquired Conditions Advanced Directives End of Life Care Discharge to Community Improving areas of clinical risk Getting a Seat at the Referral Table
6 What will the Series 1 topics include? Introduction to Transitions Integrating QAPI into Transitions Preventing Adverse Events Interact Training Reducing Healthcare Acquired Conditions Advanced Directives End of Life Care Discharge to Community Improving areas of clinical risk Getting a Seat at the Referral Table These topics contain evidence-based practices that, when applied in SNFs, can have the most effective and dramatic results. Example: Jewish Home
7 Intended Outcome Save Lives and Improve Care by ensuring that our staff: have a vast working knowledge of transitions and all of its many related facets know what to do and have a sense of confidence that they re doing the right thing As a community we become adept at transitions
8 Preparing for Series 1 (03/26-04/26) 1. Review the instructions that accompany this webinar a) Who is the Champion And alternative Who is the team b) Check your computer equipment c) Make a plan For rolling out the education program Getting staff/families engaged d) Complete the QAPI Assessment (also in survey monkey) e) When you are all done submit your responses in the survey monkey This is the means by which you will receive your link to the modules
9 Introduction to Transitions of Care: Foundations Margie McLaughlin Director of Education Development This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. CMSQIN_C2_201505_0031
10 From a system perspective, a safe transition from a hospital to the community or a nursing home requires care that centers on the patient and transcends organizational boundaries. Jencks et al, New England Journal of Medicine, April 2009
11 Learning Objectives Participants will: Review key definitions Identify settings that constitute the LTC Continuum Examine the issues Use the Introduction to Transition of Care Foundations Worksheet
12 Transitions of Care Transition of care refers to the movement of patients between health care locations, providers, or different levels of care within the same location as their conditions and care needs change.
13 A transition of care can occur... Within settings: e.g., primary care to specialty care, intensive care unit to ward; Between settings: e.g., hospital to subacute care, ambulatory clinic to senior day-care center; And also...
14 A transition of care can occur... Across health states: e.g., curative care to palliative care or hospice, personal residence to assisted living; or Between providers: e.g., generalist to specialist practitioner, acutecare provider to palliative care specialist, hospitalist to primary care practitioner (PCP).

15 Transitional Care is Transitional Care a set of actions designed to ensure coordination and continuity of care
16 Transitional Care Transitional Care should be based on: a comprehensive care plan the availability of well-trained practitioners who: have current information about the patient s treatment goals preferences health clinical status
17 Transitional Care It includes: logistical arrangements education of patient and family coordination among the health professionals involved in the transition
18 Examples It is common for residents in the long-term care continuum (LTCC) to be transferred from one care setting, level of care, or caregiver team to another. For example: 1. A resident of a center within the LTCC who experiences an acute change of condition may be transferred to the emergency department (ED), admitted to the hospital, and ultimately discharged from the hospital back to the original care setting. 2. A resident of a senior apartment complex may be hospitalized for a surgical procedure, transferred to a skilled nursing facility (SNF) for rehabilitation, and subsequently transferred either back to his or her senior apartment or, if unable to resume living independently, to an assisted living community (ALC).
19 Care Coordination Care coordination is the deliberate organization of patient care activities among two or more participants (including the patient and/or family) involved in a patient s care to facilitate the appropriate delivery of health care services.
20 Care Coordination Organizing care involves the marshalling of personnel and other resources to carry out all required patient care activities. This is often managed by the exchange of information among participants responsible for different aspects of the care.
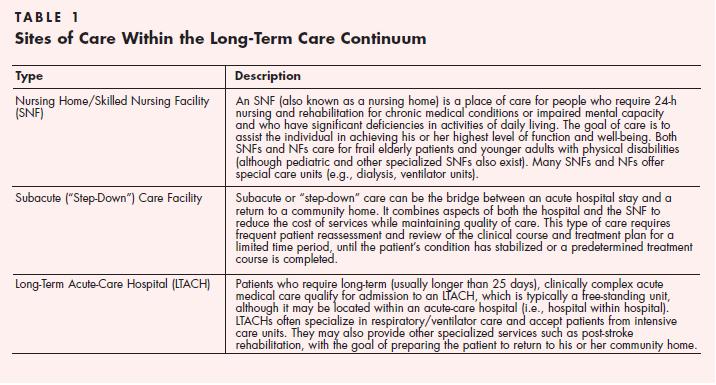
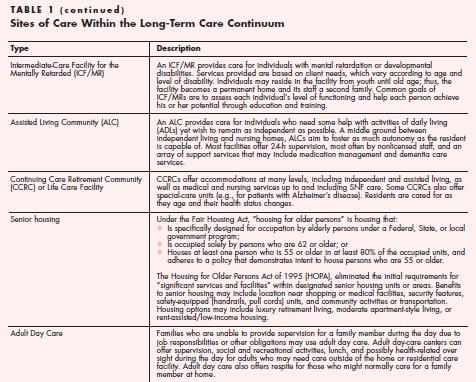
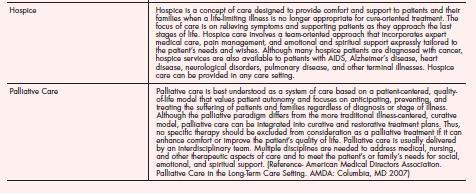
21 Long-term Care Continuum(LTCC) The long-term care continuum (LTCC) is a comprehensive, longitudinal, patient-centered system of formal and informal health and support services intended to improve, maximize, or stabilize, when possible, the function of patients with chronic disease across various settings over an extended period of time and to provide compassionate care at the end of life.
22 The Long Term Care Continuum (LTCC) Encompasses a broad range of sites of care Look at all of these!
23
24
25
26 What s the issue? It is also all too common for adverse events and avoidable complications to occur as a result of poor communication and coordination among caregivers, health care professionals, and the patient during such transitions.
27 Poorly Executed Care Transitions Increase hospital readmissions, duplicate services, and waste resources. They are the leading cause of medication errors, which frequently result from lack of coordination between prescribers across settings. It is often unclear which practitioner is responsible for the patient in the interval between discharge from one setting and admission to another.
28 High Risk Some older adults are at particular risk for transition problems following a hospitalization. Those with multiple medical problems, cognitive deficits, or depression or other mental health problems; isolated seniors; non-english speakers, immigrants, and refugees; and those with few financial assets are especially vulnerable.
29 How big? Jencks et al recently estimated that close to one fifth of all Medicare beneficiaries discharged from the hospital are readmitted within 30 days, that 90% of these readmissions are unplanned, and that the cost to Medicare of unplanned rehospitalizations amounted to $17.4 billion in 2004.
30 How big? Patients with heart failure accounted for 26.9% of all readmissions within 30 days; patients with pneumonia,20.9%.
31 From where are the problems coming? Studies have shown that medication changes upon hospital admission or discharge are a frequent reason for adverse events. A prospective study of 151 patients admitted to general internal Medicine units at a teaching hospital found that a regularly used medication was discontinued in 46.4% of cases; 38.6% of these omissions were considered to have the potential to cause moderate or severe discomfort or clinical deterioration
32 Benefits of Continuity of Care Evidence is mounting that efforts to ensure continuity of care for older patients during care transitions can improve patient outcomes. By improving core discharge planning and transition processes out of the hospital; improving transitions and care coordination at the interfaces between care settings; and enhancing coaching, education, and support for patient self-management; the rate of avoidable rehospitalizations can be reduced.
33 Will You Help? Creating safe transitions for our older patients is key to their well-being. Leading your team into a process of developing systems to ensure the safety and well-being requires a national commitment.
34 If everyone is moving forward together, then success takes care of itself. Henry Ford
35 References AMDA: Transitions of Care in the Long Term Care Continuum
36 Introduction to Transitions of Care: Solutions Margie McLaughlin Director of Education Development This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. CMSQIN_C2_201505_0032
37 Safe Transitions Reimbursement Based on Outcomes and Value Institutional Care Individualized Care Reimburseme nt Based on Volume Fragmentation
38 Factors Associated with Low Rehospitalizations 47 Nursing homes in NY (N=26,746 patients) Measured Clinical and non-clinical factors associated with rehospitalization rates Three strongest predictors: 1. Training provided to nursing staff on how to communicate effectively with physicians about a residents condition 2. Physicians who practice in this nursing home treat residents within the nursing home whenever possible, saving hospitalization as a last resort 3. Provided better information and support to nurses and aides surrounding end-of-life care 1 Young Y et al. Clinical and Nonclinical Factors Associated with potentially preventable hospitalizations among nursing home residents in NYS. JAMDA 2011;12:
39 DANGER!! 1 st 48 hours after hospital transfer/admission Transfers on Friday afternoons Critical thinking by staff Lack of close communication among CNA s nursing and other NH staff and between nursing home staff and physicians/aprn s
40 Strategies for Reducing Transitions Start with Staffing: Follow the Rule What does Friday look like Do staff know the plan
41 Strategies to Reduce Hospitalizations INTERACT III Is a comprehensive program that uses these strategies Track your rehospitalizations Improve Communication Externally (e.g. with hospital/er) Internally (e.g. between nursing & physicians) Identify small changes in a resident s status early on Change Staffing Consistent Assignment Reduce staff turnover Utilize nurse practitioners Advance Care Planning
42 INTERACT II Program Tools Comprehensive approach to reduce hospitalizations Acute care transfer log to track/measure rehospitalizations QI Improvement review tool Evaluation to assess each hospitalization (Root cause analysis) Standard Transfer Form Communication Tool with Physicians (SBAR) Resident assessment tool & algorithms Stop & Watch and Care Paths Advance care planning resources
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Presentation Objectives
 Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Thank You for Joining!
 Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Module 6: End-of-Life Care in the Skilled Nursing Center
 Module 6: End-of-Life Care in the Skilled Nursing Center Lesson 2 NE QIN-QIO & Good Shepherd Community Care This material was prepared by the New England Quality Innovation Network-Quality Improvement
Module 6: End-of-Life Care in the Skilled Nursing Center Lesson 2 NE QIN-QIO & Good Shepherd Community Care This material was prepared by the New England Quality Innovation Network-Quality Improvement
INTERACT Webinar Series
 INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Upcoming Changes in Infection Prevention: What Skilled Nursing Facilities Need to Know
 Upcoming Changes in Infection Prevention: What Skilled Nursing Facilities Need to Know Aimee Ford, QI Consultant, Qualis Health June 8, 2016 Qualis Health A leading national population health management
Upcoming Changes in Infection Prevention: What Skilled Nursing Facilities Need to Know Aimee Ford, QI Consultant, Qualis Health June 8, 2016 Qualis Health A leading national population health management
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Welcome to the New England QIN-QIO Medication Safety Webinar!
 Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
Rehospitalizations: How Do You Measure Up?
 Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP
 Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Advancing Excellence Phase 2 Goals
 Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
Special Needs Plan (SNP) Model of Care Training 2018
 Model of Care Training 2018") Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
Piloting Bundled Medicare Payments for Hospital and Post-Hospital Care /
 Piloting Bundled Medicare Payments for Hospital and Post-Hospital Care / A Study of Two Conditions Raises Key Policy Design Considerations March 2010 Policymakers are exploring many different models for
Piloting Bundled Medicare Payments for Hospital and Post-Hospital Care / A Study of Two Conditions Raises Key Policy Design Considerations March 2010 Policymakers are exploring many different models for
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Presentation Objectives
 Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Molina Medicare Model of Care
 Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Molina Medicare Model of Care Provider Network Molina Healthcare 2018 1 Molina s Mission and Vision Our Vision: We envision a future where everyone receives quality health care Our Mission: To provide
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Transitional Care and Preventing Readmissions in San Francisco
 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
The Road Map to Success Implementation Checklist STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN NOTES COMPLETION
 STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN DATE COMPLETED BARRIERS TO COMPLETION NOTES 1-1 Identify an agency champion & back up Questions to ask: 1) Who is timely
STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN DATE COMPLETED BARRIERS TO COMPLETION NOTES 1-1 Identify an agency champion & back up Questions to ask: 1) Who is timely
Home Care Medical. Respiratory Care Clinical Outcomes
 Home Care Medical Respiratory Care Clinical Outcomes 1 Over 40 Years of Experience Home Care Medical (HCM) is committed to our mission of enhancing the quality of life of those we serve. In our continual
Home Care Medical Respiratory Care Clinical Outcomes 1 Over 40 Years of Experience Home Care Medical (HCM) is committed to our mission of enhancing the quality of life of those we serve. In our continual
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Fall Prevention Toolkit
 Fall Prevention Toolkit Webinar 2 Tools 1E: Resource Needs Assessment 2A: Interdisciplinary Team 2B: Quality Improvement Process 2C: Current Process Analysis 2D: Assessing Current Fall Prevention Policies
Fall Prevention Toolkit Webinar 2 Tools 1E: Resource Needs Assessment 2A: Interdisciplinary Team 2B: Quality Improvement Process 2C: Current Process Analysis 2D: Assessing Current Fall Prevention Policies
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
What Story Is Your SNF Data Telling?
 What Story Is Your SNF Data Telling? Holly Harmon, RN, MBA, LNHA Senior Director of Clinical Services Thank you to our Launch Sponsor: Objectives Recognize the value of data informed practice Identify
What Story Is Your SNF Data Telling? Holly Harmon, RN, MBA, LNHA Senior Director of Clinical Services Thank you to our Launch Sponsor: Objectives Recognize the value of data informed practice Identify
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
New Opportunities for Case Management Leadership in our Changing Environment
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Physician Hospital/SNF Collaborative Guidelines
 Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
Overview Physician Hospital/SNF Collaborative Guidelines Effective coordination of care is an essential element in any successful health care system and this element requires the willingness of specialists,
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4
 Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Long-Term Care Program
 Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Outcomes Reporting: Be Ready to Negotiate with a Hospital
 Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,
Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,