Trauma Transitional Care Coordination. Erin Hall, MD Rebecca Tyrrell, RN
|
|
|
- Sabrina Richardson
- 5 years ago
- Views:
Transcription

1 Trauma Transitional Care Coordination Erin Hall, MD Rebecca Tyrrell, RN

2

3 Decreasing Readmissions Rates Using Transitional Care Coordination Model Michigan Trauma QI Program, May 16, 2018 Rebecca Tyrrell, RN,CCCTM, Erin C. Hall, MD MPH R Adams Cowley Shock Trauma Center
4 Objectives At the end of this presentation: Describe Transitional Care Coordination (TCC) Demonstrate the application of a traditional TCC program on a trauma patient population Demonstrate the elements of a Trauma TCC program to improve patient outcomes Describe the impact of a Trauma TCC program on reducing readmissions

5 Significance of a Readmission Affordable Care Act 30 day readmission rate Quality indicator Healthcare costs
6 Background Unplanned 30-day readmissions after trauma 2-fold increase in 1-year risk of death 3-fold increase in per-patient expense
7 Background One fourth of annual Medicare expenditures Hospital Readmission Reduction Program Introduced in 2012 Already expanded to Heart attack/failure Pneumonia COPD Hip/knee replacement CABG

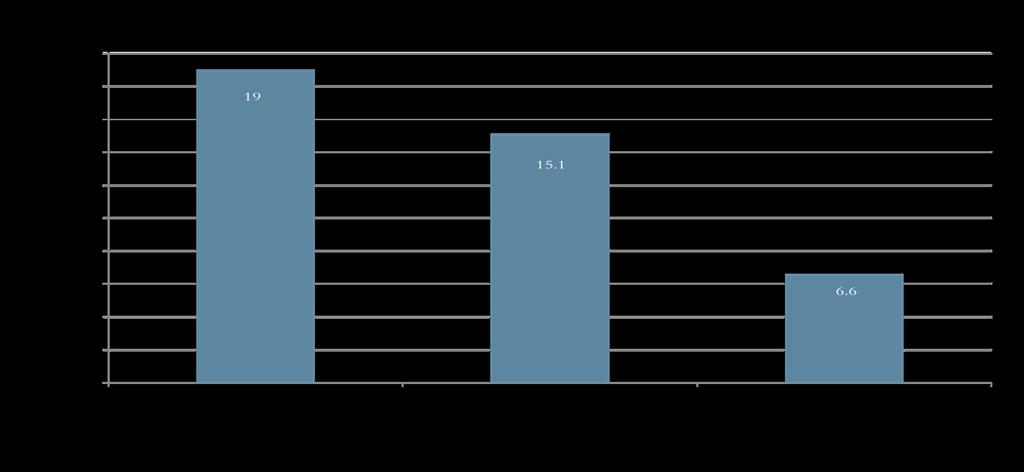
8 Shock Trauma Center Readmissions 15.1% readmission rate in in 7 patients readmitted to the acute care setting Opportunity for nursing to improve the quality of recovery and decrease readmissions
9 Background Transitional Care Coordination Focuses on highly vulnerable, chronically ill patients Time-limited Emphasis on education of patients and family caregivers
10 Background Transitional Care Coordination Proven effective in reducing 30-day readmission rates in patients with complex medical conditions In particular: Active care coordination by a nurse Active medication reconciliation Communication between PCP and hospital Home visit
11 Transitional Care Coordination Definition: the ongoing support of patients and their families over time as they navigate care and relationships among more than one provider and/or more than one health care service (Haas,Swan & Haynes,2014, p.3). Transitional Care Coordination process definition: care coordination and transition management necessitates professional assessment, patient risk identification and stratification, and identification of individual patient needs and preferences (Coleman & Boult,2003,p.556)
12 The Transitional Care Coordination Model Standardized by the American Academy of Ambulatory Care Nurses (AAACN) Support along a recovery continuum Professional assessment Risk stratification for readmission Identification of needs and resources
13 Trauma is increasingly becoming a chronic disease
14 Trauma is increasingly becoming a chronic disease Could we design and implement a TRAUMA transitional care coordination program?
15 Objectives Identify trauma patients at high risk for readmission Enroll in specially designed Trauma Transitional Care Coordination program
16 Objectives Primary Outcome Reduce 30-day readmission rate Secondary Outcomes Trauma clinic follow-up Primary care provider follow-up Patient perception of program and ability to care for self
17 Trauma Transitional Care Coordination Meet identified patient prior to discharge Call to patient (or caregiver) within 72 hours of discharge to identify barriers to care Complete medication reconciliation Coordination of medical appointments or home visits Individualized problem solving
18 Methods Identifying patients at high risk for readmission Literature review Expert opinion Nurses Case managers Intensivists Trauma surgeons
19 Methods Collected information on all 30-day readmissions Rate was compared to population, risk-adjusted benchmark for 30-day readmission rate Staudenmayer et al Trauma readmissions linked across California, stratified by injury severity
20 Methods Collected data on completed outpatient trauma and primary care provider appointments 10-item exit-questionnaire completed over the phone
21 Results
22 I would not have gotten through without the TTCC program

23 What we found Common themes Lack understanding of disease management Unable to navigate the health care system No knowledge of community resources No primary care physician (PCP)
24 Identified Risk Factors Social Factors Any previous readmission Poor or absent home assistance or home care services Poor or absent insurance Medical History Psychiatric disease Drug abuse Trauma Sequelae Pulmonary embolism without PCP Vascular injury without PCP New tracheostomy New traumatic brain injury High output fistula Large, open wounds before definitive closure Multiple co-morbidities without primary care
25 I had so many doctors it was too hard for me to remember everything. TTCC helped me with a system to remember what I needed to do for each doctor and problem TTCC showed me a better way to stretch out my pain meds and made me understand the importance of taking my Coumadin
26 Results 260 enrollees between January 2014-September % uninsured 45.4% current substance abuse 29.1% current psychiatric diagnosis 60% had multiple co-morbidities without a primary care provider
27 Results 260 enrollees between January 2014-September 2015 Average age = 41 y/o Mean ISS = 14.6 Mean length of stay = 11 days 53% White 73% Blunt trauma
28 96.6% Follow-up Only 9 patients of 260 lost to follow up
29 I had 9 doctors I was supposed to follow up with after rehab. TTCC sorted it all out and even doubled up on some of them TTCC showed me how to get transportation help. I don t know what we would have done.
30
31 Results 30-day readmission rate was 6.6% (n=16) Population, risk adjusted benchmark = 17% p=<0.001
32 Results 16 patients with 30-day readmissions 8 Preventable Readmissions Inadequate culture follow-up (1) Symptomatic pleural effusion (1) Incorrect discharge medications (1) Inappropriate discharge location (5)
33 Results 74% attended outpatient trauma clinic within 14 days of discharge 44% attended new primary care provider appointments within 30 days of discharge
34 I would not be better today if it had not been for the TTCC. She was a tremendous help Sometimes it seemed like it would have been easier to go to the ED, but I did learn how to take care of myself
35 Results 61.7% completed the exit questionnaire All agreed I feel more prepared and in more control of my new healthcare needs. I am able to take care of myself and my new normal All also agreed TTCC helped understand medications and how to take them TTCC helped sort out multiple appointments
36 I have many problems that I will have for a lifetime I am sure. The TTCC made it so I could handle my issues one at a time. Life isn t so bad. I can do this.
37 Limitations Comparison population Variability in reported readmission rates Collection method (single-center vs. population based) Risk stratification Injury severity alone Did not take into account added risk associated with Previous hospital admissions Increased number of comorbidities Lack of resources Psychiatric history
38 Potential Financial Impact University of Maryland Medical Center Up to 1% reward or 2% penalty of at risk revenue Based on comparison to hospital s previous performance Posted a loss of $860,116 (based on 2013 readmissions)
39 Potential Financial Impact Total yearly budget for TTCC: $310,000 On track to receive $3,000,000 REWARD
40 Conclusions Significantly lower 30-day readmission rates (6.6% vs. 17%) Long-term follow-up is feasible Better outpatient resource utilization High patient satisfaction Cost effective

41 I felt like I had a fairy godmother looking out for me
42 Trauma TCC Process Establish patient s recovery goals within 7 days Call patient/caregivers 24 to 72 hours after discharge Medication review/reconciliation Attend follow-up appointments Patient preparation for the next 21 days
43 TCC Timing Days 1 through 7: Develop patient and TCC relationship Work with patient on goals Establish needs and resources Transportation Insurance Ensure accessibility to PCP
44 TCC Timing Days 8 through 15: Integrate community resources Assure patient attendance at the follow-up Review treatment plan Observe for patient activation measures
45 TCC Timing Days 16 through 30: Observe patient's level of self care Ensure PCP appointment attended or made Address needs and resources Review goals Prepare for hand-off

46 Case Review 52 year old male Moped crash Found face down, unconscious, shallow respirations Temperature 38 degrees F
47 Case Review Injuries Closed head injury, subarachnoid hemorrhage, subdural hematoma Complex facial lacerations with facial droop Skull, facial, sternum, ribs, left hand, left femur, left tibia and fibula fractures
48 Case Review Hospital Course & Treatment Emerged agitated, uncontrollable Geodon, sitters 9 consulting services Future surgeries and procedures planned New diagnoses of uncontrolled hypertension and hepatitis C
49 Case Review Financial Uninsured Employer paid weekly in cash, not documented
50 Case Review Psychosocial Issues Lives with mother Criminal history History of suicide attempts History of depression/anxiety Court-ordered to take Celexa, has parole officer
51 Case Review Medical/Surgical Complexity 9 consulting services for follow-up Multiple surgeries remaining Traumatic brain injury Post concussive syndrome New diagnoses of hypertension and Hepatitis C
52 Case Review Discharge Preparation Reviewed clinical picture with the treatment team Met with patient and mother Developed patient s needs and resources Planned for transfer to inpatient traumatic brain injury rehab
53 Case Review Post Discharge Day #12 My mother says I should talk to you TBI rehab planning discharge to home in 2 days Briefly discussed tasks for the next week
54 Case Review Phone conversations Assessed as being a face to face learner Unable to process a lot of information Set up nurse visit with TCC
55 Case Review Motivational Interviewing Listening Observing breathing pattern Watching eye movements Understanding word choices
56 Case Review Nursing Assessment Patient did not know: How to call for an appointment He had to arrive on time How to manage bad news How to handle his fear of physical pain
57 Case Review Patient-Identified Recovery Goals Not drink Get rid of headache pain Go back to riding the motorcycle Take Celexa A better relationship with my son
58 Case Review Positive Outcomes Attended every appointment Obtained insurance, transportation Patient activation measures/ Goals Established a PCP and new psychiatrist All surgeries planned and scheduled
59 Case Review Quality Indicators No readmission within 30 days Not lost to follow-up Attended all follow-up appointments Attended PCP and psychiatry appointments Completed 30 day TCC program
60 Case Review Long term impact No unplanned readmissions at 3 months, 6 months 1 year following injury Established relationship with PCP, psychiatrist Learned how to navigate the healthcare system Understood limitations of insurance benefits
61 Case Review Independence Restored Successful return to: Part-time work as a cabinet maker Driving, legally Painting and copper art
62 Future for Trauma TCC Hardwire referral process Improve use of technology supporting patients and the TCC program Develop a trauma-specific predictive readmission risk tool Evaluate trauma patient healthcare literacy pre- and postprogram enrollment
63 Contact Information Rebecca Tyrrell, RN, CCCTM Erin Hall, MD MPH
64 Questions? Thank you for your time
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Kentucky Stroke Transitions Assistance Resource
 Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
30-day Readmission Survey. Monica Thurston, OMS 2 Mary Herberger, OMS 2
 30-day Readmission Survey Monica Thurston, OMS 2 Mary Herberger, OMS 2 Meet Mary Herberger and Monica Thurston, OMS 2 COMP-NW Lebanon, OR Satellite Campus of Western University of Health Sciences in Pomona,
30-day Readmission Survey Monica Thurston, OMS 2 Mary Herberger, OMS 2 Meet Mary Herberger and Monica Thurston, OMS 2 COMP-NW Lebanon, OR Satellite Campus of Western University of Health Sciences in Pomona,
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW. MetroHealth Medical Center
 Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Integrated Care Management in the Age of Population Health: What does that mean?!?
 Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
San Diego County Funded Long-Term Care Criteria
 San Diego County Funded Long-Term Care Criteria Prepared By: 6/23/16 Table of Contents San Diego County Funded Long Term Care Criteria... 2 Referral Criteria by Level of Care: Institute of Mental Disease
San Diego County Funded Long-Term Care Criteria Prepared By: 6/23/16 Table of Contents San Diego County Funded Long Term Care Criteria... 2 Referral Criteria by Level of Care: Institute of Mental Disease
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Camden Coalition of Healthcare. Management
 Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
From the Feds: Research, Programs, and Products
 FROM THE FEDS From the Feds: Research, Programs, and Products Laurie Flaherty, RN, MS, Washington, DC Department of Health and Human Services Health Consequences Among First Responders After Events Associated
FROM THE FEDS From the Feds: Research, Programs, and Products Laurie Flaherty, RN, MS, Washington, DC Department of Health and Human Services Health Consequences Among First Responders After Events Associated
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS
 BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
Italian National Institute of Statistics
 Seriously Injured in road accidents in Italy: MAIS3+ cases by national hospital discharge data Silvia Bruzzone Roberta Crialesi Italian National Institute of Statistics Directorate for Social Statistics
Seriously Injured in road accidents in Italy: MAIS3+ cases by national hospital discharge data Silvia Bruzzone Roberta Crialesi Italian National Institute of Statistics Directorate for Social Statistics
Aurora Behavioral Health System
 Aurora Behavioral Health System Outpatient Services Help is only a phone call away. Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of Guadalupe and Maple, between
Aurora Behavioral Health System Outpatient Services Help is only a phone call away. Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of Guadalupe and Maple, between
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services
 Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Harnett Health Community Needs Assessment Implementation Plan January 2014
 Introduction Harnett Health Community Needs Assessment Implementation Plan January 2014 In accordance with the Affordable Care Act, not-for-profit hospitals are required to develop Community Health Needs
Introduction Harnett Health Community Needs Assessment Implementation Plan January 2014 In accordance with the Affordable Care Act, not-for-profit hospitals are required to develop Community Health Needs
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support
 Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Maternity Management. The best part? These are available to you at no additional cost. Intro
 Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
TQIP and Risk Adjusted Benchmarking
 TQIP and Risk Adjusted Benchmarking Melanie Neal, MS Manager Trauma Quality Improvement Program TQIP Participation Adult Only Centers 278 Peds Only Centers 27 Combined Centers 46 Total 351 What s new TQIP
TQIP and Risk Adjusted Benchmarking Melanie Neal, MS Manager Trauma Quality Improvement Program TQIP Participation Adult Only Centers 278 Peds Only Centers 27 Combined Centers 46 Total 351 What s new TQIP
Value-based Care Report. February How Value-based Care is improving quality and health.
 Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
Value-based Care Report February 2018 How Value-based Care is improving quality and health. 1 Value-based Care means better health, better care and lower costs. Placing greater emphasis on value in health
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance. Our Story. What s So Special About Specialty Care?
 Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Benchmarking across sectors: Comparisons of residential dual diagnosis and mental health programs
 University of Wollongong Research Online Faculty of Health and Behavioural Sciences - Papers (Archive) Faculty of Science, Medicine and Health 2009 Benchmarking across sectors: Comparisons of residential
University of Wollongong Research Online Faculty of Health and Behavioural Sciences - Papers (Archive) Faculty of Science, Medicine and Health 2009 Benchmarking across sectors: Comparisons of residential
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Final Report. January 12, Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek
 Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks. Cheryl Crumpton, BSN, RN, CEN
 The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks Cheryl Crumpton, BSN, RN, CEN Making the Patient Call Manager (PCM) Connection Quality Initiative Improve Clinical
The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks Cheryl Crumpton, BSN, RN, CEN Making the Patient Call Manager (PCM) Connection Quality Initiative Improve Clinical
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division
 Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
 Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Policies for Controlling Volume January 9, 2014
 Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
COMMUNITY HEALTH IMPLEMENTATION STRATEGY
 COMMUNITY HEALTH IMPLEMENTATION STRATEGY COMMUNITY HEALTH IMPLEMENTATION STRATEGY Overview IRS legislation requires that hospitals follow up on the Community Health Needs Assessment (CHNA) with a strategy
COMMUNITY HEALTH IMPLEMENTATION STRATEGY COMMUNITY HEALTH IMPLEMENTATION STRATEGY Overview IRS legislation requires that hospitals follow up on the Community Health Needs Assessment (CHNA) with a strategy
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Value model in the new healthcare paradigm: Producing value at a single specialty center.
 Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Executing a Patient Experience Measurement Initiative
 Executing a Patient Experience Measurement Initiative Cathy Gorman Klug RN, MSN Director, Quality Service Line Nuance 2015 Nuance Communications, Inc. All rights reserved. Patient Experience Defined-The
Executing a Patient Experience Measurement Initiative Cathy Gorman Klug RN, MSN Director, Quality Service Line Nuance 2015 Nuance Communications, Inc. All rights reserved. Patient Experience Defined-The
Improving Care Transitions: Creating Your Evidence-Based Approach
 Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
FY2018 Outcomes Report
 FY2018 s Report PERFORMANCE IMPROVEMENT PLAN OUTCOMES Quality Improvement & Compliance TRI-COUNTY MENTAL HEALTH SERVICES, INC. 3100 N.E. 83RD ST., SUITE 1001, KANSAS CITY, MO 64119 Human Resources s Report
FY2018 s Report PERFORMANCE IMPROVEMENT PLAN OUTCOMES Quality Improvement & Compliance TRI-COUNTY MENTAL HEALTH SERVICES, INC. 3100 N.E. 83RD ST., SUITE 1001, KANSAS CITY, MO 64119 Human Resources s Report
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
American Health Quality Association Sept Baltimore Maryland Managing Behavioral Health Problems and Solutions
 American Health Quality Association Sept 9 2015 Baltimore Maryland Managing Behavioral Health Problems and Solutions Meeting the Challenges of Behavioral Health Integration IBHI IS: 501C3 Organization
American Health Quality Association Sept 9 2015 Baltimore Maryland Managing Behavioral Health Problems and Solutions Meeting the Challenges of Behavioral Health Integration IBHI IS: 501C3 Organization
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization. Andrea Plaskett, MPH
 KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital