John R. Mehall, MD, FACS, FACC Director of Cardiothoracic Surgery, Centura Health Managing Partner, Cardiac & Thoracic Surgery Associates, PC
|
|
|
- Brook Miller
- 5 years ago
- Views:
Transcription


1 John R. Mehall, MD, FACS, FACC Director of Cardiothoracic Surgery, Centura Health Managing Partner, Cardiac & Thoracic Surgery Associates, PC

2

3


4




5


6


7 MIS MVR Over 200 cases last 3 years 0% mortality 97% repair rate 0 conversions MIS AVR Right thoracotomy Over 100 last 3 years 0% mortality Overall MIS LOS 4.2 days
8 There are many parallels between Intermountain Healthcare and our primary health system Centura Health CTSA has successfully collaborated with the health system for mutual and patient benefit This collaboration has resulted in better: Patient care and patient access Hospital program growth and volume growth Increased financial reward for hospital/surgeons Busier surgeons with a better quality of life

9 Cardiovascular disease is the #1 killer in the US 40% of all Medicare funds are spent on cardiovascular disease Coronary Bypass Surgery is the #1 surgical expenditure for Medicare On average, cardiovascular disease represents 50% of a hospital s profit margin High visibility programs/surgeons
10 Cardiac Surgery Aortic Surgery Peripheral Vascular Surgery Interventional Cardiology Structural Heart Disease Cardiovascular Surgery Rhythm Cardiology Cardiology & Cardiovascular Medicine Imaging Cardiology Disease Prevention Cardiac Rehab
11
12 Intermountain Healthcare Centura Health Faith Based, Non-Profit Yes Hospitals Yes Clinics ER Visits 486, ,000 Admissions 93,000 86,000 Operations 140, ,000 Employed Physicians * * Employed and Contracted Physicians
13 Central Control Both started as local hospitals Banded together to from a system Transitioning from local to central control Increased Systemization at the cost of Local Autonomy
14 Intermountain Healthcare 4 cardiac surgery programs 1200 open heart cases MIS Valve Surgery Endovascular Aortic TAVR MitraClip/TMVR VAD/ECMO Transplant Centura Health & CTSA Practice 4 cardiac surgery programs 1200 open heart cases MIS Valve Surgery Endovascular Aortic TAVR MitraClip/TMVR VAD/ECMO

15 CTSA is an independent Surgical Group in private practice How CTSA started Why are we Independent? Group Collaboration Autonomy Finances Growth Strategies


16 Independent Surgery Practice Full Spectrum of Cardiovascular & Thoracic Surgery Surgery locations in Denver, Colorado Springs and Pueblo Contract with two main heath systems for CT Surgical Services Extensive Outreach Clinic Network across Colorado, Kansas Contract with many hospitals and cardiology groups for outpatient services
17 CTSA Staff 12 Surgeons 10 CT Surgeons 4 Cardiac surgery only 5 Cardiothoracic surgery 1 Thoracic surgery only 2 Vascular Surgeons 13 Midlevel Providers 9 PAs OR and ICU support 4 NPs coordinate CVU Care, Discharge and follow-up Full office and administrative support Full spectrum of clinical services
18 Increased Pressures on cardiac surgery Patients Health System Surgeon These pressures are changing the current delivery system


19 Patient Pressures Increased Financial Pressures Increased co-pays and co-insurance More consumer behavior Quality Increased information about quality Increased value placed on objective quality Access Increased desire to have services close to home More emphasis on convenience More insured patients
20 Health system Pressures Financial pressures Decreased DRG payments Bundled Payments No reimbursement for complications Quality Increased reimbursement tied to quality Program Growth Adoption of new procedures and techniques (TAVR) Outreach Expand their reach Access new patient populations Pull tertiary care into major centers
21 Surgeon Pressures Financial pressures Decreased case load since Stenting/PCI boom Mean compensation in 2010 less than half of mean in 1990 without adjusting for inflation Increasing employment and loss of ancillary income Increasing emphasis on productivity Quality Increased transparency Increased pressure from Health System and Patients Not included in compensation Increasing Complexity Difficult to learn new skills Difficult to do-it-all
22 Patient High Quality Access/Convenience Financially affordable Care that is: High Quality Accessible Specialized Financially Sustainable Surgeon Quality Care Quality of Life Financially Rewarding Health System Financially sound High Quality New Programs Broad Delivery

23 Increased evidence based care, standardization, protocols Loss of Physician autonomy De-emphasis of personalized relationship with Physician Admitted to the Cardiothoracic Service; Rounding Physician EHRs are Data driven Increased emphasis of productivity Medical care is now wrvus Insufficient recognition of quality Just starting to tie to dollars to quality/bundled payments Weak data, measuring systems and analysis Does not recognize that all surgeons are not equal Widget maker mentality Docs vary in skill set and quality

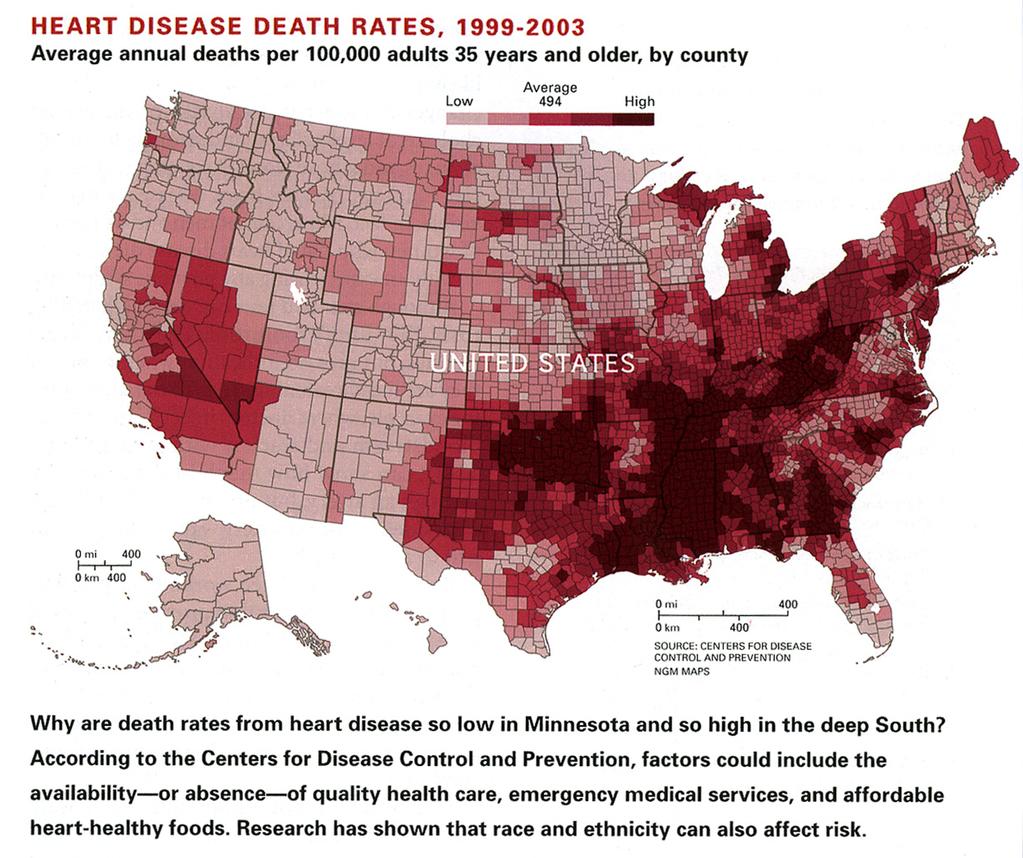
24 USA - Poor Value for our Healthcare Dollar

25 Affordable Care Act 2010 Poor value Unsustainable Uninsured burden Triple Aim Improving outcomes/quality Improving the patient experience Reducing costs
26 Quality Patient Safety Surgical Outcomes Avoidance of Complications Costs Cost per Case Supply Costs Length of Stay Un-reimbursed Costs Patient Experience Access and Convenience Satisfaction Affordability


27

28 5 YEAR AVERAGE ALL CARDIAC PROCEDURES CTSA STS National Average Mortality 2.0% 2.4% Complication Rate 37.2% 52.3% PostOp Length of Stay 6.4 days 9 days N=2,966


29 5 YEAR AVERAGE CABG PROCEDURES N= N= N= N= N=179 5-year average N=836 STS National Average Mortality 0.0% 0.7% 0.6% 1.7% 2.6% 1.4% 2.0% Major Complication Rate 9.3% 13.9% 14.7% 11.5% 13.6% 12.6% 13.0% Post- Procedure Length of Stay 7.1 days 6.0 days 5.8 days 5.8 days 6.6 days 6.3 days 6.8 days N=836
30 5 YEAR AVERAGE VALVE PROCEDURES Isolated Valve Cases CTSA STS National Average Mortality 2.0% 2.9% Major Complication 17.5% 18.2% Rate PostOp Length of Stay 5.8 days 8.1 days N=1,367


31 Standardization across the system Order Sets One set of orders for pre-op, post-op, telemetry transfer, transfusion, post-op A-fib, etc. Standardized care makes solving problems easier Standardized OR Protocols Same cardiac anesthesia approach Standardized techniques Cannulation sequence Chest tubes, wires Same Perfusion approach Same pump set-up, prime


32 Regular Meetings to review Protocols Surgeons meet quarterly Revise protocols/order sets Address surgeon outliers Trial changes in order sets M&M Conference Surgeons, Anesthesia and Perfusion Meet every six months Revise anesthesia/perfusion protocols Data Review of STS Anesthesia Module Review Blood Usage Review Ventilator times


33 Organized rounding Daily multidisciplinary rounds ICU and Telemetry Rounding surgeon of the day Rounding surgeon has first care rights If operating surgeon wants to change care then needs to call the rounding surgeon Surgeon Mentoring Hire new graduates Actively address quality fallouts through root cause analysis, outside peer review and individual surgeon mentoring


34 Active STS data management Collaborative process in real time Quarterly Meeting at each location Semi-Annual System STS meeting Online system wide metrics Deep dig on outliers CABG Process Improvement Team Multidisciplinary Cmte. looking only at ISO CABG Set quarterly goals Root cause analysis of fall-outs

35 Many things impact cost Patient factors Surgeon factors Hospital/System factors New scrutiny Cost per case Shifting of risk Bundled payment

36 Septicemia Post-Op Infection Post-Op Respiratory Distress Syndrome Reoperation Post-Op Stroke New-onset Hemodialysis Atrial Fibrillation 18 Source: Brown PP, ET al., The Frequency and Cost of Complications Associated with CABG Surgery: Results from the US Medicare Program, The Annals of Thoracic Surgery, :
37 Category Total Cost* Additive Cost Reason for Additive Cost Primary Complication Secondary Complication No Complications $26,056 $0 $0 $0 10,515 Atrial Fibrillation $38,100 $12,100 $2,700 $9,300 2,092 Mediastinitis $88,800 $62,700 $23,500 $39, Permanent Stroke $60,100 $34,100 $9,800 $24, Re-Op for Bleeding $46,100 $20,000 $4,000 $16, Prolonged Vent $66,700 $40,700 $25,700 $14,900 1,236 Renal Failure $75,100 $49,100 $22,900 $26, Operative Mortality $75,300 $49,200 $11,000 $38, Virginia Cardiac Surgery Quality Initiative (VCSQI), Speir et al. analyzed a data repository with clinical and billing data for 14,780 isolated CABG patients to estimate the additive costs of complications for the period of 2004 to N
38 CTSA Data Annual Savings Atrial Fibrillation 29.8% 11.8% $940,000 Renal Failure 6.9% 2.2% $897,000 Re-op for Bleeding 6.0% 0.9% $300,000 Readmission 11.3% 6.9% $312,000 Transfusions 43% 16% $512,000 Mortality 2.6% 0.7% unknown 87% 99% unknown Discharge Best Practice Medications Total Savings $2,961,000
39 Length of Stay Coronary Bypass Aortic Valve Replacement Mitral Valve Replacement LOS Reduction 2006 vs (days) Reduction X Cases 2014 (days) Mitral Valve Repair Valve + Coronary Other Total 1245 days
40 Category N ICU/CCU Day Non-ICU/CCU Day Average All stays 787,753 $2,801 $1,522 $2,162 CABG/CC s MC 612 $3,397 $3,117 $1,907 Valve s MC 1,220 $3,715 $3,208 $3, Source: Candrilli, S. et al. How Much Does a Hospital Day Cost? Poster Presentation at Annual Meeting of International Society of Pharmacoeconomics and Outcomes Research (ISPOR), May 20-24, Blended Average for non-icu Day $3, CTSA saved 1245 $3,163/day Annual Savings $1,968,968
41 CTSA actively works at efficiency Actively manage case load/work flow Stable OR throughput One room running after 3:00 50/50 mix of elective/urgent Distribute cases between surgeons to achieve Practice mgr., head PA collaborate daily to arrange OR schedule for maximal efficiency RamRod OR Nursing Efficiency Pre-op Communication about equipment/plan One open heart instrument set at all facilities Modular case/surgeon specific sets
42 CTSA actively works at communication Heart Team Communication Surgeons out a Pre-Brief for all cases goes to the whole Heart Team distribution list Nurses print and put up in the OR Monday RB 62 yo male for CABG/MAZE, 3V CAD, AF with EF35%, right radial A-line, on pump standard central cannulation/blood plegia, BIMA, left radial harvest, stapler for LAA, milrinone load on pump, epi to come off. Atricure OLL Clamp CVICU Sign out sheet goes from OR to CVICU with each patient Surgeon, Case, pre-op EF Current Drips and hemodynamic parameters Tracks resuscitation progress

43 Active case flow management Reduced pre-op LOS by 1.8 days Reduced OR nursing staff overtime by 50% OR Pre-brief with equipment list Reduced wasted disposables by 20% Reduced running for equipment during the case Reduced stress of not having equipment Designated rounding surgeon/multidisc rounds Reduced post-op LOS by 0.8 days
44 Restricted choice and variation in OR equipment and disposables across all programs Achieved Surgeon consensus on fewer choices and fewer vendors Collaborated with vendors to get preferred pricing for the health system in exchange for exclusive contracting Moved all items to consignment Resulted in streamlined inventory management, uniform inventory across the system
45 Action Reduced selection to three aortic and five venous cannulas Single Vendor for Vascular Grafts Single Vendor for EVH Dual Vendor Tissue valves, 80% guarantee to one vendor One Open Heart OR pack for all programs One Pump tubing set-up for all programs Savings Fewer than half as many cannulas to manage, no expired products $75/graft $179/kit $2600/valve $400/case $275/case AVR, Asc Aortic Graft with single vein graft = Savings of $3,529
46 The art of compromise: Cor-Knot device Auto-Knotting device Surgeon convenience item in most cases Incremental cost of $875/case Time savings used to justify its use Discussed Cor-Knot with the Health System Health System wanted no Cor-Knot use at all Surgeons wanted Cor-Knot for every case


47 Compromised on Cor-Knot for MIS cases only Cor-Knot in MIS avoids the use of a knot pusher (cost $147) Clinically knots better than a knot pusher True time savings over knot pusher

48 All locations cannot have all programs/procedures Examples VAD, TAVR Complex, expensive technology Inherently low to moderate volume Require an extensive support ecosystem Workshops Support personnel Economy of scale with more volume Concentrating specialty cases leads to higher volume and better outcomes

49 Collaborative decision with the Health system Must have reasonable Financial pro-forma Clinical volume Clinical expertise Equipment and workshop Support staff/infrastructure Not everyone will agree
50 St. Anthony Penrose Parkview Cath Volume Case Volume Meets NCDR Yes Yes No Expected Volume Surgical Expertise Cardiology Expertise Yes Yes Yes Yes Yes Yes Hybrid Room Yes Yes Yes Nurse Coordinator Yes Yes No
51 St. Anthony Penrose Parkview Cath Volume Case Volume Expected volume <20 Trauma Level 1 Level 2 Level 2 Critical Care Support Surgical Expertise Cardiology HF Program Hospital Support Yes Partial No Yes Yes No Yes Yes No Yes Yes No


52 CTSA Regional Cardiac Care Penrose Hospital Complex Cardiac Endo Aortic MIS Valve TAVR St. Anthony Hospital Complex Cardiac Endo Aortic MIS Valve TAVR VAD/ECMO Parkview Medical Center Routine Cardiac Surgery
 Sets the stage for success with Bundled")
53 Savings achieved through Reduced complications Reduced supply costs Reduced OR labor costs Centralizing expensive services Results Reduced cost per case by 30% Increased per case margin by 30% 3 of 4 most profitable cases in health system are CT Surgery >$10M increased annual profit (2006 versus 2014) Sets the stage for success with Bundled Payments

54 Emphasis on Patient Education Pt brochure In depth website Pt. resource guide 25 educational videos Pre-op video Timely clear communication Same day phone call return by NP All appts. within two weeks Extensive pre-op packet mailed before appointment Discharge phone follow-up 24/72 hrs.
55 94 th Percentile Patient Satisfaction 94 th percentile HealthGrades HCAP Scores th % in all categories
56 Local efforts that lower the bar for referral Problem Based Clinics PCP/ER convenience and transition of responsibility Regional efforts Cardiology outreach clinics Collaborate with out-of-town cardiologists CT Surgery outreach clinics
57 Valve Clinic (Cardiology + CT Surgery) Multidisciplinary clinic meets weekly Automatic referral with ECHO Criteria Direct PC referral NP coordinated clinic Aortic Disease Clinic (CT Surgery) Comprehensive evaluation, longitudinal surveillance, and treatment of aortic diseases. ER and PCP referral of incidental aortic disease findings Assumption of care/follow-up for aortic diseases
58 Atrial Fibrillation Clinic (EP + CT Surgery) EP NP initial evaluation Medical management/catheter ablation Hybrid Surgical management Congestive Heart Failure Clinic (Cardiology + CT Surgery) Multidisciplinary care Medical management, Pacer optimization, Rehab Surgery/VAD as needed Pulmonary Nodule Clinic (Pulmonary + CT Surgery) Multidisciplinary clinic for evaluation of lung nodules has reduced the time to diagnosis and time to treatment for lung cancer to less than half national average ER and PCP referral of incidental findings
59 CT Surgery outpatient clinics (no surgery) Done monthly in the cardiologist office See pre-op consultations and post-op patients Continuity of care for out of town patients Keeps ancillary testing locally Lowers bar for referral Strengthens cardiology relationship 40% of CTSA patients are from out of town None of the Outreach Cardiologists are employed by either health system

60 CT Surgery Center Cardiology Clinic Cath lab CT Surgery Clinic Cardiology Clinc Cath lab Cardiology Clinic
61 High Quality Reduced Costs Rich Patient Experience This has driven growth Patient Experience


62 15% year over year growth for 9 years
63 High Quality Reduced Costs Rich Patient Experience Are Surgeons happy? Is it sustainable? Patient Experience
64 Clinic Support CV Anesthesia Support OR Equipment Midlevel Support Clinical Support Internal Locums Admin Support Surgeons do Surgery Revenue Cycle Mgmt Group Financial Sharing Compensation Quality Control CME, Vacation Group Quality Incentives Disability, Benefits, 401k Outreach Clinic Growth Practice Growth Marketing Support Annual CME Meeting Recruitment and Retention Research Support CTSA Does it better than the Health System

65 CTSA provides surgeons with negotiating strength when dealing with the health system A collective voice Group versus individual contracts CTSA controls the patients Reputation Geographic footprint CTSA Outreach Clinics CTSA Direct Employer Contracting Professionally supported Own Admin, own attorneys, own FMV

66 Through these efforts and compromises surgeons achieve Better quality of life Focus on Clinical work/surgery Business is professionally handled Better case/call ratio Surgeons do >150 cases/year Take Q3-Q4 call Working at top of scale

67 Together we speak with a more powerful voice that we could ever achieve alone Get to know each other and help each other succeed Group Dinners, events Events with Midlevels Events with the OR/ICU teams Events with Anesth/Perfusion
68


69 This is what has worked for us, it may not work for you Things are always changing but high quality low cost care is always in demand
70


71 Questions

72 Surgeons Give: Clinical Autonomy Time to Program Development Time to Outreach Choice in Products and Vendors Surgeons Get: Better Workshops Better Equipment More Clinical Support Better Call support More cases Better earning/work ratio Better work/life balance
73 Hospitals Give: Financial Support Capital Investment Better Equipment Clinical Support Outreach Support Space Hospitals Get: Enhanced reputation More cases Increased market share Increased OR efficiency Cost savings Lower cost per case Shorter LOS Streamline supplies
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Developing a successful EP service line / practice
 Developing a successful EP service line / practice Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center The Ohio State University Evolution
Developing a successful EP service line / practice Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center The Ohio State University Evolution
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care
 Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
The Society of Thoracic Surgeons
 VIA EMAIL Practice Improvement and s Management Support (PIMMS) s Support The STS Headquarters 633 N Saint Clair St, Floor 23 Chicago, IL 60611-3658 (312) 202-5800 sts@sts.org STS Washington Office 20
VIA EMAIL Practice Improvement and s Management Support (PIMMS) s Support The STS Headquarters 633 N Saint Clair St, Floor 23 Chicago, IL 60611-3658 (312) 202-5800 sts@sts.org STS Washington Office 20
Changing Paradigm of Cardiovascular Care- Service Line vs Departmental
 Changing Paradigm of Cardiovascular Care- Service Line vs Departmental Michael A. Acker, MD William Measey Professor of Surgery Chief of Cardiovascular Surgery Director of Penn Medicine Heart and Vascular
Changing Paradigm of Cardiovascular Care- Service Line vs Departmental Michael A. Acker, MD William Measey Professor of Surgery Chief of Cardiovascular Surgery Director of Penn Medicine Heart and Vascular
The Day of Your TAVR
 UW MEDICINE PATIENT EDUCATION The Day of Your TAVR What to expect This handout describes what to expect on the day of your transcatheter aortic valve replacement (TAVR). It includes where to check in at
UW MEDICINE PATIENT EDUCATION The Day of Your TAVR What to expect This handout describes what to expect on the day of your transcatheter aortic valve replacement (TAVR). It includes where to check in at
About the Report. Cardiac Surgery in Pennsylvania
 Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Strategies for an Effective Structural Heart Program: Current and Future Considerations
 Strategies for an Effective Structural Heart Program: Current and Future Considerations Eric L. Sarin, MD Co-Director, Structural Heart and Valve Program Co-Director, Cardiovascular Research Inova Heart
Strategies for an Effective Structural Heart Program: Current and Future Considerations Eric L. Sarin, MD Co-Director, Structural Heart and Valve Program Co-Director, Cardiovascular Research Inova Heart
Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068
 Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068 Mission To provide excellent care in a critical care environment and to design and implement tools which maximize the utilization of all
Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068 Mission To provide excellent care in a critical care environment and to design and implement tools which maximize the utilization of all
Integrated Cardiovascular Care Private Practice Perspective
 Integrated Cardiovascular Care Private Practice Perspective Florida Hospital Cardiovascular Institute Kevin Accola, M.D., F.A.C.S. CARDIOVASCULAR SURGEONS, P.A. Program Director, Valve Center of Excellence
Integrated Cardiovascular Care Private Practice Perspective Florida Hospital Cardiovascular Institute Kevin Accola, M.D., F.A.C.S. CARDIOVASCULAR SURGEONS, P.A. Program Director, Valve Center of Excellence
The Changing Face of the Employer-Provider Relationship
 The Changing Face of the Employer-Provider Relationship Cleveland Clinic Market & Network Services Shannon Schwartzenburg August 21, 2013 Cleveland Clinic Snapshot Group practice model - 120 specialties
The Changing Face of the Employer-Provider Relationship Cleveland Clinic Market & Network Services Shannon Schwartzenburg August 21, 2013 Cleveland Clinic Snapshot Group practice model - 120 specialties
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Clinical Fellowship: Cardiac Anesthesia
 Anesthesia and Perioperative Medicine Western University Cardiac Anesthesia Program Director Dr. Anita Cave Please visit the Cardiac Anesthesia Fellowship site for most up-to-date information: http://www.schulich.uwo.ca/anesthesia/education/fellowship/fellowships_offered/cardiac_anesthesia.html
Anesthesia and Perioperative Medicine Western University Cardiac Anesthesia Program Director Dr. Anita Cave Please visit the Cardiac Anesthesia Fellowship site for most up-to-date information: http://www.schulich.uwo.ca/anesthesia/education/fellowship/fellowships_offered/cardiac_anesthesia.html
The transcatheter aortic valve replacement (TAVR)
") TM, LLC Inside One of the Nation s First Transcatheter Aortic Valve Replacement Hospitals Interview by Stephanie Wasek This article features an interview with Lisa Walsh, RN, clinical research nurse supervisor
TM, LLC Inside One of the Nation s First Transcatheter Aortic Valve Replacement Hospitals Interview by Stephanie Wasek This article features an interview with Lisa Walsh, RN, clinical research nurse supervisor
Wholehearted HEALTH CARE
 Wholehearted HEALTH CARE Chest Pain Center and Cardiovascular Intensive Care Unit: The future of cardiac care at Bon Secours St. Francis Health System 1 2 Quality Meets Compassion The Bon Secours St. Francis
Wholehearted HEALTH CARE Chest Pain Center and Cardiovascular Intensive Care Unit: The future of cardiac care at Bon Secours St. Francis Health System 1 2 Quality Meets Compassion The Bon Secours St. Francis
Buchanan, 1996; Knaus, Felton, Burton, Fobes, & Davis 1997, J. of Nsg Administration
 Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
Quality and Health Care Reform: How Do We Proceed?
 Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
EP LAB BENCHMARKING WHITEPAPER
 EP LAB BENCHMARKING WHITEPAPER C. DeLaughter, MD; K. Heist, MD, PhD; B.Kind, HRSCS in sights EP LAB BENCHMARKING EXPERT PANEL INTRODUCTION C. DeLaughter, MD; K. Heist, MD, PhD; B.Kind, HRSCS In early 2014,
EP LAB BENCHMARKING WHITEPAPER C. DeLaughter, MD; K. Heist, MD, PhD; B.Kind, HRSCS in sights EP LAB BENCHMARKING EXPERT PANEL INTRODUCTION C. DeLaughter, MD; K. Heist, MD, PhD; B.Kind, HRSCS In early 2014,
Domain 5 Cardiothoracic Standards RCoA Accreditation 2017
 1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
MOC Part IV: Your Guide to Making it Happen.
 MOC Part IV: Your Guide to Making it Happen. Joseph P. Drozda, Jr., MD, F.A.C.C. Mercy, MO Paul D. Varosy, MD, F.A.C.C., FAHA, FHRS University of Colorado Denver School of Medicine, CO Disclosures Course
MOC Part IV: Your Guide to Making it Happen. Joseph P. Drozda, Jr., MD, F.A.C.C. Mercy, MO Paul D. Varosy, MD, F.A.C.C., FAHA, FHRS University of Colorado Denver School of Medicine, CO Disclosures Course
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Clinical Program Cost Leadership Improvement
 Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
2018 Collaborative Quality Initiative Fact Sheet
 2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan
 BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers. Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care
 Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care Conclusions New paradigm has shifted towards team-based
Collaboration of the Hybrid AF Patient: Role of Advanced Practice Providers Jennifer Walker, RN, MSN, ANP-BC UNC Center for Heart and Vascular Care Conclusions New paradigm has shifted towards team-based
Nursing Unit Descriptions UCHealth Memorial Hospital Central
 Nursing Unit Descriptions UCHealth Memorial Hospital Central ACUTE CARE SERVICES Neuroscience 5C Neuroscience is a 24-bed unit with all private rooms for our patients. The department specializes in acute
Nursing Unit Descriptions UCHealth Memorial Hospital Central ACUTE CARE SERVICES Neuroscience 5C Neuroscience is a 24-bed unit with all private rooms for our patients. The department specializes in acute
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model. Rome H. Walker MD February 28, 2008
 Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Physician s Advantage The latest in clinical and patient care advances at Lakeland HealthCare
 Physician s Advantage The latest in clinical and patient care advances at July 2009 A2 Lakeland Cardiac Surgery: a Model for Quality and Efficiency A4 Lakeland Recognized for Cardiac Excellence CARDIO
Physician s Advantage The latest in clinical and patient care advances at July 2009 A2 Lakeland Cardiac Surgery: a Model for Quality and Efficiency A4 Lakeland Recognized for Cardiac Excellence CARDIO
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience
 Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
CARDIAC CARE UNIT CARDIOLOGY RESIDENCY PROGRAM MCMASTER UNIVERSITY
 CARDIAC CARE UNIT CARDIOLOGY RESIDENCY PROGRAM MCMASTER UNIVERSITY ROTATION SUPERVISOR: DR. CRAIG AINSWORTH OVERVIEW The Cardiac Care Unit (CCU) at the Hamilton General Hospital is a busy 14-bed, Level
CARDIAC CARE UNIT CARDIOLOGY RESIDENCY PROGRAM MCMASTER UNIVERSITY ROTATION SUPERVISOR: DR. CRAIG AINSWORTH OVERVIEW The Cardiac Care Unit (CCU) at the Hamilton General Hospital is a busy 14-bed, Level
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
What s Wrong with Healthcare?
 What s Wrong with Healthcare? Dan Murrey, MD, MPP Chief Executive Officer Agenda What s wrong with healthcare in the US? What would make it better? How can you help? What s wrong with US healthcare? What
What s Wrong with Healthcare? Dan Murrey, MD, MPP Chief Executive Officer Agenda What s wrong with healthcare in the US? What would make it better? How can you help? What s wrong with US healthcare? What
EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS
 EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS PURPOSE The "EuroELSO Guidelines for Training & Continuing Education of ECMO Physicians" is a document developed by the Extracorporeal
EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS PURPOSE The "EuroELSO Guidelines for Training & Continuing Education of ECMO Physicians" is a document developed by the Extracorporeal
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle
 Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle TBD 2015 The intent of the Coronary Artery Bypass Graft Surgical
Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle TBD 2015 The intent of the Coronary Artery Bypass Graft Surgical
Intermediate Coronary Care Unit Rotation
 1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
ACHP Affordability Discussion Specific Cost Savings Strategies
 ACHP Affordability Discussion Specific Cost Savings Strategies December 17, 2014 ACHP News and Upcoming Events Recent Affordability Profiles: Asthma Home Visiting and Case Management program (UCare) Behavioral
ACHP Affordability Discussion Specific Cost Savings Strategies December 17, 2014 ACHP News and Upcoming Events Recent Affordability Profiles: Asthma Home Visiting and Case Management program (UCare) Behavioral
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR.
 Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost
 Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Atrial Fibrillation: 2017 Update & Specialty Clinic Focus
 Atrial Fibrillation: 2017 Update & Specialty Clinic Focus October 21, 2017 Gopi Dandamudi, MD FHRS System Medical Director, IUH Cardiac EP Program Director, IUH Atrial Fibrillation Center Assistant Professor
Atrial Fibrillation: 2017 Update & Specialty Clinic Focus October 21, 2017 Gopi Dandamudi, MD FHRS System Medical Director, IUH Cardiac EP Program Director, IUH Atrial Fibrillation Center Assistant Professor
Perioperative Surgical Home
 None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL
 ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL Presented by: Joseph F. Corfits, Jr. FHFMA, Chief Financial Officer Unity Point Health Des Moines Stephen G. Taylor, MD Des Moines Orthopaedic
ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL Presented by: Joseph F. Corfits, Jr. FHFMA, Chief Financial Officer Unity Point Health Des Moines Stephen G. Taylor, MD Des Moines Orthopaedic
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
MSTCVS CQI: Michigan Society of Thoracic & CardioVascular Surgeons
 MSTCVS CQI: Michigan Society of Thoracic & CardioVascular Surgeons Michigan Data Group Traverse City: August 2012 BCBSM CQI - 2006 Outline Overview Who am I? What is MSTCVS? What do We Do? Why am I Here?
MSTCVS CQI: Michigan Society of Thoracic & CardioVascular Surgeons Michigan Data Group Traverse City: August 2012 BCBSM CQI - 2006 Outline Overview Who am I? What is MSTCVS? What do We Do? Why am I Here?
CIGNA Collaborative Accountable Care
 CIGNA Collaborative Accountable Care Connecting in ways that help make achieving health easier, more effective and more affordable October 14, 2016 Michael L. Howell, MD, MBA, FACP Market Medical Executive/Sr.
CIGNA Collaborative Accountable Care Connecting in ways that help make achieving health easier, more effective and more affordable October 14, 2016 Michael L. Howell, MD, MBA, FACP Market Medical Executive/Sr.
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE)
") SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE) Discussion Draft August 6, 2017 Horty, Springer & Mattern, P.C. 250979.8 ONGOING PROFESSIONAL
SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE) Discussion Draft August 6, 2017 Horty, Springer & Mattern, P.C. 250979.8 ONGOING PROFESSIONAL
The Partner of Choice for Leading Health Systems. Learning Objectives. 45+ Health System Partners 750K+ Surgical Procedures $1.
 http://www.advocatehealth.com/images/logo_advocatehealthcare.gif Co-Management: Successfully Improving Care Along the Surgical Continuum Gerald Biala, SCA Senior Vice President of Perioperative Services
http://www.advocatehealth.com/images/logo_advocatehealthcare.gif Co-Management: Successfully Improving Care Along the Surgical Continuum Gerald Biala, SCA Senior Vice President of Perioperative Services
Long-Term Fate of Patients Discharged to Extended Care Facilities After Cardiovascular Surgery
 Long-Term Fate of Patients Discharged to Extended Care Facilities After Cardiovascular Surgery James R. Edgerton, MD, Morley A. Herbert, PhD, Cecile Mahoney, BS, Drew Armstrong, MS, Todd M. Dewey, MD,
Long-Term Fate of Patients Discharged to Extended Care Facilities After Cardiovascular Surgery James R. Edgerton, MD, Morley A. Herbert, PhD, Cecile Mahoney, BS, Drew Armstrong, MS, Todd M. Dewey, MD,
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
AirStrip ONE Cardiology
 AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
Transplant Resource Guide
 Transplant Resource Guide The Transplant Resource Guide (TRG) and the supporting tools provide strategies, concepts and resources to enhance transplant program quality and value in our dynamic environment.
Transplant Resource Guide The Transplant Resource Guide (TRG) and the supporting tools provide strategies, concepts and resources to enhance transplant program quality and value in our dynamic environment.
Transforming to Value: One Way Forward
 Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Developing a Trauma Center
 Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
PATIENT CENTERED QUALITY FOCUSED
 PATIENT CENTERED QUALITY FOCUSED PROCIRCA 1 WHETHER FINDING SOLUTIONS TO CLINICAL CHALLENGES OR DEVELOPING NEW BUSINESS MODELS TO ENHANCE PERFORMANCE, PROCIRCA IS COMMITTED TO PROVIDING SOLUTIONS THAT
PATIENT CENTERED QUALITY FOCUSED PROCIRCA 1 WHETHER FINDING SOLUTIONS TO CLINICAL CHALLENGES OR DEVELOPING NEW BUSINESS MODELS TO ENHANCE PERFORMANCE, PROCIRCA IS COMMITTED TO PROVIDING SOLUTIONS THAT
Introduction to Value-Based Health Care Delivery
 Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Getting Operational Leaders on Board to Deliver the Triple Aim
 Session #37 Getting Operational Leaders on Board to Deliver the Triple Aim Lauren Anthony, MD System Medical Director Allina Health Clinical Laboratories Learning Objectives Recognize the three most important
Session #37 Getting Operational Leaders on Board to Deliver the Triple Aim Lauren Anthony, MD System Medical Director Allina Health Clinical Laboratories Learning Objectives Recognize the three most important
OVERALL GOALS & OBJECTIVES FOR EACH RESIDENT LEVEL FIRST-YEAR RESIDENT. Patient Care
 OVERALL GOALS & OBJECTIVES FOR EACH RESIDENT LEVEL FIRST-YEAR RESIDENT Patient Care 1) Demonstrate proficiency in the preoperative and postoperative care of surgical patients. 2) Demonstrate thorough,
OVERALL GOALS & OBJECTIVES FOR EACH RESIDENT LEVEL FIRST-YEAR RESIDENT Patient Care 1) Demonstrate proficiency in the preoperative and postoperative care of surgical patients. 2) Demonstrate thorough,
2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
K-HEN Acute Care/Critical Access Hospitals Measures Alignment with PfP 40/20 Goals AEA Minimum Participation Full Participation 1, 2
 Outcome Measure for Any One of the Following: Outcome Measures Meeting Either A or B: Adverse Drug Events (ADE) All measures are surveillance data Hospital Collected Anticoagulant (ADE-12) Opioid (ADE-111)
Outcome Measure for Any One of the Following: Outcome Measures Meeting Either A or B: Adverse Drug Events (ADE) All measures are surveillance data Hospital Collected Anticoagulant (ADE-12) Opioid (ADE-111)
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
Successful Integration of Advanced Practice Providers into Hospitalist Practice
 Successful Integration of Advanced Practice Providers into Hospitalist Practice Tracy E. Cardin, ACNP, SFHM Population Over Age 65 Doubles by 2030 United States Population Projection Percent Growth from
Successful Integration of Advanced Practice Providers into Hospitalist Practice Tracy E. Cardin, ACNP, SFHM Population Over Age 65 Doubles by 2030 United States Population Projection Percent Growth from
THE ROLE OF THE APP IN CARDIAC SURGERY. Mark Morosco PA-c Chief PA cardiac surgical services Southcoast Hospital Group Fall River,MA
 THE ROLE OF THE APP IN CARDIAC SURGERY Mark Morosco PA-c Chief PA cardiac surgical services Southcoast Hospital Group Fall River,MA OBJECTIVES Who are APPs PA history Np history APP advancement of clinical
THE ROLE OF THE APP IN CARDIAC SURGERY Mark Morosco PA-c Chief PA cardiac surgical services Southcoast Hospital Group Fall River,MA OBJECTIVES Who are APPs PA history Np history APP advancement of clinical
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Linking Supply Chain, Patient Safety and Clinical Outcomes
 Premier s Vision for High Performing Healthcare Organizations: Linking Supply Chain, Patient Safety and Clinical Outcomes Joe M. Pleasant Sr. VP and CIO Premier Inc. Global GS1 Conference Hong Kong October
Premier s Vision for High Performing Healthcare Organizations: Linking Supply Chain, Patient Safety and Clinical Outcomes Joe M. Pleasant Sr. VP and CIO Premier Inc. Global GS1 Conference Hong Kong October
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
STEMI RECEIVING CENTER
 Monterey County EMS System Policy Policy Number: 5150 Effective Date: 5/1/2012 Review Date: 12/31/2016 STEMI RECEIVING CENTER I. PURPOSE To define requirements for designation as a Monterey County STEMI
Monterey County EMS System Policy Policy Number: 5150 Effective Date: 5/1/2012 Review Date: 12/31/2016 STEMI RECEIVING CENTER I. PURPOSE To define requirements for designation as a Monterey County STEMI
Accomplishments Fiscal Year UPMC Passavant
 Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
TeleCardiology Platform
 TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Robot-Assisted Surgeries A Project for CADTH, a Decision for Jurisdictions
 Robot-Assisted Surgeries A Project for CADTH, a Decision for Jurisdictions 2012 CADTH Symposium Panel Discussion Dr. Janice Mann Mr. Michel Boucher Dr. Nina Buscemi We NEED this! What is a Surgical Robot?
Robot-Assisted Surgeries A Project for CADTH, a Decision for Jurisdictions 2012 CADTH Symposium Panel Discussion Dr. Janice Mann Mr. Michel Boucher Dr. Nina Buscemi We NEED this! What is a Surgical Robot?
Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD
 WHITE PAPER Accelero Health Partners, 2013 Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD ABSTRACT The volume of total hip and knee replacements
WHITE PAPER Accelero Health Partners, 2013 Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD ABSTRACT The volume of total hip and knee replacements
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
Review for Required Monitors
 Review for Required Monitors The Joint Commission Hospital Accreditation Manual, 2009 Medicare Conditions of Participation, Hospitals Update: February 2009 Indicator / Monitor Restraint, Medical (non-specific
Review for Required Monitors The Joint Commission Hospital Accreditation Manual, 2009 Medicare Conditions of Participation, Hospitals Update: February 2009 Indicator / Monitor Restraint, Medical (non-specific
An economic - quality business case for infection control & Prof. dr. Dominique Vandijck
 An economic - quality business case for infection control & prevention @VandijckD Prof. dr. Dominique Vandijck What you/we all know, (hopefully) but do our healthcare executives, and politicians know this?
An economic - quality business case for infection control & prevention @VandijckD Prof. dr. Dominique Vandijck What you/we all know, (hopefully) but do our healthcare executives, and politicians know this?
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Lisa M. Soltis, MSN, RN-BC, APRN, PCCN, CCRN-CSC-CMC, CCNS, FCCM
 2739 Laurelcherry Street, Raleigh, NC 27612 (919) 621-3921 Cell Lisa.Soltis@unchealth.unc.edu FUNCTIONAL SUMMARY Clinical Expert in Cardiovascular surgical procedures, processes and policies. Active advocate
2739 Laurelcherry Street, Raleigh, NC 27612 (919) 621-3921 Cell Lisa.Soltis@unchealth.unc.edu FUNCTIONAL SUMMARY Clinical Expert in Cardiovascular surgical procedures, processes and policies. Active advocate
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
Clinical and Financial Benefits of IT Implementation
 Clinical and Financial Benefits of IT Implementation October 24, 2014 Replace text box with chapter logo (on all master slides) Who Is HIMSS Analytics? A subsidiary of HIMSS We collect data on what information
Clinical and Financial Benefits of IT Implementation October 24, 2014 Replace text box with chapter logo (on all master slides) Who Is HIMSS Analytics? A subsidiary of HIMSS We collect data on what information
W. Douglas Weaver, MD, MACC. American College of Cardiology SENATE FINANCE COMMITTEE
 Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
Physician Compensation Directions and Health Reform. July 2017
 Physician Compensation Directions and Health Reform July 2017 Speaker Introduction Wayne Hartley Vice President, AMGA Consulting Over 20 Years of Medical Group & Consulting Experience Allina Health, Minneapolis,
Physician Compensation Directions and Health Reform July 2017 Speaker Introduction Wayne Hartley Vice President, AMGA Consulting Over 20 Years of Medical Group & Consulting Experience Allina Health, Minneapolis,
Curriculum Cardiac Catheterization
 Curriculum Cardiac Catheterization Description of Rotation or Educational Experience The goals of this rotation are for the cardiology fellow to develop effective technical skills in the performance of
Curriculum Cardiac Catheterization Description of Rotation or Educational Experience The goals of this rotation are for the cardiology fellow to develop effective technical skills in the performance of