Successful Integration of Advanced Practice Providers into Hospitalist Practice
|
|
|
- Ariel Cole
- 5 years ago
- Views:
Transcription
1 Successful Integration of Advanced Practice Providers into Hospitalist Practice Tracy E. Cardin, ACNP, SFHM Population Over Age 65 Doubles by 2030 United States Population Projection Percent Growth from ,695,904 71,453, Year Total Population 65+ Supply of Physicians 1
2 Language is powerful Appropriate terms: 1. Nurse Practitioner (NP) 2. Physician Assistant (PA) 3. Advanced practice nurse (APN) 4. Advanced practice provider (APP) What not to say Physician Extender Midlevel provider Nurse Non Physician Provider Physician s Assistant 2






3 Different Types of NPs Acute Care, Family, Adult APRN Consensus Work Group & the National Council of State Boards of Nursing APRN Advisory Committee 3
4 Resources Nurse Practitioners: American Academy of Nurse Practitioners National Council State Boards of Nursing Physician Assistants: American Association of Physician Assistants National Commission on Certification of Physician Assistants What can an NP/PA do? Admit patients Do procedures Discharge patients Succeed in administrative roles Manage patients Follow up phone calls Surgical co-management Diagnose Treat Prescribe Participate in hospital wide committees Play nice with nurses and ER Cross cover Triage Train and onboard new employees Hold family meetings Provide end of life care 4
5 Landscape evaluation Are you ready? Make sure you understand the problem you are trying to solve Evaluate by-laws State regulations Market for NP/Pas Culture Onboarding: The three P s Provider-are they new grads vs old hands Patients-are they SAPs or lower acuity Periphery-is this a new concept? Or does your system/hospital have experience with NP/PA providers All of these facts drive the duration/intervention of onboarding 5





6 Current Strategies Paired rounding Admitting Observation unit Consultant Cross Coverage Triage Telemedicine Paired rounding Results Very successful Safe, efficient Works for new NP/PA onboarding along with more experienced NP/Pas High satisfaction for both NP/PA and MD Key factors Physician Buy in Right provider for the pright 6
7 Paired rounding Pros increased MD satisfaction Increased billing, patient encounters More eyes on patients Cons NP/PAs can work different hours than MDs Resentment How will you cover when APP not there? Duplication of work Admitting Role Results Shift coverage from 7a-2am Success in absorbing both early am and late afternoon admissions Manages peak admissions in cost effective ways NP/PA role ownership May help with throughput Key Factors Allows non-admitting staff to focus on patient care, etd Co-signature by MD based on hospital bylaws Optional capture of shared visit billing 7
8 Admitting Can help with ER/HM interface Can utilize a less expensive provider to get patients tucked in May not be a super satisfying role long term for NP/PA provider Observation Unit Results Becoming more common High autonomy for NP/PA Great role ownership High levels of patient satisfaction Key Factors Need to have high functioning NP/PA Designated MD available when necessary Hospital bylaws may drive oversight 8
9 Observation Short stay, disease-specific Pros Great autonomy MDs can focus on higher acuity patients Great NP/PA satisfaction Lower cost-the sweet spot Cons Coverage when APP away Hard for MD to jump in/out when APP needs input Optimization Occurs when skill set is match for clinical need = less supervision, less cost How to approach: Increase complexity of patients on the physician side. Decrease supervision. 9
10 Physician Oversight 5 10% 10 15% 15 20% Uncomplicated patient Complex Experienced NP/PA New Grad NP/PA Physician oversight: No free lunch Need to recognize oversight as valued work: Direct pay for role Decrease physician census Attribute some portion of work generated by NP/PA to physician 10
11 Innovative Leverage of NP/PAs Consultant Manages census of only consults Continuity for surgical partners Becomes expert Cross coverage From home/in-house or overnight Off loads cc from admitting providers High functioning NP/PA Point of contact for medicine service Triage Triages all admissions from ED Provider to provider call for all outside admssions Post hospital discharge follow up Telemedicine Way of leveraging NP/PA providers when physicians are scarce and census is low Used in a variety of settings, mental health, critical access hospitals Difficulties with regulations/billing-varies from state to state You will see growth here 11
12 New Directions NP/PA productivity Months New Grad Productivity Old Hand Productivity 0-3 < 20% 60% % 80% % 100% % plus 100% 12
13 Will take a year to get to steady state. Plan for: Training Ramp up of productivity Physician oversight Setting Up Expectations Unwritten Agreement MD and APP have different ideas and expectations of roles, autonomy, professional growth, scope of practice 13


14 Retention How can I keep my APPs happy? Compensation, vacation, benefits Professional growth Treat like members of team Karaoke! Trends in NP/PA hiring 28 14

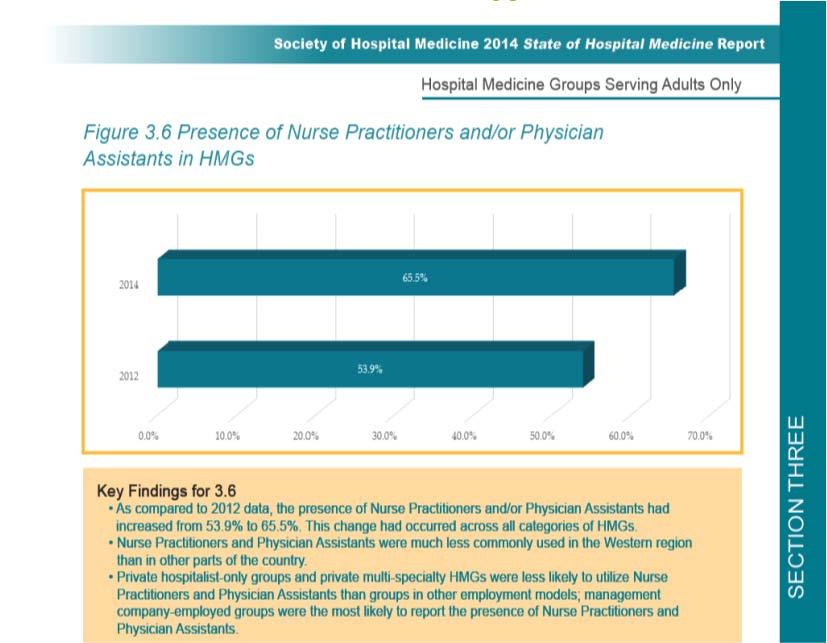
15 Trends in utilization 15






16 How NP/PA Services are billed Liability Seventeen years of observation suggest that, if anything, PAs and NPs may decrease liability Probability of making a malpractice payment was 12 times less for Pas, and 24 times less for APNs Trend analysis suggests the rate of malpractice payments for all three groups has been steady and consistent with the growth in the numbers of providers. Mean MD payment was 1.7 times greater than PAs and 0.9 times that of APNs 16
17 Questions 17
18 Admitter cont: If you are hiring NP/PA to increase volume-then measure volume with a volume metric Admitter May increase total day team volume Have to include some physician oversight time 18
19 Need an extra body: can I do it for less? Will take a year to get to steady state May note decreased productivity at first Subsequently may see decreased cost Factor in physician oversight Productivity Common measures: Encounters Limitations include whether subsequent visit or admission, each encounter looks the same. RVU-relative value unit Held constant by the payer Professional billing fee based metrics Revenue How does one account for different payers? 19
20 Productivity What is Productivity? Amount of goods or services produced with one hour of labor How do you assess productivity? Does your measurement really assess productivity What goods or services are you measuring? Productivity Commonly used measures have limitations: Not really measures of traditional productivity Do not adequately deal with team based care (co-management, cross cover, follow up, etc.) Measuring with these is better than not measuring anything 20
21 Cost: What is cost of NP/PA? Compensation + fringe(know your fringe rate) Hiring Training Malpractice Physician oversight - more later Compensation: Salary Use a similar method as for physicians National Benchmarks Local competitors Markets are local Inpatient providers with some markup Account for off-hours premium SHM salary data 21
22 Revenue Streams Professional Fees Hospital Transfers for: Coverage for work of the day Targets or incentives for: Productivity, safety, quality, experience, efficiency Contractual arrangements Billing Most services billed by a physician to Medicare are also covered when performed by NP/PA. Medicare Part A covers facility fees, supply costs. Medicare Part B covers professional services and durable medical equipment. 22
23 Billing: How to for hospital employed NP/PA Be included in the hospital s cost report and covered by facility Part A payment Not be included in hospital cost report and be billed under Part B Billing: How to for hospital employed NP/PA Part B services must be billed under NP/PA NPI number to be reimbursed at 85% of the physician fee schedule, without direct and documented physician involvement. Part B services billed under the physicians NPI number are reimbursed at 100% depending on the degree of involvement and documentation. 23
24 Billing: Independent hospital practices All services are billed under Part B. NP/PAs get 85% of the physician fee schedule. Can bill at 100% based on physician s level of interaction, decision making, based on documentation. Billing: Private insurance Contact the payor. Get (in writing) the representative s name. Obtain the written policy/contract. Identify specific issues of reimbursement. 24
25 Billing: Shared visit PA/NP and physician must be employed by the same hospital, group practice or the same employer. MD must provide face-to-face time. MD must document involvement in a shared visit. Only applies to E/M visit, does not apply to initial consultation or procedures. Billing: Shared visit Bill under physician for 100% reimbursement if the MD: Personally examined the patient Reviewed the documentation Participated in the medical decisions Documented the physician involvement 25
26 Revenue:Hospital funds transfer Volume Quality Safety Experience Efficiency Is this a good ROI? Incremental revenues>incremental costs Compare ratios to baseline total revenue/total costs including all revenues Incremental revenues=incremental costs Neutral, but project year-to-year change Incremental revenues<incremental costs Re-calculate and pro-rate funds flows transfer across the new FTE 26
27 Is this a good ROI? From whose perspective? Hospital funds flow transfers are usually not done to incentivize greater professional fees Can you demonstrate: Lower hospital costs Lower LOS, decreased penalty, etc. Higher hospital revenues Value Based Purchasing If your NP/PA is targeting these improvements, measure their effect as best you can Do NP/PAs positively affect revenue at reduced cost? NP/PA FTE lower cost than MD FTE Manage the care of patients that don t need a physician at the bedside Coordinate the process of care Can augment practice productivity Can be used to maximize hospital funds flow Services reimbursed by Medicare/Insurers 27
28 Admitter: Volume Day team has cap of 32 Average AM census 24 patients Average 10 potential admissions during day/evening and 6 night Discharge average 10 per day Potential loss of 8 admissions/day Can an admitter solve your problem? Admitter: Volume Admitter from 2pm-10pm (match admission flow) 4 days per week Average 8-10 admissions/shift Overall increase in admissions 6-8/shift (physician oversight) NP/PA does 4*9*46 = 1656 admissions/year Yearly increase in volume= 4*7*46= 1288 (all admissions) 28
29 Admitter Day team target census of 30 (2 providers) Average AM census 32 patients Average 6 admissions during day/evening and 6 night Discharge average 12 per day Each provider averaging 16 old patients, discharging 6 of them and admitting 3 news during daytime shift Can an admitter solve your problem? Admitter Admitter from 2pm-10pm (match admission flow) 4 days per week Average 8-10 admissions/shift NP/PA does 4*9*46 = 1656 admissions/year Overall increase in admissions = 0 What are you trying to fix: Physician satisfaction Turnover LOS 29
30 Problem #2: I need more people Unable to find enough physicians Can I add people for less money? I need more people Assess like an MD but recognize differences Target productivity. Evaluate cost, should be lower with NP/PA Factor in physician oversight 30
31 Physician type role Physician look-alike Same patient mix Estimate 85%-100% of volume NP/PA:Physician Physician oversight requirements higher Targeted patient population Low complexity High touch Physician oversight requirements less Evaluating this model Revenue/cost ratios should be better than adding additional physicians (if available) If unable to hire additional physicians, if revenue/cost ratios worse, than this needs to be seen as a cost of doing business for you If revenue/cost ratios similar and physicians are scarce but available: Would you rather have top of the class NP/PA or bottom of the class physician 31
32 Readmission problems First identify the problem population. NP/PA can provide: Improved care coordination Improved communication Improved follow up Total patient experience Deploy the NP/PA with the most at-risk population. Changing landscape of penalties/rewards Not just a simple formula anymore. Biggest drain right now is simply LOS - if DRG based population. In future need to worry about penalties and rewards. 32
33 Optimize financial model MD sees all patients, bills 100%, NP/PA carries out plan of care. MD would have to be 70% more efficient (about the cost of the NP/PA) to cover cost of NP Optimize financial model Can retain MD. Can increase productivity - allowing physician to bill/see more patients. But, MD would have to go from seeing 10 patients to 17 patients in order to totally defray cost of NP/PA 33
34 Another Optimization model Utilize NP/PA in a specific and limited role, i.e. Observation Unit NP/PA would see same volume as a physician, but cost less. Don t need to pay for physician oversight But, there are start up inefficiencies to NP/PA that are not there with physician. Dollars About more than money Need to look at quality Efficiency Measure those things at the beginning of implementation 34
35 NP/PA benefits Can help with patient experience problems - this is difficult to measure LOS Quality Readmissions Conclusion NP/PA additions can augment hospitalist practice in a variety of ways Consider the problem you are trying to solve before hiring Optimize skill set with patient population to reduce MD oversight 35
36 Changing landscape of penalties/rewards Not just a simple formula anymore Biggest drain right now is simply LOS-if DRG based population In future need to worry about penalties, and rewards NP/PA benefits Can help with patient experience problems-this is difficult to measure LOS Quality Readmissions 36
37 Dollars More than about money Need to look at quality Efficiency Measure those things at the beginning of implementation Compensation Salary alone Salary plus shared savings program Salary plus productivity incentive Patient encounters, RVU, patient satisfaction 37
38 Salary Look at National Benchmark Similar to way you figure hospitalist salary Call local people-remember, markets are local Return on investment Costs less than an MD FTE Manage the care of patients that don t need a physician at the bedside Coordinate the process of care Can augment practice productivity Services reimbursed by Medicare/Insurers 38
39 Billing Most services billed by a physician to Medicare are also covered when performed by NP/PA. Medicare Part A covers facility fees, supply costs Medicare Part B covers professional services and durable medical equipment How to bill for hospital employed NP/PA Be included in the hospital s cost report and covered by facility Part A payment Not be included in hospital cost report and be billed under Part B 39
40 Hospital employees billing continued Part B services must be billed under NP/PA NPI number to be reimbursed at 85% of the physician fee schedule, without direct and documented physician involvement. Part B services billed under the physicians NPI number are reimbursed at 100% depending on the degree of involvement and documentation Hospital setting-shared visits PA/NP and physician must be employed by the same hospital, group practice or the same employer MD must provide face to face time MD must document involvement in a shared visit. Only applies to E/M visit, does not apply to initial consultation, procedures. 40
41 Shared visit-continued Bill under physician for 100% reimbursement if: MD personally examined the patient Reviewed the documentation Participated in the medical decisions Documented the physician involvement. Independent hospital practices/non hospital employee All services are billed under Part B NP/PAs get 85% of the physician fee schedule Can bill at 100% based on physician s level of interaction, decision making, based on documentation. 41
42 Private insurance Contact the payor Get (in writing) the representatives name, The written policy/contract Specific issues of reimbursement 42
PRACTICE MODELS FOR INPATIENT GI CONSULTATION
 PRACTICE MODELS FOR INPATIENT GI CONSULTATION JAMES S. LEAVITT, MD, FACG PRESIDENT GASTROHEALTH MIAMI, FLORIDA JLEAVITT@GASTROHEALTH.COM An expert is somebody who is more than 50 miles from home, has no
PRACTICE MODELS FOR INPATIENT GI CONSULTATION JAMES S. LEAVITT, MD, FACG PRESIDENT GASTROHEALTH MIAMI, FLORIDA JLEAVITT@GASTROHEALTH.COM An expert is somebody who is more than 50 miles from home, has no
NP or PA as Billing Provider
 NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
State of the State: Rules & Regulations for the APRN
 State of the State: Rules & Regulations for the APRN November 4 th, 2014 Meredith Lahl, MSN, PCNS-BC, PNP-BC, CPON Senior Director Advanced Practice Nursing Nursing Institute Topics Cleveland Clinic
State of the State: Rules & Regulations for the APRN November 4 th, 2014 Meredith Lahl, MSN, PCNS-BC, PNP-BC, CPON Senior Director Advanced Practice Nursing Nursing Institute Topics Cleveland Clinic
Non-Physician i Providers
 Non-Physician i Providers Colleen M. Schmitt, MD, MHS, FACG, FASGE Galen Medical Group Chattanooga, TN cschmitt7@comcast.net 1 To define the steps to develop ancillary infusion and histopathology services
Non-Physician i Providers Colleen M. Schmitt, MD, MHS, FACG, FASGE Galen Medical Group Chattanooga, TN cschmitt7@comcast.net 1 To define the steps to develop ancillary infusion and histopathology services
ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice
 ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice AUTHORS: Jaya R. Agrawal, MD, Hampshire Gastroenterology Associates, Florence, MA Wassem Juakiem, MD, Brooke Army Medical Center,
ACG GI Practice Toolbox: Adding Advanced Practice Providers to your Practice AUTHORS: Jaya R. Agrawal, MD, Hampshire Gastroenterology Associates, Florence, MA Wassem Juakiem, MD, Brooke Army Medical Center,
SHAPING THE ED FOR EDUCATION - ALIGNING GOALS
 SHAPING THE ED FOR EDUCATION - ALIGNING GOALS Michael Gibbs, MD Chair, Carolinas Medical Center Megan Fix, MD Associate Program Director, University of Utah Why is this important? History of resident education
SHAPING THE ED FOR EDUCATION - ALIGNING GOALS Michael Gibbs, MD Chair, Carolinas Medical Center Megan Fix, MD Associate Program Director, University of Utah Why is this important? History of resident education
Aligning Advanced Practice Clinicians with New Care Models
 MGMA 2017 ANNUAL CONFERENCE OCT. 8-11 ANAHEIM, CA Aligning Advanced Practice Clinicians with New Care Models Trish Anen, RN, MBA, NEA-BC Debra Slater Principal, Sullivan, Cotter and Associates Principal,
MGMA 2017 ANNUAL CONFERENCE OCT. 8-11 ANAHEIM, CA Aligning Advanced Practice Clinicians with New Care Models Trish Anen, RN, MBA, NEA-BC Debra Slater Principal, Sullivan, Cotter and Associates Principal,
Appendix B: Formulae Used for Calculation of Hospital Performance Measures
 Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Annual Wellness Visit (AWV) Delivery Business Case
 Delivery Business Case") Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
Hospitals and HealthCare Systems What you were Not taught in PA School
 Hospitals and HealthCare Systems What you were Not taught in PA School Folusho Ogunfiditimi, DM, MPH, PA-C Administrative Director, Adult Clinical Services and Advanced Practice Providers Harper University
Hospitals and HealthCare Systems What you were Not taught in PA School Folusho Ogunfiditimi, DM, MPH, PA-C Administrative Director, Adult Clinical Services and Advanced Practice Providers Harper University
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
PANELS AND PANEL EQUITY
 PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
ADDING VALUE TO PHYSICIAN COMPENSATION A COMPREHENSIVE GUIDE TO ALIGNING PROVIDER COMPENSATION WITH VALUE-BASED REIMBURSEMENT
 ADDING VALUE TO PHYSICIAN COMPENSATION A COMPREHENSIVE GUIDE TO ALIGNING PROVIDER COMPENSATION WITH VALUE-BASED REIMBURSEMENT 1 INTRODUCTION The evolving physician compensation landscape Recently, HSG
ADDING VALUE TO PHYSICIAN COMPENSATION A COMPREHENSIVE GUIDE TO ALIGNING PROVIDER COMPENSATION WITH VALUE-BASED REIMBURSEMENT 1 INTRODUCTION The evolving physician compensation landscape Recently, HSG
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Michelle Moore Manager, OutPatient Registration Services Angelica DelVillar Registration Lead Representative, OutPatient Services
 Michelle Moore Manager, OutPatient Registration Services Angelica DelVillar Registration Lead Representative, OutPatient Services PIH Health Whittier, California PIH Health is the dominant hospital provider
Michelle Moore Manager, OutPatient Registration Services Angelica DelVillar Registration Lead Representative, OutPatient Services PIH Health Whittier, California PIH Health is the dominant hospital provider
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S
 ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
5/13/2011. Background. Anesthesia Financials: An Unbalanced Equation. Understanding Anesthesia Financial Drivers
 Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Managing Staffing Expense: H-P-P-D Initiative. Stephanie Abbu, MSN, RN Neonatal Services Clinical Business Coordinator
 Managing Staffing Expense: H-P-P-D Initiative Stephanie Abbu, MSN, RN Neonatal Services Clinical Business Coordinator Objectives After attending this presentation / discussion, the conference participant
Managing Staffing Expense: H-P-P-D Initiative Stephanie Abbu, MSN, RN Neonatal Services Clinical Business Coordinator Objectives After attending this presentation / discussion, the conference participant
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Explaining the Value to Payers
 Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Overview: Midlevels for the Medically Underserved. -Employer Information-
 Overview: Midlevels for the Medically Underserved -Employer Information- 1 In this Packet You ll Find What is Midlevels for the Medically Underserved?... 3 Why Midlevels for the Medically Underserved?....
Overview: Midlevels for the Medically Underserved -Employer Information- 1 In this Packet You ll Find What is Midlevels for the Medically Underserved?... 3 Why Midlevels for the Medically Underserved?....
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
Are NPs and PAs Right for Your Practice?
 Society of Hospital Medicine Roundtable Are NPs and PAs Right for Your Practice? January 14, 2010 Michael L. Powe, Vice President Health Systems & Reimbursement Policy American Academy of Physician Assistants
Society of Hospital Medicine Roundtable Are NPs and PAs Right for Your Practice? January 14, 2010 Michael L. Powe, Vice President Health Systems & Reimbursement Policy American Academy of Physician Assistants
What is CDI? 2016 HTH FL Boot Camp. HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race
 Race") HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
HIM/Documentation: Endurance in the Clinical Documentation Improvement (CDI) Race Presented By: Sandy Sage Developed by Annie Lee Sallee Endurance in the Clinical Documentation Improvement (CDI) Race Learning
Negotiating a Hospital Anesthesia Financial Support Agreement
 Negotiating a Hospital Anesthesia Financial Support Agreement Negotiating a Hospital Anesthesia Financial Support Agreement 1 SUMMARY AT A GLANCE: Most anesthesia groups need to create or update agreements
Negotiating a Hospital Anesthesia Financial Support Agreement Negotiating a Hospital Anesthesia Financial Support Agreement 1 SUMMARY AT A GLANCE: Most anesthesia groups need to create or update agreements
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
APNP Hospitalist Program
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital. Ministry Health Care. Program Objectives. Catholic Health Assembly June 23, 2014
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Collaborative Care Model. Post-Acute Care / Long-Term care / Sub-Acute Care. Proposal
 Definitions: Collaborative Care Model Post-Acute Care / Long-Term care / Sub-Acute Care Proposal For the purposes of this proposal, we use definitions consistent with AMDA The Society for Post-Acute and
Definitions: Collaborative Care Model Post-Acute Care / Long-Term care / Sub-Acute Care Proposal For the purposes of this proposal, we use definitions consistent with AMDA The Society for Post-Acute and
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Workload Models. Hospitalist Consulting Solutions White Paper Series
 Hospitalist Consulting Solutions White Paper Series Workload Models Author Vandad Yousefi MD CCFP Senior partner Hospitalist Consulting Solutions 1905-763 Bay St Toronto ON M5G 2R3 1 Hospitalist Consulting
Hospitalist Consulting Solutions White Paper Series Workload Models Author Vandad Yousefi MD CCFP Senior partner Hospitalist Consulting Solutions 1905-763 Bay St Toronto ON M5G 2R3 1 Hospitalist Consulting
Maximizing Value Out of PA s and NP s in Surgery Practices
 Maximizing Value Out of PA s and NP s in Surgery Practices Daniel Coll, MHS, PA-C, DFAAPA CU MBA-HA Class of 2018 Tahoe Forest Hospital District Truckee, California Acknowledgements The lecture contents
Maximizing Value Out of PA s and NP s in Surgery Practices Daniel Coll, MHS, PA-C, DFAAPA CU MBA-HA Class of 2018 Tahoe Forest Hospital District Truckee, California Acknowledgements The lecture contents
RURAL RECRUITMENT PLAYBOOK OUTLINE
 RURAL RECRUITMENT PLAYBOOK OUTLINE State of the industry and trends in rural physician recruitment Emerging strategies for recruitment into rural communities. Examples of optimized recruitment & retention
RURAL RECRUITMENT PLAYBOOK OUTLINE State of the industry and trends in rural physician recruitment Emerging strategies for recruitment into rural communities. Examples of optimized recruitment & retention
NYS Home Care Program and Financial Trends 2017
 A report on the financial and program condition of New York s home and community-based providers and managed care plans amid state reform policies and mandates The Home Care Association of New York State
A report on the financial and program condition of New York s home and community-based providers and managed care plans amid state reform policies and mandates The Home Care Association of New York State
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS
 THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
AGENDA. QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, /21/2014
 QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Clinical Documentation Improvement: Best Practice
 Revenue Cycle Solutions Consulting and Management Services Clinical Documentation Improvement: Best Practice Our mission: To help you finance yours. 2 Managing Your Audio Use Telephone Use Microphone and
Revenue Cycle Solutions Consulting and Management Services Clinical Documentation Improvement: Best Practice Our mission: To help you finance yours. 2 Managing Your Audio Use Telephone Use Microphone and
HEALTHCARE: Academic Medical Center & Health System
 HEALTHCARE: Academic Medical Center & Health System BEFORE Results ED Time in Dept (minutes) Each data point is the weekly average. Volume was relatively flat during the shown time period. [Academic Medical
HEALTHCARE: Academic Medical Center & Health System BEFORE Results ED Time in Dept (minutes) Each data point is the weekly average. Volume was relatively flat during the shown time period. [Academic Medical
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Rural Hospital Performance Improvement
 Rural Hospital Performance Improvement North Sunflower County Hospital Ruleville, Mississippi July 2003 What Was Needed Business Office Review AR Analysis Clinical Services Evaluation Core Services Planning
Rural Hospital Performance Improvement North Sunflower County Hospital Ruleville, Mississippi July 2003 What Was Needed Business Office Review AR Analysis Clinical Services Evaluation Core Services Planning
The new role of hospitalists. Keeping patients out of the hospital. Cynthia Litt, MPH Eugene Kim, MD
 The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
$traight Talk Hot Topics. Free Standing EDs. Free Standing EDs 11/6/2017. David A. McKenzie, CAE ACEP Reimbursement Director
 Free Standing EDs $traight Talk Hot Topics Free Standing EDs David A. McKenzie, CAE ACEP Reimbursement Director CPT Definition for the use of 99281-99285: Organized hospital-based facility for the provision
Free Standing EDs $traight Talk Hot Topics Free Standing EDs David A. McKenzie, CAE ACEP Reimbursement Director CPT Definition for the use of 99281-99285: Organized hospital-based facility for the provision
paymentbasics Defining the inpatient acute care products Medicare buys Under the IPPS, Medicare sets perdischarge
 Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
Hospital ACUTE inpatient services system basics Revised: October 2007 This document does not reflect proposed legislation or regulatory actions. 601 New Jersey Ave., NW Suite 9000 Washington, DC 20001
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
COMPREHENSIVE CARE JOINT REPLACEMENT MODEL CONTRACTING TOOLKIT
 COMPREHENSIVE CARE JOINT REPLACEMENT MODEL CONTRACTING TOOLKIT March 2016 INTRODUCTION Alternative, collaborative delivery systems are the wave of the future. CMS, as well as commercial payers, are committed
COMPREHENSIVE CARE JOINT REPLACEMENT MODEL CONTRACTING TOOLKIT March 2016 INTRODUCTION Alternative, collaborative delivery systems are the wave of the future. CMS, as well as commercial payers, are committed
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Three Steps to Streamline Laboratory Operations:
 Three Steps to Streamline Laboratory Operations: A GUIDE FOR IMPROVING PERFORMANCE AND QUALITY By Richard Walker, MBA, MLS (ASCP), and Kelly Straub, M.S., Huron Healthcare The evolving healthcare environment
Three Steps to Streamline Laboratory Operations: A GUIDE FOR IMPROVING PERFORMANCE AND QUALITY By Richard Walker, MBA, MLS (ASCP), and Kelly Straub, M.S., Huron Healthcare The evolving healthcare environment
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service. About Long Beach, CA. About Memorial Care
 Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service Judy Fix, MSN, CNO Megan Liego, DNP, ACNP-BC About Long Beach, CA Located in South Los Angeles County Seventh largest
Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service Judy Fix, MSN, CNO Megan Liego, DNP, ACNP-BC About Long Beach, CA Located in South Los Angeles County Seventh largest
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare
 The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
Making the Business Case
 Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Session 57 PD, Care Management in an Evolving Health Care World. Moderator/Presenter: David V. Axene, FSA, CERA, FCA, MAAA
 Session 57 PD, Care Management in an Evolving Health Care World Moderator/Presenter: David V. Axene, FSA, CERA, FCA, MAAA Presenters: Craig Butler, MD, MBA Richard Fuller Timothy Willard Smith, ASA, MAAA
Session 57 PD, Care Management in an Evolving Health Care World Moderator/Presenter: David V. Axene, FSA, CERA, FCA, MAAA Presenters: Craig Butler, MD, MBA Richard Fuller Timothy Willard Smith, ASA, MAAA
Calculating the Value of a Physician Assistant
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/calculating-the-value-of-a-physicianassistant/3649/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/calculating-the-value-of-a-physicianassistant/3649/
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Children s Hospital of Eastern Ontario
 Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE
 ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE June 2017 INTRODUCTION Alternative, collaborative health care delivery systems are the wave of the future. The Centers for Medicare and Medicaid Services (CMS),
ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE June 2017 INTRODUCTION Alternative, collaborative health care delivery systems are the wave of the future. The Centers for Medicare and Medicaid Services (CMS),
PHYSICIAN-HOSPITAL JOINT VENTURES: A STRATEGIC ALTERNATIVE
 PHYSICIAN-HOSPITAL JOINT VENTURES: A STRATEGIC ALTERNATIVE By Joseph S. Zasa, JD, Managing Partner ASD Management Since the first ambulatory surgery center was developed in Phoenix, Arizona in 1970, ambulatory
PHYSICIAN-HOSPITAL JOINT VENTURES: A STRATEGIC ALTERNATIVE By Joseph S. Zasa, JD, Managing Partner ASD Management Since the first ambulatory surgery center was developed in Phoenix, Arizona in 1970, ambulatory
ABC s of Private Practice and Academics: Your First Job
 ABC s of Private Practice and Academics: Your First Job Shamina Dhillon MD, FACG Partner, Shore Gastroenterology Associates NJ Clinical Assistant Professor of Medicine, Robert Wood Johnson Medical School
ABC s of Private Practice and Academics: Your First Job Shamina Dhillon MD, FACG Partner, Shore Gastroenterology Associates NJ Clinical Assistant Professor of Medicine, Robert Wood Johnson Medical School
SCRIBES, SMAS AND INCIDENT T0
 SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances
 WHITE PAPER The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances The OB-ED model fundamentally changes how hospitals care for expectant mothers in a way that improves
WHITE PAPER The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances The OB-ED model fundamentally changes how hospitals care for expectant mothers in a way that improves
ACCOUNTABLE CARE: ROADMAP TO VALUE
 ACCOUNTABLE CARE: ROADMAP TO VALUE Perspective The adoption of Accountable Care and value-based reimbursement has dramatically increased these past several years. New organizations are being established
ACCOUNTABLE CARE: ROADMAP TO VALUE Perspective The adoption of Accountable Care and value-based reimbursement has dramatically increased these past several years. New organizations are being established
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
Staffing and Scheduling
 Staffing and Scheduling 1 One of the most critical issues confronting nurse executives today is nurse staffing. The major goal of staffing and scheduling systems is to identify the need for and provide
Staffing and Scheduling 1 One of the most critical issues confronting nurse executives today is nurse staffing. The major goal of staffing and scheduling systems is to identify the need for and provide
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones.
 Dr. Marie S, Gustin Nursing Excellence Conference, 2012 The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones. John Maynard Keynes Chaos, Complexity,
Dr. Marie S, Gustin Nursing Excellence Conference, 2012 The greatest difficulty in the world is not for people to accept new ideas but to get them to forget their old ones. John Maynard Keynes Chaos, Complexity,
The New Jersey Gainsharing Experience By Robert G. Coates, MD, MMM, CPE
 Payment The New Jersey Gainsharing Experience By Robert G. Coates, MD, MMM, CPE In this article Examine results of a New Jersey gainsharing program and see how the cost savings used to pay the physicians
Payment The New Jersey Gainsharing Experience By Robert G. Coates, MD, MMM, CPE In this article Examine results of a New Jersey gainsharing program and see how the cost savings used to pay the physicians
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Physician Compensation for Quality Within Groups: Complying with Stark and State of The Art. Traditional Physician Compensation Models
 Physician Compensation for Quality Within Groups: Complying with Stark and State of The Art Alice G. Gosfield, Esq. Medicare and Medicaid Institute American Health Lawyers Association March 29, 2012 c.2012,
Physician Compensation for Quality Within Groups: Complying with Stark and State of The Art Alice G. Gosfield, Esq. Medicare and Medicaid Institute American Health Lawyers Association March 29, 2012 c.2012,
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Accomplishments Fiscal Year UPMC Passavant
 Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
How To Use Data To Manage Your Nonprofit
 How To Use Data To Manage Your Nonprofit Operate more like a business while staying true to your organization s mission Take a Page From the For-Profit Sector Some people don t like to think about running
How To Use Data To Manage Your Nonprofit Operate more like a business while staying true to your organization s mission Take a Page From the For-Profit Sector Some people don t like to think about running
Chad Shearer, JD, MHA, Vice President for Policy, Medicaid Institute Director Misha Sharp, Research Analyst February 28, 2018
 Testimony of the United Hospital Fund to the Council of the City of New York, Committee on Hospitals: Oversight Examining the Status of One New York: Health Care for Our Neighborhoods : What Progress Has
Testimony of the United Hospital Fund to the Council of the City of New York, Committee on Hospitals: Oversight Examining the Status of One New York: Health Care for Our Neighborhoods : What Progress Has
MACRA and the Quality Payment Program. Frequently Asked Questions Edition
 MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
General Surgery Patient Call Coverage Demand in a Community Hospital with a Limited Number of General Surgeons
 American College of Medical Practice Executives General Surgery Patient Call Coverage Demand in a Community Hospital with a Limited Number of General Surgeons Case Study Manuscript (This case study manuscript
American College of Medical Practice Executives General Surgery Patient Call Coverage Demand in a Community Hospital with a Limited Number of General Surgeons Case Study Manuscript (This case study manuscript
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
building the right physician platform
 REPRINT July 2015 James J. Pizzo Luke Sullivan Debra L. Ryan healthcare financial management association hfma.org building the right physician platform Better integration of both employed and independent
REPRINT July 2015 James J. Pizzo Luke Sullivan Debra L. Ryan healthcare financial management association hfma.org building the right physician platform Better integration of both employed and independent
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Formation of a High Performance Medical Group within a Hospital Centric Health Care System... De NOVO
 Formation of a High Performance Medical Group within a Hospital Centric Health Care System... De NOVO Jim Boswell, MBA VP Physician Services / BMHCC and CEO / BMG Robert Vest, JD COO / BMG Founded in 1912
Formation of a High Performance Medical Group within a Hospital Centric Health Care System... De NOVO Jim Boswell, MBA VP Physician Services / BMHCC and CEO / BMG Robert Vest, JD COO / BMG Founded in 1912