Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians
|
|
|
- Archibald Gilbert
- 5 years ago
- Views:
Transcription

1 Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality Improvement Organization for Virginia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. VHQC/1c/ /445
2 This Session What are we doing here patient safety Culture just or otherwise What is an error anyway Message we send Tools we use Other things that affect patient safety culture Hand offs and transitions SBAR WalkRounds Time and Timeline





3 ACT Virginians ROSC -It s About: Culture of quality improvement and patient safety TOP PRIORITY Hearing all the opportunities to make change before an error happens Patient centered family, friends, neighbors
4 Culture What is an error anyway and can we talk about it? Individual s perception Management perception Policies Literature says Legal Near miss/great save Can t address if not reported
5 If There is an Error Somebody Must Be at Fault Right? Error- not the conclusion but the beginning of the investigation System or the individual Roots of error Execution Planning Violation
6 Just Culture All in the Message Just but Accountable Everybody on the same playing field Set the rules and agree up front Write it down Just Blameless Punitive
7 Why Write the Rules Methodist Hospital in Indiana (9/17/2006) Six premies given wrong dose of Heparin Two died CEO message(9/19/2006) (9/24/2006) As Our part culture of our at Clarian continuing is one investigation that demands into these matters, forthrightness I met this when morning mistakes for are over made, two so hours that we with can learn virtually from all those of the mistakes Methodist and Hospital improve staff our involved systems and with offer the events higher of levels this of past patient care and weekend. While we will continue to investigate safety. matters in great detail, nothing we learned this morning deviates from what we reported yesterday afternoon -- namely, that human and procedural errors account for the administration of....
8 Just Culture All in the Message Some issues Different department, different message Slips Written vs. verbal cues how does it really sound and feel
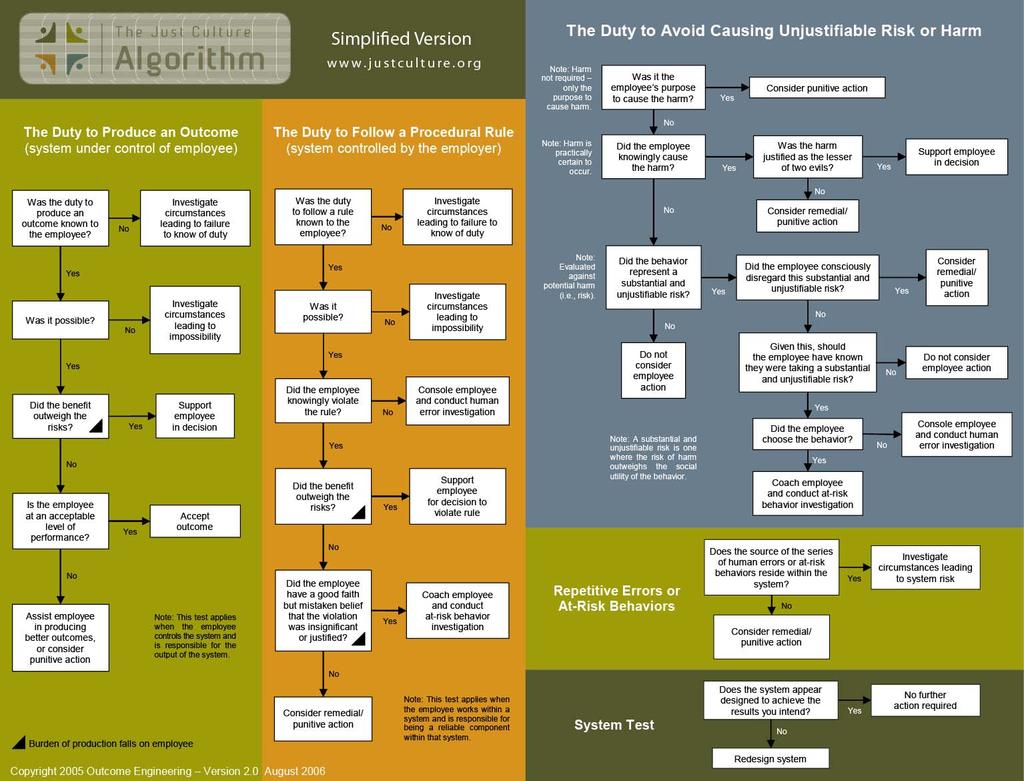
9 Tools The Nurses Role in Promoting a Culture of Patient Safety - CEU Human Factor on-line training (Patient Safety Center) Human Factor & Just Culture tutorial (free) Blood bank error reporting system ($$) %20a%20just%20culture.pdf A Roadmap to a Just Culture: Enhancing the Safety Environment Algorithm and reporting system ($$)


10 Pages 10-11
11
12 Collecting Useful Information Error Harm No harm (luck) Save (whew! Planned or unplanned) Cause Individual System Risk level and response
13 What Do You Do With Those Reports Stash in a drawer Collect in a database Set up levels of RISK Trend over time RCA Maybe fix a system fault Just do something with the data or you will lose them
14 Just Culture Group interaction Introduce yourself and area Which part of Just Culture do you think will be difficult to begin? What question do you have for others Give an example of a Just and Unjust response to error you received or have seen
15 Hand Offs and Transitions SBAR Issues and errors Amazing, it s all about communicating and understanding each other - AGAIN
16 What Do We Want? Safety is the Top Priority! Begin with behaviors that improve patient safety. Assertive Communication The Toyota Production System Pull the cord and stop the assembly line.
17 Understand Factors that Affect Communication Education Nurses narrative and descriptive. Physicians problem solve,want only the headlines. Teamwork Nurses: environment not collaborative. Physicians: fairly collaborative. Environmental Impact Interruptions and distractions, can t remember Assertiveness Skills Not everyone has the ability to speak up. The areas mentioned above are not meant to be inclusive of all factors that affect communication.
18 Assertion Cycle. This is a model to guide and improve assertion in the interest of patient safety GET PERSON S ATTENTION REACH DECISION EXPRESS CONCERN PROPOSE ACTION STATE PROBLEM Source: M. Leonard, S Graham, D Bonacum
 Photographer's Mate 2nd Class Michael D. Kennedy.")
19 US Navy Nuclear Submarine Service Communication Model SBAR S = Situation B = Background A = Assessment R = Resolution USS Dolphin (AFSS 555) Photographer's Mate 2nd Class Michael D. Kennedy. [ N-5067K-004] May 22, 2002
20 Why SBAR? Provides answers to physicians three main questions What is the problem? What do you need me to do? When do I have to respond? Standardized approach - efficient transfer of key information Helps create an environment to express concerns
21 Successful Clinical Change Requires: Visible Leadership Support Administrative and Clinical Goals and incentives aligned Physician Champion (Role) Educates physicians on the need for having patience during staff s learning curve. Culture change for some physicians. Physicians need to be careful not to alienate staff. Obtain buy in from physicians. Identify distinguishing behaviors that do not support SBAR communication and speak to those physicians.
22 What is the Definition of SBAR? S = Situation What is going on with the patient. A concise statement of the problem. B = Background What is the clinical background information that is pertinent to the situation. A = Assessment What did you find? Analysis and considerations of options. R = Recommendation What action/recommendation is needed to correct the problem. What do you want?
23
24
25 Practice Situation Mary s patient Henrietta Hobson had her spleen removed this morning. She had a little trouble in the PACU with a low urine output but that seems to be stable right now. They put in a catheter and she is putting out 30 cc/hr. Her blood pressure is low now 75/50, HR-150 and she is a little diaphoretic. Ms. Hobson is a preacher s wife and teaches Sunday school so she needs to be out of the hospital in 5 days. She had a CXR three years ago for a cough and nothing was seen. It just went away. Examining her you see that her abdomen in more distended now than it was 10 minutes ago and there is a bit of seepage bright red on her dressing. Her PPD reads normal she had that test a couple of days ago. She has no know allergies. Last labs (H/H and Glu) were drawn in the PACU and were WNL
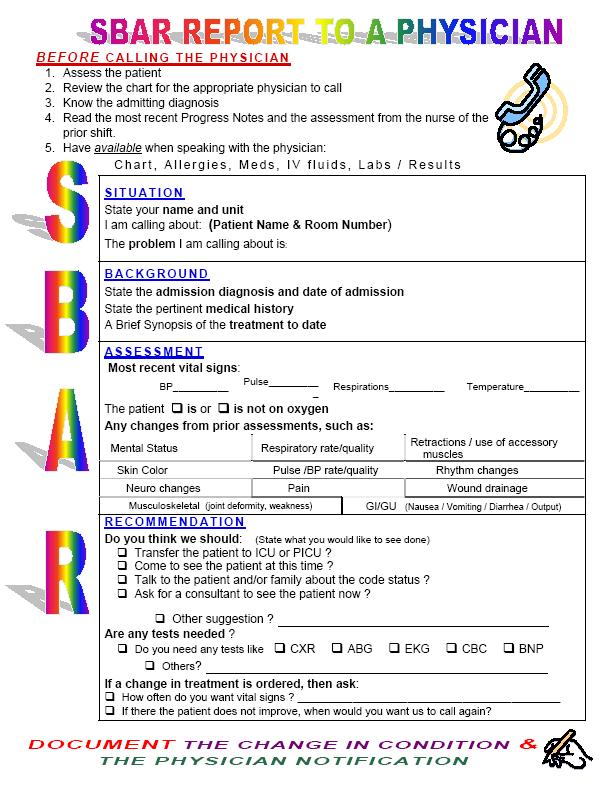
26 SBAR Guidelines: Step 1 1. Have all the patient s information available before you contact the physician. Name Medical record number Age Diagnosis Medication list Allergies Vital signs Lab results Advance Directive

27 SBAR Guidelines: Step 2 2. A physical assessment has been conducted Have I seen and assessed the patient myself before calling Review the chart for appropriate physician to call Reviewed the chart for appropriate information
28 SBAR Guidelines: Step 3 3. When calling the physician, follow the SBAR process: (S) Situation: What is the situation you are calling about? Identify self, hospital, patient, patient location in hospital What is going on with the patient. A concise statement of the problem
29 SBAR Guidelines: Step 3 (cont.) (B) Background: What is the clinical background information that is pertinent to the situation The admitting diagnosis and date of admission List of current medications, allergies, IV fluids, etc Most recent vital signs Lab results: provide the date and time test was done and results of previous tests for comparison Advance Directive
 (A)Assessment: What are the clinician s findings What is the analysis and")
30 SBAR Guidelines: Step 3 (cont.) (A)Assessment: What are the clinician s findings What is the analysis and consideration of options Is this problem severe or life threatening
 (R) Recommendation: What action/recommendation is needed to correct the problem What solution can you offer")
31 SBAR Guidelines: Step 3 (cont.) (R) Recommendation: What action/recommendation is needed to correct the problem What solution can you offer the physician What do you need from the physician to improve the patient s condition
32

33 Even used for transferring within the hospital pg 173

 B (a little about the patient s")
 2005 Institute for Healthcare")
34 SBAR POCKET CARD In the interest of Patient Safety and to ensure we are giving complete, accurate information to the physician, please use the following acronym to direct the information we provide: S (the current Situation or problem) B (a little about the patient s Background) A (your Assessment of the patient) R (your Recommendation of what is needed from the physician) 2005 Institute for Healthcare Improvement
35 What do you do if SBAR does not work? It s okay to C.U.S.!
36 C.U.S. (From Aviation United Airlines) We have a serious problem. Stop and listen to me! C = I am Concerned (with my patient s condition) U = I am Uncomfortable (with my patient s condition) S = The Safety (of the patient) is at risk
37 What to do if C.U.S. doesn t work Design policies that guide when not followed Might include: Who to contact (supervisor, physician, medical director) Consulting with Quality Improvement, Risk Management,etc.
38 Hand Offs and Transition Group interaction Can you see a place or time SBAR or CUS would be useful in your institution? Do you see any issues implementing this type of communication style?
39 WalkRounds Senior leaders, using a pre-selected script, to talk with employees Routinely monthly or more frequently visit all departments and all shifts Collect information, track it, do something with it Moves from environmental issues to other safety issues as comfort level increases
40 Change Takes TIME, a whole lot of COMMUNICATION and support from all levels Creating a safety environment is everyone s responsibility
41 Fairy Tales Describe a fairy tale that you experienced Did it work or fail? Why or why not? Was leadership supporting it throughout?
42 It is not by accident that you were chosen to be a leader. It is your destiny. Sensei Chihiro Nakao MAKE SAFETY A TOP PRIORITY
43 References Joint Commission on Accreditation of Healthcare Organizations. Sentinel Events Statistics. Root Causes of Sentinel Events, , Joint Commission on Accreditation of Healthcare Organizations. Sentinel Events Statistics. Settings of Sentinel Events, Available at: Leonard M, Bonacum D, Taggart B Using SBAR to Improve Communication Between Caregivers. Institute for Healthcare Improvement. Leonard M The SBAR Technique: Improving Verbal Communication and Teamwork in Clinical Care. PONL Bulletin. Volume 2, Issue 1. Leonard M, Graham S, Bonacum D The Human Factor: The Critical Importance of Teamwork and Communication in Providing Self Care. Qual Saf Heath Care :i85-i BMJ Publishing Group Ltd. and Institute for Healthcare Improvement.
44 References continued Nunes J Patient Safety Leadership Fellowship Learnings Help Put Theory into Practice. A Newsletter from the National Patient Safety Foundation. Volume 8: Issue 3. Whittington J, Nagamine J SBAR: Application and Critical Success Factors of Implementation. Institute for Healthcare Improvement
New England Home Health Collaborative
 New England Home Health Collaborative Clinical Collaboration: Partnering with Physicians Kathryn D. Roby, M.Ed., M.S., CHCE, CHAP QIN-QIO Home Health Consultant May 13, 2015 The New England Quality Innovation
New England Home Health Collaborative Clinical Collaboration: Partnering with Physicians Kathryn D. Roby, M.Ed., M.S., CHCE, CHAP QIN-QIO Home Health Consultant May 13, 2015 The New England Quality Innovation
An Innovative Approach to SBAR Communication. Jennifer Bello BSN, RN, C White Plains Hospital Center
 An Innovative Approach to SBAR Communication Jennifer Bello BSN, RN, C White Plains Hospital Center Presenter Disclosure Information Jennifer Bello, RN An Innovative Approach to SBAR Communication Registered
An Innovative Approach to SBAR Communication Jennifer Bello BSN, RN, C White Plains Hospital Center Presenter Disclosure Information Jennifer Bello, RN An Innovative Approach to SBAR Communication Registered
Nursing Home Quality Care Collaborative Team Communication. 20 April 2017
 Nursing Home Quality Care Collaborative Team 20 April 2017 Interacting with the Webinar 2 Slides & Recording Registrants were sent a PDF of the slides in advance of the webinar The slides and a recording
Nursing Home Quality Care Collaborative Team 20 April 2017 Interacting with the Webinar 2 Slides & Recording Registrants were sent a PDF of the slides in advance of the webinar The slides and a recording
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
SBAR Communication Tool. Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme
 Clinical Risk Advisor, Clinical Indemnity Scheme") SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
INTERACT Webinar Series
 INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Participant WebEx Training. Jacob Auger Project Coordinator
 Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots
 HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
Drug Events. Adverse R EDUCING MEDICATION ERRORS. Survey Adapted from Information Developed by HealthInsight, 2000.
 Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Teamwork and Collaboration. Lippincott Solutions [1]
![Teamwork and Collaboration. Lippincott Solutions [1]](/thumbs/75/71760159.jpg "Teamwork and Collaboration. Lippincott Solutions [1]") Teamwork and Collaboration Description Description: This lesson will provide the nurse with the knowledge, skills, and abilities needed to work collaboratively within the health care team. It will teach
Teamwork and Collaboration Description Description: This lesson will provide the nurse with the knowledge, skills, and abilities needed to work collaboratively within the health care team. It will teach
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Patient Safety Academy /8/16 PROVIDING INFORMAL FEEDBACK: AN INTERACTIVE WORKSHOP. Objectives
 PROVIDING INFORMAL FEEDBACK: AN INTERACTIVE WORKSHOP Frank Korn R.N., MBA, CPPS Risk Coordinator 9/8/2016 Patient Safety Academy 1 Objectives At the end of the presentation you should be able to explain
PROVIDING INFORMAL FEEDBACK: AN INTERACTIVE WORKSHOP Frank Korn R.N., MBA, CPPS Risk Coordinator 9/8/2016 Patient Safety Academy 1 Objectives At the end of the presentation you should be able to explain
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Putting the Person in Person- Centered Care Plans. Patty Austin, RN, CPHQ Penny Imes, RN, BSN
 Putting the Person in Person- Centered Care Plans Patty Austin, RN, CPHQ Penny Imes, RN, BSN Objectives Discuss person centered care plans as they relate to regulations and new rule Demonstrate the use
Putting the Person in Person- Centered Care Plans Patty Austin, RN, CPHQ Penny Imes, RN, BSN Objectives Discuss person centered care plans as they relate to regulations and new rule Demonstrate the use
Situational awareness: SBAR training
 Situational awareness: SBAR training Outline of this presentation Situational awareness Joint accountability SBAR These can happen to you! After the code team was finished resuscitating, someone found
Situational awareness: SBAR training Outline of this presentation Situational awareness Joint accountability SBAR These can happen to you! After the code team was finished resuscitating, someone found
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
CNA Training Advisor
 CNA Training Advisor Volume 14 Issue No. 9 SEPTEMBER 2016 As more attention is paid to quality of care, agencies need to focus on intangibles such as staff accountability and professionalism. All personnel,
CNA Training Advisor Volume 14 Issue No. 9 SEPTEMBER 2016 As more attention is paid to quality of care, agencies need to focus on intangibles such as staff accountability and professionalism. All personnel,
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Returning to the Why: Patient and Caregiver Suffering and Care. Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer
 Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations
 Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
IHI Expedition. Engaging Frontline Teams to Create a Culture of Safety. March 28 th, Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN
 March 28 th, 2013 These presenters have nothing to disclose IHI Expedition Engaging Frontline Teams to Create a Culture of Safety Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN Today s Host 2 Lizzie
March 28 th, 2013 These presenters have nothing to disclose IHI Expedition Engaging Frontline Teams to Create a Culture of Safety Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN Today s Host 2 Lizzie
SafetyFirst: The Journey to High Reliability
 SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
Setting: Emergency departments are high-risk contexts; they are over-crowded and
 QUALITY IMPROVEMENT STUDENT PROJECT PROPOSAL: IMPROVING HANDOFFS IN SAN FRANCISCO GENERAL HOSPTITAL S EMERGENCY DEPARTMENT TMIT Student Projects QuickStart Package 1. BACKGROUND Setting: Emergency departments
QUALITY IMPROVEMENT STUDENT PROJECT PROPOSAL: IMPROVING HANDOFFS IN SAN FRANCISCO GENERAL HOSPTITAL S EMERGENCY DEPARTMENT TMIT Student Projects QuickStart Package 1. BACKGROUND Setting: Emergency departments
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm. Kendra Folh, BSN, RNC-OB
 How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
Human resources. OR Manager Vol. 29 No. 5 May 2013
 Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Keeping Kids Safe TeamSTEPPS Essentials
 Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
A Just Culture: Accountability for Patient Safety. Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012
 A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Academic-Service Partnerships
 Academic-Service Partnerships to Advance Patient Safety & Quality Gregory A. DeBourgh, EdD, RN, ANEF Session Objectives Identify the elements of an effective academic-service partnership to promote accountabilities
Academic-Service Partnerships to Advance Patient Safety & Quality Gregory A. DeBourgh, EdD, RN, ANEF Session Objectives Identify the elements of an effective academic-service partnership to promote accountabilities
Into a High Performing. Team. Standardization. Healthcare Team Training. The Beginning. Limits of Systems Only Safety. Development of a Systems Focus
 Healthcare Team Training Into a High Performing How to Turn High Performing Individuals Team "Greater experience does not necessarily lead to expertise. One may simply make the same mistakes with greater
Healthcare Team Training Into a High Performing How to Turn High Performing Individuals Team "Greater experience does not necessarily lead to expertise. One may simply make the same mistakes with greater
High Reliability Organizing (HRO) in the Ambulatory Setting
 in the Ambulatory Setting") High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Better handoffs. Safer care. Just-in-time Module
 Better handoffs. Safer care. Just-in-time Module Root Causes of Sentinel Events Joint Commission. (2011). Sentinel Event Statistics Data - Root Causes by Event Type (2004 - Third Quarter 2011) 1 2 TeamSTEPPS
Better handoffs. Safer care. Just-in-time Module Root Causes of Sentinel Events Joint Commission. (2011). Sentinel Event Statistics Data - Root Causes by Event Type (2004 - Third Quarter 2011) 1 2 TeamSTEPPS
December 20, Thursday. 7 am. 12 pm. 20 Thursday. December 2012 SuMo TuWe Th Fr Sa 1. January 2013 SuMo TuWe Th Fr Sa
 December 20, 2012 Thursday December 2012 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9101112131415 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 January 2013 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9 10 11 12 13 14
December 20, 2012 Thursday December 2012 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9101112131415 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 January 2013 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9 10 11 12 13 14
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
June 2018 Phc newsletter
 June 2018 Phc newsletter News from CMS and Joint Commission Inside This Issue: ü Perspectives Leadership Session Be Prepared for Changes SAFER Matrix Placement Under Review - # RFIs Still Important Not
June 2018 Phc newsletter News from CMS and Joint Commission Inside This Issue: ü Perspectives Leadership Session Be Prepared for Changes SAFER Matrix Placement Under Review - # RFIs Still Important Not
A Journal of Rhetoric in Society. Interview: Transplant Deliberations and Patient Advocacy. Staff
 Present Tense A Journal of Rhetoric in Society Interview: Transplant Deliberations and Patient Advocacy Staff Present Tense, Vol. 2, Issue 2, 2012. www.presenttensejournal.org editors@presenttensejournal.org
Present Tense A Journal of Rhetoric in Society Interview: Transplant Deliberations and Patient Advocacy Staff Present Tense, Vol. 2, Issue 2, 2012. www.presenttensejournal.org editors@presenttensejournal.org
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Leadership Forum: Promoting a Culture of Safety
 Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Society of General Internal Medicine May 7 th, 2011 Session G
 Society of General Internal Medicine May 7 th, 2011 Session G Introductions o Gregory M. Bump, MD bumpgm@upmc.edu o Caridad A. Hernandez, MD hernandezca@upmc.edu o Efren C. Manjarrez, MD Emanjarrez@med.miami.edu
Society of General Internal Medicine May 7 th, 2011 Session G Introductions o Gregory M. Bump, MD bumpgm@upmc.edu o Caridad A. Hernandez, MD hernandezca@upmc.edu o Efren C. Manjarrez, MD Emanjarrez@med.miami.edu
Running head: ROOT CAUSE ANALYSIS 1
 Running head: ROOT CAUSE ANALYSIS 1 Death by Running: Root Cause Analysis Kristen Carey Angelo State University ROOT CAUSE ANALYSIS 2 Long QT Syndrome Over a decade ago the Institute of Medicine estimated
Running head: ROOT CAUSE ANALYSIS 1 Death by Running: Root Cause Analysis Kristen Carey Angelo State University ROOT CAUSE ANALYSIS 2 Long QT Syndrome Over a decade ago the Institute of Medicine estimated
Understanding the High Reliability Organization and Why It's Important to Your Lab
 Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
PGY1 Medication Safety Core Rotation
 PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
OAR Changes. Presented by APD Medicaid LTC Policy
 OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
Help Prevent Errors in Your Care
 Speak Up Help Prevent Errors in Your Care To prevent health care errors, patients are urged to Speak Up Everyone has a role in making health care safe physicians, health care executives, nurses and technicians.
Speak Up Help Prevent Errors in Your Care To prevent health care errors, patients are urged to Speak Up Everyone has a role in making health care safe physicians, health care executives, nurses and technicians.
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
An RN is circulating on a case when near the end, the surgeon hands the scrub
 Clinical management Does your staff understand delegation? An RN is circulating on a case when near the end, the surgeon hands the scrub technician a suture and tells her to close the wound. In another
Clinical management Does your staff understand delegation? An RN is circulating on a case when near the end, the surgeon hands the scrub technician a suture and tells her to close the wound. In another
Ensuring Patient Centered Communication, Every Patient Every Time White Paper
 Ensuring Patient Centered Communication, Every Patient Every Time White Paper 2012 www.bhclg.com 220 West Garden Street, Suite 301, Pensacola, Fl. 32502 (850)469-7978 Patient Centered Communication As
Ensuring Patient Centered Communication, Every Patient Every Time White Paper 2012 www.bhclg.com 220 West Garden Street, Suite 301, Pensacola, Fl. 32502 (850)469-7978 Patient Centered Communication As
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement. Patty Austin, RN, CPHQ Project Coordinator
 QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
To err is human. When things go wrong: apology and communication. Apology and communication position statement
 When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
3/30/2015. Objectives. Rationale for QAPI. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Karen S. Guice, MD, MPP Executive Director Federal Recovery Coordination Program MHS, January 2011
 Karen S. Guice, MD, MPP Executive Director Federal Recovery Coordination Program MHS, January 2011 Report Documentation Page Form Approved OMB No. 0704-0188 Public reporting burden for the collection of
Karen S. Guice, MD, MPP Executive Director Federal Recovery Coordination Program MHS, January 2011 Report Documentation Page Form Approved OMB No. 0704-0188 Public reporting burden for the collection of
Strong Medicine Interview with Cheryl Webber, 20 June ILACQUA: This is Joan Ilacqua and today is June 20th, 2014.
 Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
PALLIATIVE CARE NURSE PRACTITIONER
 PALLIATIVE CARE NURSE PRACTITIONER Responsible to Regional Director of Palliative Care with dotted line to Medical Director Description The Nurse Practitioner (NP) works independently and in collaboration
PALLIATIVE CARE NURSE PRACTITIONER Responsible to Regional Director of Palliative Care with dotted line to Medical Director Description The Nurse Practitioner (NP) works independently and in collaboration
Nursing Documentation Changes and Reminders. CCTC Nursing Documentation
 Nursing Documentation Changes and Reminders CCTC Nursing Documentation Change #1 Standard ph range changed to match new RRT documentation Change #2 Clarification for documentation standards for IV solutions.
Nursing Documentation Changes and Reminders CCTC Nursing Documentation Change #1 Standard ph range changed to match new RRT documentation Change #2 Clarification for documentation standards for IV solutions.
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
Understanding Health Care in America An introduction for immigrant patients
 Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
Think proactively = prevent codes Elective intubation better than PEA arrest
 Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
End of Life PSP Module. Case Study: Mr. James Lee
 Case Study: Mr. James Lee Mr. James Lee is a 74 yr old retired electrician. He is married to Mary with two children in their 30 s. They have been in Canada for 35 years and are fluent in English and Cantonese.
Case Study: Mr. James Lee Mr. James Lee is a 74 yr old retired electrician. He is married to Mary with two children in their 30 s. They have been in Canada for 35 years and are fluent in English and Cantonese.
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
National Patient Safety Goals Effective January 1, 2016
 National Patient Safety Goals Effective January 1, 2016 Goal 1 Improve the accuracy of patient identification. NPSG.01.01.01 Home are Accreditation Program Use at least two patient identifiers when providing
National Patient Safety Goals Effective January 1, 2016 Goal 1 Improve the accuracy of patient identification. NPSG.01.01.01 Home are Accreditation Program Use at least two patient identifiers when providing
Glenn Rosenbluth, MD. Glenn Rosenbluth, Director, Quality and Safety Programs, GME
 Patient Patient Safety Safety How How Can Can Residents Residents Prevent Prevent Medical Medical Errors Errors & & Improve Improve Quality Quality of of Care Care Glenn Rosenbluth, MD Director, Glenn
Patient Patient Safety Safety How How Can Can Residents Residents Prevent Prevent Medical Medical Errors Errors & & Improve Improve Quality Quality of of Care Care Glenn Rosenbluth, MD Director, Glenn
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs
 I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
Edna Evergreen Scenario. Carolyn Lewis
 Carolyn Lewis Your life: You are a Certified Nursing Assistant (CNA) and have worked at Greenhill for six months. You respond well to most residents, but sometimes, you are frustrated by your job. You
Carolyn Lewis Your life: You are a Certified Nursing Assistant (CNA) and have worked at Greenhill for six months. You respond well to most residents, but sometimes, you are frustrated by your job. You
Patient Safety Case Study. Clara K. Terral. Angelo State University
 Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Understanding the Male Caregiver. By Julie Smith Home Instead Senior Care
 Understanding the Male Caregiver By Julie Smith Home Instead Senior Care Objectives 1. Learn statistics about male caregiving 2. Understand the challenges of male caregivers 3. Identify the differences
Understanding the Male Caregiver By Julie Smith Home Instead Senior Care Objectives 1. Learn statistics about male caregiving 2. Understand the challenges of male caregivers 3. Identify the differences
POPULATION HEALTH MANAGEMENT, PROGRAMS, MODELS, AND TOOLS A. LEE MARTINEZ DBH-C, MA, LAC, CPHQ
 POPULATION HEALTH MANAGEMENT, PROGRAMS, MODELS, AND TOOLS A. LEE MARTINEZ DBH-C, MA, LAC, CPHQ Learning objectives At the conclusion of this session, the participant will be able to: Learning Objective
POPULATION HEALTH MANAGEMENT, PROGRAMS, MODELS, AND TOOLS A. LEE MARTINEZ DBH-C, MA, LAC, CPHQ Learning objectives At the conclusion of this session, the participant will be able to: Learning Objective
Primary Care Team. for Primary Care Teams
 for s Team Strategies & Tools to Enhance Performance & Patient Safety Initiative based on evidence derived from team performance leveraging more than 25 years of research in military, aviation, nuclear
for s Team Strategies & Tools to Enhance Performance & Patient Safety Initiative based on evidence derived from team performance leveraging more than 25 years of research in military, aviation, nuclear
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
Admission Avoidance. Scenario 1 Urinary Tract Infection
 Admission Avoidance Course Scenario 1 Urinary Tract Infection Course lead Colette Laws-Chapman Faculty Course / Curriculum Admission Avoidance Target Delegates Scenario name Urinary Tract Infection Group
Admission Avoidance Course Scenario 1 Urinary Tract Infection Course lead Colette Laws-Chapman Faculty Course / Curriculum Admission Avoidance Target Delegates Scenario name Urinary Tract Infection Group
2017 Quality Incentive Program (QIP) Quality Improvement Activity (QIA) Improving Kt/V Comprehensive Measure Score
 Quality Improvement Activity (QIA) Improving Kt/V Comprehensive Measure Score") 2017 Quality Incentive Program (QIP) Quality Improvement Activity (QIA) Improving Kt/V Comprehensive Measure Score Tish Lawson Team Leader February Kick Off Meeting Overview Facility Selection QIP-QIA
2017 Quality Incentive Program (QIP) Quality Improvement Activity (QIA) Improving Kt/V Comprehensive Measure Score Tish Lawson Team Leader February Kick Off Meeting Overview Facility Selection QIP-QIA
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Bedside Shift Reporting
 INCHES 1 2 3 4 5 6 Bedside Shift Reporting Pre-Bedside Checklist: 1. Notify PT/Family 30-60 minutes Before Report Starts 2. Check Pain Score/Adm. Meds if Needed Bedside Report Guide: 1. Introduce Oncoming
INCHES 1 2 3 4 5 6 Bedside Shift Reporting Pre-Bedside Checklist: 1. Notify PT/Family 30-60 minutes Before Report Starts 2. Check Pain Score/Adm. Meds if Needed Bedside Report Guide: 1. Introduce Oncoming
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
JOINT COMMISSION IS COMING!
 NEWS AND INFORMATION FROM GUARDIAN JOINT COMMISSION IS COMING! It is that time again! Joint Commission is expected to survey Guardian for continued certification anytime between October 1, 2012 and February
NEWS AND INFORMATION FROM GUARDIAN JOINT COMMISSION IS COMING! It is that time again! Joint Commission is expected to survey Guardian for continued certification anytime between October 1, 2012 and February
1. Create a heightened awareness of clinical risks and enterprise-wide challenges associated with misuse of copy and paste.
 1 2 Disclaimer The information, examples and suggestions presented in this material have been developed from sources believed to be reliable, but they should not be construed as legal or other professional
1 2 Disclaimer The information, examples and suggestions presented in this material have been developed from sources believed to be reliable, but they should not be construed as legal or other professional
Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints
 Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints Barbara Seitz, RHIA Privacy Officer/Director of HIM South Peninsula Hospital Homer, AK Becky Buegel, RHIA
Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints Barbara Seitz, RHIA Privacy Officer/Director of HIM South Peninsula Hospital Homer, AK Becky Buegel, RHIA
Patient and Family Centered Care
 Patient and Family Centered Care Lessons Learned from Changing Organizational Culture A Leader s Perspective: Maryland Patient Safety Conference March 2015 Chuck Hofius has indicated no conflict of interest
Patient and Family Centered Care Lessons Learned from Changing Organizational Culture A Leader s Perspective: Maryland Patient Safety Conference March 2015 Chuck Hofius has indicated no conflict of interest