gh Group Visits and 03/18/14 that lead 3. Be able delivery model 4. Be able CONTENTS CME Credit Page 2: Description of CHAMPS Page 3:
|
|
|
- Derek Carson
- 5 years ago
- Views:
Transcription
1 SUPPLEMENTARY INFOR RMATION PACKET Improving Diabetes Care throug gh Group Visits and Patient-Centered Medical Home (PCMH) Principles Presented by: Karen A. Funk, MD, MPP, Vice President of Clinical Services, Clinica Family Health Services Live Broadcast Date/Time: Tuesday, March 18, :30am 1:00pm Mountain Time / 12:30 2:00pm Central Time Event Overview: This webcast will introduce participants to a group-based care delivery model utilized at Clinica Family Health Services that has been transforming over the last ten years. Dr. Funk will outline the essential components of the unique care team that staffss group visits as well as the care team pods that support individual patient visits. She will explain how essential components of this care delivery model increase access to primary care and increase quality outcomes, and review core components of the this care delivery model that reflect the framework of a patient-centered medical home. Learning Objectives: Participants will: 1. Learn about a group visit model of care for chronic disease utilized at Clinica Family Health to care for diabetic patients. 2. Understand the componen nts of the group visit Clinica care team that lead to improved quality outcomes for diabetic patients. 3. Be able to identify how the components of the group visit care delivery model can increase access and increase quality. 4. Be able to identify core components of the PCMH model that promote quality outcomes for diabetic patients at Clinica Family Health. CONTENTS Page 2: Page 3: CME Credit CHAMPS Archives Description of CHAMPS Speaker Biography Additional CHAMPS Resources Page 4-32: Speaker Slides Community Health Association of Mountain/ /Plains States (CHAMPS) 1
2 CONTINUING MEDICAL EDUCATION (CME) CREDIT This Live activity, Improving Diabetes through Patient-Centered Medical Home (PCMH) Principles, with a beginning date of 03/18/2014, has been reviewed and is acceptable for up to 1.50 Prescribed credits by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Application for CME credit for the archived version of the event will be filed immediately following the live webcast. CHAMPS ARCHIVES This event will be archived online and on CD-ROM. The online version will be available within two weeks of the live event, and the CD will be available within two months. CHAMPS will all identified participants when these resources are ready for distribution. For information about all CHAMPS archives, please visit DESCRIPTION OF CHAMPS is a non-profit organization dedicated to supporting all Region VIII (CO, MT, ND, SD, UT, and WY) federally-funded Community, Migrant, and Homeless Health Centers so they can better serve their patients and communities. Currently, CHAMPS programs and services focus on education and training, collaboration and networking, workforce development, and the collection and dissemination of regional data. For more information about CHAMPS, please visit SPEAKER S BIOGRAPHY Dr. Funk has been a family physician at Clinica Family Health Service s Lafayette Clinic since 2004 and took on the role of Assistant Medical Director in She graduated with distinction from Swarthmore College where she spent a year at the London School of Economics and Political Science. She went on to the University of Chicago where she graduated with honors with a Master s degree in Public Policy. Following graduate school, Dr. Funk served as the Quality Improvement Coordinator for Planned Parenthood of Greater Chicago. Somewhere along the way, someone convinced Karen that she would be a great physician and in 2001 she received her M.D. from the University of Illinois. Dr. Funk was an Albert Schweitzer Fellow, which involved working with a Community Health Center in Chicago providing group based education to teens on obesity prevention, healthy sexuality, and pregnancy prevention. With family ties in Colorado and a growing family, Karen completed her residency in Family Medicine at Rose Medical Center. 2
3 ADDITIONAL CHAMPS RESOURCES Improving Diabetes Care through Group Visits and PCMH Principles, Diabetes Treatment Resources A compilation of resources to support the treatment of patients with diabetes, including evidence-based clinical guidelines and recommendations, articles and reports relating to diabetes, webcasts and other online CME opportunities, provider treatment tools, patient education tools, and other helpful links Diabetes.html Patient-Centered Medical Home (PCMH) Information and Resources Materials to aid health centers who are brand new to PCMH, those who have started the process of becoming a PCMH, and those who have applied for PCMH recognition/accreditation and are continuing the transformation process; includes history, definitions, recognition/accreditation steps and guides, tools for building a PCMH, training sources, etc. Templates and Samples of PCMH Policies and Procedures Samples of PCMH policy and procedure templates, including admission and scheduling, community collaboration, etc., as well as examples of PCMH recognition documents submitted by two health Region VIII health centers in their quest for 2008 NCQA Level 3 PCMH recognition Patient Satisfaction/Experience Surveys and Patient Activation/Engagement Resources Goals, information, and resources on measuring patient satisfaction and/or patient experience, and information about patient activation and engagement including strategies on activating/engaging patients to create better experiences and health outcomes 3

 by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Application for 1.")
4 IMPROVING DIABETES CARE THROUGH GROUP VISITS AND PCMH PRINCIPLES Presented by: Karen A. Funk, MD, MPP, with the support of Justin Wheeler, MD Vice Presidents of Clinical Services, Clinica Family Health Services Tuesday, March 18, :30AM-1:00PM Mountain Time 12:30-2:00PM Central Time Hosted by: This Live activity, Improving Diabetes through Patient-Centered Medical Home (PCMH) Principles, with a beginning date of 03/18/2014, has been reviewed and is acceptable for up to 1.50 Prescribed credit(s) by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Application for 1.50 Prescribed credits for the archived version of the event will be filed immediately following the live event. Karen Funk has indicated that she has no relationships to disclose relating to the subject matter of this presentation. POLL Which of the following best fits your role at your organization? 4
5 POLL How many total people are watching this event at your computer (yourself included)? Objectives Participants will learn about a group visit model of care for chronic disease utilized at Clinica Family Health to care for diabetic patients. Participants will understand the components of the group visit Clinica care team that lead to improved quality outcomes for diabetic patients. Participants will be able to identify how the components of the group visit care delivery model can increase access and quality. Participants will be able to identify core components of the PCMH model that promote quality outcomes for diabetic patients at Clinica Family Health. 5
 2010-2014: recertification NCQA PCMH all")
6 Primary care redesign at Clinica Family Health over the last ten years: a timeline Patient-Centered Medical Home Journey 1977: Founded 1998: Joined IHI Chronic Care Collaborative 2000: Delivery System Redesign : Planned Care Approach to QI : Spread & Sustain Improvements; NCQA Level 3 PCMH, NCQA DRP (Diabetes Recognition Program) : recertification NCQA PCMH all sites, recertification NCQA DRP all sites FUTURE = care team redesign PODS 2.0 and patient activation! Who is Clinica Family Health? Demographics >40,000 active pts Medical Dental Behavioral Health Pharmacy 49% uninusured 56% <Poverty, 98% <200% Poverty 6

7 Growing Groups at Clinica 2000: Began office redesign process and looked at group visits as a method of alternative care 2001: Held first PDSA Initial Prenatal group visit 2009: Conducted 845 group visits = 3.4 groups per day that the clinic was open 2012: 1466 medical group visits Clinica s group visit model 9 Essential Elements for Designing and Managing Group Care 7
8 1. Assemble the right people Designing group visits should not be done in isolation. Group visits effect all areas of the clinic and require input from a cross functional team. A Clinica Group Visit Committee Operations Manager (Front Office) Receptionist (Front Office) Nurse Manager (Back Office) Medical Assistant (Back Office) Case Manager (Care Provider/Group Facilitator) Provider (Care Provider) Behavioral Health Provider (Care Provider) Call Center Attendant (Scheduling/Call Center) Committee Facilitator Minute Taker 8
9 Key Components for a Successful Group Visit Committee Have a process for testing and retesting newly implemented groups -- Plan Do Study Act (PDSA) Get feedback from staff and patients! Be ready and willing to hear about the things that aren t working.this is what you need to address at your next meeting Don t take on too much at once. Create success, then move on What do you think? Which one of the following individuals IS NOT part of a Clinica Family Health group visit committee? 1. front desk staff 2. cleaning crew member 3. medical assistant 4 provider 9
10 #2 Know what you want to accomplish Are you dealing with supply/demand challenge and want to improve access for your patient population? (Access Groups) Do you want to improve a specific population s health outcomes? (Continuity Groups) Clinica Diabetes Groups An example of a continuity group We draw patients from an individual provider s panel or if we have trouble filling, all PCPs from the same care team Same group of patients will meet quarterly Planned care is organized around these visits 1. HBA1C, self-management goals, blood pressure, BMI at every visit 2. Visit #1 = cholesterol screening, creatinine screening, screening for urine microalbuminuria 3. Visit #2 = foot checks, flu shots, pneumococcal shots 4. Visit #3 = retinal camera screening for retinopathy 10

11 #3 Create and Use Tools to Assist You Our big lesson learned: Don t Recreate the Wheel Develop a design tool that asks the questions you need to answer in order to design and manage a smooth running group Designing a Group Visit 11
12 Chronic Disease Content Threads Nutrition Health and Prevention Communication Role Adjustment CORE CONTENT Medication Use Physical Activity Family Relationships Mental Health Sexuality Use the content thread concept to design your curriculum Diabetes Group Visit Topic Checklist What is Diabetes? Diabetes self-management Healthy eating Be Active Medications Monitoring blood sugar Preventing complications Problem solving skills Controlling blood sugar Controlling your weight Alcohol and smoking Blood pressure Cholesterol Healthy Coping Depression Stress and relaxation Sexual issues Changing your behavior Working with your PCP Retinal Camera Screening 12
13 What do you think? All of the following could be potential content threads or discussion topics for a diabetes group EXCEPT? 1. healthy nutrition 2. carbohydrate counting 3. benefits of breastfeeding 4. depression #4 Communication For each group visit, determine who needs to know about the group visit For each group visit, determine when the staff and/or patients need to be notified and/or reminded of the group visit Develop processes and tools to ensure that communication occurs! Ask yourself, How will people know? 13

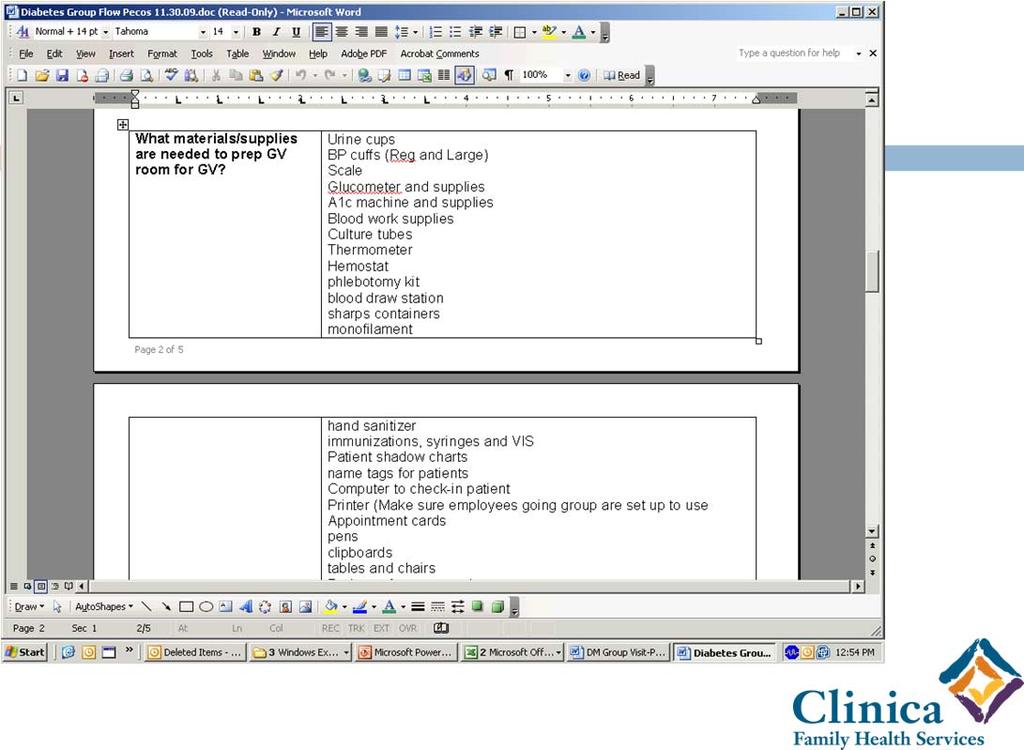
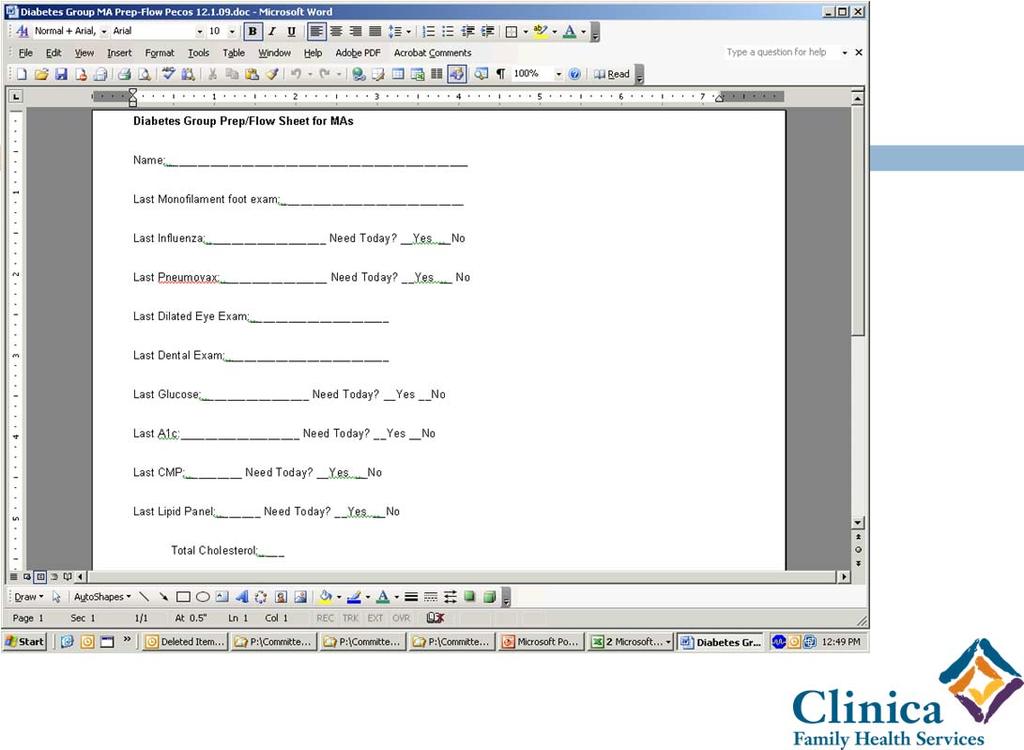
14 #5 Be Prepared for the Group Visit Being prepared for the group visit is ESSENTIAL to the success of the group visit! 14
15 15

16 An Improved Approach 16
17 #6 Tracking and Coordination of Groups Tracking and managing of group visit care is one of the most complicated and critical elements to a successful group visit process 17
18 Things to consider when creating a tracking/managing system for group visits: What are your limiting factors on how many group visits you can conduct in a given day/week/month/year? Will one person have oversight of the group visit process or will multiple people manage it? Can the group have a permanent date/time schedule? How will the room be held/reserved for the group visit? #7 Patient Recruitment Build it and they will come Depending on the group visit type, recruitment can occur in various ways: Provider recruitment Flyers/postings Registries/reports that generate cohorts that the clinic can solicit by calling/mailing Group visit recruitment from previous group Opt Out Call center attendant offers group visit when patient calls for an appointment 18

19 #8 Measure Goals and Objectives Develop techniques that will allow you to know if the objective of the group is being met. Consider the purpose of the group and why you created it? Are there health outcomes you want to achieve? Are there visit/access numbers you are want to achieve? How will you measure patient satisfaction with the group? How will you measure the staff satisfaction with the group? How will you measure success and with what frequency? 19
20 #9 Staffing Groups All of the hard work that the group visit committee puts into planning will not impact the success of group visits unless the staff participating in the group have proper training on their roles and expectations Staff Training Incorporate the expectations related to group visits into the employee job description and evaluation tools Have and keep up to date the necessary training materials for each group visit type Meet with staff prior to a new group visit type in the area where the group will occur and review the flow and materials related to the group 20



21 DIABETES MANAGEMENT Pecos Case Manager Training Schivonne Keller, MS, RD Maria Fernanda Botero, MS, RD 21
 Visit Design Check in 30 min vital signs self-assessment labs Group discussion -1 hour Provider assessment in group Case manager facilitation based on content thread CM support with goal setting")
22 A Clinica Diabetic Group In Action Provider Medical Assistant or two depending on the size Case manager Nurse or dietician Office technician THE PATIENTS (and often other family members!) Visit Design Check in 30 min vital signs self-assessment labs Group discussion -1 hour Provider assessment in group Case manager facilitation based on content thread CM support with goal setting Wrap up -30 min Social time for patients Provider follow-up assessment and charting 22
23 What do you think? Which one of the following is an essential item needed for a successful diabetic group visit? 1. paper chart 2. positive attitude of the patient 3. careful planning ahead 4. ½ a clinic day to hold the group I have found that a well-supported group (office techs, MA's, nurse, CM) is the epitome of patient-centered, efficient care. We can accomplish so much education and problem-solving as a group that could never be done in 20 minute patient slots. ~Dr Josh Messer 23







24 Overview of PCMH Framework: The Key Components Access to Care Care Team & Staffing Chronic Disease Care EHRs Patient-Centered Care Practice Efficiency Quality & Safety What do you think? Group visits can INCREASE access for the patients in your practice. TRUE or FALSE? 24



25 PCMH framework Access to Care More patients seen per hour Reduced wait times for acute & chronic care 2 hours on the care team = six patient care slots 1:1 2 hours in diabetes group = eight to twelve patients in group Group visits enhance open access for our patients on the care team 25




 26")
26 Overview of PCMH framework Access to Care Care Team & Staffing Team comes together to deliver care. Overview of PCMH framework Access to Care Care Team & Staffing Chronic Disease Care Systematic approach Focus on outcomes & planned care (Care Planner) 26

27 PCMH framework Access to Care Care Team & Staffing Chronic Disease Care EHRs Systematic use of Diabetes Template 27



28 PCMH framework Access to Care Care Team & Staffing Chronic Disease Care EHRs Patient-Centered Care Patient as agent of engagement/activation. Patient-Centered Care Patients need to be involved in self care activities and their own health assessment 28

29 Patient Activation = Patient-Centered Care What Self-Management Support is not: 1. Didactic patient education 2. Waiting for patients to ask for help 3. Sage on the stage 4. You should 5. Finger wagging 6. Lecturing PCMH framework Access to Care Care Team & Staffing Chronic Disease Care EHRs Patient-Centered Care Practice Efficiency Improved resource utilization Quality & Safety 29


30 PCMH framework Access to Care Care Team & Staffing Chronic Disease Care EHRs Patient-Centered Care Practice Efficiency Quality & Safety Improved metrics & quality outcomes 30







31 Improving Chronic Disease Outcomes Outcome Group Visit Traditional HTN BP<140/90 80% 76% DM BP<130/80 43% 40% DM LDL<130 90% 86% DM Nephropathy 43% 40% DM LEAP-foot 80% 66% Tobacco counsel. 78% 61% Current SM goal 93% 65% THE GOAL : A Patient Centered HEALTH Home! Laboratory Services Primary Medical Services Family Medicine Pediatrics Obstetrics Vaccinations Group Visits Chronic Disease Management Home Visits In-Patient Hospital Services Nutritional Support Well Visits through the Life Cycle Behavioral Health Services Oral Health Services 31
 credit, you must complete the CME questions found at the end of the Evaluation.")

32 Questions? Thank You for Joining Us! Your opinions are very important to us. Please complete the event Evaluation for this webcast. If you are applying for Continuing Medical Education (CME) credit, you must complete the CME questions found at the end of the Evaluation. Each person should fill out their own Evaluation/Credit Survey. Please refer to the SurveyMonkey link provided under the Handouts tab of the online event. The same link was provided in the reminder sent out in advance of the event, and will be included in a follow-up to those logging onto the live event. Please pass the link along to others viewing the event around a shared computer. Visit for information about other live and archived CHAMPS webcasts. 32
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Please stand by. There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1
 Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
Quality Peer Group UDS Best Practices and Data Sharing 9/9/16. ohiochc.org
 1 Quality Peer Group UDS Best Practices and Data Sharing 9/9/16 ohiochc.org Presenters 2 Ashley Ballard Director of Clinical Quality Tiffany Blair Quality Improvement Coordinator Dr. Wymyslo Chief Medical
1 Quality Peer Group UDS Best Practices and Data Sharing 9/9/16 ohiochc.org Presenters 2 Ashley Ballard Director of Clinical Quality Tiffany Blair Quality Improvement Coordinator Dr. Wymyslo Chief Medical
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Patient-Centered Medical Home
 2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
A Case Study in Primary Care Access: Clinica Family Health. Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services
 A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
The Virtual Connection: Electronic Visits. Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009
 The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Patient-Centered Medical Home
 2017 Primary Care Federally Qualified Health Centers (FQHCs) January 2017 (released December 2016) HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent
2017 Primary Care Federally Qualified Health Centers (FQHCs) January 2017 (released December 2016) HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent
Patient-Centered Medical Home
 2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
2016 Member Incentive. Program Descriptions. Our mission is to improve the health and quality of life of our members
 2016 Member Incentive Program Descriptions Our mission is to improve the health and quality of life of our members Member Incentive Program Descriptions I. Purpose Passport Health Plan (Passport) has developed
2016 Member Incentive Program Descriptions Our mission is to improve the health and quality of life of our members Member Incentive Program Descriptions I. Purpose Passport Health Plan (Passport) has developed
Expanding Access Through. Team Care. Carolyn Shepherd, M.D.
 Expanding Access Through Team Care Carolyn Shepherd, M.D. Clinica Family Health Services 2013 42,000 Patients 206,000 Ambulatory visits 5 Clinical sites Clinica Family Health Services 50% uninsured 40%
Expanding Access Through Team Care Carolyn Shepherd, M.D. Clinica Family Health Services 2013 42,000 Patients 206,000 Ambulatory visits 5 Clinical sites Clinica Family Health Services 50% uninsured 40%
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Foreign Service Benefit Plan
 Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Wellness Guide for LCRA Retirees
 2016 Wellness Guide for LCRA Retirees Contents 2 How the EmPOWER program works 3 How to register 3 Text message reminders 4 Member health assessment 4 Biometric screening 5 Earning points and saving money
2016 Wellness Guide for LCRA Retirees Contents 2 How the EmPOWER program works 3 How to register 3 Text message reminders 4 Member health assessment 4 Biometric screening 5 Earning points and saving money
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
My Complete Medications List
 Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
Guide to Accessing Quality Health Care Spring 2017
 Guide to Accessing Quality Health Care Spring 2017 MolinaHealthcare.com 5771749DM0217 MyMolina MyMolina is a secure web portal that lets you manage your own health from your computer. MyMolina.com is easy
Guide to Accessing Quality Health Care Spring 2017 MolinaHealthcare.com 5771749DM0217 MyMolina MyMolina is a secure web portal that lets you manage your own health from your computer. MyMolina.com is easy
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
CLINICA FAMILY HEALTH
 Design Solutions to Improve Healthcare ccess and Outcomes: CLINIC FMILY HELTH at Clinica Family Health People s Medical Clinic, Boulder, CO INSIDE YOU WILL LERN BOUT: How facility design facilitates population
Design Solutions to Improve Healthcare ccess and Outcomes: CLINIC FMILY HELTH at Clinica Family Health People s Medical Clinic, Boulder, CO INSIDE YOU WILL LERN BOUT: How facility design facilitates population
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Diabetes. Evidence Based/ Team Based Care in a Community Health Center ---
 Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES
 Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES 1 Name three approaches that address specific health needs of seniors Discuss how different disciplines may be integrated
Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES 1 Name three approaches that address specific health needs of seniors Discuss how different disciplines may be integrated
INTEGRATED CARE SERVICE AND OUTCOMES
 DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH
 What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
Health First Wellness Incentive
 Health First Wellness Incentive The Health First Wellness Incentive has been set up as a reward for taking steps to either maintain or obtain a healthy lifestyle. Taking healthy actions and becoming a
Health First Wellness Incentive The Health First Wellness Incentive has been set up as a reward for taking steps to either maintain or obtain a healthy lifestyle. Taking healthy actions and becoming a
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs
 HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Highmark Lifestyle Returns SM Enjoy the many rewards of a healthy lifestyle!
 SM Enjoy the many rewards of a healthy lifestyle! Page 1 of 11 Take charge of your health and enjoy the benefits! We know that the way we live has a real impact on the way we feel. When we take care of
SM Enjoy the many rewards of a healthy lifestyle! Page 1 of 11 Take charge of your health and enjoy the benefits! We know that the way we live has a real impact on the way we feel. When we take care of
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
24/7 Nurseline and Future Moms. Presenters: Blanche Callahan
 24/7 Nurseline and Future Moms Presenters: Blanche Callahan Agenda Goal: Learn about 24/7 NurseLine and Future Moms including how to promote the programs in the workplace. Frequently Asked Questions: 24/7
24/7 Nurseline and Future Moms Presenters: Blanche Callahan Agenda Goal: Learn about 24/7 NurseLine and Future Moms including how to promote the programs in the workplace. Frequently Asked Questions: 24/7
2016 Mommy Steps Program Descriptions
 2016 Mommy Steps Program Descriptions Our mission is to improve the health and quality of life of our members Mommy Steps Program Descriptions I. Purpose Passport Health Plan (Passport) has developed approaches
2016 Mommy Steps Program Descriptions Our mission is to improve the health and quality of life of our members Mommy Steps Program Descriptions I. Purpose Passport Health Plan (Passport) has developed approaches
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Making the Medical Home Work/Teamwork in Primary Care. Amy Mullins, MD Trinity Clinic Whitehouse
 Making the Medical Home Work/Teamwork in Primary Care Amy Mullins, MD Trinity Clinic Whitehouse Objectives Objectives Include: 1. Learn how to build your office team. 2. Understand various ways to use
Making the Medical Home Work/Teamwork in Primary Care Amy Mullins, MD Trinity Clinic Whitehouse Objectives Objectives Include: 1. Learn how to build your office team. 2. Understand various ways to use
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be faxed back.
 Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
2013 Mommy Steps. Program Description. Our mission is to improve the health and quality of life of our members
 2013 Mommy Steps Program Description Our mission is to improve the health and quality of life of our members I. Purpose Passport Health Plan (PHP) has developed approaches to the management of members
2013 Mommy Steps Program Description Our mission is to improve the health and quality of life of our members I. Purpose Passport Health Plan (PHP) has developed approaches to the management of members
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
CCHN Clinical Quality Improvement Plan
 CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado
CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
Welcome to BCHC Your Medical Home
 START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program
 + Welcome Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program March 6, 2012 We will begin promptly @ 1 PM EST Event
+ Welcome Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program March 6, 2012 We will begin promptly @ 1 PM EST Event
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Falcon Quality Payment Program Checklist- 2017
 Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Primary Care Innovations: Stories from the Field. PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012
 Primary Care Innovations: Stories from the Field PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012 In Search of Joy in Practice Co-Investigators Christine Sinsky- PI Tom Bodenheimer-PI
Primary Care Innovations: Stories from the Field PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012 In Search of Joy in Practice Co-Investigators Christine Sinsky- PI Tom Bodenheimer-PI
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
National Committee for Quality Assurance
 National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
WWS Health & Wellness Center. Participant Information Guide
 WWS Health & Wellness Center Participant Information Guide February 2016 Welcome to the WWS Health & Wellness Center Thank you for choosing the WWS Employee Health & Wellness Center. Our team is committed
WWS Health & Wellness Center Participant Information Guide February 2016 Welcome to the WWS Health & Wellness Center Thank you for choosing the WWS Employee Health & Wellness Center. Our team is committed
Medical Record Review Tool Standards with Definitions
 WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
Piedmont Access to Health Services. Standing Orders for Patient Work-ups
 Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Minnesota CHW Curriculum
 Minnesota CHW Curriculum The Minnesota Community Health Worker curriculum is based on the core competencies that are identified in Minnesota s CHW "Scope of Practice." The curriculum also incorporates
Minnesota CHW Curriculum The Minnesota Community Health Worker curriculum is based on the core competencies that are identified in Minnesota s CHW "Scope of Practice." The curriculum also incorporates
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated