Continuous Monitoring of Patients on Opioids: Initiatives at Community Health Network and Methodist Specialty and Transplant Hospital
|
|
|
- Alfred Thomas
- 5 years ago
- Views:
Transcription
1 Continuous Monitoring of Patients on Opioids: Initiatives at Community Health Network and Methodist Specialty and Transplant Hospital Friday, August 26, 2016
2 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National Coalition for Infusion Therapy Safety National Coalition to Promote Continuous Monitoring of Patients on Opioids Compendium: Opioid Safety & Patient Monitoring National Coalition for Alarm Management Safety Compendium: AAMI Foundation Management of Clinical Alarm Please Consider Making a Donation!

3 A Special Thanks






4 Thank You to Our Premier Industry Partners Without their financial support, we would not be able to undertake the various initiatives under the National Coalition to Promote Continuous Monitoring of Patients on Opioids. The AAMI Foundation and its co-convening organizations appreciate their generosity. The AAMI Foundation is managing all costs for the series. The seminar does not contain commercial content. Diamond Platinum Gold

5 LinkedIn Questions Please post questions on the AAMI Foundation s LinkedIn page. OR Type a question into the question box on the webinar dashboard.
6 Nursing Continuing Education Disclosure Statement This seminar is jointly provided today with our co-provider, the National Association of Clinical Nurse Specialists (NACNS). 1.0 contact hour will be awarded for this seminar. This seminar may be accessed online at the AAMI Foundation website for nursing CE up to two years from today s date. This continuing nursing education activity was approved by the Alabama State Nurses Association, an accredited approver by the American Nurses Credentialing Center's Commission on Accreditation (ANCC). Criteria for successful completion includes attendance at the session and submission of a completed evaluation form. You can submit the fee for the CE credit by going to the AAMI store at (link will be sent in follow-up ). A link to the evaluation form will be sent to you for completion and a certificate sent to you upon completion of the evaluation. The planning committee members have declared no conflict of interest along with our faculty for today s session. Contributions to the AAMI Foundation have been received from the identified sponsors to support program initiatives and projects. However, the program content for today s seminar has been planned independently by AAMI staff with the seminar presenters. Approval of the continuing education activity does not imply endorsement by the provider, ANCC or the Alabama State Nurses Association.
7 Polling Questions
8 Speaker Introductions Julie Painter MSN RN OCN, Clinical Nurse Specialist, Community Health Network Indianapolis, Indiana Theresa Kloewer, MSN, RN Vice President of Nursing Methodist Specialty and Transplant Hospital San Antonio, Texas
9 Community Health Indianapolis Indiana We are: 7 Hospital System >2million patient encounters/year 1049 staffed beds 53,576 Inpatient admissions/year 12, 662 Inpatient surgeries/year Outpatient visits >1million/year 82, 274 Outpatient surgeries/year ER visits 273,941 Births 7,899
10 Smart Pump Technology We were early adopters of CareFusion Smart Pump technology in 2007 We utilize smart pumps, Patient controlled analgesia modules, etco2 modules & syringe modules Our patient care delivery with products, processes, policies & interventions are standardized to reduce variation in care & reduce harm across all facilities and the continuum
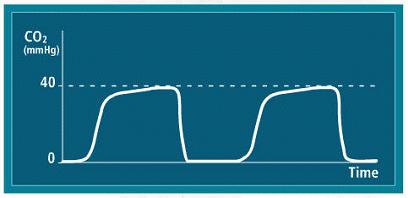
11 What is capnography & what is its value? Capnography has evolved into a standard of monitoring during anesthesia because it has proven itself to be a valuable tool in recognizing ventilatory and circulatory events that could potentially lead to deleterious effects
12 Sedation & Ventilation Status Historically we have relied on oxygen levels to tell us about a patients respiratory/ventilation status Oximetry is not an indicator of ventilation status Measurement of CO2 is a better predictor of ventilation status and helps us intervene earlier to address respiratory compromise before needing reversal agents or a higher level of care
13 Our Journey Early adopters of smart pump technology-2007 All 7 hospitals utilize same products, same policies and have a process to promote evidence based practice, standardization & reduction of variation #1 customer is the patient-do what is best for our patients! Goal is to reduce harm & provide the highest quality, safest care with the best outcomes possible Etco2 often only used with patient controlled analgesia
14 Impetus for Improvement Data from largest facility within our network, revealed a high number of patients with oversedation requiring consultation from rapid response team for respiratory compromise; use of naloxone for reversal; and many required a higher level of care & monitoring Note this project was before the Partnership in Patient Safety national projects to reduce adverse drug events with naloxone
15 Improvement Team Project Lead: Julie Painter Clinical Nurse Specialist Physician Champion: Scott Vore MD-Anesthesia & Michael Caldwell MD-Anesthesia Members: Director, manager of PACU, pharmacy, nursing leaders from acute care units
16 Goal of Improvement Goal: Reduce unwanted respiratory depression due to opioids post-operatively & reduce naloxone utilization. Data Revealed: Higher amounts of naloxone administered on the largest campus that did surgeries & at the time we were only using etco2 monitoring on PCA patients. Many patients with high BMI, COPD &/or Sleep apnea higher risk but not aware Finding: PACU staff & leaders were not aware of patient compromise once they left PACU
17 The Improvement Interventions Developed & implemented education for all PACU staff about data & how the team would work to reduce harm Implemented end tidal CO2 monitoring on all PACU patients before they left PACU Improved bedside handoff communication between PACU RN & Unit receiving RN about any issues or concerns, specifically what meds had they received that have potential to cause sedation Began process improvement October 2013 & analyzed process & data through all of 2014 and in 2015 began the spread of improvement through all facilities Patient education sheet developed with talking points
18 Changes in the PACU All patients have an end tidal CO2 module attached to Infusion pump with nasal cannula in place in the PACU The etco2 module will be activated & turned on & measuring as PACU transports patient from PACU to acute care Discharge criteria for PACU remains the same otherwise Note elevation in etco2 alerts us to help patient take deep cleansing breathes & to exhale to rid of excess CO2

19 End tidal CO2 monitoring 19


20 End tidal CO2 Module & Controls


21 Nasal Cannula
22 Key Considerations to Success Have the right team members Educate patient regarding cannula Have experts and leaders who can serve as champions aka barrier busters Engage staff & help them digest & understand the data Make it real---take the data, deep dive a couple of cases & develop a case story---reality sinks in more than probability
23 The Challenges Fear of alarms bothering patients & decreasing patient satisfaction Orders being entered to discontinue etco2 monitoring Staff ability to articulate & explain to patients why this is important & why we do it Providers desiring to select only those patients at risk for sedation? Inability to know who is at risk-providers asked why put on everyone?
24 Hardwiring Change Be methodical-don t try to do all places at one time Support both areas PACU and Acute care on go live day and ongoing after Train champions & unit experts Have building resources Immediately address concerns or issues & resolve face to face Realize change takes time & when busy we easily digress to old habits Monitor events real-time-we discuss naloxone events daily in our safe day huddles & consider them ADE s until reviewed
25 Current State Complete implementation across acute care Expansion to OB Staff nurse can place etco2 module on any patient with concerns of compromise & increased risk of sedation-this allows a nurse the ability to better assess their patients in a more accurate way
26 Current State Project team working as a network to verify that all end tidal CO2 monitoring during procedures are using most current technology Note that naloxone use remains significantly low based on percentage of patients who receive opioids & would have potential for reversal Looking beyond opioids now & other sedation medications
27 Methodist Specialty and Transplant (MSTH) Theresa Kloewer, MSN, RN Vice President of Nursing Methodist Specialty and Transplant Hospital
28 About Methodist Specialty and Transplant (MSTH) MSTH is a 275-bed acute care facility Part of Methodist Healthcare System in San Antonio, Texas MSTH is known for unique specialized care in: Kidney, pancreas and liver transplant Multi-specialty surgical services Medical rehabilitation Psychiatry Emergency medicine
29 Learning Objectives 1. Describe why failure-to-rescue is important for all hospitals, and the role for technology that is driven by clinical need. 2. Discuss the major outcome benefits associated with early detection of a deteriorating patient. 3. Define components of a vital sign surveillance monitoring solution covering technical and clinical practice and outcome metrics.
30 Failure-to-Rescue Definition: Failure to prevent a clinically important deterioration from a complication of an underlying illness or a complication of medical care
31 Nursing Surveillance The purposeful and ongoing collection and analysis of information about the patient and the environment for use in promoting and maintaining patient safety. Bulechek, G. M., Butcher, H. K., & Dochterman, J. M. (2008). Nursing interventions classification (NIC) (5th ed.). St. Louis, MO: Mosby.
32 Why Is Failure-to-Rescue Important? Up to 75 percent of adverse events and preventable deaths 1 84 percent of patients exhibit signs of deterioration 2 bed 1 2/Documents/I2_Presentation_Diagnostics_Haraden.pdf 2 AHA database, Schein RM et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 1990;98: Up to 60 percent of all hospital patients are monitored continuously 2 In order to rescue, one needs to know they re deteriorating and respond immediately 3
.")
33 Why Is Failure-to-Rescue Important? Wendlandt, B et al. Association between ICU Transfer Delay and Hospital Mortality: A Multicenter Investigation (abstract). Journal or Hospital Medicine 2015:10 (suppl 2). For every one-hour increase in transfer delay, the odds of an in-hospital death increased 3 percent For patients who survived until discharge, delayed transfer was associated with a longer length of stay
34 Why Is Failure-to-Rescue Important? The Impact of Nursing Surveillance on Failure to Rescue Leah L. Shever, PhD, RN When nursing surveillance is performed an average of 12 times a day or greater, there is a significant decrease in the odds of experiencing failure to rescue Research and Theory for Nursing Practice: An International Journal, Vol. 25, No. 2, 2011

 Efficiency number of steps and time for vital signs")
35 Metrics for Quality Improvement Early identification of deterioration (sepsis, opioid induced hypoventilation, reoperation, hypertension, etc.) Efficiency number of steps and time for vital signs Operational Code blue and rapid response calls Satisfaction
36 Three Fundamental Problems According to the Institute for Healthcare Improvement and the 5 Million Lives campaign (2007): 1. Failures in planning includes assessments, treatments, goals 2. Failure to communicate patient-to-staff, staffto-staff, staff-to-physician, etc. 3. Failure to recognize a problem These three problems often lead to failure to rescue.



37 Recognizing a Problem Vital signs obtained for five minutes every four hours represents 2 percent of a patient s day Yet it represents hours of RN/PCT time for each shift RNs are in patient rooms for 1.5 hours out of a 12-hour shift 1 Spend less than 7 percent of time assessing the patient 3 Average of nine cognitive shifts per hour 2 Refocus from one patient to another every six to seven minutes Rescue-DatamdashAre-You-Ready.html## 2. JONA, Volume 42, Number 7/8, pp Hendrich Study 4. AHA database, 2013
38 Condition vs. Surveillance Monitoring Condition Monitoring: use of a patient monitoring system which is limited to clinical targets based upon a patient s unique, identifiable risk profile Surveillance Monitoring: use of a patient monitoring system which has continuous broad clinical targeting independent of a patient s unique, identifiable risk profile, recognizing that all risks cannot be identified a priority
39 About Methodist Specialty and Transplant Two medical-surgical type units were identified to introduce surveillance and continuous vital sign monitoring: Transplant Unit: 57 beds that provide pre- and post-transplant care Surgical Unit: 47 beds that provide post-surgical care to bariatric, endocrine, gyn, urological, maxofacial, vascular, colon-rectal, plastics and general surgery patients
40 Our Method Methods Patients admitted to the medical-surgical and transplant care unit at MSTH from July to October 2015 were included Materials Continuous vital sign monitoring for heart rate, blood pressure, respiratory rate and oxygen saturation, including alarms and alerts, to notify the nurse of necessary intervention
41 Workflow Analysis - Efficiency Analyzing traditional workflow compared to the new workflow state with selected continuous vital sign system Identifying operational efficiencies Using workflow analysis tool(s) to gather data 1. Nurse finds traditional vital sign device 2. Nurse brings device to patient room 3. Nurse takes vital signs in three stages: temperature, blood pressure, pulse oximetry 4. Nurse returns vital sign device to storage location 5. Nurse documents vital signs in electronic health record (or validates if automatically transmitted)
42 Workflow Time Spent Per Day Overall assumptions: 40-bed unit, vitals every four hours for a 24-hour period Continuous vital sign assumptions: Calibrate and bump twice/day, initial setup for 1/3 of patients assuming an avg. 3-day length of stay. Traditional Vital Signs Counts: 40 pts x 6 vitals/day = 240 vitals in 24 hours Calculation: 5 min each x 240 vitals = 1200 min, or 20 hrs Total: 20 hours in a 24 hr time period Continuous Vital Signs Counts: 40 pts x.33 set up = 13 set ups in 24 hours 40 pts x 2 calibrate = 80 calibrations 40 pts x 2 bump = 80 bump / swap Calculations: 5.9 min x 13 setups = 77 min, or ~ 1.28 hrs 2.65 min x 80 calibrates = 212 min, or ~ 3.5 hrs 3.81 min x 80 bump/swaps = 305 min, or ~5 hrs Total: 9.78 hours in a 24 hour time period Potential 10 hours/day time saving


43 Components Body-worn continuous physiological monitor Four-ounce ICU-grade monitor All vital signs are continuous Wi-fi connectivity EHR-compatible Distributed monitoring and alarming possible

 Based on pulsearrival-time (PAT)")

44 Measurement Basic continuous Monitoring SpO 2 /Pulse Rate Continuous vital signs+ SpO 2 /pulse rate Respiration rate and skin temperature ECG 3 and 5 lead NIBP (cuff-based) Continuous NIBP (cnibp) Continuous non-invasive blood pressure (cnibp) Based on pulsearrival-time (PAT) Initial cuff-based calibration Cuff removed after calibration to measure PAT based beat-tobeat blood pressure ECG P Q R S T P A T PPG Time
45 Results Over 99,500 hours of patient vital sign data were logged There were over 75 clinically meaningful nursing interventions to alarms recorded that either detected or prevented deterioration Interventions were coded to determine early deterioration diagnosis (such as sepsis, hypertension and pulmonary vascular congestion) There were 33 diagnoses related to deterioration. All patients were treated and discharged alive
46 Parameters That Detected Deterioration Parameters That Detected Deterioration Analysis of RN Intervention Logs (10 week sample) RR 15% cnibp 23% Sp02 53% Sp02 HR RR BP HR 9% Events Where Nursing Intervention Prevented Deterioration (10 week sample) Hemodynamic Cardiac 14 Events Events Respiratory

47 Average Alarm Events Per Session Per Day Transplant Unit


48 Average Alarm Events Per Session Per Day Medical-Surgical Unit
49 Event Examples Hemodynamic 66-year-old female admitted with pyelonephritis Alarm: Blood pressure 200/110 on admission day two Intervention: Diltiazem ordered; patient s blood pressure returned to stable
50 Event Examples Pulmonary vascular congestion 55-year-old male with cadaver kidney transplant, post-op day four Alarm: High RR (34) with high cardiac rate (150) and temp (102) Intervention: Chest x-ray ordered, showed pulmonary vascular congestion; sepsis prevented; orders for bumetanide and oxygen; remained on floor and discharged home without further complications
51 Event Examples Cardiac 62-year-old female live donor kidney transplant, history of atrial fibrillation Alarm: High HR alarm (150) Intervention: Wave form on monitor irregular, heart sounds irregular, EKG ordered confirming AFib and rapid ventricular response (RVR); started on metoprolol, repeat EKG showed sinus rhythm with premature atrial contractions; started on amiodarone; remained on floor and discharged home after normal post-transplant hospital course
52 Re-Operation Event Examples Post-op day one for laparoscopic excision of gastric mass Alarm: Low O2 saturation (80) and hypotension Intervention: CT abdomen and upper GI ordered, showed gastric anastomotic site leak; returned to OR for repair of gastric leak; develops respiratory failure due to left base atelectasis, systematic inflammatory response syndrome due to gastric leak and acute respiratory infection due to hypovolemia and hypotension; worked up for deep vein thrombosis and pulmonary embolism (all negative); transferred to telemetry and discharged home
53 Results Staff Comments The [system] has saved lives. I was skeptical until it happened to my patient. Without the [system], we probably would have coded the patient. The [system] alerts help us to be proactive and anticipate changes. It s a timesaver. The [system] helps with healing. We don t have to wake up patients to take vitals.
54 Results Patient Comments I can have a good night sleep. I don t even know it s there. Thanks to your [system] I was comfortable and able to get six-plus uninterrupted hours of sleep additionally and have my data transmitted and recorded accurately.
55 Technology Considerations Need for conducting site survey with vendor to ensure complete Wi-Fi coverage throughout facility Plan resources appropriately to work on interfacing development/testing, for both point of use and connection to EHR Conduct weekly project status calls (to include interfacing) Keep up-to-date project plan and issue log Ensure sufficient physical space for equipment
56 Implementation Challenges Staff (RN and patient care assistant) buy-in Role and responsibility definition Staff training How to use the system How your day changes How to educate patients Physician education Physical storage limitations
57 Conclusions With timely access to more data, nurses on noncritical care units are forming meaningful conclusions to: Improve outcomes Lower costs Tailor responses to meet individual patient needs A continuous vital sign surveillance system can be implemented on any inpatient unit to help identify conditions for immediate intervention and early detection of more serious complications
58 Future/Ongoing Initiatives 9/25/
59 Thank you for attending! If you are interested in obtaining a 1.0 CE credit after you watch this Patient Safety Seminar, you may purchase the credit at the AAMI Store for $25.00 at this link: SEM
60 Mark Your Calendars! September 12, 2016; 12pm to 1pm Continuous Monitoring of Patients on Opioids: Initiative at Evergreen Health in Kirkland, WA Nancee Hoffmeister, MSN, RN, NE-BC VP Nursing Chief Nursing Officer Nancy will discuss how her hospital implemented continuous monitoring of their patients on parenteral opioids in the general care setting. To register:

61 Complimentary Resources Safety Innovations Series Alarms Management Patient Safety Seminars Seminar Recordings Webinar Slides Key Points Checklists Opioid Safety & Patient Monitoring Compendium AAMI Foundation Alarm Compendium
62 Thank You to Our Premier Industry Partners Without their financial support, we would not be able to undertake the various initiatives under the National Coalition to Promote Continuous Monitoring of Patients on Opioids. The AAMI Foundation and its co-convening organizations appreciate their generosity. The AAMI Foundation is managing all costs for the series. The seminar does not contain commercial content. Diamond Platinum Gold




63 Questions? Post a question on AAMI Foundation s LinkedIn Type your question in the Question box on your webinar dashboard Or you can your question to: mflack@aami.org.
64 Consider Making a Donation to the AAMI Foundation Today! Making Healthcare Technology Safer, Together Thank you for your support!
65 Thank you for attending! This presentation will be posted to this webpage within one week: emnumber=2933&navitemnumber=3086
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare. Friday October 14, 2016
 Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications
 Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
Vital Signs Monitoring Leads to Increased Patient Safety and Workflow Efficiency
 Safety Innovations Vital Signs Monitoring Leads to Increased Patient Safety and Workflow Efficiency Martha Vockley and Theresa Kloewer About the Authors Martha Vockley is principal of VockleyLang, LLC,
Safety Innovations Vital Signs Monitoring Leads to Increased Patient Safety and Workflow Efficiency Martha Vockley and Theresa Kloewer About the Authors Martha Vockley is principal of VockleyLang, LLC,
Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense.
 Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense January 12, 2018 Vision: Health technology enhances healthcare providers abilities
Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense January 12, 2018 Vision: Health technology enhances healthcare providers abilities
A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids
 A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids Phyllis J. Miller About the Author Phyllis J. Miller, MS, RN, FHCE, is an independent nursing consultant. At the time this article
A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids Phyllis J. Miller About the Author Phyllis J. Miller, MS, RN, FHCE, is an independent nursing consultant. At the time this article
Alarm Management: From Confusion, to Information, to Wisdom. August 3, 2015
 Alarm Management: From Confusion, to Information, to Wisdom August 3, 2015 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology Visit our website to learn more about our
Alarm Management: From Confusion, to Information, to Wisdom August 3, 2015 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology Visit our website to learn more about our
Smart Pump Interoperability: A Multi-System Safety Journey. February 23, 2018
 Smart Pump Interoperability: A Multi-System Safety Journey February 23, 2018 Jennifer Biltoft, PharmD, BCPS System Director, Clinical Pharmacy Services, SCL Health Deborah Bonnes, RN, MS Nursing Informatics
Smart Pump Interoperability: A Multi-System Safety Journey February 23, 2018 Jennifer Biltoft, PharmD, BCPS System Director, Clinical Pharmacy Services, SCL Health Deborah Bonnes, RN, MS Nursing Informatics
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Effects of Patient Load and Other Monitoring System Design Choices on Inpatient Monitoring Quality
 Effects of Patient Load and Other Monitoring System Design Choices on Inpatient Monitoring Quality August 10, 2015 8/10/2015 1 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology
Effects of Patient Load and Other Monitoring System Design Choices on Inpatient Monitoring Quality August 10, 2015 8/10/2015 1 AAMI Foundation Vision: To drive the safe adoption and use of healthcare technology
We See You When You're Sleeping
 We See You When You're Sleeping Addressing Patient Safety Risks Surrounding Opioid-Induced Sedation Jeanne J. Venella DNP, MS, CEN, CPEN November 30 th, 2016 1 Objectives Review the current state of opioids
We See You When You're Sleeping Addressing Patient Safety Risks Surrounding Opioid-Induced Sedation Jeanne J. Venella DNP, MS, CEN, CPEN November 30 th, 2016 1 Objectives Review the current state of opioids
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations,
 EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations, Houston Methodist Hospital Michael Rothman, PhD, Chief Science
EMR Surveillance Intervenes to Reduce Risk Adjusted Mortality March 2, 2016 Katherine Walsh, MS, DrPH, RN, NEA-BC Vice President of Operations, Houston Methodist Hospital Michael Rothman, PhD, Chief Science
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Surveillance Monitoring of General-Care Patients An Emerging Standard of Care
 Surveillance Monitoring of General-Care Patients An Emerging Standard of Care PART TWO NURSES, PHYSICIANS AND COST OF CARE Prepared by Sotera Wireless Benjamin Kanter, MD, FCCP Chief Medical Officer Rosemary
Surveillance Monitoring of General-Care Patients An Emerging Standard of Care PART TWO NURSES, PHYSICIANS AND COST OF CARE Prepared by Sotera Wireless Benjamin Kanter, MD, FCCP Chief Medical Officer Rosemary
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario A Postoperative Patient with Tachycardia
 Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Statement on Safe Use of Propofol (Approved by ASA House of Delegates on October 27, 2004);
;") CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
Case Study from Parallon
 Case Study from Parallon Improving Compliance with the Smart Pump drug library across a large hospital system Part 2 Monday, July 10, 2017 AAMI Foundation Vision: To drive the safe adoption and safe use
Case Study from Parallon Improving Compliance with the Smart Pump drug library across a large hospital system Part 2 Monday, July 10, 2017 AAMI Foundation Vision: To drive the safe adoption and safe use
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
STATEMENT ON GRANTING PRIVILEGES FOR ADMINISTRATION OF MODERATE SEDATION TO PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS
 NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
Rethinking Telemetry and Its Impact on Healthcare. Wireless technology that improves care and reduces costs
 Rethinking Telemetry and Its Impact on Healthcare Wireless technology that improves care and reduces costs Thinking differently about telemetry. You know it better than anyone the challenge of improving
Rethinking Telemetry and Its Impact on Healthcare Wireless technology that improves care and reduces costs Thinking differently about telemetry. You know it better than anyone the challenge of improving
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Running head: FAILURE TO RESCUE 1
 Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
Survey on ASA Standards and APSF Recommendations
 Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Predictive Analytics and the Impact on Nursing Care Delivery
 Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Protocol/Procedure XX. Title: Procedural Sedation/Moderate Sedation
 Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Mercy Virtual. Transforming Medicine and Value Through Virtual Care. Randall S Moore, MD, MBA. Orlando, FL. September, 2017
 Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Five Keys to Successful Monitoring of Patients Receiving Opioids
 Five Keys to Successful Monitoring of ients Receiving Opioids An Interview with Oglesby RRT, Manager, The Center for Pulmonary Health, Candler Hospital, St. Joseph s/candler Health System (SJ/C) Hi. This
Five Keys to Successful Monitoring of ients Receiving Opioids An Interview with Oglesby RRT, Manager, The Center for Pulmonary Health, Candler Hospital, St. Joseph s/candler Health System (SJ/C) Hi. This
EarlySense InSight. Integrating Acute and Community Care
 EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
Acute Care Workflow Solutions
 Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Bridging the Care Continuum. BSM-3500 Series bedside monitors
 Bridging the Care Continuum BSM-3500 Series bedside monitors The Right Monitoring Today s healthcare environment necessitates that patients receive the right care, at the right cost, and at the right time.
Bridging the Care Continuum BSM-3500 Series bedside monitors The Right Monitoring Today s healthcare environment necessitates that patients receive the right care, at the right cost, and at the right time.
GE Healthcare. B40 Patient Monitor Connecting intelligence and care
 GE Healthcare B40 Patient Monitor Connecting intelligence and care Simple. The B40 Monitor provides versatile clinical capabilities to help you monitor a wide range of patients. From ambulatory surgery
GE Healthcare B40 Patient Monitor Connecting intelligence and care Simple. The B40 Monitor provides versatile clinical capabilities to help you monitor a wide range of patients. From ambulatory surgery
TASCS 2017 Annual Conference 3/2/2017
 Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018
 FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018 Today s Agenda Welcome and Overview for today s HIIN Lead Virtual Meeting HIINgagment and HIINaction Florida s Success, Opportunities and Line
FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018 Today s Agenda Welcome and Overview for today s HIIN Lead Virtual Meeting HIINgagment and HIINaction Florida s Success, Opportunities and Line
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services
 Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring
 Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring Marylynn Hippe, MSN, RN, ACNS-BC, CMSRN St. Luke s Health System Boise, Idaho Objectives Learners will understand the appropriate
Achieving the Triple Aim: Decreasing Use of Inappropriate Telemetry Monitoring Marylynn Hippe, MSN, RN, ACNS-BC, CMSRN St. Luke s Health System Boise, Idaho Objectives Learners will understand the appropriate
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility
 Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Anesthesia
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
Real Time Pressure Ulcer Data Drives Quality
 Real Time Pressure Ulcer Data Drives Quality Lisa Q. Corbett APRN ACNS-BC CWOCN Carol Strycharz RN BSN MPH Jamie A Curley RN BSN Nancy Ough LPN Rebecca Morton RN BSN CWCN Catherine Yavinsky RN MS NEA-BC
Real Time Pressure Ulcer Data Drives Quality Lisa Q. Corbett APRN ACNS-BC CWOCN Carol Strycharz RN BSN MPH Jamie A Curley RN BSN Nancy Ough LPN Rebecca Morton RN BSN CWCN Catherine Yavinsky RN MS NEA-BC
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR.
 Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay
 Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE
 ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Number of sepsis admissions to critical care and associated mortality, 1 April March 2013
 Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Arrest Rates Decline Post-Implementation of Nurse Led Teams. Nicole Lincoln MS, RN, APRN-BC, CCRN Date June 16, 2016 Time: 2:45 pm- 3:15 pm
 Arrest Rates Decline Post-Implementation of Nurse Led Teams Nicole Lincoln MS, RN, APRN-BC, CCRN Date June 16, 2016 Time: 2:45 pm- 3:15 pm 2 BOSTON MEDICAL CENTER (BMC) 3 QUALITY CARE AND ENGAGEMENT 4
Arrest Rates Decline Post-Implementation of Nurse Led Teams Nicole Lincoln MS, RN, APRN-BC, CCRN Date June 16, 2016 Time: 2:45 pm- 3:15 pm 2 BOSTON MEDICAL CENTER (BMC) 3 QUALITY CARE AND ENGAGEMENT 4
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Health Technology for Tomorrow
 Diagnostic Evidence Co-operative Oxford Health Technology for Tomorrow Seminar 1: The potential for wearable technology in ambulatory care: Isansys Patient Status Engine 25 November 2016 Somerville College,
Diagnostic Evidence Co-operative Oxford Health Technology for Tomorrow Seminar 1: The potential for wearable technology in ambulatory care: Isansys Patient Status Engine 25 November 2016 Somerville College,
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Lisa M. Soltis, MSN, RN-BC, APRN, PCCN, CCRN-CSC-CMC, CCNS, FCCM
 2739 Laurelcherry Street, Raleigh, NC 27612 (919) 621-3921 Cell Lisa.Soltis@unchealth.unc.edu FUNCTIONAL SUMMARY Clinical Expert in Cardiovascular surgical procedures, processes and policies. Active advocate
2739 Laurelcherry Street, Raleigh, NC 27612 (919) 621-3921 Cell Lisa.Soltis@unchealth.unc.edu FUNCTIONAL SUMMARY Clinical Expert in Cardiovascular surgical procedures, processes and policies. Active advocate
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
To outline the criteria and management for the patient receiving moderate sedation (conscious
 Section: HRMC Division of Nursing Index: 8620.157b Page: 1 of 6 Issue Date: July 1, 1996 Revised Date: January, 2011 PROTOCOL TITLE: MODERATE SEDATION PURPOSE: sedation) To outline the criteria and management
Section: HRMC Division of Nursing Index: 8620.157b Page: 1 of 6 Issue Date: July 1, 1996 Revised Date: January, 2011 PROTOCOL TITLE: MODERATE SEDATION PURPOSE: sedation) To outline the criteria and management
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Patient Care Protocol
 Patient Care Protocol Document: prtcl_dcd.doc Donation after Circulatory Determination of Death [Pre-Mortem] Site Setting/Population Clinician BCH Only ICU/OR/All Patients with Circulatory Determination
Patient Care Protocol Document: prtcl_dcd.doc Donation after Circulatory Determination of Death [Pre-Mortem] Site Setting/Population Clinician BCH Only ICU/OR/All Patients with Circulatory Determination
Patient Controlled Analgesia Guidelines
 Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
D Bringing you closer to your patients PATIENT MONITORING AND IT SOLUTIONS
 D-41011-2012 Bringing you closer to your patients PATIENT MONITORING AND IT SOLUTIONS 02 How can I D-41498-2012 spend more time with my patients? 03 D-40970-2012 D-40373-2012 D-41225-2012 Patient monitoring
D-41011-2012 Bringing you closer to your patients PATIENT MONITORING AND IT SOLUTIONS 02 How can I D-41498-2012 spend more time with my patients? 03 D-40970-2012 D-40373-2012 D-41225-2012 Patient monitoring
The ASA defines anesthesiology as the practice of medicine dealing with but not limited to:
 1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Alaris Products. Protecting patients at the point of care
 Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
One Standard Across the Care Continuum. BSM-6000 series bedside monitors
 One Standard Across the Care Continuum BSM-6000 series bedside monitors Breaking Down Barriers to Care The Institute of Healthcare Improvement s triple aim designed to push quality initiatives while simultaneously
One Standard Across the Care Continuum BSM-6000 series bedside monitors Breaking Down Barriers to Care The Institute of Healthcare Improvement s triple aim designed to push quality initiatives while simultaneously
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient