Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017
|
|
|
- Bruno Dominic Farmer
- 5 years ago
- Views:
Transcription

1 Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell, PhD, MBA, MS VP Mercy Medical Group Mercy Regional Medical Center, Centura Health 1


2 Speaker Introduction Tamra Lavengood, RN, BSN, MSN, CPNP, CNS Clinical Performance Coordinator Centura Health Physician Group; Colorado Coordinator for Comprehensive Primary Care Initiative Mercy Family Medicine; Durango, Colorado Will McConnell, PhD, MBA, MS VP Mercy Medical Group Mercy Regional Medical Center Centura Health Physician Group Durango, Colorado 2
3 Conflict of Interest Tamra Lavengood, RN, BSN, MSN Will McConnell, PhD, MBA, MS Have no real or apparent conflicts of interest to report 3
4 Agenda The Beginning What was the Comprehensive Primary Care (CPC) Initiative? Why did Mercy Family Medicine choose to participate? The CPC movement grows to CPC+, largest initiative ever in history of CMS Key elements learned from CPC Empanelment Risk stratification Care Management Behavioral Healthcare Management Care Coordination Emergency Department and Hospital Follow-up Health Information Technology: Crucial Builds Needed for Success Outcomes and Lessons Learned 4
5 Learning Objectives Assess organizational dynamics to successfully transfer to an alternative payment model Leverage EHR clinical data and behavioral health data to successfully empanel and risk adjust patients Develop standardized care mechanisms for meeting performance thresholds for chronic disease patients 5
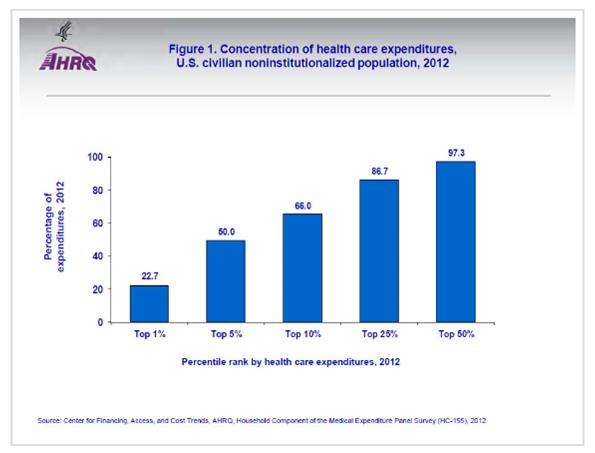
6 An Introduction of How Benefits Were Realized for the Value of Health IT Satisfaction: Provide comprehensive primary care: improves outcomes; better for the patient; better for the clinical staff Treatment/Clinical: Target comprehensive care on the sickest patients, focus on the top 20% for the best return on investment Electronic Secure Data: Attach all patients to a primary care provider; risk stratify; use data to drive improvement for clinical quality measures Savings: Decrease emergency visits and hospital visits (utilization) and realize cost avoidance 6
7 What Was the Comprehensive Primary Care Initiative? Four-year multi-payer initiative designed to strengthen primary care (October 2012 through December 2016) Population-based care management fees and shared savings opportunities to support the provision of a core set of five Comprehensive primary care functions Risk Stratified Care Management Access and Continuity Planned Care for Chronic Conditions and Preventive Care Patient and Caregiver Engagement Coordination of Care Across the Medical Neighborhood 7

8 Comprehensive Primary Care Pilot Demographics: practice sites» 2,200 practitioners» 2.7 million active patients» 38 public and private payers» 335,000 Medicare beneficiaries Purpose: - Improve care» Better health for populations» Lower costs» Inform future Medicare and Medicaid policy 8
9 Comprehensive Primary Care Pilot Payment Model Participating primary care practices receive two forms of financial support on behalf of their fee-for-service (FFS) Medicare beneficiaries: A monthly non-visit based care management fee per member The opportunity to share in any net savings CPC was a pilot to prove if building the infrastructure within Primary Care via additional revenue, would it make a difference: better health, better outcomes, lower costs. It made a difference and CMS is on board with Primary Care Reform. 9
10 Why Did Mercy Family Medicine Choose to Participate? Value-based purchasing was getting a lot of attention We needed to identify viable payment models and prepare for the future Alignment with PCMH requirements Huge potential within CPC, for additional revenue to build infrastructure within clinic Great group of clinicians and staff Timing was right 10
11 Barriers to Get the Comprehensive Primary Care Initiative Started One more thing to do Do we have the bandwidth? Moving into uncertain territory with CPC A lot of additional reporting and process work would be needed No real quantifiable risk stratification tools in the beginning Practice was recently acquired 11
12 Comprehensive Primary Care Initiative: Our Journey Clinics were given 9 milestones to complete CMS selected key elements that aligned with Patient Centered Medical Home elements Milestone 2: Empanelment Risk Stratification Care Management Behavioral Health Integration 12
13 Empanelment Empanelment End of 2012 = 79% End of 2016 = 99.9% Four Cut Method (1) Provider Panels (1) Panel Size: How Many Patients Can One doctor Have?, Mark Murray, MD,MPA, Mike Davies, MD, Barbara Boushon, RN,Fam Pract Manag Apr; 14(4):
14 Risk Stratification Risk Stratification All 500 clinics asked to develop their own risk stratification methodology Mercy Family Medicine reviewed tools from: California Quality Collaborative AAFP Risk Stratification Tool Telluride Medical Center in Colorado (another CPC practice) 14
15 Identifying and Managing High Risk Populations at Centura Health Developed our own Mercy Adult Risk Stratification Tool (MARST) and the Mercy Pediatric Risk Stratification Tool (MPRST) Critical to have not only Objective elements but Subjective elements as well 15


16 HIT Needed for Risk Stratification Using the system we had our risk stratification elements flow exactly like our EHR 16

17 Please use blank slide if more space is required for charts, graphs, etc. To remove background graphics, right click on selected slide, choose Format Background and check Hide background graphics. Remember to delete this slide, if not needed.

18 Please use blank slide if more space is required for charts, graphs, etc. To remove background graphics, right click on selected slide, choose Format Background and check Hide background graphics. Remember to delete this slide, if not needed.
19 Risk Stratification in CPC Practices Comprehensive Primary Care practices risk stratify their patients by: Clinical intuition: 71% Practice developed clinical algorithm: 61% Published clinical algorithm: 40% Claims: 24% EHR methodology: 19% Practices were able to select more than one method 19
20 ***Attention EHR Venders*** Create a methodology to risk stratify patients using objective data elements, BUT then have an end user capability for subjective, intuitive judgement 20

21 Please use blank slide if more space is required for charts, graphs, etc. To remove background graphics, right click on selected slide, choose Format Background and check Hide background graphics. Remember to delete this slide, if not needed.
22 Mercy Adult Risk Stratification Tool Have risk stratified over 15,000 patients 1.1% Highest risk Level % High risk Level 5 (6.5%) and Level 4 (13.9%) 25.3% Medium risk Level % Low risk Level % Low risk Level 1 22

23 23 23
24 24
25 Care Management for High Risk Patients (Person Focused) Care Management (person/disease centered) of patients in the highest risk quartile: For the Mercy Risk Tool Level 6 (1.1% with Mercy Risk Tool) Care Management (person/disease centered) of patients with rapidly rising risk and likely to benefit from active, ongoing, intensive care management For the Mercy Risk Tool Level 5 s and Level 4 s (20.4% with Mercy Risk Tool) Integration of behavioral health care management strategies for patients in higher risk cohorts 25

26 Risk Stratified Care Management 26
27 Get Ready for the Change Do We Have All of the Required Elements? Begins with Comprehensive Primary Care Delivery Qualified, competent Primary Care Providers Empaneled patients with care teams Risk Stratification of patients in real time using subjective as well as objective elements Integration of Behavioral Health Care Management 27
28 Behavioral Health Integration Behavioral Health care is needed for the majority of level 6 patients In house Licensed Clinical Social Worker Warm handoffs Scheduled patients Evaluation tools: PHQ9 Tracking depression screening 28
29 Care Coordination (System focused) Care Coordination across the Medical Neighborhood Emergency Department discharges Hospital discharges 29
30 30

31 Mercy Family Medicine s Care Model 31
32 HIT Critical Builds with Ability to Track Empanel all patients to a primary care provider Risk Stratify all patients with objective and subjective information Longitudinal Care Plans Episodic Care Plans ED and Hospital interoperability with clinics Clinical Quality Measures; codes built for tracking Vender collaboration with clinics!! 32
33 Medicare Expenses Per Patient Per Month All Attributed Patients 33

34 Hospital admissions, ED Visits, 30 day Re- Admissions for all attributed Medicare Patients 34
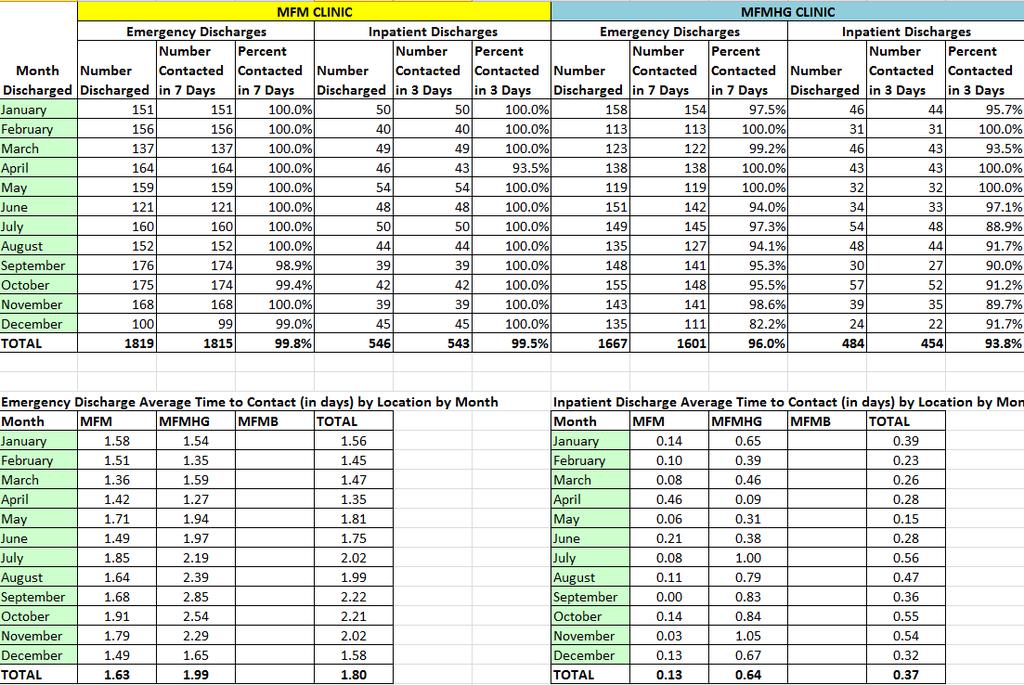
35 CPC Great Idea! Successes: Care Management for high-risk patients identified through risk stratification in real time using objective and subjective-intuitive elements, able to isolate the top 1% of our patient population Care Management and Behavioral Health Care Management for high-risk patients led to reduced ED visits; Hospitalizations for any cause; and for Hospitalizations due to Ambulatory Care Sensitive Conditions (ACSC) Care Coordination in the clinic setting providing communication between the inpatient and outpatient settings for ED and hospital discharges enabling follow up at 97.5% within 1.8 day for ED visits and 96.7% within 8hrs for hospital discharges 35
36 Successes Continued (Q15) Data is not risk adjusted so the comparison is with clinics that have a similar risk profile Decreased Per Member Per Month (PMPM) expenses for Medicare population of $617; 7 th lowest in Colorado region of 75 practices of which $716 is the median and high $1,284. Mercy Family Medicine (MFM) has over 3000 attributed Medicare patients. MFM had a cost avoidance of Medicare expenditures by $297,000 per month compared to the Colorado region average. That equals $3,564,000 of cost avoidance for our 3000 Medicare patients annually. Decreased ED utilization from 656 to 634 (not risk adjusted) per 1000 Medicare patients. Average in Colorado region is 706 for clinics with a similar risk profile. MFM reduced Medicare expenditures by $140,400 compared to the Colorado region average.* *based on Mercy Regional Medical Center average of $650/ED visit) 36
37 Successes Continued (Q15) Information is not risk adjusted so comparisons are with clinics with a similar risk profile to Mercy Decreased hospital admissions for any cause from 196 (Q1) to 180 (Q15) patients per 1000 Medicare patients, an 8% decrease. Average for Colorado region is 260 patients and had a 7% decrease throughout the initiative. Mercy Family Medicine reduced Medicare expenditures by $6,240,000 annually compared to the Colorado region average.* Decreased hospital admissions for Ambulatory Care Sensitive Conditions (ACSC) from 33 (Q1) to 26 (Q15) per 1000 Medicare patients, a 21% decrease. Average for Colorado region is 54 and had a 9% decrease throughout the initiative. Mercy Family Medicine reduced Medicare expenditures by $2,184,000 annually compared to the Colorado region average.* Decreased 30 day re-admit from 101(Q1) to 69 (Q15) per 1000 Medicare patients, a 31% decrease. Average for state of Colorado is 123 re-admits per 1000, and had a 3% decrease throughout the initiative. Mercy Family Medicine reduced Medicare expenditures by $4,212,000 annually compared to the Colorado region average.* *based on Mercy Regional Medical Center average of $26,000/hospital visit) 37
38 Variables This is a picture looking at where MFM was in Q1 and where MFM is in Q15 (3.5 years). There were some quarters that we were lower and some quarters that we were higher. This reflects the beginning of MFMs CPC journey, October 2012, though June MFM also grew from 1117 Medicare patients to 3171, an 184% increase. The Colorado region clinic s average grew from 446 to 657 Medicare patients, a 47% increase. There are differences in demographics across the 75 Colorado Primary Care clinics: age; race/ethnicity (MFM has more Native American, less African American); HCC scores (MFM has more high risk patients); dual eligible (MFM has more patients also on Medicaid). 38
39 What s Next?? CPC+ Largest initiative in the history of CMS. CPC+ is an advanced primary care medical home model. Building on lessons learned from the Comprehensive Primary Care (CPC) initiative Care Management of high risk patients Behavioral Health Care Management of high risk patients Care Coordination with transitions of care from the ED and Hospital Data driving improvement: Clinical Quality Measures; Cost; and Utilization Offering alternative payment models which pay clinics up-front to build the infrastructure for comprehensive primary care with multi-payer involvement 5 Year Model: Round 1 beginning January 1, 2017; Round 2 beginning January 1, 2018 for 10 new regions 39
40 14 CPC+ Regions Selected Arkansas: Statewide Colorado: Statewide Hawaii: Statewide Kansas and Missouri: Greater Kansas City Region Michigan: Statewide Montana: Statewide New Jersey: Statewide New York: North Hudson-Capital Region Ohio: Statewide and Northern Kentucky Region Oklahoma: Statewide Oregon: Statewide Pennsylvania: Greater Philadelphia Region Rhode Island: Statewide Tennessee: Statewide 40

41 A Summary of How Benefits Were Realized for the Value of Health IT Satisfaction: Reduced hospitalizations, ED visits, re-admissions rewarding for patients and clinical staff Treatment/Clinical: Identified high risk population to target resources, top 20% Electronic Secure Data: Empanelment 99%; risk stratification >85%; data driving improvement for 9 Clinical Quality Measures Savings: Decreased overall per-member-permonth expenditures and millions in cost avoidance for MFM s Medicare patients 41
42 Leave You With a Story: How Care Management and Care Coordination saved a life 42
43 Questions Please reach out to us: Tamra Lavengood RN, BSN, MSN Will McConnell PhD, MBA, MS Clinical Performance Coordinator VP Mercy Medical Group CPCI Coordinator Mercy Regional Medical Center Centura Health Physician Group Centura Health Physician Group Mercy Family Medicine (direct) (direct) (cell) 1 Mercado Street Suite295 Durango CO
Comprehensive Primary Care: Our Success Story
 Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
Comprehensive Primary Care Plus. Plus (CPC+) Update for Payers
 Update for Payers") Comprehensive Primary Care Plus (CPC+) Update for Payers December 19, 2016 Rayva Virginkar, Gabrielle Schechter, and Leah Hendrick Tips for a Successful Webinar 2 Webinar Overview During this webinar,
Comprehensive Primary Care Plus (CPC+) Update for Payers December 19, 2016 Rayva Virginkar, Gabrielle Schechter, and Leah Hendrick Tips for a Successful Webinar 2 Webinar Overview During this webinar,
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Elizabeth Mitchell December 1, Transforming Healthcare in an Uncertain Environment
 Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Transforming Healthcare in an Uncertain Environment Elizabeth Mitchell, President & CEO Network for Regional Healthcare Improvement 2017 We have a problem Health Spending as a Share of GDP United States,
Nicholas E. Davies Enterprise Award of Excellence Population Management Case Study
 Applicant Organization: Centura Health Organization s Address: 188 Inverness Dr. W #500, Englewood, CO 80112 Submitter: Amy Feaster, Vice President of Information Technology Email: amyfeaster@centura.org
Applicant Organization: Centura Health Organization s Address: 188 Inverness Dr. W #500, Englewood, CO 80112 Submitter: Amy Feaster, Vice President of Information Technology Email: amyfeaster@centura.org
CPC+ Oregon Practice Application Webinar. David Dorr, MD, MS Ron Stock, MD, MA
 CPC+ Oregon Practice Application Webinar David Dorr, MD, MS Ron Stock, MD, MA We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Presenters David A. Dorr,
CPC+ Oregon Practice Application Webinar David Dorr, MD, MS Ron Stock, MD, MA We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Presenters David A. Dorr,
Comprehensive Primary Care Plus (CPC+): What You Need to Know Before Applying
: What You Need to Know Before Applying") Medical Group Strategy Council Physician Practice Roundtable Comprehensive Primary Care Plus (CPC+): What You Need to Know Before Applying August 8, 2016 2 Today s Presenters Ingrid Lund, PhD Practice
Medical Group Strategy Council Physician Practice Roundtable Comprehensive Primary Care Plus (CPC+): What You Need to Know Before Applying August 8, 2016 2 Today s Presenters Ingrid Lund, PhD Practice
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
2015 State Hospice Report 2013 Medicare Information 1/1/15
 2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
The Comprehensive Primary Care Initiative: New Payment Models Will Rely on Use of Health IT
 The Comprehensive Primary Care Initiative: New Payment Models Will Rely on Use of Health IT Richard J. Baron, MD, MACP Group Director, Seamless Care Models Innovation Center, CMS Advancing Primary Care
The Comprehensive Primary Care Initiative: New Payment Models Will Rely on Use of Health IT Richard J. Baron, MD, MACP Group Director, Seamless Care Models Innovation Center, CMS Advancing Primary Care
MEDICAL HOMES Arkansas Hospital Association
 MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013
 State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
Current Medicare Advantage Enrollment Penetration: State and County-Level Tabulations
 Current Advantage Enrollment : State and County-Level Tabulations 5 Slide Series, Volume 40 September 2016 Summary of Tabulations and Findings As of September 2016, 17.9 million of the nation s 56.1 million
Current Advantage Enrollment : State and County-Level Tabulations 5 Slide Series, Volume 40 September 2016 Summary of Tabulations and Findings As of September 2016, 17.9 million of the nation s 56.1 million
Improving Care for Dual Eligibles through Health IT
 Los Angeles, October 31, 2012 Presentation Improving Care for Dual Eligibles through Health IT The National Dual Eligibles Summit Duals Market is sizable Medicare and Medicaid Populations Medicaid Total
Los Angeles, October 31, 2012 Presentation Improving Care for Dual Eligibles through Health IT The National Dual Eligibles Summit Duals Market is sizable Medicare and Medicaid Populations Medicaid Total
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Comprehensive Primary Care Plus (CPC+) toolkit: Supporting new advanced alternative payment models
 toolkit: Supporting new advanced alternative payment models") IBM Watson Health Toolkit Comprehensive Primary Care Plus (CPC+) toolkit: Supporting new advanced alternative payment models Explore how IBM Watson Health can partner with you in CPC+ Contents Here s your
IBM Watson Health Toolkit Comprehensive Primary Care Plus (CPC+) toolkit: Supporting new advanced alternative payment models Explore how IBM Watson Health can partner with you in CPC+ Contents Here s your
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
 3+ 3+ N = 155, 442 3+ R 2 =.32 < < < 3+ N = 149, 685 3+ R 2 =.27 < < < 3+ N = 99, 752 3+ R 2 =.4 < < < 3+ N = 98, 887 3+ R 2 =.6 < < < 3+ N = 52, 624 3+ R 2 =.28 < < < 3+ N = 36, 281 3+ R 2 =.5 < < < 7+
3+ 3+ N = 155, 442 3+ R 2 =.32 < < < 3+ N = 149, 685 3+ R 2 =.27 < < < 3+ N = 99, 752 3+ R 2 =.4 < < < 3+ N = 98, 887 3+ R 2 =.6 < < < 3+ N = 52, 624 3+ R 2 =.28 < < < 3+ N = 36, 281 3+ R 2 =.5 < < < 7+
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Two-Year Effects of the Comprehensive Primary Care Initiative on Practice Transformation and Medicare Fee-for-Service Beneficiaries Outcomes
 Two-Year Effects of the Comprehensive Primary Care Initiative on Practice Transformation and Medicare Fee-for-Service Beneficiaries Outcomes Deborah Peikes, Stacy Dale, Erin Taylor, Arkadipta Ghosh, Ann
Two-Year Effects of the Comprehensive Primary Care Initiative on Practice Transformation and Medicare Fee-for-Service Beneficiaries Outcomes Deborah Peikes, Stacy Dale, Erin Taylor, Arkadipta Ghosh, Ann
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
of Program Success and
 PCMH Evaluations: Key Drivers of Program Success and Measurement Development Robert Phillips, MD, MSPH, American Board of Family Medicine Deborah Peikes, PhD, MPA, Mathematica Michael Bailit, MBA, Bailit
PCMH Evaluations: Key Drivers of Program Success and Measurement Development Robert Phillips, MD, MSPH, American Board of Family Medicine Deborah Peikes, PhD, MPA, Mathematica Michael Bailit, MBA, Bailit
FY 2014 Per Capita Federal Spending on Major Grant Programs Curtis Smith, Nick Jacobs, and Trinity Tomsic
 Special Analysis 15-03, June 18, 2015 FY 2014 Per Capita Federal Spending on Major Grant Programs Curtis Smith, Nick Jacobs, and Trinity Tomsic 202-624-8577 ttomsic@ffis.org Summary Per capita federal
Special Analysis 15-03, June 18, 2015 FY 2014 Per Capita Federal Spending on Major Grant Programs Curtis Smith, Nick Jacobs, and Trinity Tomsic 202-624-8577 ttomsic@ffis.org Summary Per capita federal
Use of Medicaid MCO Capitation by State Projections for 2016
 Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Percentage of Enrolled Students by Program Type, 2016
 Percentage of Enrolled Students by Program Type, 2016 Doctorate 4% PN/VN 3% MSN 15% ADN 28% BSRN 22% Diploma 2% BSN 26% n = 279,770 Percentage of Graduations by Program Type, 2016 MSN 12% Doctorate 1%
Percentage of Enrolled Students by Program Type, 2016 Doctorate 4% PN/VN 3% MSN 15% ADN 28% BSRN 22% Diploma 2% BSN 26% n = 279,770 Percentage of Graduations by Program Type, 2016 MSN 12% Doctorate 1%
Primary Care Transformation in the Era of Value
 Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
Primary Care Transformation in the Era of Value CMS Innovation Center & Primary Care Bruce Finke, MD Janel Jin, MSPH Gabrielle Schechter, MPH Center for Medicare & Medicaid Innovation Centers for Medicare
MAP 1: Seriously Delinquent Rate by State for Q3, 2008
 MAP 1: Seriously Delinquent Rate by State for Q3, 2008 Seriously Delinquent Rate Greater than 6.93% 5.18% 6.93% 0 5.17% Source: MBA s National Deliquency Survey MAP 2: Foreclosure Inventory Rate by State
MAP 1: Seriously Delinquent Rate by State for Q3, 2008 Seriously Delinquent Rate Greater than 6.93% 5.18% 6.93% 0 5.17% Source: MBA s National Deliquency Survey MAP 2: Foreclosure Inventory Rate by State
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Fiscal Research Center
 January 2017 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
January 2017 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
Benefits by Service: Outpatient Hospital Services (October 2006)
") Page 1 of 8 Benefits by Service: Outpatient Hospital Services (October 2006) Definition/Notes Note: Totals include 50 states and D.C. "Benefits Covered" Totals "Benefits Not Covered" Totals Is the benefit
Page 1 of 8 Benefits by Service: Outpatient Hospital Services (October 2006) Definition/Notes Note: Totals include 50 states and D.C. "Benefits Covered" Totals "Benefits Not Covered" Totals Is the benefit
Salary and Demographic Survey Results
 Salary and Demographic Survey Results Executive Summary In July of 2010, Grant Professionals Association (GPA formerly AAGP) conducted a salary and demographic survey of grant professionals. The survey
Salary and Demographic Survey Results Executive Summary In July of 2010, Grant Professionals Association (GPA formerly AAGP) conducted a salary and demographic survey of grant professionals. The survey
Index of religiosity, by state
 Index of religiosity, by state Low Medium High Total United States 19 26 55=100 Alabama 7 16 77 Alaska 28 27 45 Arizona 21 26 53 Arkansas 12 19 70 California 24 27 49 Colorado 24 29 47 Connecticut 25 32
Index of religiosity, by state Low Medium High Total United States 19 26 55=100 Alabama 7 16 77 Alaska 28 27 45 Arizona 21 26 53 Arkansas 12 19 70 California 24 27 49 Colorado 24 29 47 Connecticut 25 32
Alternative Payment Models and Health IT
 Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Fiscal Research Center
 January 2018 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
January 2018 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Applications due: (December 1, 2014) at 11:59 pm ET
 Health Department Request for Technical Assistance (RTA): Applications due: (December 1, 2014) at 11:59 pm ET") State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Million Hearts Stakeholders Workshop Applications due: (December 1, 2014) at 11:59 pm ET I. Purpose: The purpose
State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Million Hearts Stakeholders Workshop Applications due: (December 1, 2014) at 11:59 pm ET I. Purpose: The purpose
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
TABLE 3c: Congressional Districts with Number and Percent of Hispanics* Living in Hard-to-Count (HTC) Census Tracts**
 Census Tracts**") living Alaska 00 47,808 21,213 44.4 Alabama 01 20,661 3,288 15.9 Alabama 02 23,949 6,614 27.6 Alabama 03 20,225 3,247 16.1 Alabama 04 41,412 7,933 19.2 Alabama 05 34,388 11,863 34.5 Alabama 06 34,849 4,074
living Alaska 00 47,808 21,213 44.4 Alabama 01 20,661 3,288 15.9 Alabama 02 23,949 6,614 27.6 Alabama 03 20,225 3,247 16.1 Alabama 04 41,412 7,933 19.2 Alabama 05 34,388 11,863 34.5 Alabama 06 34,849 4,074
Total Cost of Care in Action
 Total Cost of Care in Action Meredith Roberts Tomasi, Sr. Program Director, Q Corp Doug Rupp, Sr. Health Analyst, Q Corp The information in this presentation may be subject to copyright and may not be
Total Cost of Care in Action Meredith Roberts Tomasi, Sr. Program Director, Q Corp Doug Rupp, Sr. Health Analyst, Q Corp The information in this presentation may be subject to copyright and may not be
Holding the Line: How Massachusetts Physicians Are Containing Costs
 Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
TABLE 3b: Congressional Districts Ranked by Percent of Hispanics* Living in Hard-to- Count (HTC) Census Tracts**
 Census Tracts**") Rank State District Count (HTC) 1 New York 05 150,499 141,567 94.1 2 New York 08 133,453 109,629 82.1 3 Massachusetts 07 158,518 120,827 76.2 4 Michigan 13 47,921 36,145 75.4 5 Illinois 04 508,677 379,527
Rank State District Count (HTC) 1 New York 05 150,499 141,567 94.1 2 New York 08 133,453 109,629 82.1 3 Massachusetts 07 158,518 120,827 76.2 4 Michigan 13 47,921 36,145 75.4 5 Illinois 04 508,677 379,527
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
PRESS RELEASE Media Contact: Joseph Stefko, Director of Public Finance, ;
 PRESS RELEASE Media Contact: Joseph Stefko, Director of Public Finance, 585.327.7075; jstefko@cgr.org Highest Paid State Workers in New Jersey & New York in 2010; Lowest Paid in Dakotas and West Virginia
PRESS RELEASE Media Contact: Joseph Stefko, Director of Public Finance, 585.327.7075; jstefko@cgr.org Highest Paid State Workers in New Jersey & New York in 2010; Lowest Paid in Dakotas and West Virginia
HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016
 BACKGROUND HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016 Federal legislation (42 CFR 484.36) requires that Medicare-certified home health agencies employ home health aides who are trained and evaluated
BACKGROUND HOME HEALTH AIDE TRAINING REQUIREMENTS, DECEMBER 2016 Federal legislation (42 CFR 484.36) requires that Medicare-certified home health agencies employ home health aides who are trained and evaluated
How North Carolina Compares
 How North Carolina Compares A Compendium of State Statistics March 2017 Prepared by the N.C. General Assembly Program Evaluation Division Preface The Program Evaluation Division of the North Carolina General
How North Carolina Compares A Compendium of State Statistics March 2017 Prepared by the N.C. General Assembly Program Evaluation Division Preface The Program Evaluation Division of the North Carolina General
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
 Page 1 of 5 Health Reform Medicaid/CHIP Medicare Costs/Insurance Uninsured/Coverage State Policy Prescription Drugs HIV/AIDS Medicaid Benefits Services Covered, Limits, Copayments and Reimbursement Methodologies
Page 1 of 5 Health Reform Medicaid/CHIP Medicare Costs/Insurance Uninsured/Coverage State Policy Prescription Drugs HIV/AIDS Medicaid Benefits Services Covered, Limits, Copayments and Reimbursement Methodologies
The American Legion NATIONAL MEMBERSHIP RECORD
 The American Legion NATIONAL MEMBERSHIP RECORD www.legion.org 2016 The American Legion NATIONAL MEMBERSHIP RECORD 1920-1929 Department 1920 1921 1922 1923 1924 1925 1926 1927 1928 1929 Alabama 4,474 3,246
The American Legion NATIONAL MEMBERSHIP RECORD www.legion.org 2016 The American Legion NATIONAL MEMBERSHIP RECORD 1920-1929 Department 1920 1921 1922 1923 1924 1925 1926 1927 1928 1929 Alabama 4,474 3,246
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Fiscal Research Center
 January 2016 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
January 2016 Georgia s Rankings Among the States: Budget, Taxes and Other Indicators ABOUT THE FISCAL RESEARCH CENTER Established in 1995, the (FRC) provides nonpartisan research, technical assistance
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts
 PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
THE STATE OF GRANTSEEKING FACT SHEET
 1 THE STATE OF GRANTSEEKING FACT SHEET ORG ANIZATIONAL COMPARISO N BY C ENSUS DIV ISION S PRING 2013 The State of Grantseeking Spring 2013 is the sixth semi-annual informal survey of nonprofits conducted
1 THE STATE OF GRANTSEEKING FACT SHEET ORG ANIZATIONAL COMPARISO N BY C ENSUS DIV ISION S PRING 2013 The State of Grantseeking Spring 2013 is the sixth semi-annual informal survey of nonprofits conducted
 Page 1 of 7 Medicaid Benefits Services Covered, Limits, Copayments and Reimbursement Methodologies For 50 States, District of Columbia and the Territories (as of January 2003) CHOOSE SERVICE Go CHOOSE
Page 1 of 7 Medicaid Benefits Services Covered, Limits, Copayments and Reimbursement Methodologies For 50 States, District of Columbia and the Territories (as of January 2003) CHOOSE SERVICE Go CHOOSE
Use of Medicaid to Support Early Intervention Services
 Use of Medicaid to Support Early Intervention Services 2010 The ITCA has conducted a national survey of Part C Coordinators for over 5 years. The goal of the survey is to gather relevant information and
Use of Medicaid to Support Early Intervention Services 2010 The ITCA has conducted a national survey of Part C Coordinators for over 5 years. The goal of the survey is to gather relevant information and
Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future
 Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Developing a Game-Changing TeleHealth Strategy for Success
 Developing a Game-Changing TeleHealth Strategy for Success April 14, 2015 Jay Backstrom & Jeff Jones DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not
Developing a Game-Changing TeleHealth Strategy for Success April 14, 2015 Jay Backstrom & Jeff Jones DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Nov. 17, Dear Mr. Slavitt:
 Nov. 17, 2015 Mr. Andrew Slavitt Acting Administrator Centers for Medicare and Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, S.W. Washington, DC 20201 Re: NAMD
Nov. 17, 2015 Mr. Andrew Slavitt Acting Administrator Centers for Medicare and Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, S.W. Washington, DC 20201 Re: NAMD
Rutgers Revenue Sources
 Rutgers Revenue Sources 31.2% Tuition and Fees 27.3% State Appropriations with Fringes 1.0% Endowment and Investments.5% Federal Appropriations 17.8% Federal, State, and Municipal Grants and Contracts
Rutgers Revenue Sources 31.2% Tuition and Fees 27.3% State Appropriations with Fringes 1.0% Endowment and Investments.5% Federal Appropriations 17.8% Federal, State, and Municipal Grants and Contracts
Innovative Coordinated Care Delivery
 Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Critical Access Hospitals and HCAHPS
 Critical Access Hospitals and HCAHPS Michelle Casey, MS Senior Research Fellow and Deputy Director University of Minnesota Rural Health Research Center June 12, 2012 Overview of Presentation Why is HCAHPS
Critical Access Hospitals and HCAHPS Michelle Casey, MS Senior Research Fellow and Deputy Director University of Minnesota Rural Health Research Center June 12, 2012 Overview of Presentation Why is HCAHPS
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Medicaid MOA Update and Payment Reform Visioning Session
 Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Medicaid MOA Update and Payment Reform Visioning Session Where we are today, developing a vision for the future www.mpca.net The History PPS and Medicare cost-based reimbursement were created (2000) in
Dashboard. Campaign for Action. Welcome to the Future of Nursing:
 Welcome to the Future of Nursing: Campaign for Action Dashboard About This Dashboard: These graphs and charts show goals by which the Campaign evaluates its efforts to implement recommendations in the
Welcome to the Future of Nursing: Campaign for Action Dashboard About This Dashboard: These graphs and charts show goals by which the Campaign evaluates its efforts to implement recommendations in the
Paying for Value and Aligning with Other Purchasers
 Paying for Value and Aligning with Other Purchasers NAMD Bootcamp, Lake Tahoe, May 18, 2014 Dianne Hasselman, Director, Value Based Purchasing, Center for Health Care Strategies Deidre Gifford, MD, Medicaid
Paying for Value and Aligning with Other Purchasers NAMD Bootcamp, Lake Tahoe, May 18, 2014 Dianne Hasselman, Director, Value Based Purchasing, Center for Health Care Strategies Deidre Gifford, MD, Medicaid
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Nielsen ICD-9. Healthcare Data
 Nielsen ICD-9 Healthcare Data Healthcare Utilization Model The Nielsen healthcare utilization model has three primary components: demographic cohort population counts, cohort-specific healthcare utilization
Nielsen ICD-9 Healthcare Data Healthcare Utilization Model The Nielsen healthcare utilization model has three primary components: demographic cohort population counts, cohort-specific healthcare utilization
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet
 Cohort 3 Request for Application (RFA) Packet") Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
Fiscal Year 1999 Comparisons. State by State Rankings of Revenues and Spending. Includes Fiscal Year 2000 Rankings for State Taxes Only
 Fiscal Year 1999 Comparisons State by State Rankings of Revenues and Spending Includes Fiscal Year 2000 Rankings for State Taxes Only January 2002 1 2 published annually by: The Minnesota Taxpayers Association
Fiscal Year 1999 Comparisons State by State Rankings of Revenues and Spending Includes Fiscal Year 2000 Rankings for State Taxes Only January 2002 1 2 published annually by: The Minnesota Taxpayers Association
Introduction. Current Law Distribution of Funds. MEMORANDUM May 8, Subject:
 MEMORANDUM May 8, 2018 Subject: TANF Family Assistance Grant Allocations Under the Ways and Means Committee (Majority) Proposal From: Gene Falk, Specialist in Social Policy, gfalk@crs.loc.gov, 7-7344 Jameson
MEMORANDUM May 8, 2018 Subject: TANF Family Assistance Grant Allocations Under the Ways and Means Committee (Majority) Proposal From: Gene Falk, Specialist in Social Policy, gfalk@crs.loc.gov, 7-7344 Jameson
YOUTH MENTAL HEALTH IS WORSENING AND ACCESS TO CARE IS LIMITED THERE IS A SHORTAGE OF PROVIDERS HEALTHCARE REFORM IS HELPING
 2 3 4 MENTAL HEALTH AND SUBSTANCE USE CONDITIONS ARE COMMON MOST AMERICANS LACK ACCESS TO CARE OF AMERICAN ADULTS WITH A MENTAL ILLNESS DID NOT RECEIVE TREATMENT ONE IN FIVE REPORT AN UNMET NEED NEARLY
2 3 4 MENTAL HEALTH AND SUBSTANCE USE CONDITIONS ARE COMMON MOST AMERICANS LACK ACCESS TO CARE OF AMERICAN ADULTS WITH A MENTAL ILLNESS DID NOT RECEIVE TREATMENT ONE IN FIVE REPORT AN UNMET NEED NEARLY
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
How North Carolina Compares
 How North Carolina Compares A Compendium of State Statistics January 2013 Prepared by the N.C. General Assembly Program Evaluation Division Program Evaluation Division North Carolina General Assembly Legislative
How North Carolina Compares A Compendium of State Statistics January 2013 Prepared by the N.C. General Assembly Program Evaluation Division Program Evaluation Division North Carolina General Assembly Legislative
Rankings of the States 2017 and Estimates of School Statistics 2018
 Rankings of the States 2017 and Estimates of School Statistics 2018 NEA RESEARCH April 2018 Reproduction: No part of this report may be reproduced in any form without permission from NEA Research, except
Rankings of the States 2017 and Estimates of School Statistics 2018 NEA RESEARCH April 2018 Reproduction: No part of this report may be reproduced in any form without permission from NEA Research, except
Senior American Access to Care Grant
 Senior American Access to Care Grant Grant Guidelines SENIOR AMERICAN (age 62 plus) ACCESS TO CARE GRANT GUIDELINES: The (ADAF) is committed to supporting U.S. based organizations exempt from taxation
Senior American Access to Care Grant Grant Guidelines SENIOR AMERICAN (age 62 plus) ACCESS TO CARE GRANT GUIDELINES: The (ADAF) is committed to supporting U.S. based organizations exempt from taxation
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by February 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Alabama 3.7 33 Ohio 4.5 2 New Hampshire 2.6 19 Missouri 3.7 33 Rhode Island 4.5
States Ranked by February 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Alabama 3.7 33 Ohio 4.5 2 New Hampshire 2.6 19 Missouri 3.7 33 Rhode Island 4.5
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by November 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Indiana 4.4 37 Georgia 5.6 2 Nebraska 2.9 20 Ohio 4.5 37 Tennessee 5.6
States Ranked by November 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Indiana 4.4 37 Georgia 5.6 2 Nebraska 2.9 20 Ohio 4.5 37 Tennessee 5.6
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by April 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Colorado 2.3 17 Virginia 3.8 37 California 4.8 2 Hawaii 2.7 20 Massachusetts 3.9 37 West Virginia
States Ranked by April 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Colorado 2.3 17 Virginia 3.8 37 California 4.8 2 Hawaii 2.7 20 Massachusetts 3.9 37 West Virginia
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by August 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.3 18 Maryland 3.9 36 New York 4.8 2 Colorado 2.4 18 Michigan 3.9 38 Delaware 4.9
States Ranked by August 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.3 18 Maryland 3.9 36 New York 4.8 2 Colorado 2.4 18 Michigan 3.9 38 Delaware 4.9
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by March 2016 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 South Dakota 2.5 19 Delaware 4.4 37 Georgia 5.5 2 New Hampshire 2.6 19 Massachusetts 4.4 37 North
States Ranked by March 2016 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 South Dakota 2.5 19 Delaware 4.4 37 Georgia 5.5 2 New Hampshire 2.6 19 Massachusetts 4.4 37 North
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by September 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.4 17 Indiana 3.8 36 New Jersey 4.7 2 Colorado 2.5 17 Kansas 3.8 38 Pennsylvania
States Ranked by September 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.4 17 Indiana 3.8 36 New Jersey 4.7 2 Colorado 2.5 17 Kansas 3.8 38 Pennsylvania
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by December 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.0 16 South Dakota 3.5 37 Connecticut 4.6 2 New Hampshire 2.6 20 Arkansas 3.7 37 Delaware
States Ranked by December 2017 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.0 16 South Dakota 3.5 37 Connecticut 4.6 2 New Hampshire 2.6 20 Arkansas 3.7 37 Delaware
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by September 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.8 17 Oklahoma 4.4 37 South Carolina 5.7 2 Nebraska 2.9 20 Indiana 4.5 37 Tennessee
States Ranked by September 2015 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.8 17 Oklahoma 4.4 37 South Carolina 5.7 2 Nebraska 2.9 20 Indiana 4.5 37 Tennessee
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by November 2014 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Pennsylvania 5.1 35 New Mexico 6.4 2 Nebraska 3.1 20 Wisconsin 5.2 38 Connecticut
States Ranked by November 2014 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 North Dakota 2.7 19 Pennsylvania 5.1 35 New Mexico 6.4 2 Nebraska 3.1 20 Wisconsin 5.2 38 Connecticut
Unemployment Rate (%) Rank State. Unemployment
 Rank State. Unemployment") States Ranked by July 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Massachusetts 3.6 37 Kentucky 4.3 2 Iowa 2.6 19 South Carolina 3.6 37 Maryland 4.3
States Ranked by July 2018 Unemployment Rate Seasonally Adjusted Unemployment Unemployment Unemployment 1 Hawaii 2.1 19 Massachusetts 3.6 37 Kentucky 4.3 2 Iowa 2.6 19 South Carolina 3.6 37 Maryland 4.3
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Utilizing Grants to Achieve Your Farm Objectives
 Utilizing Grants to Achieve Your Farm Objectives Ohio Ecological Food and Farm Association Annual Conference- Granville, OH February 13, 2010 Mike Hogan Extension Educator & Associate Professor Sustainable
Utilizing Grants to Achieve Your Farm Objectives Ohio Ecological Food and Farm Association Annual Conference- Granville, OH February 13, 2010 Mike Hogan Extension Educator & Associate Professor Sustainable
CRMRI White Paper #3 August 2017 State Refugee Services Indicators of Integration: How are the states doing?
 CRMRI White Paper #3 August 7 State Refugee Services Indicators of Integration: How are the states doing? Marci Harris, Julia Greene, Kilee Jorgensen, Caren J. Frost, & Lisa H. Gren State Refugee Services
CRMRI White Paper #3 August 7 State Refugee Services Indicators of Integration: How are the states doing? Marci Harris, Julia Greene, Kilee Jorgensen, Caren J. Frost, & Lisa H. Gren State Refugee Services
Grants 101: An Introduction to Federal Grants for State and Local Governments
 Grants 101: An Introduction to Federal Grants for State and Local Governments Introduction FFIS has been in the federal grant reporting business for a long time about 30 years. The main thing we ve learned
Grants 101: An Introduction to Federal Grants for State and Local Governments Introduction FFIS has been in the federal grant reporting business for a long time about 30 years. The main thing we ve learned
Running head: NURSING SHORTAGE 1
 Running head: NURSING SHORTAGE 1 Nursing Shortage: The Current Crisis Evett M. Pugh Kent State University College of Nursing Running head: NURSING SHORTAGE 2 Abstract This paper is aimed to explain the
Running head: NURSING SHORTAGE 1 Nursing Shortage: The Current Crisis Evett M. Pugh Kent State University College of Nursing Running head: NURSING SHORTAGE 2 Abstract This paper is aimed to explain the
5 x 7 Notecards $1.50 with Envelopes - MOQ - 12
 5 x 7 Notecards $1.50 with Envelopes - MOQ - 12 Magnets 2½ 3½ Magnet $1.75 - MOQ - 5 - Add $0.25 for packaging Die Cut Acrylic Magnet $2.00 - MOQ - 24 - Add $0.25 for packaging 2535-22225 California AM-22225
5 x 7 Notecards $1.50 with Envelopes - MOQ - 12 Magnets 2½ 3½ Magnet $1.75 - MOQ - 5 - Add $0.25 for packaging Die Cut Acrylic Magnet $2.00 - MOQ - 24 - Add $0.25 for packaging 2535-22225 California AM-22225