Addressing Challenges In Pa0ent Safety: Implemen0ng Systems- Based Approaches James P. Bagian, MD, PE
|
|
|
- Cornelia Morton
- 6 years ago
- Views:
Transcription
1 Addressing Challenges In Pa0ent Safety: Implemen0ng Systems- Based Approaches James P. Bagian, MD, PE Chief Pa)ent Safety and Systems Innova)on Officer Director, Center for Health Engineering & Pa)ent Safety University of Michigan
2 Overview Defini)ons The Problem Historical Perspec)ve Cultural Factors Systems- Based Approach Priori)za)on/Risk Causes and Ac)ons Implementa)on Challenges Conclusions 2
3 Defini0ons Quality The extent to which a service or product produces a desired outcome(s). Safety Preven)on or modera)on of hazard induced harm. Hazard A circumstance or agent that can lead to harm, damage, or loss. Risk The chance of a specific event occuring. Measured in terms of consequences and likelihood.
4 What Is A System? A collec)on of elements whose opera)on is interdependent. Systems obey rules that cannot be understood by breaking them into parts, and stop func)oning (or malfunc)on) when an element is removed or altered significantly. Systems provide a coherent and unified way of viewing, interpre)ng and of organizing our thoughts about the world.
5 IOM Goals Safe Timely Efficient Effec)ve Equitable Pa)ent- Centered
6 Pa0ent Safety - The Problem Not New Schimmel (Ann. Int. Med.) Steel (NEJM) Family Prac)ce MDs (JFamPrct) 11/99 - IOM Report Deaths due to Preventable Adverse Events greater than MVA, Breast Cancer, or AIDS
7 Medicare Adverse Events % Adverse Events (Serious Events) 13.5% Temporary Harm 1.5% die (15,000/month = >150,000/yr)
 $750Billion wasted/yr Implement Best Clinical Knowledge More Rapidly Digital Infrastructure Clinical")
8 Ins0tute of Medicine (Sept. 2012) $750Billion wasted/yr Implement Best Clinical Knowledge More Rapidly Digital Infrastructure Clinical Decision Support Align Incen)ves Pa)ent Centered Care Con)nuity Op)mize Opera)ons 8
9 Where Healthcare Was/Is Cokage Industry Mentality Virtually Total Reliance on: Professional/Individual Responsibility Individual Perfec)on Train and Blame Likle Understanding of Systems Rela)ve to People and Processes Ignorance vs Arrogance Culturally Different!!!!
10 Typical Approach New Policies, Regula)ons,Repor)ng Systems, Training Good First Step But.. Lack of Systems Insight Superficial Solu)ons (?Answers) Inadequate Follow- Up Lost Opportunity
11 Typical Missing Features Clear Understanding of Goal
12 Typical Missing Features Clear Understanding of Goal Preven)ve Approach Field Understanding & Buy- In Systems Approach Sustainability Trust/Culture of Safety
13 Safety System Design High Reliability Organiza)ons Role of Repor)ng Learning or Accountability
14 Safety System Design High Reliability Organiza)ons Role of Repor)ng Learning or Accountability Systems- Based Solu)ons Pa)ent Centered DUH!!!! Importance of Close Calls
15 Pa0ent Safety System Design
16 Pa0ent Safety System Design
17 Pa0ent Safety System Design NASA Experience
18 Guiding Principles For Pa0ent Safety System Learning, Not Accountability System Repor)ng System Characteris)cs Non- puni)ve - Confiden)al and De- iden)fied Importance of Close Call Reports Should Emphasize Narra)ves Interdisciplinary Review Teams About Iden)fying Vulnerabili)es NOT Sta)s)cs Prompt Feedback
19 Safety & Human Error: Challenges Healthcare Views Errors as Failings Which Deserve Blame - Fault Train and Blame Mentality vs Systems- Based Blind Adherence To Rules Correc)ve Ac)ons Focusing on Individual No Blood No Foul Philosophy
20 Safety & Human Error: Cornerstones People Don t Come to Work to Hurt Someone or Make a Mistake Must Keep Asking Why?

21 Safety Human Error Incomplete procedures Regulatory narrowness Production pressures Responsibility shifting Mixed Messages Inadequate training Attention Distractions Deferred Maintenance Clumsy Technology LATENT FAILURES DEFENSES Accident
22 Safety Human Error Hindsight Bias
23 Pa0ent Safety - Strategy Invite People to Play Problem Recogni)on Remove Barriers (Puni)ve, Difficulty, Black Hole Effect) Learning NOT Accountability System Importance of Close Call Blameworthy Defini;on Training (Middle thru Top Management) Leadership At All Levels Human Factors Approach Tools That Guide Behavior
24 Changing Culture Tools Behavior Attitude CULTURE!!!
25 Priori0ze Risk Based Severity Probability Must Make Sense Business Processes Regulatory Environment
26 Causa0on/Ac0ons: Who vs.what &Why Who Whose Fault Is This? Ac)ons focused on correc)ng individual Corrects only aser problem occurs Limited scope of ac)on and generalizability What & Why Ac)ons focus on systems level causa)on Widespread applicability Stronger preven)ve strategy
27 Systema0c Cause and Effect Human Error Must Have Preceding Cause Failure to Follow Procedure By Itself Is NOT a Root Cause Nega)ve Descriptors Aren t Ac)onable Failure To Act Is Not A Cause Without Pre- exis)ng Requirement To Act Why,Why,Why
28 Human Factors Engineering and Ac0ons Warnings and labels (watch out!) Weaker Training (don t do that) Procedure changes (work around that) Interlock, lock- in, lock- out, etc (let me design it so you can not do that forcing func)ons) Is there one right ac0on??? Stronger
29 Ac0on Assessment Characteris)cs of Ac)ons Temporary vs. Permanent Procedural vs. Physical Ac)on Evalua)on Process Outcome
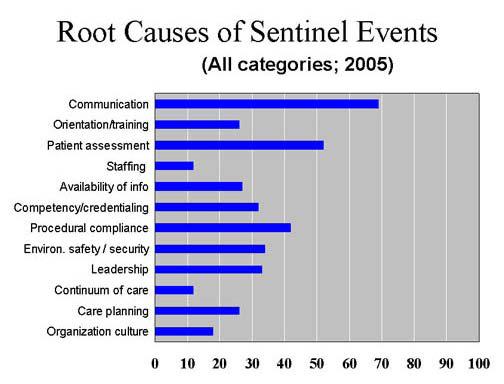
30 Communica0on - The Problem Reliability In Healthcare Is Poor Not Individually Acknowledged Basic Problems Are Same World Over Property of Being Human Organiza)onally Ignored Compared To Other High Hazard Industries
31 Communica0on Communica)on Iden)fied As Principal Factor >70% Of RCAs Medical Team Training (MTT) Developed To Improve Results Crew Resource Management Principles AND Briefings and De- Briefings
32 Root Cause Analyses (RCA) Database* ~70% to 80% of RCAs cited COMMUNICATION FAILURE as, at least one of the root causes/contributing factors for an adverse event or close call report. *SPOT Database: VA National Center for Patient Safety, April, 2008 Completed RCAs, Number = 8661.
33
34 Teamwork
onal Results Solid Rela)onships Accepted Leadership Effec)ve")
35 Characteris0cs of a Powerful Team Common Purpose Excellent Communica)ons Clear Roles Excep)onal Results Solid Rela)onships Accepted Leadership Effec)ve Processes
36 Challenge Medical Personnel, Par)cularly Physicians Have Been Rewarded Throughout Training for Individual Achievement. Highly Compe))ve Healthcare System Tradi)onally Financially Rewards Individual Ac)vity/Service Delivered, Not Outcome Teamwork Not Tradi)onally Valued, Taught, or Rewarded 36
37 Aviation Safety & Crew Resource Management (CRM)
38 Crew Resource Management (CRM)* Origin: NASA workshops examining the role of human error in airline crashes Research into aviation accidents in 1970s Definition: Using all available sources information, equipment, and people to achieve safe and efficient operations. Focus: safety, efficiency, and morale of humans working together LOFT: Line Oriented Flight Training Work in flight simulators and measurement of airline crew performance Briefings and Debriefings * Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future directions. Harvard Health Policy Review. 2004; 5(1):
39 CRM Training* Required by FAA and worldwide the way of doing business Aircrew performance measured by materials, organization, individual, and group variables Expanded aviation training from technical focus to human factors dimensions stress, fatigue, communication, shared awareness, and teamwork Outcomes: efficiency, safety, customer satisfaction Airline crew surveys: CRM relevant, useful, and effective in changing attitudes and behavior to improve safety CRM accepted by industry on face validity * Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future directions. Harvard Health Policy Review. 2004; 5(1):
40 Communica0on Definition: The exchange of thoughts, messages, or information.* A dynamic process between people: Sender (talks/writes/signals) & Receiver (listens/reads/signals) Roles alternate back & forth Verbal vs. non-verbal Feedback: Sending a message is not sufficient Was it received understood? * The American Heritage Dictionary, 4 th edition, Houghton Mifflin Company (2001): 179.
41 Communica0on Skills In medical school and nursing school, the focus is on successful communication with the patient.
42 Successful Communica0on Many communication improvements focus on improving accuracy and availability of content, e.g. CPOE, CPRS, Hand-Off templates Poor communication results from context. Context is vulnerable to culture, gender, education, experience, time pressure, stress, mood, etc.
43 Collabora0on & Teamwork in ICU = Lower Morbidity & Mortality + Increased RN Reten0on Evidence from ICUs Knaus 5030 ICU pts in 13 hospitals M&M risk improved with collaboration Baggs 286 consecutive Med ICU pts transferred M&M risk decreased from 16% to 5% Shortell pts from 42 ICU Teamwork across disciplines improved outcomes & RN retention Pronovost Daily briefings in ICU with RNs and Residents Improved quality of care
44 Impact of Team Training? VA Facility and NCPS 12 Leadership Young (1991) Observational study of VAMCs 10 Lower M&M (Observed/Expected ratios) Standardization of 8 work, hands on supervision of attending surgeons, residents, and nurses 6 Mentoring program for residents Effective interdisciplinary 4 communication Larger % of effective 2 coordination practices among providers Meterko (2004) Survey 0 of 125 VAMCs Teamwork Culture Strong correlation between teamwork culture and patient satisfaction (Teamwork Culture = Prevalent collaboration across disciplines.) Patient Satisfaction Scores
45 Culture of Safety Learns from adverse events People report things Non puni)ve Flaken hierarchies promotes teamwork and open feedback (CRM) Safety examined retrospec)vely and prospec)vely Intensive training of personnel and teams Systems thinking Build fault tolerance into the system


ll func)ons")
46 Fault Tolerance Zero error is NOT realis0c. Fault tolerant system - system can experience errors but s)ll func)ons successfully.



47 VHA NCPS Medical Team Training Program Mean = 74 Attendees Per Learning Session Largest One Day Session = 208 (Baltimore, MD Jan 14, 2010) Largest Facility Attendance = 356 (Dallas, TX December 9-11, 2008) 47
48 Briefings Dialogue among principals using concise, relevant information to promote clear and effective communication - Real time - Face-to-face - All team members present - All team members participate
49 Why do a Briefing? Establish a platform for common understanding Gives people permission to be frank & honest Gets everyone on the same page Provides a structure for collaborative planning Creates a shared mental model
50 Suppor0ng Long Term Memory Checklists Put knowledge in the world vs. in the head Recogni)on is beker than recall Tool to Guide and Improve Communica0on Checklist Philosophy Read and Verify checklists Read and Do checklists
ent..BRIEFED ACer Inser;on Tourniquet REMOVED Line...FLUSHED Pump.")
51 Before Inser;on IV Inser;on Checklist Pa)ent Iden)fica)on..CONFIRMED Correct Side CONFIRMED Catheter Size..CONFIRMED Equipment AT BEDSIDE Pa)ent..BRIEFED ACer Inser;on Tourniquet REMOVED Line...FLUSHED Pump.SET (with fluids) Sharps DISPOSED Site..LABELED Documenta)on.COMPLETE
52 Pre- Op Briefing Entire Surgical Team Attending surgeon Anesthesiologist/CRNA Circulator Scrub nurse/tech Resident, PA, perfusionist, others Guided by checklist guide (specialty specific) OR suite prior to anesthetic induction Does not replace pre-op planning Complements the TIMEOUT
53 Asking the right ques0on Any ques)ons? VS What is your biggest concern for today?

54 Checklist- Driven Preopera0ve Briefing



55 STEP BACK Use Chain of Command TAKE ACTION 4 Step Assertive Tool 1. Get Attention 2. State Concern ( Feel The Pinch ) I m uncomfortable with I m concerned about 3. Offer Solution 4. Pose Question 3 W s 1. What I see 2. What I m concerned about 3. What I want OR SBAR 1. Specific 2. Direct 3. Concise Avoid Hint and Hope
56 Post- Op Debriefing Entire Surgical Team Attending surgeon Anesthesiologist/CRNA Circulator Scrub nurse/tech Resident, PA, perfusionist, others Guided by checklist (specialty specific) What went well? What did not go well? What did we learn? What can we do to improve our processes? Timing when patient is stable before attending leaves (update prior to patient leaving OR) Method to track debrief items and follow-up
57 Post- Op Debriefing What it is NOT: Chance to whine about people Chance to collect sta)s)cs for sta)s)cs sake What it IS: Tool to iden)fy problems that impact pa)ent care Tool to solve problems as a team
58 The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again.
59 Followership Engaged and ac)ve in decision making Cri)cal thinkers? Assume ownership and responsibility for team decisions Provide honest, )mely feedback Speak up regardless of situa)on or rank Asser)ve but Respecxul
60 Situational Awareness Definition: The continuous perception of self and team in relation to the dynamic environment and the ability to make adjustments. The one most important aid in maintaining Situational Awareness is a common understanding of the briefed plan.



61 Medical Team Training Safety Aetudes Ques0onnaire In this clinical area, it is easy to speak up. * * I would feel safe being a patient here. * P < 0.05 paired, Students t-test N = 3138 Ques;onnaires
62 Nursing Turnover Operating Room 10 P = 0.02 % Turnover Per Year Pre 45 Operating Rooms and 35 Intensive Care Units Pre = 12 Months Prior to Learning Session Post = 12 Months Following Learning Session Post

63 Outcomes Morbidity / Mortality Observed / Expected Mortality Ra0os P = 0.03 Quarters of MTT August 19, 2009 MTT Preliminary Report : N = 99 facilities.
64 MTT Facility Level Impact 67% High Impact on OR Staff 73% High Impact on OR Pa)ents 69% of OR Teams Improved Teamwork 66% of OR Teams Report Improved Efficiency Eqpt U)l (61%), Starts (35%), Dura)on (19%) Safety Aytudes Ques)onnaire (SAQ) Significant Improvement (p<0.001): Working Condi)ons, Percep)on of Mgmt, Job Sa)sfac)on, Safety Climate, & Teamwork

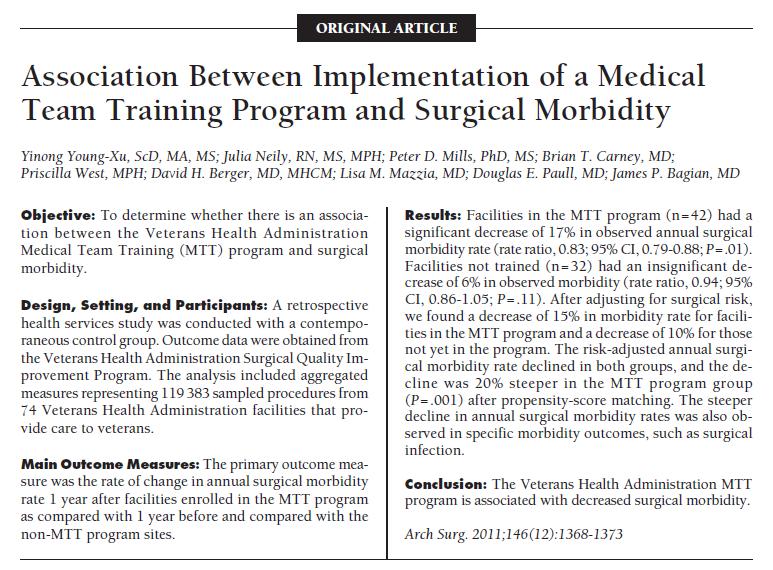
65 Neily et al. Assoc. Between MTT and Surg Mortality. JAMA. 2010;304(15):
66
67
68 MTT Impact N=108 Ins)tu)ons; 74 MTT, 34 Control MTT 50% greater decrease in mortality & morbidity than Control Dose- response 0.5 deaths/1000 procedures less per quarter p= deaths/1000 procedures per increase in briefing/debriefing p= % Reduc)on in reported OR related harm
69 What Have We Learned? Ac)ons needed well before entering the OR Timeout period is too late in many cases Systems- based approaches beyond individual Involvement of all disciplines Structured communica)on that drives discussion Briefings & debriefings, Medical Team Training essen)al
70 In Perspec0ve - Goethe Knowing is not enough; we must apply. Willing is not enough; we must do."
71 Implementa0on 71
72 Steps In OR Status Quo Pre- Induc)on Pre- Incision Sign Out MTT Pre- Induc)on Pre- Incision Post- Op Debrief Sign Out

73 OR Policy Changed to Require Attending Surgeon in OR
74 Trust But Verify!! 74
75 Observa0onal Data
76 Conclusions Need To Con)nue Improvement on Teamwork and Safety Climate in the OR and PACU MTT is beginning to address some of these issues Post- MTT data has shown some improvement Recent Data show that people more likely to be on the on same page MTT process (Debriefing) is highligh)ng issues that need and are geyng aken)on Must put system in place to deal with inputs MTT Is An Ongoing Process Requires Leadership
77 Sustainable Systems Approach Problem Iden)fica)on Clear Goal Defini)on Involvement Of All Sectors Iden)fy Systems Influences Iden)fy Systems Controls Iden)fy Constraints Cri;que Go To Worst Cri;cs Early On Pilot Volunteers First Then Others Evaluate
78 Who s On The Team? Clinicians Administra)ve Other Staff Users Pa)ents Personnel with Systems Background Opera)ons Research Management Human Factors Ergonomics
79 Essen0al Elements For Sustainable Improvement Appropriate Goal Iden)fica)on & Selec)on Transparent Priori)za)on Iden)fica)on of Real Causes System- based Countermeasures That Address Underlying Causes Stronger Ac)ons That Are Explicit Measurement of Ac)ons Process & Outcome Feedback/Transparency Top Leadership Involvement/Visibility
80 Closing Thoughts It s Everyone s Job Not About Errors!!! Coun)ng reports is not the objec)ve, iden)fying Vulnerabili)es is Hope they increase Analysis, Ac0on, & Feedback are the key Preven)on NOT Punishment Cultural change is the key takes )me Safety is the Founda;on Upon which Quality is Built
Teamwork and Communication for Quality & Safety: It s More Than Checklists
 Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
Data Collec*on and Measurement in Quality Improvement
 Data Collec*on and Measurement in Quality Improvement Tanishah Nellom, MSPH Care Improvement Specialist, CCME January 2013 Quality Improvement in Healthcare The combined and unceasing efts of everyone
Data Collec*on and Measurement in Quality Improvement Tanishah Nellom, MSPH Care Improvement Specialist, CCME January 2013 Quality Improvement in Healthcare The combined and unceasing efts of everyone
Na#onal Pa#ent Safety Goals
 Na#onal Pa#ent Safety Goals 2017 www.ahrq.gov What are Na#onal Pa#ent Safety Goals? The purpose of Na2onal Pa2ent Safety Goals is to improve pa2ent safety. The goals relate to problems in healthcare safety
Na#onal Pa#ent Safety Goals 2017 www.ahrq.gov What are Na#onal Pa#ent Safety Goals? The purpose of Na2onal Pa2ent Safety Goals is to improve pa2ent safety. The goals relate to problems in healthcare safety
Management Systems for Healthcare Environmental, Health and Safety
 Management Systems for Healthcare Environmental, Health and Safety Danial Bravard, Senior Consultant and Head of Healthcare Services, BSI EHS Services and Solu=ons Ma> Aus=n, CIH, Occupa=onal Safety Manager,
Management Systems for Healthcare Environmental, Health and Safety Danial Bravard, Senior Consultant and Head of Healthcare Services, BSI EHS Services and Solu=ons Ma> Aus=n, CIH, Occupa=onal Safety Manager,
Five Core Components for a Hospital-based Injury Preven:on Program
 Five Core Components for a Hospital-based Injury Preven:on Program Mul$ple Texas Trauma Organiza$ons Conduc$ng Injury Preven$on Governor s EMS & Trauma Advisory Council (GETAC) Injury Preven$on CommiCee
Five Core Components for a Hospital-based Injury Preven:on Program Mul$ple Texas Trauma Organiza$ons Conduc$ng Injury Preven$on Governor s EMS & Trauma Advisory Council (GETAC) Injury Preven$on CommiCee
The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE
 Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE 877.399.6538 sales@kinnser.com www.kinnser.com About the presenter SHARON HARDER President
Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE 877.399.6538 sales@kinnser.com www.kinnser.com About the presenter SHARON HARDER President
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
4/2/15. Re)na 2015 and Beyond Keys to Management Success. Financial Disclosures. Top Prac)ce Management Challenges
na 2015 and Beyond Keys to Management Success. Financial Disclosures. Top Prac)ce Management Challenges") Re)na 2015 and Beyond Keys to Management Success Panelists: Jeff Brocke
Re)na 2015 and Beyond Keys to Management Success Panelists: Jeff Brocke
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Crew Resource Management for Trauma Resuscitation. Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation
 Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
Basic Overview of Funding Opportuni6es at the Ins6tute of Educa6on Sciences
 Connecting Research, Policy and Practice Basic Overview of Funding Opportuni6es at the Ins6tute of Educa6on Sciences Erin Higgins, Ph.D. Program Officer Na6onal Center for Educa6on Research Ka6e Taylor,
Connecting Research, Policy and Practice Basic Overview of Funding Opportuni6es at the Ins6tute of Educa6on Sciences Erin Higgins, Ph.D. Program Officer Na6onal Center for Educa6on Research Ka6e Taylor,
HSOPS Analysis and Interpretation. Using The Pa,ent Safety Group (PSG)
") HSOPS Analysis and Interpretation Using The Pa,ent Safety Group (PSG) Objectives Describe post-survey activities Explain how to generate reports from PSG Identify HSOPS interpretation strategies Results,
HSOPS Analysis and Interpretation Using The Pa,ent Safety Group (PSG) Objectives Describe post-survey activities Explain how to generate reports from PSG Identify HSOPS interpretation strategies Results,
NCQC PSO Safe Tables. Failure To Rescue. Failure to Rescue
 NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
Check list and CVC Dr ROSAY Unité d accès vasculaire DAR CLB Lyon
 Check list and CVC 2015 Dr ROSAY Unité d accès vasculaire DAR CLB Lyon Provonost P Berenholtz SM To err is human Preven6on of Catheters Related Bloodstream Infec6ons Berenholtz SM, Crit Care Med,
Check list and CVC 2015 Dr ROSAY Unité d accès vasculaire DAR CLB Lyon Provonost P Berenholtz SM To err is human Preven6on of Catheters Related Bloodstream Infec6ons Berenholtz SM, Crit Care Med,
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Improving Surgical Instrument Reprocessing at the University of Michigan Health System (UMHS) Daniel Hazle*
 Daniel Hazle*") Improving Surgical Instrument Reprocessing at the University of Michigan Health System (UMHS) Daniel Hazle* ur Collaborators M Center for Healthcare Engineering and Pa9ent Safety (CHEPS) James P. Bagian
Improving Surgical Instrument Reprocessing at the University of Michigan Health System (UMHS) Daniel Hazle* ur Collaborators M Center for Healthcare Engineering and Pa9ent Safety (CHEPS) James P. Bagian
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Second Chance Act Grants: Guidance for Smart Proba7on Applicants
 Second Chance Act Grants: Guidance for Smart Proba7on Applicants Brought to you by the Na.onal Reentry Resource Center and the Bureau of Jus.ce Assistance, U.S. Department of Jus.ce 2012 Council of State
Second Chance Act Grants: Guidance for Smart Proba7on Applicants Brought to you by the Na.onal Reentry Resource Center and the Bureau of Jus.ce Assistance, U.S. Department of Jus.ce 2012 Council of State
Global Health Assessment Strategies. Ricardo Izurieta
 Global Health Assessment Strategies Ricardo Izurieta Objec;ves General strategies for data collec;on in developing countries General guidelines for qualita;ve and quan;ta;ve assessment in developing countries
Global Health Assessment Strategies Ricardo Izurieta Objec;ves General strategies for data collec;on in developing countries General guidelines for qualita;ve and quan;ta;ve assessment in developing countries
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Strategy for Universal Access to Health and Universal Health Coverage March 2015
 Strategy for Universal Access to Health and Universal Health Coverage March 2015 Health Services and Access Unit Department of Health Systems and Services Resolu
Strategy for Universal Access to Health and Universal Health Coverage March 2015 Health Services and Access Unit Department of Health Systems and Services Resolu
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Rural Health and The Pa/ent Centered Medical Home. The Compliance Team Dianne Bourque, RN, CNOR, CASC Accredita/on Advisor
 Rural Health and The Pa/ent Centered Medical Home The Compliance Team Dianne Bourque, RN, CNOR, CASC Accredita/on Advisor The Compliance Team, Inc. Exemplary ProviderTM Accredita;on Program Every pa;ent
Rural Health and The Pa/ent Centered Medical Home The Compliance Team Dianne Bourque, RN, CNOR, CASC Accredita/on Advisor The Compliance Team, Inc. Exemplary ProviderTM Accredita;on Program Every pa;ent
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Standard 3.3: Survivorship Care Plan
 : Care Plan In 2012 the Commission on Cancer introduced new Standards for Cancer Program Accredita:on. They created a new chapter of standards en:tled: CONTINUUM OF CARE SERVICES 1 Included in this sec:on
: Care Plan In 2012 the Commission on Cancer introduced new Standards for Cancer Program Accredita:on. They created a new chapter of standards en:tled: CONTINUUM OF CARE SERVICES 1 Included in this sec:on
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
Welcome! PCORI s Application Submission Process. James Hulbert, Assistant Director, Policy and Planning. James Hulbert
 PCORI s Application Submission Process James Hulbert Assistant Director, Policy and Planning January 29, 2016 Welcome! James Hulbert, Assistant Director, Policy and Planning 2 Application Requirements:
PCORI s Application Submission Process James Hulbert Assistant Director, Policy and Planning January 29, 2016 Welcome! James Hulbert, Assistant Director, Policy and Planning 2 Application Requirements:
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
An Update on Stewardship Measurement in Hospitals: Programs and An#bio#c Use
 Na#onal Center for Emerging and Zoono#c Infec#ous Diseases An Update on Stewardship Measurement in Hospitals: Programs and An#bio#c Use CAPT Arjun Srinivasan, MD Division of Healthcare Quality Promo#on
Na#onal Center for Emerging and Zoono#c Infec#ous Diseases An Update on Stewardship Measurement in Hospitals: Programs and An#bio#c Use CAPT Arjun Srinivasan, MD Division of Healthcare Quality Promo#on
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Safety Culture. QI In Ac1on 29 th June Ma; Hill Consultant Anaesthe-st, Plymouth Regional Pa-ent Safety Officer, SWAHSN.
 Safety Culture QI In Ac1on 29 th June 2016 Ma; Hill Consultant Anaesthe-st, Plymouth Regional Pa-ent Safety Officer, SWAHSN ma;.hill1@nhs.net Why talk about culture at a QI mee1ng? The culture supports
Safety Culture QI In Ac1on 29 th June 2016 Ma; Hill Consultant Anaesthe-st, Plymouth Regional Pa-ent Safety Officer, SWAHSN ma;.hill1@nhs.net Why talk about culture at a QI mee1ng? The culture supports
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Developing New Models: Integra5ng House Calls and Team- Based Care Into Primary Care
 Developing New Models: Integra5ng House Calls and Team- Based Care Into Primary Care Christa Cerra, DNP, FNP by Renaissance Family Prac7ce. All right reserved. Key Players Renaissance Family Prac7ce (RFP)
Developing New Models: Integra5ng House Calls and Team- Based Care Into Primary Care Christa Cerra, DNP, FNP by Renaissance Family Prac7ce. All right reserved. Key Players Renaissance Family Prac7ce (RFP)
Prac%ce Management. Peter Bidey, D.O. February 20, 2016 Instructor, Family Medicine Medical Director, Family PCOM PCOM
 Prac%ce Management Peter Bidey, D.O. February 20, 2016 Instructor, Family Medicine Medical Director, Family Medicine @ PCOM PCOM Outline The Man The Measures The Money The Madness hdp://maddantodd.com/2013/01/18/introverts-extroverts-and-being-fake-online/
Prac%ce Management Peter Bidey, D.O. February 20, 2016 Instructor, Family Medicine Medical Director, Family Medicine @ PCOM PCOM Outline The Man The Measures The Money The Madness hdp://maddantodd.com/2013/01/18/introverts-extroverts-and-being-fake-online/
Development and assessment of a Patient Safety Culture Dr Alice Oborne
 Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
7/9/13. PCMH Finally The Power! W H A T. What is PCMH? I S P C M H? THIS MORNING W H A T I S P C M H? Why I LOVE This! It Just Makes Sense
 PCM Finally The Power! hy OV This! t Just Makes Sense Presented by: Susan Childs, FACMP voluon ealthcare Consulng www.evohcc.com Primary and Team Care Based Paent is Responsible Potenal For ncreased ncome
PCM Finally The Power! hy OV This! t Just Makes Sense Presented by: Susan Childs, FACMP voluon ealthcare Consulng www.evohcc.com Primary and Team Care Based Paent is Responsible Potenal For ncreased ncome
A culture of safety is a culture of compassion
 A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
Infirmières/infirmiers : Prenez votre place! Jewish General Hospital Evolving Dynamic Leadership in Academia and Clinical Nursing Practice
 Infirmières/infirmiers : Prenez votre place! Jewish General Hospital Evolving Dynamic Leadership in Academia and Clinical Nursing Practice Francine Girard, RN, BN, MN, Ph. D. Gelber Center, Montréal, June
Infirmières/infirmiers : Prenez votre place! Jewish General Hospital Evolving Dynamic Leadership in Academia and Clinical Nursing Practice Francine Girard, RN, BN, MN, Ph. D. Gelber Center, Montréal, June
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Content of the Lectures. Topic 8 Peter Wiedemann. Precau'onary Measures and Risk Management
 Precau'onary Measures and Risk Management Topic 8 Content of the Lectures Topic 1: Risk concept Topic 2: Percep'on of risks Topic 3: Risk communica'ons Topic 4: Trust and credibility Topic 5: Labeling
Precau'onary Measures and Risk Management Topic 8 Content of the Lectures Topic 1: Risk concept Topic 2: Percep'on of risks Topic 3: Risk communica'ons Topic 4: Trust and credibility Topic 5: Labeling
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of the Infec*on-Related Provisions in Centers for Medicare & Medicaid Services (CMS) FY 2015 Prospec*ve Payment System Final Rules for Inpa*ent Se4ngs Hospital Value-Based Purchasing (VBP) Program
Summary of the Infec*on-Related Provisions in Centers for Medicare & Medicaid Services (CMS) FY 2015 Prospec*ve Payment System Final Rules for Inpa*ent Se4ngs Hospital Value-Based Purchasing (VBP) Program
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
1/17/18. CMS Quality Measure Repor6ng Update. ASCQR Program Measures Summary
 Keeping you in the know in the ASC industry CMS Quality Repor6ng Update Gina Throneberry, RN, MBA, CASC, CNOR Director of Educa6on and Clinical Affairs Ambulatory Surgery Center Associa6on (ASCA) ASCQR
Keeping you in the know in the ASC industry CMS Quality Repor6ng Update Gina Throneberry, RN, MBA, CASC, CNOR Director of Educa6on and Clinical Affairs Ambulatory Surgery Center Associa6on (ASCA) ASCQR
Strengths of the Nursing Workforce and Challenges Nurses and the Health Organiza9ons that Employ them will Face Over the Next 10 Years
 Strengths of the Nursing Workforce and Challenges Nurses and the Health Organiza9ons that Employ them will Face Over the Next 10 Years The Missouri Hospital Associa9on June 15, 2017 Peter I. Buerhaus PhD,
Strengths of the Nursing Workforce and Challenges Nurses and the Health Organiza9ons that Employ them will Face Over the Next 10 Years The Missouri Hospital Associa9on June 15, 2017 Peter I. Buerhaus PhD,
Monitoring & Evalua/on. Ari Probandari
 Monitoring & Evalua/on Ari Probandari Learning Objec/ves Students are able to explain the importance of monitoring and evalua/on a program management Students are able to apply concepts of monitoring and
Monitoring & Evalua/on Ari Probandari Learning Objec/ves Students are able to explain the importance of monitoring and evalua/on a program management Students are able to apply concepts of monitoring and
A Systems Approach to Patient Safety at the VA
 BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
Developing a Concept Paper & Contac2ng a Program Officer. January 2016
 Developing a Concept Paper & Contac2ng a Program Officer January 2016 w w w. h a n o v e r r e s e a r c h. c o m CONCEPT PAPERS: PURPOSE 2 Concept Paper: Purpose A concept paper provides a concise summary
Developing a Concept Paper & Contac2ng a Program Officer January 2016 w w w. h a n o v e r r e s e a r c h. c o m CONCEPT PAPERS: PURPOSE 2 Concept Paper: Purpose A concept paper provides a concise summary
Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years
 Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years Interprofessional Care for the 21 st Century October 11, 2014 Pittsburgh, Pa. Joanne
Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years Interprofessional Care for the 21 st Century October 11, 2014 Pittsburgh, Pa. Joanne
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
City of San José Community Budget Priori<za<on Exercise Citywide Zero-Based Budge<ng Exercise
 City of San José 2016 2017 Community Budget Priori
City of San José 2016 2017 Community Budget Priori
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
Bridging the communication gap in the operating room with medical team training
 The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
High Reliability Organizations Healing Without Harm by 2014
 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Popula'on Health, Public Health, & Meaningful Use
 Popula'on Health, Public Health, & Meaningful Use James W. Buehler, MD Health Commissioner Philadelphia Department of Public Health Delaware Valley Chapter HIMSS January 29, 2015 1 Overview: What are the
Popula'on Health, Public Health, & Meaningful Use James W. Buehler, MD Health Commissioner Philadelphia Department of Public Health Delaware Valley Chapter HIMSS January 29, 2015 1 Overview: What are the
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
Clinical Programs. Purpose and Structure. October 7, 2014
 Clinical Programs Purpose and Structure October 7, 2014 Our Vision Crossing the Quality Chasm What are Intermountain Clinical Programs? The major vehicle to address the delivery and support of high quality,
Clinical Programs Purpose and Structure October 7, 2014 Our Vision Crossing the Quality Chasm What are Intermountain Clinical Programs? The major vehicle to address the delivery and support of high quality,
Leveraging Meaningful Use to Assist in Reducing Hospital Readmissions
 Leveraging Meaningful Use to Assist in Reducing Hospital Readmissions REACH - Achieving - Achieving meaningful meaningful use of your use EHR of your EHR Paul Kleeberg, MD, FAAFP, FHIMSS CMIO, Stra6s Health
Leveraging Meaningful Use to Assist in Reducing Hospital Readmissions REACH - Achieving - Achieving meaningful meaningful use of your use EHR of your EHR Paul Kleeberg, MD, FAAFP, FHIMSS CMIO, Stra6s Health
Re-Engineering Medication Processes to Capitalize on Technology. Jane Englebright, PhD, RN Vice President, Quality HCA
 Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY
 SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Defining an Outcome Measures Framework for Global Surgery
 Defining an Outcome Measures Framework for Global Surgery Richard Gliklich MD Leffenfeld Professor of Otology and Laryngology, Harvard Medical School Surgeon, Mass Eye and Ear; Massachusetts General Hospital
Defining an Outcome Measures Framework for Global Surgery Richard Gliklich MD Leffenfeld Professor of Otology and Laryngology, Harvard Medical School Surgeon, Mass Eye and Ear; Massachusetts General Hospital
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
Special Measures Quality Improvement Plan Update. Sherwood Forest Hospitals NHS Founda=on Trust. 10 March 2016 KEY. Delivered. On Track to deliver
 Special Measures Quality Improvement Plan Update Sherwood Forest Hospitals NHS Founda=on Trust March 6 KEY Delivered On Track to deliver Some issues narra
Special Measures Quality Improvement Plan Update Sherwood Forest Hospitals NHS Founda=on Trust March 6 KEY Delivered On Track to deliver Some issues narra
Qatar Mental Health Law. Dr. Suhaila Ghuloum, FRCPsych
 Qatar Mental Health Law Dr. Suhaila Ghuloum, FRCPsych DISCLOSURE STATEMENT Speaker: Suhaila Ghuloum, MD Has no relevant financial rela=onships to disclose Will not be discussing any unlabeled/unapproved
Qatar Mental Health Law Dr. Suhaila Ghuloum, FRCPsych DISCLOSURE STATEMENT Speaker: Suhaila Ghuloum, MD Has no relevant financial rela=onships to disclose Will not be discussing any unlabeled/unapproved
3/25/13. Objec+ve Four. Review of Literature. Project Health Link: HRSA Nursing Educa+on, Prac+ce and Reten+on (NEPR) ini+a+ve:
 ini+a+ve:") Crea+ng Evidence- Based Clinical Guidelines to Impact Pa+ent Outcomes and Student Educa+on Brenda Dyal, DNP Maria Whyte, DHSc Project Health Link: HRSA Nursing Educa+on, Prac+ce and Reten+on (NEPR) ini+a+ve:
Crea+ng Evidence- Based Clinical Guidelines to Impact Pa+ent Outcomes and Student Educa+on Brenda Dyal, DNP Maria Whyte, DHSc Project Health Link: HRSA Nursing Educa+on, Prac+ce and Reten+on (NEPR) ini+a+ve:
Kinnser is software for better post-acute care.
 Kinnser is software for better post-acute care. HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE 4,500 + Agency Customers 49% Faster Documentation 27% More Productive 52% Faster Billing 33% Less Expense 877.399.6538
Kinnser is software for better post-acute care. HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE 4,500 + Agency Customers 49% Faster Documentation 27% More Productive 52% Faster Billing 33% Less Expense 877.399.6538
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Grants 101. Grants 101. There is no grantsmanship that will turn a bad idea into a good one, but there are many ways to disguise a good idea.
 Grants 101 1 Grants 101 There is no grantsmanship that will turn a bad idea into a good one, but there are many ways to disguise a good idea. 2 October 10-13, 2013 1 Basic steps of grant development Step
Grants 101 1 Grants 101 There is no grantsmanship that will turn a bad idea into a good one, but there are many ways to disguise a good idea. 2 October 10-13, 2013 1 Basic steps of grant development Step
Nursing Certification and Competency Summit: Building an International Research Agenda
 Nursing Certification and Competency Summit: Building an International Research Agenda Summary Document Prepared for the American Board of Nursing Specialties and the Competency and Credentialing Institute
Nursing Certification and Competency Summit: Building an International Research Agenda Summary Document Prepared for the American Board of Nursing Specialties and the Competency and Credentialing Institute
Objectives. Vessel Health and Preservation: Disclosure. Ms. Moureau has disclosed the following: Angiodynamics, Genentech
 Vessel Health and Preservation: What is the Right Line for the Right Patient at the Right Time? Nancy Moureau, BSN, RN, CRNI, CPUI, VA-BC This program is sponsored by Teleflex Saxe Communications 2012
Vessel Health and Preservation: What is the Right Line for the Right Patient at the Right Time? Nancy Moureau, BSN, RN, CRNI, CPUI, VA-BC This program is sponsored by Teleflex Saxe Communications 2012
Determining)and)Addressing)Adherence)to)the)NCCN)Guidelines)for)Chronic)Phase)CML!
and)Addressing)Adherence)to)the)NCCN)Guidelines)for)Chronic)Phase)CML!") Brewer, B Page 1 Determining)and)Addressing)Adherence)to)the)NCCN)Guidelines)for)Chronic)Phase)CML Overall) Goal: Test a novel behavior change and educa4on interven4on to improve physician adherence to
Brewer, B Page 1 Determining)and)Addressing)Adherence)to)the)NCCN)Guidelines)for)Chronic)Phase)CML Overall) Goal: Test a novel behavior change and educa4on interven4on to improve physician adherence to
! 1. Goals and Objectives. Assessment of Need. Primary Audience of the Intervention. Direct Beneficiaries of The Program
 Goals and Objectives Assessment of Need Primary Audience of the Intervention Direct Beneficiaries of The Program Intervention Design and Methods Evaluation Design Table of Contents 1 2 3 4 4 8 Detailed
Goals and Objectives Assessment of Need Primary Audience of the Intervention Direct Beneficiaries of The Program Intervention Design and Methods Evaluation Design Table of Contents 1 2 3 4 4 8 Detailed
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
PATIENT SAFETY AT TEXAS CHILDREN S. Joan E. Shook, MD, MBA
 PATIENT SAFETY AT TEXAS CHILDREN S Joan E. Shook, MD, MBA TEXAS CHILDREN S HOSPITAL PATIENT SAFETY WHERE WE HAVE BEEN, WHERE WE ARE TODAY, AND A GLIMPSE OF THE FUTURE! 1999 To Err is Human 2004 Pa8ent
PATIENT SAFETY AT TEXAS CHILDREN S Joan E. Shook, MD, MBA TEXAS CHILDREN S HOSPITAL PATIENT SAFETY WHERE WE HAVE BEEN, WHERE WE ARE TODAY, AND A GLIMPSE OF THE FUTURE! 1999 To Err is Human 2004 Pa8ent
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Are We a Team of Experts or an Expert Team?
 Are We a Team of Experts or an Expert Team? BEST PRACTICES: Care for the Complex Community Dwelling Older Adult July 11 12, 2008 NEBGEC Annual Conference Katherine Jones, PT, PhD kjonesj@unmc.edu Objectives
Are We a Team of Experts or an Expert Team? BEST PRACTICES: Care for the Complex Community Dwelling Older Adult July 11 12, 2008 NEBGEC Annual Conference Katherine Jones, PT, PhD kjonesj@unmc.edu Objectives
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians
 Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
TeamSTEPPS TM. Improving Patient Safety Worldwide Through Teamwork and Communication
 TeamSTEPPS TM Improving Patient Safety Worldwide Through Teamwork and Communication Presenters Susan M Hohenhaus, RN, MA, FAEN President, Hohenhaus & Associates, Inc. Stephen M Powell, MS, Captain, Principal,
TeamSTEPPS TM Improving Patient Safety Worldwide Through Teamwork and Communication Presenters Susan M Hohenhaus, RN, MA, FAEN President, Hohenhaus & Associates, Inc. Stephen M Powell, MS, Captain, Principal,
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Crea%ng a Culture of Quality and Safety to Reduce Hospital- Acquired Infec%ons. September 2, 2010
 Crea%ng a Culture of Quality and Safety to Reduce Hospital- Acquired Infec%ons Leo Anthony Celi, MD, MS, MPH Harvard- MIT Health Sciences & Technology Division Department of Pulmonary, Cri%cal Care & Sleep
Crea%ng a Culture of Quality and Safety to Reduce Hospital- Acquired Infec%ons Leo Anthony Celi, MD, MS, MPH Harvard- MIT Health Sciences & Technology Division Department of Pulmonary, Cri%cal Care & Sleep
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Doing Good. Neighborhood
 Doing Good in the Neighborhood 2016 Community Care Fund Tips & Insider Information for Applicants Contents About the Campaign About the Community Care Fund Eligibility Criteria Applica8on Process & Timeline
Doing Good in the Neighborhood 2016 Community Care Fund Tips & Insider Information for Applicants Contents About the Campaign About the Community Care Fund Eligibility Criteria Applica8on Process & Timeline
Joint Theater Trauma System and Joint Trauma System Review of Pre- Hospital Trauma Care in Combined Joint Opera>ng Area Afghanistan (CJOA- A)
") Joint Theater Trauma System and Joint Trauma System Review of Pre- Hospital Trauma Care in Combined Joint Opera>ng Area Afghanistan (CJOA- A) Date: 30 May 2014 Classifica>on: Unclassified Joint Theater Trauma
Joint Theater Trauma System and Joint Trauma System Review of Pre- Hospital Trauma Care in Combined Joint Opera>ng Area Afghanistan (CJOA- A) Date: 30 May 2014 Classifica>on: Unclassified Joint Theater Trauma
Parole Decision Making in Montana
 Parole Decision Making in Montana Presenta7on to the Montana Commission on Sentencing Cathy McVey, Senior Policy Advisor Overview 01 02 03 Parole Decision Making in an Evidence-Based World Parole in Montana
Parole Decision Making in Montana Presenta7on to the Montana Commission on Sentencing Cathy McVey, Senior Policy Advisor Overview 01 02 03 Parole Decision Making in an Evidence-Based World Parole in Montana
Striving for Farm to School Sustainability
 A sustainable farm to school program can take shape in many different ways and is largely a result of the aspira7ons and work of those people, organiza7ons and resources that are unique to each community.
A sustainable farm to school program can take shape in many different ways and is largely a result of the aspira7ons and work of those people, organiza7ons and resources that are unique to each community.
Implementa*on of a Con*nued Professional Cer*fica*on Program (CPC) for Nurse Anesthe*sts
 for Nurse Anesthe*sts") Implementa*on of a Con*nued Professional Cer*fica*on Program (CPC) for Nurse Anesthe*sts January 29, 2014 Ed Waters DNP, CRNA Karen Plaus PhD, CRNA FAAN Overview Evolu*on of creden*aling of Nurse Anesthe*sts
Implementa*on of a Con*nued Professional Cer*fica*on Program (CPC) for Nurse Anesthe*sts January 29, 2014 Ed Waters DNP, CRNA Karen Plaus PhD, CRNA FAAN Overview Evolu*on of creden*aling of Nurse Anesthe*sts
Medicare Wellness What is it, and how can I u1lize this in my prac1ce? Rural Health Clinic Conference Jackson, MS
 Medicare Wellness What is it, and how can I u1lize this in my prac1ce? Rural Health Clinic Conference Jackson, MS Brad Crosswhite, M.D., FAAFP Central Regional Medical Director ACO Medical Director Population
Medicare Wellness What is it, and how can I u1lize this in my prac1ce? Rural Health Clinic Conference Jackson, MS Brad Crosswhite, M.D., FAAFP Central Regional Medical Director ACO Medical Director Population
Wrong Site, Wrong Procedure, Wrong Person Surgery
 Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient