CPETS: CALIFORNIA PERINATAL TRANSPORT SYSTEMS
|
|
|
- Marilynn Maxwell
- 6 years ago
- Views:
Transcription
1 CPETS: CALIFORNIA PERINATAL TRANSPORT SYSTEMS 2016 & 2017 Data Collection and Reports What s New in The Neonatal Transport Data Program, 2018 Presented by: D. Lisa Bollman, MSN, RNC-NIC, CPHQ Director: Southern California Perinatal Transport System
2 CONFLICTS OF INTEREST I have no conflicts of interest to disclose. I will not be making any recommendations on medications, devices or equipment in this lecture.
3 OBJECTIVES Following the lecture, discussion and questions and answers, the participant will be able to: Evaluate acute neonatal transport activity in California with emphasis on issues with quality improvement potential at statewide, regional and hospital levels; Analyze CPeTS standard reports for neonatal transport data and list three potential quality improvement topics for implementation in the participant s practice or facility; Discuss facility plan for maintaining bed availability website; and Identify future topics for quality improvement and any necessary additional data points.
4 CALIFORNIA PERINATAL TRANSPORT SYSTEM Legislatively mandated by AB 4439 in 1976, required by California Perinatal Quality Care Collaborative (CPQCC), California Children's Services (CCS) and California Department of Public Health(CDPH), managed by Regional Perinatal Programs of California (RPPC). Bed Availability and Direct Referral Information Neonatal Data System Collection and Entry Standardized Reports Transports In Transports Out Tools and Support Materials Maternal Transport Data System Development
5 CALIFORNIA ACUTE NEONATAL TRANSPORT ACTIVITY, 2016

6 QUALITY CALIFORNIA NEONATAL TRANSPORT DATA Year 72,423 total records over 11 years, averaging 6,823 per completed year. Total Transports Unknowns Number of Entries per Record 2017 (YTD) 4, , , , , , , , , , ,

7 NEONATAL TRANSPORTS BY FACILITY, 2016
8 CALIFORNIA ACUTE TRANSPORT ACTIVITY BY FACILITY, 2016 Total Acute Transports 6, member facilities 100 facilities reporting acute transports Range 1 to 674, Average 67.1 Transport Volume 38 facilities reporting no transports, 30 facilities with <10 acute transports/year, 38 facilities with acute transports/year, 16 facilities with acute transports/year, 16 facilities with >101 acute transports/year.
9 DESTINATION OF FIRST ACUTE TRANSPORT BY LEVEL OF CARE Receiving Hospital Type Destination of First Transport, 2015 Number (%) Transported In* rounded independently Non-CCS ICNN 58/0.8% Intermediate NICU 82/1.2% Community NICU 2006/30% Regional NICU 4438/67% Total 6584 (100%)
10 VLBW INFANTS MAKE UP ONLY 13% OF ACUTE TRANSPORTS, CONSISTENTLY Acute Neonatal Transports, by Birthweight Category, California, 2016 VLBW (<1,500 grams) 847 LBW + ABW (> 1,500 grams) 5,897 Total 6,710
11 PERINATAL.ORG

12 PERINATAL.ORG Daily hospital updates of Neonatal, ECMO and High Risk Maternity Beds Monthly reports from Regional CPeTS on Update Compliance Quarterly and as needed updates of Contact Information Kaiser integrated into main Northern and Southern California Bed Availability Lists

13 PERINATAL.ORG Direct Referral and Contact Information. Updated quarterly and as needed by hospitals. Accessed by clicking on facility name in main listing.

14 PERINATAL.ORG All materials and support documents accessible at perinatal.org website
15 MATERIALS AND RESOURCES
16 RESOURCES Perinatal.org CPQCC.org Southern California CPeTS: Lisa Bollman: Kevin Van Otterloo: Northern California CPeTS: Te Guerra: Leona Dang-Kilduff:
17 CHANGES IN CPETS DATA COLLECTION FOR 2018 None

18 DATA COLLECTION FORM Data collection is the joint responsibility of the sending and receiving hospitals. Sending Receiving Both

19 ALTERNATE FORM Some items on the CORE CPeTS form were added over the years to improve CPQCC Admit/Discharge form data acquisition of difficult items on transported babies. There are not directly input into the neonatal transport database.

20 FOUND AT WWW. PERINATAL. ORG Form used for primary care facilities to request their transport out data. Form found on perinatal.org website. 20
21 CPQCCREPORT.ORG
22
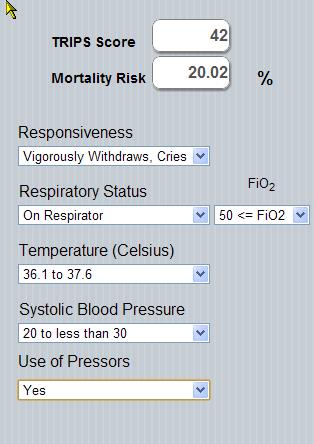
23 0.9 Predicted Probability of Death within 7 Days of NICU Admission Ca. Modified TRIPS
24 REPORT CONTENT
25 NEONATAL QUALITY IMPROVEMENT ISSUES The Neonatal Transport Database was designed to inform quality improvement efforts on the following issues as well as many more. Perceived underutilization of maternal transport; Perceived delay in decision to transport infant; Difficulty in obtaining transport placement/ acceptance; Delay in effecting transport following decision; and Consistent referring facility competency regarding infant stabilization prior to the transport team s arrival, as well as transport team competency.
26 STANDARDIZED REPORTS Statewide Regional Hospital Transport In Transport Out
27 TOOLS & MATERIALS
28 Neonatal Transports OUT Report: Infants born between 01/01/2016 and 12/31/2016 California Perinatal Quality Care Collaborative (CPQCC) and California Perinatal Transport System (CPeTS) REFERRING LOCATION: SAMPLE FACILITY This report is final. Contents: Table 1: Acute Transport OUT Activity, by Birth Weight Table 2: Acute Transport OUT Activity by Transport Type and by Birth Weight Table 3: Acute Transport OUT Activity by Transport Provider and by Birth Weight Table 4: Time from Maternal Admission to Infant Birth Table 5: Mean Time from Maternal Admission to Infant Birth, by Birth Weight Table 6: Median Time from Maternal Admission to Infant Birth, by Birth Weight Table 7: Time from Birth to Referral Table 8: California TRIPS at Referral Table 9: Mean California TRIPS at Referral, by Birth Weight Table 10: Time from Referral to Acceptance Table 11: Time from Acceptance to Transport Team Departure for Referring Hospital Table 12: Time from Acceptance to Transport Team Arrival at Referring Hospital Table 13: Time from Referral to Transport Team Arrival at Referring Hospital Table 14: Mean Change in California TRIPS from Referral to Initial Evaluation, by Birth Weight Table 15: Mean Change in California TRIPS from Initial Evaluation to NICU Admission, by Birth Weight
29 Neonatal Transports IN Report: Infants born between 01/01/2016 and 12/31/2016 California Perinatal Quality Care Collaborative (CPQCC) and California Perinatal Transport System (CPeTS) RECEIVING LOCATION: SAMPLE HOSPITAL This report is final. Contents: Table 1: Acute Transport IN Activity, by Birth Weight Table 2: Acute Transport IN Activity by Transport Type and by Birth Weight Table 3: Acute Transport IN Activity by Transport Provider and by Birth Weight Table 4: Acute Transport IN Activity by Transport Mode and by Birth Weight Table 5: Time from Referral to Initial Eval at Referring Hospital, Emergent Transports Only Table 6: Time from Acceptance to Team Departure for Referring Hospital, Emergent Transports Only Table 7: Time from Transport Team Departure to Initial Evaluation at Referring Hospital Table 8: Time from Transport Team Departure to NICU Admission at Receiving Hospital Table 9: Missing TRIPS by TRIPS Time and Birth Weight Table 10: California TRIPS at Referral Table 11: Mean California TRIPS at Referral, by Birth Weight Table 12: California TRIPS at Initial Evaluation Table 13: Mean California TRIPS at Initial Evaluation, by Birth Weight Table 14: California TRIPS at NICU Admission Table 15: Mean California TRIPS at NICU Admission, by Birth Weight Table 16: Mean Change in California TRIPS from Referral to Initial Evaluation, by Birth Weight Table 17: Mean Change in California TRIPS from Initial Evaluation to NICU Admission, by Birth Weight
30 DATA MINING USING STANDARDIZED REPORTS AS SCREENING TOOLS Variations in practice between your facility and region, or level of care or total CPQCC network Outliers in practice Data that seems unlikely or incorrect Areas where quality improvement activities for the unit are underway Areas where expansion or change in level of care are anticipated Keep in mind small numbers can be misleading. Using multiple years of data can provide clarity in these situations.
31 TRANSPORT IN STANDARDIZED REPORTS Neonatal Transports IN Report: Infants born between 01/01/2016 and 12/31/2016 California Perinatal Quality Care Collaborative (CPQCC) and California Perinatal Transport System (CPeTS) RECEIVING LOCATION: SAMPLE HOSPITAL This report is final. Contents: Table 1: Acute Transport IN Activity, by Birth Weight Table 2: Acute Transport IN Activity by Transport Type and by Birth Weight Table 5: Time from Referral to Initial Eval at Referring Hospital, Emergent Transports Only Table 6: Time from Acceptance to Team Departure for Referring Hospital, Emergent Transports Only Table 8: Time from Transport Team Departure to NICU Admission at Receiving Hospital Table 9: Missing TRIPS by TRIPS Time and Birth Weight Table 11: Mean California TRIPS at Referral, by Birth Weight Table 13: Mean California TRIPS at Initial Evaluation, by Birth Weight Table 15: Mean California TRIPS at NICU Admission, by Birth Weight Table 16: Mean Change in California TRIPS from Referral to Initial Evaluation, by Birth Weight Table 17: Mean Change in California TRIPS from Initial Evaluation to NICU Admission, by Birth Weight
32 VOLUME: IS VOLUME ADEQUATE TO MAINTAIN COMPETENCY? FOR SMALL BABIES, LARGE BABIES? IS BIRTHWEIGHT OF TRANSPORTED IN BABIES APPROPRIATE FOR LEVEL OF CARE? Table 1: Acute Transports IN Activity, by Birth Weight Birth Weight (grams) Center CPQCC Network Community NICUs N % N % N % All Birth Weights , , or less to to 1, ,001 to 1, ,501 to 2, , over 2, , ,
33 TRANSPORT TYPE: IS TRANSPORT TYPE APPROPRIATE? ARE THERE DEFINITION ISSUES? REFER TO NEONATAL TRANSPORT DATA DEFINITIONS MANUAL (PERINATAL.ORG) Birth Weight (grams) All Birth Weights Table 2: Acute Transports IN Activity by Transport Type and by Birth Weight N DR Center CPQCC Network Community NICUs Emergent Urgent Scheduled DR Emergent Urgent Scheduled DR Emergent Urgent Scheduled or less 0 NA NA NA NA to to 1, ,001 to 1, ,501 to 2, over 2, Notes: Transport Type Other is not shown in the table.
34 WHEN OUTLIERS ARE IDENTIFIED, CONSIDER CHART VIEW TO BETTER UNDERSTAND POSSIBLE ISSUES. Table 5: Time from Referral to Initial Evaluation at Referring Hospital, Emergent Transports Only Time Difference Center N % CPQCC Network % Community NICUs % All Infants Transferred In Up to 30 minutes minutes minutes minutes >2-4 hours >4-8 hours >8 hours Mean 5H 20M 2H 8M 2H 15M Median 1H 35M 1H 40M 1H 40M
35 WHAT IS YOUR INTERNAL STANDARD? Table 6: Time from Acceptance to Team Departure for Referring Hospital, Emergent Transports Only Time Difference Center N % CPQCC Network % Community NICUs % All Infants Transferred In Up to 30 minutes minutes hours hours hours > 8 hours Mean 4H 11M 56M 1H 4M Median 40M 40M 45M
36 IS THE REFERRING FACILITY PREPARED WHEN TEAM ARRIVES? IS YOUR TRANSPORT TEAM SPENDING APPROPRIATE AMOUNTS OF TIME TO PROVIDE FOR SAFE, COMPETENT TRANSPORT? DO YOU HAVE ADEQUATE PERSONNEL? Table 8: Time from Departure for Referring Hospital to NICU Admission at Receiving Hospital Time Difference Center N % CPQCC Network % Community NICUs % All Infants Transferred In Up to 30 minutes minutes hours hours hours > 8 hours Mean 2H 44M 4H 7M 2H 36M Median 2H 30M 2H 17M 2H 15M
37 TRIPS SCORES DEMONSTRATE INFANT RISK, MISSING SCORE DATA POINTS SHOULD BE ADDRESSED WITH TEAM AND REFERRAL FACILITY (BP). Table 9: Missing TRIPS by TRIPS Time and Birth Weight Birth Weight (grams) Referral Initial Evaluation NICU Admission N N Missing % N N Missing % N N Missing % All Birth Weights or less 0 0 NA 0 0 NA 0 0 NA 501 to to 1, ,001 to 1, ,501 to 2, over 2, Notes: The TRIPS at Referral is not applicable for DR attendance transports, therefore DR attendance transports are not included in the TRIPS at referral column. The TRIPS at Initial Evaluation is not applicable for self transports, therefore self transports are not included in the TRIPS at initial evaluation column.
38 THE TRIPS SCORE FOR THIS FACILITY FOR VLBW INFANTS AT REFERRAL IS HIGHER THAN TYPICAL FOR CPQCC OR OTHER COMMUNITY NICUS. DOES THE REFERRING FACILITY NEED EDUCATION, TRAINING, SUPPORT FOR RESUSCITATION AND STABILIZATION PRIOR TO TRANSPORT? Birth Weight (grams) Table 11: Mean California TRIPS at Referral, by Birth Weight N Center Mean CPQCC Network Mean Community NICUs Mean All Birth Weights or less 0 NA to to 1, ,001 to 1, ,501 to 2, over 2,
39 WOULD THIS BE A TOPIC TO DISCUSS IN JOINT MORTALITY AND MORBIDITY CONFERENCES? CASE REVIEW? Birth Weight (grams) Table 13: Mean California TRIPS at Initial Evaluation, by Birth Weight N Center Mean CPQCC Network Mean Community NICUs Mean All Birth Weights or less 0 NA to to 1, ,001 to 1, ,501 to 2, over 2,
40 NOTE SUBSTANTIAL IMPROVEMENT IN SCORES BETWEEN INITIAL TEAM EVALUATION AND NICU ADMISSION. THIS MAY BE A SIGN OF GOOD PRACTICE OR OF NEED TO CONSULT/ADVISE CHANGES IN CARE PRIOR TO TEAM ARRIVAL. Birth Weight (grams) Table 15: Mean California TRIPS at NICU Admission, by Birth Weight N Center Mean CPQCC Network Mean Community NICUs Mean All Birth Weights or less 0 NA to to 1, ,001 to 1, ,501 to 2, over 2,
41 QCP OF < 10% INDICATES THAT THERE WAS NO EXCESS DETERIORATION BETWEEN REFERRAL AND INITIAL EVALUATION. Birth Weight (grams) Table 16: Mean change in TRIPS from Referral to Initial Evaluation, by Birth Weight QCP N Infants N Infants Exceeding QCP Center % Infants Exceeding QCP Mean Change CPQCC Network Mean Change Community NICUs Mean Change All Birth Weights or less 9 0 NA NA NA to to 1, NA NA NA ,001 to 1, ,501 to 2, over 2, ***
42 Table 17: Mean change in TRIPS from Initial Evaluation to NICU Admission, by Birth Weight Birth Weight (grams) QCP N Infants N Infants Exceeding QCP Center % Infants Exceeding QCP Mean Change CPQCC Network Mean Change Community NICUs Mean Change All Birth Weights or less 11 0 NA NA NA to to 1, ,001 to 1, ,501 to 2, over 2,
43 TRANSPORT OUT STANDARDIZED REPORTS Neonatal Transports OUT Report: Infants born between 01/01/2016 and 12/31/2016 California Perinatal Quality Care Collaborative (CPQCC) and California Perinatal Transport System (CPeTS) REFERRING LOCATION: SAMPLE FACILITY This report is final. Table 1: Acute Transport OUT Activity, by Birth Weight Table 4: Time from Maternal Admission to Infant Birth Table 5: Mean Time from Maternal Admission to Infant Birth, by Birth Weight Table 8: California TRIPS at Referral Table 9: Mean California TRIPS at Referral, by Birth Weight Table 13: Time from Referral to Transport Team Arrival at Referring Hospital
44 VOLUME: THIS DEMONSTRATES APPROPRIATE CASE SELECTION AND/OR MATERNAL TRANSPORT. TOTAL TRANSPORT RATE 1.68/1,00 LBVS 2.77/1,000 LB IN CALIFORNIA. VLBW TRANSPORT RATE IN FACILITY UNABLE TO PROVIDE ONGOING CARE: 0.2/1,000 VS. 0.4/1,000 Birth Weight (grams) Births N Table 1: Acute Transport OUT Activity, by Birth Weight Center Transports N % Transports Originating From... LA-San Gabriel-Inland Orange Primary Care Hospitals Births Transports % N N California Primary Care Hospitals Births Transports % N N All 1, , ,087 2, or less 0 0 NA to NA to 1, NA ,001 to 1, ,501 to 2, , over 2,500 1, , ,504 1, The Births columns are based on birth records captured in real-time through AVSS.
45 Time Difference Table 4: Time from Maternal Admission to Infant Birth Center N % LA-San Gabriel-Inland Orange Primary Care Hospitals % California Primary Care Hospitals % All Infants Transferred Out Post Birth Admission hours >2-4 hours >4-6 hours >6-12 hours >12-36 hours >36 hours Mean 9H 14M 16H 13M 17H 51M Median 7H 1M 7H 23M 5H 43M
46 OF THE 3 INFANTS BORN WEIGHING < 1,500 GRAMS, THE MEAN TIME OF MATERNAL ADMISSION TO BIRTH WAS 3 HOURS, 16 MINUTES PROBABLY NOT SUFFICIENT TO ACCOMPLISH AND MATERNAL TRANSPORT. ONLY 12 OF THE 113 INFANTS BORN WEIGHING BETWEEN 1,500 AND 2,500 GRAMS WERE TRANSPORTED, MAKING IT DIFFICULT TO SAY WHICH MOTHERS MAY HAVE BENEFITTED FROM TRANSPORT. Birth Weight (grams) Table 5: Mean Time from Maternal Admission to Infant Birth, by Birth Weight N Center Mean LA-San Gabriel- Inland Orange Primary Care Hospitals Mean California Primary Care Hospitals Mean All 28 9H 14M 16H 13M 17H 51M 500 or less 0 NA NA 3H 2M 501 to NA 2D 18H 37M 18H 54M 751 to 1,000 0 NA 7H 46M 4H 22M 1,001 to 1, H 16M 1D 1H 26M 15H 57M 1,501 to 2, H 41M 20H 29M 16H 15M over 2, H 7M 12H 50M 19H 1M
47 AT FIRST GLANCE IT APPEARS THAT ALL INFANTS IN THIS FACILITY HAD TRIPS SCORES WITH THE LOWEST PREDICTED MORTALITY IN THE FIRST 7 DAYS FOLLOWING TRANSPORT.. TRIPS at Referral Center N % Table 8: California TRIPS at Referral LA-San Gabriel-Inland Orange Primary Care Hospitals % California Primary Care Hospitals % All Scores or less / Prob. < 1% to 31 / Prob. < 5% to 38 / Prob. < 10% 39 to 49 / Prob. < 25% >=50 / Prob. >= 25% Mean Score Median Score Notes: For each TRIPS score range, the associated estimated risk of death within 7 days of transfer is displayed in the first table column.
48 UNTIL WE NOTE THAT THE VLBW INFANTS HAD MISSING COMPONENTS OF THE TRIPS SCORE AND WE NOT ABLE TO BE CALCULATED. THIS SHOULD BE CONSIDERED A QUALITY IMPROVEMENT OPPORTUNITY. Birth Weight (grams) Table 9: Mean California TRIPS at Referral, by Birth Weight N Center Mean LA-San Gabriel-Inland Orange Primary Care Hospitals Mean California Primary Care Hospitals Mean All or less 0 NA NA to NA to 1,000 0 NA NA ,001 to 1, ,501 to 2, over 2,
49 URBAN FACILITY WITH RECEIVING NICU LESS THAN 5 MILES FROM REFERRING FACILITY. Time Difference Table 13: Time from Referral to Transport Team Arrival at Referring Hospital Center N % LA-San Gabriel-Inland Orange Primary Care Hospitals % California Primary Care Hospitals % All Infants Transferred Out minutes minutes minutes minutes >2 hours Mean 1H 22M 2H 19M 2H 42M Median 1H 17M 1H 15M 1H 45M
50 MATERNAL LEVELS OF CARE QUALITY IMPROVEMENT ISSUES Mothers who would have benefitted from transport but did not receive it.
51 THANK YOU FOR YOUR TIME AND COMMITMENT!
CPQCC. California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS JEFFREY B. GOULD, MD, MPH
 CPQCC California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS 1997-2015 JEFFREY B. GOULD, MD, MPH DIRECTOR, PERINATAL EPIDEMIOLOGY AND OUTCOMES UNIT DEPARTMENT OF PEDIATRICS STANFORD
CPQCC California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS 1997-2015 JEFFREY B. GOULD, MD, MPH DIRECTOR, PERINATAL EPIDEMIOLOGY AND OUTCOMES UNIT DEPARTMENT OF PEDIATRICS STANFORD
HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS
 HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS 2013 BORN INFANT RECORDS 2015 BORN INFANT STANDARD VISIT #1 FOR ALL EXPECTED 2016 BORN INFANT REFERRAL/REGISTRATIONS
HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS 2013 BORN INFANT RECORDS 2015 BORN INFANT STANDARD VISIT #1 FOR ALL EXPECTED 2016 BORN INFANT REFERRAL/REGISTRATIONS
CPQCC Data Center. CPQCC Satellite NICUs Version 16.1, April 28,
 CPQCC Data Center CPQCC s Version 16.1, April 28, 2016-1 - Dear CPQCC Participant, You are receiving this memo because you are one of the nine s participating in CPQCC. We are addressing the special circumstances
CPQCC Data Center CPQCC s Version 16.1, April 28, 2016-1 - Dear CPQCC Participant, You are receiving this memo because you are one of the nine s participating in CPQCC. We are addressing the special circumstances
Indicator. unit. raw # rank. HP2010 Goal
 Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services
 CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services Name of Facility: Our Lady of Lourdes Medical CN# FR 140701-04-01 Center Name of Applicant:
CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services Name of Facility: Our Lady of Lourdes Medical CN# FR 140701-04-01 Center Name of Applicant:
Lillian R. Blackmon, MD. Perinatal Regionalization Meeting October 28, 2009 Washington, DC
 Regional Perinatal Care: What do we call the components? Lillian R. Blackmon, MD Perinatal Regionalization Meeting October 28, 2009 Washington, DC What? Regionalization Organization of health care resources
Regional Perinatal Care: What do we call the components? Lillian R. Blackmon, MD Perinatal Regionalization Meeting October 28, 2009 Washington, DC What? Regionalization Organization of health care resources
Perinatal Care in the Community
 Perinatal Care in the Community Elizabeth Betty Jordan DNSc, RNC Assistant Professor Johns Hopkins School of Nursing INTRODUCTION 2 INTRODUCTION Maryland s s preterm birth rate :11.4%/Baltimore City :
Perinatal Care in the Community Elizabeth Betty Jordan DNSc, RNC Assistant Professor Johns Hopkins School of Nursing INTRODUCTION 2 INTRODUCTION Maryland s s preterm birth rate :11.4%/Baltimore City :
High Risk Infant Follow Up
 http://www.dhcs.ca.gov/services/ccs/pages/hrif.aspx Page 1 of 9 California Children's Services Contact Us Career Opportunities He Search Home > Services > California Children's Services > Select Language
http://www.dhcs.ca.gov/services/ccs/pages/hrif.aspx Page 1 of 9 California Children's Services Contact Us Career Opportunities He Search Home > Services > California Children's Services > Select Language
Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014
 Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014") + Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
+ Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
Extrauterine Growth Restriction in a Neonatal Intensive Care Unit in Argentina Catherine R. Coverston, Lisa Roos
 Extrauterine Growth Restriction in a Neonatal Intensive Care Unit in Argentina Catherine R. Coverston, Lisa Roos Purpose: To determine the incidence and attributes of extrauterine growth restriction (EGR)
Extrauterine Growth Restriction in a Neonatal Intensive Care Unit in Argentina Catherine R. Coverston, Lisa Roos Purpose: To determine the incidence and attributes of extrauterine growth restriction (EGR)
Data Collection and Reporting for MOM Initiative. Karen Fugate MSN RNC-NIC, CPHQ
 Data Collection and Reporting for MOM Initiative Karen Fugate MSN RNC-NIC, CPHQ Presentation Objectives IRB and Data Use Agreements Baseline Data Collection and Submission Prospective Data Submission Sample
Data Collection and Reporting for MOM Initiative Karen Fugate MSN RNC-NIC, CPHQ Presentation Objectives IRB and Data Use Agreements Baseline Data Collection and Submission Prospective Data Submission Sample
Case Study. Check-List for Assessing Economic Evaluations (Drummond, Chap. 3) Sample Critical Appraisal of
 Sample Critical Appraisal of") Case Study Work in groups At most 7-8 page, double-spaced, typed critical appraisal of a published CEA article Start with a 1-2 page summary of the article, answer the following ten questions, and then
Case Study Work in groups At most 7-8 page, double-spaced, typed critical appraisal of a published CEA article Start with a 1-2 page summary of the article, answer the following ten questions, and then
Agenda Information Item Memo
 Agenda Information Item Memo April 20, 2018 TO: FROM: Board of Trustees Ishwari Venkataraman/ VP Strategy and Business Planning Donna Carey/ Interim Chair, Department of Pediatrics SUBJECT: Agenda Item:
Agenda Information Item Memo April 20, 2018 TO: FROM: Board of Trustees Ishwari Venkataraman/ VP Strategy and Business Planning Donna Carey/ Interim Chair, Department of Pediatrics SUBJECT: Agenda Item:
Objective. Disclosures. L & D and Discharge Nurse Liaisons: A COLLABORATIVE APPROACH TO INCREASING FAMILY SATISFACTION IN THE NICU 4/12/2016
 L & D and Discharge Nurse Liaisons: A COLLABORATIVE APPROACH TO INCREASING FAMILY SATISFACTION IN THE NICU Arlina Carias, BPS, BSN, RN Francesca M. Leo, BSN, RN, IBCLC, CLC Nursing Care Coordinators NewYork
L & D and Discharge Nurse Liaisons: A COLLABORATIVE APPROACH TO INCREASING FAMILY SATISFACTION IN THE NICU Arlina Carias, BPS, BSN, RN Francesca M. Leo, BSN, RN, IBCLC, CLC Nursing Care Coordinators NewYork
Risky Business. Conference for Health Professionals. Register now at. Managing the Escalating Complexity of Maternal and Neonatal Care
 1050 Sansome St., 4th Floor San Francsico, CA 94111 NON-PROFIT ORG US POSTAGE PAID San Francisco, CA PERMIT NO 9506 Conference for Health Professionals Risky Business Managing the Escalating Complexity
1050 Sansome St., 4th Floor San Francsico, CA 94111 NON-PROFIT ORG US POSTAGE PAID San Francisco, CA PERMIT NO 9506 Conference for Health Professionals Risky Business Managing the Escalating Complexity
Maryland Patient Safety Center s Call for Solutions 2017
 Maryland Patient Safety Center s Call for Solutions 7 The Neonatal Intensive Care Unit at The Herman & Walter Samuelson Children s Hospital at Sinai Hospital of Baltimore Drawing Placental Blood for Admission
Maryland Patient Safety Center s Call for Solutions 7 The Neonatal Intensive Care Unit at The Herman & Walter Samuelson Children s Hospital at Sinai Hospital of Baltimore Drawing Placental Blood for Admission
Neonatal Abstinence Syndrome Surveillance in West Virginia
 Neonatal Abstinence Syndrome Surveillance in West Virginia Christina Mullins, Director Office of Maternal, Child and Family Health Bureau for Public Health West Virginia Department of Health and Human
Neonatal Abstinence Syndrome Surveillance in West Virginia Christina Mullins, Director Office of Maternal, Child and Family Health Bureau for Public Health West Virginia Department of Health and Human
POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE
 POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE Our network includes 1200+ centers across 30+ countries, collecting critical information on 2.5+ million infants and 72.5+ million patient days. 1 VERMONT
POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE Our network includes 1200+ centers across 30+ countries, collecting critical information on 2.5+ million infants and 72.5+ million patient days. 1 VERMONT
APRIL HEALTHY START INITIATIVE
 APRIL 2017 93.926 HEALTHY START INITIATIVE State Project/Program: HEALTHY START BABY LOVE PLUS COMMUNITIES U. S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Federal Authorization: PHS Title III, Section 301,
APRIL 2017 93.926 HEALTHY START INITIATIVE State Project/Program: HEALTHY START BABY LOVE PLUS COMMUNITIES U. S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Federal Authorization: PHS Title III, Section 301,
CDC s Maternity Practices in Infant and Care (mpinc) Survey. Using mpinc Data to Support
 Survey. Using mpinc Data to Support") CDC s Maternity Practices in Infant and Care (mpinc) Survey Nutrition Efforts in California Hospitals Carina Saraiva, MPH Research Scientist California Department of Public Health, Center for Family Health
CDC s Maternity Practices in Infant and Care (mpinc) Survey Nutrition Efforts in California Hospitals Carina Saraiva, MPH Research Scientist California Department of Public Health, Center for Family Health
Project Title: Establishing Retinopathy of Pre-maturity (ROP) Screening and Treatment Services in Bangladesh
 Screening and Treatment Services in Bangladesh") Project Title: Establishing Retinopathy of Pre-maturity (ROP) Screening and Treatment Services in Bangladesh 1 Summary 1.1 Project Goal: To reduce avoidable childhood blindness due to Retinopathy of Pre-maturity
Project Title: Establishing Retinopathy of Pre-maturity (ROP) Screening and Treatment Services in Bangladesh 1 Summary 1.1 Project Goal: To reduce avoidable childhood blindness due to Retinopathy of Pre-maturity
Baby-MONITOR. Composite Measure of NICU Quality
 Baby-MONITOR Composite Measure of NICU Quality By The Numbers Working across the continuum of care 500K 17K 140 7K 9K BIRTHS NICU ADMITS MEMBER HOSPITALS ACUTE NEONATAL TRANSPORTS HIGH-RISK INFANTS REGISTERED
Baby-MONITOR Composite Measure of NICU Quality By The Numbers Working across the continuum of care 500K 17K 140 7K 9K BIRTHS NICU ADMITS MEMBER HOSPITALS ACUTE NEONATAL TRANSPORTS HIGH-RISK INFANTS REGISTERED
KANGAROO MOTHER CARE PROGRESS MONITORING TOOL (Version 4)
") MRC Research Unit for Maternal and Infant Health Care Strategies, 2002, 2004, 2007, 2009 University of Pretoria and Kalafong Hospital PO Box 667, Pretoria 0001, South Africa KANGAROO MOTHER CARE PROGRESS
MRC Research Unit for Maternal and Infant Health Care Strategies, 2002, 2004, 2007, 2009 University of Pretoria and Kalafong Hospital PO Box 667, Pretoria 0001, South Africa KANGAROO MOTHER CARE PROGRESS
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative. May 4, :00-2:00pm ET
 Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
Neonatal Rules Webinar
 Neonatal Rules Webinar Today is our Kick-off for the Neonatal Designation Program! Power Point Presentation which will be mailed out to participants and RACs. Questions will be answered at the end of the
Neonatal Rules Webinar Today is our Kick-off for the Neonatal Designation Program! Power Point Presentation which will be mailed out to participants and RACs. Questions will be answered at the end of the
Progress on the AAP Quality Measures Task Force Town Hall Dialogue!
 Progress on the AAP Quality Measures Task Force Town Hall Dialogue! John A. F. Zupancic MD Associate Professor of Pediatrics, Harvard Medical School Neonatologist Beth Israel Deaconess Medical Center Boston,
Progress on the AAP Quality Measures Task Force Town Hall Dialogue! John A. F. Zupancic MD Associate Professor of Pediatrics, Harvard Medical School Neonatologist Beth Israel Deaconess Medical Center Boston,
APPENDIX D INSTRUCTIONS FOR COMPLETION OF CERTIFICATE OF NEED APPLICATION FOR DESIGNATION AS A PERINATAL FACILITY SECTION I. GENERAL REQUIREMENTS
 APPENDIX D INSTRUCTIONS FOR COMPLETION OF CERTIFICATE OF NEED APPLICATION FOR DESIGNATION AS A PERINATAL FACILITY SECTION I. GENERAL REQUIREMENTS 1. CERTIFICATE OF NEED A. PRE-SUBMISSION Prior to the preparation
APPENDIX D INSTRUCTIONS FOR COMPLETION OF CERTIFICATE OF NEED APPLICATION FOR DESIGNATION AS A PERINATAL FACILITY SECTION I. GENERAL REQUIREMENTS 1. CERTIFICATE OF NEED A. PRE-SUBMISSION Prior to the preparation
Perinatal Services Guidelines for Care: A Compilation of Current Standards
 2011 Perinatal Services Guidelines for Care: A Compilation of Current Standards 2011 Regional Perinatal Programs of California Supported in part through contracts with the State of California, Department
2011 Perinatal Services Guidelines for Care: A Compilation of Current Standards 2011 Regional Perinatal Programs of California Supported in part through contracts with the State of California, Department
The Family Health Outcomes Project: Overview and Orientation. The Story of FHOP. Webinar Objectives. Dr. Gerry Oliva
 The Family Health Outcomes Project: Overview and Orientation Gerry Oliva MD, MPH Jennifer Rienks PhD Katie Gillespie MA, MPH Family Health Outcomes Project November, 2010 The Story of FHOP Featuring an
The Family Health Outcomes Project: Overview and Orientation Gerry Oliva MD, MPH Jennifer Rienks PhD Katie Gillespie MA, MPH Family Health Outcomes Project November, 2010 The Story of FHOP Featuring an
2018 Hospital Pay For Performance (P4P) Program Guide. Contact:
 Program Guide. Contact:") 2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
XIII. Health Statistics and Research. Kathy C. Trawick, EdD, RHIA, FAHIMA
 XIII. Health Statistics and Research Kathy C. Trawick, EdD, RHIA, FAHIMA Health Statistics and Research 369 As noted in the main Introduction section, you will be able to access some statistical formulas
XIII. Health Statistics and Research Kathy C. Trawick, EdD, RHIA, FAHIMA Health Statistics and Research 369 As noted in the main Introduction section, you will be able to access some statistical formulas
Early Childhood: Interactions, Environment, and Culture
 Early Childhood: Interactions, Environment, and Culture The topic Chairs at the PACRIM 2014 Early Childhood Strand are looking for presentation proposals pertaining to the following topic areas: Neonatal
Early Childhood: Interactions, Environment, and Culture The topic Chairs at the PACRIM 2014 Early Childhood Strand are looking for presentation proposals pertaining to the following topic areas: Neonatal
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
1 A similar approach is described by Karp (2003) 2 National center for Health Statistics (NCHS)
 2 National center for Health Statistics (NCHS)") Creating Birth Data Quality Reports: Identifying hospitals that submit high volumes of invalid data using PROC REPORT and ODS Thaer Baroud, John Senner, PhD, Paul Johnson, Little Rock, Arkansas ABSTRACT
Creating Birth Data Quality Reports: Identifying hospitals that submit high volumes of invalid data using PROC REPORT and ODS Thaer Baroud, John Senner, PhD, Paul Johnson, Little Rock, Arkansas ABSTRACT
Retrospective Study of Risks of Infant Skin Breakdown using the Seton Infant Skin Risk Assessment tool
 Retrospective Study of Risks of Infant Skin Breakdown using the Seton Infant Skin Risk Assessment tool Deborah A. Vance, MSN, RN; Lead Investigator, Neonatal Intensive Care Unit, Seton Medical Center at
Retrospective Study of Risks of Infant Skin Breakdown using the Seton Infant Skin Risk Assessment tool Deborah A. Vance, MSN, RN; Lead Investigator, Neonatal Intensive Care Unit, Seton Medical Center at
2110 Pediatric Newborn Care
 Course: Pediatric Newborn Care Course Number: PED 2110 Department: Faculty Coordinator: Assistant Faculty Coordinators: Pediatrics Kathryn Johnson, MD N/A UTSW Education Coordinator Contact: Anthony Lee
Course: Pediatric Newborn Care Course Number: PED 2110 Department: Faculty Coordinator: Assistant Faculty Coordinators: Pediatrics Kathryn Johnson, MD N/A UTSW Education Coordinator Contact: Anthony Lee
Chan Man Yi, NC (Neonatal Care) Dept. of Paed. & A.M., PMH 16 May 2017
 Dept. of Paed. & A.M., PMH 16 May 2017") The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
Sepsis in the NICU and Interventions to Improve Care
 Sepsis in the NICU and Interventions to Improve Care Joseph El Khoury, MD Children s Hospital of Richmond at VCU Virginia Neonatal Perinatal Collaborative Meeting May 12 th, 2017 Significance of Sepsis
Sepsis in the NICU and Interventions to Improve Care Joseph El Khoury, MD Children s Hospital of Richmond at VCU Virginia Neonatal Perinatal Collaborative Meeting May 12 th, 2017 Significance of Sepsis
Data Arm Data Center Develop and maintain a responsive, real time, risk adjusted perinatal data system.
 The California Perinatal Quality Care Collaborative is committed to improving the quality of care to California s mothers and our most vulnerable infants. Data Arm Data Center Develop and maintain a responsive,
The California Perinatal Quality Care Collaborative is committed to improving the quality of care to California s mothers and our most vulnerable infants. Data Arm Data Center Develop and maintain a responsive,
EP7f, CN III OB Hemorrhage.pdf OBSTETRIC HEMORRHAGE. Amelia Indig RN Clinical Nurse III Candidate December 17, 2009
 OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
Community Health Needs Assessment. Implementation Plan FISCA L Y E AR
 Community Health Needs Assessment Implementation Plan FISCA L Y E AR 2 0 1 5-2 0 1 8 Table of Contents: I. Background 1 II. Areas of Priority 2 a. Preventive Care and Chronic Conditions b. Community Health
Community Health Needs Assessment Implementation Plan FISCA L Y E AR 2 0 1 5-2 0 1 8 Table of Contents: I. Background 1 II. Areas of Priority 2 a. Preventive Care and Chronic Conditions b. Community Health
PATIENT EVACUATION PLANNING AND RESPONSE FORM FOR SENDING (EVACUATING) HOSPITALS
 HOSPITALS") PATIENT EVACUATION PLANNING AND RESPONSE FORM FOR SENDING (EVACUATING) HOSPITALS Instructions: This form can be used to planning for and respond to hospital evacuations. Only PURPLE cells can be edited.
PATIENT EVACUATION PLANNING AND RESPONSE FORM FOR SENDING (EVACUATING) HOSPITALS Instructions: This form can be used to planning for and respond to hospital evacuations. Only PURPLE cells can be edited.
Breastfeeding Initiatives in Estonia. Anneli Sammel, MA National Institute for Health Development
 Breastfeeding Initiatives in Estonia Anneli Sammel, MA National Institute for Health Development 28.10.2015 Topics of the presenation National policy farework Monitoring The Role of Health Care (Primary
Breastfeeding Initiatives in Estonia Anneli Sammel, MA National Institute for Health Development 28.10.2015 Topics of the presenation National policy farework Monitoring The Role of Health Care (Primary
Saving Every Woman, Every Newborn and Every Child
 Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
The Mommies Program An Integrated Model of Care. Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist
 The Mommies Program An Integrated Model of Care Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist Objectives Discuss the effects of opioid epidemic on pregnant women Recognize the importance
The Mommies Program An Integrated Model of Care Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist Objectives Discuss the effects of opioid epidemic on pregnant women Recognize the importance
Welcome! Neonatal Abstinence Syndrome Project Action Period Call
 Welcome! Neonatal Abstinence Syndrome Project Action Period Call Ohio Perinatal Quality Collaborative April 15, 2014 Please don t put us on HOLD! If you need to step away: Use the MUTE button on your phone
Welcome! Neonatal Abstinence Syndrome Project Action Period Call Ohio Perinatal Quality Collaborative April 15, 2014 Please don t put us on HOLD! If you need to step away: Use the MUTE button on your phone
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS
 SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
Medicaid Policy Changes and its Detrimental Effects on Neonatal Reimbursement and Care
 Fall 2015 Medicaid Policy Changes and its Detrimental Effects on Neonatal Reimbursement and Care John A. Kohler, Sr., MD 1, Ronald N. Goldberg, MD 1, and David T. Tanaka, MD 1 1 Division of Neonatal-Perinatal
Fall 2015 Medicaid Policy Changes and its Detrimental Effects on Neonatal Reimbursement and Care John A. Kohler, Sr., MD 1, Ronald N. Goldberg, MD 1, and David T. Tanaka, MD 1 1 Division of Neonatal-Perinatal
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
Reducing the risks for mother and baby
 2015 Swanman Perinatal Conference Reducing the risks for mother and baby May 7 8, 2015 Legacy Women s Services Course description The 2015 Swanman Perinatal Conference will present two days of lectures
2015 Swanman Perinatal Conference Reducing the risks for mother and baby May 7 8, 2015 Legacy Women s Services Course description The 2015 Swanman Perinatal Conference will present two days of lectures
Optimal Pregnancy Outcomes for Women on Medicaid The Optima Partners in Pregnancy Program
 Optimal Pregnancy Outcomes for Women on Medicaid The Optima Partners in Pregnancy Program The Disease Management Colloquium Karen Bray, PhD(c), RN, CDE Nancy Jallo, RNC, MSN, CS, FNP June 22, 2005 Overview
Optimal Pregnancy Outcomes for Women on Medicaid The Optima Partners in Pregnancy Program The Disease Management Colloquium Karen Bray, PhD(c), RN, CDE Nancy Jallo, RNC, MSN, CS, FNP June 22, 2005 Overview
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
FINAL REPORT FOR DINING FOR WOMEN
 Organization Information a. Organization Name: One Heart World-Wide b. Program Title: Implementing a Network of Safety around mothers and newborns in Western Nepal c. Grant Amount: $50,000 USD d. Contact:
Organization Information a. Organization Name: One Heart World-Wide b. Program Title: Implementing a Network of Safety around mothers and newborns in Western Nepal c. Grant Amount: $50,000 USD d. Contact:
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM
 SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM EFFECTIVE DATE: REVISED DATE: STANDARD TYPE:, 4/95 1/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS PROVIDING NURSING
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM EFFECTIVE DATE: REVISED DATE: STANDARD TYPE:, 4/95 1/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS PROVIDING NURSING
San Francisco Transitional Care Program
 San Francisco Transitional Care Program A presentation for Make History at California Readmissions Summit Avoid Readmissions through Collaboration May 6, 2014 at Oakland Scottish Rite Center Presenters
San Francisco Transitional Care Program A presentation for Make History at California Readmissions Summit Avoid Readmissions through Collaboration May 6, 2014 at Oakland Scottish Rite Center Presenters
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
Perinatal Designation Matrix 3/21/07
 Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
Assignment 2: KMC Global: Ghana
 Assignment 2: KMC Global: Ghana Ghana o Household About 1/3 are women 40% of Ghanaian population is under age 15 Families often live with extended family members Tradition of either move in to live with
Assignment 2: KMC Global: Ghana Ghana o Household About 1/3 are women 40% of Ghanaian population is under age 15 Families often live with extended family members Tradition of either move in to live with
Texas Department of State Health Services and March of Dimes Austin, Texas January 6-7, 2011
 Texas Department of State Health Services and March of Dimes Austin, Texas January 6-7, 2011 Mario Drummonds, MS, LCSW, MBA CEO, Northern Manhattan Perinatal Partnership, Inc. Strategies are choices Strategies
Texas Department of State Health Services and March of Dimes Austin, Texas January 6-7, 2011 Mario Drummonds, MS, LCSW, MBA CEO, Northern Manhattan Perinatal Partnership, Inc. Strategies are choices Strategies
2/1/2016. LACTATION CARE MAP at CHOC Children s Neonatal Intensive Care Unit. Disclosures. Crystal Deming has nothing to disclose.
 LACTATION CARE MAP at CHOC Children s Neonatal Intensive Care Unit Disclosures Crystal Deming has nothing to disclose. Cindy Baker-Fox is an adjunct instructor for the University of California San Diego
LACTATION CARE MAP at CHOC Children s Neonatal Intensive Care Unit Disclosures Crystal Deming has nothing to disclose. Cindy Baker-Fox is an adjunct instructor for the University of California San Diego
Critical Care Services Benefits to Change for the CSHCN Services Program
 Critical Care Services Benefits to Change for the CSHCN Services Program Information posted July 14, 2008 Effective for dates of service on or after September 1, 2008, the benefit criteria for critical
Critical Care Services Benefits to Change for the CSHCN Services Program Information posted July 14, 2008 Effective for dates of service on or after September 1, 2008, the benefit criteria for critical
ALIGNING STATE AND LOCAL HEALTH DEPARTMENTS TO IMPROVE MATERNAL AND CHILD HEALTH
 ALIGNING STATE AND LOCAL HEALTH DEPARTMENTS TO IMPROVE MATERNAL AND CHILD HEALTH National membership organization of city and county health departments' maternal and child health (MCH) programs and leaders
ALIGNING STATE AND LOCAL HEALTH DEPARTMENTS TO IMPROVE MATERNAL AND CHILD HEALTH National membership organization of city and county health departments' maternal and child health (MCH) programs and leaders
AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS
 CHAPTER VII AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS This chapter includes background information and descriptions of the following tools FHOP has developed to assist local health jurisdictions
CHAPTER VII AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS This chapter includes background information and descriptions of the following tools FHOP has developed to assist local health jurisdictions
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience.
 Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission
 Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission Seth Freedman University of Michigan and Indiana University October 7, 2011 Abstract The supply of
Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission Seth Freedman University of Michigan and Indiana University October 7, 2011 Abstract The supply of
NEARBY CARE POPULATION HEALTH
 NEARBY EXPERTISE PEDIATRIC ACTIVE CARE POPULATION HEALTH CREATING NEW VALUE IN HEALTH CARE MILLER CHILDREN S & WOMEN S HOSPITAL LONG BEACH With specialized pediatric care for children and young adults,
NEARBY EXPERTISE PEDIATRIC ACTIVE CARE POPULATION HEALTH CREATING NEW VALUE IN HEALTH CARE MILLER CHILDREN S & WOMEN S HOSPITAL LONG BEACH With specialized pediatric care for children and young adults,
Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport
 Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport Transport Service Facilities 1. Access to 24/7 Cheshire and Merseyside Perinatal Cot Bureau and Data Management
Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport Transport Service Facilities 1. Access to 24/7 Cheshire and Merseyside Perinatal Cot Bureau and Data Management
New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration
: Improving Perinatal Health through Partnerships and Collaboration") New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration Marilyn Kacica, MD, MPH Kristen Farina, MS New York State Department of Health
New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration Marilyn Kacica, MD, MPH Kristen Farina, MS New York State Department of Health
Empowering Parents of High Risk Infants in the ICU (Intensive Care Unit) Kellie Kainer, MSN, RNC
 Kellie Kainer, MSN, RNC") Empowering Parents of High Risk Infants in the ICU (Intensive Care Unit) Kellie Kainer, MSN, RNC Objectives 1) Discuss the why behind the development of the Parenting your High Risk Infant class 2) Discuss
Empowering Parents of High Risk Infants in the ICU (Intensive Care Unit) Kellie Kainer, MSN, RNC Objectives 1) Discuss the why behind the development of the Parenting your High Risk Infant class 2) Discuss
93% client retention rate
 Cover Page Partner with a leading provider of children s services. For over 30 years, Sheridan has been a leading provider of children s services, specializing in acute inpatient care and treatment of
Cover Page Partner with a leading provider of children s services. For over 30 years, Sheridan has been a leading provider of children s services, specializing in acute inpatient care and treatment of
Friday: April 4, 2014 Rutgers University Inn and Conference Center 178 Ryders Lane, New Brunswick, NJ
 Updates on Best Practices for Managing Obstetrical Emergencies Presented by AWHONN New Jersey Section Association of Women s Health, Obstetric and Neonatal Nurses Friday: April 4, 2014 Rutgers University
Updates on Best Practices for Managing Obstetrical Emergencies Presented by AWHONN New Jersey Section Association of Women s Health, Obstetric and Neonatal Nurses Friday: April 4, 2014 Rutgers University
Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission
 Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission Seth Freedman University of Michigan and Indiana University Preliminary: Please Do Not Cite or Circulate
Capacity and Utilization in Health Care: The Effect of Empty Beds on Neonatal Intensive Care Admission Seth Freedman University of Michigan and Indiana University Preliminary: Please Do Not Cite or Circulate
Standards for competence for registered midwives
 Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
CoIIN: Using the Science of Quality Improvement and Collaborative Learning to Reduce Infant Mortality
 CoIIN: Using the Science of Quality Improvement and Collaborative Learning to Reduce Infant Mortality NGA s Learning Network Conference on Improving Birth Outcomes May 17, 2013 David S. de la Cruz, PhD,
CoIIN: Using the Science of Quality Improvement and Collaborative Learning to Reduce Infant Mortality NGA s Learning Network Conference on Improving Birth Outcomes May 17, 2013 David S. de la Cruz, PhD,
EXHIBIT A Performance Matrix
 EXHIBIT A Performance Matrix Contract Number: 07499 Agency Name: County of Los Angeles Department of Public Health Project Name: Black Infant Health Program Project Length: 12 months Contract Period: July
EXHIBIT A Performance Matrix Contract Number: 07499 Agency Name: County of Los Angeles Department of Public Health Project Name: Black Infant Health Program Project Length: 12 months Contract Period: July
Implementing a Statewide Maternal Transport Nurse Course: An Academic and Clinical Partnership
 Implementing a Statewide Maternal Transport Nurse Course: An Academic and Clinical Partnership Margaret-Rose Agostino, DNP, MSW, RN-BC, CNE, IBCLC 9 th National Doctors of Nursing Practice Conference Baltimore,
Implementing a Statewide Maternal Transport Nurse Course: An Academic and Clinical Partnership Margaret-Rose Agostino, DNP, MSW, RN-BC, CNE, IBCLC 9 th National Doctors of Nursing Practice Conference Baltimore,
Prospectus Summary Brief: NICU Communication Improvement
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 Prospectus
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 Prospectus
Standardizing Care for Perinatal Patient Safety
 Standardizing Care for Perinatal Patient Safety Mercy Medical Center Clinton, Iowa Colleen Meggers RNC, BSN, MHA Director of Maternal Child Services Laura Gassman RNC, BSN, MHA Supervisor/ Perinatal Safety
Standardizing Care for Perinatal Patient Safety Mercy Medical Center Clinton, Iowa Colleen Meggers RNC, BSN, MHA Director of Maternal Child Services Laura Gassman RNC, BSN, MHA Supervisor/ Perinatal Safety
The Honorable Diana Dooley Secretary, California Health and Human Services Agency 1600 Ninth Street, Room 460 Sacramento, CA 95814
 Sutter Health Sutter Medical Center, Sacramento We Plus You 5151 F Street Sacramento, CA 95819 916.733.1038 April 14, 2015 The Honorable Diana Dooley Secretary, California Health and Human Services Agency
Sutter Health Sutter Medical Center, Sacramento We Plus You 5151 F Street Sacramento, CA 95819 916.733.1038 April 14, 2015 The Honorable Diana Dooley Secretary, California Health and Human Services Agency
Indiana Perinatal Hospital Standards
 Indiana Perinatal Hospital Standards 2013 Indiana Perinatal Hospital Summit Indiana Perinatal Quality Improvement Collaborative Mission To improve maternal and perinatal outcomes in Indiana through a collaborative
Indiana Perinatal Hospital Standards 2013 Indiana Perinatal Hospital Summit Indiana Perinatal Quality Improvement Collaborative Mission To improve maternal and perinatal outcomes in Indiana through a collaborative
VICTORIAN PUBLIC HOSPITALS NEONATAL FELLOW POSITIONS REFEREE ASSESSMENT FORM
 VICTORIAN PUBLIC HOSPITALS NEONATAL FELLOW POSITIONS REFEREE ASSESSMENT FORM INSTRUCTIONS TO APPLICANT: 1. Three (3) Referee Assessments are required. At least two (2) should be from Consultants. Registrars
VICTORIAN PUBLIC HOSPITALS NEONATAL FELLOW POSITIONS REFEREE ASSESSMENT FORM INSTRUCTIONS TO APPLICANT: 1. Three (3) Referee Assessments are required. At least two (2) should be from Consultants. Registrars
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE NEONATAL TRANSPORT TEAM
 UNIT: SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE NEONATAL TRANSPORT TEAM STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: 11/93 3/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS
UNIT: SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE NEONATAL TRANSPORT TEAM STANDARD #: EFFECTIVE DATE: REVISED DATE: STANDARD TYPE: 11/93 3/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS
NURSE FAMILY PARTNERSHIP PROGRAM
 1 NURSE FAMILY PARTNERSHIP PROGRAM Kelly Murphy, RN, MSN, IBCLC CAPT USPHS Clinical Coordinator Nutaqsiivik Program Home Based Services Southcentral Foundation Patty Wolf RNC-OB, BSN Team Manager Nurse
1 NURSE FAMILY PARTNERSHIP PROGRAM Kelly Murphy, RN, MSN, IBCLC CAPT USPHS Clinical Coordinator Nutaqsiivik Program Home Based Services Southcentral Foundation Patty Wolf RNC-OB, BSN Team Manager Nurse
The deadline for submitting an application is September 6, 2018.
 July 2, 2018 Dear Florida Hospital Leaders, It s with great enthusiasm we invite you to participate in the Florida Perinatal Quality Collaborative (FPQC) initiative for Neonatal Abstinence Syndrome (NAS)
July 2, 2018 Dear Florida Hospital Leaders, It s with great enthusiasm we invite you to participate in the Florida Perinatal Quality Collaborative (FPQC) initiative for Neonatal Abstinence Syndrome (NAS)
Bright Futures: An Essential Resource for Advancing the Title V National Performance Measures
 A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
ASTHO Breastfeeding Learning Community. Learning Session. February 8, 2018 For Audio, Please Dial: Ext #
 ASTHO Breastfeeding Learning Community Year 4 Learning Session #2 February 8, 2018 For Audio, Please Dial: 1-866-740-1260 Ext. 5222301# ASTHO Breastfeeding Learning Community Orange: Award States Blue:
ASTHO Breastfeeding Learning Community Year 4 Learning Session #2 February 8, 2018 For Audio, Please Dial: 1-866-740-1260 Ext. 5222301# ASTHO Breastfeeding Learning Community Orange: Award States Blue:
SUBJECT: Certificate Change Proposal Maternal and Child Health
 UNIVERSITY OF KENTUCKY D r e a m C h a l l e n g e S u c c e e d COLLEGE OF PUBLIC HEALTH M E M O R A N D U M TO: FROM: Health Care Colleges Council James W. Holsinger, Jr., PhD, MD Associate Dean for
UNIVERSITY OF KENTUCKY D r e a m C h a l l e n g e S u c c e e d COLLEGE OF PUBLIC HEALTH M E M O R A N D U M TO: FROM: Health Care Colleges Council James W. Holsinger, Jr., PhD, MD Associate Dean for
Jennifer Habert BHS, RRT-NPS, C-NPT Critical Care Transport Children s Mercy Kansas City
 Jennifer Habert BHS, RRT-NPS, C-NPT Critical Care Transport Children s Mercy Kansas City Learning Outcomes Participants will identify important operational and safety measures in the transport environment.
Jennifer Habert BHS, RRT-NPS, C-NPT Critical Care Transport Children s Mercy Kansas City Learning Outcomes Participants will identify important operational and safety measures in the transport environment.
By Dianne I. Maroney
 Evidence-Based Practice Within Discharge Teaching of the Premature Infant By Dianne I. Maroney Over 400,000 premature infants are born in the United States every year. The number of infants born weighing
Evidence-Based Practice Within Discharge Teaching of the Premature Infant By Dianne I. Maroney Over 400,000 premature infants are born in the United States every year. The number of infants born weighing
Managing Programmes to Improve Child Health Overview. Department of Child and Adolescent Health and Development
 Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
From Baby Bump to Baby Buggy A Maternal-Child Training Workshop
 From Baby Bump to Baby Buggy A Maternal-Child Training Workshop A comprehensive series of courses on the care of the mother and her newborn infant Orange County: 3303 Harbor Blvd. Suite G3 Costa Mesa,
From Baby Bump to Baby Buggy A Maternal-Child Training Workshop A comprehensive series of courses on the care of the mother and her newborn infant Orange County: 3303 Harbor Blvd. Suite G3 Costa Mesa,
An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience
 PRRINN-MNCH Experience") An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience I. Background Introduction of Kangaroo Mother Care in Nigeria KMC was first introduced
An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience I. Background Introduction of Kangaroo Mother Care in Nigeria KMC was first introduced
Hospital Quality Improvement Program (QIP) Measurement Specifications
 Measurement Specifications") Hospital Quality Improvement Program (QIP) 2015-2016 Measurement Specifications Developed by: The Hospital QIP Team Contact: HQIP@partnershiphp.org 2015-2016 Hospital QIP Page 1 Table of Contents 2015-2016
Hospital Quality Improvement Program (QIP) 2015-2016 Measurement Specifications Developed by: The Hospital QIP Team Contact: HQIP@partnershiphp.org 2015-2016 Hospital QIP Page 1 Table of Contents 2015-2016
SUTTER MEDICAL CENTER, SACRAMENTO DEPARTMENT OF PEDIATRICS RULES AND REGULATIONS
 REVIEW DATE: 8/2014 SUTTER MEDICAL CENTER, SACRAMENTO DEPARTMENT OF PEDIATRICS RULES AND REGULATIONS I MEMBERSHIP The Department of Pediatrics will consist of members of the Medical Staff of Sutter Medical
REVIEW DATE: 8/2014 SUTTER MEDICAL CENTER, SACRAMENTO DEPARTMENT OF PEDIATRICS RULES AND REGULATIONS I MEMBERSHIP The Department of Pediatrics will consist of members of the Medical Staff of Sutter Medical
Your Connection to a Healthier Life
 Your Connection to a Healthier Life The Northwest Ohio Pathways HUB is a regional care coordination system that connects low-income residents to needed medical and social services, including insurance
Your Connection to a Healthier Life The Northwest Ohio Pathways HUB is a regional care coordination system that connects low-income residents to needed medical and social services, including insurance
Research Design: Other Examples. Lynda Burton, ScD Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
MANUAL OF OPERATIONS FOR INFANTS BORN IN 2009
 VERMONT OXFORD NETWORK DATABASE MANUAL OF OPERATIONS FOR INFANTS BORN IN 2009 RELEASE 13.2 REVISED APRIL, 2009 2008 Vermont Oxford Network This Network publication is copyrighted and is not to be reproduced
VERMONT OXFORD NETWORK DATABASE MANUAL OF OPERATIONS FOR INFANTS BORN IN 2009 RELEASE 13.2 REVISED APRIL, 2009 2008 Vermont Oxford Network This Network publication is copyrighted and is not to be reproduced
The Mathematics of Morality in the NICU
 The Mathematics of Morality in the NICU William Meadow, MD, PhD Department of Pediatrics MacLean Center for Clinical Medical Ethics The University of Chicago I have, sadly, no relevant financial relationships
The Mathematics of Morality in the NICU William Meadow, MD, PhD Department of Pediatrics MacLean Center for Clinical Medical Ethics The University of Chicago I have, sadly, no relevant financial relationships
April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings
 April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings Shannon Richey, R.N. Assistant Bureau Chief Bureau of Community Health Care Facilities and Services Ohio Department of Health
April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings Shannon Richey, R.N. Assistant Bureau Chief Bureau of Community Health Care Facilities and Services Ohio Department of Health