MANUAL OF OPERATIONS FOR INFANTS BORN IN 2009
|
|
|
- Edith Osborne
- 6 years ago
- Views:
Transcription
1 VERMONT OXFORD NETWORK DATABASE MANUAL OF OPERATIONS FOR INFANTS BORN IN 2009 RELEASE 13.2 REVISED APRIL, Vermont Oxford Network This Network publication is copyrighted and is not to be reproduced in whole or in part without written permission from Vermont Oxford Network.
2 Database Eligibility 1 VLBW Database Eligibility Any infant who is born at your hospital and whose birth weight is between 401 and 1500 grams OR whose gestational age is between 22 weeks 0 days and 29 weeks 6 days (inclusive) is eligible, regardless of where in your hospital the infant receives care. Any outborn infant who is admitted to any location in your hospital within 28 days of birth, without first having gone home, and whose birth weight is between 401 and 1500 grams OR whose gestational age is between 22 weeks 0 days and 29 weeks 6 days (inclusive) is eligible, regardless of where in your hospital the infant receives care. Birth Weight Gestational Age (Wks/Days) Eligible for VLBW DB? /0 Yes /6 No /6 Yes /0 Yes /0 Yes /0 No /6 Yes /4 Yes /0 No Examples These examples assume that the infant was born in your hospital or was admitted to your hospital within 28 days of birth. Expanded Database Eligibility All infants eligible for the VLBW Database are also eligible for the Expanded Database. In addition, the following infants are also eligible for the Expanded Database only: (1) Any infant whose birth weight is over 1500 grams and who is admitted to a Neonatal Intensive Care Unit (NICU) in your hospital within the first 28 days of life without first having gone home, regardless of gestational age. A NICU is any location within the hospital in which newborn infants receive continuous positive airway pressure (CPAP) or intermittent mandatory ventilation (IMV). (2) Any infant whose birth weight is over 1500 grams and who dies at any location in your hospital within 28 days of birth without first having gone home. This includes inborn and outborn infants. 1 For further information on database eligibility, see Chapter 4.
3 Revisions for 2009 New Items: Transfer Code of Center from which Infant Transferred (outborn infants only), Item 4c on the Day Form. Periventricular-Intraventricular Hemorrhage (PIH), Where First Occurred, Item 19c on the Day Form. Inhaled Nitric Oxide, Where Given, Item 24b on the 2009 Discharge Form. Steroids for Chronic Lung Disease (CLD), Where Given, Item 26b on the 2009 Discharge Form. PDA Ligation, Where Done, Item 29b on the 2009 Discharge Form. ROP Surgery, Where Done, Item 30b on the 2009 Discharge Form. Location of Surgery (10 new items), Item 33a on the 2009 Discharge Form. Pneumothorax, Where Occurred, Item 35b on the 2009 Discharge Form. Necrotizing Enterocolitis, Where Occurred, Item 37b on the 2009 Discharge Form. Gastrointestinal Perforation, Where Occurred, Item 38b on the 2009 Discharge Form. Bacterial Pathogen, Where Occurred, Item 39b on the 2009 Discharge Form. Coagulase Negative Staph, Where Occurred, Item 40b on the 2009 Discharge Form. Fungal Infection, Where Occurred, Item 41b on the 2009 Discharge Form. Transfer Code of Center to which Infant Transferred, Item 52 on the 2009 Transfer and Readmission Form. Revised Definitions: Inhaled Nitric Oxide, Item 24 on the 2009 Discharge Form. In previous years, the question was asked whether Inhaled Nitric Oxide was given in your hospital. In 2009, the definition asks whether Inhaled Nitric Oxide was given prior to discharge and a Where Given question is asked for infants who transfer to or from your hospital. The item Reason for Transfer, Item 51 on the 2009 Transfer and Readmission Form, has been revised for infants born in 2009 to add ECMO as a reason for transfer. The item ECMO, Item S1.B on the 2009 Supplemental Data Form, has been revised for infants born in 2009 to indicate whether ECMO was done at your i
4 hospital prior to discharge. In previous years, the item was not restricted to procedures at your hospital. Discontinued Items: The following items will no longer be submitted for infants born in 2009 and later years. These items will remain applicable to infants born in prior years. Infant Transferred to a Vermont Oxford Network Hospital (Yes/No), Item 46 on the 2008 Transfer and Readmission Form. This item is no longer required because the new item has been added, Transfer Code of Center to which Infant Transferred, Item 52. ECMO, Where Done, Item S1.B2 on the 2008 Supplemental Data Form. The ECMO item and Reason for Transfer items have been modified for infants born in 2009, as discussed in Revised Definitions above, and the ECMO, Where Done item will no longer be collected. Nitric Oxide, Item S1.C1 on the 2008 Supplemental Data Form. In 2009 this item will be on the Discharge Form. Item 24a. Nitric Oxide, Where Given, Item S1.C2 on the 2008 Supplemental Data Form. In 2009 this item will be on the Discharge Form, Item 24b. Surgery for Congenital Heart Disease, Item S1.D1 on the 2008 Supplemental Data Form. In 2009 this information will be reported in the Surgical Codes item on the Discharge Form, Item 33a. Surgery for Congenital Heart Disease, Where Done, Item S1.D2 on the 2008 Supplemental Data Form. In 2009 this information will be reported in the location part of the Surgical Codes item on the Discharge Form, Item 33a. Other Changes: The Patient Log has been modified to include information on birth location, transfer codes for outborn infants and infants who transfer and to include date of admission for outborn infants. The date of forms submission has been replaced by date of record submission. See Chapter 6. The Transfer Log has been modified to include information on infants who are readmitted after initial transfer and infants who are transferred more than once. The dates for forms submission have been removed. ii
5 Contents Revisions for i New Items:... i Revised Definitions:... i Discontinued Items:...ii Other Changes:...ii Chapter 1: Welcome to the Vermont Oxford Network...1 Introduction... 1 Mission... 1 Reports... 1 enicq Software... 2 Database Options... 2 Confidentiality and Patient Privacy... 3 Methods for Submitting Data... 3 Getting Help... 3 Chapter 2: Understanding Network Reports...5 Introduction... 5 Nightingale Internet Reporting System... 6 Quarterly Reports... 7 Annual Quality Management Reports (QMR)... 8 QMR for VLBW Infants... 9 QMR for Expanded Data Centers... 9 Network Database Summaries... 9 Chapter 3: The Annual Data Submission and Report Cycle...10 Introduction Develop and Submit an Eligibility Verification Plan Submit Data for Each Eligible Infant Review Data Summaries Complete the Annual Hospital Membership Survey Finalize Data for the Annual Report Use the Network Reports for Quality Improvement Chapter 4: Organizing Your Data Management System...15 Introduction Step 1: Choose a Database Option Step 2: Designate a Team Leader Step 3: Assign Other Roles Step 4: Establish Procedures for Data Security and Patient Privacy Step 5: Establish Procedures for Data Collection, Submission and Correction Step 6: Establish a System for Filing and Storing Forms Step 7: Train Data Management Staff Step 8: Organize a Multidisciplinary Team iii
6 Chapter 5: Identifying Eligible Infants...19 Database Eligibility Criteria Additional Considerations for Expanded Database Eligibility Applying Eligibility Criteria Stillborn Infants Gestational Age and Eligibility Infants Discharged Home Prior to Admission Infants Who Die Frequently Asked Questions about Database Eligibility Chapter 6: Keeping Track of Eligible Infants...23 Introduction Patient Confidentiality Considerations Disposition of Data Forms, Logs and Worksheets Completing the Logs Patient Log Transfer Log Patient Data Booklet Patient Identification Worksheet Length of Stay Calculation Worksheet Completing the Delivery Room Death Booklet Patient Identification Worksheet Chapter 7: Submitting Data to the Network...36 Introduction Records and Data Items Ways of Submitting Data Guidelines for Data Submission Submitting Data Using Paper Forms Completing the 28 Day Form Completing the Discharge Form Completing the Transfer and Readmission Form Completing the Supplemental Data Form Completing the Delivery Room Death Form Chapter 8: Definitions of Data Items...48 Introduction Day Form Data Definitions Discharge Form Data Definitions Transfer and Readmission Form Data Definitions Part A of Transfer and Readmission Form Part B of Transfer and Readmission Form Part C of Transfer and Readmission Form Part D of Transfer and Readmission Form Supplemental Data Form Data Definitions iv
7 Chapter 9: Correcting and Finalizing Data...89 Introduction Data Summaries Error and Warning Summary Data Form Status Summaries Data Management Summary Submitting Data Corrections Avoiding Common Errors APPENDICES APPENDIX A: Logs, Worksheets, and Data Forms...99 APPENDIX B: Bacterial Pathogens APPENDIX C: Birth Defect Codes APPENDIX D: Surgery Codes APPENDIX E: Calculation Charts for Date of Day APPENDIX F: Calculation Charts for Date of Week APPENDIX G: Day Number Chart APPENDIX H: Timeline for Database Activities, APPENDIX I: Fahrenheit to Centigrade Conversion Table APPENDIX J: Vermont Oxford Network Directors, Advisory Board, and Database Advisory Committee INDEX v
8
9 CHAPTER 1 Welcome to the Vermont Oxford Network Introduction This manual is a user s guide for centers that submit data for the Very Low Birth Weight (VLBW) or Expanded Databases. It provides background information, instructions, and reference information that you will need to understand data collection and submit data to the Network. Mission The Vermont Oxford Network is a non-profit voluntary collaboration of health care professionals dedicated to improving the quality and safety of medical care for newborn infants and their families. Established in 1988, the Network is today comprised of over 750 Neonatal Intensive Care Units at hospitals worldwide. The mission of the Vermont Oxford Network is to improve the quality and safety of medical care for newborn infants and their families through a coordinated program of research, education and quality improvement. In support of its mission, the Network maintains databases that contain information about the care and outcomes of high-risk newborn infants. The Network s databases: Provide unique, reliable and confidential data to participating units for use in quality management, process improvement, internal audit, and peer review. Provide core data for randomized clinical trials, outcomes research, and epidemiological studies. Create the foundations for educational materials and programs for healthcare professionals, policy makers, families of high-risk infants, and the public. Reports The Network produces reports of clinical results to provide participating members with feedback about their performance (see Chapter 2). These detailed, confidential reports assist you in identifying opportunities for improvement at your center and monitoring the effects of your local quality improvement initiatives. Nightingale provides centers with secure Internet access to comprehensive quality improvement data for assessment of patient care and outcomes. The Annual Quality Management Report (QMR) documents patient characteristics, treatment practices, morbidity, mortality, and length of stay at your center for a birth year. The QMR tracks performance over time, and compares your individual institution's performance with that of the Network as a whole and with subgroups of hospitals similar to your own. A QMR for very low birth weight (VLBW) infants is provided to all members who complete the data finalization process for the birth year, and a separate QMR is provided to Expanded Database centers. 1
10 Quarterly reports are provided four times a year at the end of each quarter, and a final version is included with the annual QMR. Each quarterly report provides summarized year-to-date information by birth year for demographics, outcomes and interventions, with comparison data for your center last year and for the Network as a whole. Members who participate in the Expanded Database receive additional quarterly reports. enicq Software The enicq software allows electronic data entry and secure submission of de-identified data files via the Internet. With a simple, menu-driven user interface, the software supports the Very Low Birth Weight Database, the Expanded Database and the Neonatal Encephalopathy Registry (NER). The enicq software supports: Extensive range and error checking. On-line help to include all data item definitions. Reports and logs to simplify tracking of infants and record status. Secure application login. Administrator control of user access. Version checking and downloading of new versions via the Internet. Multiple search criteria for finding and viewing records. Vermont Oxford Network user assistance. For additional information about enicq, go online to and select enicq Software under Member Tools. Database Options As a member of the Vermont Oxford Network, your center may choose to participate in either the Very Low Birth Weight (VLBW) Database or in the Expanded Database. For details about eligibility criteria for these databases, see Chapter 5. The VLBW Database includes data for each eligible infant whose birth weight is between 401 and 1500 grams, or whose gestational age is between 22 weeks, 0 days and 29 weeks, 6 days (inclusive), regardless of where in your hospital the infant receives care. The Expanded Database includes additional data items for infants in the VLBW database and also includes data for eligible infants with birth weights over 1500 grams. Members participating in the VLBW or Expanded Databases may also participate in the Neonatal Encephalopathy Registry (NER). A Manual of Operations for the Registry is published separately. The Registry captures data to characterize the population of infants with encephalopathy, evaluate variations in current practice, identify opportunities for improvement in the quality and safety of care for infants with encephalopathy, monitor the introduction and dissemination of new neuroprotective therapies such as hypothermia, assess selection criteria for neuroprotective therapy, define important questions for clinical research, and plan prospective research and randomized trials. For additional information on the Registry, please contact the Network NER Coordinator (Table 1.2). To assure that the Network databases are representative of the eligible infant population, it is important that all members follow a consistent set of rules for identifying eligible infants and collecting data for these infants. Locations in the hospital where eligible infants are born or treated must be checked to assure that the data are complete. Each year, members complete and submit an Eligibility Verification Plan to facilitate this process (see Chapter 3). There are unusual situations that may lead to questions about interpreting the meaning of your hospital when applying infant eligibility criteria. These include legal and leasing arrangements whereby different locations within the hospital are under the control of different authorities, as well as situations in which the same group of neonatologists care for infants at multiple locations. In such situations it is important to recognize that eligibility is determined based on all infants delivered or cared for at your hospital, where hospital refers to a building or group of buildings on the same 2
11 campus among which infants can be moved without the routine need for ambulance transfer. Please check with your Account Manager at the Vermont Oxford Network if you have any questions about how the eligibility criteria should be applied at your hospital. Confidentiality and Patient Privacy The Vermont Oxford Network strictly maintains the confidentiality of the data in its databases. Although data at Network or group levels are summarized for comparative purposes, individual center data are only reported to the submitting center. None of the data submitted to the Network includes patient identifiers, as defined by the U.S. Health Insurance Portability and Accountability Act of 1996 (HIPAA). Vermont Oxford Network does not accept protected health care information. Your hospital must take appropriate measures to assure that patient data stored at your hospital are protected and secure from unauthorized access. Methods for Submitting Data Members can submit data to the Network for the VLBW Database either electronically or on paper forms. Expanded Database members must submit data electronically. If you choose electronic submission you will use a data entry and export program that uploads files to the Network. This may be done using the VON enicq software, which is available at no charge to VON centers, or other software of your choosing. The enicq software may be downloaded from the Network web site If you use software other than enicq for electronic submission, refer to the separately published Member Instructions for Submitting Electronic Data in 2009, which are available on the Network web site (Member Tools/Downloads/EDS Instructions). These instructions contain technical information for data entry application programmers and for staff at your center who manage the submission of data files to the Network. These instructions also include key points for successful submission of electronic data files. Contact your VON Account Manager for assistance with electronic submission. Getting Help When your center becomes a member of the Vermont Oxford Network, an Account Manager is assigned to assist you with data submission. The Account Manager will answer any questions you may have about collecting, recording, or submitting data and will support your center in achieving complete and accurate data reporting. If you have questions, don t hesitate to contact your Account Manager. If your Account Manager is unavailable, you can speak to anyone on the Data Processing Team listed in Table 1.1. You can get copies of the booklets, forms and worksheets described in this manual by copying them from Appendix A. They are also available on the Network web site at (Member Tools/Downloads). 3
12 Account Manager ( ) Phone Extension Address Kathy Arcovitch 215 Paula Beales 214 Annie Blanchette 218 Marilyn Eick 227 Pat Lavalette 260 Joan Schillhammer 224 Andy Warner 226 Ellen Wilhite 216 Table 1.1: How to Contact Your Account Manager Other Assistance: Type Assistance Membership, Agreements, Fees Neonatal Encephalopathy Registry (NER), Web Services, Nightingale, enicq, HIPAA Quality Improvement Contact ( ) Phone Address Extension Lynn Stillman 211 Nancy Cloutier 208 Kathy Leahy 205 Table 1.2: Other Assistance For other questions or assistance, please contact: Vermont Oxford Network 33 Kilburn Street Burlington, Vermont Phone: Fax: Web site: 4
13 CHAPTER 2 Understanding Network Reports Introduction One of the important benefits of membership in the Vermont Oxford Network is the feedback you get through the Network s confidential, customized reports. They document patient characteristics, treatment practices, morbidity, mortality, and length of stay at your institution. They also track performance over time, comparing your center s performance with its performance in previous years, with that of the Network as a whole, and with subgroups of institutions similar to your own. Table 2.1 lists the reports provided by the Network for centers participating in the VLBW and Expanded databases. Report Name How You Use It Frequency VON Nightingale Quarterly Reports Annual Quality Management Reports (QMR) Network Database Summaries Group Reports Special Reports Comprehensive historical and up-to-date information on patient demographics, outcomes and interventions via the Internet, substantially extending the availability and timeliness of audit and quality improvement data. Nightingale provides secure access to confidential center and Network data, with access controlled by center administrators. To track the clinical picture to date and identify any trends that indicate clinical problems or problems in data reporting. Expanded Database Members receive an additional quarterly report for all eligible infants. To make quality improvement interventions and for data audit and peer reviews. Expanded Database Members receive an additional QMR for all eligible infants. As a summary of clinical results appropriate for public distribution. Expanded Database Members receive an additional database summary for all eligible infants. To assist regional and other groups of hospitals improve the quality of care. To analyze hospital measures in ways not provided in standard reports. Table 2.1: Network Reports Electronic submissions updated daily Paper submissions updated after processing Quarterly April, July, October, and January Annually September Annually with QMR Annually after QMR On request (additional fee) 5
14 All Network reports are sent to your center s Report Contact. To effectively use the Network reports for quality improvement, organize a multidisciplinary team to review them as part of the ongoing quality improvement efforts at your NICU. The reports can be used as the starting point for in-depth analyses of specific clinical practices and patient outcomes at your center. Create an internal plan for how the Report Contact shares the information in the reports with the rest of the multidisciplinary team. Nightingale Internet Reporting System The Network s Internet Reporting system, Nightingale, is available to all members who have signed the applicable membership agreement. This online reporting system significantly extends the availability of neonatal care and outcome data for Network members and provides near real time information for quality improvement initiatives. Nightingale provides reports for members via the Internet. Named after the renowned 19 th century nurse and statistician, Florence Nightingale ( ), the system allows users to access historical and up-to-date information on infant care and outcomes. System access is controlled by administrators appointed by the member center, with strict confidentiality maintained for center level data. Access to your center s data on the Nightingale system is controlled by Web Services Administrators appointed by your center. All transmissions to the Nightingale server by users are encrypted using 128 bit secure socket layer technology. The features of the system include: The following infant populations are reported on Nightingale. You can view your center data and Network or group comparison data for each of these populations. o Infants with birth weights 501 to 1500 grams (inclusive). o Infants whose gestational age is between 22 weeks 0 days and 29 weeks 6 days (inclusive). o o All eligible VLBW infants (infants 401 to 1500 grams or 22 weeks 0 days to 29 weeks 6 days for 2005 and later, infants 401 to 1500 grams for years prior to 2005). All eligible Expanded Database infants (Expanded Data centers only). Users can select from four different types of graphs or view the results in a table. Once displayed, users may download tables and graphs as PDF documents and save or print them. Risk adjusted outcomes and other summary information for a birth year are available in a center summary PDF document, which may be downloaded and printed. From a clinical category such as Infection, users can choose a specific type of infection and view results by birth year, birth weight category, gestational age category or birth location. At the category level, overall results for related measures can be viewed and compared to Network results or results for centers in the member center s NICU Type. If your center participates in a group of hospitals, you can also compare your center performance to that of the group as a whole. From the measure level, the user can view results within the clinical 6
15 grouping of interest (e.g., birth weight or gestational age category), then drill down to the infant level to identify specific cases with the infection. Year-to-Date reports on Nightingale are similar to the quarterly reports distributed to members. Nightingale users can view up-to-date information on all collected data items for the current birth year and prior years. Center Web Services Administrators can download their center s infant data as an Excel spreadsheet for current or prior years. Data collected from the Annual Membership Survey is tabulated and available for comparison with the Network and the member center s NICU Type. A workspace allows users to save a set of queries for future reference. Members can provide online feedback and suggest improvements to the Nightingale system. Quarterly Reports The VLBW and Expanded Database Quarterly Reports provide a cumulative snapshot of the clinical data reported by your center for the current year-to-date. For a description of the Nightingale Year-to-Date Report available via the Internet, please see above. The Quarterly Report compares your year-to-date data with the data your center reported the previous year and with the data reported for the entire Network for the previous year. This report can be used to determine accuracy of data submitted as well as indicate changes in clinical practices in your hospital. A dramatic change in demographics, interventions, diagnoses, or outcomes may signal a trend you should investigate. Figure 2.1 shows the format of a sample Quarterly Report. The Quarterly Reports list most of the items on the Network s data forms and shows the number and percentage of patients that fall into various categories for these items. For some patients, no data may have been reported for a specific item. The Quarterly Reports are published in April, July, October and January, giving you frequent access to concise summaries of your center s data as it accumulates in the database. Expanded Database members also receive the Expanded Database Quarterly Report which shows data for infants in all weight categories and includes responses to the Supplemental Data items for all infants. A final version of the Quarterly Report for the birth year is included in the Annual NICU Quality Management Report, published in September of the following year. A final version of the Expanded Database Quarterly Report is in the Annual NICU Quality Management Report for Expanded Data Centers. Keep in mind that the Quarterly Report is of increasing value as the year continues. Data accumulate throughout the year; as data are submitted and as patients are discharged, the remaining data items for these patients can be completed. Early in the year, the data are likely to be significantly less complete and therefore less reliable than in the third and fourth quarters. Incomplete data may not reflect the true clinical picture. 7
16 Figure 2.1: First Page of a Sample Quarterly Report Annual Quality Management Reports (QMR) The Annual Quality Management Reports (QMR) provide a comprehensive, confidential analysis of your center s individual data and that of the Network as a whole. The detailed figures and tables in the QMR allow you to confidentially compare your center s morbidity, mortality, and length of stay to the total Network and to a subgroup of centers similar to your own. 8
17 The reports for a given birth year cohort are produced in August and September of the following calendar year. The reason for this reporting lag is the long length of stay for some infants. Disposition information is not available for some infants until six months or more after birth. To be eligible to receive an Annual NICU Quality Management Report, your center must have: Remitted the annual membership fee for the birth year reported in the QMR. Submitted an approved Eligibility Verification Plan (Chapter 3, Figure 3.1). Submitted a completed Membership Survey for the applicable birth year. Met the requirements for data completeness, timeliness and accuracy described in Chapter 3. Submitted a signed Report Contact Finalization confirming the completeness of data submitted for the birth year and the inclusion of all eligible infants. QMR for VLBW Infants The VLBW QMR is based on a cohort of infants born in a calendar year with birth weights between 401 and 1500 grams or gestational ages between 22 weeks 0 days and 29 weeks 6 days, inclusive. See Chapter 5 for details on the population included in the VLBW Database. The report includes measures which have been risk adjusted to account for case mix at your hospital, as well as data stratified by birth weight, gestational age, birth location and birth year. QMR for Expanded Data Centers If your center participates in the Expanded Database, you will receive the Annual Quality Management Report for Expanded Data Centers, in addition to the VLBW QMR. See Chapter 5 for details on the population included in the Expanded Database. This report is similar to the VLBW QMR, except that it includes eligible records on infants with birth weights over 1500 grams and responses to the Supplemental Data items. As with the VLBW QMR, risk adjusted measures and summary measures stratified by birth weight, gestational age and other categories are provided to facilitate comparisons of your center s performance with other Expanded Database participants. Network Database Summaries The Network Database Summaries for the VLBW and Expanded Databases report the results for all eligible infants who were born during the birth year at all Network institutions. The reports summarize Network results; there are no institution-specific data included other than the participating institution names, countries, cities and states. The two reports are produced and distributed publicly for the VLBW and the Expanded Databases. Group Reports Reports are prepared for groups of hospitals that wish to view comparative data for individual group members and for the group as a whole. Comparison data for the entire group are also available in Nightingale for all measures collected by the Network. These reports can be useful for facilitating collaborative efforts by group members. Special Reports Reports designed to meet special needs of members may be prepared on request for an additional fee. 9
18 CHAPTER 3 The Annual Data Submission and Report Cycle Introduction Network reports are based on birth year, and each January 1 st marks the beginning of a new cycle which includes data submission for each eligible infant and continues until the Network reports are published and are used by your center for quality improvement. The events in this annual cycle are listed in Table 3.1. Before reports are published, guidelines are distributed and checks are done to assure that all errors in submitted records have been corrected, that all records are complete and that all eligible infants have been identified. Your Account Manager will let you know about the requirements for data finalization. The expectation is that members will assure that records for all eligible infants have been submitted and that all submitted records are complete and correct by June of the following birth year. The Annual Cycle for Data Submission and Reporting Develop and Submit an Eligibility Verification Plan. Submit Data for Each Eligible Infant. Correct Data Errors as Necessary. Complete the Annual Hospital Membership Survey. Finalize Data for the Annual Report. Use the Network Reports for Quality Improvement. Table 3.1: The Annual Cycle for Data Submission and Reporting Develop and Submit an Eligibility Verification Plan The Eligibility Verification Plan (EVP) is intended to help establish a method for identifying eligible infants and their locations in your hospital and is prepared and submitted annually to the Network. When you first become a member of the Network and at the beginning of each calendar year, the Network sends you an Eligibility Verification Plan as shown in Figure 3.1. When you complete the EVP, indicate the sources you will use to identify eligible infants and the frequency with which you will collect data from these sources. If your center uses a data source that isn t listed, specify what this source is on the line below Other. The frequency with which you check each source depends on various factors, including the number of infants who are born or receive care at your center, staffing at your center, and whether your center has a computerized clinical data system. 10
19 Notice that the EVP has a special section on data sources for Delivery Room Deaths. These patients can be difficult to track since they are not admitted to your NICU. List all the locations in your hospital where infants might die, note the data sources associated with these locations and specify these sources on the EVP. If your center participates in the Expanded Database or the Neonatal Encephalopathy Registry (NER), it is important to identify all locations in your center where an eligible infant may receive continuous positive airway pressure (CPAP) or intermittent mandatory ventilation (IMV). To ensure that these infants aren t inadvertently omitted from your center s data, write these locations below the line Other and routinely check these locations for eligible infants. Figure 3.1: Eligibility Verification Plan 11
20 Submit Data for Each Eligible Infant Members of your data collection team need to fully understand the eligibility criteria described in Chapter 5. These criteria depend on whether your center participates in the VLBW or the Expanded Database. When eligible infants are identified, use the logs and worksheets shown in Chapter 6 to keep track of each infant and to assign Network ID numbers. The Network ID Number that you assign is the unique infant identifier for all Vermont Oxford Network data submissions. Use the Network ID number on the Patient and/or Transfer Log to associate data reported to the Network with patient records in your local system. This is important when you need to re-examine a patient s records to make corrections to the data you ve submitted, as well as for data audits, quality improvement activities and peer reviews. For each eligible infant, start data entry by choosing either the Patient Data Booklet or the Delivery Room Death Booklet. Each year, logs, forms, and data items may change. Based on the infant s year of birth use the appropriate forms and database documentation for each infant. The data forms are labeled with a unique release number. The release number for the Manual of Operations for 2009 data collection is For infants born in 2008, use release 12.1 of the Manual of Operations. Complete the Network data forms on each eligible infant as data are available using the procedures described in Chapter 7. This includes the Delivery Room Death Form for infants who meet the delivery room death criteria described in Chapter 5 or the 28 Day Form and Discharge Form for other eligible infants. For infants who transfer from your center to another hospital, complete the Transfer and Readmission Form. If your center participates in the Expanded Database, complete the Supplemental Data Form for each eligible infant. If your center participates in the Neonatal Encephalopathy Registry but not in the Expanded Database, complete the Supplemental Data Form for each infant who is eligible for the Registry. TIP: Keep the original forms and the worksheets for each infant together for the extended period of time that may be required to complete the data forms. This decreases the chances of losing or misplacing original paperwork. Also establishing this habit of always returning forms (keeping all infant forms together) to the booklet will help prevent such loss of information. If your center mails paper forms to the Network, make a copy of all forms before mailing. However, avoid duplication when submitting data: mail or fax, not both! Although data forms can be removed from the booklets for copying, please be sure to return the forms and worksheets to the booklet and file them carefully. If you submit data electronically, collect the data using the paper forms and enter the data into your computer system. Electronically submit data records to the Network at least monthly and more often when requested. Keep copies of the paper forms for reference and audit purposes, but do not submit paper forms to the Network. 12
21 Review Data Summaries Data submissions are checked for accuracy and completeness. You can review data summaries in the Data Management Section of the Members Area at These data summaries provide feedback about your data, making it easier to correct and complete forms efficiently. Data correction procedures are described in detail in Chapter 9. Submit all new, updated and corrected data monthly or more often when requested. Complete the Annual Hospital Membership Survey At the beginning of each year, the Annual Hospital Membership Survey will be sent to your hospital and should be completed based on your hospital characteristics as of the previous year. For example, in early 2009 you will receive the Membership Survey for Data from the membership surveys are summarized and reported in the Annual Quality Management Reports and on the Nightingale Internet Reporting system. These reports allow you to compare characteristics and capabilities at your hospital to other hospitals in the Network. Reports are also generated using survey data which allow you to compare infant procedures and outcomes to other hospitals with your NICU Type. Three NICU Types are currently identified based on these criteria: Type A: Restrictions on ventilation and/or major surgery not performed. Type B: No restrictions on ventilation and major surgery performed. Type C: No restrictions on ventilation and major surgery performed, including cardiac surgery. Finalize Data for the Annual Report Centers that complete the requirements for participation in the database during the previous year receive a customized annual Quality Management Report (QMR) for eligible infants born in that year. In order to maintain your center s data in the Network Database and to receive the QMR, your center must finalize all data for the birth year by correcting errors, submitting data for all eligible infants and meeting timelines for data submission. This process is called data finalization. To implement this process, the Data Finalization Guidelines for the 2009 Birth Year will be published in early These guidelines provide timelines and procedures for completing your center s data requirements for infants born in that year. Data for a birth year are considered complete and accurate when the following requirements are met: Records are complete and accurate for all eligible infants who have died, who have been discharged home or who have reached their first birthday. Records are as complete and accurate as possible for all eligible infants who are less than a year old and are still hospitalized without having been discharged home. 13
22 No errors exist in any data for the birth year. Your center has accounted for any unused ID numbers (gaps in ID number sequencing). Your center has confirmed the number of records submitted for the birth year. Your center has confirmed the first and last ID numbers used for the birth year. Your center has confirmed that all eligible infants have been reported for the birth year, including eligible infants who die in the delivery room/initial resuscitation area. Your center has confirmed that infants with missing disposition status are still hospitalized. If these requirements and submission timelines are met, your center s data will be permanently included in the Network Database, and your center will receive the annual Quality Management Report. Use the Network Reports for Quality Improvement As discussed in Chapter 2, the Network reports provide a wealth of information that can be used by your hospital interdisciplinary teams to improve the quality of care. For example, the Annual Quality Management Reports include risk adjusted statistics for key outcomes like mortality and infection, as well as for total hospital stay. These measures are also available in your hospital center summary on Nightingale. Together with the information on observed rates for procedures and outcomes and the capabilities provided to drill down to the infant level, the reports can be the basis for assessing the strengths and weaknesses of care and planning for improvement. 14
23 CHAPTER 4 Organizing Your Data Management System Introduction This chapter provides suggestions for organizing a data management system to submit timely and accurate data. Table 4.1 lists the recommended steps for this organization. Whenever you need help, use your Account Manager as a resource. Steps to Organize Your VON Data Management System Step 1: Choose a database option. Step 2: Designate a Team Leader. Step 3: Assign other roles. Step 4: Establish procedures for data security and patient privacy. Step 5: Establish procedures for data collection, submission and correction. Step 6: Establish a system for filing and storing forms. Step 7: Train data management staff. Step 8: Organize a multidisciplinary team. Table 4.1: Steps to Organize Your VON Data Management System Step 1: Choose a Database Option Your center may choose to participate in the Very Low Birth Weight (VLBW) Database or the Expanded Database. When deciding on a database option, keep in mind that you must submit data for all the infants at your center who meet the eligibility criteria for that database. Participation in the Expanded Database means managing a significantly greater volume of data and collecting additional data items for all eligible infants. Carefully review Chapter 5 to understand who is eligible for the databases. Centers participating in the VLBW Database submit data items on the 28 Day Form, Discharge Form and Transfer and Readmission Form for infants eligible for the VLBW Database. Centers that only participate in the VLBW database may submit data electronically or by using Network paper forms. Centers participating in the Expanded Database must submit data electronically for data items on the 28 Day Form, Discharge Form, Transfer and Readmission Form and Supplemental Data Form (see Chapter 7). You may use the Network enicq data entry software to submit data electronically. enicq is free to all Network members and may be downloaded from the Network web site at the following link: 15
24 Step 2: Designate a Team Leader The Team Leader is the person at your center who assumes ultimate responsibility for leading and coordinating the activities involved in participating in the Network. Selecting the right person for this job will help ensure that your center s participation in the Network runs smoothly. The Team Leader is responsible for: Supervising all Vermont Oxford Network Database activities at your center. Establishing procedures for data collection and submission, and monitoring their implementation. Developing an Eligibility Verification Plan and monitoring its implementation. Overseeing training. Supervising the data collection and submission tasks. Determining data submission schedules. Verifying that all eligible infants are included. Verifying that the data conform to all the definitions and conventions of the database. Step 3: Assign Other Roles The Network s membership application lists four other roles or contacts at your center in addition to the Team Leader. These contacts are the members of your team who are authorized to communicate with the Network about various aspects of your center s participation in the database. The Team Leader usually functions as one or more of these contacts. At small centers, the Team Leader may serve all four roles. The four contacts you must designate are: The Report Contact is the only person at your center who can receive Network reports. This person should be a member of your center s peer review committee and be active in quality improvement activities. The Data Contact is the person with whom the Network corresponds regarding data status, submission, and errors. Depending on the size of your center, the Data Contact may be the person who actually collects and submits the data or someone who supervises other data management staff. The Financial Contact is the person who handles membership fees and membership agreements. The Neonatologist Contact has clinical and/or research experience and should be available to the Data Contact as a resource for medical questions pertaining to the data definitions. This is the person to whom the Network sends information about ongoing clinical trials, research projects, quality improvement collaboratives, projects, and meetings. 16
25 Your center may decide to include additional staff to collect, submit, and maintain the data. We recommend that you develop an internal plan detailing the roles of the various members of your team and their access to the data. You must inform the Network when designated contact information changes. Step 4: Establish Procedures for Data Security and Patient Privacy As a member of the Vermont Oxford Network, your center is responsible for protecting patient privacy and for ensuring that patient data are secure. Patient Logs, Transfer Logs, Patient Identification Worksheets, and Length of Stay Calculation Worksheets contain personal patient identifiers and are considered to be protected health care information by HIPAA (the Health Insurance Portability and Accountability Act of 1996). Do not send any of these forms or any other personal patient identifying information to the Vermont Oxford Network. The Vermont Oxford Network does not accept protected health care information. Step 5: Establish Procedures for Data Collection, Submission and Correction The goal is to implement procedures to ensure that all eligible infants are identified and reported, and that the data you submit are accurate and timely. You also need a system for correcting errors and for responding to other potential problems that the Network may identify in your center s data. If your center submits data electronically, you may find it useful to first collect data on paper forms and to use the paper forms as a basis for data entry. This will allow you to double-check data before submission and also provide backup data in case you have problems with your computer. Step 6: Establish a System for Filing and Storing Forms To ensure the integrity of the data you submit, it is important to keep all original forms and worksheets for each infant together. The Patient Data Booklet and the Delivery Room Death Booklet help you keep the data for each infant separate from the data for other infants. If infants transfer from your center to another hospital, the Transfer and Readmission Form should be kept with the other forms in the Patient Data Booklet. When you send paper forms to the Network, first make a copy and mail or fax (not both) the copies to the Network. Be sure to return the original forms to the booklets. It is the responsibility of each participating center to maintain and store all logs, worksheets, and forms to ensure that patient privacy and data security requirements are met. One advantage of electronic data submissions (EDS) is that the data entry program you use automatically organizes the data for each infant in a separate data record. In addition, many data entry programs automatically cross-check records to prevent 17
26 duplication and to help ensure that the correct data are being reported for each infant. Of course, it is still critical to double-check any data you enter against patient logs and other data sources. While EDS systems make it easier to keep data organized, errors can still be created during the data entry process. If you submit data electronically, you may choose to use the Network s paper forms to collect the data, and then enter the data into your data entry application, but do not submit the paper forms to the Vermont Oxford Network. Step 7: Train Data Management Staff All staff members who are involved in data collection, submission, and maintenance should be thoroughly familiar with: The purposes of the database The eligibility criteria for patients The data definitions the information required for each data item Procedures for collecting and submitting data Procedures for filing and storing forms This manual is your resource for training your center s data management staff. Anyone involved in collecting and submitting data at your center should thoroughly understand how to identify eligible infants, collect and submit data and make data corrections. Step 8: Organize a Multidisciplinary Team Your center should establish a multidisciplinary team to review the Network s quarterly and annual reports. The team s goal is to help direct your center s local quality improvement efforts using the comprehensive performance data provided by the Network. The team may include doctors, nurses, respiratory therapists, nutritionists, pharmacists, and any other health professionals involved in NICU care at your center. The team should use the comparative data and the analyses of interventions and outcomes provided by the reports to target specific clinical practices and identify opportunities for improvement. The team should also track change, monitoring the effect of your center s quality improvement interventions over time. We recommend that you develop an internal system for sharing the data from reports and the Nightingale reporting system with the multidisciplinary team. The reports contain sensitive data, including data on morbidity, mortality and length of stay at your hospital. It is important to protect the confidentiality of this information, while at the same time making the most effective use of it to advance your center s quality improvement projects. If you need help with any aspect of organizing your system or managing your data, contact the Account Manager who was assigned to you when you became a Network member. Your Account Manager will help you keep your center s data up-to-date and assist you with any problems that arise. 18
27 CHAPTER 5 Identifying Eligible Infants Database Eligibility Criteria Infant eligibility criteria for the VON databases have been established so that data from your center will be comparable to other Network centers. To assure that your data are useful for quality improvement, it is very important that data are collected for all eligible infants. If your center participates in the VLBW Database, only Table 5.1 below is applicable. If your center participates in the Expanded Database, both Tables 5.1 and 5.2 are applicable. VLBW Database Eligibility Any live born infant who is born at your hospital and whose birth weight is between 401 and 1500 grams OR whose gestational age is between 22 weeks 0 days and 29 weeks 6 days (inclusive) is eligible, regardless of where in your hospital the infant receives care. A live born infant is one who breathes or has any evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles. Stillborn infants (those who are not live born) are not eligible for the VLBW database. Any outborn infant who is admitted to any location in your hospital within 28 days of birth, without first having gone home, and whose birth weight is between 401 and 1500 grams OR whose gestational age is between 22 weeks 0 days and 29 weeks 6 days (inclusive) is eligible, regardless of where in your hospital the infant receives care. Examples These examples assume that the infant was born in your hospital or was admitted to your hospital within 28 days of birth without first having gone home. Eligible for Birth Weight Gestational Age (Wks/Days) VLBW DB? /0 Yes /6 No /6 Yes /0 Yes /0 Yes /0 No /6 Yes /4 Yes /0 No Table 5.1: Eligibility Criteria for the VLBW Database 19
28 Expanded Database Eligibility All infants eligible for the VLBW Database are also eligible for the Expanded Database. In addition, the following infants are also eligible for the Expanded Database only: (1) Any infant whose birth weight is over 1500 grams and who is admitted to a Neonatal Intensive Care Unit (NICU) in your hospital within the first 28 days of life without first having gone home, regardless of gestational age. A NICU is any location within the hospital in which newborn infants receive continuous positive airway pressure (CPAP) or intermittent mandatory ventilation (IMV). (2) Any infant whose birth weight is over 1500 grams and who dies at any location in your hospital within 28 days of birth without first having gone home. This includes inborn and outborn infants. Table 5.2: Eligibility Criteria for the Expanded Database As Table 5.2 shows, the Expanded Database is a superset of the VLBW Database. The Expanded Database includes data for all infants in the VLBW Database as well as data for all eligible infants over 1500 grams, regardless of gestational age, who are either admitted to a Neonatal Intensive Care Unit (NICU) in your hospital or who die in your hospital within 28 days of birth. Additional Considerations for Expanded Database Eligibility If your center participates in the Expanded Database, you must identify all the units in your hospital that qualify as a NICU by applying the following definition: A NICU is any location within the hospital in which newborn infants receive continuous positive airway pressure (CPAP) or intermittent mandatory ventilation (IMV). When applying this definition, do not include those areas in which these modalities of respiratory support are used only for brief periods of stabilization prior to transfer to another location. The intent is that units designated as Neonatal Intensive Care Units routinely provide these services for ongoing care beyond an initial period of stabilization. Applying Eligibility Criteria The following guidelines and examples will be helpful as you determine whether infants are eligible for the VLBW and Expanded Databases. Stillborn Infants Stillborn infants are not eligible, only live born infants are eligible. A live born infant is an infant who breathes or has any evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles. 20
29 Gestational Age and Eligibility Infants who meet the gestational age and admission criteria are eligible regardless of birth weight. All live born infants with gestational ages between 22 weeks 0 days and 29 weeks 6 days, who are born at your center or admitted to your center within 28 days of birth, are eligible for both the VLBW and Expanded Databases, regardless of birth weight. This applies to infants with birth weights less than 401 grams and to infants with birth weights greater than 1500 grams. See Table 5.1 for examples. Infants Discharged Home Prior to Admission Infants who are discharged home prior to admission to your hospital are not eligible. Whether you participate in the VLBW Database or the Expanded Database, the infants for whom you report data must not have gone home before being admitted to your hospital. For instance, infants discharged home from another hospital before being admitted to your hospital are not eligible. The one exception is infants born at home or in transit. These infants are eligible if they arrive at your hospital alive and meet all the other criteria. Infants Who Die Data for all eligible live born infants who die must be reported, regardless of where in your hospital they die, including the delivery room. Your Eligibility Verification Plan asks you to identify data sources for infants who die. To be sure you do not omit infants in this category; make a list of the locations at your center where infants might die. For the VLBW Database these infants are eligible: All live born infants who are born in your hospital and who die are eligible if their birth weights are between 401 and 1500 grams or if their gestational ages are between 22 weeks 0 days and 29 weeks 6 days (inclusive). All outborn infants with birth weights of 401 through 1500 grams or gestational ages between 22 weeks 0 days and 29 weeks 6 days (inclusive) are eligible if they are admitted to your hospital within 28 days of birth and who die. For the Expanded Database these infants are eligible: Any eligible VLBW infant who dies, as described above. Any eligible infant with birth weight over 1500 grams who is admitted to a NICU in your hospital within 28 days of birth and who dies. Any inborn or outborn infant with birth weight over 1500 grams who is never admitted to a NICU but who dies at any location in your hospital within 28 days of birth. NOTE: Infants who never received care in a NICU, and who would therefore not have been included in the Expanded database, must be reported if they die within the first 28 days of life and have not been discharged home. This includes full-term infants and infants who are not in the very low birth weight category. 21
30 Infants Who Die in the Delivery Room Eligible infants who meet the Delivery Room Death Criteria in Table 5.3 must be reported to the Network. Monitor delivery room logs to verify that all eligible infants are reported. Delivery Room Death Criteria Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a Delivery Room Death. These locations may include the mother s room, resuscitation rooms, or any location other than the NICU in your hospital. Outborn infants and infants who are admitted to the NICU should not be classified as Delivery Room Deaths. Do not use a Delivery Room Death Booklet for these infants, regardless of where death occurs. Table 5.3: Delivery Room Death Criteria Frequently Asked Questions about Database Eligibility Table 5.4 includes some commonly asked questions about database eligibility. If you have other questions, please contact your VON Account Manager. Q: Should planned terminations resulting in a live birth be reported to the Network? A: Yes. Data for all eligible live born infants should be submitted regardless of the circumstances of birth. A live born infant is one who breathes or has any evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles. Q: An infant was transferred from another Vermont Oxford Network hospital. Should our hospital also send data on this infant? A: If the infant is admitted to your center within 28 days of life and meets the other eligibility criteria, your center should submit data to the Vermont Oxford Network. Q: An infant was transferred to our unit from another hospital. Should information received from the other hospital be included in our data on that infant? A: Yes, with one exception noted below. If the infant meets the eligibility criteria, the data forms for this infant should include information from the other hospital s medical records, as well as from your hospital s medical records. The only exception is that, for centers participating in the Expanded Database, Items S1.A1 and S1.A2 (Duration of Assisted Ventilation) only apply to ventilation at your center (see Chapter 8 for details). Q: An infant was admitted to our hospital for surgery and transferred back to the other hospital on the same day. Should data be reported on this infant? A: Yes. If the infant meets the eligibility criteria, your center should submit data for this infant, regardless of the reason for admission or the length of stay at your hospital. Table 5.4: Frequently asked Questions on Database Eligibility 22
31 CHAPTER 6 Keeping Track of Eligible Infants Introduction Use the Patient Log, the Transfer Log, the Patient Booklets and the data forms to keep track of data for eligible infants. To avoid data entry errors it is a good idea to keep together all data forms for each infant in a separate folder. Patient Booklets bind together the worksheets and forms needed when collecting data for most patients, making it easier to keep documentation for patients together. The Delivery Room Death Booklet includes a Patient Identification Worksheet and a Delivery Room Death Form. The Patient Data Booklet includes a Patient Identification Worksheet, a Length of Stay Calculation Worksheet, a 28 Day Form and a Discharge Form. The Patient Booklets are available on the VON website and in Appendix A. The Transfer and Readmission Form is used to collect and submit data to the Network for all infants who transfer from your center to another hospital before being discharged home. The Transfer and Readmission Form is printed separately. You can find this form on the VON website and in Appendix A. Supplemental data are submitted for all infants eligible for the Expanded Database (see Chapter 5 for eligibility criteria) and for all infants who are eligible for the Neonatal Encephalopathy Registry (See NER Manual of Operations). Patient Confidentiality Considerations The Patient Log and the Transfer Log contain patient identifiers which are defined as protected health care information by the U.S. HIPAA (Health Insurance Portability and Accountability Act) regulations. Do not submit logs to the Vermont Oxford Network. The Vermont Oxford Network does not accept protected health care information. The worksheets (but not the data forms) in the Patient Booklet and the Delivery Room Death Booklet include protected health care information. Do not submit worksheets to the Network. The data forms in the Patient Data Booklet and the Delivery Room Death Booklet include items that are submitted to the Network for all eligible infants. The 28 Day Form, Discharge Form and Delivery Room Death Form have been de-identified and do not include any patient identifiers. 23
32 Disposition of Data Forms, Logs and Worksheets Table 6.1 shows which forms are retained at your center and which are submitted to the Network. If you have any questions about these forms, contact your Account Manager. Logs, Worksheets & Forms Logs Patient Log Transfer Log Keep at Your Center 1 Send to Network Patient Data Booklet Patient ID Worksheet Length of Stay Worksheet 28 Day Form Discharge Form Transfer and Readmission Form Delivery Room Death Booklet Delivery Room Death Patient ID Worksheet Delivery Room Death Form Supplemental Data Form (Applies to electronic data submissions for the Expanded Database and centers submitting NER data) Table 6.1: Disposition of Network Logs, Worksheets and Forms 1 A copy of all forms sent to the Network should be kept on file in your hospital. 24
33 Completing the Logs There are two confidential logs to facilitate tracking of eligible infants and their disposition status, as well as to provide a record of data submission. All eligible infants should be noted in the Patient Log. Eligible infants who transfer to other hospitals before being discharged home should be entered into the Transfer Log. NOTE: Do not submit Patient or Transfer Logs to the Network. These logs contain personal patient identifiers and must be treated as protected health care information. The Vermont Oxford Network does not accept protected health care information. Patient Log Enter data into the Patient Log (Figure 6.1) for each eligible infant. This will allow you to cross check the Network ID Number with the patient name for data integrity. The Patient Log provides a link between the data in your local system and the data you have submitted to the Network. Because this log contains both patient identifiers, such as the infant s name and medical record number, and an anonymous Network ID you have assigned to that infant, it allows you to associate a specific infant s records in your local system with the data about that infant that you have reported to the Network. This is important when you need to make corrections to the data you have submitted, as well as for data audits and peer reviews. Use the Patient Log to assign a unique Network ID for each infant, to document and track the submission of the necessary data forms and to re-identify infants you have reported to the Network. Consult it when you enter data on a form for a particular patient. By cross-checking the Network ID you have entered on the log against the Network ID on each form, you can reduce the chance of reporting data for the wrong infant. Figure 6.1: Patient Log 25
34 Guidelines for Completing the Patient Log Before you enter data in the Patient Log, establish the infant s eligibility for inclusion in the Network database. Eligibility criteria are described in Chapter 5. Enter your VON Center Number at the top of the Patient Log. This number was assigned to your hospital when joining the Network. Enter the Network ID Number for the patient. Network ID Numbers are assigned sequentially for each new patient. If you are just beginning data entry, assign ID number 1 to the first patient record and increment the number for each additional infant record. Different Network ID Numbers must be assigned to each eligible infant in multiple births. At the beginning of each new year, sequential numbering must continue so that ID numbers from previous years are not reused. For example, if the last Network ID Number assigned to an infant born in 2008 is 535, then the first eligible infant born in 2009 should be assigned Network ID Number 536. Enter the patient s name, medical record number, and birth date. With this information you will be able to accurately match the patient with the data submitted to VON. In the column labeled DR Death?, enter Yes or No to indicate whether the infant meets the delivery room death criteria. Delivery room death criteria are described in Chapter 5, Table 5.3. Records for infants who die in the delivery room or initial resuscitation area within 12 hours are submitted on the Delivery Room Death Form. Enter the Patient s Birth Location. If outborn, enter the date that the infant was admitted to your hospital and the transfer code of the hospital from which the infant was transferred. The transfer code of hospitals may be found on the Network Web Site, Data submitted for outborn infants must include events that occurred at the hospital from which transferred, unless the item definition only asks whether the event occurred at your hospital. Enter the infant s Initial Disposition (Home, Transfer, Died or Still Hospitalized as of First Birthday) and the date of Initial Disposition. This column indicates the infant s status when first discharged from your center. VON data collection ends at the infant s first birthday if the infant is still hospitalized and has not been discharged home. If the infant was transferred to another hospital without first having gone home, enter the Transfer Code of the hospital to which the infant transferred. Use the Transfer Log to track infants who transfer from your center to another hospital. The transfer code of hospitals may be found at this link: Enter the date when your center first submitted the patient record or data forms to VON. Submitting data for all eligible infants helps assure accurate reporting of your center data and for the Network database as a whole. This information will help track which infant records have not been submitted to the Network. 26
35 Transfer Log Use the Transfer Log (Figure 6.2) to identify and track individual patients who are transferred from your center to other hospitals. Some patients have complex transfer histories. The Transfer Log captures information that will be helpful when you submit data to the Network. NOTE: Infants who relocate from one unit in your hospital to another unit within your hospital are NOT considered to have transferred. Do not complete the Transfer Log in these cases. Guidelines for Completing the Transfer Log Enter your VON Center Number at the top of the Transfer Log. This number was assigned to your hospital when joining the Network. Enter the Network ID Number that was assigned to the infant in the Patient Log. Enter the Patient s Name, Birth Date and Transfer Hospital Name. Enter the infant s Post Transfer Disposition. This is the status of the infant when the infant was discharged from the transferred to hospital (initial transfer). Enter Home, Transferred Again, Died, Readmitted, or Still Hospitalized as of First Birthday (whichever occurred first following transfer). VON data collection ends at the infant s first birthday if the infant is still hospitalized and has not been discharged home. Enter whether the infant was readmitted to your hospital (Yes/No) after initial transfer and, if so, the Disposition after Readmission (Home, Transferred Again, Died or Still Hospitalized at First Birthday). If the infant was transferred more than once, either after readmission to your hospital or after initial transfer, enter Yes in the Transferred More than Once column and enter the infant s Ultimate Disposition (Home, Transferred Again, Died or Still Hospitalized at First Birthday, whichever occurs first). The Ultimate Disposition is the infant s final discharge status if transferred more than once. Enter the date that the infant was discharged home or died or the infant s first birthday (if still hospitalized), whichever is soonest. 27
36 Figure 6.2: Transfer Log 28
37 Patient Data Booklet The Patient Data Booklet includes the Patient Identification Worksheet and the Length of Stay Calculation Worksheet. These worksheets include confidential patient data and are not to be sent to the Network. Patient Identification Worksheet NOTE: Verify that the infant is eligible and does not meet delivery room death criteria before completing the Patient Identification Worksheet. The Patient Identification Worksheet (Figure 6.3) is on the front cover of the Patient Data Booklet. It lists the Patient s Name, Mother s Name, Medical Record Number, Date of Birth, Date of Admission, Date of Day 28, Date of Week 36, Date of Initial Disposition and, if the infant is transferred to another hospital, the date discharged home, died or first birthday (if still hospitalized), whichever is soonest. Guidelines for Completing the Patient Identification Worksheet Check the Patient Identification Worksheet with the Patient Log to ensure consistency of information in the logs, worksheets, and forms. Enter your VON Center Number at the top of the Patient Log. This number was assigned when joining the Network. The Network ID Number was assigned to the infant in the Patient Log (see the Guidelines for Completing the Patient Log earlier in this chapter). Enter the Patient s name in Item W1. Enter the Mother s name in Item W2. Enter the Patient s Medical Record Number in Item W3. Enter the Patient s date of birth in Item W4. For Item W5, Date of Admission, enter the date of birth if the infant is born in your hospital. If the infant is born elsewhere, enter the date that the infant was admitted to your hospital. For Item W6, Date of Day 28, enter the date on which the infant is 28 days old using the calculation chart in Appendix E. The Date of Day 28 is used when determining whether the infant had a cranial imaging on or before Day 28. Cranial Imaging on or before Day 28 is an item on the 28 Day Form. NOTE: The Date of Day 28 is determined by using the calendar date of birth as day 1, regardless of the time of birth, and adding 27 to this date. Thus, for an infant born at 11:59 PM on September 1, day 1 is September 1. Day 28 for this infant is September
38 For Item W7, enter the Date of Week 36. The Date of Week 36 is used when determining whether the infant was on oxygen on the date of week 36. Oxygen at 36 Weeks is an item on the Discharge Form. The calculation charts in Appendix F are used to determine this date after you have determined the infant s gestational age in rounded weeks. o First determine the best estimate of gestational age, item 2 on the 28 Day Form and round to the nearest week. NOTE: If the rounded gestational age is 37 weeks or more, leave item W7 blank if you submit data on paper forms, or enter the code for Not Applicable for the Date of Week 36 if you submit data electronically. o If the rounded gestational age is less than 36 weeks, use the Calculation Charts in Appendix F to find the date of week 36 that corresponds to the rounded gestational age. For Item W8, enter the Date of Initial Disposition. The Date of Initial Disposition is the date that the infant was discharged home from your hospital, transferred to another hospital, died in your hospital or the date of the infant s first birthday if still hospitalized, whichever comes first. This date is used to calculate the infants Initial Length of Stay on the Discharge Form. NOTE: Infants transferred from one unit in your hospital to another unit within your hospital are not considered to have been transferred or discharged. For Item W9, if the infant is transferred from your center to another hospital, enter the date that the infant was discharged home, died or reached his or her first birthday (if still hospitalized), whichever comes first. This date is used to calculate the infant s Total Length of Stay on the Transfer and Readmission Form. 30
39 Figure 6.3: Patient Identification Worksheet 31
40 Length of Stay Calculation Worksheet The Length of Stay Calculation Worksheet (Figure 6.4) is used to calculate the Initial Length of Stay and, if the infant transfers to another hospital, the Total Length of Stay. The Initial Length of Stay is reported on the Discharge Form. The Total Length of Stay is reported on the Transfer and Readmission Form. NOTE: Do not submit the Length of Stay Calculation Worksheet to the Network. This worksheet contains personal patient identifiers and must be treated as protected health care information. Vermont Oxford Network does not accept protected health care information. Figure 6.4: Length of Stay Calculation Worksheet 32
41 The Length of Stay Calculation Worksheet is divided into two parts. Use Part A to calculate the Initial Length of Stay for all eligible infants and to answer the Initial Length of Stay item on the Discharge Form. Use Part B only for infants who transfer from your center to another hospital when calculating the Total Length of Stay item on the Transfer and Readmission Form. To complete this worksheet, you will need to use the Day Number Chart in Appendix G to convert dates such as the Date of Admission and the Date of Initial Discharge, Transfer, or Death into Day Numbers. Each date in Appendix G lists the corresponding Day Number for each date in 2009 and The Day Number is assigned sequentially to each date starting with January 1, 2009 (Day Number =1) and ending with December 31, 2010 (Day Number = 730). Guidelines for Completing the Length of Stay Calculation Worksheet Complete Part A, Initial Length of Stay, for all eligible infants. o o o o o o Enter the Date of Initial Discharge, Transfer or Death, as recorded in Item W8 on the Patient Identification Worksheet. If an infant is still hospitalized on his or her first birthday, and has not been home, enter the date of the infant s first birthday in the Date of Initial Discharge, Transfer or Death (W8). Enter the Day Number for the date recorded in step 1 in the boxes to the right of this date. Use the Day Number Chart in Appendix G to determine the Day Number. Enter the Date of Admission to your hospital as recorded in Item W5 on the Patient Identification Worksheet. For inborn infants, the Date of Admission is the Date of Birth. For outborn infants, the Date of Admission is the date the infant was admitted to your hospital. Enter the Day Number for the date as recorded in step 3 in the boxes to the right of this date. Use the Day Number Chart in Appendix G to determine the Day Number. Subtract the Day Number for Date of Admission from the Day Number for Date of Initial Discharge, Transfer or Death. Enter the result in the boxes below the Day Numbers. Add one day. o Enter the sum in boxes for the Initial Length of Stay, Item L1. Complete Part B, Total Length of Stay, for infants who transfer from your center to another hospital regardless of disposition after transfer. o Enter the Date of Final Discharge or Death, as recorded in Item W9 on the Patient Identification Worksheet. If an infant who transfers is still hospitalized on his or her first birthday, and has not been home, enter the date of the infant s first birthday in the Date of Final Discharge (W9). NOTE: If the Date of Final Discharge or Death is Unknown, Total Length of Stay will also be Unknown. 33
42 o o o o o o Enter the Day Number for the date recorded in step 1 in the boxes to the right of this date. Use the Day Number Chart in Appendix G to determine the Day Number. Enter the Date of Admission to your hospital as recorded in Item W5 on the Patient Identification Worksheet. For inborn infants, the Date of Admission is the Date of Birth. For outborn infants, the Date of Admission is the date the infant was admitted to your hospital. Enter the Day Number for the date recorded in step 3 in the boxes to the right of this date. Use the Day Number Chart in Appendix G to determine the Day Number. Subtract the Day Number for the Date of Admission from the Day Number for the Date of Final Discharge or Death. Enter the result in the boxes below the Day Numbers. Add one day. Enter the sum in the boxes for Item L2, Total Length of Stay. Completing the Delivery Room Death Booklet Patient Identification Worksheet The Patient Identification Worksheet in the Delivery Room Death Booklet (Figure 6.5) is used to record patient information for infants who meet the delivery room death criteria described in Chapter 5, Table 5.3. This worksheet is on the front cover of the booklet. It lists the Patient s Name, Mother s Name, Patient Medical Record Number and Patient Date of Birth. NOTE: Do not submit the Delivery Room Death Patient Identification Worksheet to the Network. This worksheet includes confidential patient information. The Vermont Oxford Network does not accept protected health care information. Guidelines for Completing the Delivery Room Death Patient Identification Worksheet Check the Patient Identification Worksheet with the Patient Log to ensure consistency of information in the logs, worksheets, and forms. Enter your VON Center Number. This number was assigned when your center joined the Network. Enter the Network ID Number that was assigned to the infant in the Patient Log Enter the Patient s name in Item W1. Enter the Mother s name in Item W2. Enter the Patient s Medical Record Number in Item W3. Enter the Patient s date of birth in Item W4. 34
43 Figure 6.5: Delivery Room Death Patient Identification Worksheet 35
44 CHAPTER 7 Submitting Data to the Network Introduction In order to provide accurate indicators of your hospital s performance, it is important that the data submitted by your hospital be complete and correct. This in turn requires that your staff understand the data item definitions in Chapter 8, that all eligible infants be identified and that procedures and events are accurately recorded. Records and Data Items The data in the Network s databases are organized into individual infant records, and each record includes all the data items on the various data forms: 28 Day Form, Discharge Form, Transfer and Readmission Form and Supplemental Data Form. Each record is uniquely identified by your VON center number, which was assigned when your hospital joined the Network, and by the infant s Network ID Number, which your center assigns as a sequential number to each eligible infant. A data item contains a single piece of information within a record. Each data item is identified by a number and a name. For instance, Item 1 is Birth Weight and is on the 28 Day Form. Some form numbers include multiple data items. For instance, the Initial Resuscitation Item on the Discharge Form includes five data items. Data items that do not apply are coded as Not Applicable or N/A in the databases. For example, for infants that do not transfer from your hospital to another hospital, all items on the Transfer and Readmission Form are N/A. If your center only participates in the VLBW Database, all items on the Supplemental Data Form are N/A. For infants who meet the delivery room death criteria described in Chapter 5, Table 5.3, only items on the Delivery Room Death Form are applicable. Ways of Submitting Data If your hospital participates in the VLBW Database, you may submit data to the Network either electronically or on paper forms. Most centers submit electronically using the Network s enicq software, which is available to all members at no charge, or you may use other software to send data electronically. If you use software other than enicq, or to understand more about electronic submission, please refer to the Member Instructions for Submitting Electronic Data in 2009, which is available on the Network web site, (click on Member Tools/Downloads/EDS Instructions). If your hospital participates in the Expanded Database, you may only submit data electronically. Guidelines for Data Submission Figure 7.1 shows which forms are applicable for data submission depending on the infant s birth status and disposition when leaving your hospital. Use this figure and the guidelines in Tables 7.1 and 7.2 when submitting data to the Network. 36
45 Patient Eligible? No Do not include in VON Database Patient Log 001 Janet Smith 002 Sam Jones Yes Patient: Sam Jones Network ID: 002 DR Death? Delivery Room Death Booklet Delivery Room Death Patient ID Worksheet Items W1 - W4 Patient Data Booklet Patient ID Worksheet Items W1 - W9 Delivery Room Death Form All Delivery Room Death Form Items Length of Stay Worksheet L1 Initial Length of Stay L2 Total Length of Stay 28 Day Form If your center is an Expanded Database participant, or if your center submits NER data and infant is eligible for NER, provide Supplemental Data. All 28 Day Form Items Discharge Form All Discharge Form Items Supplemental Data Form Supplemental Data Items S2.B1 - S2.B2 If your center is an Expanded Database participant, provide Supplemental Data. If the patient is transferred to another hospital, complete the Transfer and Readmission Form. For all infants readmitted for the first time, update items on the 28 Day Form and the Discharge Form as specified in Chapter 7. Keep at your center Submit to Network Instructions Supplemental Data Form All Supplemental Data Items Transfer and Readmission Form Part A: All Transfers Part B: Readmitted Part C: Transferred More than Once Part D: All Transfers Transfer Log 002 Sam Jones 011 Gil Smart 014 Celia Lopez Figure 7.1: Completing the Network s Forms 37
46 General Guidelines for Completing and Submitting Data Forms 1. Collect and submit data for eligible infants only. Eligibility criteria depend on whether your center participates in the VLBW Database or Expanded Database, as well as whether the infant is included in the Neonatal Encephalopathy Registry. See Chapter 5 for eligibility criteria. 2. Follow the guidelines in Chapter 6 to keep track of eligible infants. Use the logs and worksheets to keep track of patients and data submissions. Do not submit the patient worksheets or logs to the Network. These include personal patient identifiers and must be retained at your hospital. Vermont Oxford Network does not accept protected health care information. 3. For each eligible infant, complete the data forms that are applicable. When completing the data forms, understand and carefully apply the data definitions in Chapter 8 for items on the data forms. This will assure that data submitted by your hospital are comparable to other hospitals in the Network. 4. The data forms may include different data items from year to year. Use the appropriate forms and database documentation for each infant, based on the infant s year of birth. For infants born in 2009, use the data forms shown in this manual. Always use the forms in the Manual of Operations that matches the infant s birth year. 5. Code data items as Unknown only if the answer to an item is truly unknown and cannot be obtained. Do not code items as unknown to indicate temporary or pending values in electronic files. Leave these items blank until an answer is known. 6. To encourage data accuracy, complete data forms while the infant is hospitalized and when procedures are done or events are observed. 7. Use the calculation charts in Appendices E, F, and G to calculate the Date of Day 28, the Date of Week 36, and the Day Number Chart for calculating Initial and Total Length of Stay if your data entry program does not automatically calculate these values for you. 8. When completing the data forms for eligible outborn infants who transferred to your hospital, record events that occurred in the transferring hospital as well as at your own hospital after admission. For example, if an infant received Indomethacin at the transferring hospital, answer this data item Yes on the Discharge Form. If the infant had a cranial ultrasound exam at the transferring hospital, answer this item Yes on the 28 Day Form and record the worst grade of PIH. 9. For eligible inborn infants who meet the delivery room death criteria described in Chapter 5, Table 5.3, use the Delivery Room Death Form rather than the 28 Day Form and Discharge Form. Complete the 28 Day Form and Discharge Form for all other eligible infants. See Figure For infants who transfer from your hospital to another hospital, follow the guidelines in Table 7.2. Table 7.1: General Guidelines for Completing and Submitting Data Forms 38
47 Guidelines for Infants Who Transfer from Your Hospital 1. Complete Part A of the Transfer and Readmission Form for all infants who transfer from your center to another hospital. NOTE: Infants who transfer from one unit to another within your hospital are not considered to have been transferred. Only use the Transfer and Readmission Form for infants who transfer from your center to another hospital. 2. Complete Part B of the Transfer and Readmission Form for all infants who are readmitted to your hospital after initial transfer. NOTE: Readmitted after initial transfer means that the infant s Initial Disposition is transferred to another hospital and that the infant was readmitted to your center after this initial transfer without having gone home or transferred again prior to readmission. For example, if the infant transferred from your center to hospital B and was readmitted to your center from hospital B, the infant was readmitted after initial transfer. But if the infant transferred from hospital B to hospital C prior to being readmitted to your center, the infant would not be considered to have been readmitted after initial transfer. When infants are readmitted to your hospital, there are other data collection considerations: a. If an infant is transferred from your center to another hospital and is not readmitted after initial transfer, the data collected on the 28 Day Form and the Discharge Form should only reflect events which occur prior to initial transfer. b. If the infant is readmitted to your hospital after initial transfer, (1) Update Items 17, 18 and 19 on the 28 Day Form and Items 21 through 46 on the Discharge Form to reflect events at the transferred-to hospital, as well as events at your hospital following readmission, until the Disposition After Readmission occurs (Item 54). (2) Do not change Items 47 through 50 on the Discharge Form based on events following transfer or readmission. Items 47 through 50 should reflect the Status at Initial Disposition, prior to transfer from your center. (3) If your center participates in the Expanded Database, update the Items S2.A (Hypoxic-Ischemic Encephalopathy) and S2.C (Seizures) on the Supplemental Data Form for eligible infants to reflect events at the transferred to hospital and events at your hospital following readmission. Update the Item S1.B (ECMO at Your Hospital) if ECMO is done at your hospital following readmission after initial transfer. (4) Do not update items on the 28 Day Form, Discharge Form or Supplemental Data Form based on events following transfer if the infant is not readmitted to your hospital, if the infant is transferred more than once prior to readmission to your hospital or after the infant is transferred again following readmission. 3. Complete Part C of the Transfer and Readmission Form for infants who transfer more than once. For example, if an infant transfers from your hospital to hospital B and then transfers again to hospital C, or if an infant is readmitted to your hospital following initial transfer to hospital B and then transfers again either back to hospital B or to hospital C, you should complete Part C of the form. Table 7.2: Guidelines for Infants Who Transfer from Your Hospital 39
48 Submitting Data Using Paper Forms If you submit data on paper forms, please note the following guidelines: a. Use the Patient Log and the Transfer Log to keep track of form submissions. b. If a form for a particular patient has already been sent, do not send another copy, except when you are updating or correcting previously submitted data. c. Submit your records in numerical sequence. Keep all Network IDs in numerical order when you submit data. d. Submit forms that are as complete as possible and check them for accuracy. e. If you choose to fax data forms to the Network, do not fax colored paper. The quality is generally poor. Try making white copies and faxing those for better resolution. f. Be sure that all responses are easy to read. g. Do not use the following symbols: >, <,,, +, -, Ø,. These symbols will be coded as errors. h. Do not use decimal points or commas when you record infant weights. i. If you revise a previously submitted form, please cross out or white-out the incorrect answer. Then circle or highlight revised data items on the forms to indicate revisions to previously submitted data. j. If Parts B and/or C of the Transfer and Readmission Form don t apply to an infant who transfers, leave the items in these sections blank when submitting the Transfer and Readmission Form. Completing the 28 Day Form Data on the 28 Day Form must be submitted for each eligible infant who does not meet the Delivery Room Death Criteria that are described in Chapter 5, Table 5.3. The 28 Day Form includes demographic data and other data available within 28 days of birth. This form does not contain personal patient identifiers. The 28 Day Form for infants born in 2009 is shown in Figure 7.2. Use the definitions in Chapter 8 when recording data on the 28 Day Form. For database integrity and accuracy of reporting, assure that the data item definitions are understood and uniformly applied by staff members who are recording these data. 40
49 Figure 7.2: 28 Day Form for Infants Born in 2009 Completing the Discharge Form Data on both pages of the Discharge Form (Figures 7.3 and 7.4) must be submitted for each eligible infant who does not meet the Delivery Room Death Criteria as described in Chapter 5, Table 5.3. Page 1 of the form includes the Interventions section; Page 2 includes the Diagnoses and Discharge sections. Use the definitions in Chapter 8 when recording data on the Discharge Form. For database integrity and accuracy of reporting, assure that the data item definitions are understood and uniformly applied by staff members who are recording these data. 41
50 Figure 7.3: Discharge Form for Infants Born in 2009, Page 1 42
51 Figure 7.4: Discharge Form for Infants Born in 2009, Page 2 43
52 Completing the Transfer and Readmission Form NOTE: The Transfer and Readmission Form is printed separately and can be found in Appendix A or printed from our website. Refer to the guidelines in Table 7.2 earlier in this chapter for guidelines when collecting data when infants are transferred from your hospital. Data on the Transfer and Readmission Form must be submitted for each infant who transfers from your hospital to another hospital. Use the definitions in Chapter 8 when recording data on the Discharge Form. For database integrity and accuracy of reporting, assure that the data item definitions are understood and uniformly applied by staff members who are recording these data. The data items in Parts A and D of the Transfer and Readmission Form are applicable to and should be completed for all infants who transfer. The data items in Part B are only applicable to infants who are readmitted to your center following initial transfer. See Table 7.2 earlier in this chapter for guidelines. Complete Part B if an infant is readmitted to any location in your hospital after initial transfer. Locations in your hospital to which the infant may be readmitted include the neonatal intensive care unit, a step-down unit, newborn nursery, intermediate care area, pediatric intensive care unit, pediatric ward, or any other location where care is given. Check these locations as necessary to collect data for all readmissions. If the infant is readmitted after initial transfer and subsequently is discharged home, dies or is still in your hospital as of first birthday, complete Parts B and D of the Transfer and Readmission Form and submit the data items to the Network. The data item in Part C is only applicable for infants who have been transferred more than once. This includes infants who transfer from your center to another hospital and subsequently are transferred again, as well as infants who have been transferred to another hospital, readmitted to your hospital, and subsequently transferred again. Periodically check with hospitals to which infants are transferred to determine their disposition. When the Ultimate Disposition is known, complete Parts C and D of the Transfer and Readmission Form and submit the data items to the Network. Use the Length of Stay Calculation Worksheet (Chapter 6) to calculate the Total Length of Stay in Part D of the Transfer and Readmission Form. 44
53 Figure 7.5: Transfer and Readmission Form for Infants Born in
54 Completing the Supplemental Data Form The Supplemental Data Form is completed for all eligible infants by members at centers participating in the Expanded Database. If your center participates in the Expanded Database, the data items on the Supplemental Data Form are applicable to all eligible infants at your center. Items on the Supplemental Data Form are submitted electronically. A paper version of the Supplemental Data items is provided to assist members in collecting data and in creating an electronic data form. Refer to the separately published document, Member Instructions for Submitting Electronic Data in 2009, for appropriate item response codes and for unknown and N/A codes. This document is available on under Member Tools/Downloads. Figure 7.6 shows the Supplemental Data Form for infants born in Use the definitions in Chapter 8 when recording data on the Supplemental Data Form. For database integrity and accuracy of reporting, assure that the data item definitions are understood and uniformly applied by staff members who are recording these data. For infants who meet the delivery room death criteria described in Chapter 5, Table 5.3, Items S2.B1 and S2.B2 on the Supplemental Data Form are applicable. Figure 7.6: Supplemental Data Form for Infants Born in
55 Completing the Delivery Room Death Form For eligible infants who meet the delivery room death criteria described in Chapter 5, Table 5.3, the only data items that are applicable are those on the Delivery Room Death Form (Figure 7.7) and, if your center participates in the Expanded Database, two items on the Supplemental Data Form (Items S2.B1 and S2.B2). The Delivery Room Death Form includes items from the 28 Day Form and Discharge Form that are applicable to infants who meet these criteria. All of these items must be submitted for eligible infants who meet the delivery room death criteria. Figure 7.7: Delivery Room Death Form 47
56 CHAPTER 8 Definitions of Data Items Introduction Each data item has its own data definition, a precise explanation of the information required for the item. As you enter data, use the data definitions presented in this chapter as a reference. Read the explanations carefully so that you understand the details for each item. To assure data integrity and accuracy of reports to your hospital, it is very important that the definitions provided in this chapter be followed as closely as possible. If you have any questions about these definitions, please contact your VON Account Manager. 28 Day Form Data Definitions Some items on the 28 Day Form do not apply to infants who not meet the delivery room death criteria described in Chapter 5, Table 5.3. Use the Delivery Room Death Form for these infants. You should also be familiar with the instructions in Chapter 7 when completing the 28 Day Form. ITEM 1: Birth Weight Record the birth weight in grams. Since many weights may be obtained on an infant shortly after birth, enter the weight from the Labor and Delivery record if available and judged to be accurate. If unavailable or judged to be inaccurate, use the weight on admission to the neonatal unit or lastly, the weight obtained on autopsy (if the infant expired within 24 hours of birth). ITEM 2: Gestational Age Record the best estimate of gestational age in weeks (Item 2a) and days (Item 2b) using the following hierarchy: 1. Obstetrical measures based on last menstrual period, obstetrical parameters, and prenatal ultrasound as recorded in the maternal chart. 2. Neonatologist s estimate based on physical criteria, neurologic examination, combined physical and gestational age exam (Ballard or Dubowitz), or examination of the lens. The best estimate should be recorded in weeks and days. In instances when the best estimate of gestational age is an exact number of weeks, enter the number of weeks in the space provided for weeks and enter 0 in the space provided for days. Do not leave the number of days blank. 48
57 ITEM 3: Died in Delivery Room Check "Yes" if the infant was born in your center, was never admitted to the NICU, and died in the delivery room or at any other location in your hospital within 12 hours after birth. These locations may include the mother s room, resuscitation rooms or any location other than the NICU in your hospital. NOTE: If the infant meets the above criteria, do not use the 28 Day Form or Discharge Form. Use the Delivery Room Death Form instead. Check "No" if the infant did not die in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU. Check No for all outborn infants. If No, continue to complete the 28 Day and Discharge Forms. ITEM 4a. Location of Birth Check "Inborn" if the infant was delivered at your center. Check "Outborn" if the infant was delivered outside your center. Any infant requiring ambulance transfer will be considered outborn. When completing the Network data forms for outborn infants, use all information available from the hospital that transferred the infant to your center as well as from your own hospital. ITEM 4b: If Outborn, Day of Admission to Your Hospital For outborn infants only, Day of Admission is the day of life on which the infant is admitted to your hospital. The Date of Birth is day 1. For example, if an outborn infant is born on June 1, and admitted to your hospital on June 1, the Day of Admission would be 1. If that same infant were admitted on June 3, the Day of Admission would be 3. To determine the Day of Admission for outborn infants you must know the Date of Birth and the Date of Admission. The time of birth does not matter. If the infant is born at 11:30 PM and admitted to your hospital at 11:59 PM on the same day, the Day of Admission is 1, since the infant was admitted on the Date of Birth. NOTE: This item applies only to outborn infants. The acceptable range for Day of Admission is from 1 (for infants admitted on their Date of Birth) to 28, (since outborn infants admitted more than 28 days after birth are not eligible for the database). ITEM 4c: If Outborn, Transfer Code of Center from which Infant Transferred If the infant is outborn, enter the Transfer Code of the VON center or other location from which the infant transferred. The Transfer Code may be accessed at this website address: 49
58 ITEM 5: Head Circumference at Birth Enter the head circumference to the nearest tenth of a centimeter as recorded in the chart or clinical flow sheets on the day of birth. If the head circumference is not recorded on the day of birth, record the first head circumference measurement on the following day. If the head circumference is not measured on the day of birth or on the following day, record as unknown. ITEM 6a. Ethnicity of Mother The response to this item should be obtained by personal interview with the mother or review of the birth certificate or medical record, in that order of preference. Check "Hispanic" if the biological mother is a person of Cuban, Mexican, Puerto Rican, South or Central American or other Spanish culture or origin, regardless of race. Check "Not Hispanic" if the biological mother s ethnicity is not of Hispanic or Latino origin as defined above. ITEM 6b. Race of Mother (check only one) The response to this item should be obtained by personal interview with the mother or review of the birth certificate or medical record, in that order of preference. Check "Black" if the biological mother is a person having origins in any of the original peoples of Africa. Check "White" if the biological mother is a person having origins in any of the original peoples of Europe, the Middle East, North Africa (Arabic origins) or Western Russia (including Afghanistan and South Russia). Check "Asian or Pacific Islander" if the biological mother is a person having origins in the original peoples of the Far East, Southeast Asia, the Indian Subcontinent or the Pacific Islands. This includes Cambodia, China, Guam, Hawaii, India, Japan, Korea, Laos, Philippines, Samoa, Thailand, Vietnam or any Pacific Island. Check "Native American" if the biological mother is an American Indian or Alaskan Native. Check "Other" if none of the race categories above applies to the biological mother. ITEM 7: Prenatal Care Check "Yes" if the mother received any prenatal obstetrical care prior to the admission during which birth occurred. Check "No" if the mother did not receive any prenatal obstetrical care. 50
59 ITEM 8: Antenatal Steroids Check "Yes" if corticosteroids were administered IM or IV to the mother during pregnancy at any time prior to delivery. Corticosteroids include betamethasone, dexamethasone, and hydrocortisone. Check "No" if no corticosteroids were administered IM or IV to the mother during pregnancy at any time prior to delivery. ITEM 9: Chorioamnionitis Check "Yes" if a diagnosis of chorioamnionitis was recorded in the maternal or infant medical record. Check "No" if a diagnosis of chorioamnionitis was not recorded in the maternal or infant medical record. ITEM 10: Maternal Hypertension, Chronic or Pregnancy-Induced Check "Yes" if maternal hypertension, chronic or pregnancy-induced, with or without edema and proteinuria, was recorded in the maternal or infant medical record, or if a maternal blood pressure above 140 systolic or 90 diastolic was recorded prior to or during the present pregnancy. Check "No" if maternal hypertension, chronic or pregnancy induced, with or without edema and proteinuria, was not recorded in the maternal or infant medical record, and if a maternal blood pressure above 140 systolic or 90 diastolic was not recorded prior to or during the present pregnancy. NOTE: Eclampsia and pre-eclampsia should be considered forms of pregnancyinduced hypertension. ITEM 11: Mode of Delivery Check "Vaginal" for any vaginal delivery (spontaneous or induced). Check "Cesarean Section" for any cesarean delivery (elective or emergent). ITEM 12: Sex of Infant Check "Male" or "Female". ITEM 13a. Multiple Gestation Check "Yes" if two or more live fetuses were documented at any time during the pregnancy which resulted in the birth of the infant. Otherwise check "No". ITEM 13b: If Multiple Gestation, Number of infants delivered If Multiple Gestation is answered "Yes", enter the number of infants actually delivered (count both live born and stillborn infants). For example, if twins were delivered, enter 2 ; if triplets were delivered, enter 3. Do not count fetuses which have been reabsorbed in utero and are not delivered. This item is not applicable if Multiple Gestation is answered "No". 51
60 ITEM 14: APGAR Scores Enter the APGAR score at 1 minute and at 5 minutes as noted in the Labor and Delivery record. ITEM 15: Initial Resuscitation NOTE: Initial Resuscitation refers to interventions performed in the delivery room or in an initial resuscitation area immediately following birth and prior to admission to the NICU. There are situations in which infants receive their initial neonatal resuscitation in locations other than a delivery room. These include cases in which birth occurs outside of a delivery room (home, automobile, ambulance, hospital room, emergency room, etc.) and cases in which resuscitation is provided in locations adjacent to or close-by the delivery room. In such situations, the responses to the Initial Resuscitation items should be based on the initial resuscitation provided immediately after birth, regardless of where the resuscitation took place. Check "Yes" for all interventions that apply. ITEM 15a. Oxygen Check "Yes" if the infant received any supplemental oxygen in the delivery room or during the initial resuscitation performed immediately after birth. Check "No" if the infant did not receive supplemental oxygen in the delivery room or during the initial resuscitation performed immediately after birth. ITEM 15b. Face Mask Ventilation Check "Yes" if the infant received any positive pressure breaths via a face mask in the delivery room or during the initial resuscitation performed immediately after birth. Positive pressure may be administered using a resuscitation bag or other device that generates intermittent positive pressure. Check "No" if the infant did not receive any positive pressure breaths via a face mask in the delivery room or during the initial resuscitation performed immediately after birth. Check "No" if a face mask was only used to administer CPAP (continuous positive airway pressure) and no positive pressure breaths were given. ITEM 15c. Endotracheal Tube Ventilation Check "Yes" if the infant received ventilation through an endotracheal tube in the delivery room or during the initial resuscitation performed immediately after birth. Check "No" if the infant did not receive ventilation through an endotracheal tube in the delivery room or during the initial resuscitation performed immediately after birth. If an endotracheal tube was placed only for suctioning and assisted ventilation was not given through the tube, check "No". 52
61 ITEM 15d. Epinephrine Check "Yes" if epinephrine was given in the delivery room or during the initial resuscitation performed immediately after birth via intravenous, intracardiac or intratracheal (through an endotracheal tube) routes. Check "No" if epinephrine was not given in the delivery room or during the initial resuscitation performed immediately after birth via intravenous, intracardiac or intratracheal routes. ITEM 15e. Cardiac Compression Check "Yes" if external cardiac massage was given in the delivery room or during the initial resuscitation performed immediately after birth. Check "No" if external cardiac massage was not given in the delivery room or during the initial resuscitation performed immediately after birth. ITEM 16a. Temperature Measured within the First Hour after Admission to Your NICU NOTE: This item applies to the temperature of the infant during the first hour after admission to your NICU. Do not record temperature measurements taken at the transferring center for outborn infants. Check "Yes" if the infant s core body temperature was measured and recorded within the first hour after admission to your NICU. Core body temperature may be measured by taking a rectal, esophageal, tympanic or axillary temperature. NOTE: If an attempt was made to measure the temperature during the first hour after admission to your NICU, and the temperature of the infant was lower than the thermometer could measure, check Yes and record the lowest temperature on the thermometer in 16b. If the infant s core body temperature was not measured within the first hour after admission to the NICU, Item 16b. is not applicable and should be left blank on paper form submissions. Check "No" if the infant s core body temperature was not measured and recorded within the first hour after admission to your NICU. Check "N/A" if the infant is eligible but was never admitted to your NICU. 53
62 ITEM 16b. If Yes, enter first Temperature after admission If the infant s core body temperature was measured and recorded within the first hour after admission to your NICU, enter the infant s temperature in degrees centigrade to the nearest tenth of a degree. If the infant s temperature is measured multiple times within the first hour after admission to your NICU, enter the value of the first temperature measurement. For centers that measure temperature in degrees Fahrenheit, a Fahrenheit to Centigrade Conversion Table is provided in Appendix I. Use rectal temperature or, if not available, esophageal temperature, tympanic temperature or axillary temperature, in that order. ITEM 17: Bacterial Sepsis, Early (on or before Day 3 of life) Check "Yes" if a bacterial pathogen from the list in Appendix B was recovered from a blood and/or cerebrospinal fluid culture obtained on day 1, 2 or 3 of life. Check "No" if a bacterial pathogen from the list in Appendix B was not recovered from a blood culture or cerebrospinal fluid culture obtained on day 1, 2 or 3 of life, or if no blood or cerebrospinal fluid cultures were obtained on day 1, 2 or 3 of life. NOTE: The date of birth counts as day 1 regardless of the time of birth. For an infant born at 11:59 PM on September 1, day 3 will be September 3 rd. ITEM 18: Oxygen on Day 28 NOTE: Use the Date of Day 28 from the Patient Identification Worksheet, Item W6, and the criteria below when answering this question. This item is not applicable if: The infant is discharged home or dies prior to the Date of Day 28. The infant is transferred from your center to another hospital prior to the Date of Day 28 and either, o Is not readmitted to your center following initial transfer and before discharge home, death or first birthday, or o Is transferred a second time before the Date of Day 28. Otherwise the item is applicable. NOTE: Infants who are moved from one unit to another unit within your hospital are not considered to have been transferred. Check "Yes" if the item is applicable and the infant received any supplemental oxygen on the Date of Day 28. Check "No" if the item is applicable and the infant did not receive supplemental oxygen on the Date of Day 28. Check "Not Applicable" if the item is not applicable based on the criteria above. 54
63 ITEM 19a. Cranial Imaging (US/CT/MRI) on or before Day 28 NOTE: Use the date from the Patient Identification Worksheet, Item W6, (Date of Day 28) when completing this question. Check "Yes" if at least one cranial ultrasound, cranial CT or cranial MRI was performed on or before day 28. Check "No" if no cranial ultrasound, CT or MRI was performed on or before day 28. ITEM 19b. If Yes to Cranial Imaging, enter Worst Grade of PIH (0-4) If a cranial ultrasound, CT or MRI was performed on or before day 28, enter the worst grade based on any study using the criteria below. If multiple ultrasounds, CT scans or MRI s were done on or before day 28, record the most severe grade. Do not answer Worst Grade if the answer to Item 19a is "No". Grade 0: No subependymal or intraventricular hemorrhage Grade 1: Subependymal germinal matrix hemorrhage only Grade 2: Intraventricular blood, no ventricular dilation Grade 3: Intraventricular blood, ventricular dilation Grade 4: Intraparenchymal hemorrhage ITEM 19c. If PIH, Where First Occurred If the infant had a periventricular-intraventricular hemorrhage (PIH) documented on an ultrasound, CT or MRI on or before day 28, indicate where a PIH first occurred. Note that this item does not ask where the worst grade occurred but rather where any PIH (grades 1 to 4) first occurred. Answer either "Your Hospital" or "Other Hospital". This item is not applicable if no ultrasound, CT or MRI was done on or before day 28 or if no PIH occurred. If a PIH first occurred at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If a PIH first occurred at another hospital based on the following criteria, select "Other Hospital". When infants transfer to your hospital or are readmitted to your hospital after initial transfer, a PIH will be considered to have occurred at another hospital in the following situations: 1. If a PIH was first diagnosed on an ultrasound, CT or MRI at the other hospital either prior to admission to your hospital or prior to readmission following initial transfer. 2. If a PIH was first diagnosed on an ultrasound, CT or MRI within 4 hours of admission to your hospital. 55
64 ITEM 20: Died Within 12 Hours of Admission to Your NICU Check "Yes" if the infant died 12 hours or less from the time of admission to your NICU. NOTE: There may be eligible infants who die without ever having been admitted to your NICU. For eligible inborn infants who are never admitted to your NICU and who die within 12 hours of birth, use the Delivery Room Death Form rather than the 28 Day Form. For eligible outborn infants who are never admitted to your NICU, check Yes to Item 20 if they die within 12 hours of admission to your hospital and complete all Items on the 28 Day Form and Discharge Form. Check "No" if the infant did not die 12 hours or less from the time of admission to your NICU. End of 28 Day Form Definitions 56
65 Discharge Form Data Definitions Most items on the Discharge Form do not apply to infants who not meet the delivery room death criteria described in Chapter 5, Table 5.3. Use the Delivery Room Death Form for these infants. You should also be familiar with the instructions in Chapter 7 when completing the Discharge Form. ITEM 21: Respiratory Support after Leaving the Delivery Room ITEM 21a. Oxygen Check "Yes" if the infant was given supplemental oxygen at any time after leaving the Initial Resuscitation Area. Check "No" if the infant was never given supplemental oxygen after leaving the Initial Resuscitation Area. ITEM 21b. Conventional Ventilation (Con Vent) Check "Yes" if the infant was given intermittent positive pressure ventilation through an endotracheal tube with a conventional ventilator (IMV rate <240/minute) at any time after leaving the Initial Resuscitation Area. Check "No" if the infant was never given intermittent positive pressure ventilation through an endotracheal tube with a conventional ventilator (IMV rate <240/minute) after leaving the Initial Resuscitation Area. NOTE: Intermittent positive pressure ventilation (IPPV) via nasal prongs is not considered conventional ventilation. Synchronized intermittent positive pressure ventilation (SIMV) via nasal prongs is not considered conventional ventilation. ITEM 21c. High Frequency Ventilation (HIFI Vent) Check "Yes" if the infant received high frequency ventilation (IMV rate >240/minute) at any time after leaving the Initial Resuscitation Area. Check "No" if the infant never received high frequency ventilation (IMV rate >240/minute) after leaving the Initial Resuscitation Area. NOTE: High frequency ventilation via nasal prongs is not considered high frequency ventilation. ITEM 21d. High Flow Nasal Cannula Check "Yes" if the infant received air or oxygen (any FiO2) at a flow rate of one liter per minute or more via nasal cannula at any time after leaving the Initial Resuscitation Area. Check "No" if the infant did not receive air or oxygen (any FiO2) at a flow rate of one liter per minute or more via nasal cannula at any time after leaving the Initial Resuscitation Area. 57
66 ITEM 21e. Nasal IMV or Nasal SIMV Check "Yes" if the infant received intermittent positive pressure ventilation (intermittent mandatory ventilation or synchronized intermittent mandatory ventilation) via nasal prongs or other nasal device at any time after leaving the Initial Resuscitation Area. Check "No" if the infant did not receive intermittent positive pressure ventilation via nasal prongs or other nasal device at any time after leaving the Initial Resuscitation Area. NOTE: Nasal IMV or Nasal SIMV should be coded "Yes" if the infant receives positive pressure patterns that include two or more levels of positive pressure such as BiPAP or SiPAP. Intermittent positive pressure ventilation (IPPV) via nasal prongs is not considered conventional ventilation. Synchronized intermittent positive pressure ventilation (SIMV) via nasal prongs is not considered conventional ventilation. ITEM 22a. Nasal CPAP NOTE: Nasal IMV (intermittent mandatory ventilation) and nasal SIMV (synchronized intermittent mandatory ventilation) are both considered forms of nasal CPAP for the purpose of this definition. High flow nasal cannula oxygen is NOT considered nasal CPAP for the purpose of this definition. Check "Yes" if the infant was given continuous positive airway pressure applied through the nose at any time after leaving the Initial Resuscitation Area. Check "No" if the infant was never given continuous positive airway pressure applied through the nose after leaving the Initial Resuscitation Area. ITEM 22b. If yes, Nasal CPAP before ETT Ventilation Check "Yes" if the infant was given continuous positive airway pressure applied through the nose without having previously received intermittent positive pressure breaths through an endotracheal tube. NOTE: Intermittent positive pressure breaths refer to assisted breaths given through an endotracheal tube using a mechanical ventilator or by using a bag. Check "No" if the infant received intermittent positive pressure breaths through an endotracheal tube before being given continuous positive airway pressure applied through the nose. 58
67 Item 22b is only completed when the answer to Item 22a is "Yes". When responding to Item 22b, the important point is whether the Nasal CPAP was given before or after assisted positive pressure breaths through an endotracheal tube. If an infant was first treated with Nasal CPAP and later was intubated and ventilated, the response to Item 22b would be "Yes". If an infant was treated with Nasal CPAP and never was subsequently intubated the response to Item 22b would also be "Yes". If an infant was intubated and given intermittent positive pressure breaths through the endotracheal tube and then later received Nasal CPAP, the response to Item 22b would be "No". If an infant was intubated in the Initial Resuscitation Area solely for suctioning meconium, this does not count as prior intubation when responding to Item 22b. Thus, for an infant suctioned for meconium via an endotracheal tube who had the tube removed immediately after the suctioning was completed and who was later treated with Nasal CPAP the response to Item 22b would be "Yes" if the infant was subsequently ventilated. ITEM 23a. Surfactant in the DR Check "Yes" if surfactant was administered to the infant in the delivery room or as part of the stabilization immediately after birth even if that occurred in a location other than the delivery room. Check "No" if surfactant was not administered when the infant was in the delivery room or as part of the stabilization immediately after birth. NOTE: The initial resuscitation and stabilization of infants immediately after birth may occur in locations other than a delivery room. These may include a designated resuscitation area, hospital room, emergency room, operating room, ambulance, etc. If surfactant is administered during stabilization and resuscitation immediately following birth, the answer to this question is "Yes" regardless of location. If the stabilization immediately after birth occurs in a delivery room, resuscitation room or other location and the infant is then transferred to the NICU for further stabilization during which surfactant is administered, check "No". ITEM 23b. Surfactant at Any Time Check "Yes" if the infant received an exogenous surfactant at any time. If the answer to question 23a. is "Yes", 23b. must also be answered "Yes". Check "No" if the infant never received an exogenous surfactant. 59
68 ITEM 23c. and ITEM 23d. If "Yes" to 23b, Enter Age at First Dose If surfactant was given at any time, enter the infant s postnatal age in hours and minutes at the time when the first dose of surfactant was administered. For inborn infants, the first dose may have occurred prior to or after NICU admission. For outborn infants, the first dose may have occurred before transfer, during transport or at your hospital. Do not answer this item if the answer to Surfactant at Any Time is "No". The postnatal age at first dose is the interval in hours and minutes, to the nearest minute, between the date and time of birth and the date and time at which the first dose was given. If the postnatal age at the time of the first dose was exact in hours, a 0 should be entered in the minutes portion of this item. Do not leave hours or minutes blank. If the precise age at first dose is unknown, but an estimated age at first dose can be reliably determined to the nearest 15 minutes, please record this estimate. If the best estimate of age at first dose to the nearest 15 minutes cannot be determined, write the word "Unknown" next to Item 23c and 23d for paper form submissions, or use the appropriate unknown code for electronic data submissions. EXAMPLE 1: An infant is born at 15:30 hours on October 1 in your hospital. The first dose of surfactant is given at 15:45 hours on October 1 in the delivery room. The postnatal age at first dose is 0 hours and 15 minutes. EXAMPLE 2: An infant is born at 15:30 hours on October 1 in an outlying hospital. The first dose of surfactant is given at 15:45 hours on October 1 in the delivery room at that hospital. The infant is subsequently transferred to your hospital. The postnatal age at first dose is 0 hours and 15 minutes. EXAMPLE 3: An infant is born at 15:30 hours on October 1. The first dose of surfactant is given at 15:00 hours on October 4. The age at first dose is 71 hours and 30 minutes. EXAMPLE 4: An infant is born at 15:30 hours on October 1. The first dose of surfactant is given at 16:30 hours on October 1. The age at first dose is 1 hour and 0 minutes. (Please record as 1 hour and 0 minutes, rather than 0 hours and 60 minutes.) ITEM 24a: Inhaled Nitric Oxide (ino) Check "Yes" if the infant received inhaled nitric oxide. Check "No" if the infant did not receive inhaled nitric oxide. 60
69 ITEM 24b: If Yes, where given (ino) If the infant received Inhaled Nitric Oxide (), indicate where was given. This item is not applicable if was not given. If was given only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If was given only at another hospital, select "Other Hospital". NOTE: ino will be considered to be given at another hospital in the following situations: 1. ino is given before being admitted to your hospital. 2. ino is given prior to readmission to your hospital after initial transfer. Select "Both" if was given both at your hospital and at another hospital as defined above. ITEM 25: Oxygen at 36 Weeks (Corrected Gestational Age) NOTE: Use the Date of Week 36 from the Patient Identification Worksheet, Item W7, and the criteria below when answering this question. This item is not applicable if: The infant s gestational age in rounded weeks is greater than 36 weeks. The infant is discharged home or dies prior to the Date of Week 36. The infant is transferred from your center to another hospital prior to the Date of Week 36 and either, o Is not readmitted to your center before discharge home, death or first birthday, or o Is transferred a second time before the Date of Week 36. Otherwise the item is applicable. NOTE: Infants who are moved from one unit to another unit within your hospital are not considered to have been transferred. For infants who are readmitted to your center, see instructions for the Transfer and Readmission Form, Part B, in Chapter 7. Check "Yes" if the item is applicable and the infant received any supplemental oxygen on the Date of Week 36. Check "No" if the item is applicable and the infant did not receive supplemental oxygen on the Date of Week 36. Check "Not Applicable" if the item is not applicable based on the criteria above. 61
70 ITEM 26a: Steroids for CLD Check "Yes" if systemic corticosteroids were used after birth to treat or prevent bronchopulmonary dysplasia or chronic lung disease. Check "No" if systemic corticosteroids were not used after birth to treat or prevent bronchopulmonary dysplasia or chronic lung disease. Inhaled corticosteroids are not considered systemic corticosteroids. Thus, if an infant received inhaled corticosteroids but did not receive systemic corticosteroids after birth to treat or prevent bronchopulmonary dysplasia or chronic lung disease, then the answer to Item 26 is "No". ITEM 26b: If Yes, where given (Steroids for CLD) If Steroids for CLD is answered "Yes", indicate where steroids for CLD were given. This item is not applicable if the infant did not receive steroids for CLD. If Steroids for CLD are given only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If Steroids for CLD are given only at another hospital, select "Other Hospital". NOTE: Steroids for CLD will be considered to be given at another hospital in the following situations: 1. Steroids for CLD is given before being admitted to your hospital. 2. Steroids for CLD is given prior to readmission to your hospital after initial transfer. Select "Both" if Steroids for CLD are given both at your hospital and at another hospital as defined above. ITEM 27: Indomethacin for Any Reason Check "Yes" if Indomethacin was administered after birth. The answer to this question may be "Yes" even if an infant did not meet the definition of PDA given in Item 36, Patent Ductus Arteriosus. Check "No" if Indomethacin was not administered after birth. NOTE: Ibuprofen should not be counted as Indomethacin. 62
71 ITEM 28: Ibuprofen for PDA Check "Yes" if Ibuprofen was administered at any time after birth for the prevention or treatment of PDA. The answer to this question may be "Yes" even if an infant did not meet the definition of PDA given for Patent Ductus Arteriosus in Item 36. Check "No" if Ibuprofen was not administered after birth for the prevention or treatment of PDA. NOTE: Ibuprofen use other than for the prevention or treatment of PDA should not be coded as "Yes" for this item. ITEM 29a. PDA Ligation Check "Yes" if surgical ligation of the ductus arteriosus was attempted either in the operating room or NICU. This item can be checked even if an infant did not meet the definition of PDA given for Item 36, Patent Ductus Arteriosus. Check "No" if surgical ligation of the ductus arteriosus was not attempted either in the operating room or NICU. ITEM 29b. If PDA Ligation, where done If PDA Ligation is answered "Yes", indicate where PDA ligation was done. This item is not applicable if PDA ligation was not done. If PDA Ligation is done only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If PDA Ligation is done only at another hospital, select "Other Hospital". NOTE: PDA Ligation will be considered to be done at another hospital in the following situations: 1. PDA Ligation is done before being admitted to your hospital. 2. PDA Ligation is done prior to readmission to your hospital after initial transfer. Select "Both" if PDA Ligation is done both at your hospital and at another hospital as defined above. 63
72 ITEM 30a. ROP Surgery Check "Yes" if retinal cryosurgery and/or laser surgery were performed for ROP. Check "No" if retinal cryosurgery and/or laser surgery were not performed for ROP. ITEM 30b. If Yes, where done (ROP Surgery) If ROP Surgery is answered "Yes", indicate where ROP surgery was done. This item is not applicable if ROP surgery was not done. If ROP Surgery is done only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If ROP Surgery is done only at another hospital, select "Other Hospital". NOTE: ROP Surgery will be considered to be done at another hospital in the following situations: 1. ROP Surgery is done before being admitted to your hospital. 2. ROP Surgery is done prior to readmission to your hospital after initial transfer. Select "Both" if ROP Surgery is done both at your hospital and at another hospital as defined above. ITEM 31: NEC Surgery Check "Yes" if one or more of the following procedures: laparotomy, laparoscopy, bowel resection or intraperitoneal drain placement was performed for necrotizing enterocolitis, suspected necrotizing enterocolitis, or bowel perforation. Enter the applicable surgical codes in Item 33. NOTE: If NEC Surgery is answered "Yes", at least one of the following surgery codes must be entered in Item 33: S302 Laparoscopy S303 Laparotomy S307 Jejunostomy, ileostomy, colonoscopy for intestinal diversion S308 Small bowel resection S309 Large bowel resection S333 Primary peritoneal drainage for NEC, suspected NEC or intestinal perforation. Check "No" if none of the following procedures: laparotomy, laparoscopy, bowel resection or intraperitoneal drain placement was performed for necrotizing enterocolitis, suspected necrotizing enterocolitis, or bowel perforation. 64
73 ITEM 32: Other Surgery Check "Yes" if a surgical procedure other than PDA Ligation, ROP Surgery and NEC Surgery was performed and either: The surgical procedure is included in Appendix D, or The specific surgical procedure is not listed in Appendix D and the procedure was performed under general or spinal anesthesia, or Other cardiac catheterization procedures are performed (code S600), whether or not the procedure is performed under general or spinal anesthesia. NOTE: If Other Surgery is answered "Yes", at least one of the surgery codes in Appendix D other than the NEC Surgery codes listed above must be entered in Item 33b. Check "No" if the infant does not have other surgery as defined above. If the infant only had PDA Ligation, ROP Surgery or NEC Surgery, check "No". NOTE: Central lines are not considered Other Surgery. Please do not consider any of the following as Other Surgery: Broviac catheters, percutaneous venous catheters, central venous catheters, PICC lines, umbilical artery lines, umbilical venous lines, or any other intravascular catheter. We recognize that some of these lines may be placed while the infant is under anesthesia for other procedures. Do not code any lines as surgery even if they are placed under general or spinal anesthesia. ECMO, ECMO cannulation and ECMO decannulation are not considered Other Surgery. Please do not code ECMO, ECMO cannulation, or decannulation as surgery even if the procedures are performed under anesthesia. Chest tube placement is not considered Other Surgery. Peritoneal dialysis and placement or removal of peritoneal dialysis catheters are not considered Other Surgery. 65
74 ITEM 33a: Surgery Codes If you answered "Yes" to NEC Surgery (Item 31) or Other Surgery (Item 32), enter up to ten Surgery Code numbers that are listed in Appendix D in the spaces provided. For each Surgical Code reported, check the location of surgery for that procedure. If the specific surgical procedure is not listed in Appendix D and the procedure was performed under general or spinal anesthesia, use the code for other surgery in that category (for example, S100, S200, etc.) and provide a description in the text field. NOTE: If a specific procedure is not on the list of surgical codes, do not use codes S100, S200, S300, S400, S500, S700, S800, or S900 unless the procedure is performed under general or spinal anesthesia. These other codes require that the procedure was done under general or spinal anesthesia. Codes for other procedures S100, S200, S300, etc., should only be used to identify procedures for which there is no specific code. Do not use other codes to further describe surgical procedures that are on the list or to indicate why procedures are performed. For example, do not use S500 to add a description for the S504 procedure or to explain why heart surgery was performed. Cardiac surgery for the repair or palliation of congenital heart disease is coded as S504. Do not use code S500 to further describe the details of that surgery. Isolated PDA ligation is coded using item 29a. If PDA ligation is performed as an isolated procedure for PDA, do not enter a surgery code in Item (only check Yes to Item 29a and enter the location of surgery in Item 29b). If the PDA is ligated as a component of the repair or palliation of congenital heart disease, use code S504. Location of Surgery For each Surgical Code reported, indicate where the procedure was done. These items are only applicable when a surgery code is entered in Item 33a. If the surgical procedure is performed only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If the surgical procedure is performed only at another hospital, select "Other Hospital". NOTE: The surgical procedure will be considered to be done at another hospital in the following situations: 1. The surgical procedure is performed before being admitted to your hospital. 2. The surgical procedure is performed prior to readmission to your hospital after initial transfer. Select "Both" if the surgical procedure is done both at your hospital and at another hospital as defined above. 66
75 ITEM 33b: Description of Surgical Codes The following Surgery Codes in Appendix D require a description in the space provided in Item 33b. Only provide a description if one or more of the codes below is reported. Code S100 S200 S300 S400 S500 S600 S700 S800 S900 S1000 S1001 Description Other head and neck surgery requiring general or spinal anesthesia Other thoracic surgery requiring general or spinal anesthesia Other abdominal surgery requiring general or spinal anesthesia Other genito-urinary surgery requiring general or spinal anesthesia Other open heart or vascular surgery requiring general or spinal anesthesia Other interventional cardiac catheterization NOTE: Record procedures for other cardiac catheterization (S600) whether or not the infant received general or spinal anesthesia. Skin or soft tissue surgery requiring general or spinal anesthesia Other musculoskeletal surgery requiring general or spinal anesthesia Other central nervous system surgery requiring general or spinal anesthesia Fetal surgery at your hospital Fetal surgery at another hospital ITEM 34: Respiratory Distress Syndrome Check "Yes" if the infant had respiratory distress syndrome (RDS), defined as: A. PaO2 <50 mmhg in room air, central cyanosis in room air, a requirement for supplemental oxygen to maintain PaO2 >50 mmhg, or a requirement for supplemental oxygen to maintain a pulse oximeter saturation over 85% within the first 24 hours of life. AND B. A chest radiograph consistent with RDS (reticulogranular appearance to lung fields with or without low lung volumes and air bronchograms) within the first 24 hours of life. Check "No" if the infant did not satisfy both of the criteria A and B above. 67
76 ITEM 35a. Pneumothorax Check "Yes" if the infant had extrapleural air diagnosed by chest radiograph or needle aspiration (thoracentesis). For infants who had thoracic surgery and then later developed extrapleural air diagnosed by CXR or needle thoracentesis, check "Yes". Check "No" if the infant did not have extrapleural air as defined above. For infants who had thoracic surgery and a chest tube was placed at the time of surgery OR if free air was only present on a CXR taken immediately after thoracic surgery and was not treated with a chest tube, check "No". ITEM 35b. If Pneumothorax, Where Occurred If the infant had a pneumothorax as defined above, indicate where the pneumothorax occurred. If the pneumothorax occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If the pneumothorax occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, pneumothorax will be considered to have occurred at another hospital in the following situations: 1. The pneumothorax was diagnosed at the other hospital or during transport either prior to admission to your hospital or prior to readmission following initial transfer. 2. The pneumothorax was diagnosed within 4 hours of admission to your hospital. NOTE: If the pneumothorax that occurred at another hospital was initially drained without insertion of a chest tube, and recurred or reaccumulated at your hospital on the same side within 24 hours of admission, it will be considered to have occurred at the other hospital. If a chest tube was inserted at another hospital, and the pneumothorax recurred or reaccumulated at your hospital on the same side within 24 hours of removing the chest tube placed at initial diagnosis, it will be considered to have occurred at the other hospital. Select "Both" if the pneumothorax occurred both at your hospital and at another hospital as defined above. 68
77 ITEM 36: Patent Ductus Arteriosus Check "Yes" if clinical evidence of left to right PDA shunt documented by continuous murmur, hyperdynamic precordium, bounding pulses, wide pulse pressure, congestive heart failure, increased pulmonary vasculature or cardiomegaly by CXR, and/or increased oxygen requirement or ECHO evidence of PDA with documentation of left to right ductal shunting. Check "No" if the infant does not satisfy the above definition. ITEM 37a. Necrotizing Enterocolitis (NEC) NOTE: Infants who satisfy the definition of Necrotizing Enterocolitis below but are found at surgery or post-mortem examination for that episode to have a Focal Gastrointestinal Perforation should be coded as having focal gastrointestinal perforation, not as having NEC. Check "Yes" if the infant had Necrotizing Enterocolitis (NEC) diagnosed at surgery, at postmortem examination or clinically and radiographically using the following criteria: A. One or more of the following clinical signs present: 1. Bilious gastric aspirate or emesis 2. Abdominal distension 3. Occult or gross blood in stool (no fissure) AND B. One or more of the following radiographic findings present: 1. Pneumatosis intestinalis 2. Hepato-biliary gas 3. Pneumoperitoneum Check "No" if the infant did not satisfy the above definition of NEC. ITEM 37b. If Yes, Where Occurred (NEC) If NEC, indicate where occurred. This item is not applicable if NEC did not occur. If NEC occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If NEC occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, NEC will be considered to have occurred at another hospital in the following situations: 1. NEC was diagnosed at the other hospital prior to admission to your hospital or prior to readmission following initial transfer. 2. NEC was diagnosed within 4 hours of admission to your hospital. NOTE: Recurrence or recrudescence of NEC that had previously occurred at another hospital will not be considered to be NEC that occurred at your hospital unless the original case of NEC had resolved and the infant had been on full feedings for 1 week or more. Select "Both" if NEC occurred both at your hospital and at another hospital as defined above. 69
78 ITEM 38a. Gastrointestinal Perforation Check "Yes" if the infant has a Gastrointestinal Perforation separate from Necrotizing Enterocolitis. This diagnosis will be based on visual inspection of the bowel at the time of surgery or post-mortem examination that demonstrates a single focal perforation with the remainder of the bowel appearing normal. Check "No" if the infant did not have a Gastrointestinal Perforation as defined above. ITEM 38b. If Gastrointestinal Perforation, Where Occurred If GI perforation occurred, indicate where occurred. This item is not applicable if GI perforation did not occur. If GI Perforation occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If GI Perforation occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, GI Perforation will be considered to have occurred at another hospital in the following situations: 1. GI Perforation was diagnosed at the other hospital prior to admission to your hospital or prior to readmission following initial transfer. 2. GI Perforation was diagnosed within 4 hours of admission to your hospital. Select "Both" if GI Perforation occurred both at your hospital and at another hospital as defined above. ITEMS 39 to 41: Sepsis and/or Meningitis, Late (after Day 3 of life) NOTE: Each of the late infection items is based on whether the infant had the infection after Day 3 of life. In determining the date of Day 3, the date of birth counts as Day 1 regardless of the time of birth. For an infant born at 11:59 PM on September 1, Day 3 is September 3 rd. Use the criteria below when answering each of the late infection questions. The three late infection items are not applicable if: The infant is discharged home or dies on or before Day 3, or The infant is transferred from your center to another hospital on or before Day 3 and either, o Is not readmitted to your center before discharge home, death or first birthday, or o Is transferred a second time on or before Day 3. Otherwise the item is applicable. 70
79 ITEM 39a. Late Bacterial Pathogen Check "Yes" if the item is applicable and a bacterial pathogen from the list in Appendix B is recovered from a blood and/or cerebral spinal fluid culture obtained after Day 3 of life. Check "No" if the item is applicable and a bacterial pathogen from the list in Appendix B is not recovered from a blood and/or cerebral spinal fluid culture obtained after day 3 of life. Check "N/A" if the item is not applicable based on the criteria in the note above Item 39 above. NOTE: If a bacterial pathogen and a coagulase negative staph are recovered during the same sepsis workup performed after Day 3, check only Bacterial Pathogen for that episode. If a bacterial pathogen is recovered during one episode of sepsis after Day 3, and coagulase negative staphylococcus is recovered during another episode of sepsis after Day 3 (associated with the three clinical criteria for coagulase negative staph), check both Bacterial Pathogen and Coagulase Negative Staph. ITEM 39b. If Late Bacterial Pathogen, Where Occurred If late bacterial pathogen occurred, indicate where occurred. This item is not applicable if late bacterial pathogen did not occur. If late bacterial pathogen occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If late bacterial pathogen occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, late bacterial pathogen will be considered to have occurred at another hospital in the following situations: 1. Late bacterial pathogen was diagnosed at the other hospital prior to admission to your hospital or prior to readmission following initial transfer. 2. Late bacterial pathogen was diagnosed within 4 hours of admission to your hospital. NOTE: Recurrence or recrudescence of a late bacterial pathogen with the same organism that had previously occurred at another hospital will not be considered to be a late bacterial pathogen that occurred at your hospital unless the original case of late bacterial pathogen had resolved and the infant had been off of antibiotics for 1 week or more. Select "Both" if late bacterial pathogen occurred both at your hospital and at another hospital as defined above. 71
80 ITEM 40a. Coagulase Negative Staph Infection after Day 3 Check "Yes" if the item is applicable and the infant has all 3 of the following after day 3 of life: Coagulase negative staphylococcus is recovered from a blood culture obtained from either a central line, or peripheral blood sample, and/or is recovered from cerebrospinal fluid obtained by lumbar puncture, ventricular tap or ventricular drain. AND Signs of generalized infection (such as apnea, temperature instability, feeding intolerance, worsening respiratory distress or hemodynamic instability). AND Treatment with 5 or more days of intravenous antibiotics after the above cultures were obtained. If the infant died, was discharged, or transferred prior to the completion of 5 days of intravenous antibiotics, this condition would still be met if the intention were to treat for 5 or more days. Check "No" if the item is applicable and any or all of the above are not true. Check "Not Applicable" if the item is not applicable based on the criteria above. ITEM 40b. If Coagulase Negative Staph, Where Occurred If coagulase negative staph after day 3 occurred, indicate where occurred. This item is not applicable if coagulase negative staph did not occur. If coagulase negative staph occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If coagulase negative staph occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, Coagulase Negative Staph will be considered to have occurred at another hospital in the following situations: 1. Coagulase negative staph was diagnosed at the other hospital prior to admission to your hospital or prior to readmission following initial transfer. 2. Coagulase negative staph was diagnosed within 4 hours of admission to your hospital. NOTE: Recurrence or recrudescence of a coagulase negative staph infection that had previously occurred at another hospital will not be considered to be a coagulase negative staph infection that occurred at your hospital unless the original case of coagulase negative staph infection had resolved and the infant had been off of antibiotics for 1 week or more. Select "Both" if coagulase negative staph occurred both at your hospital and at another hospital as defined above. 72
81 ITEM 41a. Fungal Infection Check "Yes" if the item is applicable and a fungus was recovered from a blood culture obtained from either a central line or peripheral blood sample after day 3 of life. Check "No" if the item is applicable and a fungus was not recovered from a blood culture obtained from either a central line or peripheral blood sample after day 3 of life. Check "Not Applicable" if the item is not applicable based on the criteria above. ITEM 41b. If Fungal Infection, Where Occurred If fungal infection after day 3 occurred, indicate where occurred. This item is not applicable if fungal infection did not occur. If Fungal Infection occurred only at your hospital prior to Initial Disposition or following readmission after initial transfer, select "Your Hospital". If Fungal Infection occurred only at another hospital, select "Other Hospital". NOTE: When infants transfer to your hospital or are readmitted to your hospital after initial transfer, fungal infection will be considered to have occurred at another hospital in the following situations: 1. Fungal infection was diagnosed at the other hospital prior to admission to your hospital or prior to readmission following initial transfer. 2. Fungal infection was diagnosed within 4 hours of admission to your hospital. NOTE: Recurrence or recrudescence of a fungal infection with the same organism that had previously occurred at another hospital will not be considered to be a fungal infection that occurred at your hospital unless the original case of fungal infection had resolved and the infant had been off of antifungal agents for 1 week or more. Select "Both" if fungal Infection occurred both at your hospital and at another hospital as defined above. 73
82 ITEM 42: Cystic Periventricular Leukomalacia NOTE: To be considered cystic periventricular leukomalacia there must be multiple small periventricular cysts identified. Periventricular echogenicity on ultrasound without cysts should not be coded as cystic periventricular leukomalacia. A porencephalic cyst in the area of previously identified intraparenchymal hemorrhage should not be coded as cystic periventricular leukomalacia. Periventricular abnormalities on CT or MRI should not be coded as cystic periventricular leukomalacia unless multiple small periventricular cysts are identified. Check "Yes" if the infant has evidence of cystic periventricular leukomalacia on a Cranial Ultrasound, CT, or MRI scan obtained at any time. Check "No" if there was no evidence of cystic periventricular leukomalacia on any Cranial Ultrasound, CT, or MRI and at least one cranial imaging study (ultrasound, CT, or MRI) was done. Check "Not Applicable" if no cranial imaging study (Ultrasound, CT, or MRI) was ever done. ITEM 43: Retinopathy of Prematurity ITEM 43a. Retinal Examination Done Check "Yes" if an indirect ophthalmologic examination for retinopathy of prematurity (ROP) was performed at any time. Check "No" if an indirect ophthalmologic examination for ROP was not performed. ITEM 43b. If Yes, enter Worst Stage of ROP If a retinal examination was performed, enter the worst stage documented on any exam in the eye with the most advanced stage 1. Do not answer this item if the answer to Item 43a is "No". Stage 0: No evidence of ROP Stage 1: Presence of demarcation line (+/- abnormal vascularization) Stage 2: Presence of intraretinal ridge Stage 3: Presence of a ridge with extraretinal fibrovascular proliferation Stage 4: Partial retinal detachment Stage 5: Total retinal detachment 1 An International Committee for the Classification of Retinopathy of Prematurity: The International Classification of Retinopathy of Prematurity Revisited. Arch Ophthalmol 2005; 123:
83 ITEM 44: Birth Defect Present Check "Yes" if the infant had one or more of the birth defects listed in Appendix C. In the spaces provided, you may enter as many as five 3-digit code numbers of birth defects from the list. Check "Yes" if the infant had birth defects, not listed in Appendix C, which were lethal, or life threatening. In this case use the defect code of 100 (in addition to any other applicable code) and describe the defects in detail in the space provided for description. Be specific. Do not use general descriptions such as multiple congenital anomalies or complex congenital heart disease. To be considered as lethal or life threatening a birth defect must either; 1) be the primary cause of death, or 2) be treated prior to discharge with specific surgical or medical therapy to correct a major anatomic defect or a life threatening physiologic dysfunction. Check "No" if an infant was not diagnosed as having one or more of the birth defects listed in Appendix C and did not have an unlisted birth defect which was lethal or life threatening. The following Birth Defect Codes require a detailed description in the space provided for Item 44 on the Discharge Form: Code Other Chromosomal Anomaly Code Skeletal Dysplasia Code Inborn Error of Metabolism Code Other Lethal or Life Threatening Central Nervous System Defects Code Other Lethal or Life Threatening Congenital Heart Defects Code Other Lethal or Life Threatening Gastro-Intestinal Defects Code Other Lethal or Life Threatening Genito-Urinary Defects Code Other Lethal or Life Threatening Pulmonary Malformation Code Other Lethal or Life Threatening Defects not listed in Appendix C The following conditions should NOT be coded as Major Birth Defects: Cleft Lip without Cleft Palate Club Feet Congenital Dislocation of the Hips Congenital CMV Extreme Prematurity Fetal Alcohol Syndrome Hypospadias Hypothyroidism Intrauterine Growth Retardation Intrauterine Infection Limb Abnormalities Patent Ductus Arteriosus Persistent Pulmonary Hypertension (PPHN) Polydactyly Pulmonary Hypoplasia (use code 401 for bilateral renal agenesis, or 604 for oligohydramnios sequence, if applicable) Small Size for Gestational Age Syndactyly 75
84 ITEM 45: Enteral Feeding At Discharge NOTE: When completing this item, Discharge refers to initial disposition in most cases. If an infant is transferred from your center to another hospital and readmitted to your center following transfer, update this item based on the infant s enteral feeding status at the time of discharge after readmission. Complete this item based on enteral feedings received during the 24 hour period prior to discharge, transfer, or death. For infants who remained in your hospital on their first birthday, complete the item, Enteral Feeding at Discharge, based on enteral feedings received on that day. Enteral feedings may be given by any method including breast, bottle, gavage tube, gastrostomy tube, feeding cup, etc. Formula milk includes all standard newborn formulas, premature formulas, and special formulas. Please answer this question based only on the enteral feedings at discharge. Do not consider parenteral feedings when answering this item. For example, if an infant was discharged on IV TPN as well as human milk, the correct response would be Human Milk Only since human milk was the only enteral feeding. Check "None" if the infant was not receiving any enteral feedings with either formula milk or human milk at discharge. Check "Human Milk Only" if the infant was discharged receiving human milk as their only enteral feeding, either by being breast fed and/or by receiving pumped human milk. Check "Formula Only" if the infant was discharged receiving formula milk as their only enteral feeding. Check "Human Milk in Combination with Either Fortifier or Formula" if the infant was discharged receiving human milk, plus human milk fortifier and/or formula milk. If an infant was discharged on IV TPN alone, the correct response would be "None" since the infant was not receiving any enteral feedings. If an infant was discharged only on sterile water or glucose water, the correct response would be "None" since the infant was not receiving either formula milk or human milk. 76
85 ITEM 46: Oxygen and Monitor at Discharge NOTE: When completing these items, Discharge refers to initial disposition in most cases. If an infant is transferred from your center to another hospital and readmitted to your center following transfer, update. These items based on whether the infant was on oxygen or monitor at the time of discharge after readmission. ITEM 46a. Oxygen at Discharge For infants who went home or were transferred, check "Yes" if the infant was discharged on supplemental oxygen. Check "No" if the infant was not discharged on supplemental oxygen. For infants who remained in your hospital on his/her first birthday, check "Yes" if the infant was on supplemental oxygen on the date of the infant s first birthday. Check "No" if the infant was not on supplemental oxygen on his/her first birthday. For infants who died prior to discharge, check "Yes" if the infant received supplemental oxygen at any time on the day of death. Check "No" if the infant did not receive supplemental oxygen at any time on the day of death. ITEM 46b. Monitor at Discharge For infants who went home or were transferred, check "Yes" if the infant was discharged on an Apnea Monitor or Cardio-Respiratory Monitor. If arrangements were made to provide Cardio-Respiratory or Apnea monitoring at home following discharge, check "Yes" even if the infant was not actually on the monitor at the time he/she left your hospital. NOTE: A pulse oximeter is considered a cardio-respiratory monitor. Check "No" if the infant was not discharged on an Apnea or Cardio-Respiratory Monitor and arrangements were not made to provide Cardio-Respiratory or Apnea monitoring at home following discharge. For infants who remained in your hospital on his/her first birthday, check "Yes" if the infant was on an Apnea Monitor or Cardio-Respiratory Monitor on the date of the infant s first birthday. Check "No" if the infant was not on an Apnea or Cardio- Respiratory Monitor on his/her first birthday. For infants who died prior to discharge, check "Yes" if the infant was on an Apnea Monitor or Cardio-Respiratory Monitor at any time on the day of death. Check "No" if the infant was not on an Apnea or Cardio-Respiratory Monitor at any time on the day of death. 77
86 ITEM 47: Initial Disposition From Your Hospital Initial Disposition refers to the first time that the infant was discharged or transferred from your hospital. Do not change this item based on later dispositions following transfer or readmission. Check "Home" if the infant was discharged home on or before his/her first birthday from your hospital without ever transferring to another hospital. Complete the remaining items on the Discharge Form. Do not complete the Transfer and Readmission Form. Check "Died" if the infant died on or before his/her first birthday at your hospital prior to being discharged home or transferred. Complete the remaining items on the Discharge Form. Do not complete the Transfer and Readmission Form. Check "Transferred to another Hospital" if the infant was transferred to another hospital or chronic care facility on or before his/her first birthday and before going home. Complete the remaining items on the Discharge Form. Complete the Transfer Log and the Transfer and Readmission Form for infants who transfer (see Appendix A). See instructions for the Transfer and Readmission Form. NOTE: Infants transferred from one unit to another within your hospital are not considered to have been transferred or discharged. Continue collecting data until the first birthday for all eligible infants who have not been discharged and who remain anywhere within your hospital. Check "Still Hospitalized as of First Birthday" if the infant was still at your center on the date of the infant s first birthday. Complete the remaining items on the Discharge Form. Do not complete the Transfer and Readmission Form. ITEM 48: Weight at Initial Disposition This item refers to the Initial Disposition (first discharge or transfer) from your hospital. Do not change this item based on later dispositions following transfer or readmission. Enter the weight in grams obtained on the Date of Initial Discharge, Transfer or Death (Item W8 on the Patient Identification Worksheet). If the answer to Initial Disposition from Your Hospital (Item 47) is Still Hospitalized as of First Birthday, enter the infant s weight in grams on the infant s first birthday. If the infant was not weighed on the date of his/her first birthday, enter the weight in grams from the previous day. ITEM 49: Head Circumference at Initial Disposition Enter the head circumference as recorded in the chart or clinical flow sheets on the Date of Initial Disposition (Item W8 on the Patient Identification Worksheet). If the head circumference is not recorded on the Date of Initial Disposition, record the most recent head circumference measured on the day prior to discharge. If the head circumference is not recorded on the Date of Initial Disposition or day prior to discharge, record as unknown. 78
87 ITEM 50: Initial Length of Stay This item refers to the first discharge or transfer from your hospital. Do not change this item based on later dispositions following transfer or readmission. Initial Length of Stay is not applicable to infants who meet Delivery Room Death Criteria. For all other infants, enter the Initial Length of Stay, Item L1, from Part A on the Length of Stay Calculation Worksheet. Initial Length of Stay is the number of days from the date the infant was admitted to your hospital (Item W5 on the Patient Identification Worksheet) until the Date of Initial Discharge, Transfer or Death (Item W8 on the Patient Identification Worksheet). Calculate the Initial Length of Stay as ([Date of Initial Discharge, Transfer or Death] minus [Date of Admission] plus one). Infants who die on the day of birth, other than those who meet Delivery Room Death Criteria, will have an Initial Length of Stay of 1 day. The maximum value of Initial Length of Stay is 366 (or 367 if leap day must be added) because tracking ends on the infant s first birthday. NOTE: For inborn infants, the Date of Admission is the Date of Birth. For outborn infants, the Date of Admission is the date the infant was admitted to your center. If the Date of Initial Discharge, Transfer or Death is Unknown, Initial Length of Stay will also be Unknown. If an infant is still in your hospital on his or her first birthday, and has not transferred or been home, use the date of the infant s first birthday as the Date of Initial Discharge, Transfer or Death. End of Discharge Form Definitions 79
88 Transfer and Readmission Form Data Definitions Items on the Transfer and Readmission Form only apply to infants who transfer from your center to another hospital. You should be familiar with the instructions in Chapter 7 when completing the Transfer and Readmission Form. NOTE: Infants transferred from one unit to another within your hospital are not considered to have been transferred or discharged. Only use the Transfer and Readmission Form for infants who transfer from your center to another hospital. Part A of Transfer and Readmission Form ITEM 51: Reason for Transfer Check only one response indicating the primary reason for transfer. Check "Growth/Discharge Planning" if an infant is transferred to another hospital for continuing care in preparation for eventual discharge home. This category will include back transfers to a hospital closer to the parents home. If the facility to which the infant is transferred is a tertiary care facility, the answer to this question will be "Growth/Discharge Planning" as long as the purpose of the transfer is not for the provision of surgical, medical or diagnostic services, or long term chronic care which were unavailable at your hospital. Check "Medical/Diagnostic Services" if the infant is transferred to another hospital to receive medical care or diagnostic tests which are not available at your hospital. If an infant is transferred to have a diagnostic work-up and the work-up results in surgery, the reason for transfer is still Medical/Diagnostic Services. Check "Surgery" if an infant is transferred to another hospital specifically to have surgery even if surgery is not actually performed after the transfer. Check "ECMO" if the infant is transferred to another hospital for extracorporeal membrane oxygenation. Check "Chronic Care" if the infant is transferred to an institution for long term chronic care. Check "Other" if the reason for transfer does not meet any of the above criteria. ITEM 52: Transfer Code of Center to which Infant Transferred Please refer to the current Transfer Code List of the Vermont Oxford Network when answering this question. The Transfer Code List may be accessed at this website address: 80
89 ITEM 53: Post Transfer Disposition Check "Home" if the infant was discharged to home on or before his/her first birthday from the hospital to which he/she was transferred. If this answer is checked, Parts B and C of this Form are not applicable; only complete Part D of this Form. Check "Transferred Again to Another Hospital" if the infant was transferred again to another hospital or to a chronic care facility from the hospital to which he/she was originally transferred. If this answer is checked, Part B of this Form is not applicable; complete Part C of this Form. Check "Died" if the infant died on or before his/her first birthday at the hospital to which he/she was initially transferred. If this answer is checked, Parts B and C of this Form are not applicable; only complete Part D of this Form. Check "Readmitted to Any Location in Your Hospital" if an infant is readmitted on or before his/her first birthday (before ever having gone home) to any location in your hospital such as the neonatal intensive care unit, a step-down unit, newborn nursery, intermediate care, pediatric intensive care unit, pediatric ward, etc. If this answer is checked, complete Part B of this Form. Check "Still Hospitalized as of First Birthday" if infant was still in the Transferred To hospital on his/her first birthday. If this answer is checked, Parts B and C of this Form are not applicable, complete only Part D of this Form. Part B of Transfer and Readmission Form ITEM 54: Disposition After Readmission Check "Home" if the infant was discharged to home on or before his/her first birthday from any location in your hospital after readmission. If this answer is checked, Part C of this Form is not applicable; complete Part D of this Form. Check "Died" if the infant died on or before his/her first birthday at any location in your hospital after readmission. If this answer is checked, Part C of this Form is not applicable; complete Part D of this Form. Check "Transferred Again to Another Hospital" if the infant was transferred again to another hospital or to a chronic care facility on or before his/her first birthday after readmission. If this answer is checked, complete Part C of this Form. Check "Still Hospitalized as of First Birthday" if infant was still in your hospital as of his/her first birthday. If this answer is checked, Part C of this Form is not applicable; complete Part D of this Form. ITEM 55: Weight at Disposition After Readmission Enter the weight in grams obtained on the date at which the Disposition after Readmission, Item 54, occurred. If the infant was not weighed on the day of Disposition After Readmission, enter the weight in grams from the previous day. If the answer to Disposition After Readmission (Item 54) is Still Hospitalized as of First Birthday, enter the infant s weight on his or her first birthday. If the infant was not weighed on the date of the first birthday, enter the weight in grams from the previous day. 81
90 Part C of Transfer and Readmission Form ITEM 56: Ultimate Disposition Check "Home" if the infant ultimately went home on or before the first birthday. Check "Died" if the infant ultimately died on or before the first birthday and before being discharged home. Check "Still Hospitalized as of First Birthday" if the infant was still hospitalized on his/her first birthday, without ever having gone home. Part D of Transfer and Readmission Form ITEM 57: Total Length of Stay The Total Length of Stay is the number of days from the date the infant was first admitted to your hospital (Item W5 on the Patient Identification Worksheet) until the date of Final Discharge or Death (Item W9 on the Patient Identification Worksheet). Calculate the Total Length of Stay as ([Date of Final Discharge or Death] minus [Date of Admission] plus one). The maximum value of Total Length of Stay is 366 (or 367 if leap day must be added), because tracking ends on the infant s first birthday. Use the Length of Stay Calculation Worksheet to calculate the Total Length of Stay. Enter total length of stay, Item L2, from Part B on the length of stay calculation worksheet. NOTE: For inborn infants, the Date of Admission is the Date of Birth. For outborn infants, the Date of Admission is the date the infant was admitted to your center. If the Date of Final Discharge or Death is Unknown, Total Length of Stay will also be Unknown. If an infant who transfers is still hospitalized on his or her first birthday, and has not been home, use the date of the infant s first birthday as the Date of Final Discharge or Death. End of Transfer and Readmission Form Definitions 82
91 Supplemental Data Form Data Definitions Items on the Supplemental Data Form only apply to centers participating in the Expanded Database or Neonatal Encephalopathy Registry. Most items on the Supplemental Data Form do not apply to infants who not meet the delivery room death criteria described in Chapter 5, Table 5.3. Use the Delivery Room Death Form for these infants. You should also be familiar with the instructions in Chapter 7 when completing the Supplemental Data Form. ITEMS S1.A.1 and S1.A.2: Duration of Assisted Ventilation NOTE: Only include the Duration of Assisted Ventilation which occurs during the initial stay in your hospital. Do not include duration of ventilation at other hospitals or duration following readmission for infants who are transferred from your center to another hospital. NOTE: Only consider conventional ventilation or high frequency ventilation when answering the questions on Duration of Assisted Ventilation. ITEM S1.A.1: Duration of Assisted Ventilation After Admission Enter "None" if the infant did not receive assisted ventilation after admission to a NICU in your hospital. Enter "<4 hours" if the infant received assisted ventilation for <4 hours after admission to a NICU in your hospital. Enter "4-24 hours" if the infant received assisted ventilation for 4-24 hours after admission to a NICU in your hospital. Enter ">24 hours" if the infant received assisted ventilation for more than 24 hours after admission to a NICU in your hospital. Enter "N/A" if the infant meets the Delivery Room Death Criteria. ITEM S1.A.2: If >24 Hours, Total Days of Assisted Ventilation After Admission If the duration of assisted ventilation after admission to your NICU was more than 24 hours, enter the total number of days of assisted ventilation after admission to your NICU. The number of days should include any complete or partial day during which the infant received assisted ventilation. ITEM S1.B: ECMO at your Hospital Enter "Yes" if the infant was treated with ECMO at your hospital. Enter "No" if the infant was not treated with ECMO at your hospital. Enter "N/A" if the infant meets the Delivery Room Death Criteria. 83
92 ITEM S1.C.1 and S1.C.2: Hypothermic Therapy at Your Hospital NOTE: This item is answered "Yes" only if the infant is cooled at your hospital. This may include cooling at your hospital prior to initial disposition or following readmission to your center if the infant is transferred. NOTE: Infants may be treated with hypothermia during surgery. If hypothermic therapy is only performed during and immediately around the time of cardiac surgery or other surgery, Item S1.C.1, "Hypothermic Therapy at Your Hospital" should be answered "No". ITEM S1.C.1: Was Hypothermic Therapy Performed at Your Hospital Enter "Yes" if either selective head or whole body cooling was provided at your hospital. Enter "No" if neither selective head nor whole body cooling was provided at your hospital. ITEM S1.C.2: If Yes, Cooling Method If the infant received hypothermic therapy at your hospital, choose the method of cooling received there. Choose "Selective Head" cooling, or "Whole Body" cooling based on the following criteria. "Selective Head" Cooling: Active cooling restricted to the head and brain. This is an intervention to reduce the temperature of the head and brain by exposing the head to lower than environmental temperature. Specially designed head cooling devices, other cooling devices and ice packs applied to the head would be considered active cooling. Passive exposure to environmental temperature and cooling of the face for treatment of supraventricular tachycardia are not considered active cooling of the head and brain. "Whole Body" Cooling: Active cooling of the body not restricted to the head and brain. This is an intervention to reduce the core body temperature and temperature of the brain by exposing the body to lower than environmental temperature. Cooling blankets, other cooling devices and ice packs applied to the body would be considered active cooling. Passive exposure to environmental temperature would not be considered active cooling. Whole body cooling may include cooling of the head in addition to the rest of the body. 84
93 ITEMS S2.A.1 and S2.A.2: Hypoxic-Ischemic Encephalopathy (HIE) NOTE: These items are only applicable if the infant s gestational age is 36 weeks, 0 days, or greater. They are not applicable for infants whose gestational age is less than 36 weeks or infants who meet the delivery room death criteria described in Chapter 5. If the infant is readmitted to your center following transfer, update these HIE items if they are applicable and if HIE is diagnosed at the transferred to hospital or at your center following readmission; continue to collect data for these items until Disposition after Readmission occurs. ITEM S2.A.1: Hypoxic-Ischemic Encephalopathy Enter "Yes" if the infant was diagnosed with hypoxic-ischemic encephalopathy as defined below. Enter "No" if the infant was not diagnosed with hypoxic-ischemic encephalopathy. Enter "N/A" if the infant meets the Delivery Room Death Criteria. Enter "N/A" for infants with a gestational age less than 36 weeks. The diagnosis of hypoxic-ischemic encephalopathy requires the presence of all 3 of the following criteria: 1. The presence of a clinically recognized encephalopathy within 72 hours of birth. Encephalopathy is defined as the presence of 3 or more of the following findings within the first 72 hours after birth: a. Abnormal level of consciousness: hyper alertness, lethargy, stupor or coma. b. Abnormal muscle tone: hypertonia, hypotonia or flaccidity. c. Abnormal deep tendon reflexes: increased, depressed or absent. d. Seizures: subtle, multifocal or focal clonic. e. Abnormal Moro reflex: exaggerated, incomplete or absent. f. Abnormal suck: weak or absent. g. Abnormal respiratory pattern: periodic, ataxic or apneic. h. Oculomotor or pupillary abnormalities: skew deviation, absent or reduced Doll's eyes or fixed unreactive pupils. AND 2. Three or more supporting findings from the following list: a. Arterial cord ph<7.00. b. APGAR score at 5 minutes of 5 or less. c. Evidence of multiorgan system dysfunction (see below). d. Evidence of fetal distress on antepartum monitoring: persistent late decelerations, reversal of end-diastolic flow on Doppler flow studies of the umbilical artery or a biophysical profile of 2 or less. e. Evidence on CT, MRI, technetium or ultrasound brain scan performed within 7 days of birth of diffuse or multifocal ischemia or of cerebral edema. f. Abnormal EEG: low amplitude and frequency, periodic, paroxysmal or isoelectric 85
94 AND 3. The absence of an infectious cause, a congenital malformation of the brain or an inborn error of metabolism, which could explain the encephalopathy. NOTE: Multiorgan system dysfunction (2.c. above) requires evidence of dysfunction of one or more of the following systems within 72 hours of birth: a. Renal: oliguria or acute renal failure. b. GI: Necrotizing enterocolitis, hepatic dysfunction. c. Hematologic: thrombocytopenia, disseminated intravascular coagulopathy. d. Endocrine: hypoglycemia, hyperglycemia, hypercalcemia, syndrome of inappropriate ADH secretion (SIADH). e. Pulmonary: persistent pulmonary hypertension. f. Cardiac: myocardial dysfunction, tricuspid insufficiency. ITEM S2.A.2: HIE Severity If the infant was diagnosed with hypoxic-ischemic encephalopathy, record the worst stage observed during the first 7 days following birth based on the infant's level of consciousness and response to arousal maneuvers such as persistent gentle shaking, pinching, shining a light or ringing of a bell: Check "Mild" if normal or hyperalert. Infants in this category are alert or hyperalert with either a normal or exaggerated response to arousal. Check "Moderate" if lethargic or mild stupor. Infants in this category are arousable but have a diminished response to arousal maneuvers. Check "Severe" if deep stupor or coma. Infants in this category are not arousable in response to arousal maneuvers. Check "N/A" if S2.A.1. (Hypoxic-Ischemic Encephalopathy) is answered either "No" or "N/A". Check "N/A" if the infant meets the Delivery Room Death Criteria. 86
95 ITEMS S2.B.1 and S2.B.2: Meconium Aspiration NOTE: Items S2.B.1, Meconium Aspiration Syndrome, is applicable to all infants, including infants who die in the delivery room. Item S2.B.2, Suctioned for Meconium, is applicable to all infants who are diagnosed with Tracheal Suctioning for Meconium Attempted, i.e., when Item S2.B.1 is answered "Yes". ITEM S2.B.1: Meconium Aspiration Syndrome NOTE: This item is applicable to all infants, including those who meet the Delivery Room Death Criteria. Check "Yes" if all 5 of the following criteria are satisfied: 1. Presence of meconium stained amniotic fluid at birth. 2. Respiratory distress with onset within 1 hour of birth. Respiratory distress will be defined as the presence of one of the following signs: tachypnea, grunting, nasal flaring or intercostal retractions. 3. A PaO2<50 mmhg in room air, central cyanosis in room air or a requirement for supplemental oxygen to maintain PaO2>50 mmhg. 4. Abnormal chest x-ray compatible with the diagnosis of meconium aspiration. Findings may include coarse irregular or nodular pulmonary densities, areas of diminished aeration or consolidation alternating with areas of hyperinflation and generalized hyperinflation. 5. Absence of culture proven early onset bacterial sepsis or pneumonia. The diagnosis of culture proven early onset bacterial sepsis or pneumonia requires a positive blood culture obtained within 72 hours of birth. Check "No" if all 5 of the criteria for Meconium Aspiration Syndrome are not satisfied. 87
96 ITEM S2.B.2: Tracheal Suctioning for Meconium Attempted in the DR NOTE: This item is applicable if Meconium Aspiration Syndrome is diagnosed; otherwise the item is not applicable. If Meconium Aspiration Syndrome is present, enter "Yes" for Item S2.B.2 if tracheal suctioning through an endotracheal tube or suction catheter in the trachea was performed in the delivery room in an attempt to remove meconium. If suctioning was performed, the answer is "Yes" even if no meconium was recovered. Check "No" for Item S2.B.2 if Meconium Aspiration is present (Item S2.B.1) and tracheal suctioning is not attempted. Check "N/A" if Meconium Aspiration is not present (Item S2.B.1 is "No"). ITEM S2.C: Seizures Check "Yes" if there is clinical evidence of subtle seizures, or of focal or multifocal clonic or tonic seizures within the first 3 days after birth. Check "No" if there was no evidence of seizures. Check "N/A" if the infant meets the Delivery Room Death Criteria. End of Supplemental Data Form Definitions 88
97 CHAPTER 9 Correcting and Finalizing Data Introduction Chapter 3 discusses the annual cycle for data submission and reporting. As stated in that chapter, each year guidelines are distributed and checks are done to assure that all errors in submitted records have been corrected, that all records are complete and that all eligible infants have been identified. Your Account Manager will let you know about the requirements for data finalization. The expectation is that members will assure that records for all eligible infants have been submitted by April 1 and that all submitted records are complete and correct by June 1 following the end of the birth year. When data are submitted by your hospital, the infant records are processed using specially designed software. Your submissions go through an extensive series of checks to identify data that are missing, out of range, or inconsistent with another answer given. This chapter explains the processes used to provide feedback to your staff on data management issues to be resolved, as well as the processes for correcting data problems. Data Summaries The Network s data summaries provide a complete set of tools for identifying errors in the data you submit and for monitoring the accuracy and completeness of your center s data throughout the year. After data submissions have been received and processed, your center Data Contact will be notified and the data summaries can be viewed on the Members Area Data Management Area of the Network web site. Summary Name How You Use It Frequency Members Area, Error and Warning Summary Data Form Status Summaries Births During Period Incomplete Records Data Management Summary Data summaries are now available online at the Network web site. Just login! To correct errors in your data, which you then resubmit. To check unusual answers to be sure they are correct. To identify records that may be missing (eligible infants that may not have been reported). To follow up on incomplete or incorrect forms for each patient record. As a summary of the information in the Error and Warning and Data Form Status Summaries. To review the overall status of data and encourage up-to-date, complete and accurate submissions. Table 9.1: Data Summaries Electronic submissions immediately. Paper submissions after processing. Paper submissions: Monthly or quarterly EDS: After submission Paper submissions: Monthly or quarterly Paper submissions: Monthly or quarterly EDS: After submission 89



98 Each Data Contact should have access to the Members Area. Data Contacts who do not have access to the Members Area should contact their hospitals VON Web Services Administrator for assistance. Your Account Manager can also help if you are having problems identifying your Web Services Administrator. If your Data Contact does not have access to the Members Area, printed summaries will be sent via or fax. In either case it is important to review these summaries and stay current on the status of your center s data. Video tutorials are available in the Members Area at this link: Error and Warning Summary Data records submitted by your center are processed using specially designed software. An extensive series of checks are made to identify data that are missing, out of range, or inconsistent with another answer given. The results of this process are reflected in the Error and Warning Summary, which documents all records that require correction or verification. Figure 9.1 shows a sample Error and Warning Summary. Table 6.1: Data Summaries Figure 9.1: Error and Warning Summary 90
99 Errors occur when the response you have entered for a data item is incorrect or in conflict with an answer to another data item. Out of range responses also generate errors. If paper data contain an error, you must submit revised data forms. Centers submitting data electronically must correct errors in their local database and then submit a file containing the corrected records. For Common Errors and Suggestions see Table 9.4 later in this chapter. Warnings occur when the response to a data item needs to be reviewed and corrected if necessary. An example might be a discharge weight of 750 grams for an infant discharged to home. It is important to evaluate all warnings when they are first issued and submit corrections as necessary. The Data Contact at your center will receive an Error and Warning Summary when data files or paper forms are submitted. Your center should make the necessary corrections and submit the corrected data with the next regularly scheduled submission. Note that corrections must be made on the forms or in the files, not on the Error and Warning Summary itself. Data Form Status Summaries There are two types of Data Form Status Summaries. Figure 9.2 shows the Births During Period version, which lists the status of all forms received and entered into the database for a specific birth year (or optionally, for more than one birth year). There is one row for each record. Figure 9.3 shows the All Records which are Incomplete or Require Correction version of this summary. This version lists any record, regardless of birth year, that has not been completed or is incorrect. Both versions help you track the status of data submissions and identify individual patient records that require further action. The Data Form Status Summary, Births during Period, shows the status of all records and forms for a period of time and can be used to verify that all eligible infants have been reported to the Network. Another important function of this summary is to indicate gaps in the center s Network ID sequence. A gap in the sequence, as indicated by an asterisk next to the record number, may mean that: Your center has decided not to use an ID number, but your Account Manager has not been informed. For a specific infant, your center has assigned an ID number, but for some reason, the data have either not been sent to the Network or cannot be processed. Records and/or forms that cannot be processed fall in one of the following categories: o No ID Number given o No Birth Year given o Incorrect form used based on the answer given to Item 3, Died in the Delivery Room o Use of the wrong data form for the birth year. No asterisk will appear for the following gap in sequence: The Data Contact has decided and informed the Account Manager that a specific Network ID or range of IDs will not be used. A note appears in the Comments column for any IDs that are Unused ID Confirmed. 91
 to another.")


100 Your center has changed from paper data submissions to electronic data submissions or from one database option (VLBW or Expanded) to another. Gaps in ID number sequencing sometimes occur as a result of these changes. The ID number has been deleted by your center. It is important to investigate any gaps in the Network ID sequence and inform your Account Manager of all ID numbers that will not be submitted to the Network. Figure 9.2: Sample Data Form Status Summary Births During Period 92



101 Figure 9.3: Sample Data Form Status Summary All Records which Are Incomplete or Require Correction The All Records which are Incomplete or Require Correction Data Form Status Summary provides a snapshot of all the records from your center that still require completion or correction. Records that are complete and without error are not listed. Tables 9.2 and 9.3 summarize the record status codes and form status codes used in the Data Form Status Summaries. Code Definition Comments C E I R S Correct Error Incomplete VON Record Received, NER Record not Received Still Hospitalized The record has been completely error checked and is correct. There are no errors or blank items in the record. The record has one or more errors. Table 9.2: Record Status Codes The record is partially complete but has some blank items. Error checking on the entire record cannot be completed. VLBW-NER centers only. As a minimum, Items 1 through 44 on the 28 Day and Discharge Forms have been submitted, there are no errors noted on the forms, but final disposition data have not been received. This code is temporary when the infant is discharged and and the record is complete, all forms are checked again for errors. Your Account Manager will continue to track these records until final status is known. 93
102 Code Definition Comments C E I Correct Errors Incomplete The form has been completely error checked and is correct. There are no errors or blank items on the form. The form has errors in one or more items. The errors must be corrected. The form is partially complete but has some blank items. N Not Applicable The form is Not Applicable for the record. P R Pending Received but not completely verified The data for the form has not been received (all items on the form are blank). The form has been received and has no known errors but cannot be completely verified because one or more other forms are missing. For instance, a complete Discharge Form will have an R status if a 28 Day Form has not been received for that record. Table 9.3: Form Status Codes Data Management Summary The Data Management Summary (Figure 9.4) provides an overview of the status of the data your center has submitted for the last three years. It is a useful tool for determining if there are problems with data completeness or data accuracy and as a springboard for discussions between your center Data Contact and the VON Account Manager. 94

103 Figure 9.3: Sample Data Management Summary Figure 9.4: Sample Data Management Summary 95
104 Submitting Data Corrections After you submit data to the Network, either electronically or using paper forms, you will be able to view the various data summaries by logging into the Members Area on the Network Web Site, If you do not have access to the Members Area, your Account Manager will send you copies of the data summaries. Use the information on the data summaries to prepare corrections and resubmit the data records requiring correction. If you submit corrections on paper forms, submit corrections along with your regular monthly data submission and follow these procedures to differentiate corrected forms: Write REVISION at the top of each corrected form. Be sure to include the infant s Birth Year and Network ID on the form. Send complete forms indicating the items you have corrected by circling or highlighting the corrected answer. Circling works best if you are faxing your corrections or send forms that contain only those items being corrected. Please remember to white-out the incorrect answer. If you submit corrections electronically, make the corrections using your computer software and submit corrections in a file. Submitted files may include new and updated records. You don t need to do anything special to indicate that the file you are sending contains corrected records. Avoiding Common Errors Table 9.4 shows errors that are commonly made when submitting data and suggestions for preventing these errors. 96
105 COMMON ERROR Inconsistent or illegible entries for Center Number, Network ID Number and/or Year of Birth on paper forms. Leaving Gestational Age, Days, blank on the 28 Day Form. Inconsistency in Oxygen on Day 28 on the 28 Day Form and Length of Stay. Inconsistency in Nasal CPAP and Nasal CPAP before ETT Ventilation on the Discharge Form. Inconsistency in Surfactant Given in the Delivery Room and Surfactant At Any Time on the Discharge Form. Inconsistency in Surfactant At Any Time and Age at First Dose on the Discharge Form. The answers given for Late Bacterial Pathogen, Coag Negative Staph and/or Fungal Infection on the Discharge Form are inconsistent with Length of Stay. The answer given for Duration of Assisted Ventilation on the Supplemental Data Form is inconsistent with answers given for Conventional Ventilation and/or HIFI Ventilation on the Discharge Form (Expanded Data/NER centers only). Inconsistency in answers given to Gestational Age on the 28 Day Form and Hypoxic-Ischemic Encephalopathy on the Supplemental Data Form (Expanded Data/NER centers only). SUGGESTION Enter the Center Number, Network ID Number and/or Year of Birth on all paper forms submitted. Be sure that these are consistent on all forms for each infant. If the estimated gestational age is determined to be an exact number of weeks, (0 days), enter zero for Gestational Age, Days. Do not leave this item blank. If the infant is discharged home, dies or is transferred more than once prior to day 28 of life, Oxygen on Day 28 must be answered N/A. This item is also answered N/A when an infant transfers to another hospital prior to day 28 and is not readmitted to your hospital after initial transfer. If Nasal CPAP is answered No, Nasal CPAP before ETT Ventilation must be left blank on paper forms and coded N/A for electronic data submissions. If Surfactant Given in the Delivery Room is answered Yes, Surfactant At Any Time must also be answered Yes. If Surfactant At Any Time is Yes, both Hours and Minutes must be answered. Do not leave either of these items blank. If the infant is discharged home, dies or is transferred more than once prior to day 4 of life, the late infection items must be answered N/A. These items are also answered N/A when an infant transfers to another hospital prior to day 4 and is not readmitted to your hospital after initial transfer. If infant was inborn, the answer to either Conventional Ventilation or HIFI Ventilation is Yes and Initial Disposition is Died or Home, Duration of Assisted Ventilation cannot be answered None. Select the appropriate response depending on the number of days ventilated. If the infant s gestational age is 36 weeks, 0 days or more, and the infant does not meet the delivery room death criteria, the answer to Hypoxic-Ischemic Encephalopathy cannot be answered N/A. If the infant s GA is less than 36 weeks or meets the DR death criteria this item must be answered N/A. Table 9.4: Common Errors and Suggestions 97
106 APPENDICES Appendix A Appendix B Appendix C Appendix D Logs, Worksheets, and Data Forms Bacterial Pathogens Birth Defect Codes Surgery Codes Appendix E Calculation Charts for Date of Day 28 Appendix F Calculation Charts for Date of Week 36 Appendix G Appendix H Appendix I Appendix J Day Number Chart Timeline for Database Activities Fahrenheit to Centigrade Conversion Table Vermont Oxford Network Directors, Advisory Board and Database Advisory Committee 98
107 APPENDIX A Logs, Worksheets, and Data Forms 99
108 100
109 101
110 Patient Data Booklet 102
111 103
112 104
113 105
114 106
115 107
116 Transfer and Readmission Form NOTE: Since the Transfer and Readmission Form is not required for most infants, this form is printed separately and is not included in the Patient Data Booklet. 108
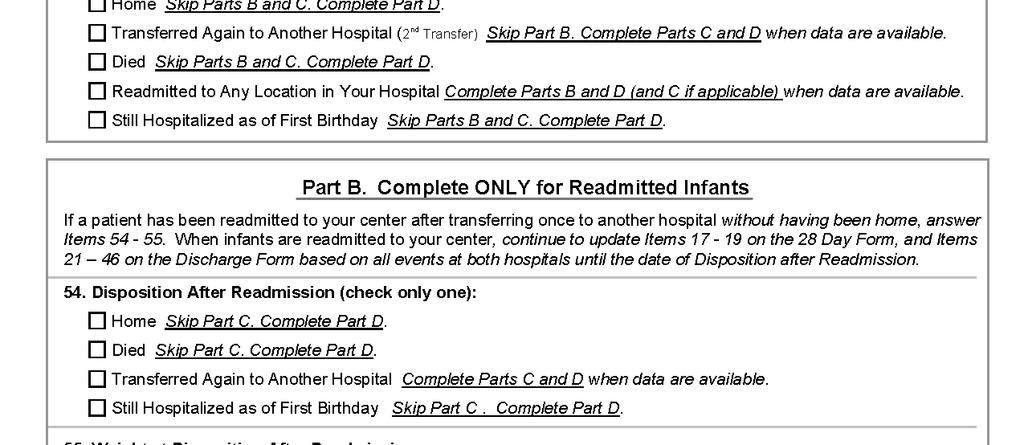
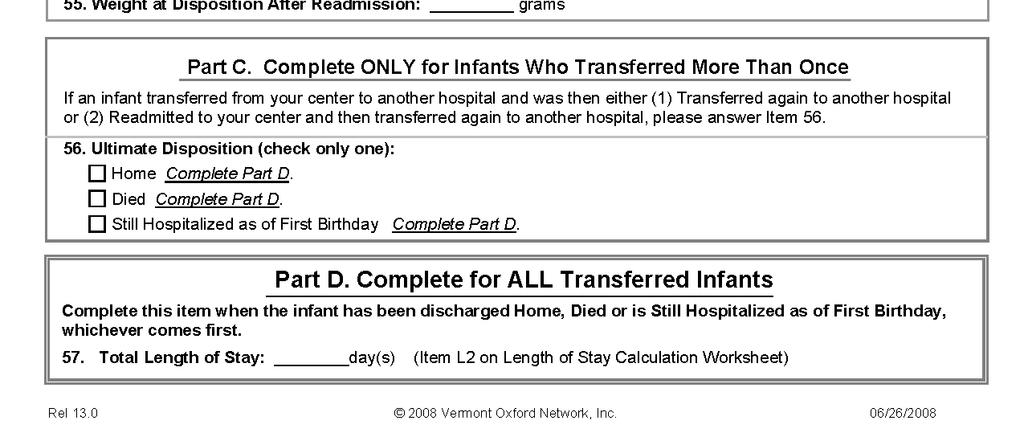
117 109
118 Delivery Room Death Booklet 110
119 111
120 112
121 Supplemental Data 113
122 114
123 APPENDIX B Bacterial Pathogens 1. Achromobacter species [including Achromobacter xylosoxidans (also known as Alcaligenes xylosoxidans) and others] 2. Acinetobacter species 3. Aeromonas species 4. Alcaligenes species [Alcaligenes xylosoxidans and others] 5. Bacteroides species 6. Burkholderia species [Burkholderia capecia and others] 7. Campylobacter species [Campylobacter fetus, C. jejuni and others] 8. Chryseobacterium species 9. Citrobacter species [Citrobacter diversus, C. freundii, C. koseri and others] 10. Clostridium species 11. Enterobacter species [Enterobacter aerogenes, E. cloacae, and others] 12. Enterococcus species [Enterococcus faecalis (also known as Streptococcus faecalis), E. faecium, and other Enterococcus species] 13. Escherichia coli 14. Flavobacterium species 15. Haemophilus species [Haemophilus influenzae and others] 16. Klebsiella species [Klebsiella oxytoca, K. pneumoniae and others] 17. Listeria monocytogenes 18. Moraxella species [Moraxella catarrhalis (also known as Branhamella catarrhalis) and others] 19. Neisseria species [Neisseria meningitidis, N. gonorrhoeae and others] 20. Pasteurella species 21. Prevotella species 22. Proteus species [Proteus mirabilis, P. vulgaris and others] 23. Providencia species [Providencia rettgeri, and others] 24. Pseudomonas species [Pseudomonas aeruginosa and others] 25. Ralstonia species 26. Salmonella species 27. Serratia species [Serratia liquefaciens, S. marcescens and others] 28. Staphylococcus coagulase positive [aureus] 29. Stenotrophomonas maltophilia 30. Streptococcus species [including Streptococcus Group A, Streptococcus Group B, Streptococcus Group D, Streptococcus pneumoniae, Strep milleri and others] 115
124 APPENDIX C Birth Defect Codes Central Nervous System Defects Code Description 101 Anencephaly 102 Meningomyelocele 103 Hydranencephaly 104 Congenital Hydrocephalus 105 Holoprosencephaly 901 Other lethal or life threatening central nervous system defects not listed above (Description Required) Congenital Heart Defects Code Description 201 Truncus Arteriosus 202 Transposition of the Great Vessels 203 Tetralogy of Fallot 204 Single Ventricle 205 Double Outlet Right Ventricle 206 Complete Atrio-Ventricular Canal 207 Pulmonary Atresia 208 Tricuspid Atresia 209 Hypoplastic Left Heart Syndrome 210 Interrupted Aortic Arch 211 Total Anomalous Pulmonary Venous Return 212 Penatalogy of Cantrell (Thoraco-Abdominal Ectopia Cordis) 902 Other lethal or life threatening congenital heart defects not listed above (Description Required) Gastro-Intestinal Defects Code Description 301 Cleft Palate 302 Tracheo-Esophageal Fistula 303 Esophageal Atresia 304 Duodenal Atresia 305 Jejunal Atresia 306 Ileal Atresia 307 Atresia of Large Bowel or Rectum 308 Imperforate Anus 309 Omphalocele 310 Gastroschisis 311 Biliary Atresia 903 Other lethal or life threatening gastro-intestinal defects not listed above (Description Required) 116
125 APPENDIX C, Birth Defect Codes (continued) Genito-Urinary Defects Code Description 401 Bilateral Renal Agenesis 402 Bilateral Polycystic, Multicystic, or Dysplastic Kidneys 403 Obstructive Uropathy with Congenital Hydronephrosis 404 Exstrophy of the Urinary Bladder 904 Other lethal or life threatening Genito-Urinary defects not listed above (Description Required) Chromosomal Abnormalities Code Description 501 Trisomy Trisomy Trisomy Other Chromosomal Anomaly (Description Required) 505 Triploidy Other Birth Defects Code Description 601 Skeletal Dysplasia (Description Required) 602 Congenital Diaphragmatic Hernia 603 Hydrops Fetalis with anasarca and one or more of the following: ascites, pleural effusion, pericardial effusion 604 Oligohydramnios sequence including all 3 of the following: (1) Oligohydramnios documented by antenatal ultrasound 5 or more days prior to delivery, (2) evidence of fetal constraint on postnatal physical exam (such as Potter's facies, contractures, or positional deformities of limbs), and (3) postnatal respiratory failure requiring endotracheal intubation and assisted ventilation. 605 Inborn Error of Metabolism (Description Required) 606 Myotonic Dystrophy requiring endotracheal intubation and assisted ventilation 607 Conjoined Twins 608 Tracheal Agenesis or Atresia 609 Thanatophoric Dysplasia Types 1 and Hemoglobin Barts Pulmonary Abnormalities Code Description 701 Congenital Cystic Adenomatoid Malformation of the Lung 907 Other lethal or life threatening pulmonary malformation (Description Required) Other Lethal or Life Threatening Birth Defects Code Description 100 Other lethal or life threatening birth defects, which are not listed below. (See definition in Chapter 8, Item 44, for instructions). 117
126 APPENDIX D Surgery Codes NOTE: If NEC Surgery and/or Other Surgery on the Discharge Form are checked "Yes", record all applicable codes in Item 33a of the Discharge Form (see Chapter 8). Head and Neck Code S101 S102 S103 Description Tracheostomy/Tracheotomy Cricoid split Ophthalmologic surgery OTHER THAN laser or cryosurgery for ROP NOTE: Record ROP surgery in Item 30. Do not record ROP surgery in Item 33. S104 S105 S106 S107 S108 S100 Cleft lip or palate repair Branchial cleft sinus excision Thyroglossal duct excision Palliative or definitive repair of choanal atresia Mandibular (jaw) distraction Other head and neck surgery requiring general or spinal anesthesia (Description Required) Thorax Code S201 S202 S203 S204 S205 S206 S207 S208 S209 S210 S211 S212 S213 S200 Description Tracheal Resection Aortopexy Tracheoesophageal atresia and/or fistula repair Thoracoscopy (with or without pleural or lung biopsy) Thoracotomy (with or without pleural or lung biopsy) Thoracotomy (or thoracoscopy) with lobectomy or partial lobectomy Resection of pulmonary sequestration (intrathoracic or extrathoracic) Resection of mediastinal mass Resection of chest wall Bronchoscopy (with or without biopsy) Esophagoscopy (with or without biopsy) Surgery for Congenital Cystic Adenomatoid Malformation of the Lung Lung transplant Other thoracic surgery requiring general or spinal anesthesia (Description Required) Abdomen Code Description S301 Rectal biopsy with or without anoscopy S302 Laparoscopy (diagnostic, with/without biopsy) 118
127 APPENDIX D, Surgery Codes (continued) Abdomen (continued) Code S303 S304 S305 S306 S307 S308 S309 S310 S311 S312 S313 S314 S315 S316 S317 S318 S319 S320 S321 S322 S323 S324 S325 S326 S327 S328 S329 S330 S331 S332 S333 S334 S335 S336 S300 Description Laparotomy (diagnostic or exploratory, with/without biopsy) Fundoplication Pyloromyotomy Pyloroplasty Jejunostomy, ileostomy, enterostomy, colostomy for intestinal diversion (with/without bowel resection) Small bowel resection with or without primary anastomosis Large bowel resection Duodenal Atresia/Stenosis Repair Jejunal, ileal, or colonic atresia repair (or repair of multiple intestinal atresias) Excision of Meckel s diverticulum Drainage of intra-abdominal abscess (not as primary treatment for NEC, see code S 333) Surgery for meconium ileus Excision of omphalomesenteric duct or duct remnant Gastroschisis repair (primary or staged) Omphalocele repair (primary or staged) Lysis of adhesions Repair of imperforate anus (with or without vaginal, urethral, or vesicle fistula) Pull through for Hirschsprung s disease (any technique) Pancreatectomy (partial, near total or total) Splenectomy (partial or total) Resection of retroperitoneal tumor Resection of sacrococcygeal tumor Repair of diaphragmatic hernia Plication of the diaphragm Gastrostomy tube Upper endoscopy (stomach or duodenum, with or without biopsy) Colonoscopy (with or without biopsy) Takedown of ostomy and/or reanastomosis of bowel (small or large bowel) Ladd s or other procedure for correction of malrotation Appendectomy Primary peritoneal drainage for NEC, suspected NEC or intestinal perforation (If infant subsequently has other applicable surgical procedures, code those also.) Anoplasty Kasai procedure Open liver biopsy Other abdominal surgery requiring general or spinal anesthesia (Description Required) Genito-Urinary Code Description S401 Cystoscopy (diagnostic, with or without biopsy) S402 Adrenalectomy S403 Nephrectomy 119
128 APPENDIX D, Surgery Codes (continued) Genito-Urinary (continued) Code S404 S405 S406 S407 S408 S409 S410 S411 S412 S413 S414 S416 S417 S400 Description Nephrostomy Urteterostomy Resection of urachal cyst Cystostomy Closure of bladder exstrophy Resection of posterior urethral valves Inguinal hernia repair Orchiopexy Orchiectomy Drainage, excision or removal of ovarian cyst Oopherectomy (partial or complete) Pyeloplasty Renal transplant Other genito-urinary surgery requiring general or spinal anesthesia (Description Required) Open Heart or Vascular Procedures NOTE: PDA ligation is recorded in Item 29. Do not record PDA Ligation in Item 33. Code S501 S502 S503 S504 S505 S500 Description Vascular Ring division Repair of coarctation of the aorta Repair of major vascular injury Repair or palliation of congenital heart disease Heart transplant Other open heart or vascular surgery requiring general or spinal anesthesia (Description Required) Diagnostic or interventional cardiac catheterization Code S601 S602 S603 S604 S600 Description Diagnostic cardiac catheterization Interventional catheterization with balloon septostomy Interventional catheterization with aortic valvuloplasty Interventional catheterization with pulmonary valvuloplasty Other interventional catheterization whether or not anesthesia was required (Description Required) Skin and Soft Tissue Code S700 Description Skin or soft tissue surgery requiring general or spinal anesthesia (Description Required) 120
129 APPENDIX D, Surgery Codes (continued) Musculoskeletal System Code S800 Description Other musculoskeletal surgery requiring general or spinal anesthesia (Description Required) Central Nervous System Code S901 S902 S903 S904 S900 Description Ventriculoperitoneal or other ventricular shunt External ventricular drain Ventricular drain with reservoir Myelomeningocele repair Other central nervous system surgery requiring general or spinal anesthesia (Description Required) Fetal Surgery (record if fetal surgery was done at your hospital or another hospital) Code S1000 S1001 Description Fetal surgery at your hospital (Description Required) Fetal surgery at another hospital (Description Required) Conjoined Twins Code S1101 Description Separation of conjoined twins 121
130 APPENDIX E Calculation Charts for Date of Day 28

131 APPENDIX E: Calculation for Date of Day 28 July to December

132 APPENDIX E: Calculation for Date of Day 28 January to June
133 APPENDIX F Calculation Charts for Date of Week 36


134 APPENDIX F: Calculation Chart for Date of Week 36 January

135 APPENDIX F: Calculation Chart for Date of Week


136 APPENDIX F: Calculation Chart for Date of Week 36 February
137 APPENDIX F: Calculation Chart for Date of Week

138 APPENDIX F: Calculation Chart for Date of Week 36 March
139 APPENDIX F: Calculation Chart for Date of Week

140 APPENDIX F: Calculation Chart for Date of Week 36 April

141 APPENDIX F: Calculation Chart for Date of Week
142 APPENDIX F: Calculation Chart for Date of Week 36 May
143 APPENDIX F: Calculation Chart for Date of Week


144 APPENDIX F: Calculation Chart for Date of Week 36 June
145 APPENDIX F: Calculation Chart for Date of Week


146 APPENDIX F: Calculation Chart for Date of Week 36 July
147 APPENDIX F: Calculation Chart for Date of Week


148 APPENDIX F: Calculation Chart for Date of Week 36 August
149 APPENDIX F: Calculation Chart for Date of Week



150 APPENDIX F: Calculation Chart for Date of Week 36 September
151 APPENDIX F: Calculation Chart for Date of Week


152 APPENDIX F: Calculation Chart for Date of Week 36 October
153 APPENDIX F: Calculation Chart for Date of Week


154 APPENDIX F: Calculation Chart for Date of Week 36 November


155 APPENDIX F: Calculation Chart for Date of Week

156 APPENDIX F: Calculation Chart for Date of Week 36 December
157 APPENDIX G Day Number Chart



158 APPENDIX G: Day Number Chart January March


159 APPENDIX G: Day Number Chart April June


160 APPENDIX G: Day Number Chart July September


161 APPENDIX G: Day Number Chart October December


162 APPENDIX G: Day Number Chart January March


163 APPENDIX G: Day Number Chart April June


164 APPENDIX G: Day Number Chart July September


165 APPENDIX G: Day Number Chart October December
166 APPENDIX H Timeline for Database Activities, 2009 January 1, 2009: January 8, 2009: January 2009: April 8, 2009: April 2009: July 8, 2009: July 2009: Start using new data forms for infants born in the year 2009 Centers submitting data electronically begin using the 2009 file format Deadline for submitting data to be included in the Fourth Quarter Report for 2008 Fourth Quarter Report for 2008 mailed to participating Database members 2008 Membership Survey mailed to participating Database members Data Finalization Guidelines published for centers submitting infant data for 2008 includes deadlines to assure that all infant data are complete and correct for the annual reports. Deadline for submitting data to be included in the First Quarter Report for 2009 First Quarter Report for 2009 mailed to participating Database members 2008 Membership Survey due from participating Database members Deadline for submitting data to be included in the Second Quarter Report for 2009 Second Quarter Report for 2009 mailed to participating Database members September 2009: Annual NICU Quality Management Report for 2008 mailed to centers that finalized their 2008 data October 8, 2009: October 2009: Deadline for submitting data to be included in the Third Quarter Report for 2009 Third Quarter Report for 2009 mailed to participating Database members January 8, 2010: Deadline for submitting data to be included in the Fourth Quarter Report for 2009 data 158
167 APPENDIX I Fahrenheit to Centigrade Conversion Table 159
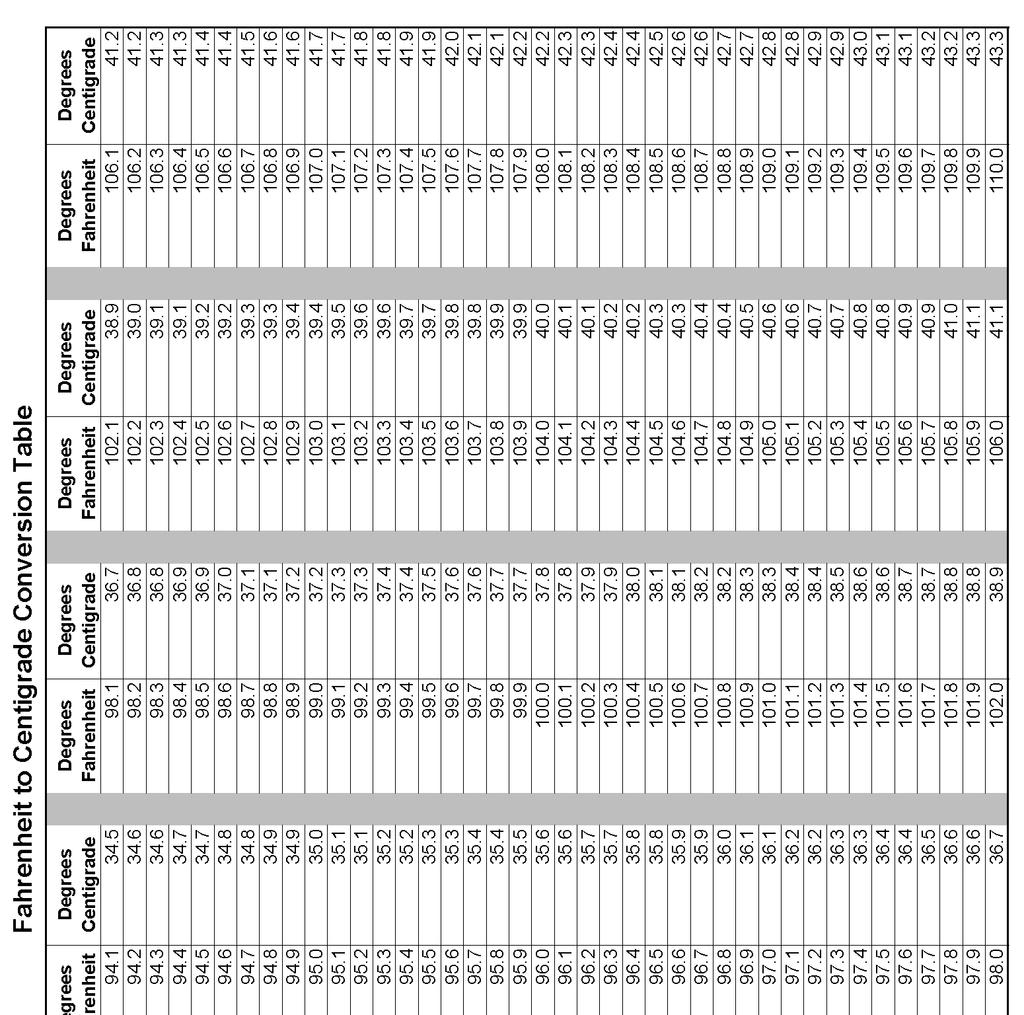
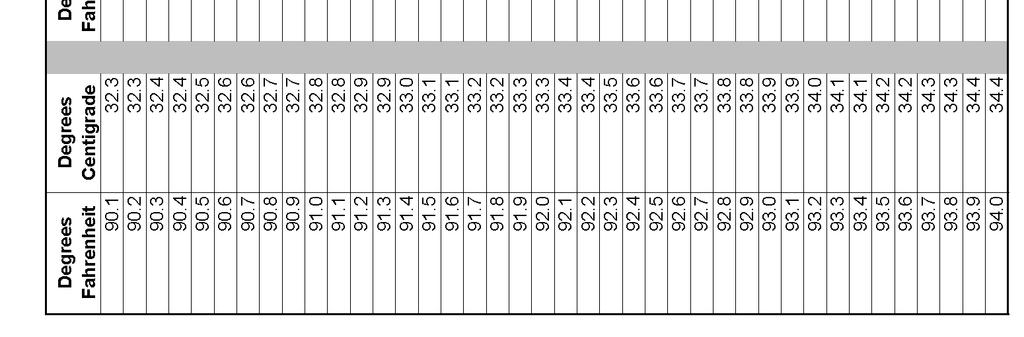
168 160
Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014
 Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014") + Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
+ Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE
 POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE Our network includes 1200+ centers across 30+ countries, collecting critical information on 2.5+ million infants and 72.5+ million patient days. 1 VERMONT
POSITIVELY AFFECTING NEONATAL OUTCOMES WORLDWIDE Our network includes 1200+ centers across 30+ countries, collecting critical information on 2.5+ million infants and 72.5+ million patient days. 1 VERMONT
Quality Improvement in Neonatology. July 27, 2013
 Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Preparing and Registering S.T.A.B.L.E. Support Instructors
 Preparing and Registering S.T.A.B.L.E. Support Instructors If a person is unable to attend an official National or Private Instructor course, but they wish to co-teach a S.T.A.B.L.E. Learner course with
Preparing and Registering S.T.A.B.L.E. Support Instructors If a person is unable to attend an official National or Private Instructor course, but they wish to co-teach a S.T.A.B.L.E. Learner course with
Organization: Adventist Healthcare Shady Grove Medical Center
 Organization: Adventist Healthcare Shady Grove Medical Center Title: A Team-Based, Innovative Approach to Providing Safer Care by Reducing the Incidence of Chronic Lung Disease in the Premature Newborn
Organization: Adventist Healthcare Shady Grove Medical Center Title: A Team-Based, Innovative Approach to Providing Safer Care by Reducing the Incidence of Chronic Lung Disease in the Premature Newborn
93% client retention rate
 Cover Page Partner with a leading provider of children s services. For over 30 years, Sheridan has been a leading provider of children s services, specializing in acute inpatient care and treatment of
Cover Page Partner with a leading provider of children s services. For over 30 years, Sheridan has been a leading provider of children s services, specializing in acute inpatient care and treatment of
PFF Patient Registry Protocol Version 1.0 date 21 Jan 2016
 PFF Patient Registry Protocol Version 1.0 date 21 Jan 2016 Contents SYNOPSIS...3 Background...4 Significance...4 OBJECTIVES & SPECIFIC AIMS...5 Objective...5 Specific Aims... 5 RESEARCH DESIGN AND METHODS...6
PFF Patient Registry Protocol Version 1.0 date 21 Jan 2016 Contents SYNOPSIS...3 Background...4 Significance...4 OBJECTIVES & SPECIFIC AIMS...5 Objective...5 Specific Aims... 5 RESEARCH DESIGN AND METHODS...6
HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS
 HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS 2013 BORN INFANT RECORDS 2015 BORN INFANT STANDARD VISIT #1 FOR ALL EXPECTED 2016 BORN INFANT REFERRAL/REGISTRATIONS
HIGH RISK INFANT FOLLOW-UP QUALITY OF CARE INITIATIVE DATA FINALIZATION PROCESS GUIDELINES AND TOOLS 2013 BORN INFANT RECORDS 2015 BORN INFANT STANDARD VISIT #1 FOR ALL EXPECTED 2016 BORN INFANT REFERRAL/REGISTRATIONS
The Vermont Oxford Network: A Community of Practice
 The Vermont Oxford Network: A Community of Practice Jeffrey D. Horbar, MD a,b, *, Roger F. Soll, MD a,b, William H. Edwards, MD b,c KEYWORDS Vermont Oxford Network Newborn Safety Quality The Vermont Oxford
The Vermont Oxford Network: A Community of Practice Jeffrey D. Horbar, MD a,b, *, Roger F. Soll, MD a,b, William H. Edwards, MD b,c KEYWORDS Vermont Oxford Network Newborn Safety Quality The Vermont Oxford
The Criminal Justice Information System at the Department of Public Safety and the Texas Department of Criminal Justice. May 2016 Report No.
 An Audit Report on The Criminal Justice Information System at the Department of Public Safety and the Texas Department of Criminal Justice Report No. 16-025 State Auditor s Office reports are available
An Audit Report on The Criminal Justice Information System at the Department of Public Safety and the Texas Department of Criminal Justice Report No. 16-025 State Auditor s Office reports are available
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
High Risk Infant Follow Up
 http://www.dhcs.ca.gov/services/ccs/pages/hrif.aspx Page 1 of 9 California Children's Services Contact Us Career Opportunities He Search Home > Services > California Children's Services > Select Language
http://www.dhcs.ca.gov/services/ccs/pages/hrif.aspx Page 1 of 9 California Children's Services Contact Us Career Opportunities He Search Home > Services > California Children's Services > Select Language
Quality Improvement Plan
 Quality Improvement Plan Agency Mission: The mission of MMSC Home Care Plus is to at all times render high quality, comprehensive, safe and cost-effective home health care and public health services to
Quality Improvement Plan Agency Mission: The mission of MMSC Home Care Plus is to at all times render high quality, comprehensive, safe and cost-effective home health care and public health services to
The Leapfrog Hospital Survey Scoring Algorithms. Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey
 The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
Chan Man Yi, NC (Neonatal Care) Dept. of Paed. & A.M., PMH 16 May 2017
 Dept. of Paed. & A.M., PMH 16 May 2017") The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 1
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
State Policy in Practice
 July 2005 State Policy in Practice Community Living Exchange Funded by Centers for Medicare & Medicaid Services (CMS) South Carolina s Care Call Susan Reinhard Ann Bemis This document was prepared by Susan
July 2005 State Policy in Practice Community Living Exchange Funded by Centers for Medicare & Medicaid Services (CMS) South Carolina s Care Call Susan Reinhard Ann Bemis This document was prepared by Susan
The Cost of a Misfiled Medical Document
 : The Cost of a Misfiled Medical Document INTRODUCTION Misfiling of medical documents is a common problem in all types of medical practices. A document may be misfiled for a number of reasons, and each
: The Cost of a Misfiled Medical Document INTRODUCTION Misfiling of medical documents is a common problem in all types of medical practices. A document may be misfiled for a number of reasons, and each
Neonatal Intensive Care Unit (NICU) Level of Care Authorization and Reimbursement Policy
 Level of Care Authorization and Reimbursement Policy") In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
Micro-Preemies.Macro Outcomes Keywords: Background: Global AIM: Secondary Aims: Golden Hour Charter (Focus on thermoregulation): Respiratory Charter
: Respiratory Charter") Micro-Preemies.Macro Outcomes Carey Gaede, NNP-BC; Mary Jane Zonfrilli, NNP-BC; Stephanie King, RRT; Sara Dalbey, NNP-BC; Lisa Davis, NNP-BC; William Stratton, MD Primary: Carey Gaede, NNP-BC; e-mail:
Micro-Preemies.Macro Outcomes Carey Gaede, NNP-BC; Mary Jane Zonfrilli, NNP-BC; Stephanie King, RRT; Sara Dalbey, NNP-BC; Lisa Davis, NNP-BC; William Stratton, MD Primary: Carey Gaede, NNP-BC; e-mail:
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Page 1 of 26. Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014
 Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
Uniform Data System for Medical Rehabilitation
 Uniform Data System for Medical Rehabilitation 270 Northpointe Parkway, Suite 300, Amherst, New York 14228 tel: 716-817-7800 fax: 716-568-0037 The Functional Assessment Specialists UDSMR Credentialing
Uniform Data System for Medical Rehabilitation 270 Northpointe Parkway, Suite 300, Amherst, New York 14228 tel: 716-817-7800 fax: 716-568-0037 The Functional Assessment Specialists UDSMR Credentialing
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Baby-MONITOR. Composite Measure of NICU Quality
 Baby-MONITOR Composite Measure of NICU Quality By The Numbers Working across the continuum of care 500K 17K 140 7K 9K BIRTHS NICU ADMITS MEMBER HOSPITALS ACUTE NEONATAL TRANSPORTS HIGH-RISK INFANTS REGISTERED
Baby-MONITOR Composite Measure of NICU Quality By The Numbers Working across the continuum of care 500K 17K 140 7K 9K BIRTHS NICU ADMITS MEMBER HOSPITALS ACUTE NEONATAL TRANSPORTS HIGH-RISK INFANTS REGISTERED
Newborn bloodspot screening
 Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012
 HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 2
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
The Makings of a Small Baby Unit. Objectives. What s the big deal? 9/28/16
 The Makings of a Small Baby Unit Anamika B. Mukherjee, MD, MS Assistant Professor of Pediatrics Loma Linda Children s Hospital Division of Neonatology September 28, 2016 Objectives What is a Small Baby
The Makings of a Small Baby Unit Anamika B. Mukherjee, MD, MS Assistant Professor of Pediatrics Loma Linda Children s Hospital Division of Neonatology September 28, 2016 Objectives What is a Small Baby
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures
 The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
Hirslanden promotes quality and safety in patient care by subscribing to the European Foundation
 CLINICAL GOVERNANCE REPORT LEADERSHIP IS INDISPENSABLE in THE PROMOTION OF QUALITY AND SAFETY OF PATIENT CARE 54 MEDICLINIC INTEGRATED ANNUAL REPORT 2012 Clinical Governance INTRODUCTION Mediclinic strives
CLINICAL GOVERNANCE REPORT LEADERSHIP IS INDISPENSABLE in THE PROMOTION OF QUALITY AND SAFETY OF PATIENT CARE 54 MEDICLINIC INTEGRATED ANNUAL REPORT 2012 Clinical Governance INTRODUCTION Mediclinic strives
Study Management PP STANDARD OPERATING PROCEDURE FOR Safeguarding Protected Health Information
 PP-501.00 SOP For Safeguarding Protected Health Information Effective date of version: 01 April 2012 Study Management PP 501.00 STANDARD OPERATING PROCEDURE FOR Safeguarding Protected Health Information
PP-501.00 SOP For Safeguarding Protected Health Information Effective date of version: 01 April 2012 Study Management PP 501.00 STANDARD OPERATING PROCEDURE FOR Safeguarding Protected Health Information
Appendix: Data Sources and Methodology
 Appendix: Data Sources and Methodology This document explains the data sources and methodology used in Patterns of Emergency Department Utilization in New York City, 2008 and in an accompanying issue brief,
Appendix: Data Sources and Methodology This document explains the data sources and methodology used in Patterns of Emergency Department Utilization in New York City, 2008 and in an accompanying issue brief,
Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS
 Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS Welcome to the 2017 Leapfrog Hospital Survey... 6 Important Notes about the 2017 Survey... 6 Overview
Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS Welcome to the 2017 Leapfrog Hospital Survey... 6 Important Notes about the 2017 Survey... 6 Overview
National Cervical Screening Programme Policies and Standards. Section 2: Providing National Cervical Screening Programme Register Services
 National Cervical Screening Programme Policies and Standards Section 2: Providing National Cervical Screening Programme Register Services Citation: Ministry of Health. 2014. National Cervical Screening
National Cervical Screening Programme Policies and Standards Section 2: Providing National Cervical Screening Programme Register Services Citation: Ministry of Health. 2014. National Cervical Screening
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
EHDI TSI Program Narrative
 EHDI TSI Program Narrative Executive Summary Achievements The beginning of the Tennessee Early Hearing Detection and Intervention Tracking, Surveillance, and Integration (EHDI TSI) project was marked by
EHDI TSI Program Narrative Executive Summary Achievements The beginning of the Tennessee Early Hearing Detection and Intervention Tracking, Surveillance, and Integration (EHDI TSI) project was marked by
The following policy was adopted by the San Luis Obispo County EMS Agency and will become effective March 1, 2012 at 0800 hours.
 SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
SOFTWARE REQUIREMENTS SPECIFICATION Hospital Management System
 Introduction: SOFTWARE REQUIREMENTS SPECIFICATION Hospital Management System This is a Software Requirements Specification (SRS) for the Hospital Management System. It describes the functions, goals and
Introduction: SOFTWARE REQUIREMENTS SPECIFICATION Hospital Management System This is a Software Requirements Specification (SRS) for the Hospital Management System. It describes the functions, goals and
Randomized Controlled Trials to Test Interventions for Frequent Utilizers of Multiple Health, Criminal Justice, and Social Service Systems
 REQUEST FOR PROPOSALS: Randomized Controlled Trials to Test Interventions for Frequent Utilizers of Multiple Health, Criminal Justice, and Social Service Systems August 2017 PROJECT OVERVIEW AND REQUEST
REQUEST FOR PROPOSALS: Randomized Controlled Trials to Test Interventions for Frequent Utilizers of Multiple Health, Criminal Justice, and Social Service Systems August 2017 PROJECT OVERVIEW AND REQUEST
CPQCC. California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS JEFFREY B. GOULD, MD, MPH
 CPQCC California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS 1997-2015 JEFFREY B. GOULD, MD, MPH DIRECTOR, PERINATAL EPIDEMIOLOGY AND OUTCOMES UNIT DEPARTMENT OF PEDIATRICS STANFORD
CPQCC California Perinatal Quality Care Collaborative DESIGN AND ACCOMPLISHMENTS 1997-2015 JEFFREY B. GOULD, MD, MPH DIRECTOR, PERINATAL EPIDEMIOLOGY AND OUTCOMES UNIT DEPARTMENT OF PEDIATRICS STANFORD
Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS
 Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS Welcome to the 2018 Leapfrog Hospital Survey... 6 Important Notes about the 2018 Survey... 6 Overview
Leapfrog Hospital Survey Hard Copy QUESTIONS & REPORTING PERIODS ENDNOTES MEASURE SPECIFICATIONS FAQS Welcome to the 2018 Leapfrog Hospital Survey... 6 Important Notes about the 2018 Survey... 6 Overview
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
NYS Congenital Malformations Registry Converting to a Web-based System. NYS Congenital Malformations Registry Converting to a Web-based System
 NYS Congenital Malformations Registry Converting to a Web-based System National Birth Defects Prevention Network Nashville, TN February 23-25, 2009 NYS Congenital Malformations Registry Converting to a
NYS Congenital Malformations Registry Converting to a Web-based System National Birth Defects Prevention Network Nashville, TN February 23-25, 2009 NYS Congenital Malformations Registry Converting to a
About the Report. Cardiac Surgery in Pennsylvania
 Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Cardiac Surgery in Pennsylvania This report presents outcomes for the 29,578 adult patients who underwent coronary artery bypass graft (CABG) surgery and/or heart valve surgery between January 1, 2014
Clinical Practice Guideline Development Manual
 Clinical Practice Guideline Development Manual Publication Date: September 2016 Review Date: September 2021 Table of Contents 1. Background... 3 2. NICE accreditation... 3 3. Patient Involvement... 3 4.
Clinical Practice Guideline Development Manual Publication Date: September 2016 Review Date: September 2021 Table of Contents 1. Background... 3 2. NICE accreditation... 3 3. Patient Involvement... 3 4.
e-sdrt User Guide, Update April 2014 First Nations and Inuit Home and Community Care Program: e-sdrt User Guide
 e-sdrt User Guide, Update April 2014 First Nations and Inuit Home and Community Care Program: e-sdrt User Guide 1 e-sdrt User Guide, Update April 2014 2 e-sdrt User Guide, Update April 2014 TABLE OF CONTENTS
e-sdrt User Guide, Update April 2014 First Nations and Inuit Home and Community Care Program: e-sdrt User Guide 1 e-sdrt User Guide, Update April 2014 2 e-sdrt User Guide, Update April 2014 TABLE OF CONTENTS
Sevocity v Advancing Care Information User Reference Guide
 Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
Sevocity v.12 User Reference Guide 1 877 877-2298 support@sevocity.com Table of Contents About Advancing Care Information... 3 Setup Requirements... 3 Product Support Services... 3 About Sevocity v.12...
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA
 REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
September 2011 Report No
 John Keel, CPA State Auditor An Audit Report on The Criminal Justice Information System at the Department of Public Safety and the Texas Department of Criminal Justice Report No. 12-002 An Audit Report
John Keel, CPA State Auditor An Audit Report on The Criminal Justice Information System at the Department of Public Safety and the Texas Department of Criminal Justice Report No. 12-002 An Audit Report
How to Add an Annual Facility Survey
 Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
Registry Evaluation Form
 Evaluator Name: Areas of Evaluation Registry Evaluation Form 1. User friendliness a) Training time to learn b) Screen readability c) Navigation intuitiveness (is it easy to figure out where you want to
Evaluator Name: Areas of Evaluation Registry Evaluation Form 1. User friendliness a) Training time to learn b) Screen readability c) Navigation intuitiveness (is it easy to figure out where you want to
Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors. Summer 2012
 Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors Summer 2012 Developed by the U.S. Department of Education Office of Migrant Education through a contract with
Migrant Education Comprehensive Needs Assessment Toolkit A Tool for State Migrant Directors Summer 2012 Developed by the U.S. Department of Education Office of Migrant Education through a contract with
National Police Promotion Framework. Data Capture Force Guidance 2011/2012. May Version 1.3
 National Police Promotion Framework Data Capture Force Guidance 2011/2012 May 2011 Version 1.3 National Police Promotion Framework Force Guidance For Data Capture (c) - NPIA (National Policing Improvement
National Police Promotion Framework Data Capture Force Guidance 2011/2012 May 2011 Version 1.3 National Police Promotion Framework Force Guidance For Data Capture (c) - NPIA (National Policing Improvement
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES
 CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES STANDARD OPERATING PROCEDURES Ysbyty Glan Clwyd Telephone No: 01745 534686 Fax No: 01745 534681 Date: June 2015 Authors: Neonatal Transport
CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES STANDARD OPERATING PROCEDURES Ysbyty Glan Clwyd Telephone No: 01745 534686 Fax No: 01745 534681 Date: June 2015 Authors: Neonatal Transport
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Efficacy of Tympanostomy Tubes for Children with Recurrent Acute Otitis Media Randomization Phase
 CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
Northern Ireland Peer Review of Cancer MDTs. EVIDENCE GUIDE FOR LUNG MDTs
 Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Indicator. unit. raw # rank. HP2010 Goal
 Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Case-Mix Data for Case Ascertainment
 Case-Mix Data for Case Ascertainment Mary Jane King, MPH, CTR Registry Operations Massachusetts Cancer Registry Tel: (617) 624-5622 Fax: (617) 624-5695 mary.jane.king@state.ma.us 1 Outline History, Needs
Case-Mix Data for Case Ascertainment Mary Jane King, MPH, CTR Registry Operations Massachusetts Cancer Registry Tel: (617) 624-5622 Fax: (617) 624-5695 mary.jane.king@state.ma.us 1 Outline History, Needs
SurgiVision Consultants, Inc. February 10, 2009
 DataLink Alcon Edition Data Entry Tutorial February 10, 2009 DataLink Alcon Edition This is a web-based program, which means that - You do not have to install or update any software - You do have to remember
DataLink Alcon Edition Data Entry Tutorial February 10, 2009 DataLink Alcon Edition This is a web-based program, which means that - You do not have to install or update any software - You do have to remember
PRIVACY IMPACT ASSESSMENT (PIA) For the
 For the") PRIVACY IMPACT ASSESSMENT (PIA) For the Marine Sierra Hotel Aviation Readiness Program (M-SHARP) Department of the Navy - United States Marine Corps (USMC) SECTION 1: IS A PIA REQUIRED? a. Will this Department
PRIVACY IMPACT ASSESSMENT (PIA) For the Marine Sierra Hotel Aviation Readiness Program (M-SHARP) Department of the Navy - United States Marine Corps (USMC) SECTION 1: IS A PIA REQUIRED? a. Will this Department
Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013
 GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
Application Process for Individual HCPs
 HCF Program Training Application Process for Individual HCPs HCF Program Training I Application Process I September 2015 1 This training is just a general overview and starting point for applicants Every
HCF Program Training Application Process for Individual HCPs HCF Program Training I Application Process I September 2015 1 This training is just a general overview and starting point for applicants Every
Privacy Toolkit for Social Workers and Social Service Workers Guide to the Personal Health Information Protection Act, 2004 (PHIPA)
") Social Workers and Social Service Workers Guide to the Personal Health Information Protection Act, 2004 (PHIPA) COPYRIGHT 2005 BY ONTARIO COLLEGE OF SOCIAL WORKERS AND SOCIAL SERVICE WORKERS ALL RIGHTS
Social Workers and Social Service Workers Guide to the Personal Health Information Protection Act, 2004 (PHIPA) COPYRIGHT 2005 BY ONTARIO COLLEGE OF SOCIAL WORKERS AND SOCIAL SERVICE WORKERS ALL RIGHTS
Purpose: To create a record capturing key data about a submitted proposal for reference and reporting purposes.
 Kuali Research User Guide: Create Institutional Proposal Version 4.0: vember 206 Purpose: To create a record capturing key data about a submitted proposal for reference and reporting purposes. Trigger
Kuali Research User Guide: Create Institutional Proposal Version 4.0: vember 206 Purpose: To create a record capturing key data about a submitted proposal for reference and reporting purposes. Trigger
AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS
 CHAPTER VII AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS This chapter includes background information and descriptions of the following tools FHOP has developed to assist local health jurisdictions
CHAPTER VII AVAILABLE TOOLS FOR PUBLIC HEALTH CORE DATA FUNCTIONS This chapter includes background information and descriptions of the following tools FHOP has developed to assist local health jurisdictions
Case Study. Check-List for Assessing Economic Evaluations (Drummond, Chap. 3) Sample Critical Appraisal of
 Sample Critical Appraisal of") Case Study Work in groups At most 7-8 page, double-spaced, typed critical appraisal of a published CEA article Start with a 1-2 page summary of the article, answer the following ten questions, and then
Case Study Work in groups At most 7-8 page, double-spaced, typed critical appraisal of a published CEA article Start with a 1-2 page summary of the article, answer the following ten questions, and then
XIII. Health Statistics and Research. Kathy C. Trawick, EdD, RHIA, FAHIMA
 XIII. Health Statistics and Research Kathy C. Trawick, EdD, RHIA, FAHIMA Health Statistics and Research 369 As noted in the main Introduction section, you will be able to access some statistical formulas
XIII. Health Statistics and Research Kathy C. Trawick, EdD, RHIA, FAHIMA Health Statistics and Research 369 As noted in the main Introduction section, you will be able to access some statistical formulas
A Randomized Trial of Supplemental Parenteral Nutrition in. Under and Over Weight Critically Ill Patients: The TOP UP Trial. CRS & REDCap Manual
 A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients: The TOP UP Trial CRS & REDCap Manual Intended Audience: Research Coordinators This study is registered
A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients: The TOP UP Trial CRS & REDCap Manual Intended Audience: Research Coordinators This study is registered
ENTERPRISE INCOME VERIFICATION (EIV) SECURITY POLICY
 SECURITY POLICY") ENTERPRISE INCOME VERIFICATION (EIV) SECURITY POLICY Rev. October 2011 EIV Security Policy Acknowledgment Form By signing this form I acknowledge my receipt of the EIV System Security Policy approved by
ENTERPRISE INCOME VERIFICATION (EIV) SECURITY POLICY Rev. October 2011 EIV Security Policy Acknowledgment Form By signing this form I acknowledge my receipt of the EIV System Security Policy approved by
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
CHAPTER 1. Documentation is a vital part of nursing practice.
 CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
Request for Proposal Congenital Syphilis Study
 Request for Proposal Congenital Syphilis Study INTRODUCTION AND BACKGROUND The March of Dimes Foundation (MOD) is a national voluntary health agency whose mission is to improve the health of babies by
Request for Proposal Congenital Syphilis Study INTRODUCTION AND BACKGROUND The March of Dimes Foundation (MOD) is a national voluntary health agency whose mission is to improve the health of babies by
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
Hospital IQR Program Hybrid Hospital-Wide 30-Day Readmission Measure Core Clinical Data Elements for Calendar Year 2018 Voluntary Data Submission Questions and Answers Moderator Artrina Sturges, EdD, MS
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM
 RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE May 2017 Contents Introduction... 3 Access to REACH... 3 Homepage... 3 Roles within REACH... 4 Hospital Administrator... 4 Hospital User... 4
RETRIEVAL AND CRITICAL HEALTH INFORMATION SYSTEM USER GUIDE May 2017 Contents Introduction... 3 Access to REACH... 3 Homepage... 3 Roles within REACH... 4 Hospital Administrator... 4 Hospital User... 4
total health and wellness
 total health and wellness Programs exclusively for our Blue Shield members total health and wellness Whether you want to ease stress, lose weight, or quit smoking we ll help you reach your goals. Our health
total health and wellness Programs exclusively for our Blue Shield members total health and wellness Whether you want to ease stress, lose weight, or quit smoking we ll help you reach your goals. Our health
TOWN HALL CALL 2017 LEAPFROG HOSPITAL SURVEY. May 10, 2017
 2017 LEAPFROG HOSPITAL SURVEY TOWN HALL CALL May 10, 2017 Matt Austin, PhD, Armstrong Institute for Patient Safety and Quality, Johns Hopkins Medicine 2 Leapfrog Hospital Survey Overview Annual Survey
2017 LEAPFROG HOSPITAL SURVEY TOWN HALL CALL May 10, 2017 Matt Austin, PhD, Armstrong Institute for Patient Safety and Quality, Johns Hopkins Medicine 2 Leapfrog Hospital Survey Overview Annual Survey
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
Efficiency Research Programme
 Efficiency Research Programme A Health Foundation call for innovative research on system efficiency and sustainability in health and social care Frequently asked questions April 2016 Table of contents
Efficiency Research Programme A Health Foundation call for innovative research on system efficiency and sustainability in health and social care Frequently asked questions April 2016 Table of contents
Study Guide for Emergency Care Clinicians. (Version /09/2014)
") Study Guide for Emergency Care Clinicians (Version 1.2 26/09/2014) Notes 1. These learning materials are aimed primarily at paramedics, ambulance nurses, emergency care practitioners and doctors recruiting
Study Guide for Emergency Care Clinicians (Version 1.2 26/09/2014) Notes 1. These learning materials are aimed primarily at paramedics, ambulance nurses, emergency care practitioners and doctors recruiting
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage
 PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
Skills Assessment. Monthly Neonatologist evaluation of the fellow s performance
 Patient Care Interviews patients The Y1 will be able to verbally obtain an accurate history on new NICU: Observation of Neonatologist evaluating a Goal: Practice patient care accurately and effectively
Patient Care Interviews patients The Y1 will be able to verbally obtain an accurate history on new NICU: Observation of Neonatologist evaluating a Goal: Practice patient care accurately and effectively
WHO Pharmacovigilance Indicators. Dr. Nitin Gaikwad Co-coordinator, ADR Monitoring Center, PvPI Additional Professor, Pharmacology AIIMS Raipur
 WHO Pharmacovigilance Indicators Dr. Nitin Gaikwad Co-coordinator, ADR Monitoring Center, PvPI Additional Professor, Pharmacology AIIMS Raipur Scope of presentation Sensitization of Coordinators, Co-coordinators,
WHO Pharmacovigilance Indicators Dr. Nitin Gaikwad Co-coordinator, ADR Monitoring Center, PvPI Additional Professor, Pharmacology AIIMS Raipur Scope of presentation Sensitization of Coordinators, Co-coordinators,
Healthy Kids Connecticut. Insuring All The Children
 Healthy Kids Connecticut Insuring All The Children Goals & Objectives Provide affordable and accessible health care to the 71,000 uninsured children Eliminate waste in the system Develop better ways to
Healthy Kids Connecticut Insuring All The Children Goals & Objectives Provide affordable and accessible health care to the 71,000 uninsured children Eliminate waste in the system Develop better ways to
Family Integrated Care in the NICU
 Family Integrated Care in the NICU Shoo Lee, MBBS, FRCPC, PhD Scientific Director, Institute of Human Development, Child & Youth Health, Canadian Institutes of Health Research Professor of Paediatrics,
Family Integrated Care in the NICU Shoo Lee, MBBS, FRCPC, PhD Scientific Director, Institute of Human Development, Child & Youth Health, Canadian Institutes of Health Research Professor of Paediatrics,
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Office of Clinical Research. CTMS Reference Guide Patient Entry & Visit Tracking
 Se Office of Clinical Research CTMS Reference Guide Patient Entry & Visit Tracking Table of Contents Logging into CTMS... 3 Search and Recruitment / Quick Search... 4 How to Configure Quick Search Fields...
Se Office of Clinical Research CTMS Reference Guide Patient Entry & Visit Tracking Table of Contents Logging into CTMS... 3 Search and Recruitment / Quick Search... 4 How to Configure Quick Search Fields...
HCAHPS Quality Assurance Guidelines V6.0 Summary of Updates and Emphasis
 This document is a reference tool that highlights the major changes from the HCAHPS Quality Assurance Guidelines V5.0 to V6.0. This document is not a substitute for reviewing the HCAHPS Quality Assurance
This document is a reference tool that highlights the major changes from the HCAHPS Quality Assurance Guidelines V5.0 to V6.0. This document is not a substitute for reviewing the HCAHPS Quality Assurance
July 2, 2010 Hospital Compare: New ED and Outpatient. Information; Annual Update to Readmission and Mortality Rates
 July 2, 2010 Hospital Compare: New ED and Outpatient Information; Annual Update to Readmission and Mortality Rates AT A GLANCE The Issue: In early July, information on care provided in the hospital outpatient
July 2, 2010 Hospital Compare: New ED and Outpatient Information; Annual Update to Readmission and Mortality Rates AT A GLANCE The Issue: In early July, information on care provided in the hospital outpatient
Health Quality Ontario
 Health Quality Ontario The provincial advisor on the quality of health care in Ontario November 15, 2016 Under Pressure: Emergency department performance in Ontario Technical Appendix Table of Contents
Health Quality Ontario The provincial advisor on the quality of health care in Ontario November 15, 2016 Under Pressure: Emergency department performance in Ontario Technical Appendix Table of Contents