Care Transition Strategies To Reduce Readmissions
|
|
|
- Chester Johnson
- 6 years ago
- Views:
Transcription

1 Session Codes D:6 & E:6 Premier Inc. provides services to Hackensack University Medical Center for which it receives a fee. The presentation materials are for informational purposes only and are not offered as legal or other advice. Care Transition Strategies To Reduce Readmissions Jenny Bernard, APN Advanced Practice Nurse, Transitions of Care Jeanette Previdi, MPH, BSN, RN, CPPS Patient Safety and Quality Advisor Madeleine Biondolillo, MD,MBA VP, Quality and Safety Quest/Premier Wednesday, December 13, :30am 10:45am 11:15am 12:30pm #IHIFORUM
2 Learning Objectives Develop an understanding of practical measurement approaches and rigorous evaluation to identify gaps in care Learn how to test interventions to reduce readmissions in high-risk patients, track results and identify improvement areas Access proven methods to implement and sustain improvement

3 A group of hospitals collectively reduced readmissions by 32% in under 8 years. How did they do this?

4 QUEST 2020 National Collaborative supporting over 200 hospitals and health systems to reliably deliver the highest quality care in a value-based health care environment Madeleine Biondolillo, MD, MBA VP, Quality and Safety Madeleine_Biondolillo@Premierinc.com TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 4
5 Quality Efficiency Safety Transparency A collaborative designed to help hospitals and health systems reliably deliver the highest quality care in a value-based healthcare environment. QUEST leverages analytics, education and best practices to accelerate performance improvement, with complete transparency within the membership. TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 5

6 QUEST over 10 Years an Award Winning Collaborative Premier and the health systems that participate in QUEST have made exceptional achievements in patient safety and healthcare quality We can only improve patient safety if we can measure and report on our efforts and the QUEST participants inspire the industry to improve care safety and quality across all settings of care. -National Quality Forum MALCOLM BALDRIGE NATIONAL QUALITY AWARD WINNER TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 6
7 Thought Leadership, Advocacy, Collaboration QUEST Advisory Panel Agency for Healthcare Research and Quality (AHRQ) Alliance for Nursing Informatics, University of Minnesota American Board of Internal Medicine American College of Surgeons American Health Information Management Association American Heart Association American Hospital Association American Society for Healthcare Risk Management (ASHRM) Blue Cross Blue Shield Association (BCBSA) Centers for Disease Control and Prevention (CDC) Centers for Medicare & Medicaid Services (CMS Institute for Healthcare Improvement (IHI) International Center for Nursing Leadership University of Minnesota John D. Stoeckle Center for Primary Care Innovation, Massachusetts General Hospital National Business Coalition on Health National Patient Safety Foundation (NPSF) National Quality Forum Office of the National Coordinator for Health Information Technology The Commonwealth Fund The Joint Commission The Rand Corporation TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 7


8 QUEST Proven Collaborative Methodology ACCELERATING IMPROVEMENT Measure with defined metrics Report transparently Share best practice Execute collaboratively Knowing is not enough; we must apply. Willing is not enough; we must do. -Johann Wolfgang von Goethe TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 8


9 QUEST 2020 Data Alignment and Continuum of Care Focus Supports Hospitals Success Acute Ambulatory Community Measures Align with National Quality Strategy Safety Care coordination Affordable care Person family experience Health and well-being Prevention and treatment TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 9
10 QUEST Delivering Differentiated Performance Improving Care More winners under Value-Based Purchasing Program Higher scores under Hospital Compare s 5-Star Rating System QUEST FY 2016 Inpatient Non-QUEST Matched Sample FY 2016 Inpatient QUEST 1% 6% 3.34 RATING 36% 44% 64% 50% Non-QUEST Matched Sample 2.93 RATING Exempt Lose Win TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 10 Premier compared the CMS star ratings between Premier QUEST hospitals and non-quest hospitals (non-premier facilities) to explore potential differences in facility performance. Facilities were propensity-score matched using facility size (licensed beds), region (Northeast, Midwest, West, South), urban/rural population, and teaching status. Mean performance was compared using an independent samples t-test. The results showed that Premier QUEST members scored significantly higher (3.25 vs. 2.95; p<0.0001) than non-quest facilities. Similar results were obtained from comparing the HCAHPS star ratings (3.29 vs. 2.93; p<0.0001) indicating a consistent trend in higher performance for Premier QUEST members.
11 The next wave of high performance collaboration QUEST Performance ( ) 203,600 Deaths Avoided in 9 Years of QUEST $17.7B Saved in 9 Years of QUEST 45,222 Readmissions Prevented During ,382 Harm Events Prevented During ,352 Patients Receiving Evidence Based Care During QUEST 3.0 TRANSFORMING HEALTHCARE TOGETHER 2017 PROPRIETARY & CONFIDENTIAL 11




12 Hackensack University Medical Center 775 bed, non-profit, teaching, and research hospital in Bergen County, NJ Our Mission to provide the full spectrum of life-enhancing care and services to create and sustain healthy, vibrant communities Healthgrades America s 50 Best Hospitals - one of only five major academic medical centers in the nation to receive Healthgrades America s 50 Best Hospitals Award for five or more years in a row U.S. News & World Report - #1 hospital in NJ and top four in New York metro area Leapfrog - Top Hospital list Magnet designated for 5 years The Joint Commission - 25 Gold Seals of Approval, including Heart Failure and AMI the most in the country Becker's Hospital Review in one of 100 Great Hospitals in America



13 Healthcare Trends US Healthcare spending $3.2 trillion in % increase in 2015 $9,990 per person Impact of affordable care act Readmission penalties Medicare reimbursements Target diagnoses groups Shift in healthcare culture Change in hospital practices Focused on reducing readmissions Creation of discharge programs Models to improve patient satisfaction 41% Medicare 13% Private Insurance 25% 21% Medicaid Out of Pocket 18% of paid admissions readmitted within 30 days us.ahrq.gov/reports/statbriefs/sb196- Readmissions-Trends-High-Volume- Conditions.pdf
14 Hospital Challenges Value CMS Pay For Performance CMS Shifting from Fee for Service to Paying for Value 2,597 hospitals were financially penalized in Medicare payments in in 5 patients readmitted to hospital within 30 days Lots of chronic disease I don t understand what to do These drugs are expensive I don t have transportation
 Dollars at Risk At Hackensack University Medical Center, approximate")
15 CMS Pay For Performance Shift from Fee for Service to Paying for Value CMS Pay For Performance for Value CMS Shifting from Fee for Service to Paying for Value Inpatient Center for Medicare and Medicaid Services Payments At Risk for FY 2017 (Based on Approximately $150M in DRG Payments and $200M in DRG, DSH, IME Payments) Dollars at Risk At Hackensack University Medical Center, approximate cost of one excess readmission = $19,000

 Team")





16 Our Transitions of Care (TOC) Team Administrator TOC APN Mgr. TOC Pharmacist Quality Advisor Senior VP, Quality Director, Finance Director, Data TOC Case Mgr.


17 TOC Project Stakeholders Leadership Safety & Quality Physicians Case Management Finance Pharmacy External Partners Patient & Caregiver
18 Case Study Mr. J.G. is a 64-year-old single Hispanic male Undocumented from Honduras - in USA for 2 years History of CHF, DM, HTN, High Cholesterol, recent AMI and multiple hospital readmissions No children and lives with his sister Unemployed without health insurance and very limited financial resources Poor health literacy and low educational level Spanish speaking only and unable to read

19 Literature review Evaluate current process Review of data Multidisciplinary Rounds Observations Chart review Patient interviews Identifying Gaps
20 Pre-Intervention Readmission Data For 2-yr period prior to The First Thirty TOC program (1/12 3/15), in a like group of 242 AMI/CHF patients, readmission rate was 13.22% (expected rate 13.24, O/E index 1.00) Pre-Intervention First Thirty (DSRIP) Readmission Rates vs. Expected Readmission Rates from Jan 2012 March 2015 EXPECTED READMIT RATE 13.24% READMIT RATE 13.22% 13.00% 13.10% 13.20% 13.30% 13.40% 13.50%
21 Multi-disciplinary Rounds (MDR) Analysis Strengths Patients are well known by team members Increased trust and comfortability amongst regular members Engaged physician advisors lead to greater efficiency Units with a pharmacist reported a greater number of medication interventions Opportunities No focus on readmission prevention No consistent emphasis on socio-economic challenges, including access to medications Heavy reliance on paper notes vs. real time EMR Team members split between multiple units Nurse managers who were not in attendance failed to follow up with patient issues Delays in rounds leading to inefficiency

22 Discussion Question What additional information might be obtained by interviewing readmitted patients that may not be found by only reviewing the chart?
23 CHF Readmitted Patients Chart Reviews Jan May 2017 N = 70 Age Range Average Age 78 CHF Readmissions by Gender CHF Readmissions by Insurance Type Male Female Medicare Charity Care/Medicaid Private Managed Care CHF Readmissions by APR DRG Severity of Illness & Mortality Risk CHF Readmissions by Discharge Disposition group 1 & 2 group 3 & Home Homecare SNF/LTC Intermediate Care AMA
24 CHF Readmitted Patients Chart Reviews Jan May 2017 N = 70 Age Range Average Age CHF Readmissions by Days to Next Readmission days 8-15 days days days 20 7 CHF Readmissions By MD Specialty Cardiology Internal Medicine Family Medicine Geriatric Medicine Hospitalist Medicine CHF Readmission Reasons Skin Trauma Intestinal Obstruction Renal Disease/Failure Pulm Edema/ARF COPD GI Bleed Valvular Disease/Arrhythmia CHF

25 Readmission Interviews
26 Operational Gaps Lack of process to identify 30-day readmissions Need for a risk assessment tool to identify high risk patients Discharge plan initiated late during the hospitalization Poor education about community resources Follow up appointment not made Appointments not coordinated with caregiver to assure transportation Appointment made with provider who does not take patient s insurance Limited options for uninsured patients Medication management issues, especially during transitions of care
27 Patient Related Gaps Low socioeconomic status Low educational level and health literacy Lack of trust in the health care system VNS services that participate with patient s insurance Delay in Medicaid application process Inability to be discharged to rehab due to lack of coverage Social access issues: food, shelter, subpar housing Locating and following up with patients post-discharge

28 Interventions To Reduce Readmissions Identify high risk patients Patient and caregiver education Coordination of follow up care/post discharge plan Provide community resources and support service information Medication reconciliation on admission and discharge
 ED Utilization (Last 6 months) +")

29 High Risk Assessment Identification Identify high risk patients at admission utilizing LACE L A C E Length of Stay Acuity Co-morbidity (Charleson Score) ED Utilization (Last 6 months) + Additional demographic and clinical information. Additional methods: Nursing assessment TOC team needs assessment Case management/social services referrals Low Risk: 0-28 Moderate Risk: High Risk: 59+
30 LACE+ Variables + equals: Age and sex Hospital teaching status at discharge Acute diagnoses and procedures during the index admission Number of days on alternate care during the index admission Number of elective and urgent admissions to the hospital in the year before the index admission.
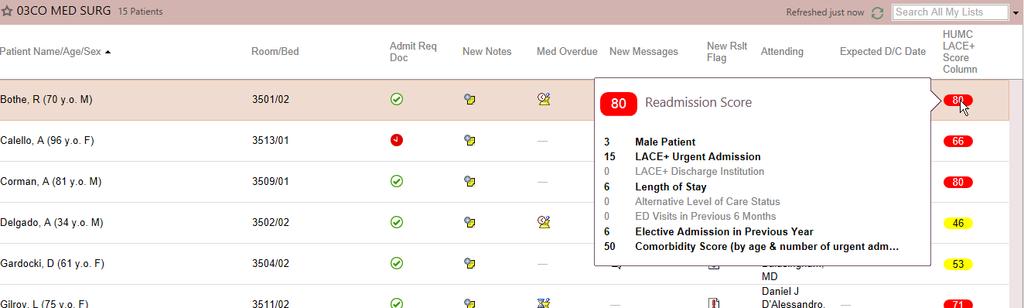
31 Readmission Score
. Each condition is assigned a score of 1, 2, 3, or 6, depending on the risk of dying associated with each one.")
32 Charleson Comorbidity Predicts the one-year mortality for a patient who may have a range of comorbid conditions, such as heart disease, AIDS, or cancer (a total of 22 conditions). Each condition is assigned a score of 1, 2, 3, or 6, depending on the risk of dying associated with each one.

33 30-Day Readmission Banner Collaboration with IT/EPIC on Electronic Solutions
 Diabetic and home care supplies (as")
34 The First Thirty' Wellness Package The First Thirty' Tote Bag Digital Weight Scale Automatic Blood Pressure Machine Pill Box for 7-day am/pm Calendar for 30-day appointments Appointment pad and First Thirty Pen Pulse ox (if needed) Diabetic and home care supplies (as needed)

35 Patient Education NJ Care Act: Caregiver is identify on admission, educated about the plan of care and provide contact info for questions post discharge Education is Consistent, Organized, Utilizes Teach Back, and includes: Self care Disease states Medications Management of chronic conditions Self monitoring tools Emergency instructions


36 Follow-Up Care Develop a post discharge plan with patient and caregiver Follow-up phone call within 72hrs of discharge Appointments scheduled 7 10 days of discharge PMDs/Specialist Diagnostics procedures Reminder 24hrs prior to appointment Transportation Confirm 24hrs prior/verify address and phone number VNS First visit within 24 hours of discharge Access to Care Expedite insurance applications

37 Discharge Process Collaborate with Patient/RN/Case Manager regarding d/c plan Review/complete Discharge Med Rec with Provider Offer Meds to Beds program Schedule follow-up appointments VNS referral and bedside enrollment Communicate plan of care to patient and caregiver & discuss any challenges Arrange transportation if needed Provide patients with Wellness Package Medication education & counseling by Pharmacist APN education on self care, disease state management, and available resources Weekly calls to patient for 4 weeks, as well as appt reminder calls Post-discharge follow up phone call in 24 hours Discharge patient








38 Post-Discharge Challenges Appointment scheduled & confirmed Transportation is set up No Show Process Patient is called 24hrs prior Patient misses appointment VNS is notified to visit patient Provider/clini c notifies team If transportation was arranged, driver alerts the team

39 TOC Team Discharge Checklist Include patient in discussion Identify and address barriers prior to discharge Coordinate plan of care with primary nurse, case manager, social worker, and provider Fax discharge summary to outpatient provider Confirm transportation Ensure access to medications and self-monitoring tools

40 Medication Management National Patient Safety Goal #3 Improve the safety of using medications About 20% of Medicare patients are readmitted More than half potentially preventable Cost = $15-$25 billion/year Mismanagement includes: Adverse events Poor compliance Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165:
41 Pharmacist s Role Conduct medication reconciliation Admission and discharge Patient and caregiver counseling Participation in multi-disciplinary rounds Address prescription coverage needs for the first 30 days post-discharge Enrollment in Meds to Beds Program Ensure vaccine compliance Follow-up phone call within 48 hrs. Medication refill reminder phone call

42 Admission Med Rec Interventions Error Profile 4000 # of Patients to 5 6 to to >20 Errors
43 Med Rec 2016: Types of Errors Incorrect dose Dose omissions Incorrect entries* Incorrect frequencies Duplications Omissions Number of errors * Incorrect entries include wrong strengths, medications patient is no longer taking, has been discontinued, and completed therapies

44 Meds to Beds Plaza Pharmacy program designed to fill prescriptions and deliver to patients prior to discharge Nurse driven, Pharmacy technician managed Benefits Prevent 30-Day readmissions Improve patient understanding and outcomes Improve patient satisfaction scores Drive successful population health management of high risk populations 44
45 Post-Intervention Readmission Data for The First Thirty - It Works! March 2015 through June 2017 # of Mortalities 6 30 Day Readmissions 24 Readmit Rate 6.5% Expected Readmissions 54.2 Expected Readmit Rate 14.69% O/E Readmissions 0.44 n = 369 discharges First Thirty (DSRIP) Readmission Rates vs. Expected Readmission Rates for DSRIP AMI/CHF Patients March 2015 June 2017 EXPECTED READMIT RATE 14.7% READMIT RATE 6.5% 0.0% 2.0% 4.0% 6.0% 8.0% 10.0% 12.0% 14.0% 16.0%

46 Suggested Metrics and Data Readmission rates Patient satisfaction scores Medication reconciliation compliance on admission and discharge Adherence to follow-up appointments Medication compliance and access

47 Sustaining Improvement Leadership engagement Development of TOC Charter Team Optimize available resources Community partnerships Return on investment/business plan Monitor interventions Use of risk stratification tool and readmission banner Multidisciplinary rounds Med rec compliance Collect and share metrics/data with stakeholders Regular monitoring of patient s self care skills/independence for 30 days and beyond Share, share and share some more!

48 Case Study Closing Summary So how did this patient do? How did he and others evaluate the program?

49 Questions? Contacts
QUEST: Collaboration for Performance
 QUEST: Collaboration for Performance The National Pay for Performance Summit San Francisco, CA March 8, 2010 Carolyn Scott, RN, M.Ed., MHA Vice President, Performance Improvement and Quality, Premier,
QUEST: Collaboration for Performance The National Pay for Performance Summit San Francisco, CA March 8, 2010 Carolyn Scott, RN, M.Ed., MHA Vice President, Performance Improvement and Quality, Premier,
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Impact of an Innovative ADC System on Medication Administration
 Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Partnering with Public Health Departments in Managed Care. THIS AREA CAN BE LEFT BLANK or ADD A PICTURE
 Partnering with Public Health Departments in Managed Care THIS AREA CAN BE LEFT BLANK or ADD A PICTURE 2/3/2017 The Value of Medicaid Managed Care States Have Seen the Value of Medicaid Managed Care 75
Partnering with Public Health Departments in Managed Care THIS AREA CAN BE LEFT BLANK or ADD A PICTURE 2/3/2017 The Value of Medicaid Managed Care States Have Seen the Value of Medicaid Managed Care 75
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
A Call to Action: Readmission Strategies from the Field
 A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
Conflict of Interest. Objectives. The Solution. The Need. Reaching for the Stars Advanced Roles for Pharmacy Technicians.
 8/14/2014 Reaching for the Stars Advanced Roles for Pharmacy Conflict of Interest No conflicts of interest to disclose Informatics Bryan Shaw, Pharm.D. PGY-1 Non-Traditional Resident Northwestern Memorial
8/14/2014 Reaching for the Stars Advanced Roles for Pharmacy Conflict of Interest No conflicts of interest to disclose Informatics Bryan Shaw, Pharm.D. PGY-1 Non-Traditional Resident Northwestern Memorial
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
The Cleveland Super-Utilizer Project: Red Carpet Care
 The Cleveland Super-Utilizer Project: Red Carpet Care Alice Stollenwerk Petrulis, MD The MetroHealth System Cleveland, OH Bernadette Yohe, RN Buckeye Community Health Plan Picture of MH MetroHealth 750
The Cleveland Super-Utilizer Project: Red Carpet Care Alice Stollenwerk Petrulis, MD The MetroHealth System Cleveland, OH Bernadette Yohe, RN Buckeye Community Health Plan Picture of MH MetroHealth 750
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
BreakThrough Care Center: A New Care Model for High Risk Patients. Dr. Richard Krouse Dr. Paul Merrick
 BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Quality Circles. Nursing as a Revenue Center NDNQI
 IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
PPMI in a Community Teaching Hospital
 Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Social Determinants of Health: Advocating on behalf of our patients
 Social Determinants of Health: Advocating on behalf of our patients MONICA BHAREL, MD, MPH CHIEF MEDICAL OFFICER BOSTON HEALTH CARE FOR THE HOMELESS PROGRAM Case Study: Boston in the setting of Massachusetts
Social Determinants of Health: Advocating on behalf of our patients MONICA BHAREL, MD, MPH CHIEF MEDICAL OFFICER BOSTON HEALTH CARE FOR THE HOMELESS PROGRAM Case Study: Boston in the setting of Massachusetts
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network
 Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Readmission Partnership Between Acute Care and Post-Acute Care
 Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
AACVPR Update for. Tom Draper, MBA, FAACVPR President, AACVPR
 AACVPR Update for Tom Draper, MBA, FAACVPR President, AACVPR Mission To reduce morbidity, mortality, and disability from cardiovascular and pulmonary disease through education, prevention, rehabilitation,
AACVPR Update for Tom Draper, MBA, FAACVPR President, AACVPR Mission To reduce morbidity, mortality, and disability from cardiovascular and pulmonary disease through education, prevention, rehabilitation,
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute