Risk Management and Safety in Health Care Organizations
|
|
|
- Morgan Heath
- 6 years ago
- Views:
Transcription
1 Risk Management and Safety in Health Care Organizations Fadi El-Jardali, MPH, PhD November 1, 2016 Day 1 1
2 Objectives Increase knowledge about concepts of safety and risk management in health care organizations Understand the concepts of errors and human factors, incident reporting system and steps of risk management to increase the knowledge to effectively implement risk management and safety approaches and tools to prepare participants to develop risk management and safety plan for your organizations. provide participants with hands on experience and practical knowledge on risk management and safety in primary health care 2
3 Learning outcomes 3 Understand the concepts of safety and risk management in health care organizations Understand the concepts of errors and human factors, incident reporting system and steps of risk management Understand the system approach related Risk Management and Safety in health organizations Develop the knowledge regarding different type of risks in the health care organizations Understand and apply the risk management steps including identifying, analyzing, evaluating, treating, monitoring and communicating risk
4 Learning Outcomes (Cont d) Conduct risk assessment using the Severity Assessment Code (SAC) score Apply skills to implement common tools for identifying and addressing the root causes of critical incidences in organizations Failure mode and effects analysis (FMEA) & RCA Apply incident reporting and investigation by using the incident reporting system / guidelines / form used in Kuwait Develop skills to fill incident report Develop corrective action plan based on risk quantification results Apply skills on HOW to effectively develop, implement a risk management and safety plan 4
5 When you usually get to the end of the day, you always find two things 1. You didn t accomplish everything you imagined you would. 2. Your day wasn t anything like how you d imagined.
6 This distinction between Work as Imagined (WAI) and Work As Done (WAD) is everywhere Thanks to Drs. Jeffrey Braithwaite and David Marx

7 What they do seems perfectly logical, obvious and feasible.

8 In health care, those doing WAI have designed, mandated or encouraged a bewildering range of tools, techniques and methods, to reduce harm to patients.

9 E.g., root cause analysis, hand hygiene campaigns, failure modes effects analysis... And there s lots of others

10 But the rate of harm has flatlined at 10%

11 Meanwhile work is getting done, often despite all the policies, rules and mandates
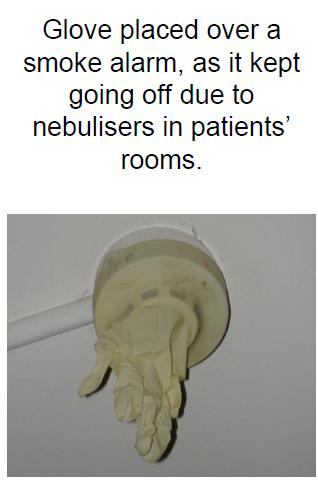
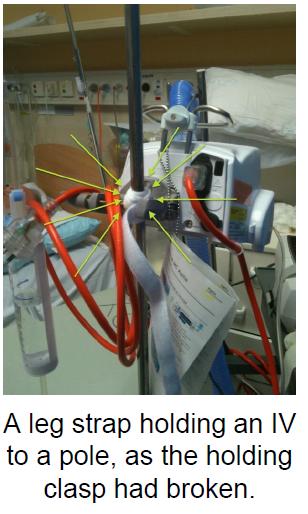

12 WAD workarounds
13 WAD fragmentation Doctors in Emergency Departments in a study: Were interrupted 6.6 times per hour. Were interrupted in 11% of all tasks. Multitasked for 12.8% of the time.
14 Doctors in Emergency Departments in a study: Spent on average 1:26 minutes on any one task. When interrupted, spent more time on tasks. And failed to return to approximately 18.5% of interrupted tasks.

15 So work-as-imagined often have some sort of linear, mechanistic view of the system.
16 Instead, health care is a complex adaptive system delivered by people on the front line who flex and adjust to the circumstances.

17 The amazing thing about health care isn t that it produces adverse events in 10% of all cases, but that it produces safe care in 90% of cases.
18 Few people have ever looked at why things go right so often

19 What none of them know is that there are 600+ policies in operation right now, meant to guide their work.
20 Then when we observe their behaviours and see them taking patients histories, or giving out medications, or doing procedures, or taking x-rays of patients, or tending to their needs, or caring for them



21 We can notice instead a lot of fraught, timepressed, relentlessly busy work going on virtually across the entire shift.

22 Sometimes it never, ever unfolds like a policy or procedure says it should.

23 So, health care doesn t look like this.

24 It looks like this.

25 And therefore the only real solution is to try and reconcile work-asimagined and work-as-done.

26 A health system where the work-asimagined policies, regulations, standards etc are much closer to an understanding of how work is actually done.


27 SUBWAY SAFETY NEW YORK CITY

28 THE PROBLEM, AND THE SOLUTION


29 WHAT ABOUT BETTER SYSTEM DESIGN?
30 YET, IT S NOT ONLY ABOUT SYSTEM DESIGN




31 Architecture examples
32 FOCUSING ON THE RIGHT THINGS Ø Monitor it all Ø But actively manage: System Design Safety Culture

33 SAFETY How do we prevent backing over a child?
34 Solutions TECHNOLOGICAL SYSTEMS Backup camera Backup sensor with automatic breaking Backup horn PROCEDURAL SYSTEMS Walk around back of car before getting in Use a spotter Yet, the most simple of steps, the walk around, most drivers do not do Is that our culture?
35 Quality is about achieving optimal outcomes and also about avoiding risks minimizing harms
36 What Patient Safety Is and Is Not It is not what most of us were thinking about 10 years ago It is not what we have always done It is the most significant change in the healthcare system in over a century It is changing the face of modern healthcare
37 Patient Safety: Challenges and Concerns Difficulty recognizing errors Lack of information systems to identify errors Relationship of trust with providers Shortages of clinical professionals Concern about liability Limited capacity on how to use quality improvement tools Culture of patient safety is lacking
38 What is patient safety? Patient safety is the prevention of harm or injury to patients Patient safety is that which allows you to pursue quality I.e., without basic safety you can t have quality. Patient safety is the identification and control of things that could cause harm to patients (i.e. hazards)
39 Patient Safety Terms Adverse Event Medical Error Sentinel Event Near Miss Retrospective Analysis Prospective Analysis Ø Identifying risks and processes before they happen Ø Bad outcome from care Ø Major & enduring loss of function Ø An examination of past events Ø Deficient process of care ØCould have resulted in loss, injury or illness, but did not
40 Myth: Everyone else has a patient safety problem except us.
41 An Organization s Goal Should Be To prevent or minimize risk of harm to patients, staff, visitors, and volunteers, thereby reducing or eliminating any potential losses including financial ones Risk Management is about harm reduction which could be achieved by risk identification, risk assessment, risk control and evaluation 41
42 Risk Management in Healthcare Institutions Risk management in the healthcare industry is increasingly becoming an important area of concern for health care organization, administrators, medical practitioners, insurers, consumer organizations and other key stakeholders. Medical institutions and medical professionals must take pro active actions to ensure the minimization and elimination of medical errors Risk management in health care emerged as a result of the malpractice crisis of the 1970s. 42
43 Risk Management in Healthcare Institutions Objectives of include: The delivery of safe and quality healthcare to patients Ensuring safety among patients, staff and visitors Identifying and controlling hazards and injuries Protection of assets and other resources 43
44 Risk Management in Healthcare Institutions Stakeholders in Risk Management include: Patients- right to safe and effective medical treatment Government- ensure safety, clinical performance and quality to protect public health Manufacturers of medical equipment and drugs- required to ensure good manufacturing practice and apply established standards for safety and risk Healthcare Facility-Proper selection of equipment / facilities; minimize the occurrence of injury or death to patient, employee or property damage. 44
45 Risk Management is a Proactive Strategy Its components include: Risk identification Risk assessment Risk control Evaluation of risk management activities 45
46 Evaluation of Risk Management Activities Organizations should regularly ask itself: How effective is our risk management system? Organization s risk management practices need to be evaluated. This includes: Reviewing the frequency and severity of losses Analyzing incident and occurrence trends Reviewing policies and procedures that might prevent or minimize risk Assessing new or increased risk Assessing the effectiveness of risk management education and communication strategies 46
47 We cannot change the human condition, but we can change the conditions under which humans work. (Reason 2000) 47
48 Exercise Identify patient safety issues in your organization 48
49 From a Traditional View to a System Approach Person approach to patient safety (practitioner as potential culprit to be blamed) System approach to patient safety 49
50 Some Reasons Why Errors Occur System Factors Complexity of health care processes Complexity of health care work environments Lack of consistent administration practices Deferred maintenance Clumsy technology Human Factors Limited knowledge Poor application of knowledge Fatigue Sub-optimal teamwork Attention distraction Inadequate training Reliance on memory Poor handwriting 50

51 Multi-Causal Theory Swiss Cheese diagram (Reason, 1991) Triggers Lack of Procedures Punitive policies Production Pressures Mixed Messages Zero fault tolerance Sporadic Training Attention Distractions Deferred Maintenance Clumsy Technology DEFENSES Adverse Event 51


52 The Swiss Cheese Model of Accident Causation Organizational Factors w Untested Equipment w Changing Patient Population Procedures wtailored to fit wis Support Communication Patterns w Loss of Situational Awareness w Method of Report Failures in the System Environment wlayout of Unit wnoise Level 52
53 Two Ends of Health Care Systems PATIENT Sharp End Practitioners Tools of the Trade Physical Infrastructure Health Plans, Payers Blunt End Regulations... Financing, policies
54 Quality & Safety Framework Continuous Assessment DEFENCES Report Survey Selfassessment THE GAPS Standard s External Review 54 Safe System Sustaining Improvement Priority Areas for Action Adapted from J. Reason
55 No Quality & Safety Framework DEFENCES Assessment Standards Continuous Improvement Identification THE GAPS Goals? Measurement? 55 Unsafe System Risk Management? Sustaining Improvements? Adapted from J. Reason
56 Life at the Sharp End PATIENT SAFETY TRIGGER (wrong drug prescribed) 1 st Defense (distracted nurse) 2 nd Defense (pharmacy) 3 rd Defense (another distracted nurse) Latent failure (understaffing) Latent failure (no Rx tracking) Latent failure (understaffing) 56 EVENT
57 Life at the Sharp End TRIGGER (wrong drug prescribed) 57 1 st Defense (distracted nurse) 2 nd Defense (pharmacy) 3 rd Defense (vigilant nurse) Adverse Event Averted Latent failure (understaffing) Latent failure (no Rx tracking) Latent failure (understaffing) Sources: Reason J Human error: Models and Management, BMJ, 18 March Cook R. University of Chicago,
58 Life at the Sharp End Standardized approaches can reduce variability and improve system efficiency TRIGGER (wrong drug prescribed) 1 st Defense Template Adverse Event Averted 58
59 What is the difference between focusing on the person and focusing on the system? Person approach Focus on individuals Blaming individuals for forgetfulness, inattention, or carelessness, poor production Methods: poster campaigns, writing another procedure, disciplinary measures, threat of litigation, retraining, blaming and shaming Target: Individuals System approach Focus on the conditions under which individuals work Building defenses to avert errors/poor productivity or mitigate their effects Methods: creating better systems Targets: System (team, tasks, workplace, organization) 59
60 System Approach to Human Error Humans are fallible and errors are to be expected, even in the best organisations. Focus: conditions under which individuals work 60
61 Errors are inevitable.but most are preventable 61
62 Not Who caused the accident but What caused the accident? Medical errors most often result from a complex interplay of multiple factors. Only rarely are they due to the carelessness or misconduct of single individuals. Lucien L. Leape, M.D. 62
63 We cannot change the human condition, but we can change the conditions under which humans work. (Reason 2000) 63
64 Questions Surveyors Might Ask Is there a reporting policy and process for actual and potential adverse events? Are improvements made following incident investigation and follow-up 64
65 Risk Management Focus on the system rather than the individual incident Is anticipatory not reactive in emphasis Incident investigation and reporting supports risk management by monitoring it 65
66 concepts--- Hazard versus Risk Safety culture & the elements of a safe and healthy work environment Classification (categorization) of hazards in a PHC The individual versus the work environment (Who is our concern?) 66
67 I. Hazard vs. Risk- 1 Hazard is any activity, situation or, substance that can cause harm. It is a potential source of risk. Risk is the probability (odds) of a hazard causing harm. 67
68 What is Risk? The chance of something happening that will have an impact on the objectives. It is measured in terms of consequences and likelihood 68
69 What is Risk? Risk is the possibility of exposure to such factors as financial loss, physical damage, injury or delay as a consequence of action or a lack of it. The level of risk exposure is the combination of the likelihood of risk occurring and consequences if it does occur. 69
70 What is Risk? Risks and their consequences might include, but are not limited to: Breach of legal or contractual responsibility Breach of security A threat to physical safety An adverse event during the care process Deficiencies in financial controls and reporting Failure of a project to reach its objectives Failure of equipment or computer system Fraud Patient or family dissatisfaction Unfavorable publicity In any healthcare organization risks can arise from internal and external sources 70
71 Hazard vs. Risk- 2 Risk = Hazard x f (Exposure) 71
72 Describing risk the 3 C s Risk is inherently negative, implying the possibility of adverse consequences. 1. Describe the potential consequences if the risk were to materialise 2. Describe the causal factors that could make the risk materialise 3. Ensure that the context of the risk is clear, e.g. is the risk target well defined (e.g. staff, patient, department, PHC, etc.) and is the nature of the risk clear (e.g. financial, safety, physical loss, perception, etc.) 72
73 Which of the following are adequate descriptions of risk? Risk to patients due to errors and unsafe clinical practice caused by reduced skill base and competence of junior and middle grade medical staff Needlestick injury OSH Reduced staff retention and increased sickness absence due to reduction in morale caused by increased workload, pressure and stress to achieve targets Inadequate patient transfer Budget overrun and financial deficit due to cost of introducing new technologies/medicines as required by NICE guidance Medication error 73
74 Why Risk Management? The culture, process and structures that are directed towards the effective management of potential opportunities and adverse effects 74
75 Accreditation Requirements Organizations must have a documented risk management plan 75

76 76 Healthcare Risk Categories
77 A. Patient Care-related Risks 1. Inappropriate or incorrectly performed medical treatment / diagnosis 2. Confidentiality and appropriate release of information 3. Protection from abuse, neglect and assault 4. Securing appropriate informed patient consent for treatment 5. Nondiscriminatory treatment 77
78 A. Patient Care-related Risks 6. Protection of patient valuables from loss or damage 7. Appropriate assessment and transfer of patients 8. Patient participation in research studies 9. Access to care 78
79 B. Employee-related Risks 1. Occupational illness and injury Infections Exposure to toxic chemicals Electrical hazards Sprains and back injuries Burnout 2. Allegations of discrimination in recruitment, hiring, and promotion based on age, race, sex, national origin, disability; wrongful termination 3. Impaired physicians and other providers who pose a threat to patient or employee safety 79
80 C. Risks related to visitors 1. Infections 2. Injuries caused by slips, falls, and other mishaps 80
81 D. Property-related Risks 1. Buildings and valuable equipment: risk of losses due to fires, floods, etc 2. Paper and/or electronic records (patient, business and financial): risk of damage, destruction 3. Property and liability losses 81
82 Reducing harm by identifying and controlling hazards 82
83 What is a hazard? In safety, a HAZARD is anything that can put somebody or something at risk of damage or injury or harm. In medicine, hazards are called risk factors. 83
84 Why focus on hazards and harm? In medicine, if we want to reduce the incidence rate of a disease we Look for risk factors Figure out how they contribute to the disease Figure out how to reduce or eliminate the risk factor. In safety, if we want to reduce adverse events, we Look for hazards Figure out they contribute to the adverse events Figure out how to reduce or eliminate the hazard. 84
85 How do you identify safety hazards? Proactive techniques, such as Healthcare Failure Mode and Effect Analysis (preventive medicine) Focused upon complex, face-paced areas of the hospital Accomplished prior to implementing new software or new devices Reactive techniques, such as Root Cause Analysis (RCA) (acute care medicine) Based on reports of close calls Based on reports of injuries 85
86 Contributory Factors 1. Individual factors 2. Team and social factors 3. Communication factors 4. Task factors 5. Education and training factors 6. Equipment and resources factors 7. Working conditions 8. Organizational and strategic factors 9. Patient factors 86
87 IV. Types (classes) of hazards Biological (infectious) Chemical Physical Ergonomic Psycho-social Health hazards Safety 87
88 Examples of hazards in a hospital Biological Chemical Physical Ergonomic Psychosocial Safety Hepatitis (B, C); Tuberculosis; HIV; Rubella Anti-neoplastics; Ethylene oxide; Anesthetic gases; Mercury; Asbestos; Formaldehyde Noise; Ionizing radiation; Laser Work stations; Lifting & manual handling Stress; Shift work; Violence Personal (Falls)/ Institutional (fire, explosions) 88
89 89 Risk perception
90 90 Risk perception

91 91 Risk perception



92 92




93 93
94 94


95 95

96 96 Daily Telegraph 20 August 2002
97 Clinicians Delay or missed diagnosis/treatment resulting in increased mortality & morbidity Risk of harming patients associated with invasive procedures Long waiting lists resulting in increased morbidity & complaints Medication error Harm to staff due to violent patients 97
98 Radiology/Pathology Risk associated with missing specimen or X ray films Patient Identification Medication, Xray & Path reports Miss labeling of specimen Risk associated with Equipment Maintenance & Validation Risk associated with Manual handling Risk associated with chemical waste handling Risk associated with understaffing 98
99 IT Concerns Non-human events: these events typically happen on an unpredictable basis without direct human influence local infrastructure failure: Emergency room is disconnected from the network backbone but some emergency help must be provided to patients. major industrial accidents: A large number of injuries must be treated while a power failure caused by that accident hinders provision of health care natural disasters: They may cause injury to the local community as well as to the local infrastructure. A power failure may hinder the operation of the medical equipment, but many injuries flood the emergency room at the same time. 99
100 How to control hazards RISK MANAGEMENT For example, in the case of occupational health and safety (OHS): Hazard mapping Job safety (hazard) analysis 100
101 Example of Effective RISK MANAGEMENT (OHS related) Leadership and support, with a broader role for OHS committee (specialists) Developing knowledge, ability and motivation Solid, local understanding of OHS principles. Proactive, systematic and comprehensive identification of hazards, assessment and control of risks. Solutions to control risks 101
102 Steps in risk management Step 1 Step 2 Step 3 Step 4 Step 5 Identify hazards and hazardous jobs Assign priority for each hazard and hazardous job Assess the risk to find out exactly what makes it hazardous Work through the hazards and hazardous jobs in order of priority Control the risk(s) or fix the problem(s) Evaluate periodically to verify how successfully OHS risks are being managed 102
103 PHC hazards by group at risk HAZARD Staff Patient Guest Biological Chemical Physical Ergonomic Psychosocial Safety 103
104 Who is the staff? Office workers Clerks on floors Physicians Physicians-in-training Medical students Nurses/ Midwives Nursing students Orderlies/nursing assistants Nursing supervisors Pharmacists Nutritionists Social workers Lab technologists Radiology technicians Protection officers Housekeeping Drivers Staff in laundry Staff in kitchen Staff in restaurants Mortician Technicians (electricity, painting, plumbing, mechanic) 104
105 PHC hazards by department HAZARD Laboratory Radiology Etc.. Biological Chemical Physical Ergonomic Psychosocial Safety 105




106 106
107 Hazard mapping tool Name of staff/ officer: Work area Date Area Diagram Key Hazards Control measure
108
109
110 Excercise 1. Think about yourself and your colleagues list 3 issues or concerns you have at work. 2. Now think about patients list 3 issues or concerns you might have in relation to the safety or quality of care provided to patients in your department, PHC, etc. 3. Finally, think about your organisation list 3 issues or concerns.. 110
111 111 Wrap up Day 1
Risk Management and Safety in Health Care Organizations
 Risk Management and Safety in Health Care Organizations Fadi El-Jardali, MPH, PhD October 2016 Day 1 1 Objectives to increase the knowledge to effectively implement risk management and safety approaches
Risk Management and Safety in Health Care Organizations Fadi El-Jardali, MPH, PhD October 2016 Day 1 1 Objectives to increase the knowledge to effectively implement risk management and safety approaches
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant
 Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
The CARE CERTIFICATE. Duty of Care. What you need to know. Standard THE CARE CERTIFICATE WORKBOOK
 The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Development and assessment of a Patient Safety Culture Dr Alice Oborne
 Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Certified Healthcare Safety Long Term Care (CHS-LTC) Examination Blueprint/Outline
 Examination Blueprint/Outline") Certified Healthcare Safety Long Term Care (CHS-LTC) Examination Blueprint/Outline Exam Domains 100-130 1. Safety Management Principles 31-40 (31%) 2. Hazard Control Concepts 46-60 (46%) 3. Compliance
Certified Healthcare Safety Long Term Care (CHS-LTC) Examination Blueprint/Outline Exam Domains 100-130 1. Safety Management Principles 31-40 (31%) 2. Hazard Control Concepts 46-60 (46%) 3. Compliance
POLICY & PROCEDURE FOR INCIDENT REPORTING
 POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
ACCIDENT AND ILLNESS PREVENTION PROGRAM (AIPP)
") ACCIDENT AND ILLNESS PREVENTION PROGRAM (AIPP) Effective October 3, 2016 TABLE OF CONTENTS Section Page Introduction.. 3 I. Accident and Illness Prevention Policy... 4 II. Accident and Illness Prevention
ACCIDENT AND ILLNESS PREVENTION PROGRAM (AIPP) Effective October 3, 2016 TABLE OF CONTENTS Section Page Introduction.. 3 I. Accident and Illness Prevention Policy... 4 II. Accident and Illness Prevention
Goals for this Training
 Accident Investigation Training How to Conduct a Workplace Accident Investigation Emma Corell, Accident Prevention Manager EH&S, Research and Occupational Safety Goals for this Training Learn simple tools
Accident Investigation Training How to Conduct a Workplace Accident Investigation Emma Corell, Accident Prevention Manager EH&S, Research and Occupational Safety Goals for this Training Learn simple tools
Safety Courses SAFETY 581 Motor Fleet Safety 3 u SAFETY 582 Safety In The Construction Industry 3 u SAFETY 583 Introduction To Security 3 u
 Safety Courses SAFETY 581 Motor Fleet Safety 3 u An analysis of fleet safety problems and programs. Detailed study of the truck transportation industry, motor carrier responsibilities, federal regulations
Safety Courses SAFETY 581 Motor Fleet Safety 3 u An analysis of fleet safety problems and programs. Detailed study of the truck transportation industry, motor carrier responsibilities, federal regulations
SCDHSC0042 Lead practice for health and safety in the work setting
 Lead practice for health and safety in the work setting Overview This standard identifies the requirements when leading practice for health and safety in settings where children, young people or adults
Lead practice for health and safety in the work setting Overview This standard identifies the requirements when leading practice for health and safety in settings where children, young people or adults
1.01 To implement procedures to identify hazards at the University of Windsor.
 Revision No: 1 Page: 1of 6 1.0 PURPOSE 1.01 To implement procedures to identify hazards at the University of Windsor. 1.02 A hazard is a condition, practice, behaviour or situation, or a combination of
Revision No: 1 Page: 1of 6 1.0 PURPOSE 1.01 To implement procedures to identify hazards at the University of Windsor. 1.02 A hazard is a condition, practice, behaviour or situation, or a combination of
Faculty of Science Risk Assessment Procedure
 Faculty of Science Risk Assessment Procedure Version 1.0 TRIM file number 11/ Faculty of Science Doc No Short description Relevant to Authority Responsible officer Responsible office Procedure outlining
Faculty of Science Risk Assessment Procedure Version 1.0 TRIM file number 11/ Faculty of Science Doc No Short description Relevant to Authority Responsible officer Responsible office Procedure outlining
Occupational Health & Safety Policy and Procedure
 Purpose: To affirm the commitment of the Daylesford Neighbourhood Centre (DNC) to provide and maintain an environment that is free from risks to the health and safety of staff, students and members of
Purpose: To affirm the commitment of the Daylesford Neighbourhood Centre (DNC) to provide and maintain an environment that is free from risks to the health and safety of staff, students and members of
1 OCCUPATIONAL HEALTH AND SAFETY PROGRAM
 CAPE BRETON UNIVERSITY OCCUPATIONAL HEALTH & SAFETY MANUAL 1 OCCUPATIONAL HEALTH AND SAFETY PROGRAM 1.1 Cape Breton University Health and Safety Policy Cape Breton University ( University ) is committed
CAPE BRETON UNIVERSITY OCCUPATIONAL HEALTH & SAFETY MANUAL 1 OCCUPATIONAL HEALTH AND SAFETY PROGRAM 1.1 Cape Breton University Health and Safety Policy Cape Breton University ( University ) is committed
Management Standards. EHS Policy and Program
 Global Environment, Health and Safety Standards Abbott has an established Environment, Health and Safety (EHS) Policy and set of management and technical standards that form the basis of our EHS management
Global Environment, Health and Safety Standards Abbott has an established Environment, Health and Safety (EHS) Policy and set of management and technical standards that form the basis of our EHS management
UV21096 Health and safety in catering and hospitality
 UV21096 Health and safety in catering and hospitality The aim of this unit is to develop your knowledge and understanding of health and safety legislation and its impact within the catering and hospitality
UV21096 Health and safety in catering and hospitality The aim of this unit is to develop your knowledge and understanding of health and safety legislation and its impact within the catering and hospitality
Extract from Managing Infection Control
 TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
HEALTH AND SOCIAL CARE
 2016 Suite Cambridge TECHNICALS LEVEL 2 HEALTH AND SOCIAL CARE Unit 2 Health and safety in practice A/615/1464 Guided learning hours: 30 Version 1 September 2016 ocr.org.uk/healthandsocialcare LEVEL 2
2016 Suite Cambridge TECHNICALS LEVEL 2 HEALTH AND SOCIAL CARE Unit 2 Health and safety in practice A/615/1464 Guided learning hours: 30 Version 1 September 2016 ocr.org.uk/healthandsocialcare LEVEL 2
Quality Improvement Overview. Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International
 Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Commonwealth Nurses Federation in Conjunction with the Sierra Leone Nurses Association Freetown 4 Safety Workshop - April, 2010
 Michael M. Koroma RGN. Dip(Ghana, 2002) BSc(Hons)Nursing (USL, 2008) Vice President(SLNA) ! INTRODUCTION It is a pressing reality. Health systems worldwide are increasingly challenged faced with a growing
Michael M. Koroma RGN. Dip(Ghana, 2002) BSc(Hons)Nursing (USL, 2008) Vice President(SLNA) ! INTRODUCTION It is a pressing reality. Health systems worldwide are increasingly challenged faced with a growing
A FRAMEWORK FOR MAKING HOSPITALS A SAFER WORKPLACE FREE FROM WORKPLACE VIOLENCE
 A FRAMEWORK FOR MAKING HOSPITALS A SAFER WORKPLACE FREE FROM WORKPLACE VIOLENCE Health care workers have the right to do their jobs in a safe environment free of violence. Hospitals that are safer workplaces
A FRAMEWORK FOR MAKING HOSPITALS A SAFER WORKPLACE FREE FROM WORKPLACE VIOLENCE Health care workers have the right to do their jobs in a safe environment free of violence. Hospitals that are safer workplaces
HealthWISE: An ILO WHO Quality Improvement Tool for Health Facilities. Disclosures. Objectives 9/25/2014. None
 HealthWISE: An ILO WHO Quality Improvement Tool for Health Facilities Claudine Holt, MD, MPH Staff Physician Temple University Hospital Occupational Health Services None Disclosures Objectives At the conclusion
HealthWISE: An ILO WHO Quality Improvement Tool for Health Facilities Claudine Holt, MD, MPH Staff Physician Temple University Hospital Occupational Health Services None Disclosures Objectives At the conclusion
RISK ASSESSMENT ON HEALTH AND SAFETY: ASEAN EXPERIENCE
 RISK ASSESSMENT ON HEALTH AND SAFETY: ASEAN EXPERIENCE Dr. Pennapa Matayompong OIE Sub-Regional Representation for South-East Asia Regional Seminar for OIE National Focal Points for Veterinary Laboratories
RISK ASSESSMENT ON HEALTH AND SAFETY: ASEAN EXPERIENCE Dr. Pennapa Matayompong OIE Sub-Regional Representation for South-East Asia Regional Seminar for OIE National Focal Points for Veterinary Laboratories
POLICY ON WORK HEALTH AND SAFETY
 POLICY ON WORK HEALTH AND SAFETY Re-Endorsed by Annual Conference 2017 NSW Nurses and Midwives' Association 50 O Dea Avenue Waterloo NSW 2017 P 02 8595 1234 (metro) 1300 367 962 (regional) www.nswnma.asn.au
POLICY ON WORK HEALTH AND SAFETY Re-Endorsed by Annual Conference 2017 NSW Nurses and Midwives' Association 50 O Dea Avenue Waterloo NSW 2017 P 02 8595 1234 (metro) 1300 367 962 (regional) www.nswnma.asn.au
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
Administrative Policies and Procedures
 Administrative Policies and Procedures Originating Venue: Environment of Care Policy No.: EC 2007 Title: Environment of Care Management Program Cross Reference: EC 2001 Date Issued: 04/14 Authority Environmental
Administrative Policies and Procedures Originating Venue: Environment of Care Policy No.: EC 2007 Title: Environment of Care Management Program Cross Reference: EC 2001 Date Issued: 04/14 Authority Environmental
Self Assessment Guide for an Effective Safety and Health Program
 Self Assessment Guide for an Effective Safety and Health Program The revised Rural Electric Safety Achievement Program provides the frame work for cooperatives to develop safety and health programs that
Self Assessment Guide for an Effective Safety and Health Program The revised Rural Electric Safety Achievement Program provides the frame work for cooperatives to develop safety and health programs that
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Purpose and Goals of Risk Management in the Sleep Center. Melinda Trimble, RPSGT, RST, LRCP
 The Purpose and Goals of Risk Management in the Sleep Center Melinda Trimble, RPSGT, RST, LRCP Objectives Overview of Risk Management as a concept What is the purpose of Risk Management and what are its
The Purpose and Goals of Risk Management in the Sleep Center Melinda Trimble, RPSGT, RST, LRCP Objectives Overview of Risk Management as a concept What is the purpose of Risk Management and what are its
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Towards Quality Care for Patients. Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care
 Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Licentiate of the Faculty of Occupational Medicine (LFOM)
") Employee Handbook of the Royal College of Physicians of Ireland Licentiate of the Faculty of Occupational Medicine (LFOM) Examination Syllabus, 2016 Table of contents Heading 1... Error! Bookmark not defined.
Employee Handbook of the Royal College of Physicians of Ireland Licentiate of the Faculty of Occupational Medicine (LFOM) Examination Syllabus, 2016 Table of contents Heading 1... Error! Bookmark not defined.
Certified Hazard Control Manager (CHCM) Certified Hazard Control Manager Security (CHCM-SEC) Examination Blueprint/Outline
 Certified Hazard Control Manager Security (CHCM-SEC) Examination Blueprint/Outline") Certified Hazard Control Manager (CHCM) Certified Hazard Control Manager Security (CHCM-SEC) Examination Blueprint/Outline (Effective October 1, 2017) Exam Domains 145 Items 1. Safety Management 43 Items/30%
Certified Hazard Control Manager (CHCM) Certified Hazard Control Manager Security (CHCM-SEC) Examination Blueprint/Outline (Effective October 1, 2017) Exam Domains 145 Items 1. Safety Management 43 Items/30%
Managing Safely v5.0 course syllabus
 Guided learning hours A total of 22 hours made up of: - 21 hours of learning - one hour for assessment (including introduction/ instruction time of 15 minutes). You have the flexibility to deliver this
Guided learning hours A total of 22 hours made up of: - 21 hours of learning - one hour for assessment (including introduction/ instruction time of 15 minutes). You have the flexibility to deliver this
Certified Healthcare Safety Environmental Services (CHS-EVS) Examination Blueprint/Outline
 Examination Blueprint/Outline") Certified Healthcare Safety Environmental Services (CHS-EVS) Examination Blueprint/Outline Exam Domains 100-130 1. Safety Management 38-50 (38%) 2. Hazard Control 38-50 (38%) 3. Compliance & Voluntary
Certified Healthcare Safety Environmental Services (CHS-EVS) Examination Blueprint/Outline Exam Domains 100-130 1. Safety Management 38-50 (38%) 2. Hazard Control 38-50 (38%) 3. Compliance & Voluntary
Unit 2 Clinical Governance & Risk Management Awareness
 Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Psychosocial risks and violence at work: prevalence and prevention approaches in Europe
 Psychosocial risks and violence at work: prevalence and prevention approaches in Europe A+A ILO International Occupational Safety and Health Conference 2017 18-19 October 2017, Dusseldorf Malgorzata Milczarek,
Psychosocial risks and violence at work: prevalence and prevention approaches in Europe A+A ILO International Occupational Safety and Health Conference 2017 18-19 October 2017, Dusseldorf Malgorzata Milczarek,
Resilience in Health Care
 Resilience in Health Care Erik Hollnagel, Ph.D. Professor, University of Southern Denmark Chief Consultant, Center for Kvalitet, Region of Southern Denmark E-mail: erik.hollnagel@rsyd.dk There is something
Resilience in Health Care Erik Hollnagel, Ph.D. Professor, University of Southern Denmark Chief Consultant, Center for Kvalitet, Region of Southern Denmark E-mail: erik.hollnagel@rsyd.dk There is something
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Health & Safety Policy
 Health & Safety Policy DATE ISSUED: 1 April 2014 DATE TO BE REVIEWED: 1 April 2014 Health & Safety Policy Page 1 of 11 CONTENTS POLICY OVERVIEW 1 Introduction 2 Purpose 3 Who This Policy Applies To 4 Key
Health & Safety Policy DATE ISSUED: 1 April 2014 DATE TO BE REVIEWED: 1 April 2014 Health & Safety Policy Page 1 of 11 CONTENTS POLICY OVERVIEW 1 Introduction 2 Purpose 3 Who This Policy Applies To 4 Key
PHOENIX FIRE DEPARTMENT. VOLUME 1 Operations SAFETY MANAGEMENT SYSTEM
 PHOENIX FIRE DEPARTMENT VOLUME 1 Operations SAFETY MANAGEMENT SYSTEM MP110.15 04/06 - R PURPOSE The purpose of this procedure is to establish guidelines for the organization and operation of a Safety Management
PHOENIX FIRE DEPARTMENT VOLUME 1 Operations SAFETY MANAGEMENT SYSTEM MP110.15 04/06 - R PURPOSE The purpose of this procedure is to establish guidelines for the organization and operation of a Safety Management
University of Arkansas for Medical Sciences. Part III - Hazardous Materials and Waste Management Plan FY18
 University of Arkansas for Medical Sciences Part III - Hazardous Materials and Waste Management Plan FY18 I. MISSION STATEMENT The purpose of the Hazardous Materials and Waste Management Plan is to identify
University of Arkansas for Medical Sciences Part III - Hazardous Materials and Waste Management Plan FY18 I. MISSION STATEMENT The purpose of the Hazardous Materials and Waste Management Plan is to identify
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
University of Arkansas for Medical Sciences. Part I - Safety Management Plan FY18
 University of Arkansas for Medical Sciences Part I - Safety Management Plan FY18 I. MISSION STATEMENT The mission of UAMS is to improve the health, healthcare and well-being of all Arkansans and of others
University of Arkansas for Medical Sciences Part I - Safety Management Plan FY18 I. MISSION STATEMENT The mission of UAMS is to improve the health, healthcare and well-being of all Arkansans and of others
C H A P T E R HAZARD ANALYSIS
 C H A P T E R 8 HAZARD ANALYSIS 8.1. Safety Inspections All areas and operations of each workplace, including office areas, must be inspected at least once a year. More frequent inspections shall be conducted
C H A P T E R 8 HAZARD ANALYSIS 8.1. Safety Inspections All areas and operations of each workplace, including office areas, must be inspected at least once a year. More frequent inspections shall be conducted
GENERAL HOSPITAL ORIENTATION Revised: January 2013 EE Intl Hosp Ort
 GENERAL HOSPITAL ORIENTATION 2013-2014 1 GOOD SAMARITAN HOSPITAL MANDATORY EDUCATION CLASSES ATTENDANCE OR SELF-LEARNING MODULE ACKNOWLEDGEMENT Organizational Mission, Vision, and Goals Cultural Diversity
GENERAL HOSPITAL ORIENTATION 2013-2014 1 GOOD SAMARITAN HOSPITAL MANDATORY EDUCATION CLASSES ATTENDANCE OR SELF-LEARNING MODULE ACKNOWLEDGEMENT Organizational Mission, Vision, and Goals Cultural Diversity
Certified Healthcare Safety Nursing (CHSN) Examination Blueprint/Outline
 Examination Blueprint/Outline") Certified Healthcare Safety Nursing (CHSN) Examination Blueprint/Outline (Effective October 1, 2017) Exam Domains 135 Items 1. Patient Safety Fundamentals 54 Items/40% 2. Healthcare Safety Management 54
Certified Healthcare Safety Nursing (CHSN) Examination Blueprint/Outline (Effective October 1, 2017) Exam Domains 135 Items 1. Patient Safety Fundamentals 54 Items/40% 2. Healthcare Safety Management 54
Occupational Health and Safety Policy
 Occupational Health and Safety Policy Ratified by the School Board: 15/09/2011 Version: 2.0 (Sept. 2011) Table of Contents 1. Policy... 3 1.1 Background... 3 1.2 Definitions... 3 1.2.1 Employees of Sophia
Occupational Health and Safety Policy Ratified by the School Board: 15/09/2011 Version: 2.0 (Sept. 2011) Table of Contents 1. Policy... 3 1.1 Background... 3 1.2 Definitions... 3 1.2.1 Employees of Sophia
JCI 6 th ed. Hospital Standards Review: Patient-Centered Standards
 JCI 6 th ed. Hospital Standards Review: Patient-Centered Standards Standards Overview This presentation provides a general sense of what types of issues and themes are covered in our Patient- Centered
JCI 6 th ed. Hospital Standards Review: Patient-Centered Standards Standards Overview This presentation provides a general sense of what types of issues and themes are covered in our Patient- Centered
SAMPLE. HLTWHS300A Contribute to WHS processes Children s Services. Learner Guide. CHC08 Community Services Training Package Version 4.
 CHC08 Community Services Training Package Version 4 HLTWHS300A Contribute to WHS processes Children s Services Learner Guide Version 2 INDUSTRY SKILLS UNIT MEADOWBANK Product Code: 5696 Acknowledgments
CHC08 Community Services Training Package Version 4 HLTWHS300A Contribute to WHS processes Children s Services Learner Guide Version 2 INDUSTRY SKILLS UNIT MEADOWBANK Product Code: 5696 Acknowledgments
WorkSafeBC Overview for CDAs A credit
 WorkSafeBC Overview for CDAs A0003 1 credit Hand out and Test developed by: Dave Scott, Occupational Safety Officer Aaron Kong, Occupational Hygiene Officer WorkSafeBC Lecture recorded February 2010 Certified
WorkSafeBC Overview for CDAs A0003 1 credit Hand out and Test developed by: Dave Scott, Occupational Safety Officer Aaron Kong, Occupational Hygiene Officer WorkSafeBC Lecture recorded February 2010 Certified
Health and Safety Policy and Procedures
 DRD Builders Health and Safety Policy and Procedures VALID TO: 7 June 2016 Prepared on Wednesday, 5 August 2015-11:09am Page 1 of 33 Table of Contents 1. Policy Statement 3 2. Health and Safety Procedures
DRD Builders Health and Safety Policy and Procedures VALID TO: 7 June 2016 Prepared on Wednesday, 5 August 2015-11:09am Page 1 of 33 Table of Contents 1. Policy Statement 3 2. Health and Safety Procedures
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Section 5 General Policies Work, Health and Safety Policy. The Gums Childcare Centre Policies
 The Gums Childcare Centre Policies Section 5 General Policies 3.14 Work, Health and Safety Policy Background 1. The Gums Childcare Centre is committed to ensuring a safe and healthy working and learning
The Gums Childcare Centre Policies Section 5 General Policies 3.14 Work, Health and Safety Policy Background 1. The Gums Childcare Centre is committed to ensuring a safe and healthy working and learning
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
Incident Reporting and Investigation Guideline
 Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Policy for the Reporting and Management of Incidents Including Serious Incidents. Version Number: 006
 CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Wellness Director. FLSA Status: Salaried, Exempt Updated: SUMMARY OF POSITION FUNCTIONS
 Wellness Director Department: Wellness Community: Highgrove at Tates Creek Reports To: Executive Director Position Status: FT FLSA Status: Salaried, Exempt Updated: 08.2016 SUMMARY OF POSITION FUNCTIONS
Wellness Director Department: Wellness Community: Highgrove at Tates Creek Reports To: Executive Director Position Status: FT FLSA Status: Salaried, Exempt Updated: 08.2016 SUMMARY OF POSITION FUNCTIONS
Why is RP training and education so important?
 F6.1 Worker Education and Training (IAEA/ILO/NEA) 11:00-12:30, Tuesday, May 15, 2012 Room: Forth Why is RP training and education so important? Dr. Shengli Niu International Labour Organization Geneva,
F6.1 Worker Education and Training (IAEA/ILO/NEA) 11:00-12:30, Tuesday, May 15, 2012 Room: Forth Why is RP training and education so important? Dr. Shengli Niu International Labour Organization Geneva,
Note: 44 NSMHS criteria unmatched
 Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
WESTMINSTER SCHOOL DISTRICT
 WESTMINSTER SCHOOL DISTRICT TITLE: ASSISTANT DIRECTOR OF NUTRITION SERVICES BASIC FUNCTION: In association with the Director of Nutrition Services, assists in planning, coordinating, and directing a district-wide
WESTMINSTER SCHOOL DISTRICT TITLE: ASSISTANT DIRECTOR OF NUTRITION SERVICES BASIC FUNCTION: In association with the Director of Nutrition Services, assists in planning, coordinating, and directing a district-wide
Occupational Health Policy
 Policy No: PP45 Version: 2.0 Name of Policy: Occupational Health Policy Effective From: 14/03/2016 Date Ratified 09/02/2016 Ratified Human Resources Committee Review Date 01/02/2018 Sponsor Director of
Policy No: PP45 Version: 2.0 Name of Policy: Occupational Health Policy Effective From: 14/03/2016 Date Ratified 09/02/2016 Ratified Human Resources Committee Review Date 01/02/2018 Sponsor Director of
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
21 Questions. Key risks (other) 9. related to finances? related to leadership?
 9. related to finances? related to leadership?") 21 Questions Guidance for healthcare boards on what they should ask senior leaders about risk. Drawing on strong ethical and evidence-based principles, HIROC, in collaboration with subscribers, has developed
21 Questions Guidance for healthcare boards on what they should ask senior leaders about risk. Drawing on strong ethical and evidence-based principles, HIROC, in collaboration with subscribers, has developed
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
Problem Solving Tools
 Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
Sample Reportable Events
 Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Health Science Career Cluster (HL) Therapeutic Services - Patient Care Career Pathway (HL-THR) 13 CCRS CTE
 Therapeutic Services - Patient Care Career Pathway (HL-THR) 13 CCRS CTE") Health Science Career Cluster (HL) 1. Determine academic subject matter, in addition to high school graduation requirements, necessary for pursuing a health science career. 2. Explain the healthcare worker
Health Science Career Cluster (HL) 1. Determine academic subject matter, in addition to high school graduation requirements, necessary for pursuing a health science career. 2. Explain the healthcare worker
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
Contact Hours FL (CE version ONLY) Suggested Target Audience. staff that provide care to patients. Page 1 of 8 Updated: 10/30/2017
 Suggested Target Audience. staff that provide care to patients. Page 1 of 8 Updated: 10/30/2017") PA CE 1 Active Shooter Response in Healthcare Settings - An HCCS Regulatory 1/8/2016 1 1 N/A 20 N/A N/A all staff 2 Advance Directives - An HCCS Regulatory 10/15/2015 1 1 N/A 54 N/A N/A all staff 3 Annual
PA CE 1 Active Shooter Response in Healthcare Settings - An HCCS Regulatory 1/8/2016 1 1 N/A 20 N/A N/A all staff 2 Advance Directives - An HCCS Regulatory 10/15/2015 1 1 N/A 54 N/A N/A all staff 3 Annual
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
HEALTH AND SAFETY POLICY STATEMENT AND ARRANGMENTS MANUAL
 HEALTH AND SAFETY POLICY STATEMENT AND ARRANGMENTS MANUAL Revision Description of change Date Approved 2 Sections 2.18 to 2.22 added and various minor alterations 22/01/10 Copyright 2009 Phoenix Steel
HEALTH AND SAFETY POLICY STATEMENT AND ARRANGMENTS MANUAL Revision Description of change Date Approved 2 Sections 2.18 to 2.22 added and various minor alterations 22/01/10 Copyright 2009 Phoenix Steel
POSITION DESCRIPTION
 POSITION DESCRIPTION POSITION: Specialist Orthopaedic Surgeon RESPONSIBLE TO: Service Manager, Surgical Services Our Vision: Nelson Marlborough Health s (NMH s) vision is to work with the people of our
POSITION DESCRIPTION POSITION: Specialist Orthopaedic Surgeon RESPONSIBLE TO: Service Manager, Surgical Services Our Vision: Nelson Marlborough Health s (NMH s) vision is to work with the people of our
Workplace Violence: Nurse Safety Issue Analysis. Rachel Fox & Abby Densmore
 Workplace Violence: Nurse Safety Issue Analysis Rachel Fox & Abby Densmore Nurse Safety: Workplace Violence, Health & Safety Introduction Objectives Define workplace violence and identify three examples
Workplace Violence: Nurse Safety Issue Analysis Rachel Fox & Abby Densmore Nurse Safety: Workplace Violence, Health & Safety Introduction Objectives Define workplace violence and identify three examples
Storage, Labeling, Controlled Medications Instructor s Guide CFR (b)(2)(3)(d)(e) F431
(2)(3)(d)(e) F431") Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN
 NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN Wisconsin Organization of Nurse Executives 2017 Annual Convention April 28, 2017 Barbara Pinekenstein DNP, RN-BC, CPHIMS Linsey Steege PhD Presentation
NURSE LEADER FATIGUE: IMPLICATIONS FOR WISCONSIN Wisconsin Organization of Nurse Executives 2017 Annual Convention April 28, 2017 Barbara Pinekenstein DNP, RN-BC, CPHIMS Linsey Steege PhD Presentation
A Study to Assess Patient Safety Culture amongst a Category of Hospital Staff of a Teaching Hospital
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
POLYTECHNIC OF NAMIBIA SCHOOL OF BUSINESS AND MANAGEMENT EMPLOYEE HEALTH AND SAFETY. 21 BHUR and 07BHRM MS. BARBARA GOWASEB
 POLYTECHNIC OF NAMIBIA SCHOOL OF BUSINESS AND MANAGEMENT DEPARTMENT OF HUMAN RESOURCES MANAGEMENT EMPLOYEE HEALTH AND SAFETY 21 BHUR and 07BHRM SUBJECT CODE: EHS712S DURATION: DATE: MARKS: EXAMINERS: MODERATOR:
POLYTECHNIC OF NAMIBIA SCHOOL OF BUSINESS AND MANAGEMENT DEPARTMENT OF HUMAN RESOURCES MANAGEMENT EMPLOYEE HEALTH AND SAFETY 21 BHUR and 07BHRM SUBJECT CODE: EHS712S DURATION: DATE: MARKS: EXAMINERS: MODERATOR:
(NAME OF HOME) 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.
 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.") Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
Healthcare Risk Control
 Topics Covered 2016 Administrative Support Services Healthcare Advertising and Marketing Media Relations Social Media in Healthcare Critical Care Clinical Alarms Invasive Lines Pulse Oximetry Risk Management
Topics Covered 2016 Administrative Support Services Healthcare Advertising and Marketing Media Relations Social Media in Healthcare Critical Care Clinical Alarms Invasive Lines Pulse Oximetry Risk Management
Safety and Health Movement: An Overview p. 1 Developments Before the Industrial Revolution p. 2 Milestones in the Safety Movement p.
 Safety and Health Movement: An Overview p. 1 Developments Before the Industrial Revolution p. 2 Milestones in the Safety Movement p. 3 Tragedies That Have Changed the Safety Movement p. 5 Role of Organized
Safety and Health Movement: An Overview p. 1 Developments Before the Industrial Revolution p. 2 Milestones in the Safety Movement p. 3 Tragedies That Have Changed the Safety Movement p. 5 Role of Organized
Health and Safety Policy
 Health and Safety Policy 2015 Statement of Health and Safety Policy The University recognises its obligations to properly control the risks to the health of its staff, students and visitors. Strong strategic
Health and Safety Policy 2015 Statement of Health and Safety Policy The University recognises its obligations to properly control the risks to the health of its staff, students and visitors. Strong strategic
Summers-Inman Group Health and Safety Policy SUMMERS-INMAN GROUP HEALTH AND SAFETY POLICY. Revision -
 SUMMERS-INMAN GROUP HEALTH AND SAFETY POLICY 4 th November 2015 1 Table of Contents 1. Revision History... 5 2. Health and Safety Policy Statement... 7 3. Organisation... 9 Managing Director... 9 Group
SUMMERS-INMAN GROUP HEALTH AND SAFETY POLICY 4 th November 2015 1 Table of Contents 1. Revision History... 5 2. Health and Safety Policy Statement... 7 3. Organisation... 9 Managing Director... 9 Group
12.01 Safety Management Plan UWHC Administrative Policies
 Page 1 of 7 12.01 Safety Management Plan Category: UWHC Administrative Policy Policy Number: 12.01 Effective Date: October 8, 2013 Version: Revision Section: Environmental Safety (Hospital Administrative)
Page 1 of 7 12.01 Safety Management Plan Category: UWHC Administrative Policy Policy Number: 12.01 Effective Date: October 8, 2013 Version: Revision Section: Environmental Safety (Hospital Administrative)
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
What we have learned:
 What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.