Resilience in Health Care
|
|
|
- Loraine Russell
- 5 years ago
- Views:
Transcription



1 Resilience in Health Care Erik Hollnagel, Ph.D. Professor, University of Southern Denmark Chief Consultant, Center for Kvalitet, Region of Southern Denmark
 The rate of adverse events in acute care ranges from 3% to 17% (international studies). CA Medical Insurance Feasibility study (Mills, 1978) 4.")
. 30 121 cases from acute care hospitals in NY State in 1984. Adverse events rate: 3.7%. The influence of negligence varied from 22.2 51.")
2 There is something rotten... 10% of patients admitted to hospital suffer iatrogenic harm. More than half of this could have been prevented if staff had followed established good practice. (Vincent et al. BMJ, 2001) The rate of adverse events in acute care ranges from 3% to 17% (international studies). CA Medical Insurance Feasibility study (Mills, 1978) 4.65% iatrogenic harm ( cases from 23 hospitals Adverse effects of treatment or procedures: 82% Effects of incomplete diagnosis or treatment: 15% Effects of incomplete prevention or protection: 3% Harvard Medical Practice Study (Brennan et al., 1991) cases from acute care hospitals in NY State in Adverse events rate: 3.7%. The influence of negligence varied from % and was significantly higher for the more serious outcomes.

3 A need to explain and understand... A need to be safe A need to feel safe Act of god Technical failure Human factor Organisational culture Complex systems The types of causes have changed over time, but we still believe in causality




4 and to feel safe, secure, and stable (t)o trace something unknown back to something known is alleviating, soothing, gratifying and gives moreover a feeling of power. Danger, disquiet, anxiety attend the unknown the first instinct is to eliminate these distressing states. First principle: any explanation is better than none The cause creating drive is thus conditioned and excited by the feeling of fear. Twilight of the Idols Friedrich Wilhelm Nietzsche ( ) Maslow s hierarchy of needs. Erik Hollnagel, 2014
5 Simple, linear model (cause-effect chain) Simple linear models (cause-effect chains) If accidents are the culmination of a chain of events... then risks can be found as the probability of component failures Mechanical hazard Find the component that failed by reasoning backwards from the final consequence. Heinrich (1931) Human error Find the probability that something breaks, either alone or by simple, logical and fixed combinations.
 failure.")
6 Composite linear models If accidents happen as a combination of active failures and latent conditions... Composite linear models then risks are the likelihood of weakened defences in combination with active failures Look for how degraded barriers or defences combined with an active (human) failure. Combinations of single failures and latent conditions, leading to degradation of barriers and defences.
7 The causality credo (1) Adverse outcomes happen because something has gone wrong. (2)Adverse outcomes therefore have causes, which can be found and treated. (3) All accidents are preventable (zero harm principle). Accident investigation Find the component that failed by reasoning backwards from the final consequence. Accidents result from a combination of active failures (unsafe acts) and latent conditions (hazards). Risk analysis Find the probability that components break, either alone or in simple combinations. Look for combinations of failures and latent conditions that may constitute a risk.
8 Different process different outcome Function (work as imagined) Success (no adverse events) Acceptable outcomes Things that go right and things that go wrong happen in different ways. Malfunction, non-compliance, error Failure (accidents, incidents) Unacceptable outcomes
 Acceptable outcomes Identification and measurement of adverse medical events is")
 Unacceptable outcomes")
9 Increasing safety by reducing failures Function (work as imagined) Success (no adverse events) Acceptable outcomes Identification and measurement of adverse medical events is central to patient safety. Malfunction, non-compliance, error Failure (accidents, incidents) Unacceptable outcomes Zero Accident Mindset No repeats Simple and non-negotiable standards
.")

10 Safety-I when nothing goes wrong Safety is the condition where the number of adverse outcomes (accidents / incidents / near misses) is as low as possible. Safety-I Safety-I is is defined defined by by its its opposite opposite by by the the lack lack of of safety safety (accidents, (accidents, incidents, incidents, risks). risks). If we want something to increase, why do we use a proxy measure that decreases? The The premise premise for for Safety-I Safety-I is is the the need need to to understand understand why why accidents accidents happen. happen. Accidents and incidents are situations that, by definition, lack safety. How can we improve safety by studying situations where there is NO safety?
11 Why only look at what goes wrong? 10-4 := 1 failure in events Adverse outcomes = Absence of safety Focus is on what goes wrong. Look for failures and malfunctions. Try to eliminate causes and improve barriers. Focus is on what goes right. Use that to understand everyday performance, to do better and to be safer. Intended outcomes = Presence of safety := successes in events Safety and core business compete for resources. Learning only uses a fraction of the data available Safety and core business help each other. Learning uses most of the data available




12 The need to imagine how others work Plan and design work: roles, workplace Manage work: lean - quality - guidelines Manage safety: investigations & auditing Work-As-Imagined Work-As-Imagined Work-As-Imagined Work-As-Done
13 Designing for work-as-imagined Work-asimagined What support does the people need? What have they been thinking of? How should it be provided? What is this supposed to do? How will it fit existing ways of working? Why does it not fit the way we work? Designer(s) How should it be used correctly? How can we get it to work?

 do Work-As-Done What I")

14 We all have to think about work Work-As-Done What we do! Work-As-Imagined What someone should do Work-As-Imagined What someone did t Work-As-Imagined What someone did Work-As-Imagined What they (should) do Work-As-Done What I do! Work-As-Imagined What they (should) do Plans are the structure of behaviour Work-As-Done What I do! Erik Hollnagel, 2014


.")
15 Work as imagined work as done Work-as-imagined (formal work) is what designers, managers, regulators, and authorities believe happens or should happen. Work-as-done (informal work) is what people have to do to get the job done. It is what actually happens. Failure is explained as a breakdown or malfunctioning of a system and/or its components (non-compliance, violations, error). Individuals and organisations must adjust what they do to the current conditions. Performance variability is necessary for things to work.
 may be limited and uncertain. People adjust what they do to match the situation.")

16 Everyday clinical work must be flexible Resources (time, manpower, materials, information, etc.) may be limited and uncertain. People adjust what they do to match the situation. Performance variability is inevitable, ubiquitous, and necessary. Because of resource limitations, performance adjustments will always be approximate. Performance variability is the reason why everyday work is safe and effective. Performance variability is the reason why things sometimes go wrong.


17 Work as imagined follow the rules! Emergency surgery on a fractured neck of femur involves app. 75 clinical guidelines and policies. UK Government guideline on Working Together to Safeguard Children is 390 pages long! Carthey et al (2011). Breaking the rules: understanding non-compliance with policies and guidelines. BMJ


18 Medication s 30-minute rule The 30-minute rule is a requirement in the Centers for Medicare & Medicaid Services (CMS) Conditions of Participation Interpretive Guidelines to administer scheduled medications within 30 minutes before or after the scheduled time. Responses from 17,500 front-line nurses (USA) showed that most nurses felt that the 30-minute rule was unsafe, unrealistic, impractical, and virtually impossible to follow. For 70% of the nurses, their organization enforces the 30-minute rule. Of these nurses, only 5% were always able to comply with the policy, while 59% were infrequently or only sometimes compliant. For paper Medication Administration Record systems, nurses often initial the medication entry or document the drug as being administered at the scheduled time, not the actual time. For emar systems, many nurses documented drug administration at the scheduled time, not the actual time.
19 Work as imagined follow the rules! Survey Protocol - Introduction (Rev. 37, Issued: ; Effective/Implementation Date: ) Hospitals are required to be in compliance with the Federal requirements set forth in The Medicare Conditions of Participation (CoP) in order to receive Medicare/Medicaid payment. The goal of a hospital survey is to determine if the hospital is in compliance with the CoP set forth at 42 CFR Part 482. Also, where appropriate, the hospital must be in compliance with the PPS exclusionary criteria at 42 CFR Subpart B and the swing-bed requirements at 42 CFR Certification of hospital compliance with the CoP is accomplished through observations, interviews, and document/record reviews. The survey process focuses on a hospital s performance of patient - focused and organizational functions and processes. The hospital survey is the means used to assess compliance with Federal health, safety, and quality standards that will assure that the beneficiary receives safe, quality care and services. Internet Only Manual (IOM) Contains 1164 Regulations and Interpretive Guidelines on 457 pages.

20 What happens when work is interrupted? In an Australian study 210 hours of observation (131 sessions) found the following: Doctors were interrupted 6.6 times/h. 11% of all tasks were interrupted, 3.3% more than once. Doctors multitasked for 12.8% of time. The mean TOT was 1:26 min. Interruptions were associated with a significant increase in TOT. When accounting for length-biased sampling, interrupted tasks were unexpectedly completed in a shorter time than uninterrupted tasks. Doctors failed to return to 18.5% of interrupted tasks. Average task time (min) for Emergency physicians Direct care 2.88 (2.34 to 3.42) Indirect care 1.44 (1.29 to 1.60) Professional communication 0.99 (0.90 to 1.09) Documentation 2.28 (1.74 to 2.81) Westbrook, J. I. et al. (2010). The impact of interruptions on clinical task completion. Qual Saf Health Care, 19(4).
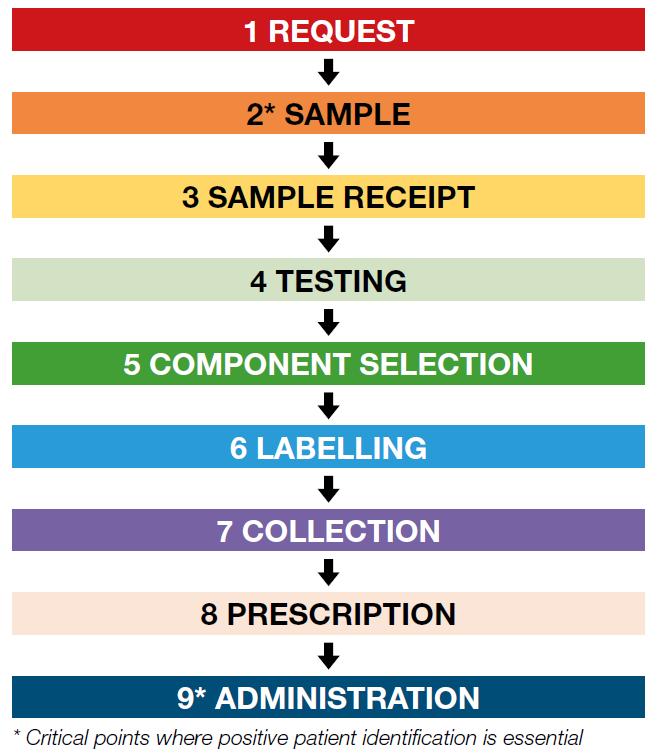
21 Blood transfusion



22 How are adjustments made? AVOID anything that may have negative consequences for yourself, your group, or organisation COMPENSATE FOR MAINTAIN/CREATE conditions that are necessary to carry out the work. conditions that makes work difficult or impossible.



23 Hand over of patients HANDOVER CHECKLIST EDIS boxes completed Highly individualized and sometimes unpredictable. Not simple, non-linear. Time constrained. Complex dynamic ETTOs (workarounds, shortcuts). Local rationality conflicting priorities and tasks. Mentally stressful. Reliance on memory / few cues. All available results acknowledged Interim order plan completed or Discharge letter completed (if applicable) No Yes HANDOVER


24 The second, secret hand-over The English NHS mandates formal handover of emergency patients from ambulance paramedics to receiving clinicians. Staff use a structured communication tool providing information to the nurse in charge who passes it to the bedside nurse. Observations showed that paramedics and bedside nurses conducted a secret second handover. Senior nurses thought this represented duplication, but clinical front line staff felt it told a more complete story and reduced the risk that important information was missed. Clinicians were adjusting to circumstances, providing tractability and increasing the capacity for resilience in the everyday activity of handing over patients.
25 Same process different outcomes Function (work as imagined) Success (no adverse events) Acceptable outcomes Everyday work (performance variability) Things that go right and things that go wrong happen in the same way. Malfunction, non-compliance, error Failure (accidents, incidents) Unacceptable outcomes

 Malfunction, non-compliance, error Failure (accidents, incidents) Unacceptable outcomes")
26 Increase safety by doing things right Safety must be begin by understanding the variability of everyday performance. Function (work as imagined) Success (no adverse events) Acceptable outcomes Everyday work (performance variability) Malfunction, non-compliance, error Failure (accidents, incidents) Unacceptable outcomes Constraining performance variability to remove failures will also remove successful everyday work.
27 What should we be looking for? When we notice something that has gone wrong it is a safe bet that it has gone right many times before and that it will go right many times in the future. In order to understand WHY this happened... we need to understand HOW this happens!
28 Safety II when everything goes right Safety-II: Safety is a condition where the number of successful outcomes (meaning everyday work) is as high as possible. It is the ability to succeed under varying conditions. Safety-II is achieved by trying to make sure that things go right, rather than by preventing them from going wrong. Safety Safety is is defined defined by by its its presence. presence. The The focus focus is is on on everyday everyday situations situations where where things things go go right right as as they they should. should. Individuals and organisations must adjust everything they do to match the current conditions. Everyday performance must be variable in order for things to work. Performance variability Acceptable outcomes Unacceptable outcomes
29 Resilient health care Resilience is an expression of how people, alone or together, cope with everyday situations - large and small by adjusting their performance to the conditions. An organisation s performance is resilient if it can function as required under expected and unexpected conditions alike (changes / disturbances / opportunities). Respond Learn Monitor Anticipate To do so, the organisation must be able to adjust its functioning prior to, during, or following events. The organisation must therefore have the abilities to respond, monitor, learn, and anticipate.
30 What makes performance resilient? Improve everyday performance by being able to respond to threats and opportunities alike Learn Respond Monitor Improve everyday performance by being able to anticipate longterm changes to demands and resources. Anticipate Improve everyday performance by being able to learn both from what goes right and what goes wrong. Improve everyday performance by being able to monitor what happens externally and internally. CREATE & MAINTAIN conditions required for work to be done COMPENSATE FOR conditions that may impede work to be done AVOID anything that may imperil your or your organisation
31 Resilience: Focus on everyday work Things that are difficult but go right Early completion Excellence Innovation Things that go wrong Unwanted outcomes Planned outcomes Positive surprises
32 Assessing the potential for resilience Which events can the system respond to? How were events and responses chosen? When is a response given (threshold)? How is readiness maintained and ensured? Respond What is the official model of the future? What is the time horizon of anticipation? Which risks are acceptable/affordable? Who thinks about the future and when? Learn Monitor Anticipate What is learning based on? When does learning take place? How are learning outcomes implemented? How is learning maintained and verified? How have indicators been defined? Are they leading or lagging? When are indicators read? What is the validity of indicators?
33 Resilience Analysis Grid (RAG) RAG profile for the ability to respond (constructed example)
34 Resilience Analysis Grid (RAG) RAG profiles from different groups of staff (actual data)

35 What does responding depend on?

36 What does monitoring depend on?

37 What does learning depend on?

38 What does anticipation depend on?
39 Revise safety management practices Look for what goes right - breadth-before-depth The arbitrariness of accident analysis Look for work-as-done - the habitual adjustments and why they are made Creating and maintaining good working conditions Compensating for something that is missing Avoid future problems Learning from events that are frequent rather than severe The accumulated effects of many small events can be larger than one big event. It is easier to improve on small events than on large ones. No need to wait for an accident to learn. Remain sensitive to the possibility of failure (mindfulness) Avoid being complacent. Past successes are no guarantee for future performance.
40 Towards resilient health care Safety-I: No lack of safety Safety-II: Resilient safety management We are safe if there is as little as possible of this We are safe if there is as much as possible of this Prevent, eliminate, constrain. Safety, quality, etc. are different and require different measures and methods. Support, augment, facilitate. Safety, quality, etc. are inseparable and need matching measures and methods.


41 Thank you for your attention
6/17/2014. Resilient health care: forging new directions. Australian Institute of Health Innovation s mission
 Question 1: what s your definition of resilience, please? Resilient health care: forging new directions Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Professor of Health
Question 1: what s your definition of resilience, please? Resilient health care: forging new directions Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Professor of Health
Case study: how reliable are our healthcare systems?
 Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Presentation to the Resilient Health Care Net Summer Meeting
 The Resilient Health Care Net Summer Meeting, August 26-28, 2013 How everyday functioning in acute care really works: the case of nurses workarounds The Resilience of Everyday Clinical Work Tentative programme
The Resilient Health Care Net Summer Meeting, August 26-28, 2013 How everyday functioning in acute care really works: the case of nurses workarounds The Resilience of Everyday Clinical Work Tentative programme
The CARE CERTIFICATE. Duty of Care. What you need to know. Standard THE CARE CERTIFICATE WORKBOOK
 The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
The NHS Constitution
 2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Resilience in Healthcare
 Resilience in Healthcare The Other Side of Human Error Dr Carl Horsley, Critical Care Complex, Middlemore Hospital Patient Safety Staff Safety Outline The current model of safety The problems with the
Resilience in Healthcare The Other Side of Human Error Dr Carl Horsley, Critical Care Complex, Middlemore Hospital Patient Safety Staff Safety Outline The current model of safety The problems with the
A culture of safety is a culture of compassion
 A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
Applying a human factors approach
 AUSTRALIAN INSTITUTE OF HEALTH INNOVATION Faculty of Medicine and Health Sciences Applying a human factors approach to improve the quality of health care 2 Applying a human factors approach to improve
AUSTRALIAN INSTITUTE OF HEALTH INNOVATION Faculty of Medicine and Health Sciences Applying a human factors approach to improve the quality of health care 2 Applying a human factors approach to improve
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Summary of Responses to Open Ended Questions
 Summary of Responses to Open Ended Questions Thank you for your patience in waiting for this rather long response. It covers a summary of all the open ended responses and is to be read alongside the original
Summary of Responses to Open Ended Questions Thank you for your patience in waiting for this rather long response. It covers a summary of all the open ended responses and is to be read alongside the original
Changes in practice and organisation surrounding blood transfusion in NHS trusts in England
 See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Understanding resilient clinical practice in Emergency Department ecosystems. Jeffrey Braithwaite, PhD Robyn Clay-Williams, PhD
 Understanding resilient clinical practice in Emergency Department ecosystems Australian Institute of Health Innovation Jeffrey Braithwaite, PhD Robyn Clay-Williams, PhD Presentation to the Resilient Healthcare
Understanding resilient clinical practice in Emergency Department ecosystems Australian Institute of Health Innovation Jeffrey Braithwaite, PhD Robyn Clay-Williams, PhD Presentation to the Resilient Healthcare
Incident Reporting Systems
 Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Ward pharmacists perceptions on how e-prescribing and administration systems impact their activities
 Ward pharmacists perceptions on how e-prescribing and administration systems impact their activities UCL-Cerner epma Symposium 8 February 2017 Monsey McLeod Lead Pharmacist, Medication Safety and Anti-infectives
Ward pharmacists perceptions on how e-prescribing and administration systems impact their activities UCL-Cerner epma Symposium 8 February 2017 Monsey McLeod Lead Pharmacist, Medication Safety and Anti-infectives
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE
 Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Psychologist-Patient Services Agreement
 Psychologist-Patient Services Agreement Welcome! This document contains important information about my professional services and business policies. This document also contains a brief summary of information
Psychologist-Patient Services Agreement Welcome! This document contains important information about my professional services and business policies. This document also contains a brief summary of information
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
#104 - Prevention of Medical Errors [1]
![#104 - Prevention of Medical Errors [1]](/thumbs/74/70423609.jpg "#104 - Prevention of Medical Errors [1]") Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
NHS Constitution The NHS belongs to the people. This Constitution principles values rights pledges responsibilities
 for England 8 March 2012 2 NHS Constitution The NHS belongs to the people. It is there to improve our health and well-being, supporting us to keep mentally and physically well, to get better when we are
for England 8 March 2012 2 NHS Constitution The NHS belongs to the people. It is there to improve our health and well-being, supporting us to keep mentally and physically well, to get better when we are
Lone Worker Policy Children s Social Care, Bath and North East Somerset
 Lone Worker Policy Children s Social Care, Bath and North East Somerset Policy Date: June 2017 Renewal Date: June 2020 1. Introduction. This policy sets out the approach of Bath and North East Somerset
Lone Worker Policy Children s Social Care, Bath and North East Somerset Policy Date: June 2017 Renewal Date: June 2020 1. Introduction. This policy sets out the approach of Bath and North East Somerset
Overview SKASS2. Control the movement of spectators and deal with crowd issues at an event
 issues at an Overview This standard is about keeping a careful watch over spectators including their entry to and exit from the venue. It also covers dealing with crowd issues such as unexpected movements,
issues at an Overview This standard is about keeping a careful watch over spectators including their entry to and exit from the venue. It also covers dealing with crowd issues such as unexpected movements,
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process
 Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
A Review of Current EMTALA and Florida Law
 A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
Patient Safety. Annual Accidental Deaths. Medical Errors in History. How Hazardous Is Health Care (Amalberti)
") Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
Adverse Incident Management. Mid Highland Community Health Partnership. Report for Governance Committee
 Adverse Incident Management Mid Highland Community Health Partnership Report for Governance Committee Introduction There are two ways risk in its broadest sense can be managed. Firstly, the proactive approach.
Adverse Incident Management Mid Highland Community Health Partnership Report for Governance Committee Introduction There are two ways risk in its broadest sense can be managed. Firstly, the proactive approach.
CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
DEALING WITH DIFFICULT, ABUSIVE, AGGRESSIVE OR NON-COMPLIANT PATIENTS
 DEALING WITH DIFFICULT, ABUSIVE, AGGRESSIVE OR NON-COMPLIANT PATIENTS INTRODUCTION There is growing concern throughout Australia as to how health facilities respond to patients who are considered difficult,
DEALING WITH DIFFICULT, ABUSIVE, AGGRESSIVE OR NON-COMPLIANT PATIENTS INTRODUCTION There is growing concern throughout Australia as to how health facilities respond to patients who are considered difficult,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses
 Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
SAMPLE. Certificate in Understanding Dignity and Safeguarding in Adult Health and Social Care. Workbook 1 DUTY OF CARE SAFEGUARDING.
 Level 2 Certificate in Understanding Dignity and Safeguarding in Adult Health and Social Care INFORMATION AND SUPPORT DUTY OF CARE PERSON-CENTRED SAFEGUARDING DILEMMAS PROMOTING DIGNITY In this section
Level 2 Certificate in Understanding Dignity and Safeguarding in Adult Health and Social Care INFORMATION AND SUPPORT DUTY OF CARE PERSON-CENTRED SAFEGUARDING DILEMMAS PROMOTING DIGNITY In this section
Safeguarding Vulnerable Adults Policy
 POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
The Reliable Design of Obstetric and Gynecologic Care
 VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
The Regulatory Focus. Critical Access Hospitals The Regulatory Process
 Critical Access Hospitals The Regulatory Process Montana DPHHS Quality Assurance Division Roy Kemp, Deputy Administrator rkemp@mt.gov The Regulatory Focus The fundamental principal of the state regulatory
Critical Access Hospitals The Regulatory Process Montana DPHHS Quality Assurance Division Roy Kemp, Deputy Administrator rkemp@mt.gov The Regulatory Focus The fundamental principal of the state regulatory
Management of Violence and Aggression Policy
 Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
Risk Management Fundamentals
 Chapter 1 Risk Management Fundamentals Sizing up opponents to determine victory, assessing dangers and distances is the proper course of action for military leaders. Sun Tzu, The Art of War, Terrain Risk
Chapter 1 Risk Management Fundamentals Sizing up opponents to determine victory, assessing dangers and distances is the proper course of action for military leaders. Sun Tzu, The Art of War, Terrain Risk
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Nursing Documentation 101
 Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
CREATE A GREAT QUALITY SYSTEM IN SIX MONTHS USING THE
 1 CREATE A GREAT QUALITY SYSTEM IN SIX MONTHS USING THE STRATEGIC QUALITY SYSTEM Dr Cathy Balding www.cathybalding.com 10 years after QAHCS Medical Journal of Australia Editorial: Ten years on can we confidently
1 CREATE A GREAT QUALITY SYSTEM IN SIX MONTHS USING THE STRATEGIC QUALITY SYSTEM Dr Cathy Balding www.cathybalding.com 10 years after QAHCS Medical Journal of Australia Editorial: Ten years on can we confidently
Patient-Centered Case Management Assessment & Patient Interview Techniques
 Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
June 19, Submitted Electronically
 June 19, 2018 Seema Verma Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1694-P PO Box 8011 Baltimore, MD 21244-1850 Submitted Electronically
June 19, 2018 Seema Verma Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1694-P PO Box 8011 Baltimore, MD 21244-1850 Submitted Electronically
Sarah Bloomfield, Director of Nursing and Quality
 Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Unit 2 Clinical Governance & Risk Management Awareness
 Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY
 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
Parliamentary and Health Service Ombudsman. Complaints about the NHS in England: Quarter
 Parliamentary and Health Service Ombudsman Complaints about the NHS in England: Quarter 1 2018-19 Contents Our role 3 The purpose of this report 3 Our data 3 Our process 3 Step one: initial checks 4 Step
Parliamentary and Health Service Ombudsman Complaints about the NHS in England: Quarter 1 2018-19 Contents Our role 3 The purpose of this report 3 Our data 3 Our process 3 Step one: initial checks 4 Step
Home administration of intravenous diuretics to heart failure patients:
 Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Reducing Risk: Mental health team discussion framework May Contents
 Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Risk Assessment Scoring and Matrix
 Risk Assessment Scoring and Matrix Appendix 2 Consequence score (severity levels) and examples of descriptors 1 2 3 4 5 Domains Negligible Minor Moderate Major Catastrophic Impact on the safety of patients,
Risk Assessment Scoring and Matrix Appendix 2 Consequence score (severity levels) and examples of descriptors 1 2 3 4 5 Domains Negligible Minor Moderate Major Catastrophic Impact on the safety of patients,
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
POLICY ON LONE WORKING JANUARY 2012
 POLICY ON LONE WORKING JANUARY 2012 Author: Sheena Gordon V&A Co-ordinator Responsible Director: Ian Reid Director of HR Approved by: Health and Safety Forum Date for Review: January 2014 Version: 2.0
POLICY ON LONE WORKING JANUARY 2012 Author: Sheena Gordon V&A Co-ordinator Responsible Director: Ian Reid Director of HR Approved by: Health and Safety Forum Date for Review: January 2014 Version: 2.0
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Nurse Managers Role in Promoting Quality Nursing Practice
 Nurse Managers Role in Promoting Quality Nursing Practice Mission Critical: Nurse Manager Summit Fredericton, New Brunswick April 30, 2015 Jeanne Besner, C.M., PhD, RN 1 Outline of Presentation Background
Nurse Managers Role in Promoting Quality Nursing Practice Mission Critical: Nurse Manager Summit Fredericton, New Brunswick April 30, 2015 Jeanne Besner, C.M., PhD, RN 1 Outline of Presentation Background
SafetyFirst: The Journey to High Reliability
 SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
Sharing your information to improve care
 Sharing your information to improve care North West London health and care professionals are working together to provide your care. Those involved can see relevant information about you, so you can receive
Sharing your information to improve care North West London health and care professionals are working together to provide your care. Those involved can see relevant information about you, so you can receive
MASSACHUSETTS COLLEGE OF EMERGENCY PHYSICIANS. Mandated Nurse Staffing Ratios in Emergency Departments: Unworkable & Harmful to the Community
 MASSACHUSETTS COLLEGE OF EMERGENCY PHYSICIANS Mandated Nurse Staffing Ratios in Emergency Departments: Unworkable & Harmful to the Community September 2018 Mandated Nurse Staffing Ratios in Emergency Departments:
MASSACHUSETTS COLLEGE OF EMERGENCY PHYSICIANS Mandated Nurse Staffing Ratios in Emergency Departments: Unworkable & Harmful to the Community September 2018 Mandated Nurse Staffing Ratios in Emergency Departments:
10: Beyond the caring role
 10: Beyond the caring role This section provides support if you no longer need to give the same level of care to a person with MND or your caring role has come to an end. The following information is a
10: Beyond the caring role This section provides support if you no longer need to give the same level of care to a person with MND or your caring role has come to an end. The following information is a
These Things (Don t Have to) Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013
 Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013") These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Cambridge Technicals Health and Social Care. Mark Scheme for January Unit 3: Health, safety and security in health and social care
 Cambridge Technicals Health and Social Care Unit 3: Health, safety and security in health and social care Level 3 Cambridge Technical Certificate/Diploma in Health and Social Care 05830-05871 Mark Scheme
Cambridge Technicals Health and Social Care Unit 3: Health, safety and security in health and social care Level 3 Cambridge Technical Certificate/Diploma in Health and Social Care 05830-05871 Mark Scheme
Incident Reporting Systems and Future Strategies for Patient Safety Improvement
 WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
National findings from the 2013 Inpatients survey
 National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
Extract from Managing Infection Control
 TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
2014 Hospital Admission Criteria
 2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
Reducing Attendances and Waits in Emergency Departments A systematic review of present innovations
 Reducing Attendances and Waits in Emergency Departments A systematic review of present innovations Report to the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO) January
Reducing Attendances and Waits in Emergency Departments A systematic review of present innovations Report to the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO) January
PROFESSIONAL COMMUNICATION AND BEHAVIOR
 Interpersonal Communication Skills Interpersonal communications means "showing appropriate ways to exchange your ideas and needs. Interpersonal Skills, these are the skills one relies on most in order
Interpersonal Communication Skills Interpersonal communications means "showing appropriate ways to exchange your ideas and needs. Interpersonal Skills, these are the skills one relies on most in order
Risk Assessment in Safeguarding Adults
 Risk Assessment in Safeguarding Adults The primary aim of the Safeguarding Risk Assessment is to assess: Individuals for the current risks that they face Potential risks they may face The secondary aim
Risk Assessment in Safeguarding Adults The primary aim of the Safeguarding Risk Assessment is to assess: Individuals for the current risks that they face Potential risks they may face The secondary aim
NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS
 Appendix 1 NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS Contents 1 Introduction Page 3 1.1 Purpose of this Policy Page 3 1.2 Rationale
Appendix 1 NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS Contents 1 Introduction Page 3 1.1 Purpose of this Policy Page 3 1.2 Rationale
QI TALK TIME. Building an Irish Network of Quality Improvers. Leading for Quality. Speaker: Peter Lachman ISQua CEO. 21st Nov 2017
 QI TALK TIME Building an Irish Network of Quality Improvers Leading for Quality Speaker: Peter Lachman ISQua CEO 21st Nov 2017 Connect Improve Innovate Speaker Peter Lachman - M.D. MPH. M.B.B.Ch., FRCPCH,
QI TALK TIME Building an Irish Network of Quality Improvers Leading for Quality Speaker: Peter Lachman ISQua CEO 21st Nov 2017 Connect Improve Innovate Speaker Peter Lachman - M.D. MPH. M.B.B.Ch., FRCPCH,
GPhC response to the Rebalancing Medicines Legislation and Pharmacy Regulation: draft Orders under section 60 of the Health Act 1999 consultation
 GPhC response to the Rebalancing Medicines Legislation and Pharmacy Regulation: draft Orders under section 60 of the Health Act 1999 consultation Background The General Pharmaceutical Council (GPhC) is
GPhC response to the Rebalancing Medicines Legislation and Pharmacy Regulation: draft Orders under section 60 of the Health Act 1999 consultation Background The General Pharmaceutical Council (GPhC) is
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Working together for better health The NHS is your NHS, use it well and it will serve you better.
 Working together for better health The NHS is your NHS, use it well and it will serve you better. The NHS belongs to all of us. It is a limited resource and there are things that we can all do for ourselves
Working together for better health The NHS is your NHS, use it well and it will serve you better. The NHS belongs to all of us. It is a limited resource and there are things that we can all do for ourselves
community links Intermediate Hostels Evaluating the Social Return on Investment community links hostels
 community links Intermediate Hostels Evaluating the Social Return on Investment community links hostels Community Links Intermediate Hostels: Evaluating the Social Return on Investment About the Hostels
community links Intermediate Hostels Evaluating the Social Return on Investment community links hostels Community Links Intermediate Hostels: Evaluating the Social Return on Investment About the Hostels
Why do we make mistakes? Human factors in transfusion practice
 Why do we make mistakes? Human factors in transfusion practice East of England Regional Transfusion Committee Blood transfusion: What now? What if? What next? Alison Watt SHOT Operations Manager Paula
Why do we make mistakes? Human factors in transfusion practice East of England Regional Transfusion Committee Blood transfusion: What now? What if? What next? Alison Watt SHOT Operations Manager Paula
CREATING SAFETY IN AN EMERGENCY DEPARTMENT
 T H E U N I V E R S I T Y O F B R I T I S H C O L U M B I A! CREATING SAFETY IN AN EMERGENCY DEPARTMENT Garth Hunte, MD PhD Clinical Associate Professor Department of Emergency Medicine Research Scientist,
T H E U N I V E R S I T Y O F B R I T I S H C O L U M B I A! CREATING SAFETY IN AN EMERGENCY DEPARTMENT Garth Hunte, MD PhD Clinical Associate Professor Department of Emergency Medicine Research Scientist,
The Primary Care Trigger Tool: Practical Guidance
 The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Our plans for NHS patient safety investigation
 ,.,,:f.j Improvement Our plans for NHS patient safety investigation What do you think? collaboration trust respect innovation courage compassion Contents Page Introduction 3 Keeping people safe 5 Serious
,.,,:f.j Improvement Our plans for NHS patient safety investigation What do you think? collaboration trust respect innovation courage compassion Contents Page Introduction 3 Keeping people safe 5 Serious
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Julia Galliers and Stephanie Wilson, CHCID, City University London, UK
 DATA GATHERING FOR THE SAFER HANDOVER PROJECT Julia Galliers and Stephanie Wilson, CHCID, City University London, UK Introduction The terminology issue Introduction The Safer Handover project was initiated
DATA GATHERING FOR THE SAFER HANDOVER PROJECT Julia Galliers and Stephanie Wilson, CHCID, City University London, UK Introduction The terminology issue Introduction The Safer Handover project was initiated
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Copyright, Joint Commission International. Tracer Methodology
 Tracer Methodology 2 What is a Tracer? JCI s key assessment method Traces a real patient s journey through the hospital, using their record as a guide Along the path, JCI observes and assesses compliance
Tracer Methodology 2 What is a Tracer? JCI s key assessment method Traces a real patient s journey through the hospital, using their record as a guide Along the path, JCI observes and assesses compliance
SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy
 SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy First Issued January 2007 Issue Version One Purpose of Issue/Description of Change Outlines the process that staff
SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy First Issued January 2007 Issue Version One Purpose of Issue/Description of Change Outlines the process that staff
Bowel Screening Wales Information booklet for care homes and associated health professionals. Available in other formats on request. October.14.v.2.
 Bowel Screening Wales Information booklet for care homes and associated health professionals Available in other formats on request October.14.v.2.0 Contents Section 1 Page 3 Who are Bowel Screening Wales
Bowel Screening Wales Information booklet for care homes and associated health professionals Available in other formats on request October.14.v.2.0 Contents Section 1 Page 3 Who are Bowel Screening Wales
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Building a Safe Healthcare System
 Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
Returning to the Why: Patient and Caregiver Suffering and Care. Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer
 Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death