2015 Na(onal Medicaid and CHIP Oral Health Symposium. Pediatric Den(st Opinion and Inter- professional Prac(ce in 2015.
|
|
|
- Shannon Ford
- 6 years ago
- Views:
Transcription
1 MSDA Medicaid CHIP State Dental Association 2015 Na(onal Medicaid and CHIP Oral Health Symposium Session # 8 Pediatric Den(st Opinion and Inter- professional Prac(ce in 2015 Maria Cordero- Ricardo, DDS, MS Paul Casamassimo, DDS, MS Washington Marrio: Wardman Park Monday, June 1 st, 2015
2 Learning Objec-ve(s) Par-cipants will gain knowledge in: 1. Understanding contemporary IP prac-ce in pediatric den-stry 2. Those IP procedures currently ac-ve in pediatric den-stry prac-ce 3. Obstacles and issues relate to IP as stated by a sample of pediatric den-sts
3 Disclosure and Conflict of Interest Declara-on q I declare that neither I nor any member of my family have a financial arrangement or affilia-on with any corporate organiza-on offering financial support or grant monies for this con-nuing dental educa-on program, nor do I have a financial interest in any commercial product(s) or service(s) I will discuss in the presenta-on.
4 Background Pediatric den-sts treat children with special needs, provide seda-on and GA services and have an interest and commitment to the health of young children Typically, pediatric den-sts may perform BPs, height/weight, check on immuniza-ons, and address other health issues in a variety of contexts These procedures are typically uncompensated, but have importance in the care of the child
5 Addi-onal Background HRSA recommends: Apply oral health core competencies within PCP to increase oral health care access for safety net popula-ons in US Develop infrastructure. that enhances adop-on of oral health core competencies Modify payment policies to address costs of implemen-ng oral health competencies Execute programs to develop and evaluate implementa(on strategies USDHHS, HRSA. Integra-on of Oral Health and Primary Care Prac-ce. February 2014
6 Addi-onal Background Ins-tute of Medicine (IOM) concludes: Without a purposeful and more comprehensive system of engagement between educa-on and health delivery system, evalua-ng impact of IPE and outcomes will be difficult, Having a comprehensive conceptual model would enhance descrip-on and purpose of IPE, More purposeful, well- designed and thoughjully reported studies are needed
7 Addi-onal Background from IOM IOM recommends: All par(es should commit resources to a coordinated series of well- designed studies on associa(on between IPE and collabora(ve behavior Health professions educators and academic and health systems leaders should adopt a mixed methods research approach for evalua-ng the impact of IPE on health and systems outcomes IOM. Measuring the Impact of Interprofessional Educa-on on Collabora-ve Prac-ce and Pa-ent Outcomes. Report Brief, April, 2015
8 Pediatric Dental Workforce A_tudes Toward Interprofessional Collabora-ve Prac-ce This is inves-ga-on a`empted to determine a_tudes, barriers, and feasibility of interprofessional prac-ce in context of current pediatric den-stry in the US. The study a`empted to quan-fy current prac-ces, applica-on of knowledge, interest and an-cipated barriers to expansion of responsibili-es and scope of prac-ce of pediatric den-sts.
9 Study Design and Implementa-on Sample of all pediatric den-st members of AAPD across the US University IRB approved Non- validated ques-onnaire, expert reviewed Survey Monkey distribu-on Resurvey once
 Large Private (3+ prac--oners) (163, 24.7%) Corporate Prac-ce (28, 4.2%), Federally Qualified Health Center (45, 6.")
10 Results 1025 Surveys were started 606 (64%) were completed Male 56.4% 4.5% in training Small Private (1-2 prac--oners) (315, 47.7%) Large Private (3+ prac--oners) (163, 24.7%) Corporate Prac-ce (28, 4.2%), Federally Qualified Health Center (45, 6.8%) Academia (109, 16.5%)

11 ICP Important to 92% of Pediatric Den-sts (610 of 661)


12 PDs Likely to Screen, Refer, Discuss Screen by Interview Refer to Physician for Consultation Discuss Results Chairside

13 PD are Less Likely to Screen with Biometric Data (BMI)

14 PDs Unlikely to Screen by Specimen Collec-on
15 What Most PDs Do in ICP AcCvity ParCcipaCon Rate Verifica-on of Immuniza-ons 45% Validate Medical Home 83% Ask about Child Safety 46% Take Blood Pressure Measurements 52% Take Height and Weight Measurements 54% Calculate BMI 19% Screen for GERD 43% Screen for Diabetes 26%

16 Of 52% Who Take BP Measurements, Only 13% Perform it on All Pa-ents
 I do not want any liability for errors (55, 10.3%) I do not want to follow up with families (31, 5.8%) It does not alter my willingness or ability to treat the child (292, 54.")
17 81% of PDs do not Calculate BMI Most common reasons: I do not consider it part of my professional responsibility (263, 49.3%) I do not want to track the most current medical guidelines (30, 5.6%) I do not want any liability for errors (55, 10.3%) I do not want to follow up with families (31, 5.8%) It does not alter my willingness or ability to treat the child (292, 54.7%) I do not want to train or retrain my staff in this service (45, 8.4%)
18 Finances May Be More Important Than A_tudes I should be reimbursed for all these services comparable to other health professionals. I am willing to do these to enhance my praccce without reimbursement. I need to be reimbursed only for those that deviate from my current praccce roucne. I need to be reimbursed only for those that require staff Cme and equipment. Third parces should reimburse pediatric dencsts performing the interprofessional services described above. Third party reimbursement would make you perform some interprofessional services you do not currently provide. Agreed 70% 59% 51% 65% 81% 61%
19 Conclusions 1. Pediatric den-sts believe ICP is important 2. The greatest mo-vator is a PD s sense of professionalism and duty toward pa-ent care 3. Barriers are: a. The greatest barrier is the a_tude that the findings will not alter treatment b. The prac-ce or the PD s responsibility 4. Financial considera-ons would impact individuals willingness to par-cipate
20 Diverse Comments Revealing I have to pick my ba`les We pediatric den-sts have to do what we do best. all other areas refer to pediatrician If we do these, they need to be reported to medical providers to prevent duplica-on I get a lot of denials for fluoride because the pediatricians are billing insurance. These are money losers for pediatric den-sts in private prac-ce and money could be be`er invested elsewhere It can be difficult to get compliance for OHI, so why burden parents with BMI? I think ICP is important when there is no MD. I prac-ce in an area with excellent pediatricians, so not necessary If we are doing these, we be`er be darn sure we are doing them right.. Best done if access to EHR. If I have concerns, I refer to pediatricians Seems like a reasonable demand for a pediatric den-st without compensa-on. Who came up with this stuff? I have more kids to care for than to get into MD stuff! 20
21 Contact Informa-on Paul Casamassimo, DDS, MS, Professor The Ohio State University and Na-onwide Children s Hospital, Columbus, OH Casamassimo.1@osu.edu 21
22 MSDA Medicaid CHIP State Dental Association 2015 Na(onal Medicaid and CHIP Oral Health Symposium Session # 6 When Two Becomes One Mark Doherty DMD MPH Safety Net SoluCons Washington Marrio: Wardman Park Monday, June 1 st,

23

24 The comprehensive health care system supports Oral Health collaborations/integration that treats the patient at the point of care where the patient is most comfortable and applies a patient-centered approach to treatment.


25 Collabora-on or Integra-on CollaboraCon = primary care and oral health working with one another IntegraCon = oral health working within and as part of primary care or vice versa..provision of dental services within primary care
26 Primary Care Workforce Can make a difference! Family Medicine 105,000 Pediatrics 45,000 General Internists 70,000 Nurse Prac--oners 150,000 Physician Assistants 36,000
27 Menu Components Caries Risk Assessment OH Screening/evalua-on Behavior Change through An-cipatory Guidance The FL varnish piece Ins-tu-onalized Referral Process Designated Access Appointments EMR/EDR Interface Case/Care Management Warm- handoffs Curbside Consults Installed a dental suite in Pediatrics
28 Barriers We are brought up in a Bifurcated care system Educated separately Licensed separately Regulated separately Prac-ce independently PCPs see the mouth as the property of den-sts Sharing of informa-on rarely occurs Seen by the public/pa-ents as separate Oral Health training for health professionals has been sparse to non- existent Non- integrated benefits/insurance programs
29 Outcomes Improved Health Improves Accountability Early Interven-ons Healthy People 2020 Preven-on Expanded Workforce Portal to the family Increased Access One stop shopping Improved Efficiency > OH Literacy Reimbursement for children s dental services < OH dispari-es Pa-ent Centric >OH Promo-on Wellness Achieved Innova-ve Finance and Service Delivery
30 The ECOH Model The Early Childhood Oral Health (ECOH) program was developed in Ohio with a goal of improving oral health outcomes for Ohio s youngest and most vulnerable ci-zens by integra1ng preven1ve oral health prac1ces within the primary care se8ng. To achieve that goal, the ECOH business plan was developed. The purpose of the ECOH business plan is to clearly define the goals and objec-ves of an early childhood oral health program and provide the strategy to achieve them.
31 ECOH (con-nued) Sustainability of the ECOH ini-a-ve will not come from the applica-on of preven-ve oral health prac-ces within the primary care se_ng as Medicaid will not reimburse for these services as a separate visit apart from the well- child visit. Sustainability will be achieved by the increase in dental revenue that will result from referrals of children of all ages from pediatrics and family prac-ce to the dental clinic. To facilitate medical referrals to dental, ensure that
32 Case Managers Facilita-ng referrals Help parents enroll in publicly available insurance programs Assist in removing barriers to care Referral follow up Track and report the results of the ini-a-ve An effec1ve and accountable case manager will be able to cover his or her salary several 1mes over through the addi1onal dental revenue that will result from his or her efforts.
 cri-cal to program success Dental reimburses medical $18,842 to reimburse medical for supplies and staff -me to do screenings,")
33 ECOH Vision Improvement in payer mix through referral of more children of all ages to dental (50% Medicaid to 62% Medicaid) Increased revenue for dental as a result of change in payer mix (+$137,020) Dental invests $65,000 in case manager/coordinator (salary plus fringe) cri-cal to program success Dental reimburses medical $18,842 to reimburse medical for supplies and staff -me to do screenings, referrals, AG and FL varnish Baby Days in dental one day per week generates 736 addi-onal visits to dental for children <age 3 Investment generates nearly $53,000 in addi-onal revenue for dental AFTER all costs
34 ECOH Program Assump-ons Dental Program w/o ECOH IntegraCon Dental Program with ECOH and IntegraCon Clinic operates 46 weeks/year Clinic operates 46 weeks/year 4 operatories 4 operatories Total visits: 5,313 Total visits: 6,049 Hours: M- F 8-5 Hours: M- F 8-5 Staffing: 1 FTE den-st/clinical director, 2 FTE dental assistant, 1 FTE hygienist, 2 FTE recep-on/ registra-on clerks Staffing: 1 FTE den-st/clinical director, 2 FTE dental assistant, 1 FTE hygienist, 2 FTE recep-on/registra-on clerks, plus 1 FTE case manager ECOH program adds 736 addi-onal visits to the dental program (ages 0-3)
35 Calcula-ons Looked at UDS data for Ohio and divided total number of pediatricians by number of FQHCS to get an average of 1.5 FTE pediatricians per health center 33,808 unduplicated children in Ohio health centers under age 3 in health centers = average of 1,057 unduplicated children under age 3 per health center Guess-mated on the 1,035 well child visits where FL varnish would be applied: Pediatrician would see 18 pa-ents per day. 9 of these would be well- child visits x 230 days for a total of 2,070 well child visits per year. Assumed that half of these would be children under 3 years of age (given the high number of well child visits in the first three years of life) Assumed each pediatrician would have a panel size of 1,000 unduplicated pa-ents for a total of 1,500 unduplicated pediatric pa-ents per health center
36 Calcula-ons cont. Assumed a third of these unduplicated pa-ents are over age 3 and are referred to dental at least once per year Assumed the following for the 500 unduplicated pa-ents >age 3: All 500 would get a new pa-ent visit 250 would come back in 6 months for a recall visit 150 children would need at least one restora-ve visit 150 children referred would be eligible for sealants For a total of 1,050 visits For a Health Center dental program doing Baby Days one morning per week with block scheduling for children 3 years of age, 16 kids would be seen per morning x 46 weeks = 736 visits (70% of unduplicated children under age 3)
37 Calcula-ons cont. Payer mix axer integra-on is 62% Medicaid, 23% Uninsured/ SFS, 10% Commercial and 5% $0 pay $130 average per visit fee from Medicaid, $40 per visit fee from uninsured Assumed average pediatrician or FP s hourly rate would be $75. Assumed it would take 10 minutes of their -me to do screening and an-cipatory guidance (with mid- level doing the actual FL varnish applica-on). 10 minutes x 1035 visits = 10,350 minutes 60 minutes = hours per year x $75/ hour = $12,938 (value of physician s -me)
38 Dental Program Without ECOH & Integration Dental Program With ECOH & Integration REVENUE Year 1 5,313 visits REVENUE Year 1 6,049 visits* Self-Pay (35%) $74,400$40/visit Self-Pay (23%) 55,640$40/visit Medicaid (50%) $345,410$130/visit Medicaid (62%) $487,500$130/visit Commercial Insurance (10%) $98,235$185/visit Commercial Insurance (10%) $111,925$185/visit Free care patients (5%) $0 $0 Free care patients (5%) $0 $0 Total Patient Net Revenue $518,045 Total Patient Net Revenue $655,065 Grant Revenue Grant Revenue 330 Allocation $250, Allocation $250,000 Total Revenue $768,045 Total Revenue $905,065 Direct Expenses Direct Expenses Personnel Related Personnel Related Salaries $322,400 Salaries $374,400 Fringe Benefits (25%) $80,600 Fringe Benefits (25%) $93,600 Malpractice Insurance $0 Malpractice Insurance $0 Subtotal Personnel Costs $403,000 Subtotal Personnel Costs $468,000
39 Support costs Support costs Dental Supplies $42,504$8/visit Dental Supplies $42,504$8/visit 75 Dental Lab Services 130 $150/ $20,000patient Dental Lab Services patients $150/ $11,250patient Equipment Repair/ Maintenance $9,500 Equipment Repair/ Maintenance $9,500 Housekeeping $6,000 Housekeeping $6,000 Conference/Travel $2,000 Conference/Travel $2,000 Office Supplies $3,000 Office Supplies $3,000 Computer Maintenance, License Fees $12,000 Computer Maintenance, License Fees $12,000 Books & Subscriptions $1,000 Books & Subscriptions $1,000 Fees & Dues $3,500 Fees & Dues $3,500 Recruitment Expenses $3,000 Recruitment Expenses $3,000 Insurance $10,000 Insurance $10,000 Printing $2,000 Printing $2,000 Postage $2,000 Postage $2,000 Depreciation $30,000 Depreciation $30,000 Bad Debt $11,500 Bad Debt $11,500 Total Support Costs $158,004 Total Support Costs $149,254
40 Building-Related Costs ECOH Program Costs Maintenance FL Varnish $1,367$1.32/visit Rent/Mortgage $6,000 Utilities $30,000 Medical Materials Costs (Anticipatory Guidance) $4,500$3/visit Medical Staff allocation to reimburse for time spent in screening, FV application and AG $12,975 Telephone/Internet $10,000 Total ECOH Program Costs $18,842 Total Building Costs $5,000 $51,000 Building-Related Costs Total Direct Expenses Maintenance $6,000 $612,004 Rent/Mortgage $30,000 Indirect Expenses Utilities $10,000 Total Support & Admin Allocation (12% of direct expenses) $73,440 Telephone/Internet $5,000 TOTAL EXPENSES $685,444 Total Building Costs $51,000 TOTAL REVENUE $768,045 PROFIT $82,601 Total Direct Expenses $687,096 Indirect Expenses Total Support & Admin Allocation (12% of direct expenses) $82,452 TOTAL EXPENSES $769,548 TOTAL REVENUE $905,065 PROFIT $135,517


41 Partnering to Strengthen and Preserve the Oral Health Safety Net A PROGRAM OF THE Mark J. Doherty, DMD, MPH 2400 Computer Drive, Westborough, MA Tel: Fax:
42 MSDA Medicaid CHIP State Dental Association 2015 Na(onal Medicaid and CHIP Oral Health Symposium Session # 8 Opera(ons Manager School Based Oral Health Clinic Project Director Jennifer Pilapil Washington Marrio: Wardman Park Monday, June 1 st,
43 Disclosure and Conflict of Interest Declara-on q I declare that neither I nor any member of my family have a financial arrangement or affilia-on with any corporate organiza-on offering financial support or grant monies for this con-nuing dental educa-on program, nor do I have a financial interest in any commercial product(s) or service(s) I will discuss in the presenta-on. 43
44 Learning Objec-ve(s) Par-cipants will gain knowledge and understanding of: How school based healthcare may advance health outcomes for children How integrated oral and primary healthcare models in school based clinics have advanced to comprehensive healthcare service delivery Why Medicaid policies should support school- based healthcare How integrated models can help sustain school based healthcare services 44
45 Background Mommy, It Hurts to Chew, conducted in 2006 by the Dental Health Founda-on assessed the oral health of California s 3rd graders with the result that the oral health of California s children is substan-ally worse than na-onal objec-ves set forth by Healthy People Project developed in response to Health Resource Services Administra-on (HRSA) Funding Opportunity Announcement (FOA) 45
46 Integra-on Within School District Mental Health Vision Audiometry School Based Dental Office Child Health and Disability Program Primary Health Care School Nurses 46

47 Iden-fying Need and Loca-on for Services Spa-al analysis conducted Loca-on (s) iden-fied Coordina-on with: Head Start programs Early Educa-on Centers WICs Schools Hospitals Dental providers Other community agencies Community health navigators 47

48 The CHDP Program and Medicaid Enrollment 48
49 49
50 Table 21.1 CHDP PERIODICITY SCHEDULE FOR HEALTH ASSESSMENT REQUIREMENTS BY AGE GROUPS Screening Requirement 1 < 1 mo. 2 mos 4 mos 6 mos Age of Person Being Screened 12 mos 15 mos 18 mos 2 Yr 3 Yr 9 mos Interval Until Next CHDP Exam 1 mo 2 mos 2 mos 3 mos 3 mos 3 mos 3 mos 6 mos 1 yr 1 yr 2 yr 3 yr 4 yr 4 yr None History and Physical Examination 2 Dental Assessment 3 Nutritional Assessment Psychosocial/Behavioral Assessment 4 Developmental Screening 4 o o o Developmental Surveillance Other Laboratory Tests Tobacco Assessment When health history and/or physical examination warrants: Pelvic Exam 5 * * Urine Dipstick or Urinalysis 11 Measurements TST 12 - see Tuberculosis HAG Head Circumference Sickle Cell Height/Length and Weight Ova and Parasites BMI Percentile FBG and Total Cholesterol Blood Pressure 6 Papanicolaou (Pap) Smear Sensory Screening VDRL or RPR 13 Vision 7 - Visual Acuity Test Annually if sexually active; more often as clinically indicated: Vision 7 - Clinical Observation Gonorrhea Test 13 Hearing 8 - Audiometric Chlamydia Test 13 Hearing 8 - Clinical Assessment Immunizations 14 Procedures/Tests Hematocrit or Hemoglobin 9 * * * * * * * Key: Blood Lead Risk Assessment/ Anticipatory Guidance 10 Required by CHDP one time within the interval given Blood Lead Test 10 X o Recommended by AAP, Bright Futures and CHDP TB Risk Assessment 12 * Perform when indicated by risk assessment. Anticipatory Guidance x Perform if no documented lead level at 24 months 4-5 Yr 6-8 Yr 9-12 Yr Yr Yr Section 21 Note: The number of health assessments may be increased using MNIHA, as appropriate. 1 Note: Perform health assessment within 1 month of screening requirement age for children 2 years and under, and within 6 months for children 3 years and older. Note: Children coming under care who have not received all the recommended procedures for an earlier age should be brought up-todate as appropriate. 1. CHDP intervals are greater than recommended by Bright Futures. Providers may use MNIHA for necessary assessments that fall outside of periodicity such as school, sports or camp physical, foster care or out-of-home placement, or follow up indicated by findings on a prior health assessment that need monitoring including additional anticipatory guidance, perinatal problems or significant developmental delay. 2. Age-appropriate physical examination, including oral examination, is essential with child unclothed, and draped for older child or adolescent. 3. See Dental HAG. 4. Schedule indicates recommended ages for developmental screening and psychosocial/behavioral assessment. For reimbursement information, see CHDP PIN Pelvic exam recommended within 3 years of first sexual intercourse. Subsequent pelvic exams may be performed as part of MNIHA when clinically indicated by symptoms such as pelvic pain, dysuria, dysmenorrhea. See STI HAG. 6. Blood pressure before 3 years for at risk patients, then at each subsequent health assessment. See Blood Pressure HAG. 7. See Vision Screening HAG. 8. See Hearing Assessment HAG. 9. Hb/Hct starting at 9-12 months of age. See Iron Deficiency Anemia (IDA) HAG. 10. Test between the ages of 2 and 6 years if no documented lead level at or after 24 months. Test at any age when indicated by risk assessment or if lead risk changes. See Lead HAG. 11. Urine Dipstick or Urinalysis only when clinically indicated. See Urinalysis HAG. 12. Tuberculosis risk factor screen at each visit. TST when indicated. See TB HAG. 13. STI testing when risk identified by history/physical. See STI HAG. 14. Provide immunizations as recommended by the Advisory Committee on Immunization Practices (ACIP). 201 California Department of Health Care Services, Systems of Care Division, Children's Medical Services 50

51 American Academy Pediatrics Periodicity Schedule INFANCY AGE 1 Prenatal 2 Newborn d 4 By 1 mo 2 mo 4 mo 6 mo 9 mo HISTORY Initial/Interval MEASUREMENTS Length/Height and Weight Head Circumference Weight for Length Body Mass Index 5 Blood Pressure 6 SENSORY SCREENING DEVELOPMENTAL/BEHAVIORAL ASSESSMENT Vision Hearing 8 Developmental Screening 9 Autism Screening 10 Developmental Surveillance Psychosocial/Behavioral Assessment Alcohol and Drug Use Assessment 11 Depression Screening 12 PHYSICAL EXAMINATION 13 PROCEDURES 14 Newborn Blood Screening 15 Critical Congenital Heart Defect Screening 16 Immunization 17 Hematocrit or Hemoglobin 18 Lead Screening 19 or 20 or 20 Tuberculosis Testing 21 Dyslipidemia Screening 22 STI/HIV Screening 23 Cervical Dysplasia Screening 24 ORAL HEALTH 25 or or or o ANTICIPATORY GUIDANCE 1. If a child comes under care for the first time at any point on the schedule, or if any items are not accomplished at the suggested age, the schedule 11. A recommended screening tool is available at 51

52 Integra-on between SBC and SBOHC CHDP School Based Health Clinic Provides Early Periodic Screening services School Based Oral Health Clinic Provides Diagnos-c and Treatment services Temporarily enrolled into benefits Cross Referral System Medicaid Enrolled into benefits Health Insurance Navigators 52



53 Presence of a quality dashboard Community Collabora-ve Prac-ce Model Mul-- Site Model Presence of a solid business plan Suppor-ve State Medicaid Policies Sustainable School- based Oral Health Model Comprehensive on- site care Suppor-ve School Oral Health Policies Mul-disciplinary Teams Portable Clinic Model 53
54 Conclusion Expand preven-ve services to comprehensive primary care Evolve public health screening and preven-on programs to becoming true healthcare access sites in schools where children are located Expand collabora-on and coordina-on of school- based programs and providers U-lize Medicaid and other third party payment for sustainability of services U-lize Medicaid administra-ve ac-vi-es for outreach, enrollment and educa-on of families Monitor program services regularly for PI
55 Considera-ons for Policy Makers Mandate public policies that support integrated healthcare in school- based sites e.g. kindergarten oral health screenings, coordinate efforts with 6 th graders Tdap (whooping cough) immuniza-ons Develop a business plan & metrics u-lizing Plan, Do, Study, Act Measure procedures performed, staff -me, reimbursements collected Create a dashboard 55
56 References 1. American Academy of Pediatrics Periodicity Schedule Bright Futures, California Department of Health Care Services, Systems of Care Division, Children's Medical Services, CHDP Periodicity Schedule for Health Assessment Requirements By Age Groups, January Dental Health Founda-on. Mommy, It Hurts to Chew. Oakland, CA: Dental Health Founda-on, Sustaining School- Based Oral Health Care: Challenges and Opportuni-es of Much Needed Service NNOHA Winter 2014 Quarterly Newsle`er, Barzaga, Conrado, MD. 56
57 Acknowledgements This project is/was supported by the Health Resources and Services Administra-on (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number and -tle for grant amount (specify grant number, -tle, total award amount and percentage financed with nongovernmental sources). This informa-on or content and conclusions are those of the author and should not be construed as the official posi-on or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government. Addi-onal funding provided by First 5 Los Angeles and the DentaQuest Founda-on. Special thanks to Mary Foley, Dr. Timothy Mar-nez, Theresa Anselmo, Los Angeles Unified School District, LA Trust, and Western University College of Dental Medicine. 57
 and communicable disease programs.")
58 Contact Informa-on Jennifer Pilapil, is the Opera-ons Manager at the Center for Oral Health. Jennifer started her career in public health 20 years ago working in health educa-on and project coordina-on for a variety of MCH (Maternal, Child, and Health) and communicable disease programs. She was formerly a trainer and LAUSD School Outreach Coordinator for the Healthy Families program when outreach efforts were being conducted State- wide by RHA. During this -me, she provided health insurance outreach and technical assistance for Healthy Families and Medi- Cal insurance enrollment in the southern region of California and was on the California School Health Connec-ons School Outreach Advisory Board. She worked with community based agencies, school districts, and Los Angeles County Department of Public Social Services and Department of Public Health helping coordinate efforts in their We ve Got You Covered campaign and collabora-vely crea-ng the Los Angeles Unified School District s Children s Health Access and Medi- Cal Program (CHAMP). By 2001, she moved to the Pasadena Public Health Department to administer Medi- Cal programs, and later became the Deputy Director for the Child Health and Disability Preven-on (CHDP) program at the Pasadena Public Health Department. She administra-vely oversaw the child health clinic, tuberculosis, comprehensive perinatal services program, and Medi- Cal programs. She co- chaired the Health Access Task Force and served on the Los Angeles County Service Planning Area (SPA) 3 Access to Care Commi`ee. Jennifer graduated from the University of California, Irvine, with a BA in Social Sciences and completed post baccalaureate studies in GIS. Center for Oral Health, 309 E. 2 nd Street, Pomona, CA Phone: (909) jpilapil@tc4oh.org 58
59 MSDA Medicaid CHIP State Dental Association 2015 Na(onal Medicaid and CHIP Oral Health Symposium Session # 8 Pa(ent Centered Integrated Healthcare Emerging Models of Service Delivery and Payment John Snyder, DMD Washington Marrio: Wardman Park Monday, June 1 st,
60 Learning Objec-ve(s) Par-cipants will gain knowledge in: Kaiser Permanente Integrated Model Key Enablers for Integrated Care Current Challenges for Integra-on 60
61 Disclosure and Conflict of Interest Declara-on q I declare that neither I nor any member of my family have a financial arrangement or affilia-on with any corporate organiza-on offering financial support or grant monies for this con-nuing dental educa-on program, nor do I have a financial interest in any commercial product(s) or service(s) I will discuss in the presenta-on. q I declare that I have a financial interest/arrangement or affilia-on with the corporate organiza-on offering financial support or grant monies for this con-nuing dental educa-on program, or I do have a financial interest in any commercial product(s) or service(s) I will discuss in the presenta-on. 61



 Memorandum of")

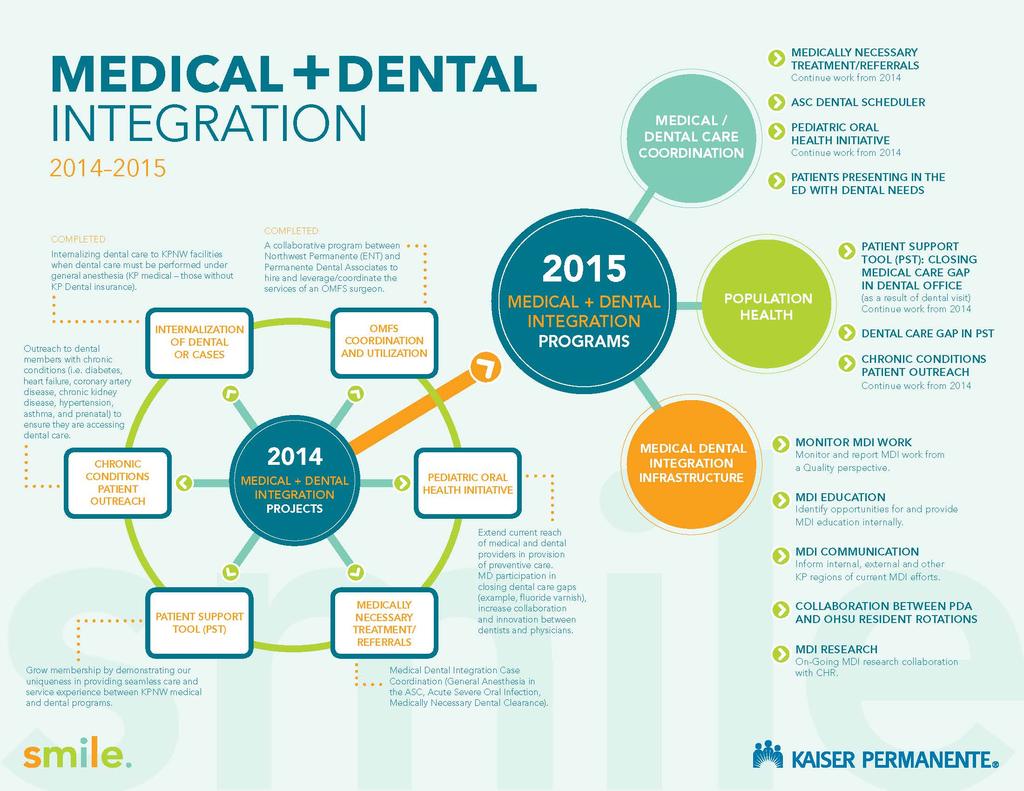
62 PDA Rela-onship with Kaiser Kaiser FoundaCon Health Plan, Inc. KAISER PERMANENTE DENTAL CARE PROGRAM Permanente Dental Associates, P.C. Dental Service Agreement (DSA) Memorandum of Understanding (MOU) - Annual Contract Global Payment Copyright 2015 Permanente Dental Associates, PC
63 KP Membership / Permanente Physician Groups 7 autonomous KP regions (Colorado, Hawaii, Georgia, Mid- Atlan-c, Northern California, Southern California, and Pacific NW (OR & WA) Nearly 10 Million medical members across all 7 Regions 7 autonomous Permanente physician groups 1 autonomous Permanente Dental group (Pacific NW) 236,000 Dental members and 502,000 Medical members in the NW region 90% Dental members also have KP Medical coverage






64 Cowlitz 5 N Longview Skamania Columbia 30 Clark Vancouver 26 Washington Portland Multnomah Clackamas Vancouver Yamhill Salem Polk Hillsboro Portland Beaverton 217 Tigard Tualatin 5 Milwaukie 205 Oregon City KAISER PERMANENTE DENTAL + MEDICAL FACILITIES
65 PDA Den-sts ASSOCIATES 37 SHAREHOLDERS SPECIAL CONTRACT AVERAGE TENURE *Ave Tenure > 1 Yr w PDA YEARS *11 YEARS
66 Evidence- Based Den-stry Philosophy An approach to oral health care that requires the judicious integra-on of systema-c assessments of clinically relevant scien-fic evidence, rela-ng to the pa-ent's oral and medical condi-on and history, with the den-st's clinical exper-se and the pa-ent's treatment needs and preferences. *ADA ADA Policy- - DefiniCon of Oral Health Oral health is a func-onal, structural, aesthe-c, physiologic and psychosocial state of well- being and is essen-al to an individual s general health and quality of life. *2014 ADA House of Delegates
 snapshot view of EMR")

67 Integrated Technology & Human Resources Epic (HealthConnect) snapshot view of EMR Pa-ent Support Tool: iden-fied care gaps Shared Human Resources: Tobacco Cessa-on Counselors
68
69 Diabetes Outreach Project- Comparison PopulaCon Health Outreach Calls Pilot Comparison of Interven-on Group and Usual Group Data ran on 10/27/14 Cascade Park Interven-on Group Salmon Creek Usual Group Difference between Interven-on Group and Usual Group Star-ng number in group - As of 4/1/ Number in group as of 9/15/ Number that lost coverage % % 0.9% Number that were seen, but programming unable to determine new OHS 4 0.8% 0 0.0% 0.8% Number that had either had or scheduled an exam appointment as of 10/27/ % % 17.1% - Number that had an exam appointment % % 16.4% - Number that had scheduled an exam appointment % % 0.7% Improved OHS % % 15.6% - Improved to OHS % 1 0.2% 1.7% - Improved to OHS % % 6.2% - Improved to OHS % % 7.7%
70 HEALTH OUTCOMES Diabe-c popula-on receiving dental care have lower costs per member per month (PMPM) than those NOT receiving dental care; axer adjus-ng for pa-ent characteris-cs. Overall costs: Inpatient costs: ED-Urgent care costs Diabetic population receiving dental care had $129 PMPM lower costs overall than those NOT receiving dental care Diabetic population receiving dental care had $101 PMPM lower inpatient costs than those NOT receiving dental care Diabetic population receiving dental care had $13 PMPM lower ED/ urgent costs than those NOT receiving dental care
71 Prac-ce of Choice for Den-sts and Care Teams DENTIST COMPENSATION
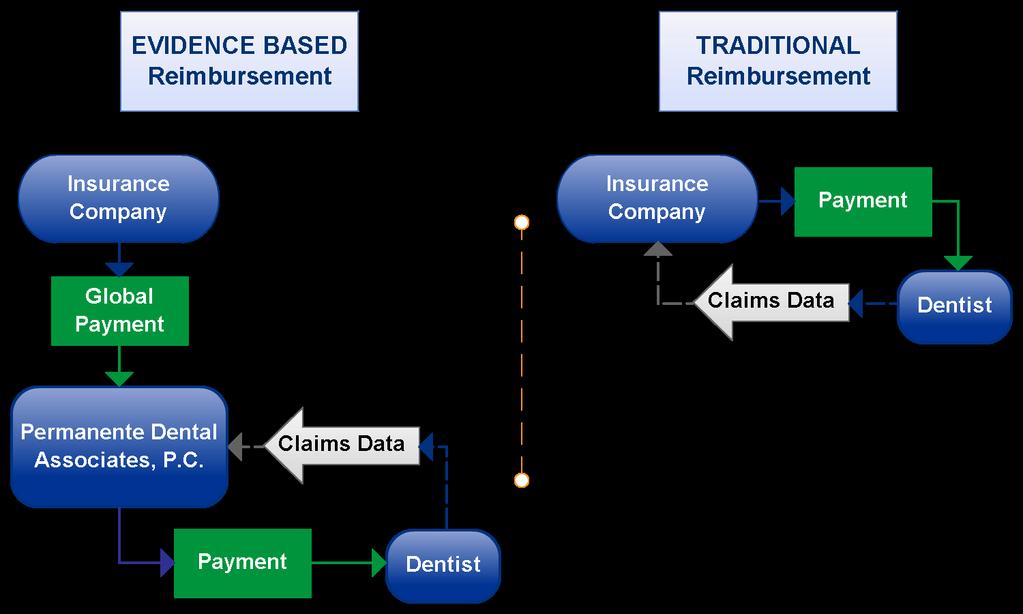
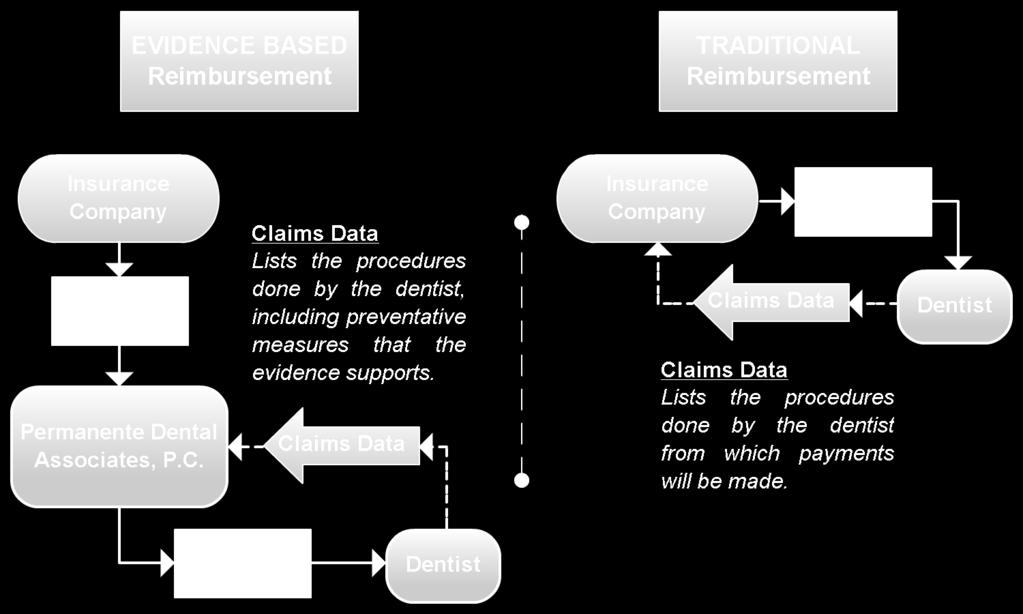
72 PDA Reimbursement vs. Tradi-onal Reimbursement
73 How the Measures for Reimbursement are Structured Pay for den-sts is structured according to performance incen-ves. The total pay is derived from three methods of reimbursement: 55%: Fixed salary 25%: Individual performance 20%: Dental office performance
 % of eligible pa-ents receiving PST")
74 Variable Base Compensa-on (VBC): General Den-sts TOTAL HEALTH SOLUTION % of Den-sts using Pa-ent Support Tool (PST) % of eligible pa-ents receiving PST sheet
75 Summary: Cri-cal Enablers Shared Total Health Philosophy Shared Popula-on (Medical and Dental) Co- located Facili-es Shared Informa-c Pla orm Global Payment

76 Contact Informa-on John J. Snyder, DMD Completed his dental educa-on at Oregon Health & Science University School of Den-stry General Prac-ce Residency at Har ord Hospital in Connec-cut Joined Permanente Dental Associates (PDA) in 1987 Elected Dental Director in 2008 Remains a strong advocate for evidence- based dental prac-ce, oral health research, and medical- dental integra-on and has enjoyed numerous na-onal and interna-onal speaking opportuni-es to share his passion for expanding total health and wellness. John.J.Snyder@kp.org PDA- Dental.com 76
A review of medical consent requirements and the Georgia Families 360 program required timelines for services and assessment
 A review of medical consent requirements and the Georgia Families 360 program required timelines for services and assessment Amber Hammontree, LPC Clinical Trainer Georgia Families 360 GAPEC-1203-16 March
A review of medical consent requirements and the Georgia Families 360 program required timelines for services and assessment Amber Hammontree, LPC Clinical Trainer Georgia Families 360 GAPEC-1203-16 March
IA Health Link and Amerigroup Iowa
 IA Health Link and Amerigroup Iowa Navigating the Transition to Amerigroup Foster Care Caretaker Orientation 1 Who is Amerigroup Iowa? A partner with the Iowa Department of Human Services (DHS), which
IA Health Link and Amerigroup Iowa Navigating the Transition to Amerigroup Foster Care Caretaker Orientation 1 Who is Amerigroup Iowa? A partner with the Iowa Department of Human Services (DHS), which
Training Workers with Disabilities Grant Program Announcement (GPA)
") BLUEPRINT FOR PROSPERITY JUNE 2014 Training Workers with Disabilities Grant Program Announcement (GPA) Grants of $5,000 to $100,000 Applications must be submitted no later than 11:59 p.m. on September
BLUEPRINT FOR PROSPERITY JUNE 2014 Training Workers with Disabilities Grant Program Announcement (GPA) Grants of $5,000 to $100,000 Applications must be submitted no later than 11:59 p.m. on September
An Innovative Journey: A Nurse Managed Health Clinic Serving the Vulnerable Population Lisa Bursch, DNP, APRN, CPNP
 An Innovative Journey: A Nurse Managed Health Clinic Serving the Vulnerable Population Lisa Bursch, DNP, APRN, CPNP California California Popula-on 38,802,506 Riverside County Popula-on 2,329,271 California
An Innovative Journey: A Nurse Managed Health Clinic Serving the Vulnerable Population Lisa Bursch, DNP, APRN, CPNP California California Popula-on 38,802,506 Riverside County Popula-on 2,329,271 California
Data Quality Improvement Plan
 Data Quality Improvement Plan Goal This interac ve document is for Clinical Health Informa on Technology Advisors (CHITAs) to work with a prac ce to ins tute sustainable quality improvement. The Data Quality
Data Quality Improvement Plan Goal This interac ve document is for Clinical Health Informa on Technology Advisors (CHITAs) to work with a prac ce to ins tute sustainable quality improvement. The Data Quality
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Florida FLORIDA (FL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Florida FLORIDA (FL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
HEALTH PROFESSIONS DEPARTMENT Physician Assistant Studies
 This form can also be completed online at: http://tinyurl.com/y8d9lj9x Date: To: From: Subject: (Preceptor) (Site Name) Troy K. Bender, Northeastern State University Physician Assistant Program Required
This form can also be completed online at: http://tinyurl.com/y8d9lj9x Date: To: From: Subject: (Preceptor) (Site Name) Troy K. Bender, Northeastern State University Physician Assistant Program Required
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Alabama ALABAMA (AL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Alabama ALABAMA (AL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Alaska ALASKA (AK) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Alaska ALASKA (AK) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment
 Early and Periodic Screening, Diagnosis and Treatment 1 Healthchek Ohio Medicaid EPSDT Services Early Periodic Screening Diagnosis Treatment Identify problems early, starting at birth Check children s
Early and Periodic Screening, Diagnosis and Treatment 1 Healthchek Ohio Medicaid EPSDT Services Early Periodic Screening Diagnosis Treatment Identify problems early, starting at birth Check children s
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Wisconsin WISCONSIN (WI) Medicaid s EPSDT benefit provides comprehensive health care services to children under age
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Wisconsin WISCONSIN (WI) Medicaid s EPSDT benefit provides comprehensive health care services to children under age
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Oregon OREGON (OR) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Oregon OREGON (OR) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Park Nicollet Midwife Dept Telephonic Breastfeeding and Postpartum Support Pilot Project
 1/26/17 Project Leaders: Jennifer Bourgoine, RN, BSN Ivy Emery, RN, BSN, PHN Kate Johnson, RN, MN, PHN, DNP Student Park Nicollet Midwife Dept Telephonic Breastfeeding and Postpartum Support Pilot Project
1/26/17 Project Leaders: Jennifer Bourgoine, RN, BSN Ivy Emery, RN, BSN, PHN Kate Johnson, RN, MN, PHN, DNP Student Park Nicollet Midwife Dept Telephonic Breastfeeding and Postpartum Support Pilot Project
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Virginia VIRGINIA (VA) Medicaid s EPSDT benefit provides comprehensive health care services to children under age
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Virginia VIRGINIA (VA) Medicaid s EPSDT benefit provides comprehensive health care services to children under age
AGENDA Thursday, October 12, :00 a.m. to 9:00 a.m. Breakfast/Registra on/vendors 9:00 a.m. to 9:15 a.m. Opening Remarks/Bureau Update 9:15 a.m.
 2017 Annual Leadership Conference Collabora ve Problem Solving with Challenging Students with Ross W. Greene, Ph.D School Threat /Risk Assessment with Eric Frazer, Psy. D October 12-13, 2017 Har ord/farmington
2017 Annual Leadership Conference Collabora ve Problem Solving with Challenging Students with Ross W. Greene, Ph.D School Threat /Risk Assessment with Eric Frazer, Psy. D October 12-13, 2017 Har ord/farmington
WORKER TRAINING GRANTS for WISCONSIN HEALTH SCIENCE, HEALTH CARE, AND RELATED OCCUPATIONS
 MAY 2015 WORKER TRAINING GRANTS for WISCONSIN HEALTH SCIENCE, HEALTH CARE, AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: August 20, 2015 @ 11:59
MAY 2015 WORKER TRAINING GRANTS for WISCONSIN HEALTH SCIENCE, HEALTH CARE, AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: August 20, 2015 @ 11:59
WORKER TRAINING GRANTS for WISCONSIN HEALTH CARE AND RELATED OCCUPATIONS
 JULY 2014 WORKER TRAINING GRANTS for WISCONSIN HEALTH CARE AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: October 21, 2014 Grant Program Announcement
JULY 2014 WORKER TRAINING GRANTS for WISCONSIN HEALTH CARE AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: October 21, 2014 Grant Program Announcement
2014 ANNUAL REPORT. Improving Health and Achieving Excellence
 2014 ANNUAL REPORT Improving Health and Achieving Excellence Serving ALL residents of Henry County 1843 Oakwood Avenue Napoleon, Ohio 43545 (419) 599-5545 Office Hours: Monday - Friday, 8:30 AM - 4:30
2014 ANNUAL REPORT Improving Health and Achieving Excellence Serving ALL residents of Henry County 1843 Oakwood Avenue Napoleon, Ohio 43545 (419) 599-5545 Office Hours: Monday - Friday, 8:30 AM - 4:30
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Indiana INDIANA (IN) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Indiana INDIANA (IN) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
MASTER S PROGRAMME: HEALTH SYSTEMS RESEARCH AND MANAGEMENT
 MASTER S PROGRAMME: HEALTH SYSTEMS RESEARCH AND MANAGEMENT Welcome Message You are warmly welcome to the Kwame Nkrumah University of Science and Technology (KNUST)! The KNUST-School of Public Health exists
MASTER S PROGRAMME: HEALTH SYSTEMS RESEARCH AND MANAGEMENT Welcome Message You are warmly welcome to the Kwame Nkrumah University of Science and Technology (KNUST)! The KNUST-School of Public Health exists
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Mississippi MISSISSIPPI (MS) Medicaid s EPSDT benefit provides comprehensive health care services to children under
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Mississippi MISSISSIPPI (MS) Medicaid s EPSDT benefit provides comprehensive health care services to children under
WORKER TRAINING GRANTS for WISCONSIN CONSTRUCTION TRADES AND RELATED OCCUPATIONS
 JULY 2014 WORKER TRAINING GRANTS for WISCONSIN CONSTRUCTION TRADES AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: September 30, 2014 Grant Program
JULY 2014 WORKER TRAINING GRANTS for WISCONSIN CONSTRUCTION TRADES AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: September 30, 2014 Grant Program
WORKER TRAINING GRANTS for WISCONSIN ARCHITECTURE, CONSTRUCTION, AND RELATED OCCUPATIONS
 MAY 2015 WORKER TRAINING GRANTS for WISCONSIN ARCHITECTURE, CONSTRUCTION, AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: November 19, 2015 @11:59
MAY 2015 WORKER TRAINING GRANTS for WISCONSIN ARCHITECTURE, CONSTRUCTION, AND RELATED OCCUPATIONS Award Amount: $5,000 to $400,000 Applications must be submitted no later than: November 19, 2015 @11:59
Documentation of Early and Periodic Screening, Diagnosis, and Treatment (HealthWatch) Screening Exams. Overview
 Screening Exams. Overview") P R O V I D E R B U L L E T I N B T 2 0 0 0 3 5 N O V E M B E R 1, 2 0 0 0 To: Subject: All Indiana Health Coverage Programs Acute Care Hospitals, Federally Qualified Health Clinics, Rural Health Clinics,
P R O V I D E R B U L L E T I N B T 2 0 0 0 3 5 N O V E M B E R 1, 2 0 0 0 To: Subject: All Indiana Health Coverage Programs Acute Care Hospitals, Federally Qualified Health Clinics, Rural Health Clinics,
FFA Career Development Event: Telling the Beef Story Contest Toolkit
 The Beef Checkoff presents: FFA Career Development Event: Telling the Beef Story Contest Toolkit Resources and tools to engage in the growth and development of the beef ca le community. Revision date:
The Beef Checkoff presents: FFA Career Development Event: Telling the Beef Story Contest Toolkit Resources and tools to engage in the growth and development of the beef ca le community. Revision date:
Roles and Responsibili-es of ICU Nurses in End-of-Life Decisions Making. Cheryl Carter Durban
 Roles and Responsibili-es of ICU Nurses in End-of-Life Decisions Making Cheryl Carter Durban Context -Distribu-on of beds Majority of beds 86% Limpopo < 100 beds North West Gauteng Mpumalanga Northern
Roles and Responsibili-es of ICU Nurses in End-of-Life Decisions Making Cheryl Carter Durban Context -Distribu-on of beds Majority of beds 86% Limpopo < 100 beds North West Gauteng Mpumalanga Northern
January What You Should Do. Background
 in the news Nonprofit Organizations January 2015 IRS Issues Long Awaited Final Regula ons for Charitable Hospitals In this Issue: What You Should Do Background... 1 Final Regula ons Hospital Facili es
in the news Nonprofit Organizations January 2015 IRS Issues Long Awaited Final Regula ons for Charitable Hospitals In this Issue: What You Should Do Background... 1 Final Regula ons Hospital Facili es
SYNCORP Clincare Technologies (P) Ltd.
 Ltd.") SYNCORP Clincare Technologies (P) Ltd. India Office: Corporate Office: Novel Business Centre No. 10, 100 Feet Ring Road, BTM Layout 1st Stage. Bangalore - 560 068 (INDIA) Tel: 91-080-65474772 / 91-080-50072226
SYNCORP Clincare Technologies (P) Ltd. India Office: Corporate Office: Novel Business Centre No. 10, 100 Feet Ring Road, BTM Layout 1st Stage. Bangalore - 560 068 (INDIA) Tel: 91-080-65474772 / 91-080-50072226
Pediatric Update NEW PEDIATRIC PREVENTION GUIDELINES ADOPTED INFANTS WILL HAVE AN EXTRA VISIT AND MORE FLEXIBLE TIMING OF EXAMS
 Contra Costa Health Plan Winter 2004/2005 Contra Costa Regional Medical Center Department of Pediatrics NEW PEDIATRIC PREVENTION GUIDELINES ADOPTED Contra Costa Health Plan (CCHP) and Contra Costa Regional
Contra Costa Health Plan Winter 2004/2005 Contra Costa Regional Medical Center Department of Pediatrics NEW PEDIATRIC PREVENTION GUIDELINES ADOPTED Contra Costa Health Plan (CCHP) and Contra Costa Regional
Medical Officer Welcome Packet
 Washington State Hospital Association Medical Officer Welcome Packet A collabora ve publica on of the Washington State Hospital Associa on and the Washington State Medical Associa on Electronic Updates!
Washington State Hospital Association Medical Officer Welcome Packet A collabora ve publica on of the Washington State Hospital Associa on and the Washington State Medical Associa on Electronic Updates!
STANDARDS OF CARE HIV AMBULATORY OUTPATIENT MEDICAL CARE STANDARDS I. DEFINITION OF SERVICES
 S OF CARE Oakland Transitional Grant Area Care and Treatment Services J ANUARY 2007 Office of AIDS Administration 1000 Broadway, Suite 310 Oakland, CA 94612 Tel: 510. 268.7630 Fax: 510.268-7631 AREAS OF
S OF CARE Oakland Transitional Grant Area Care and Treatment Services J ANUARY 2007 Office of AIDS Administration 1000 Broadway, Suite 310 Oakland, CA 94612 Tel: 510. 268.7630 Fax: 510.268-7631 AREAS OF
Gold Coast Primary Health Network STRATEGIC PLAN
 Gold Coast Primary Health Network Building one world class health system for the Gold Coast Table of Contents Se ng our Strategic Direc ons 1 Na onal Context 1 Local Context 2 The Gold Coast Primary Health
Gold Coast Primary Health Network Building one world class health system for the Gold Coast Table of Contents Se ng our Strategic Direc ons 1 Na onal Context 1 Local Context 2 The Gold Coast Primary Health
17 th Annual Occupational Health Symposium 2015 Total Worker Health
 17 th Annual Occupational Health Symposium 2015 April 16 17, 2015 Cedar Rapids, Iowa The Hotel at Kirkwood Jointly provided by: The University of Iowa s College of Public Health s Healthier Workforce Center
17 th Annual Occupational Health Symposium 2015 April 16 17, 2015 Cedar Rapids, Iowa The Hotel at Kirkwood Jointly provided by: The University of Iowa s College of Public Health s Healthier Workforce Center
Substantive Change Report by Quality Assurance Agency for Higher Education, UK (QAA)
") Substantive Change Report by Quality Assurance Agency for Higher Education, UK (QAA) Register Committee Decision of: 16/11/2017 Report received on: 13/07/2017 Agency registered since: 23/10/2017 Last external
Substantive Change Report by Quality Assurance Agency for Higher Education, UK (QAA) Register Committee Decision of: 16/11/2017 Report received on: 13/07/2017 Agency registered since: 23/10/2017 Last external
California Community Health Centers
 California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Absolute Total Care. Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program Description 2016
 Program Description 2016") Absolute Total Care Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program Description 2016 TABLE OF CONTENTS INTRODUCTION: --------------------------------------------------------------
Absolute Total Care Early and Periodic Screening, Diagnostic and Treatment (EPSDT) Program Description 2016 TABLE OF CONTENTS INTRODUCTION: --------------------------------------------------------------
Date: Illinois Health Connect PCP 6/23/14 Page 1 of 8. Signature:
 Illinois Department of Healthcare and Family Services Illinois Health Connect Primary Care Provider Agreement This Agreement pertains only to the relationship between the Illinois Department of Healthcare
Illinois Department of Healthcare and Family Services Illinois Health Connect Primary Care Provider Agreement This Agreement pertains only to the relationship between the Illinois Department of Healthcare
MPAH Newsletter. one of the ways in which knowledge and lessons learned will be produced and disseminated
 MAPUTALAND-PONDOLAND-ALBANY HOTSPOT MPAH Newsletter Issue 1 Autumn 2013 Welcome to the first newsle er of the Maputaland Pondoland Albany Hotspot (MPAH) learning network! This quarterly newsle er will
MAPUTALAND-PONDOLAND-ALBANY HOTSPOT MPAH Newsletter Issue 1 Autumn 2013 Welcome to the first newsle er of the Maputaland Pondoland Albany Hotspot (MPAH) learning network! This quarterly newsle er will
The Affordable Care Act and Its Potential to Reduce Health Disparities Cara V. James, Ph.D.
 The Affordable Care Act and Its Potential to Reduce Health Disparities Cara V. James, Ph.D. Director, Office of Minority Health Centers for Medicare & Medicaid Services April 22, 2013 The Affordable Care
The Affordable Care Act and Its Potential to Reduce Health Disparities Cara V. James, Ph.D. Director, Office of Minority Health Centers for Medicare & Medicaid Services April 22, 2013 The Affordable Care
Welcome Providers. Thursday, November 11, Page 1
 Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
National Fire Academy Emmitsburg, MD. Sponsored in part through the generosity of Globe Manufacturing Company, LLC
 National Fire Academy Emmitsburg, MD Sponsored in part through the generosity of Globe Manufacturing Company, LLC THREE STATE 2015 Course Offerings Course Name: Poli cs and the White Helmet Course Code:
National Fire Academy Emmitsburg, MD Sponsored in part through the generosity of Globe Manufacturing Company, LLC THREE STATE 2015 Course Offerings Course Name: Poli cs and the White Helmet Course Code:
Maternal and Child Health Oregon Health Authority, Public Health Division. Portland, Oregon. Assignment Description
 Maternal and Child Health Oregon Health Authority, Public Health Division Portland, Oregon Assignment Description Overview of the Fellow's assignment including description of fellow's placement in division
Maternal and Child Health Oregon Health Authority, Public Health Division Portland, Oregon Assignment Description Overview of the Fellow's assignment including description of fellow's placement in division
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Model Application. Funeral Service. For. Presented By:
 Model Application For Funeral Service Presented By: Model Application 2016 I The Interna onal Conference of Funeral Service Examining Boards is pleased to introduce The Conference Model Applica on. Recognizing
Model Application For Funeral Service Presented By: Model Application 2016 I The Interna onal Conference of Funeral Service Examining Boards is pleased to introduce The Conference Model Applica on. Recognizing
State Breas)eeding Coali1ons Webinar 2/8/2016 CHAMPS. Communi-es and Hospitals Advancing Maternity Prac-ces. CHAMPS Background
eeding Coali1ons Webinar 2/8/2016 CHAMPS. Communi-es and Hospitals Advancing Maternity Prac-ces. CHAMPS Background") CHAMPS Communi-es and Hospitals Advancing Maternity Prac-ces Reducing Dispari/es in Maternity Care and Breas5eeding 1 CHAMPS Background Funded by a grant from the W. K. Kellogg Foundation 3- year grant
CHAMPS Communi-es and Hospitals Advancing Maternity Prac-ces Reducing Dispari/es in Maternity Care and Breas5eeding 1 CHAMPS Background Funded by a grant from the W. K. Kellogg Foundation 3- year grant
CROSS BORDER COOPERATION PROGRAMME POLAND BELARUS UKRAINE NEWSLETTER
 CROSS BORDER COOPERATION PROGRAMME POLAND BELARUS UKRAINE 2007 2013 NEWSLETTER NO.1 JANUARY, 2010 CONTENT Welcome Programme events history Development of the Programme and its approval by the European
CROSS BORDER COOPERATION PROGRAMME POLAND BELARUS UKRAINE 2007 2013 NEWSLETTER NO.1 JANUARY, 2010 CONTENT Welcome Programme events history Development of the Programme and its approval by the European
A guide to Kaiser On-the-Job
 A guide to Kaiser On-the-Job Work as medical treatment Modified duty is an important part of your employee s medical treatment. For most sick or injured workers, the best way to recover is to return to
A guide to Kaiser On-the-Job Work as medical treatment Modified duty is an important part of your employee s medical treatment. For most sick or injured workers, the best way to recover is to return to
I can choose my doctor
 Kaiser Permanente Enrollment Book Oregon / Washington test results online excellent prenatal care I can choose my doctor a wide range of specialists All plans offered and underwritten by Kaiser Foundation
Kaiser Permanente Enrollment Book Oregon / Washington test results online excellent prenatal care I can choose my doctor a wide range of specialists All plans offered and underwritten by Kaiser Foundation
Tune-Up Your Check Up, Mississippi! Jonathan Shook, MD, FAAP April 21, 2017
 Tune-Up Your Check Up, Mississippi! Jonathan Shook, MD, FAAP April 21, 2017 Tune-Up Your Check Up, Mississippi! Topics in Well Child Care, Coding, Documentation, and Payment. Jonathan Shook, MD, FAAP April
Tune-Up Your Check Up, Mississippi! Jonathan Shook, MD, FAAP April 21, 2017 Tune-Up Your Check Up, Mississippi! Topics in Well Child Care, Coding, Documentation, and Payment. Jonathan Shook, MD, FAAP April
San ago Canyon College Freshman Scholarships
 1 San ago Canyon College (SCC) Freshman Scholarships are awarded to recognize academic and specialized achievement among incoming college Freshmen a ending SCC in Fall 2017 and Spring 2018 semesters. To
1 San ago Canyon College (SCC) Freshman Scholarships are awarded to recognize academic and specialized achievement among incoming college Freshmen a ending SCC in Fall 2017 and Spring 2018 semesters. To
Imperial Clinical Research Facility User Guidelines
 Imperial Clinical Research Facility User Guidelines Imperial CRF Users Guidelines The NIHR/Wellcome Trust Imperial CRF is a mul user facility for clinical research involving both pa ents and healthy volunteers.
Imperial Clinical Research Facility User Guidelines Imperial CRF Users Guidelines The NIHR/Wellcome Trust Imperial CRF is a mul user facility for clinical research involving both pa ents and healthy volunteers.
GhanaVeg. Commercial Vegetable Sector Development in Ghana. Fund Manual for the: Business Opportunity Fund & R&D Innova on Fund
 GhanaVeg Commercial Vegetable Sector Development in Ghana Fund Manual for the: Business Opportunity Fund & R&D Innova on Fund GhanaVeg, February 2015 Edi on : 2 TABLE OF CONTENT LIST OF ACRONYMS iii 1
GhanaVeg Commercial Vegetable Sector Development in Ghana Fund Manual for the: Business Opportunity Fund & R&D Innova on Fund GhanaVeg, February 2015 Edi on : 2 TABLE OF CONTENT LIST OF ACRONYMS iii 1
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Gilliam County Community Advisory Council Community Health Improvement Plan OVERARCHING PRIORITY ISSUE AREAS
 Gilliam County Community Advisory Council Community Health Improvement Plan OVERARCHING PRIORITY ISSUE AREAS THERE WERE FOUR AREAS THAT WERE PRIORITIZED THROUGH THE COMMUNITY HEALTH ASSESSMENT PROCESS:
Gilliam County Community Advisory Council Community Health Improvement Plan OVERARCHING PRIORITY ISSUE AREAS THERE WERE FOUR AREAS THAT WERE PRIORITIZED THROUGH THE COMMUNITY HEALTH ASSESSMENT PROCESS:
Preventive Health Guidelines
 Preventive Health Guidelines Section N-1 Overview The objective of Molina Healthcare of New Mexico, Inc. (Molina Healthcare) is the delivery of a core package of clinical preventive health services that
Preventive Health Guidelines Section N-1 Overview The objective of Molina Healthcare of New Mexico, Inc. (Molina Healthcare) is the delivery of a core package of clinical preventive health services that
Bright Futures: An Essential Resource for Advancing the Title V National Performance Measures
 A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES
 SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES Compiled by the Strengthen the Evidence for Maternal and Child Health Programs Initiative: Strengthen the Evidence is a collaborative
SAMPLE STRATEGIES AND EVIDENCE-BASED OR -INFORMED STRATEGY MEASURES Compiled by the Strengthen the Evidence for Maternal and Child Health Programs Initiative: Strengthen the Evidence is a collaborative
Gynecology Exam. Rehearsal Guide... preparing women with intellectual and developmental disabili es (I/DD) to successfully complete a gynecology exam
 to successfully complete a gynecology exam") Gynecology Exam Rehearsal Guide... preparing women with intellectual and developmental disabili es (I/DD) to successfully complete a gynecology exam INTRODUCTION FOR CAREGIVERS A rehearsal guide contains
Gynecology Exam Rehearsal Guide... preparing women with intellectual and developmental disabili es (I/DD) to successfully complete a gynecology exam INTRODUCTION FOR CAREGIVERS A rehearsal guide contains
Improving EPSDT screening for Amerigroup Iowa, Inc. members. Education for PCPs
 Improving EPSDT screening for Amerigroup Iowa, Inc. members Education for PCPs WEBPIA-0002-15 December 2015 What is EPSDT? Early and periodic screening, diagnosis and treatment (EPSDT) is Medicaid s comprehensive
Improving EPSDT screening for Amerigroup Iowa, Inc. members Education for PCPs WEBPIA-0002-15 December 2015 What is EPSDT? Early and periodic screening, diagnosis and treatment (EPSDT) is Medicaid s comprehensive
PUBLIC HEALTH. Mission Statement. Mandates. Expenditure Budget: 3.2% of Human Services
 Mission Statement Public Health will promote optimum health and the adoption of healthful lifestyles; assure access to vital statistics, health information, preventive health, environmental health and
Mission Statement Public Health will promote optimum health and the adoption of healthful lifestyles; assure access to vital statistics, health information, preventive health, environmental health and
Clinical Simula on Center. Pa ent Safety Starts Here 2016 Year in Review
 Clinical Simula on Center Pa ent Safety Starts Here 2016 Year in Review Our Mission The mission of the Penn State Hershey Clinical Simula on Center is to improve pa ent outcomes with effec ve programs
Clinical Simula on Center Pa ent Safety Starts Here 2016 Year in Review Our Mission The mission of the Penn State Hershey Clinical Simula on Center is to improve pa ent outcomes with effec ve programs
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
CAREGIVER RESOURCES. An Infopeople Webinar January 19, 2011 Presented by Kelli Ham
 CAREGIVER RESOURCES An Infopeople Webinar January 19, 2011 Presented by Kelli Ham Infopeople webinars are supported by the U.S. Institute of Museum and Library Services under the provisions of the Library
CAREGIVER RESOURCES An Infopeople Webinar January 19, 2011 Presented by Kelli Ham Infopeople webinars are supported by the U.S. Institute of Museum and Library Services under the provisions of the Library
Health and Safety Training for Schools Health and Safety Unit
 Health and Safety Training for Schools 2018-2019 Health and Safety Unit C O N T E N T S Why do you need health and safety training? 03 Health and Safety for Head Teachers and 06 Senior Leaders Managing
Health and Safety Training for Schools 2018-2019 Health and Safety Unit C O N T E N T S Why do you need health and safety training? 03 Health and Safety for Head Teachers and 06 Senior Leaders Managing
Health Care Transition for Youth with Special Health Care Needs (YSHCN)
") Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training
 Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training EPSDT Overview EPSDT purpose and requirements mandated by the Agency for Health Care Administration
Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training EPSDT Overview EPSDT purpose and requirements mandated by the Agency for Health Care Administration
Consumer-Centered Data and Strategies to Advance Evidence- Based Advocacy in Child Health
 Consumer-Centered Data and Strategies to Advance Evidence- Based Advocacy in Child Health Highlights from the Child and Adolescent Health Measurement Initiative Toolbox Christina Bethell, PhD, MBA, MPH
Consumer-Centered Data and Strategies to Advance Evidence- Based Advocacy in Child Health Highlights from the Child and Adolescent Health Measurement Initiative Toolbox Christina Bethell, PhD, MBA, MPH
The Health Center Program Quality Improvement
 The Health Center Program Quality Improvement National Network for Oral Health Access Annual Conference November 8, 2016 Vy Nguyen, DDS, MPH Dental Officer, Office of Quality Improvement Bureau of Primary
The Health Center Program Quality Improvement National Network for Oral Health Access Annual Conference November 8, 2016 Vy Nguyen, DDS, MPH Dental Officer, Office of Quality Improvement Bureau of Primary
Meaningful Use of an EHR System
 Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
PUBLIC HEALTH 264 HUMAN SERVICES. Mission Statement. Mandates. Expenditure Budget: $3,939, % of Human Services
 Mission Statement Public Health will promote optimum health and the adoption of healthful lifestyles; assure access to vital statistics, health information, preventive health, environmental health and
Mission Statement Public Health will promote optimum health and the adoption of healthful lifestyles; assure access to vital statistics, health information, preventive health, environmental health and
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Who should get admission to inpa-ent hospice/pallia-ve care beds?
 1 Ethics and Resource Allocation: How to Respect Human Dignity in the Making of Tough Choices Hospice & Pallia-ve Care Manitoba 19th Annual Provincial Conference Bashir Jiwani, PhD Ethicist & Director
1 Ethics and Resource Allocation: How to Respect Human Dignity in the Making of Tough Choices Hospice & Pallia-ve Care Manitoba 19th Annual Provincial Conference Bashir Jiwani, PhD Ethicist & Director
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Oregon's Health System Transformation
 Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
The Next Chapter in Kids Medicaid Coverage: Improving Care Delivery for Children and Leveraging the Medicaid Benefit for Children & Adolescents
 The Next Chapter in Kids Medicaid Coverage: Improving Care Delivery for Children and Leveraging the Medicaid Benefit for Children & Adolescents NAMD Fall Conference 2014 Claudia Schlosberg, JD Interim
The Next Chapter in Kids Medicaid Coverage: Improving Care Delivery for Children and Leveraging the Medicaid Benefit for Children & Adolescents NAMD Fall Conference 2014 Claudia Schlosberg, JD Interim
Nutrition and Prevention A Golden Opportunity: How Can MCH Practitioners Get Involved?
 Nutrition and Prevention A Golden Opportunity: How Can MCH Practitioners Get Involved? Nutrition Leadership Network Meeting Los Angeles March 4, 2016 What We ll Cover Learn about Nutrition-Related Clinical
Nutrition and Prevention A Golden Opportunity: How Can MCH Practitioners Get Involved? Nutrition Leadership Network Meeting Los Angeles March 4, 2016 What We ll Cover Learn about Nutrition-Related Clinical
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Sonoma State University Department of Nursing Family Nurse Practitioner Program
 1 Sonoma State University Department of Nursing Family Nurse Practitioner Program Pediatric Preceptor Packet N550ABC MEW 3/15 2 Department of Nursing 1801 East Cotati Avenue, Rohnert Park, California 94928-3609
1 Sonoma State University Department of Nursing Family Nurse Practitioner Program Pediatric Preceptor Packet N550ABC MEW 3/15 2 Department of Nursing 1801 East Cotati Avenue, Rohnert Park, California 94928-3609
Benefit Explanation And Limitations
 Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
A Message from The Of ice of Graduate Studies
 Spring 2016 Nursing Highlights : 2 Graduate Student Apprecia on Week: 3 Campus Town Updates: 4 MEd i Stem : 5 Con nuing Educa on Opportuni es : 5 Tradi ons: 6 A Message from The Of ice of Graduate Studies
Spring 2016 Nursing Highlights : 2 Graduate Student Apprecia on Week: 3 Campus Town Updates: 4 MEd i Stem : 5 Con nuing Educa on Opportuni es : 5 Tradi ons: 6 A Message from The Of ice of Graduate Studies
Improving Oral Health Outcomes for Children: Progress and Opportunities
 Improving Oral Health Outcomes for Children: Progress and Opportunities About Children Now Non-partisan research, policy development, communications, and advocacy organization working on all key kids issues,
Improving Oral Health Outcomes for Children: Progress and Opportunities About Children Now Non-partisan research, policy development, communications, and advocacy organization working on all key kids issues,
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Medi-Cal & Children. California Association of Health Plans. Kelly Hardy August 3, 2017
 Medi-Cal & Children California Association of Health Plans Kelly Hardy August 3, 2017 Overview 1) Enrollment; federal threats 2) Preventive care 3) Developmental screenings 4) Quality measurement 5) Consumer/family
Medi-Cal & Children California Association of Health Plans Kelly Hardy August 3, 2017 Overview 1) Enrollment; federal threats 2) Preventive care 3) Developmental screenings 4) Quality measurement 5) Consumer/family
Office of Sponsored Programs Newsletter
 IN THIS ISSUE >>> NSF Grants Conference Updates Cayuse Reporting UTIA Faculty Spotlights Compliance Corner University of Tennessee Ins tute of Agriculture Sponsored Programs Office 2018 January Office
IN THIS ISSUE >>> NSF Grants Conference Updates Cayuse Reporting UTIA Faculty Spotlights Compliance Corner University of Tennessee Ins tute of Agriculture Sponsored Programs Office 2018 January Office
2016 Social Service Funding Application Non-Alcohol Funds
 2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
Dell Children s Health Plan Texas Health Steps program provider presentation
 Dell Children s Health Plan Texas Health Steps program provider presentation TSPEC-0231-17 May 2017 Overview The Early and Periodic Screening, Diagnosis and Treatment (EPSDT) service is Medicaid s comprehensive
Dell Children s Health Plan Texas Health Steps program provider presentation TSPEC-0231-17 May 2017 Overview The Early and Periodic Screening, Diagnosis and Treatment (EPSDT) service is Medicaid s comprehensive
School-Based Health Centers and Health Care Reform November, 2013
 Background School-Based Health Centers and Health Care Reform November, 2013 Since they were first established in the 1980s, California s school-based health centers (SBHCs) have been growing in number.
Background School-Based Health Centers and Health Care Reform November, 2013 Since they were first established in the 1980s, California s school-based health centers (SBHCs) have been growing in number.
PROJECT IMPLEMENTATION MANUAL
 COMMUNITY WATER AND SANITATION AGENCY (CWSA) PROJECT IMPLEMENTATION MANUAL COMMUNITY WATER AND SANITATION AGENCY PRIVATE MAIL BAG KOTOKA INTERNATIONAL AIRPORT - ACCRA TEL: 0302-518401/518404/983104 FAX
COMMUNITY WATER AND SANITATION AGENCY (CWSA) PROJECT IMPLEMENTATION MANUAL COMMUNITY WATER AND SANITATION AGENCY PRIVATE MAIL BAG KOTOKA INTERNATIONAL AIRPORT - ACCRA TEL: 0302-518401/518404/983104 FAX
2017 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
GERRI L. MATTSON, MD, FAAP, MSPH Public Health Pediatrician
 GERRI L. MATTSON, MD, FAAP, MSPH Public Health Pediatrician PERSONAL Dr. Mattson has worked on program development and implementation in the NC Title V program in the NC Division of Public Health for 12
GERRI L. MATTSON, MD, FAAP, MSPH Public Health Pediatrician PERSONAL Dr. Mattson has worked on program development and implementation in the NC Title V program in the NC Division of Public Health for 12
Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19
 Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19 Coverage of Preventive Health Services (Sec. 2708) Stipulates that a group health plan and a health insurance issuer offering
Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19 Coverage of Preventive Health Services (Sec. 2708) Stipulates that a group health plan and a health insurance issuer offering
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
AETNA BETTER HEALTH OF VIRGINIA Provider Newsletter
 AETNA BETTER HEALTH OF VIRGINIA Provider Newsletter Winter 2016 Table of Contents 2017 HEDIS Tips...1 Member Rights and Responsibilities..2 Interpreter and Translation Services..2 Practice Guidelines...3
AETNA BETTER HEALTH OF VIRGINIA Provider Newsletter Winter 2016 Table of Contents 2017 HEDIS Tips...1 Member Rights and Responsibilities..2 Interpreter and Translation Services..2 Practice Guidelines...3
June Thank you for attending today s Webinar. We will begin shortly. June Brian Clark. Diana Charlton. Debbie Barkley Aetna Inc.
 June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,