Palmetto GBA Hospice Coalition Questions November 6, 2001
|
|
|
- Sherman Frederick Butler
- 5 years ago
- Views:
Transcription
1 Palmetto GBA Hospice Coalition Questions November 6, 2001 Billing 1) A hospice patient needs to have an outpatient procedure that is not directly related to the patient's terminal diagnosis. The hospital refuses to bill Medicare because of past denials. What steps would you suggest that we take? When a patient receives services not related to their terminal diagnosis, the patient s regular Medicare benefits should cover those services, this is assuming that the other criteria is met, services are ordered and reasonable and necessary, etc. The provider of the services should list an 07 condition code on their claim to indicate the services provided are not related to the terminal illness. The hospital should contact their Part A Intermediary for assistance in the processing of their claim. 2) A Medicare beneficiary in the skilled nursing facility is allowed to elect the Medicare hospice benefit, provided that the skilled care is for a medical problem unrelated to the terminal illness. a) I believe that CMS has released a statement to that effect. Could we have a copy of it? b) What additional documentation would you suggest that each provider submit to avoid the claim being denied on the first submission? a) We do not have a copy of the statement that the question refers to. However, notes from a conference call with CMS on October 5, 1999 indicate: Our expectation [CMS] is that hospice services provided to a hospice patient residing in a nursing home look no different than hospice services provided to a hospice patient residing in a private residence. Hospice is responsible for all care related to terminal illness/related conditions. The NH is responsible for room and board. (Medicare does not pay for room and board). The hospice maintains professional management responsibility for all services related to the terminal illness/related conditions and is required to provide all core services (including nursing services). The hospice can arrange for another entity/provider (including the nursing home) to provide the non-core services. 1
2 The hospice and the NH must have a written agreement. Medicare can make a hospice payment and a SNF payment if the reason for the hospice election and the reason for the SNF stay are unrelated. A SNF stay can be confusing with a hospice patient in a SNF. b) The hospice agency should submit the specific documentation requested in the ADR. Any other supporting documentation that shows evidence that the reason for hospice care is unrelated to the SNF stay and that the SNF is the beneficiary s place of residence should be included. The best way to ensure payment for the claim is to sufficiently document the patient s condition, terminal illness, reason for hospice care, etc in the clinical record and nurse s notes, so as to paint the most thorough picture of the patient for the nurse reviewers to base their determinations on. The SNF should include the 07 condition code on their claims to indicate the services provided are not related to the terminal illness. The SNF should contact their Part A Intermediary for assistance in the processing of their claim. We contacted the Claims Department at Palmetto GBA for additional information concerning the use of the 07 condition code on the SNF claim. If the SNF bills the original claim without the 07 condition code included, when the notice of election is submitted, the SNF claim will process, but an alert will be sent to the Claims Department to take back the SNF payment. If the SNF claim is submitted with the 07 condition code, then everything will process and no alert will be sent. 3) Occasionally our medical director makes home visits to patients for whom he is not the attending physician. May we bill for those visits? Is so, what procedure should we follow? Any service rendered by a physician other than the attending physician is classified as a consulting physician service. Medically necessary visits to provide professional physician services by a medical director would fit this category. Please note that professional physician services as designated by the appropriate CPT-4 code are the only physician services which are separately billable to Medicare Part A. The visits should be billed using the HCFA 1450 (UB-92). On the UB-92 use revenue code 0657 with the appropriate CPT-4 code that was valid during the time the service was provided. The unit field should report the total number of times each type of service was provided during the billing period, i.e., each visit represents one unit. These services will then be paid to the hospice at 100% of the fee schedule for the area in which the hospice is located. This physician payment is included in the hospice aggregate cap amount. 4) When a patient transfers from one hospice to another, can both programs bill for the day of transfer? 2
3 The reference to this question can be found in the HCFA Publication 21 Hospice Manual, Transmittal 56; dated November 1999, Clarification of Reimbursement for Transfers that result in same day Hospice Discharge and Admission. This section clarifies that both the discharging and admitting hospice can bill for the same patient on the same day. You may also reference the Palmetto GBA Hospice training manual, section 4, page 82. This section states that hospices should communicate with each other to decide exactly how the coordination of the beneficiary's HMB will be handled. Hospice 1 should send the patient's history and POC to hospice 2 along with the change statement. Hospice 1 should then discharge the patient with a 811/821 or a 814/824 bill type and a status code of 01. The first hospice should not include an occurrence code of 42. The 42 would terminate the patient from the HMB. The new hospice must send the Notification of Change (81C/82C) to the Intermediary. The date of admission on the Notification of Change should be the date the patient was admitted to hospice 2. The second hospice agency should maintain the current benefit period by obtaining a physician certification (short certification) to continue the current benefit period. Palmetto GBA will request clarification from CMS concerning obtaining a short physician certification from the second hospice agency. Clarification: The following clarification was received on 2/4/02: We (CMS) do not have anything in the statute or regulations to require a short certification. The certification from agency one should transfer with the patient to agency two. Instead of requiring a short certification, it is recommended that the first agency provide the second agency with the documentation that supported the original diagnosis and prognosis, along with the copy of the actual certification. Cost Report 5) Following the desk audit of our cost report, we received a letter via fax after 3:00 p.m. on Friday stating that we needed to review Palmetto GBA s findings and respond within 10 days, or the findings would stand. Because the executive director was scheduled to be off the next week and the 10 days ran out on the following Sunday, the task to follow-up on her questions about the findings were delegated to the compliance coordinator. She called the person identified as the contact in the faxed letter. The following should be noted: a) The contact person was astonished to receive our call, as she did not know she had been listed and stated she did not have the expertise to help. 3
4 b) We spoke with different people and no one could tell us why an adjustment in patients served and days of care had been made. c) There was no trail that we could find indicating who made the adjustment or why it was made. At every step of the way, we were told not to worry about it because no money was connected with the adjustment. d) We explained that apparently we have made an error and we need to ensure that we have not perpetuated the error in the fiscal year that has just closed. e) Everyone was pleasant and friendly but no one had answers. We still do not know what the problem was. f) The blue cover final report was received last week with a Program Integrity Review letter indicating what will happen if an adjustment occurs that though not meeting the HCFA criteria of abuse on their initial identification, could, if repeated in subsequent cost filings (after identification and notification to the provider), be considered as program abuse and at that time would be reported to the HCFA Regional Office. How can this type of letter be justified if Palmetto GBA cannot identify or explain the error that led to the adjustment? Where do we go from here? Without a provider name or number, I cannot comment specifically on the situation identified in this question. However, I can address the two main issues in this question: the adjustment to patient census and Medicare days and the issue of the Program Integrity Review form. 1) As is noted in the adjustment report that goes out to the provider, we adjust the Medicare days and patient census to agree to what is reported in the PS&R. If the provider does not agree with the PS&R summary report, they would need to contact their reimbursement consultant to request a detail report. They can then compare this report to their own data to identify the discrepancies. If the provider can show that there was an error in the PS&R, they can submit the documentation to the audit department and request a reopening of their Medicare cost report. 2) Audit is required to conduct a Medicare Integrity Review of all finalized cost reports. The purpose for the review is to identify adjustments that could be considered by CMS to be an abuse to the Program. Most cost adjustments would not be considered abusive on their initial identification; however, if these adjustments are repeated year after year, they could be considered a program abuse at a later date. The purpose of the Program Integrity Review form is to notify the provider of these specific adjustments. Any adjustments of this nature are listed specifically on the form and if there are no adjustments of this nature, the word "NONE" usually appears. It should be noted that all cost report settlements receive this form. It should also be noted that Palmetto does not consider settlement data adjustments (or adjustments to agree the provider's Medicare census and statistics to the PS&R) to be program integrity issues. These adjustments would not be listed on this form. I have reviewed all hospice 4
5 settlements performed thus far to verify that settlement data adjustments were not reported on this form. I found no exceptions. Additional information was shared during the 1:00 P.M. conference call with the Gulf Coast Office. Please refer to the Additional Information Section. 6) We believe the patient count variance cited in the cost report question above could be related to MSP patients, although the days of care adjustment does not agree. How does Palmetto GBA count MSP patients and the days of care provided to them? Are they private insurance or Hospice Medicare? The audit department simply adjusts the patient census reported on the provider's cost report to what is on the PS&R. It is recommended that the provider request a detail PS&R from the reimbursement department to identify exactly what makes up the patient census number. Additional information was shared during the 1:00 P.M. conference call with the Gulf Coast Office. Please refer to the Additional Information Section. LMRPs 7) We received a denied rebuttal for a patient with dementia from the Benefit Integrity Unit. The denial was based on the fact that the patient had no documented change in condition or functional abilities since her admission to hospice, which indicates that there was not a rapid decline in the patient s condition. This patient met the 7C Functional Assessment Staging Scale with the exception that she, on occasion, could ambulate independently with the use of a walker, but she was at high risk for falls. Due to her dementia it was difficult to keep her from ambulating independently. In fact, during the denied period she fell and injured her back and required pain management. The patient experienced a 6% weight loss in the two months prior and an additional 8% weight loss in the two months following the review period. The denial stated the criteria requires evidence of a 10% weight loss during the previous six months. This patient also had congestive heart failure with an exacerbation episode just prior to her admission. During this episode she was hospitalized with chest pain, bradycardia and an oxygen saturation level of 82%. The chest pain was unrelieved with medication so it was treated with a lidocaine drip. Following hospice admission her CHF symptoms were fairly well controlled due to close monitoring by the hospice staff. a) The LMRP for dementia does not require a change in condition or functional abilities. Is this now a requirement? 5
6 b) Even though the patient had a clearly downward weight trajectory, the period was denied because the full 10% did not occur in the previous six months. Please explain this rationale. The purpose of the coalition meeting is not to discuss specific beneficiary cases. In order for Palmetto GBA to provide assistance concerning specific beneficiary cases, we would suggest that the provider write a letter to the Benefit Integrity Unit and the Reconsideration and Appeals department with a copy of the letter also being sent to Dr. Feliciano. The request would need to identify the beneficiary, HICN and the dates of service. Each area would then be able to review the details of the actual documentation and then respond accordingly. During the Hospice Coalition meeting the beneficiary specific information was given to the Manager of the Reconsideration/Appeals Department. 8) We recently were denied payment for services provided to a patient with end stage Parkinson s disease. The reconsideration determination upheld the decision for the denial. The documentation indicated that his condition was extremely compromised and deteriorating. The letter from Palmetto denying the reconsideration stated that the documentation did not show the patient experienced a decline in condition or support a prognosis of six months or less according to the local medical review policy criteria for dementia or heart disease. The letter goes on to list all the requirements for the LMRPs for dementia and heart disease elaborating on why the patient did not meet the criteria for those two diagnoses. The patient did not have dementia and there was no documentation in our appeal packet that this diagnosis was ever present. Although the patient had severe coronary artery disease along with hypertension, arrhythmia and an unresectable abdominal aortic aneurysm, heart disease was not his terminal diagnosis; however, it was a very significant comorbid condition along with dysphagia resulting from a previous transischemic accident. This patient s terminal diagnosis was Parkinson s disease. Why is care being denied based on LMRPs for diagnoses when neither is the beneficiary s terminal diagnosis? The purpose of the coalition meeting is not to discuss specific beneficiary cases. In order for Palmetto GBA to provide assistance concerning specific beneficiary cases, we would suggest that the provider write a letter to the Benefit Integrity Unit and the Reconsideration and Appeals department with a copy of the letter also being sent to Dr. Feliciano. The request would need to identify the beneficiary, HICN and the dates of service. Each area would then be able to review the details of the actual documentation and then respond accordingly. During the Hospice Coalition meeting the beneficiary specific information was given to the Manager of the Reconsideration/Appeals Department. General 6
7 9) A patient is admitted to a hospital for a non-related diagnosis (hip fracture). At some point during the stay, the patient's terminal diagnosis becomes the primary reason the patient continues to be hospitalized (heart disease in the ICU). Please explain how to handle this situation from a billing, care plan and visit frequency perspective. At the point that it becomes necessary for the patient to be hospitalized for care related to the terminal illness the standard general inpatient care guidelines become applicable. The necessary changes to the care plan should be made, and services should be provided in a contracted facility. The hospice remains the professional manager of the patient s care, despite the physical setting. The hospice begins to bill for general inpatient upon meeting the above guidelines. At this time the hospital would no longer be billing Medicare, rather they would be billing the hospice based upon the contract in place. The visit frequency would be based on the needs of the patient with the care that is being provided by the hospital staff taken into account. 10) Can Palmetto PBA report the average number of days billed per episode of general inpatient, respite and continuous care levels of care? Please refer to Attachment A. 11) The COPs state that the election statement must include the effective date of the election. Nothing in the language states or implies that the beneficiary has to be the one writing the election date on the statement. Recently, however, medical review indicated that the patient must be the one completing this date. Please clarify medical review's perspective with the law. If the hospice representative completes the form, including the election date and the patient then signs it, is this acceptable? As stated in the Code of Federal Regulations, 42CFR, Section Election of Hospice Care, when the beneficiary elects hospice, they or their legally identified representative must sign the election form to indicate that they are electing hospice and understand what the election of the benefit means. The Medical Review representative suggested that the beneficiary should date the form to ensure that the beneficiary is aware of what they are signing. 12) Under what circumstances can an advanced practice nurse or PA be paid for the care of a hospice patient? Nurse Practitioners services are only billable if they are providing services on behalf of the non-employed attending physician. Those services are billed to the Medicare Part B Carrier and would have to adhere to the Medicare Part B billing guidelines. They couldn t bill unless it was under the incident to provision and billed under the attending doctor s provider number. If the non-employed 7
8 attending physician has to be out of the office, then he/she needs to get a locum physician to substitute or have a reciprocal arrangement, as only services related to the terminal condition provided under the non-employee attending physician s UPIN will be paid. Palmetto GBA is requesting additional information from the South Carolina Part B Carrier and from CMS. 13) If the service is for a diagnosis unrelated to the terminal diagnosis, under what circumstances can the above provider bill? According to the Centers for Medicare & Medicaid Services (CMS) Publication 21, Section 303.2, Billing for Covered Medicare Services Unrelated to Hospice Care, Any covered Medicare services not related to the treatment of the terminal condition for which hospice care was elected, and are furnished during a hospice election period, are billed to the intermediary or carrier for nonhospice Medicare payment. Additional Information: Palmetto GBA has received the following clarification from CMS concerning two questions from the August 7, 2001 meeting. 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example, the verbal certification was not obtained and the written was obtained 5 days after admission. For clarification, the certification timelines are that for the first 90-day benefit period of hospice coverage, the hospice agency must obtain, no later than two calendar days after hospice care is initiated (by the end of the third day), the certification of terminal illness from the medical director of the hospice or the physician member of the hospice interdisciplinary group and the individual s attending physician (if the attending physician is not the medical director). The certification may be completed up to two weeks (14 days) before the hospice care is elected (effective date on the election statement). If a written certification is not obtained within two calendar days following the initiation of hospice care, then a verbal certification may be obtained within the two days following the initiation of hospice care, with the written certification obtained prior to billing for hospice services. According to Section 201 of the CMS Publication 21, if these requirements are not met, then no payment is made for the days prior to date that the certification is received. Therefore, in the example given above, if a verbal certification was not obtained and the written certification was obtained 5 8
9 days after the initiation of hospice care, then the hospice will not be able to bill for days 1 4 of the benefit period. The hospice would submit an 8X1 or 8X2 bill type and bill for only the covered days. (Do not submit the non-covered days as non-covered charges) Once the claim is received, the claims processing system will return the claim to provider (RTP) with a reason code for having a gap in service. Upon receiving the RTP, the provider should call the Provider Service Center and report the issue. The service center will write up the claim information and request that the claims department manually process the claim. Palmetto GBA will forward the question to CMS for additional clarification. Clarification: There is no additional clarification. Publication 21, Section 201, specifically states that if the timely certification requirements are not met, then no payment is made for the days prior to the (signed) certification. Instead, payment begins with the day of certification. 15. A nursing facility owns a hospice and will only allow its residents to receive services from that hospice. Please comment on this practice. Medicare beneficiaries should have access to all providers regardless of relationships to other facilities. As a part of the Medicare provider agreement, providers should not deny access to services for Medicare eligible beneficiaries. Additionally, the BBA 1997 indicated that upon discharging from a hospital the patient should receive information concerning all providers in their service area. Palmetto GBA will forward the question to CMS for additional clarification. Clarification: These requirements of the BBA of 1997 pertain to hospitals. Nursing Facilities (NFs) may contract with the hospice of their choice. The patient then, must decide if they wish to receive hospice services from that NF or whether or not they will go with another NF. Ultimately, the patient has the right to choose a provider of services (Section 1802), providing the provider can accept him/her. As long as the patient is satisfied with their choice of the NF and hospice, even thought it may be the only hospice the NF contracts with, then we accept it. If you as the FI suspect fraud and/or abuse you may report it to the local Office of Inspector General (OIG). If you suspect that the NF is not providing the appropriate level of services or lacks the appropriate quality of care, you may report it to the local Sate Survey and Certification Agency. 9
10 2. Hospice Reversal Rates, Attachment B. 3. Population-level information relating to the Non-Cancer Length of Stay (NCLOS) Rates. The information is stratified by region/policy and includes the NCLOS Rate frequency and distribution for each region/policy as well as the frequency and distribution of the General, Provider-Specific NCLOS Rates. Attachment C. Explanation of Attachment C-NCLOS Rate Analysis, Palmetto GBA Provider Population, January 1, 2001-June 30, Second and third slides provide an overview of the NCLOS Rates. 2. The next ten slides provide information on Policy-specific, Population NCLOS Rates for Palmetto GBA s four regions. Gulf Coast (FL, GA, AL, MS), Midwest (IL, IN, OH) Southeast (SC, NC, TN, KY), Southwest (TX, OK, AR, NM, LA) and then the four regions combined. 3. The next 45 slides show the frequency and distribution of Policy-specific, Provider specific NCLOS Rates for each of the four regions and then for the four regions combined. 4. The final slide shows the frequency and distribution of General, Providerspecific NCLOS Rates (i.e., all non-cancer claims subject to the non-cancer LMRPs, for a single provider) for the four regions combined. 1:00 Conference call concerning focused review of Cost Report A conference call was held with the Manager Lynda Hebbeln of the Gulf Coast Audit and Reimbursement Department concerning questions surrounding the Hospice Cost Report and specifically questions concerning a agency which was selected for a focused review of their cost report. Ms. Hebbeln indicated that she may be contacted concerning questions about focused review of cost reports. She may be reached at (727) , extension The on-site audits are considered the first efforts in obtaining information concerning the hospice cost reports. It is an educational process for both sides (Palmetto GBA and the hospice provider). If a provider is selected for a focused review of the cost report they will receive a letter of notification. The reviews will be completed during the time period of October 2001 July Comments were received concerning the letter of notification. The hospice community has indicated that the letter is confusing. A letter should have specifically been developed for the hospice community. The letter used was 10
11 geared more towards home health agencies, and a letter should be developed to include more language geared towards hospice. The following requests were made concerning additional information about the focused reviews: 1) A What s New article was requested concerning what action or documentation the hospice provider should be expected to obtain for the review. Ms. Hebbeln indicated that her staff would be able to provide some additional information concerning the focused review process. 2) Develop a Provider Tips list concerning on - site review; for example, depreciation tax purposes versus Medicare purposes longest life, information concerning salvage value assigned and information concerning the Section of the HIM 2150, about Home Office Providers. 3) Develop Most Common Errors from the settlement of the focused review of the cost reports. 11
12 ATTACHMENT A The following table contains mean and median values for selected revenue codes by provider state. The unit for revenue code 652 is hours and the unit for the other revenue codes is days. For the purposes of the current analysis, an episode was defined as the period from the admit date through the last billed to date for a beneficiary. Please note that by using this definition, it is possible for a beneficiary to be represented more than once in the data. Hospice claims with an admit date of January 1, 2001 or later processed on or before September 30, 2001 were included in the analysis. The mean and median is calculated using only episodes that have a least one claim line with that revenue code. Mean & Median for Selected Revenue Codes by Provider State State (State Code) & Total Episodes Alabama (01) N = 7,237 Arkansas (04) N = 2,974 Florida (10) N = 37,477 Georgia (11) N = 9,516 Illinois (14) N = 14,248 Indiana (15) N = 6,286 Kentucky (18) N = 4,999 Louisiana (19) N = 4,332 Mississippi (25) N = 4,041 New Mexico (32) N = 2,077 North Carolina (34) N = 8,452 Ohio (36) N = 17,204 Oklahoma (37) N = 6,326 South Carolina (42) N = 3,792 Revenue Code Episodes Having Revenue Code Mean Median hrs 32.0 hrs days 5.0 days days 5.0 days , , , , , , , ,
13 Tennessee (44) N = 4,995 Texas (45/67) N = 24, ,
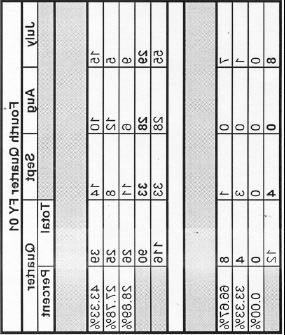
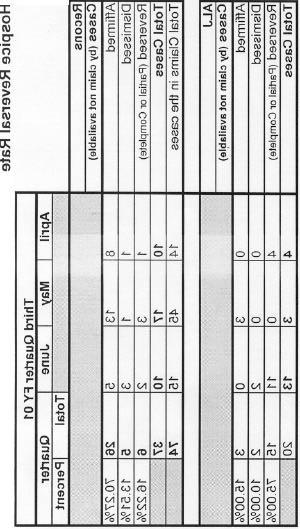
14 ATTACHMENT B 14
15 ATTACHMENT C NCLOS Rate Analysis Power Point Presentation 15
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions
 Palmetto GBA Hospice Coalition Questions November 1, 1999 Billing/Reimbursement/FISS 1. The hospice medical director fails to sign a patient's recertification of terminal prognosis in a timely fashion.
Palmetto GBA Hospice Coalition Questions November 1, 1999 Billing/Reimbursement/FISS 1. The hospice medical director fails to sign a patient's recertification of terminal prognosis in a timely fashion.
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY
 STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA
 1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
1 ELIGIBILITY & CERTIFICATION THE CONTINUING SAGA Hospice Fundamentals Charlene Ross, MSN, MBA, RN Consultant / Educator 2 What You Will Learn Today The regulatory requirements of certification, recertification
MEMORANDUM Texas Department of Human Services * Long Term Care/Policy
 MEMORANDUM Texas Department of Human Services * Long Term Care/Policy TO: FROM: LTC-R Regional Directors Section/Unit Managers Marc Gold Section Manager Long Term Care Policy State Office MC: W-519 SUBJECT:
MEMORANDUM Texas Department of Human Services * Long Term Care/Policy TO: FROM: LTC-R Regional Directors Section/Unit Managers Marc Gold Section Manager Long Term Care Policy State Office MC: W-519 SUBJECT:
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
MEDICARE COVERAGE SUMMARY: OUTPATIENT PSYCHIATRIC AND PSYCHOLOGICAL SERVICES
 OPTUM MEDICARE COVERAGE SUMMARY: OUTPATIENT PSYCHIATRIC AND PSYCHOLOGICAL SERVICES MEDICARE COVERAGE SUMMARY: OUTPATIENT PSYCHIATRIC AND PSYCHOLOGICAL SERVICES Guideline Number: Effective Date: April,
OPTUM MEDICARE COVERAGE SUMMARY: OUTPATIENT PSYCHIATRIC AND PSYCHOLOGICAL SERVICES MEDICARE COVERAGE SUMMARY: OUTPATIENT PSYCHIATRIC AND PSYCHOLOGICAL SERVICES Guideline Number: Effective Date: April,
Palmetto GBA Hospice Coalition Questions and Answers
 Palmetto GBA Hospice Coalition Questions and Answers September 23, 2008 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 23, 2008 Location: Palmetto GBA Attachment A:
Palmetto GBA Hospice Coalition Questions and Answers September 23, 2008 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 23, 2008 Location: Palmetto GBA Attachment A:
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
General Inpatient Level of Care: Managing Risks
 General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
06-01 FORM HCFA WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the
 06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
Medicaid-Enrolled Hospice and Nursing Facility Providers
 M E D I C A I D B U L L E T I N B T 1 9 9 9 2 4 J U L Y 3 0, 1 9 9 9 To: Subject: Medicaid-Enrolled Hospice and Nursing Facility Providers Treatment for Non-Terminal Conditions for Hospice Recipients Admitted
M E D I C A I D B U L L E T I N B T 1 9 9 9 2 4 J U L Y 3 0, 1 9 9 9 To: Subject: Medicaid-Enrolled Hospice and Nursing Facility Providers Treatment for Non-Terminal Conditions for Hospice Recipients Admitted
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
Hospice Coalition. Questions and Answers
 Hospice Coalition Questions and Answers September 9, 2009 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 9, 2009 Location: Palmetto GBA Attachment AD: Palmetto GBA
Hospice Coalition Questions and Answers September 9, 2009 To: Hospice Coalition Members From: Palmetto GBA Provider Education Date: September 9, 2009 Location: Palmetto GBA Attachment AD: Palmetto GBA
The Concerns. Hospice Care in The Nursing Home NHPCO MLC All Rights Reserved 1.
 Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 PAYMENTS POLICY CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM Issue Date: November 28,
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 PAYMENTS POLICY CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM Issue Date: November 28,
KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization. Nancy Jobe
 KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization Nancy Jobe 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the Beneficiary
KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization Nancy Jobe 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the Beneficiary
Table of Contents. 1.0 Description of the Procedure, Product, or Service Definitions Hospice Terminal illness...
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
08-16 FORM CMS
 08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
The Monthly Publication of the National Hospice and Palliative Care Organization
 The Monthly Publication of the National Hospice and Palliative Care Organization Print-friendly PDF From September 2012 Issue A Hospice Provider s Guide to Live Discharges By Jennifer Kennedy, MA, BSN,
The Monthly Publication of the National Hospice and Palliative Care Organization Print-friendly PDF From September 2012 Issue A Hospice Provider s Guide to Live Discharges By Jennifer Kennedy, MA, BSN,
Hospices Under the Microscope: Are You Prepared for ZPICs? Medicare Integrity Programs. Objectives. Fraud or Abuse? 3/3/2014
 Hospices Under the Microscope: Are You Prepared for ZPICs? Paula G. Sanders, Esquire Principal & Chair Health Care Practice Post & Schell, PC Diane Baldi, RN CHPN Chief Executive Officer Hospice of the
Hospices Under the Microscope: Are You Prepared for ZPICs? Paula G. Sanders, Esquire Principal & Chair Health Care Practice Post & Schell, PC Diane Baldi, RN CHPN Chief Executive Officer Hospice of the
ABOUT AHCA AND FLORIDA MEDICAID
 Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
SNF Determinations of Non-Coverage Denial Letters, ABNs & Expedited Determinations
 SNF Determinations of Non-Coverage Denial Letters, ABNs & Expedited Determinations for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240
SNF Determinations of Non-Coverage Denial Letters, ABNs & Expedited Determinations for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Report to Congressional Defense Committees
 Report to Congressional Defense Committees The Department of Defense Comprehensive Autism Care Demonstration December 2016 Quarterly Report to Congress In Response to: Senate Report 114-255, page 205,
Report to Congressional Defense Committees The Department of Defense Comprehensive Autism Care Demonstration December 2016 Quarterly Report to Congress In Response to: Senate Report 114-255, page 205,
hospic Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals.
 Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
Organization and administration of services
 418.106 Condition of participation: Drugs and biologicals, medical supplies, and durable medical equipment and 6 standards Medical supplies and appliances, as described in 410.36 of this chapter; durable
418.106 Condition of participation: Drugs and biologicals, medical supplies, and durable medical equipment and 6 standards Medical supplies and appliances, as described in 410.36 of this chapter; durable
ATTACHMENT I. Outpatient Status: Solicitation of Public Comments
 ATTACHMENT I The following text is a copy of the Federation of American Hospitals ( FAH ) comments in response to the solicitation of public comments on outpatient status that was contained in CMS-1589-P;
ATTACHMENT I The following text is a copy of the Federation of American Hospitals ( FAH ) comments in response to the solicitation of public comments on outpatient status that was contained in CMS-1589-P;
HOSPICE POLICY UPDATE
 #02-56-13 Bulletin June 24, 2002 Minnesota Department of Human Services # 444 Lafayette Rd. # St. Paul, MN 55155 OF INTEREST TO County Directors Administrative contacts AC, EW, CAC, CADI, TBI DD Waiver
#02-56-13 Bulletin June 24, 2002 Minnesota Department of Human Services # 444 Lafayette Rd. # St. Paul, MN 55155 OF INTEREST TO County Directors Administrative contacts AC, EW, CAC, CADI, TBI DD Waiver
KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization. Brittny Bratcher, MS, CHES
 KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization Brittny Bratcher, MS, CHES 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO
KEPRO The Beneficiary and Family Centered Care Quality Improvement Organization Brittny Bratcher, MS, CHES 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO
ABOUT FLORIDA MEDICAID
 Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Connecticut interchange MMIS
 Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
RESPITE CARE LEGACY HOSPICE
 RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
Objectives. The Alphabet Soup Of Hospice Scrutiny
 Leadership And The Interdisciplinary Group: Overcoming Organizational Challenges In A Time of Change Alphabet Soup For The Hospice Soul: Understanding The Impact Of RHHI, MAC, RAC, CMS, OIG, FBI and DOJ
Leadership And The Interdisciplinary Group: Overcoming Organizational Challenges In A Time of Change Alphabet Soup For The Hospice Soul: Understanding The Impact Of RHHI, MAC, RAC, CMS, OIG, FBI and DOJ
MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY
 OPTUM MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY Guideline Number: Effective Date: June, 2017 INTRODUCTION
OPTUM MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY: HOME HEALTH PSYCHIATRIC CARE MEDICARE COVERAGE SUMMARY Guideline Number: Effective Date: June, 2017 INTRODUCTION
Reference Guide for Hospice Medicaid Services
 Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual
 HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual Issued April 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10 diagnosis
HOSPICE PROVIDER MANUAL Chapter twenty-four of the Medicaid Services Manual Issued April 15, 2012 Claims/authorizations for dates of service on or after October 1, 2015 must use the applicable ICD-10 diagnosis
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Use of Medicaid MCO Capitation by State Projections for 2016
 Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Use of Medicaid MCO Capitation by State Projections for 5 Slide Series September, 2015 Summary of Findings This edition projects Medicaid spending in each state and the percentage of spending paid via
Topics. Overview of the Medicare Recovery Audit Contractor (RAC) Understanding Medicaid Integrity Contractor
 Understanding Medicaid Integrity Contractor") RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG. Effective September 1, 2014
 FOR APR-DRG. Effective September 1, 2014") INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG Effective September 1, 2014 Who are we? eqhealth has a 16 year partnership with Mississippi Division of Medicaid (DOM) as the Utilization
INDEPENDENT VERIFICATION AND CODING VALIDATION (IV & V) FOR APR-DRG Effective September 1, 2014 Who are we? eqhealth has a 16 year partnership with Mississippi Division of Medicaid (DOM) as the Utilization
Framework for Post-Acute Care: Current and Future Issues for Providers
 Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
Framework for Post-Acute Care: Current and Future Issues for Providers Alan G. Rosenbloom Alliance for Quality Nursing Home Care March 2012 Overview of Presentation Post-Acute Care: Background and Trends
10.0 Medicare Advantage Programs
 10.0 Medicare Advantage Programs This section is intended for providers who participate in Medicare Advantage programs, including Medicare Blue PPO. In addition to every other provision of the Participating
10.0 Medicare Advantage Programs This section is intended for providers who participate in Medicare Advantage programs, including Medicare Blue PPO. In addition to every other provision of the Participating
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Disclaimer. January 2015 Palmetto GBA - Jurisdiction 11 Medicare Administrative Contractor 2
 Disclaimer The information enclosed was current at the time it was presented. Medicare policy changes frequently; links to the source documents have been provided within the document for your reference.
Disclaimer The information enclosed was current at the time it was presented. Medicare policy changes frequently; links to the source documents have been provided within the document for your reference.
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT
 CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
2015 State Hospice Report 2013 Medicare Information 1/1/15
 2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
2015 State Hospice Report 2013 Medicare Information 1/1/15 www.hospiceanalytics.com 2 2013 Demographics & Hospice Utilization National Population 316,022,508 Total Deaths 2,529,792 Medicare Beneficiaries
CONNECTICUT: ECONOMIC FUTURE WITH EDUCATIONAL REFORM
 CONNECTICUT: ECONOMIC FUTURE WITH EDUCATIONAL REFORM This file contains detailed projections and information from the article: Eric A. Hanushek, Jens Ruhose, and Ludger Woessmann, It pays to improve school
CONNECTICUT: ECONOMIC FUTURE WITH EDUCATIONAL REFORM This file contains detailed projections and information from the article: Eric A. Hanushek, Jens Ruhose, and Ludger Woessmann, It pays to improve school
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
# December 29, 2000
 #00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
#00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
Medical Review and Appeals 3/25/2010
 The Medical Review and Appeals Show Presented by Cahaba Government Benefit Administrators Provider Outreach and Education March 25, 2010 2 1 Disclaimer This resource is not a legal document. This presentation
The Medical Review and Appeals Show Presented by Cahaba Government Benefit Administrators Provider Outreach and Education March 25, 2010 2 1 Disclaimer This resource is not a legal document. This presentation
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
Dashboard. Campaign for Action. Welcome to the Future of Nursing:
 Welcome to the Future of Nursing: Campaign for Action Dashboard About This Dashboard: These graphs and charts show goals by which the Campaign evaluates its efforts to implement recommendations in the
Welcome to the Future of Nursing: Campaign for Action Dashboard About This Dashboard: These graphs and charts show goals by which the Campaign evaluates its efforts to implement recommendations in the
(f) Department means the New Hampshire department of health and human services.
 Department means the New Hampshire department of health and human services.") Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Medicare General Information, Eligibility, and Entitlement
 Medicare General Information, Eligibility, and Entitlement Chapter 4 - Physician Certification and Recertification of Services Transmittals for Chapter 4 Table of Contents (Rev. 50, 12-21-07) 10 - Certification
Medicare General Information, Eligibility, and Entitlement Chapter 4 - Physician Certification and Recertification of Services Transmittals for Chapter 4 Table of Contents (Rev. 50, 12-21-07) 10 - Certification
OIG Hospice Risk Areas With Footnotes
 Moreover, the compliance programs should address the ramifications of failing to cease and correct any conduct criticized in a Special Fraud Alert, if applicable to hospices, or to take reasonable action
Moreover, the compliance programs should address the ramifications of failing to cease and correct any conduct criticized in a Special Fraud Alert, if applicable to hospices, or to take reasonable action
UTILIZATION MANAGEMENT AND CARE COORDINATION Section 8
 Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
Medicare Recovery Audit Contractors. Chicago, IL August 1, 2008
 Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
PRESCRIBED PEDIATRIC EXTENDED CARE CENTERS CSHCN SERVICES PROGRAM PROVIDER MANUAL
 PRESCRIBED PEDIATRIC EXTENDED CARE CENTERS CSHCN SERVICES PROGRAM PROVIDER MANUAL SEPTEMBER 2018 CSHCN PROVIDER PROCEDURES MANUAL SEPTEMBER 2018 PRESCRIBED PEDIATRIC EXTENDED CARE CENTERS Table of Contents
PRESCRIBED PEDIATRIC EXTENDED CARE CENTERS CSHCN SERVICES PROGRAM PROVIDER MANUAL SEPTEMBER 2018 CSHCN PROVIDER PROCEDURES MANUAL SEPTEMBER 2018 PRESCRIBED PEDIATRIC EXTENDED CARE CENTERS Table of Contents
Mississippi Medicaid Hospice Services Provider Manual
 Mississippi Medicaid Hospice Services Provider Manual Effective: January 2011 Revised: January 2017 Table of Contents I. Introduction II. Frequently Used Terms III. Getting Started Helpful Tips A. Before
Mississippi Medicaid Hospice Services Provider Manual Effective: January 2011 Revised: January 2017 Table of Contents I. Introduction II. Frequently Used Terms III. Getting Started Helpful Tips A. Before
Figure 10: Total State Spending Growth, ,
 26 Reason Foundation Part 3 Spending As with state revenue, there are various ways to look at state spending. Total state expenditures, obviously, encompass every dollar spent by state government, irrespective
26 Reason Foundation Part 3 Spending As with state revenue, there are various ways to look at state spending. Total state expenditures, obviously, encompass every dollar spent by state government, irrespective
Medicare Hospice Billing 2015 & Beyond!
 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Overview of Presentation
 End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
Extended Care Health Option (ECHO)
") Extended Care Health Option (ECHO) General information about ECHO: The TRICARE Extended Care Health Option (ECHO) is available to active duty family members who have severe physical or moderate to severe
Extended Care Health Option (ECHO) General information about ECHO: The TRICARE Extended Care Health Option (ECHO) is available to active duty family members who have severe physical or moderate to severe
State Operations Manual. Appendix M - Guidance to Surveyors: Hospice - (Rev. 1, )
") State Operations Manual Appendix M - Guidance to Surveyors: Hospice - (Rev. 1, 05-21-04) Part I Investigative Procedures I - Introduction A - Initial Certification Surveys B - Recertification Survey of
State Operations Manual Appendix M - Guidance to Surveyors: Hospice - (Rev. 1, 05-21-04) Part I Investigative Procedures I - Introduction A - Initial Certification Surveys B - Recertification Survey of
Medical Review: Past, Present and Future
 Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
COMPLIANCE ALERT. Department Chairs, Compliance Leaders, and UFJPI Management
 UNIVERSITY OF FLORIDA COLLEGE OF MEDICINE - JACKSONVILLE Office of Physician Billing Compliance 653-1 West 8 th Street, LRC-3 Jacksonville, Florida 32209 Phone: (904) 244-2158 Fax: (904) 244-5323 COMPLIANCE
UNIVERSITY OF FLORIDA COLLEGE OF MEDICINE - JACKSONVILLE Office of Physician Billing Compliance 653-1 West 8 th Street, LRC-3 Jacksonville, Florida 32209 Phone: (904) 244-2158 Fax: (904) 244-5323 COMPLIANCE
FIELD BY FIELD INSTRUCTIONS
 TRANSPORTATION EMEDNY 000201 CLAIM FORM INSTRUCTIONS The following guide gives instructions for proper claim form completion when submitting claims for Transportation Services using the emedny 000201 claim
TRANSPORTATION EMEDNY 000201 CLAIM FORM INSTRUCTIONS The following guide gives instructions for proper claim form completion when submitting claims for Transportation Services using the emedny 000201 claim
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
You recently called the Medicare Rights helpline for assistance with a denial from your Medicare private health plan.
 Date: Dear Helpline Caller: The Medicare Rights Center is a national, nonprofit organization. We help older adults and people with disabilities with their Medicare problems. We support caregivers and train
Date: Dear Helpline Caller: The Medicare Rights Center is a national, nonprofit organization. We help older adults and people with disabilities with their Medicare problems. We support caregivers and train
Having the Difficult Conversation: We need to Discharge You from Hospice
 Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Having the Difficult Conversation: We need to Discharge You from Hospice Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Identify the regulatory requirements
Alaska (AK) Arizona (AZ) Arkansas (AR) California-RN (CA-RN) Colorado (CO)
 Arizona (AZ) Arkansas (AR) California-RN (CA-RN) Colorado (CO)") Beth Radtke 49 Included in the report: 7/22/2015 11:17:54 AM Alaska (AK) Arizona (AZ) Arkansas (AR) California-RN (CA-RN) Colorado (CO) Connecticut (CT) Delaware (DE) District Columbia (DC) Florida (FL)
Beth Radtke 49 Included in the report: 7/22/2015 11:17:54 AM Alaska (AK) Arizona (AZ) Arkansas (AR) California-RN (CA-RN) Colorado (CO) Connecticut (CT) Delaware (DE) District Columbia (DC) Florida (FL)
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
TABLE OF CONTENTS. Therapy Services Provider Manual Table of Contents
 Table of Contents TABLE OF CONTENTS Table of Contents...1 About AHCA...2 About eqhealth Solutions...2 Accessibility and Contact Information...5 Review Requirements and Submitting PA Requests...9 First
Table of Contents TABLE OF CONTENTS Table of Contents...1 About AHCA...2 About eqhealth Solutions...2 Accessibility and Contact Information...5 Review Requirements and Submitting PA Requests...9 First
Home Health, Hospice, and Nursing Facility. Indiana Health Coverage Programs DXC Technology October 2017
 Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Molina Healthcare MyCare Ohio Prior Authorizations
 Molina Healthcare MyCare Ohio Prior Authorizations Agenda Eligibility Medicare Passive Enrollment Transition of Care Definition Submission Time Frame Standard vs. Urgent How to Submit a Prior Authorization
Molina Healthcare MyCare Ohio Prior Authorizations Agenda Eligibility Medicare Passive Enrollment Transition of Care Definition Submission Time Frame Standard vs. Urgent How to Submit a Prior Authorization
Coding Alert. Michigan State Medical Society. Medicare Consultation Services Payment Policy
 Michigan State Medical Society Coding Alert Medicare Consultation Services Payment Policy Policy Summary Despite strong objections from organized medicine, the US Centers for Medicare & Medicaid Services
Michigan State Medical Society Coding Alert Medicare Consultation Services Payment Policy Policy Summary Despite strong objections from organized medicine, the US Centers for Medicare & Medicaid Services
Hospice: Background 1963: 1965: 1968: 1969: 1972: 1974: : 1978:
 Hospice: Background In celebration of the 30th year of enactment of the Medicare Hospice Benefit (MHB), the Hospice Association of America would like to share a chronology of Hospice care in the United
Hospice: Background In celebration of the 30th year of enactment of the Medicare Hospice Benefit (MHB), the Hospice Association of America would like to share a chronology of Hospice care in the United
SEP Memorandum Report: "Trends in Nursing Home Deficiencies and Complaints," OEI
 DEPARTMENT OF HEALTH &. HUMAN SERVICES Office of Inspector General SEP 18 2008 Washington, D.C. 20201 TO: FROM: Kerry Weems Acting Administrator Centers for Medicare & Medicaid Services Daniel R. Levinson~
DEPARTMENT OF HEALTH &. HUMAN SERVICES Office of Inspector General SEP 18 2008 Washington, D.C. 20201 TO: FROM: Kerry Weems Acting Administrator Centers for Medicare & Medicaid Services Daniel R. Levinson~
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Administrative Guide. KanCare Program Chapter 11: Hospice. Physician, Health Care Professional, Facility and Ancillary. UHCCommunityPlan.
 KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY
 MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MLN Matters Number: MM6699 Related Change Request (CR) #: 6699
 #: 6699") News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor. NJHFMA Finance for Clinicians Session March 24, 2016
 1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
MEMORANDUM Texas Department of Human Services * Long Term Care/Policy
 MEMORANDUM Texas Department of Human Services * Long Term Care/Policy TO: FROM: LTC-R Regional Directors & Program Managers State Office Section/Unit Managers HCSSA Program Administrators Jim Lehrman Associate
MEMORANDUM Texas Department of Human Services * Long Term Care/Policy TO: FROM: LTC-R Regional Directors & Program Managers State Office Section/Unit Managers HCSSA Program Administrators Jim Lehrman Associate
Readmission Policy REIMBURSEMENT POLICY UB-04. Reimbursement Policy Oversight Committee
 Readmission Policy Policy Number 2018F7001A Annual Approval Date 11/11/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Readmission Policy Policy Number 2018F7001A Annual Approval Date 11/11/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1
 Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
July 26, Dear Ms. Stein-Ordonez:
 Department of Health & Human Services Centers for Medicare & Medicaid Services 233 North Michigan Avenue, Suite 600 Chicago, Illinois 60601-5519 Refer to: July 26, 2002 Michelle Stein-Ordonez, Policy Analyst
Department of Health & Human Services Centers for Medicare & Medicaid Services 233 North Michigan Avenue, Suite 600 Chicago, Illinois 60601-5519 Refer to: July 26, 2002 Michelle Stein-Ordonez, Policy Analyst