CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
|
|
|
- Lydia Wood
- 6 years ago
- Views:
Transcription

1 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants
2 Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the MDS as the underpinning for documentation and coding 3. Oversight of claims and self-audit opportunities 4.Review of current RAC and other audits

3 WHY DO WE NEED APPROPRIATE?

4 The importance of appropriate, accurate and complete documentation of clinical services provided to swing-bed patients cannot be overemphasized
5 Documentation is important to validate the care rendered to the resident. Documentation is important to support reimbursement for the services rendered Documentation is the main source of evidence that usually determines the outcome of the inquiry Attorneys use documentation to make the facility and the caregivers appear to be negligent. Documentation is the Facility and caregiver s best protection.


6 Establish a timeline of care beginning at admission Paint a picture If it is not documented... Project a team approach to care (i.e. nursing can document how a therapy patient is improving/not improving in ambulation during the evening) 6
7 Medical Necessity Documentation Tips Answer the following in your documentation: Why should you be involved? What did you do? Did you say that? What was the patient s response to your actions? If the patient s response was not positive, what did you do about it?
8 Medical Necessity Documentation Tips Chart to support the skilled care provided Must be detailed and specific-justifies Medicare reimbursement Needs to be Daily (per Medicare regulations) Recommend every shift Not charting by exception If Rehab is the primary skill, nursing must document patient participation, tolerance and progress in therapy
9 Medical Necessity Documentation Tips For exceptional documentation, remember to include: Who Performing, supervising and referring practitioners What (and how many) Services and quantities of services performed Where Place of service When Date of service Why Medical necessity and diagnosis

10 Example: Medical Necessity Documentation Tips Lisa continues to require PT and OT for strengthening and balance. Ambulates to bathroom with 2 person extensive assist and becomes SOB with exertion. Uses the toilet with staff oversight and transfers with limited assist into bed.
11 The CAH is substantially in compliance with the following SNF requirements contained in subpart B of part 483 of this chapter: Comprehensive assessment, comprehensive care plan, and discharge planning ( (b), (k), and (l) of this chapter, except that the CAH is not required to use the resident assessment instrument (RAI) specified by the State that is required under (b), or to comply with the requirements for frequency, scope, and number of assessments prescribed in (b) of this chapter). SOM Appendix W; C-0360; (d) SNF Services


12 THREE KEY ELEMENTS COMPREHENSIVE ASSESSMENT COMPREHENSIVE CARE PLAN DISCHARGE PLANNING 12
13 The facility must conduct initially and periodically a comprehensive, accurate, standardized, reproducible assessment of each resident s functional capacity. State Operations Manual Appendix W - Survey Protocol, Regulations and Interpretive Guidelines for Critical Access Hospitals (CAHs) and Swing-Beds in CAHs
14 (b) Comprehensive assessment. (1) Resident assessment instrument A facility must make a comprehensive assessment of a resident s needs The assessment must include at least the following: (i) Identification and demographic information
15 (ii) Customary routine (iii) Cognitive patterns (iv) Communication (v) Vision (vi) Mood and behavior patterns (vii) Psychosocial well-being (viii) Physical functioning and structural problems
16 (ix) Continence (x) Disease diagnoses and health condition. (xi) Dental and nutritional status (xii) Skin condition (xiii) Activity pursuit (xiv) Medication. (xv) Special treatments and procedures (xvi) Discharge potential
17 (xvii) Documentation of summary information regarding the additional assessment performed through the resident assessment protocols (xviii) Documentation of participation in assessment State Operations Manual Appendix W - Survey Protocol, Regulations and Interpretive Guidelines for Critical Access Hospitals (CAHs) and Swing-Beds in CAHs

18 The assessment process must include direct observation and communication with the resident, as well as communication with licensed and non-licensed direct care staff members on all shifts.
19 Minimum Data Set (MDS) definition: A core set of screening, clinical and functional status elements including common definitions and coding categories, which forms the foundation of a comprehensive assessment..rai Manual; Chapter 1; page 6

20 The MDS should be used as a guideline for Swing Bed documentation. The actual MDS does not have to be completed but rather the components used as a documentation template.

21
22 CAH-based Swing Beds are costreimbursed No MDS Assessment is required for Medicare billing Exempt from SNF PPS Consolidated Billing provisions
23 Patient must have prior qualifying inpatient hospital stay of at least 3 days Qualifying stay does not count time in outpatient status (observation) Can be more than one hospital, but must be at least 3 consecutive days This is reported with occurrence span code 70 in FL Reference IOM , Chapter 8, Section 2
24 30 Day Transfer Requirement Skilled care must start within 30 days of qualifying stay Medically predictable and appropriate delayed admissions Readmissions to same or other facility Returned to skilled care within days 1-30 No new qualifying stay Days Reference IOM , Chapter 8, Sections and
25 Swing Beds Part A Only No Part B benefit in Swing Beds Switch to hospital provider number Type of bill = 12x Billable inpatient Part B services c04.pdf (Section 240)
26 Although there are items excluded from a PPS swing bed program (i.e., CT scan), all charges while the patient is in a CAH s swing bed should be included on the swing bed claim, regardless of the reason for the service, the findings, or whether additional services were required. Social Security Act 1888(e)(7), 1883(b)(3), 42 CFR , MLN Matters SE0606
27 If your MAC provides conflicting information they are basing it on the Balanced Budget Act of 1997 which required swing beds to be incorporated into the SNF PPS beginning July 1, Those rural facilities must use the MDS and bill services under RUG.
28 Swing Bed Bill Types 180 Non-Covered Stay 181 Admit to Discharge claim 182 Interim first claim (status 30) 183 Interim subsequent claims (status 30) 184 Interim last claim Patient status would be discharged/expired 12X Ancillary hospital claim Part A benefits exhaust Non-skilled level of care
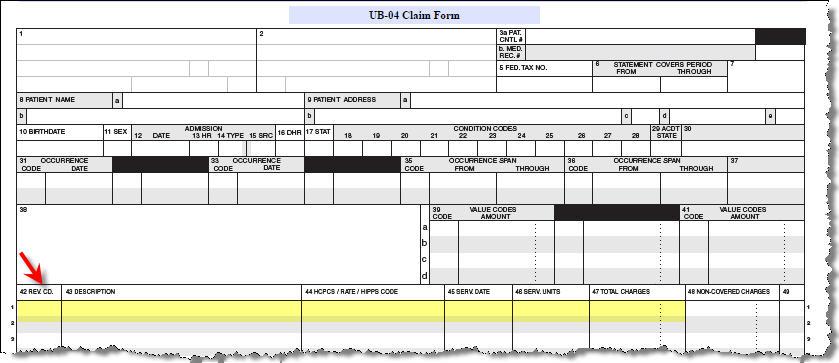
29 Revenue Code Examples: Room & Board Pharmacy Lab/Chemistry Physical Therapy Physical Therapy Eval-0424 Supplies Reference: , Chapter 6, Section 20
30

31 All CAH swing bed SNF-level care bills are submitted and processed with a "z" in the third position of the provider number.

32 Don t forget about these requirements: Physician Certification/Re-certification MSP-Medicare Secondary Payer Consent to Treat/Bill CMS R-193-Important Message from Medicare NOMNC-CMS Notice of Medicare Noncoverage
33 Swing Bed Medicare Advantage (MA) Claims Swing Bed (SB) providers must submit covered claims with condition code 04 (in FL 18-28, information only bill) for beneficiaries enrolled in MA plans and receiving skilled care in order to take benefit days from beneficiary and/or update beneficiary s benefit period in the Common Working File (CWF) IOM, Chapter 6, Section and CR 5653
34 Billing for Leave of Absence (LOA) Away at Midnight Beneficiary is on a Leave of Absence (LOA) Benefit Day is NOT Taken 30-day transfer requirements Discharge bill if patient doesn t return Date of discharge is date the individual actually left facility
35 LOA Claim Coding: Occurrence Span Code 74 Non-covered days in FL with value code 81 Revenue code 018X with no charges Do NOT include LOA days in 12X revenue code line
36 Benefits Exhaust, No-Pay and Demand Bills IOM, , Chapter 6, Section Full Benefits Exhaust Claims no benefit days remain for the billing period (statement covers from/through dates) Partial Benefits Exhaust Claims only one or some days are available for the billing period (statement covers from/through dates) Must be submitted monthly by calendar month
37 Benefits Exhaust Claims Use appropriate covered type of bill (FL 4)(181, 182, 183, 184) Note: Do not use bill types 180 (Swing Beds) Bill all days and charges as covered- Covered/Coinsurance Days Occurrence Span Code 70 (FL35-37)with the qualifying hospital stay dates Value Code 09 or 11 (FL 39-41), as applicable to coinsurance days with dollar amount Occurrence code 22 (date active care ended) Patient status = 30 (still a patient)
38 No-Payment Claims Claims for patients no longer at a skilled level of care Two options Patient dropped to non-skilled care within the month, needs denial for other insurance Patient previously dropped to non-skilled care
39 No-Payment Claims-180 TOB Denial Notice Type of Bill 180 (no-payment bill) Statement covers from-through dates depend on billing frequency Days and charges all entered as non-covered Condition code 21 (billing for denial) Occurrence Span Code 74 with applicable dates Patient status code as appropriate
40 No-Payment Claims-180 TOB Demand Bills TOB 180 Patient in certified bed Days and charges submitted as non-covered Condition code 20 (demand bill) Occurrence Span Code 74 & applicable dates Patient status code as appropriate
41 If expedited review has taken place, include appropriate Condition Code on both denial claims and demand claims C3 partial approval C4 admission denied C7 extended authorization
42 Common Demand/ No Pay Errors No submission of no-pay claims after 100 days used No ABN submitted No documentation that beneficiary/family wants demand bill submitted Incorrect usage of condition code 20 and 21 Billing ancillary services prior to demand bill processed Claim submitted after expedited review with no condition codes C3, C4 or C7
43 Recovery Audit Contractor The Recovery Audit Program s mission is to reduce Medicare improper payments through the efficient detection and collection of overpayments, the identification of underpayments and the implementation of actions that will prevent future improper payments.
44 The purpose of this contract will be to support the Centers for Medicare & Medicaid Services (CMS) in completing this mission. The identification of underpayments and overpayments and the recoupment of overpayments will occur for claims paid under the Medicare program for services for which payment is made under part A or B of title XVIII of the Social Security Act. The CMS expects that Recovery Auditors review all claim types to assist the Agency in lowering the error rate and in identifying improper payments that have the greatest impact on the Trust Fund. Statement of Work for the Recovery Audit Program
45 OIG has focused its efforts on identifying and offering recommendations to reduce improper payments, prevent and deter fraud, and foster economical payment policies. Future planning efforts for FY 2016 and beyond will include: additional oversight of hospice care, including oversight of certification surveys and hospice-worker licensure requirements; oversight of Skilled Nursing Facilities (SNF) compliance with patient admission requirements; and evaluation of CMS s Fraud Prevention System 45
46 CERT-Comprehensive Error Rate Testing ZPICs-Zone Program Integrity Contractor MAC-Medicare Administrative Contractor(FI) GAO-Government Accountability Office

47 QUESTIONS
48 CMS LINKS NetworkMLN/MLNProducts/downloads/CritAccessHospfctsht.pdf NetworkMLN/MLNProducts/downloads/SwingBedFactsheet.pdf NetworkMLN/MLNProducts/downloads/RuralChart.pdf NetworkMLN/MLNProducts/downloads/CritAccessHospfctsht.pdf
49 REFERENCES Medicare Benefit Policy Manual, CMS IOM Publication , Chapters 1,6,8 and 10 Medicare Claims Processing Manual, CMS Publication , Chapters 1,3,4 and 15; IOM, , Chapter 1; Section 50.2; Chapter 6. SOM Appendix W
50 CAH RESOURCES CMS CAH Webpage - A Hs.html State Operation Manual Chapter Two - s om107c02.pdf
51 GPS HEALTHCARE CONSULTANTS Lisa Pando, RN, BA, CCRN, CLNC, C-DONA, RAC-CT, AHIMA Approved ICD-10 Trainer Senior Consultant Kerry Dunning, MHA, MSH, CPAR, RAC-CT Chief Senior Services Officer
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Webinar Etiquette. Webinar Resources
 Georgia State Office of Rural Health & HomeTown Health, LLC Welcome you to the: Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds
Georgia State Office of Rural Health & HomeTown Health, LLC Welcome you to the: Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #21 Compliance = Confidence! Tuesday, August 6 2:30 to 4:30 p.m. Diplomat 1 & 2 Upon completion of this presentation,
Annual Leadership Institute August 25, Triple Check: A Process for Preventing False Claims
 Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Alabama Rural Health Conference 03/25/2010
 1 This resource is not a legal document. This presentation was prepared as a tool to assist our providers. This presentation was current at the time it was created. Although every reasonable effort has
1 This resource is not a legal document. This presentation was prepared as a tool to assist our providers. This presentation was current at the time it was created. Although every reasonable effort has
Public Policy HCA Public Policy No
 Public Policy HCA Public Policy No.2-2014 TO: FROM: RE: HCA CHHA & LTHHCP PROVIDER MEMBERS PATRICK CONOLE, VICE PRESIDENT, FINANCE & MANAGEMENT UPDATES FROM NGS HOME HEALTH ADVISORY MEETING DATE: MARCH
Public Policy HCA Public Policy No.2-2014 TO: FROM: RE: HCA CHHA & LTHHCP PROVIDER MEMBERS PATRICK CONOLE, VICE PRESIDENT, FINANCE & MANAGEMENT UPDATES FROM NGS HOME HEALTH ADVISORY MEETING DATE: MARCH
The Medicare Admissions Process and Strategies for Success. Your Speakers
 The Medicare Admissions Process and Strategies for Success Leading Age Michigan 2014 Annual Leadership Institute Thursday, August 14, 2014 10:45 am 11:45 am 1 Your Speakers Betsy Anderson, President FR&R
The Medicare Admissions Process and Strategies for Success Leading Age Michigan 2014 Annual Leadership Institute Thursday, August 14, 2014 10:45 am 11:45 am 1 Your Speakers Betsy Anderson, President FR&R
MDS Language Impacts CAHs
 MDS Language Impacts CAHs April 2014 Kerry Dunning, MHA, MSH, CPAR, RAC-CT Sr VP, Long Term Care Division GPS Healthcare Consultants Objectives To Sufficiently Understand: Medicare intent for documentation
MDS Language Impacts CAHs April 2014 Kerry Dunning, MHA, MSH, CPAR, RAC-CT Sr VP, Long Term Care Division GPS Healthcare Consultants Objectives To Sufficiently Understand: Medicare intent for documentation
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
Medicare Recovery Audit Contractors. Chicago, IL August 1, 2008
 Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
General Inpatient Level of Care: Managing Risks
 General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor. NJHFMA Finance for Clinicians Session March 24, 2016
 1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
More than a Century of Legal Experience
 Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
8/6/2013. More than a Century of Legal Experience. Agenda
 Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Swing Bed Services: 3 Day Qualifying Stays, Medically Necessary Admissions, and Observation Services Oh My!!! August 13, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience This
Addressing Documentation Insufficiencies
 Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Continuing Education Unit Conditions
 Georgia State Office of Rural Health & HomeTown Health Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds in CAH Hospitals: SKILLED
Georgia State Office of Rural Health & HomeTown Health Best Practices for Compliance & Efficiency 2016-2017 Rural Swing Bed Management (RSBM) Training Program Use of Swing Beds in CAH Hospitals: SKILLED
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
4/20/2015. NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals. Today s Objectives. Background
 NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1
 PEPPER to Support Auditing and Monitoring Efforts: Session 1") Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Topics. Overview of the Medicare Recovery Audit Contractor (RAC) Understanding Medicaid Integrity Contractor
 Understanding Medicaid Integrity Contractor") RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
Using SNF Data to Manage Federal & State Audit Initiatives
 Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
Using SNF Data to Manage Federal & State Audit Initiatives 2012 OIG & GAO Reports In 2009 OIG estimated that 47% of claims had misreported information on the MDS that caused significant errors in Billing
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
More than a Century of Legal Experience
 Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
6/25/2013. Knowledge and Education. Objectives ZPIC, RAC and MAC Audits. After attending this presentation, the attendees will be able to :
 Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
SNF Consolidated Billing Exclusions/Inclusions
 SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Cotiviti Approved Issues List as of February 26, 2018
 Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
RAC Audits and Denials Management WHCA Fall Conference September 9, 2014
 JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
JoLynn Munro, MS,OTR/L, Regional Vice President Infinity Rehab Carolyn Staples, CCC/SLP, Area Rehab Director Infinity Rehab RAC Audits and Denials Management WHCA Fall Conference September 9, 2014 Objectives
MLN Matters Number: MM6699 Related Change Request (CR) #: 6699
 #: 6699") News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Recovery Audit Contractors (RACs) and Medicare. The Who, What, When, Where, How and Why?
 and Medicare. The Who, What, When, Where, How and Why?") Recovery Audit Contractors (RACs) and Medicare The Who, What, When, Where, How and Why? 1 Agenda What is a RAC? Will the RACs affect me? Why RACs? What does a RAC do? What are the providers options? What
Recovery Audit Contractors (RACs) and Medicare The Who, What, When, Where, How and Why? 1 Agenda What is a RAC? Will the RACs affect me? Why RACs? What does a RAC do? What are the providers options? What
OIG Work Plan Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant
 OIG Work Plan 2014 Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant Agenda Introduction to, and how to interpret, the OIG Work Plan Review of Hospital
OIG Work Plan 2014 Darci Friedman, Director of Regulatory Products Lynne Rinehimer, Sr. Healthcare Solutions Consultant Agenda Introduction to, and how to interpret, the OIG Work Plan Review of Hospital
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
Compliance Issues under Medicare Prospective Payment for Nursing Facilities. Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group
 Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
Swing Bed More Questions AUGUST 3, 2018 BUILDING LEADERS TRANSFORMING HOSPITALS IMPROVING CARE HTS3 2018
 Swing Bed More Questions AUGUST 3, 2018 BUILDING LEADERS TRANSFORMING HOSPITALS IMPROVING CARE 1 Carolyn began her healthcare career as a staff nurse in Intensive Care. She has worked in a variety of staff,
Swing Bed More Questions AUGUST 3, 2018 BUILDING LEADERS TRANSFORMING HOSPITALS IMPROVING CARE 1 Carolyn began her healthcare career as a staff nurse in Intensive Care. She has worked in a variety of staff,
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
RURAL SWING BED MANAGEMENT (RSBM) TRAINING PROGRAM
 TRAINING PROGRAM") RURAL SWING BED MANAGEMENT (RSBM) The Georgia State Office of Rural Health and HOMETOWN HEALTH Present: The Need for Rural Swing Bed Training One of the challenges that rural hospitals face today is a
RURAL SWING BED MANAGEMENT (RSBM) The Georgia State Office of Rural Health and HOMETOWN HEALTH Present: The Need for Rural Swing Bed Training One of the challenges that rural hospitals face today is a
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Medical Review Preparation. Supporting Rehab RUG Levels. Some of the Medical Review Types. >90% of Medicare Part A stays are skilled by rehab
 Supporting Rehab RUG Levels Through Interdisciplinary Documentation >90% of Medicare Part A stays are skilled by rehab Some of the Medical Review Types Review Entity Pre-pay Post Pay RAC Recovery Audit
Supporting Rehab RUG Levels Through Interdisciplinary Documentation >90% of Medicare Part A stays are skilled by rehab Some of the Medical Review Types Review Entity Pre-pay Post Pay RAC Recovery Audit
5010 Changes. CHAMPS Changes 01/01/12 4/4/12. Copyright Kearney & Associates, Inc 1. 01/01/2012 Change From 4010 to 5010
 Flowing Change Julie Kearney Kearney & Associates, Inc. 5010 Changes 01/01/2012 Change From 4010 to 5010 Went From Allowing 8 Diagnosis to 12 Diagnosis Postponed fines, and compliance until 04/01/2012
Flowing Change Julie Kearney Kearney & Associates, Inc. 5010 Changes 01/01/2012 Change From 4010 to 5010 Went From Allowing 8 Diagnosis to 12 Diagnosis Postponed fines, and compliance until 04/01/2012
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
MDS Accuracy and Compliance: Where There s Smoke
 MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Hospice House Network Inpatient Conference
 Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
Medicare Hospice Billing 2015 & Beyond!
 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Zone Program Integrity Program & Recovery Audit Contractors
 Zone Program Integrity Program & Recovery Audit Contractors Advance Planning and Responsive Tools. AHLA Long Term Care and the Law Program Feb 26, 2013 Presented by: Brain Daucher Esq. Sheppard Mullin
Zone Program Integrity Program & Recovery Audit Contractors Advance Planning and Responsive Tools. AHLA Long Term Care and the Law Program Feb 26, 2013 Presented by: Brain Daucher Esq. Sheppard Mullin
CRITICAL ACCESS HOSPITAL SWING BED PROGRAM
 CRITICAL ACCESS HOSPITAL SWING BED PROGRAM Operational and Management Strategies March 1, 2016 Andrea Elliott, CPA Senior Managing Consultant aelliott@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing Consultant
CRITICAL ACCESS HOSPITAL SWING BED PROGRAM Operational and Management Strategies March 1, 2016 Andrea Elliott, CPA Senior Managing Consultant aelliott@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing Consultant
The following is a summary of each of the updates from the meeting.
 This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
2013 OIG Work Plan. Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas
 2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
CMS , Ch 13, Sec
 Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change. November 22, 2013
 Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Effective with Admissions August 1, 1992 OFFICE OF MEDICAL ASSISTANCE PROGRAMS DEPARTMENT OF HUMAN SERVICES
 Manual for Concurrent Hospital Review of Inpatient Hospital Services Effective with Admissions August 1, 1992 OFFICE OF MEDICAL ASSISTANCE PROGRAMS DEPARTMENT OF HUMAN SERVICES Last Revision Date June
Manual for Concurrent Hospital Review of Inpatient Hospital Services Effective with Admissions August 1, 1992 OFFICE OF MEDICAL ASSISTANCE PROGRAMS DEPARTMENT OF HUMAN SERVICES Last Revision Date June
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness. October 12, 2009
 Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Section A Identification Information
 r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
CRS Report for Congress Received through the CRS Web
 CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
Medicare Consolidate Billing & Overview
 Medicare Consolidate Billing & Overview Julie Kearney, Kearney & Associates Consolidated Billing The Balanced Budget Act of 1997, Congress mandated that payment for the majority of services provided to
Medicare Consolidate Billing & Overview Julie Kearney, Kearney & Associates Consolidated Billing The Balanced Budget Act of 1997, Congress mandated that payment for the majority of services provided to
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts
 PEPPER to Support Auditing and Monitoring Efforts") Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
Using the New Home Health Agency (HHA) PEPPER to Support Auditing and Monitoring Efforts July 30, 2015 Kimberly Hrehor 2 Agenda History and basics of PEPPER HHA PEPPER target areas Percents, rates and
Surviving Targeted Probe & Educate
 Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
Surviving Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe & Educate
State Medicaid Recovery Audit Contractor (RAC) Program
 Program") State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION
 HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION Mary Carr, BSN,MPH V.P. for Regulatory Affairs National Association for Home Care & Hospice October 19, 2014 Proposed rule HH COPS Federal Register
HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION Mary Carr, BSN,MPH V.P. for Regulatory Affairs National Association for Home Care & Hospice October 19, 2014 Proposed rule HH COPS Federal Register
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY
 STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
Combatting Denials. NJ HFMA January 10, 2017
 Combatting Denials NJ HFMA January 10, 2017 1 Denial Challenges PAYER INDUCED Aggressive Commercial Payer Denials (Concurrent and Retrospective) Pre-Payment Review Denials for Medicare Unilateral Payer
Combatting Denials NJ HFMA January 10, 2017 1 Denial Challenges PAYER INDUCED Aggressive Commercial Payer Denials (Concurrent and Retrospective) Pre-Payment Review Denials for Medicare Unilateral Payer
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
WHAT YOU NEED TO KNOW! CMS (Medicare)! and! The Joint Commission CSC! Updates!
! and! The Joint Commission CSC! Updates!") !!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
!!! Lombardi Hill Consulting Group WHAT YOU NEED TO KNOW!! CMS (Medicare)! and! The Joint Commission CSC! Updates! Debbie Lombardi Hill, FAHA Dunedin, Florida w May 4, 2016 Lombardi Hill Consulting Group!
New in Current payment risks. Tips & strategies. Revenue Cycle: The Ca$h Connection. CPAs & ADVISORS
 Revenue Cycle: The Ca$h Connection CPAs & ADVISORS M. Aaron Little, CPA Managing Director Springfield, MO mlittle@bkd.com New in 2017 Current payment risks Tips & strategies 2 1 3 Payment rates SN HCPCS
Revenue Cycle: The Ca$h Connection CPAs & ADVISORS M. Aaron Little, CPA Managing Director Springfield, MO mlittle@bkd.com New in 2017 Current payment risks Tips & strategies 2 1 3 Payment rates SN HCPCS
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
routine services furnished by nursing facilities (other than NFs for individuals with intellectual Rev
 4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
Pharmacy Compliance: Beyond Med Errors. Overview
 Pharmacy Compliance: Beyond Med Errors Daniel P. Fitzgerald, Senior Attorney Litigation & Regulatory Law Department Walgreen Co. James S. Mathis, Esq., Nashville, TN Overview Med Errors & Controlled Substances
Pharmacy Compliance: Beyond Med Errors Daniel P. Fitzgerald, Senior Attorney Litigation & Regulatory Law Department Walgreen Co. James S. Mathis, Esq., Nashville, TN Overview Med Errors & Controlled Substances
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid
 Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
Nursing Facility UB-04 Paper Billing Guide
 Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 2859 Date: January 17, 2014
 Centers for Medicare & Medicaid Services (CMS) Transmittal 2859 Date: January 17, 2014") CMS Manual System Pub 100-04 Medicare Claims Processing Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 2859 Date: January 17, 2014 Change Request
CMS Manual System Pub 100-04 Medicare Claims Processing Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 2859 Date: January 17, 2014 Change Request
Home Health Targeted Probe & Educate
 Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
Home Health Targeted Probe & Educate PRESENTED BY: MELINDA A. GABOURY, CEO HEALTHCARE PROVIDER SOLUTIONS, INC. WWW.TARGETEDPROBEANDEDUCATE.COM INFO@HEALTHCAREPROVIDERSOLUTIONS.COM CMS expansion on Probe
2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc.
 2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc. Welcome from Kaiser Permanente It is our pleasure to welcome you as a contracted provider (Provider) participating under
2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc. Welcome from Kaiser Permanente It is our pleasure to welcome you as a contracted provider (Provider) participating under
Home Health Market Overview
 Home Health Market Overview December 2013 Investment banking services are provided by Harris Williams LLC, a registered broker-dealer and member of FINRA and SIPC, and Harris Williams & Co. Ltd, which
Home Health Market Overview December 2013 Investment banking services are provided by Harris Williams LLC, a registered broker-dealer and member of FINRA and SIPC, and Harris Williams & Co. Ltd, which
Roadmap. AAH Best Practices and Mobility Documentation. Policy History. History Continued. History Understanding Documentation
 Roadmap AAH Best Practices and Mobility Documentation May 2008 History Understanding Documentation MAE NCD Key Concepts Audits The WHY of MR CMS Requirements 1 2 Policy History Original National Policy
Roadmap AAH Best Practices and Mobility Documentation May 2008 History Understanding Documentation MAE NCD Key Concepts Audits The WHY of MR CMS Requirements 1 2 Policy History Original National Policy
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged