Medicare Hospice Billing 2015 & Beyond!
|
|
|
- Erika Stevens
- 5 years ago
- Views:
Transcription

 does not meet the sequential billing requirement. Claims must be consecutive.")

1 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first claim. Claims must be submitted sequentially. This means that the prior claim must be processed and in S/LOC P, D or R. A suspended claim (in S/LOC S ) does not meet the sequential billing requirement. Claims must be consecutive. This means there cannot be a skip in days between the prior claim and the subsequent claim. Claims must be submitted monthly. The Medicare Claims Processing Manual (Pub ), Chapter 11, Section 90 states Hospices must bill for their Medicare beneficiaries on a monthly basis. This will significantly reduce errors related to sequential billing. 1
2 Levels of Care Description Revenue Code Unit=Time Routine Home Care Continuous Home Care Inpatient Respite Care General Inpatient Care unit = 1 day 1 unit = 15 minutes 1 unit = 1 day 1 unit = 1 day Routine Home Care (RHC) Hospice is paid the routine home care rate for each day the patient is under the care of the hospice and not receiving one of the other categories of hospice care paid without regard to the volume or intensity 2
3 Continuous Home Care CHC is provided during periods of crisis as needed to maintain the patient in their home. To qualify as CHC, a minimum of 8-hours of care must be provided in a 24-hour period, beginning and ending at midnight. The care does not need to be continuous. Care can be provided by nurses (RN or LPN) and home health aides; however, at least half (50%) of the care must be provided by a nurse. When billing CHC, units are billed to indicate the number of 15-minute increments provided in each 24-hour period of CHC. Example: 8 hours of CHC = 32 units If these criteria are not met (e.g. only 7 hours of care was provided), routine home care must be billed. Inpatient Respite Care Respite care is provided in a hospital, skilled nursing facility, or other inpatient facility, to provide temporary relief to the patient s family members or other caregivers. Respite care should be used on a short-term, occasional basis, when necessary to relieve the caregiver. Respite is payable for up to 5 consecutive days. Days beyond day 5 are billed at the routine rate. More than one respite stay in a billing period is allowed. The day of admission to respite is billed as a respite day. The day of discharge is billed as a routine home care day. If the patient dies while in respite, the day of death is billed as respite. 3
4 General Inpatient Care (GIP) GIP is provided in an inpatient setting to control the patient s pain or manage the symptoms of their terminal illness that cannot feasibly be provided in another setting. The day of admission to GIP is billed as a GIP day. The day of discharge is billed as a routine home care day. If the patient dies while in GIP, the day of death is billed as GIP. Sequential Claim Billing HIC Required: Enter the beneficiary's Health Insurance Claim Number (HICN) TOB Required: Type of bill (system generated). FISS Page 01 defaults the type of bill (TOB) to 81A. You may need to change this depending on the TOB you are entering. 1st Digit 2nd Digit 8 Hospice 1 Hospice (nonhospital based) 2 Hospice (hospital based) 3rd Digit 1 Admit through discharge; 2 Interim first claim 3 Interim continuing claim; 4 Interim last claim NPI Required: Enter your Hospice National Provider Identifier. PAT.CNTL# - Optional: Up to 20 digits are available for you to enter your internal account number for tracking purposes. This number will display on your Remittance Advice or your Electronic Remittance Advice 4
5 Sequential Claim Billing STMT DATES FROM Required: Enter the begin and end dates of the billing period LAST Required: Enter the beneficiary's last name exactly as it appears on the Medicare card or the beneficiary's eligibility file, including any spaces, apostrophes, hyphens or suffixes. FIRST Required: Enter the beneficiary's first name exactly as it appears on the Medicare card or the beneficiary's eligibility file. MI Optional: Enter the beneficiary's middle initial. DOB Required: Enter the beneficiary's date of birth. ADDR 1-6 Required: Enter the beneficiary's full mailing address, including street name and number, post office box number or RFD, city and state. ZIP Required: Enter the beneficiary's 5- or 9- digit zip code. SEX Required: Enter the beneficiary's gender using the appropriate alpha character. M = Male F= Female Sequential Claim Billing MS Optional: Beneficiary's marital status ADMIT DATE Required: Enter the effective date of the hospice election or date of hospice transfer. (must match the Admit date on the NOE or Change) HR Required (DDE ONLY): Hour of Admission Enter the hour of admission (based on a 24-hour clock). If the hour of admission is unknown, enter '01'. TYPE Required: Enter the Priority (Type) of Admission code. 1 Emergency; 2 Urgent; 3 Elective; 4 Newborn 5 Trauma; 9 Information not available SRC Required: Enter a Point of Origin (Source of Admission) code 1 Non-health care facility; 2 Clinic or Physician's office; 4 Transfer from hospital (different facility); 5 Transfer from skilled nursing facility (SNF) or intermediate care facility (ICF); 6 Transfer from another health care facility; 8 Court/Law enforcement; 9 Information not available 5
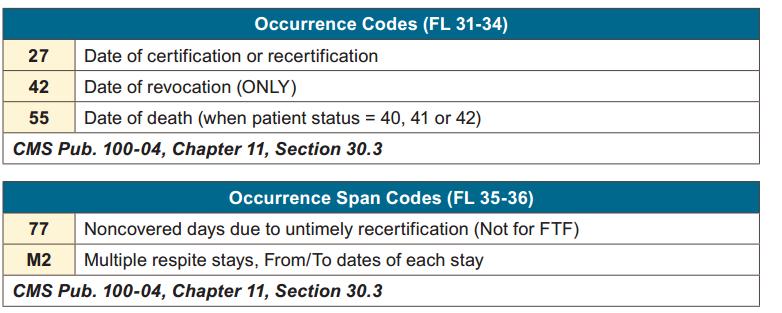
6 Occurrence & Condition Codes Occurrence & Condition Codes 6

.")
7 Sequential Claim Billing FAC.ZIP Required: Facility ZIP code of the provider or the subpart (5- or 9-digit). The ZIP code entered must match the ZIP code in the Master Address field of the provider's address file at Medicare MAC Value Codes Amounts Required: Value code 61 and the core based statistical area (CBSA) code are required when billing routine (revenue code 0651) and/or continuous home care (revenue code 0652). Value code G8 and the CBSA code are required when billing respite (revenue code 0655) and/or general inpatient care (revenue code 0656). Revenue Codes - Visits 7

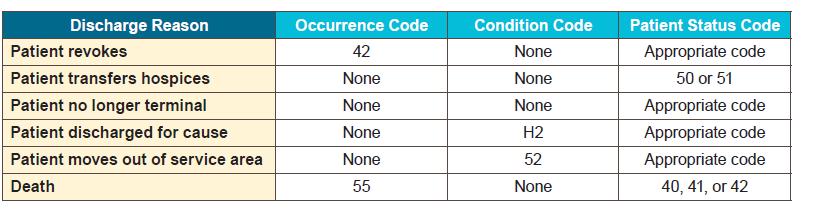
8 Location Codes Location Codes 8


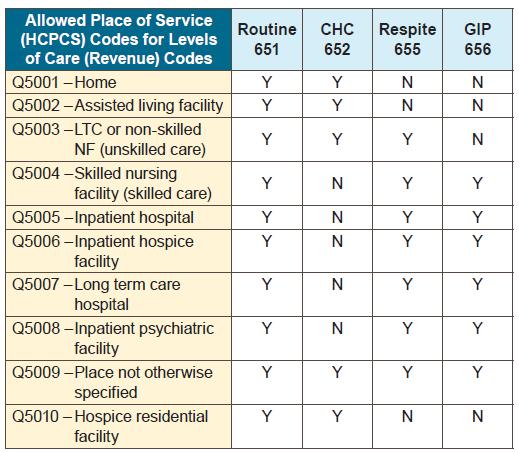
9 Multiple Location Codes If care is rendered at multiple locations, each location is to be identified on the claim with a corresponding HCPCS code For example, routine home care may be provided for a portion of the billing period in the patient s residence and another portion in an assisted living facility Report one revenue code 651 line with HCPCS code Q5001 and another revenue code 651 line with HCPCS code Q5002 Claim Form Locators 9
10 *Attending Physician Update CMS will amend the regulations at (b)(1) and require the election statement to include the patient s choice of attending physician Information identifying the attending physician should be recorded on the election statement in enough detail so that it is clear which physician or NP was designated as the attending physician.hospices have the flexibility to include this information on their election statement in whatever format works best for them, provided the content requirements in (b) are met. Language on the election form should include an acknowledgement by the patient (or representative) that the designated attending physician was the patient s (or representative s) choice. *Attending Physician Update If a patient (or representative) wants to change his or her designated attending physician, he or she must follow a procedure similar to that which currently exists for changing the designated hospice. Specifically, the patient (or representative) must file a signed statement, with the hospice, that identifies the new attending physician in enough detail so that it is clear which physician or NP was designated as the new attending physician. The statement needs to include the date the change is to be effective, the date that the statement is signed, and the patient s (or representative s) signature, along with an acknowledgement that this change in the attending physician is the patient s (or representative s) choice. The effective date of the change in attending physician cannot be earlier than the date the statement is signed. 10
11 *Attending Physician Update CMS provides clarification that attending physician status need not change when a patient enters GIP. If attending physician is not available, hospice physician fills in. Hospice should document in medical record situations where attending is no longer willing or available to follow patient. Hospice should inform patient or representative that new attending may be chosen. CMS will issue educational materials to alert hospices and treating physicians about inappropriate use of attending physician modifier on claim and update beneficiary materials. General Inpatient Care (GIP) Visits Inpatient Facility Identification Post-Mortem Visits Injectable Drugs Non-Injectable Drugs Infusion Pumps 11

 Q5005 inpatient hospital Q5007 long term care hospital Q5008")

12 General Inpatient (GIP) Visit Changes Claims must report line item visits provided to patients receiving GIP Only by hospice employed personnel Includes visits by all billable disciplines of service: Nurses, aides, social workers, social worker phone calls, & physical, occupational & speech-language pathologists Visit reporting the same as for routine & continuous home care Includes visits provided to patients in billable GIP locations Q5004 skilled nursing facility (SNF) Q5005 inpatient hospital Q5007 long term care hospital Q5008 inpatient psychiatric facility Visits must be reported in 15-minute increments Inpatient hospice facility patients receiving GIP excluded from line-item reporting requirement Q5006 = HCPCS location code No changes to current visit reporting requirements Visits remain reported by week 12
13 GIP UB04 Claim Detail GIP - Facility OTHER THAN Hospice Inpatient Facility 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G GIP - Hospice Inpatient Facility 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- Inpatient Hospice Q Skilled Nursing G Inpatient Facility Identification Claims must report inpatient facility NAME, ADDRESS & National Provider Identifier (NPI) number Only when facility is different than provider submitting claim Includes claims billed with inpatient locations: Q5003 Nursing facility (NF), patient receiving unskilled care Q5004 SNF, patient receiving skilled care Q5005 inpatient hospital Q5006 inpatient hospice facility, only if facility is not same as hospice submitting claim Q5007 long term care hospital Q5008 inpatient psychiatric facility 13
 for corrections if inpatient facility identifying information missing When the patient has received care in more than one facility during the billing month, the hospice shall report the NPI")
14 Inpatient Facility Identification Reported in HIPAA 5010 electronic claim format - Other Provider Location Loop 2310 E Claims billed with inpatient facility location codes will be returned (RTP) ( T Status) for corrections if inpatient facility identifying information missing When the patient has received care in more than one facility during the billing month, the hospice shall report the NPI of the facility where the patient was last treated. Page 3 DDE Entry Hospice 14
15 Post Mortem Visits Claims must report post-mortem visits when occurring on date of death - after time of death Date of death is defined as the date of death that is reported on the death certificate Includes visits performed by hospice employed nurses, aides, social workers & therapists Regardless of level of care or site of service Requires visits to be reported in 15-minute increments Post Mortem Visits Requires modifier code PM Requires split visit billing if death occurs during visit Hospices shall report hospice visits that occur before death on a separate line from those which occur after death. Excludes visits occurring on dates after the date of death Q&A #5 - Would an on call nurse pronouncement visit be considered a post-mortem visit? Answer: Any time prior to the pronouncement would be reported as an actual visit. Time from the pronouncement and beyond would be reported as a post-mortem visit. Source: CGS 15
16 GIP UB04 Claim Detail GIP - Facility with Post-Mortem Visit 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G Skilled Nursing-Post-Mortem G0154PM GIP - Facility with SPLIT Post-Mortem Visit 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G Skilled Nursing G Skilled Nursing-Post-Mortem G0154PM Injectable Drugs Claims must report injectable prescription drugs Requires line-item reporting on claim per fill Requires revenue code 0636 Requires applicable HCPCS code Requires applicable units Should represent amount filled based on drug & HCPCS definition Requires charge amount Excludes over-the-counter (OTC) drugs 16


 qualifier HCPCS code not required Requires applicable units")
17 GIP UB04 Claim Detail GIP - Facility with Injectable Drugs 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G Inj Lorazepam, 2 mg J Non-Injectable Drugs Claims must report non-injectable prescription drugs (excludes OTC drugs) Requires line-item reporting on claim per fill Requires revenue code 0250 Requires National Drug Code (NDC) qualifier HCPCS code not required Requires applicable units Should represent amount filled based on drug definition Requires charge amount 17
18 GIP UB04 Claim Detail GIP - Facility with Non-Injectable & Injectable Drugs 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G Inj Lorazepam, 2 mg J N UN100 (not applicable) Begin by entering the qualifier N4 immediately followed by the 11-digit NDC code. The NDC codes must be in the format required by HIPAA guidelines, do not report hyphens. It may be necessary to pad NDC numbers with zeroes in order to report eleven digits. Next enter the two digit unit of measurement qualifier immediately followed by the. numeric quantity administered to the patient (amount of fill). Measurement Qualifiers: F2 International Unit - - GR Gram - - ML Milliliter - - UN Units CR 8358 Revisions 01/31/14 New Clarification - Hospices shall report multi-ingredient compound prescription drugs (non-injectable) using revenue code The hospice shall specify the same prescription number for each ingredient of a compound drug according to the 837i guidelines in loop In addition, the hospice shall provide the NDC for each ingredient in the compound; the NDC qualifier represents the quantity of the drug filled (meaning the amount dispensed) and shall be reported as the unit measure. 18
19 Infusion Pumps Claims must report infusion pumps Requires line-item reporting on claim per each pump order Requires revenue codes 029X 0290 for general equipment classification 0291 for rental 0292 for purchase of new equipment 0293 for purchase of used equipment 0299 for other equipment Requires applicable HCPCS code Requires applicable units Requires charge amount Infusion Pumps Claims must also report related medication necessary for effective use of pump Requires line-item reporting per medication fill Requires revenue code 0294 Requires applicable HCPCS code Requires applicable units Should represent amount filled based on drug definition Requires charge amount Excludes OTC drugs & nutrition 19



20 GIP UB04 Claim Detail GIP - Facility with Injectable Drugs & Infusion Pump 42 REV.CD 43 DESCRIPTION 44 HCPCS/RATE/HIPPS 45 SERV. DATE 46 SERV. UNITS 0656 GIP- SNF Q Skilled Nursing G Skilled Nursing G Inj Lorazepam, 2 mg J Infusion Pump Rental E Infusion Saline 1000cc J Hospice Coding Edits & Issues 20
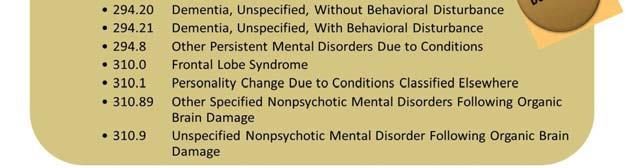
21 Symptoms, Signs & Ill-Defined Conditions CMS has stated that the following are NOT acceptable as Primary Diagnosis for Hospice (edits in place 10/01/14) Failure to thrive Adult failure to thrive Debility Unspecified Other ill-defined conditions Other unknown and unspecified cause of morbidity or mortality Symptoms, Signs, and Ill-Defined Conditions, such as debility or adult failure to thrive, does not encompass the comprehensive, holistic nature of the assessment and care to be provided under the Medicare hospice benefit. Coding Edits for Primary Diagnosis claims received with these codes in the principal diagnosis field will be returned to the provider for more definitive coding of the principal diagnosis and additional diagnoses, effective for claims dated on or after October 1, 2014.This will not affect claims submitted before October 1, Debility and adult failure to thrive may be reported on the hospice claims as additional diagnoses in the appropriate claim fields. Although claims will not be returned to the provider until the start of FY 2015, we remind hospices that they are currently, and have always been, required to code all related diagnoses in the additional coding fields on the hospice claim and thus should be doing so now. *Federal Register Center for Medicare & Medicaid Services42 CFR Part 418 Medicare Program; FY 2014 Hospice Wage Index and Payment Rate Update; Hospice Quality Reporting Requirements; and Updates on Payment Reform; Final Rule 21



22 CR 8877 Attachment A Codes Not Allowed as Principal CR 8877 Attachment A Codes Not Allowed as Principal 22
23 Related Conditions Defined Clinically, related conditions are any physical or mental condition(s) that are related to or caused by either the terminal illness or the medications used to manage the terminal illness. *Paolini, DO, Charlotte. (2001). Symptoms Management at End of Life. JAOA. 101(10). p CMS' Hospice Claims Processing manual requires that hospice claims include other diagnoses as required by ICD-9-CM Coding Guidelines (IOM , chapter 11, section 30.1, available at): Guidance/Guidance/Manuals/Downloads/clm104c11.pdf Coding Guidelines Hospice Other diagnoses is interpreted as additional conditions that affect patient care in terms of requiring: Clinical evaluation; or therapeutic treatment; or diagnostic procedures; or extended length of hospital stay; or increased nursing care and/or monitoring. *Official Guidelines for Coding and Reporting Hospices should report on hospice claims all coexisting or additional diagnoses that are related to the terminal illness; they should not report coexisting or additional diagnoses that are unrelated to the terminal illness. *Coding Clinic - AHIMA 23
24 Proposed 2016 Changes Changes in County Designations: CMS reports that the use of the new delineations will result in new CBSAs, 37 counties that were urban and are now rural, 105 counties that were rural and are now urban, and existing CBSAs that have been split apart. Transition Period: CMS proposes that there will be a one year transition period to the new delineations, at 50% at the old CBSA or rural value and 50% at the new value. Rural Floor: The 0.8 rural floor has been maintained and applies to counties designated as rural. For rural counties with a wage index value under 0.8, the hospice s wage index receives a 15% increase up to 0.8 Proposed 2016 Changes Tiered Routine Home Care Rate: CMS is proposing to establish two tiers of routine home care payments, one payment for days 1-60 and a reduced payment for days 61+. This two-tiered approach is a proposed rule! Service Intensity Add-on: CMS also proposes to establish a service intensity add-on (SIA) for patients in the last 7 days of life, if certain criteria are met. The rate is proposed to be established at the hourly continuous home care rate of $39.44 and limited to: a minimum of 1 hour and a maximum of 4 hours in a 24 hour period. The proposed criteria include services provided only by an RN or social worker services provided to patients not residing in a skilled nursing facility or nursing facility 24
25 MSP on/materials/msp.html on/materials/mspresources.html Guidance/Guidance/Manuals/downloads/ msp105c03.pdf Questions 25


26 Thank You For Listening! Healthcare Provider Solutions, Inc. 810 Royal Parkway, Suite 200 Nashville, TN
Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services (CMS) Transmittal 2867 Date: February 5, 2014
 Centers for Medicare & Medicaid Services (CMS) Transmittal 2867 Date: February 5, 2014") CS anual System Pub 100-04 edicare Claims Processing Department of Health & Human Services (DHHS) Centers for edicare & edicaid Services (CS) Transmittal 2867 Date: February 5, 2014 Change Request 8569
CS anual System Pub 100-04 edicare Claims Processing Department of Health & Human Services (DHHS) Centers for edicare & edicaid Services (CS) Transmittal 2867 Date: February 5, 2014 Change Request 8569
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims
 Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
CMS CR 6440: Additional Documentation on Hospice Claims Related Q&A s
 CMS CR 6440: Additional Documentation on Hospice Claims Related Q&A s ID# 8901 - Published 02/13/2008 Updated 04/09/2010 What constitutes a patient care visit that is reasonable and necessary? A reasonable
CMS CR 6440: Additional Documentation on Hospice Claims Related Q&A s ID# 8901 - Published 02/13/2008 Updated 04/09/2010 What constitutes a patient care visit that is reasonable and necessary? A reasonable
NATIONAL ASSOCIATION FOR HOME CARE & HOSPICE/ HOSPICE ASSOCIATION OF AMERICA
 NATIONAL ASSOCIATION FOR HOME CARE & HOSPICE/ HOSPICE ASSOCIATION OF AMERICA ADDITIONAL DATA REPORTING REQUIREMENTS FOR HOSPICE CLAIMS Comparison of CMS Proposed and Final Requirements Change Request 8358/Transmittal
NATIONAL ASSOCIATION FOR HOME CARE & HOSPICE/ HOSPICE ASSOCIATION OF AMERICA ADDITIONAL DATA REPORTING REQUIREMENTS FOR HOSPICE CLAIMS Comparison of CMS Proposed and Final Requirements Change Request 8358/Transmittal
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Subject: Updated UB-04 Paper Claim Form Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
HOW TO STAY INFORMED: MEDICARE UPDATES & REMINDERS FROM CGS
 HOW TO STAY INFORMED: MEDICARE UPDATES & REMINDERS FROM CGS NATIONAL ASSOCIATION FOR HOME CARE & HOSPICE 2014 ANNUAL MEETING & EXPOSITION PHOENIX, AZ OCTOBER 19-22, 2014 RECENT MEDICARE CHANGES Home Health
HOW TO STAY INFORMED: MEDICARE UPDATES & REMINDERS FROM CGS NATIONAL ASSOCIATION FOR HOME CARE & HOSPICE 2014 ANNUAL MEETING & EXPOSITION PHOENIX, AZ OCTOBER 19-22, 2014 RECENT MEDICARE CHANGES Home Health
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
 Tacking The New Requirements: NOEs, NOTRs & Designation of the Attending Physician Subscriber Webinar This Round of Changes Let s Get Straight On History & intent Exactly what the new regulatory language
Tacking The New Requirements: NOEs, NOTRs & Designation of the Attending Physician Subscriber Webinar This Round of Changes Let s Get Straight On History & intent Exactly what the new regulatory language
UB-92 Billing Instructions
 August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
National Hospice and Palliative Care OrganizatioN. Facts AND Figures. Hospice Care in America. NHPCO Facts & Figures edition
 National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
National Hospice and Palliative Care OrganizatioN Facts AND Figures Hospice Care in America 2017 Edition NHPCO Facts & Figures - 2017 edition Table of Contents 2 Introduction 2 About this report 2 What
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
Insight into Hospice and PACE
 Insight into Hospice and PACE Defining Hospice Care A form of palliative care designed to provide medical, spiritual and psychological care to individuals facing a life limiting illness. Focuses on caring,
Insight into Hospice and PACE Defining Hospice Care A form of palliative care designed to provide medical, spiritual and psychological care to individuals facing a life limiting illness. Focuses on caring,
Page 1. I. QUESTIONS ABOUT HETs SYSTEM
 CMS Hospice-related Q&A s April 2011 This list is compiled from the CMS Hospice Center (http://www.cms.gov/center/hospice.asp) with questions and answers that were posted or updated in April, 2011. Each
CMS Hospice-related Q&A s April 2011 This list is compiled from the CMS Hospice Center (http://www.cms.gov/center/hospice.asp) with questions and answers that were posted or updated in April, 2011. Each
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
The Medicare Hospice Program: New Billing Requirements & Hot Topics from Your Medicare New England Home Care & Hospice Conference and Trade Show
 The Medicare Program: New Billing Requirements & Hot Topics from Your Medicare New England Home Care & Conference and Trade Show Add doc ctrl no. Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider
The Medicare Program: New Billing Requirements & Hot Topics from Your Medicare New England Home Care & Conference and Trade Show Add doc ctrl no. Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
HOW TO SUBMIT OWCP-04 BILLS TO ACS
 HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
Reference Guide for Hospice Medicaid Services
 Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
Reference Guide for Hospice Medicaid Services for Florida s Statewide Medicaid Managed Care Plans (MMA & LTC) This reference guide is intended to provide general hospice information on Florida Medicaid.
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc.
 HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
HOSPICE TARGETED PROBE & EDUCATE Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. www.targetedprobe&educate.com Targeted Probe and Educate October 1, 2017 Targets providers based on data Can
UB-04 Claim Form Instructions
 UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
State of California Health and Human Services Agency Department of Health Care Services TOBY DOUGLAS Director EDMUND G. BROWN JR. Governor DATE: OCTOBER 28, 2013 ALL PLAN LETTER 13-014 SUPERSEDES ALL PLAN
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
FY 2017 Hospice Proposed Rule. Hospice Regulatory Review May Webinar Agenda. Hospice Regulatory Review
 Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
Hospice Regulatory Review May 2016 Presented by: Deanna Loftus, Director of Regulatory Compliance Liz Silva, Director of Hospice Webinar Agenda CY 2017 Proposed Rule o New Payment Rates o Diagnosis Code
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY
 MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
MEDICARE PROGRAM; FY 2014 HOSPICE WAGE INDEX AND PAYMENT RATE UPDATE; HOSPICE QUALITY REPORTING REQUIREMENTS; AND UPDATES ON PAYMENT REFORM SUMMARY On April 29, 2013, the Centers for Medicare & Medicaid
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY
 STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
STATE HOSPICE ORGANIZATION AND PALMETTO GBA COALITION MEETING SUMMARY For meeting held on August 19, 2010 Included in this report: NCLOS audits update on status Various other audit types (ZPIC) Palmetto
hospic Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals.
 Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
Hospice Care 1 Hospice care is a medical multidisciplinary care designed to meet the unique needs of terminally ill individuals. Hospice care is used to alleviate pain and suffering, and treat symptoms
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Format Specifications For the MHA DMS Publish Date: 11/20/2017
 Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims
 Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices. Presenter. Objectives 08/31/16
 Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
Hot Off the Press! The FY2017 Final Rule & Its Implications for Hospices August 31, 2016 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org
06-01 FORM HCFA WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the
 06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
06-01 FORM HCFA-1728-94 3204 3203. WORKSHEET S - HOME HEALTH AGENCY COST REPORT The intermediary indicates in the appropriate box whether this is the initial cost report (first cost report filed for the
Medical Review: Past, Present and Future
 Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
Medical Review: Past, Present and Future HPCAI Fall Conference Annette Lee of Provider Insights, Inc. 11/5/2013 1 Progressive Corrective Action (PCA) Process designed by CMS, ensures a logical, fair methodology
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
Place of Service Code Description Conversion
 Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
08-16 FORM CMS
 08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
CMS-1500 Billing and Reimbursement. HP Provider Relations/October 2013
 CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
Section A Identification Information
 r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
How to Account for Hospice Reimbursement Changes. Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016
 How to Account for Hospice Changes Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016 marcumllp.com Disclaimer This Presentation has been prepared for informational purposes
How to Account for Hospice Changes Indiana Association for Home & Hospice Care Annual Conference May 10-11, 2016 marcumllp.com Disclaimer This Presentation has been prepared for informational purposes
RESPITE CARE LEGACY HOSPICE
 RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
10 Ancillary Networks
 10 Ancillary Networks This chapter discusses information specific to healthcare providers in our contracted ancillary network. Content Section 1: Overview Section 2: Claims and Billing Section 3: Home
10 Ancillary Networks This chapter discusses information specific to healthcare providers in our contracted ancillary network. Content Section 1: Overview Section 2: Claims and Billing Section 3: Home
ICD-CM Coding The Structural Considerations
 The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
2015 National Training Program. History of Modern Hospice. Hospice Legislative History. Medicare s Coverage of Hospice Services
 2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEDI-CAL PROVIDER MANUAL CLAIMS DEPARTMENT
 III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
Risk Adjustment for EDS & RAPS Webinar Q&A Documentation
 Risk Adjustment for EDS & RAPS Webinar Q&A Documentation 11:00 a.m. 12:00 p.m. EDS Duplicate Logic Q1. Will CMS consider validation of diagnosis codes for the EDS duplicate logic? A1. At this time, CMS
Risk Adjustment for EDS & RAPS Webinar Q&A Documentation 11:00 a.m. 12:00 p.m. EDS Duplicate Logic Q1. Will CMS consider validation of diagnosis codes for the EDS duplicate logic? A1. At this time, CMS
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Outpatient Observation Services
 Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
SECTION A: IDENTIFICATION INFORMATION. A0100: Facility Provider Numbers. Item Rationale. Coding Instructions
 SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
LOUISIANA MEDICAID PROGRAM ISSUED: 04/15/12 REPLACED: CHAPTER 24: HOSPICE SECTION 24.3: COVERED SERVICES PAGE(S) 5 COVERED SERVICES
 5 COVERED SERVICES") COVERED SERVICES Hospice care includes services necessary to meet the needs of the recipient as related to the terminal illness and related conditions. Core Services (Core services) must routinely be provided
COVERED SERVICES Hospice care includes services necessary to meet the needs of the recipient as related to the terminal illness and related conditions. Core Services (Core services) must routinely be provided
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Hospice Codes. Table 1 ALS Diagnosis. Table 2 Alzheimer s Disease and Related Disorder Diagnoses. Table 3 Heart Disease Diagnoses
 I N D I A N A H E A L T H C O V E R A G E P R O G R A M S P R O V I D E R C O D E S E T S Hospice Codes Table 1 ALS Diagnosis Table 2 Alzheimer s Disease and Related Disorder Diagnoses Table 3 Heart Disease
I N D I A N A H E A L T H C O V E R A G E P R O G R A M S P R O V I D E R C O D E S E T S Hospice Codes Table 1 ALS Diagnosis Table 2 Alzheimer s Disease and Related Disorder Diagnoses Table 3 Heart Disease
4/24/17. Today s Presenters. Disclaimer. Nursing Documentation-Supporting Terminal Prognosis
 Nursing Documentation-Supporting Terminal Prognosis Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant Email: J6.provider.training@anthem.com 2 Disclaimer National
Nursing Documentation-Supporting Terminal Prognosis Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant Email: J6.provider.training@anthem.com 2 Disclaimer National
Connecticut interchange MMIS
 Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
Connecticut interchange MMIS Provider Manual Chapter 7 Hospice August 10, 2009 Connecticut Department of Social Services (DSS) 55 Farmington Ave Hartford, CT 06105 DXC Technology 195 Scott Swamp Road Farmington,
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Q & A. HHA Requirements for Certifying Physician. Influenza Vaccine for Season. Coding & Billing for Prospective Payment Systems
 Volume 13, Issue 6 October 7, 2013 Coding & Billing for Prospective Payment Systems October 2013 Update of Hospital OPPS Influenza Vaccine for 2013 2014 Season Q & A HHA Requirements for Certifying Physician
Volume 13, Issue 6 October 7, 2013 Coding & Billing for Prospective Payment Systems October 2013 Update of Hospital OPPS Influenza Vaccine for 2013 2014 Season Q & A HHA Requirements for Certifying Physician
10 Ancillary Networks
 10 Ancillary Networks This chapter provides information specific to healthcare providers in our contracted ancillary network. Content Section 1: Overview Section 2: Claims and Billing Section 3: Home Based
10 Ancillary Networks This chapter provides information specific to healthcare providers in our contracted ancillary network. Content Section 1: Overview Section 2: Claims and Billing Section 3: Home Based
UPDATED Nursing/Intermediate Care Facility Providers
 December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
Archived SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS. Section 14 - Special Documentation Requirements
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 PLAN OF CARE... 2 14.2 HCFA-485 HOME HEALTH CERTIFICATION AND PLAN OF TREATMENT (FOR DOCUMENTATION PURPOSES... 2 14.3 HCFA-486 MEDICAL UPDATE AND PATIENT
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 PLAN OF CARE... 2 14.2 HCFA-485 HOME HEALTH CERTIFICATION AND PLAN OF TREATMENT (FOR DOCUMENTATION PURPOSES... 2 14.3 HCFA-486 MEDICAL UPDATE AND PATIENT
Medicare Program; FY 2017 Hospice Wage Index and Payment Rate Update and Hospice. AGENCY: Centers for Medicare & Medicaid Services (CMS), HHS.
, HHS.") This document is scheduled to be published in the Federal Register on 08/05/2016 and available online at http://federalregister.gov/a/2016-18221, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
This document is scheduled to be published in the Federal Register on 08/05/2016 and available online at http://federalregister.gov/a/2016-18221, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
CY 2016 Hospice Proposed Rule. HEALTHCAREfirst 5/13/2015. Hospice Regulatory Update FY Hospice Regulatory Review May 2015.
 Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
Hospice Regulatory Review May 2015 Presented by: Deanna Loftus Director of Regulatory Compliance Webinar Agenda CY 2016 Proposed Rule o New Payment Rates o New Service Intensity Add-On o HQRP Updates o
Chapter 13 Section 2. Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups
 Groups") Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Ages Ages 3 through 64.
 Medicaid: Follow-Up After Discharge from Community Hospitals, State Psychiatric Hospitals, and Facility Based Crisis Services for Mental Health Treatment The percentage of discharges for individuals ages
Medicaid: Follow-Up After Discharge from Community Hospitals, State Psychiatric Hospitals, and Facility Based Crisis Services for Mental Health Treatment The percentage of discharges for individuals ages
Home Health, Hospice, and Nursing Facility. Indiana Health Coverage Programs DXC Technology October 2017
 Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Home Health, Hospice, and Nursing Facility Indiana Health Coverage Programs DXC Technology October 2017 Agenda Billing Tips Home Health Hospice Nursing Facility Claim Form Update Helpful Tools Questions
Automating documentation helps hospice agencies withstand greater scrutiny
 White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
White Paper Automating documentation helps hospice agencies withstand greater scrutiny Documenting care plan, procedures key to staying in regulatory compliance Abstract The importance of strong documentation
Administrative Guide. KanCare Program Chapter 11: Hospice. Physician, Health Care Professional, Facility and Ancillary. UHCCommunityPlan.
 KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1
 Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
Using the Hospice PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER PEPPER target areas Percents and percentiles Comparison
PREPARING FOR THE 2016 HOSPICE PAYMENT CHANGES 12/15/2015. December 16, Mark Sharp Partner
 PREPARING FOR THE 2016 HOSPICE PAYMENT CHANGES December 16, 2015 Mark Sharp Partner msharp@bkd.com M. Aaron Little Managing Director mlittle@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire webinar
PREPARING FOR THE 2016 HOSPICE PAYMENT CHANGES December 16, 2015 Mark Sharp Partner msharp@bkd.com M. Aaron Little Managing Director mlittle@bkd.com 1 TO RECEIVE CPE CREDIT Participate in entire webinar
Complete RHC Medicare Billing
 Complete RHC Medicare Billing 1 RHC Basics 2 What is a Rural Health Clinic? This CMS publication is an excellent resource as an overview of the RHC Program. Program Basics Certification Process Qualified
Complete RHC Medicare Billing 1 RHC Basics 2 What is a Rural Health Clinic? This CMS publication is an excellent resource as an overview of the RHC Program. Program Basics Certification Process Qualified
HOMECARE AND HOSPICE REIMBURSEMENT
 Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Hospice Modeling Hospice Changes to Prepare for Medicare Reimbursement and Care Delivery Reform Robert J. Simione Managing Principal Simione Healthcare Consultants, LLC HOMECARE AND HOSPICE REIMBURSEMENT
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule
![Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule](/thumbs/73/68786685.jpg "Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule") Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
Medicare Program; FY 2016 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements [CMS-1629-P] Summary of Proposed Rule TABLE OF CONTENTS Issue Page I. Introduction and Background
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
The Concerns. Hospice Care in The Nursing Home NHPCO MLC All Rights Reserved 1.
 Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
Hospice Care in The Nursing Home Navigating The Regulatory Challenges Roseanne Berry, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 480 650 5604 roseanne@rchealthcaresolutions.com
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
RHC Billing - Introduction Fall, 2017
 RHC Billing - Introduction www.ruralhealthclinic.com Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
RHC Billing - Introduction www.ruralhealthclinic.com Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
Version 5010 Errata Provider Handout
 Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Place of Service Codes (POS) and Definitions
 and Definitions") 2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
Medicare Regulations and Rules Update What Should You Know?
 Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Overview of the Hospice Proposed Rule
 HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
HOSPICE Overview of Hospice Payment Reform Robert J. Simione Managing Principal Simione Healthcare Consultants On April 29, 2013 CMS issued the proposed rule that would update FY 2014 Medicare payment
Home Health Services
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Home Health Services L I B R A R Y R E F E R E N C E N U M B E R P R O M O D 0 0 0 3 2 P U B L I S H E D : N O V E M B E R 7, 2 0 1 7 P O L I
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Home Health Services L I B R A R Y R E F E R E N C E N U M B E R P R O M O D 0 0 0 3 2 P U B L I S H E D : N O V E M B E R 7, 2 0 1 7 P O L I
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Medicare Part A provides a special program for persons needing hospice care.
 MEDICARE HOSPICE BENEFIT Medicare Part A provides a special program for persons needing hospice care. These services are delivered to hospice patients wherever the patient resides by a Medicarecertified
MEDICARE HOSPICE BENEFIT Medicare Part A provides a special program for persons needing hospice care. These services are delivered to hospice patients wherever the patient resides by a Medicarecertified
TCS FAQ s. How will the implementation of national standard code sets reduce burden on the health care industry?
 TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
MLN Matters Number: MM6699 Related Change Request (CR) #: 6699
 #: 6699") News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW
 2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW PRESENTED BY: MELINDA A. GABOURY, COS-C CHIEF EXECUTIVE OFFICER HEALTHCARE PROVIDER SOLUTIONS, INC. HEALTHCAREPROVIDERSOLUTIONS.COM ADDITIONAL
2017 FOCUSED ON DOCUMENTATION NECESSITIES & PRE-CLAIM REVIEW PRESENTED BY: MELINDA A. GABOURY, COS-C CHIEF EXECUTIVE OFFICER HEALTHCARE PROVIDER SOLUTIONS, INC. HEALTHCAREPROVIDERSOLUTIONS.COM ADDITIONAL
FHCA 2014 Annual Conference & Trade Show
 FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
Hospice Billing: Two Tier and SIA Payments
 Billing: Two Tier and SIA Payments January 2016 1787_1215 Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant Email: J6.provider.training@anthem.com 2 Disclaimer
Billing: Two Tier and SIA Payments January 2016 1787_1215 Today s Presenters Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant Email: J6.provider.training@anthem.com 2 Disclaimer
4/3/2017. Hospice Reimbursement Explained
 Hospice Reimbursement Explained Indiana Association for Home and Hospice Care Annual Conference & Exposition May 9, 2017 3:30 PM 5:00 PM marcumllp.com Your Speakers Joshua S. Banach, CPA Senior Manager
Hospice Reimbursement Explained Indiana Association for Home and Hospice Care Annual Conference & Exposition May 9, 2017 3:30 PM 5:00 PM marcumllp.com Your Speakers Joshua S. Banach, CPA Senior Manager
2016 Hospice Regulatory Blueprint for Action. Hospice Association of America 228 Seventh Street, SE Washington DC
 2016 Hospice Regulatory Blueprint for Action Hospice Association of America 228 Seventh Street, SE Washington DC 20003-4306 HOSPICE ASSOCIATION OF AMERICA 2016 REGULATORY BLUEPRINT FOR ACTION TABLE OF
2016 Hospice Regulatory Blueprint for Action Hospice Association of America 228 Seventh Street, SE Washington DC 20003-4306 HOSPICE ASSOCIATION OF AMERICA 2016 REGULATORY BLUEPRINT FOR ACTION TABLE OF
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Louisiana DHH Medicaid UB-92 Code Reference for LTC NF/ADHC/ICF-MR/ Hospice (Room & Board)
") Louisiana DHH Medicaid UB-92 Code Reference for LTC NF/ADHC/ICF-MR/ Hospice (Room & Board) Release Name: Long Term Care Release Date: 10/1/2003 Revised: 8/1/2003 Prepared By: Shannon L. Clark, HIPAA Operations
Louisiana DHH Medicaid UB-92 Code Reference for LTC NF/ADHC/ICF-MR/ Hospice (Room & Board) Release Name: Long Term Care Release Date: 10/1/2003 Revised: 8/1/2003 Prepared By: Shannon L. Clark, HIPAA Operations
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation