ATTACHMENT I. Outpatient Status: Solicitation of Public Comments
|
|
|
- Jayson Jefferson
- 5 years ago
- Views:
Transcription
1 ATTACHMENT I The following text is a copy of the Federation of American Hospitals ( FAH ) comments in response to the solicitation of public comments on outpatient status that was contained in CMS-1589-P; Medicare and Medicaid Programs: Hospital Outpatient Prospective and Ambulatory Surgical Center Payment Systems and Quality Reporting Programs; Electronic Reporting Pilot; Inpatient Rehabilitation Facilities Quality Reporting Program; Quality Improvement Organization Regulations; 77 Fed. Reg. 45,061(July 30, 2012). We incorporate these comments by reference into our current comment letter as referenced under the section titled V.N. Policy Proposal on Admission and Medical Review Criteria for Hospital Inpatient Services under Medicare Part A. XI. Outpatient Status: Solicitation of Public Comments The FAH appreciates that CMS is soliciting public comments on the important issue involving hospital inpatient/outpatient status determinations. Hospitals and CMS share the goal of proper Medicare payments made in the first instance. Determining inpatient/outpatient status is an issue that hospitals spend a substantial amount of time, money and energy trying to manage effectively. A. Defining the Problem Even with this commitment in place, hospitals still experience significant confusion and uncertainty by physicians regarding these important decisions, and those decisions can be second guessed during post-payment Medicare audits or even through fraud and abuse allegations or investigations. Thus, this is an important topic requiring additional guidance and clarification from the Medicare program. The fundamental starting point is that physicians not hospitals must make the decision regarding whether to designate a Medicare beneficiary as a hospital inpatient or an outpatient. The Medicare Hospital Conditions of Participation ( CoPs ) require a patient to be admitted pursuant to a physician order. (See 42 C.F.R (c)(1).) Unfortunately, in most instances, physicians may not be very knowledgeable about standards that the Medicare program may use to assess whether a patient should be an inpatient or outpatient. Hospitals routinely provide case managers to consult with physicians to assist with, and to educate about, patient status decisions. While hospitals endeavor to provide this support, physicians often are challenged to maintain indepth knowledge of the various standards that address this issue and often have strong personal views on the issue. Also, physicians may be less attentive to the nuances of making these determinations because Medicare payment for a physician s professional service is the same regardless of whether the patient is an inpatient or outpatient for hospital payment purposes. Patient status determinations have become more challenging over time for a variety of reasons. Technology and medical advances now allow certain procedures to be performed in an outpatient setting that were historically provided only to inpatients. Also, there has been a rise in Recovery Audit Contractor ( RAC ) recoveries related to overturning short stay inpatient admissions because the site of service was not medically necessary (i.e., the service should have
2 been provided during an outpatient encounter). There even have been cases alleging that certain inpatient determinations are fraudulent and should be sanctioned under the Civil False Claims Act or other fraud and abuse authorities. Understandably, the current landscape has led hospitals to employ a very cautious approach to billing for inpatient admissions. This cautious approach has created other issues, including increased use of outpatient observation services and longer lengths of observation encounters issues that CMS has expressed concern about to the hospital industry. 1 In addition, policies requiring the use of Condition Code 44, which is a cumbersome process used to change a patient s status from inpatient to outpatient during a hospital stay, have further complicated matters in the name of protecting patients from the impact on beneficiary out-of-pocket liability. The reality of the current situation is hospitals now find themselves caught in the middle. On one hand, their inpatient admissions are being closely scrutinized and second guessed more than ever before through multiple activities including post-payment reviews, fraud allegations, and even lawsuits by Medicare beneficiary advocacy groups. In many instances, the same clinical services are being furnished to patients regardless of whether the patient can qualify for inpatient status, yet they are being paid much less than the cost of providing that care under CMS s Part B Only payment policy. On the other hand, while the Medicare program presumably prefers to make the lower hospital payments associated with outpatient services, classifying a patient as an outpatient has a significant financial impact on beneficiaries through higher cost sharing and ineligibility for coverage of post-hospital skilled nursing services. For all of these reasons, the FAH believes it is time for CMS to clarify these policies in a way that recognizes the challenging environment under which hospitals operate in good faith, promotes objective standards, and better respects a physician s real time judgment with hospital assistance. CMS s formal solicitation of public comments is an important step in the process, and the FAH looks forward to working with CMS as it considers and develops necessary changes in this policy area. In our view, there are several issues to address. First, the front end determination of when a patient should be classified as an inpatient needs more guidance and clarity. While certain industry standards (e.g. Interqual and Millman) are often used to assist in making patient status determinations, there are no definitive Medicare policy guidelines that govern these decisions. Whether it s patients being held in observation status longer than desired because they may not meet inpatient criteria, or a patient requiring surgical services for whom a physician must decide between an inpatient admission or outpatient encounter, the challenge is the same an attending physician, with hospital support, tries to make the proper, real time patient status decision. Even so, hospitals face the distinct possibility of a post-payment denial and appeals process or even possible fraud and abuse allegations made based upon a physician s good faith decision. 1 In 2010, we responded to a letter from the CMS Principal Deputy Administrator raising concerns about the length of stays for Medicare patients in observation status and the financial impact that has on beneficiaries. While we acknowledged the trend and concern for beneficiaries, the FAH explained that hospitals felt it was the Medicare program s policies that were driving those results. We attach a copy of the FAH s correspondence with these comments, and ask that our letter be incorporated into this rulemaking record. 2
3 Second, in cases where a Medicare contractor denies that an inpatient admission was appropriate, hospitals can only receive a partial, very minimal Part B payment under the existing Part B Only payment policy. Essentially, Medicare has made a policy judgment (not mandated by statute or regulation) not to pay the full Part B reimbursement in these situations. This outcome is illogical and fundamentally unfair. A common example illustrates the point. Assume a physician orders an inpatient admission during which an internal defibrillator is implanted in a patient to address a cardiac clinical condition. The hospital bills a Part A claim to Medicare, which reimburses for all of the services and related device through the appropriate inpatient payment Diagnostic Related Group. Later, the Part A payment is overturned because of a finding that the claim did not represent a medically necessary inpatient service. In this case, no one disputes the patient had a clinical condition that required a defibrillator to be implanted, but a Medicare contractor questions whether the procedure needed to be done as an inpatient service. In light of the postpayment denial, Medicare s Part B Only policy would not allow the hospital to rebill Medicare and be paid for the surgical service and implanted device as a covered outpatient service. Also, the patient sees an increase in his out-of-pocket cost sharing under Part B and could become responsible for the cost of the implant and related service, because they are a noncovered Medicare item and service. However, it is often difficult for the hospital to collect these charges when the patient is responsible, making the final result uncompensated care for the hospital that cannot even be claimed as Medicare bad debt. In our view, the impact on the Medicare program is nonsensical, the shifting of financial responsibility to the beneficiary seems unconscionable, and the likely negative financial impact on the hospital is patently unfair. Yet, this example and outcome is a common occurrence today for hospitals. B. Potential Solutions There are a number of potential solutions that can address these ongoing problems. 1. Hospital case managers should play a more formal role in making hospital patient status determinations through Case Management Admission Protocols. CMS should approve the use of Case Management Admission Protocols ( CMAP ) to make hospital patient status determinations. The concept of CMAP is not new to the Medicare program, but is one that has not been embraced fully in Medicare policy to date. Under such a process, physicians, through a CMAP approved by a hospital s Medical Executive Committee, can delegate patient status determinations to hospital case managers, with the physicians signing a validation order at some reasonable point after clinical care commences. Here s how a CMAP would work. At the time of ordering hospital services, a physician would order necessary clinical services based upon the stated diagnosis and the patient is admitted per Case Management Protocol. Consistent with other Medicare policies, the clinical care then could begin. For patient status purposes, the patient would remain in a hold status for a specified amount of time, during which the hospital s utilization management team would 3
4 assign a status using specific, internally-adopted criteria. The physician would then be made aware of utilization management s decision and co-sign the final order to authenticate the appropriate patient status. If and when physicians do not agree with utilization management s patient status assignment, a specific process would be available for the physician to protest and the disagreement resolved. We believe the CMAP approach would satisfy the Medicare Hospital CoPs, because a physician first orders the clinical care with the first CMAP order, and then the physician subsequently would approve the case management order or seek a change to that order as the final patient status determination. Essentially, the physician would be approving the order twice. While the CMAP approach has not been embraced fully, the concept is consistent with verbal order authentication and medical protocol policies already permissible under the CoPs. (See 42 C.F.R (c).) Notably, there are several demonstration projects that support using CMAP. First, in 2003, the Florida Quality Improvement Organization, FMQAI, implemented the protocol at 20 hospitals and experienced a 67 percent drop in denials for short stay admissions. In another CMS-funded project, FMQAI focused on medically unnecessary chest pain admissions and recruited 10 hospitals to use CMAP. Participating hospitals reduced inappropriate chest pain admissions by 37 percent, with a projected decrease annually of 67 percent. Health Services Advisory Group conducted a similar project in Arizona which resulted in a 90 percent reduction in one-day inpatient admissions for chest pain. The New Mexico Medical Review Association implemented a later CMAP demonstration project (ending in 2008) with 16 select hospitals in six states, which showed a 53 percent drop in unnecessary short-stay admissions. While these demonstrations are dated, their results at the time were unassailable, yet there was no clear indication why CMS did not move to adopt the approach across the Medicare program. Thus, we strongly urge CMS to state officially that the use of CMAP is an acceptable practice. This will help with patient status determinations on the front end, which has both benefits for hospitals (receiving in the first instance proper, full payments) and to the Medicare program (reducing its payment error rate). Implementing CMAP is also likely to go a long way to reducing, if not eventually eliminating, the need for the Condition Code 44 process, which is cumbersome as a practical matter and also can result in negative interactions between physicians and hospital personnel. 2. CMS should adopt a policy allowing hospitals to receive full Part B payment when a Part A inpatient admission is denied as not medically necessary. The FAH has corresponded with CMS previously on this recommendation. Specifically, in 2011, the FAH sent two letters to CMS advocating that full Part B payment should be made when a Part A inpatient admission is denied as not medically necessary due to patient status. In our view, there is nothing in the Medicare statute that prohibits CMS from adopting this policy. In fact, the statute does not differentiate between Part B Only services and other Part B services, so we respectfully think the better reading of the statute is to provide full Part B payment over Part B Only payment. 4
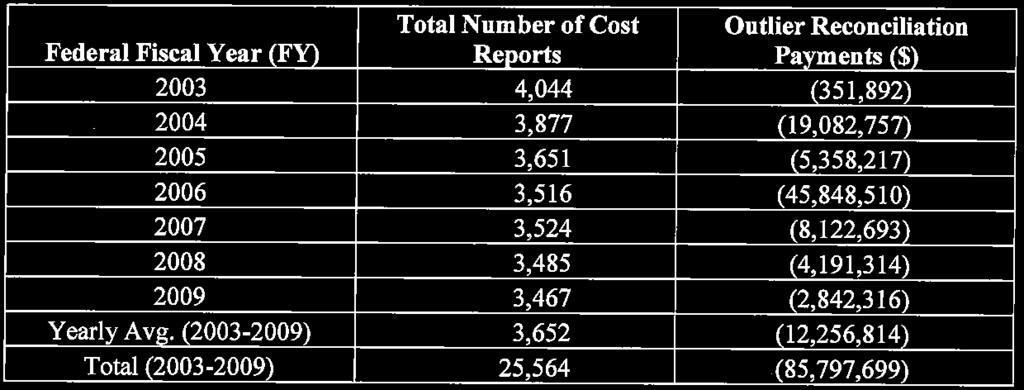
5 We also presented the trend emanating from the Departmental Appeals Board decision in the O Connor Hospital case that has resulted in Administrative Law Judges ( ALJ ) ordering full Part B payment when there are Part A medical necessity denials. We also offered operational suggestions and our members cooperation and support for logistics on how Medicare contractors could effectuate the proper Part B payment. We attach a copy of those letters with these comments, and ask that they be incorporated into this rulemaking record. Separately but similarly, the Proposed Rule provides an update on the AB rebilling demonstration project. We appreciate the update, but are compelled to express that overall our members are disappointed by the scope of this demonstration project. Hospitals feel that the combination of being required to forego your appeal rights and the best-case outcome of less than 100 percent of total Part B reimbursement for outpatient services were significant disincentives to participation in the demonstration project. There is even less incentive to participate in the demonstration because hospitals can achieve the remedy of full Part B payment by going through appeals process and obtaining an ALJ order requiring full Part B payment. In summary, we maintain that CMS has the authority to implement a permanent policy change that would allow for providers to receive a full Part B payment when a Part A claim is denied for lack of medical necessity due to improper patient status. As we believe this is the better reading of the statute, we are unclear as to the purpose and rationale of the current Part B Only policy. While logistical issues arise regarding the need to obtaining appropriate information to determine Part B payment, FAH members are prepared to work with CMS to implement a reasonable process that balances the burden on both providers and the Medicare program to receive an appropriate Part B claim. 3. CMS should consider implementing a short stay outlier to address the Agency s concerns about short stay admissions CMS should consider implementing a short stay outlier payment policy under the hospital inpatient prospective payment system ( IPPS ). This would reduce the financial incentive of hospitals receiving full IPPS payments for short stay admissions, which has been an ongoing concern for CMS and law enforcement, while preserving respect for the clinical judgment of physicians who believe those patients should be admitted as inpatients. A short stay outlier may also help mitigate CMS s concern about increasing use of observation status, as it could be crafted in a way to make hospitals feel more comfortable about admitting observation patients as inpatients in appropriate circumstances. The possibility that such cases may come under scrutiny later on because a hospital has received a full IPPS payment should decrease because of the reduced financial incentive to the hospital. There is precedent for this type of payment adjustment, as it has been adopted under the Long Term Acute Care Hospital Prospective Payment System ( LTACH PPS ). Under that payment system, the short stay outlier is an adjustment to the applicable base payment for cases that are considerably shorter that the average length of stay for similar cases. 5
6 4. Longer term, CMS may wish to evaluate implementing a preauthorization process for inpatient admissions like those used by private insurance plans. For hospitals, such an approach would not create significant additional burden given hospitals already have appropriate staff in place to handle pre-authorizations with most private payers. While implementing a pre-authorization process would require new processes by Medicare contractors, we believe the program would potentially eliminate and/or reduce some existing processes. For example, pre- and post-payment audits of the medical necessity of inpatient status could likely be significantly reduced or eliminated by a pre-authorization program. Medicare contractor resources from these services could likely be reallocated to the new pre-authorization process. In addition, a pre-authorization process would be in sync with both CMS and the administration s desire to make appropriate payments for quality care and reduce the payment error rate and need for the current pay and chase recovery audit contractor process. An inpatient status pre-authorization program would also help to improve the transparency of appropriate inpatient stays for Medicare beneficiaries. CMS indicates that stakeholders believe hospitals are electing to treat beneficiaries as outpatients receiving observation services instead of as inpatients due to financial risk of the stay being denied at a later date. A pre-authorization program for inpatients status should eliminate and/or significantly reduce such concerns. 6
7
8
9
10

11
12
13
14
15
16
17
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
Executive Summary, December 2015
 CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from
 Consultation Services and Transfer of Care CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from these services to increase payments for visits, including
Consultation Services and Transfer of Care CMS has finalized its proposal to eliminate Medicare payment for consultations and use the money from these services to increase payments for visits, including
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As
 Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As INTRODUCTION On May 4, 2016, the Centers for Medicare & Medicaid Services (CMS) temporarily paused the Beneficiary
Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As INTRODUCTION On May 4, 2016, the Centers for Medicare & Medicaid Services (CMS) temporarily paused the Beneficiary
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations
 50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations The quality, utility, and clarity of the information to be collected. Recommendations to minimize the information
50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations The quality, utility, and clarity of the information to be collected. Recommendations to minimize the information
2014 Hospital Admission Criteria
 2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and
 In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and Certification requirements for physicians Outpatient Observation
In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and Certification requirements for physicians Outpatient Observation
PATIENT STATUS DEFINITIONS, 2 MIDNIGHT RULE AND 96 HOUR RULE
 PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
State Medicaid Recovery Audit Contractor (RAC) Program
 Program") State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
9/18/2014. Agenda. Final IPPS 2015 AKA CMS 1607-F (Published in Federal Register on August 22, 2014)
") 2015 Inpatient Prospective Payment Services (IPPS) and Insights on Best Practices John Zelem, MD, FACS Executive Medical Director, Client Relations and Education Agenda 2014/2015 IPPS Final Rule 2015 proposed
2015 Inpatient Prospective Payment Services (IPPS) and Insights on Best Practices John Zelem, MD, FACS Executive Medical Director, Client Relations and Education Agenda 2014/2015 IPPS Final Rule 2015 proposed
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
See page 16. Drug diversion in healthcare facilities, Part 1: Identify and prevent. Erica Lindsay
 Compliance TODAY May 2015 a publication of the health care compliance association www.hcca-info.org From the courtroom to Compliance one lawyer s journey and the lessons learned an interview with Tracy
Compliance TODAY May 2015 a publication of the health care compliance association www.hcca-info.org From the courtroom to Compliance one lawyer s journey and the lessons learned an interview with Tracy
Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape
 Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
CMS New Standards for Hospital Inpatient Admissions October Physician Admission Order Check List Detail
 Providing technologically supported physician advisory and case management services to healthcare providers and payors CMS New Standards for Hospital Inpatient Admissions October 2013 Physician Admission
Providing technologically supported physician advisory and case management services to healthcare providers and payors CMS New Standards for Hospital Inpatient Admissions October 2013 Physician Admission
Observation vs. Inpatient: How to Get it Right. November 5, 2013
 Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers
 AIS s Management Insight Series The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers Adapted from an AIS webinar presented by Abby Pendleton, Esq. Founding Partner The Health Law
AIS s Management Insight Series The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers Adapted from an AIS webinar presented by Abby Pendleton, Esq. Founding Partner The Health Law
Submission #1. Short Description: Medicare Payment to HOPDs, Section 603 of BiBA 2015
 Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
August 14, 2013 COF Bi- Monthly Call. Questions or comments? Contact Ivy Baer: or
 August 14, 2013 COF Bi- Monthly Call Questions or comments? Contact Ivy Baer: ibaer@aamc.org or 202-828-0499 OPPS Comment Period Is NOW Comments Due 9/6 Hospital Outpatient Services Proposal (OPPS) On
August 14, 2013 COF Bi- Monthly Call Questions or comments? Contact Ivy Baer: ibaer@aamc.org or 202-828-0499 OPPS Comment Period Is NOW Comments Due 9/6 Hospital Outpatient Services Proposal (OPPS) On
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL
 Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
General Inpatient Level of Care: Managing Risks
 General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
General Inpatient Level of Care: Managing Risks THE CAROLINAS CENTER, 2015 1 Presenter Annette Kiser, MSN, RN, NE-BC Director of Quality & Compliance The Carolinas Center akiser@cchospice.org THE CAROLINAS
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change. November 22, 2013
 Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Medicare Recovery Audit Contractors. Chicago, IL August 1, 2008
 Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective
 MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective 10-1-13 TIMELINE August 2, 2013 Final rule published August 19, 2013 CMS holds open door forum. Many questions raised Sept 5, 2013 CMS
MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective 10-1-13 TIMELINE August 2, 2013 Final rule published August 19, 2013 CMS holds open door forum. Many questions raised Sept 5, 2013 CMS
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
The Importance of the Conditions of Participation for Hospitals
 The Importance of the Conditions of Participation for Hospitals The Centers for Medicare & Medicaid Services (CMS) issued Transmittal R37SOMA (Transmittal 37) revising the Interpretive Guidelines to Hospitals
The Importance of the Conditions of Participation for Hospitals The Centers for Medicare & Medicaid Services (CMS) issued Transmittal R37SOMA (Transmittal 37) revising the Interpretive Guidelines to Hospitals
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations. Agenda
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
Medical Necessity Certification 3/4/2014. CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations. Agenda. Valid Admissions What Changed?
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
November 16, Dear Dr. Berwick:
 November 16, 2010 Don Berwick, MD Administrator Centers for Medicare and Medicaid Services Department for Health and Human Services Attn: CMS-6028-P P.O. Box 8020 Baltimore, MD 21244-8017 RE: Medicare,
November 16, 2010 Don Berwick, MD Administrator Centers for Medicare and Medicaid Services Department for Health and Human Services Attn: CMS-6028-P P.O. Box 8020 Baltimore, MD 21244-8017 RE: Medicare,
10.0 Medicare Advantage Programs
 10.0 Medicare Advantage Programs This section is intended for providers who participate in Medicare Advantage programs, including Medicare Blue PPO. In addition to every other provision of the Participating
10.0 Medicare Advantage Programs This section is intended for providers who participate in Medicare Advantage programs, including Medicare Blue PPO. In addition to every other provision of the Participating
Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule
 Calendar Year (CY) 2013 Final Rule") Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Recovery Audit Contractors: AHA Perspective. Elizabeth Baskett, Policy, AHA February 23, 2012
 Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Recovery Audit Contractors: AHA Perspective Elizabeth Baskett, Policy, AHA February 23, 2012 Agenda Lay of the Land = Audit Overload RACs (Medicare & Medicaid) MACs ZPICs and OIG and DOJ, oh my! AHA and
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
RE: Medicare Program; Request for Information Regarding the Physician Self-Referral Law
 1055 N. Fairfax Street, Suite 204, Alexandria, VA 22314, TEL (703) 299-2410, (800) 517-1167 FAX (703) 299-2411 WEBSITE www.ppsapta.org August 24, 2018 Seema Verma, MPH Administrator Centers for Medicare
1055 N. Fairfax Street, Suite 204, Alexandria, VA 22314, TEL (703) 299-2410, (800) 517-1167 FAX (703) 299-2411 WEBSITE www.ppsapta.org August 24, 2018 Seema Verma, MPH Administrator Centers for Medicare
Leslie Demaree Goldsmith
 LESLIE DEMAREE GOLDSMITH Shareholder is a shareholder in Baker Donelson's Baltimore office. Overview Ms. Goldsmith brings more than 25 years of experience to her practice, representing health care providers
LESLIE DEMAREE GOLDSMITH Shareholder is a shareholder in Baker Donelson's Baltimore office. Overview Ms. Goldsmith brings more than 25 years of experience to her practice, representing health care providers
June 2, Dear Secretary Sebelius:
 Ms. Kathleen Sebelius Secretary U.S. Department of Health and Human Services Hubert H. Humphrey Building, Suite 120F 200 Independence Avenue S.W. Washington, D.C. 20201 Dear Secretary Sebelius: On behalf
Ms. Kathleen Sebelius Secretary U.S. Department of Health and Human Services Hubert H. Humphrey Building, Suite 120F 200 Independence Avenue S.W. Washington, D.C. 20201 Dear Secretary Sebelius: On behalf
Partnering with hospitals to create an accountable care organization Elias N. Matsakis, Esq.
 Partnering with hospitals to create an accountable care organization Elias N. Matsakis, Esq. There are many opportunities for physicians and hospitals to affiliate and clinically integrate so as to enable
Partnering with hospitals to create an accountable care organization Elias N. Matsakis, Esq. There are many opportunities for physicians and hospitals to affiliate and clinically integrate so as to enable
REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004)
") REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004) Lester J. Perling Broad and Cassel Fort Lauderdale, Florida I. Case Summaries CMNs Document Medical Necessity In Maximum
REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004) Lester J. Perling Broad and Cassel Fort Lauderdale, Florida I. Case Summaries CMNs Document Medical Necessity In Maximum
Hospice Program Integrity Recommendations
 Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
INSTITUTE ON MEDICARE/MEDICAID PAYMENT ISSUES MEDICARE CONDITIONS OF PARTICIPATION: WHAT IS YOUR GRADE?
 INSTITUTE ON MEDICARE/MEDICAID PAYMENT ISSUES MEDICARE CONDITIONS OF PARTICIPATION: WHAT IS YOUR GRADE? Cindy Wisner, Esq. Teresa A. Williams, Esq. Trinity Health INTEGRIS Health, Inc. 20555 Victor Parkway
INSTITUTE ON MEDICARE/MEDICAID PAYMENT ISSUES MEDICARE CONDITIONS OF PARTICIPATION: WHAT IS YOUR GRADE? Cindy Wisner, Esq. Teresa A. Williams, Esq. Trinity Health INTEGRIS Health, Inc. 20555 Victor Parkway
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
AHLA. GG. Physician Orders. Timothy P. Blanchard Blanchard Manning LLP Orcas, WA
 AHLA GG. Physician Orders Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Institute on Medicare and Medicaid Payment Issues March 26-28, 2014 Physician Orders Timothy P. Blanchard, MHA, JD Medicare
AHLA GG. Physician Orders Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Institute on Medicare and Medicaid Payment Issues March 26-28, 2014 Physician Orders Timothy P. Blanchard, MHA, JD Medicare
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
HFMA WEBINAR. CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases?
 HFMA WEBINAR CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases? Date: September 24, 2013 Time: 2:00 3:30 p.m. Central (12:00 1:30 pm Pacific/1:00 2:30 pm Mountain/3:00 4:30 pm Eastern) Follow
HFMA WEBINAR CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases? Date: September 24, 2013 Time: 2:00 3:30 p.m. Central (12:00 1:30 pm Pacific/1:00 2:30 pm Mountain/3:00 4:30 pm Eastern) Follow
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness. October 12, 2009
 Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
CMS -1599F. The 2 Midnight Rule Effective October 1, 2013
 Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
A Review of Current EMTALA and Florida Law
 A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018
 Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment
 Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
PARITY IMPLEMENTATION COALITION
 PARITY IMPLEMENTATION COALITION Frequently Asked Questions and Answers about MHPAEA Compliance These are some of the most commonly asked questions and answers by consumers and providers about their new
PARITY IMPLEMENTATION COALITION Frequently Asked Questions and Answers about MHPAEA Compliance These are some of the most commonly asked questions and answers by consumers and providers about their new
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
What is an Inpt & How to get it right. The Challenges of Coverage and Compliance Why is it so hard?
 What is an Inpt & How to get it right The Challenges of Coverage and Compliance Why is it so hard? 1 From the pt: AARP Jan-Feb 2010 issue Hospital Stays are Under Observation Ruth Way fell, was admitted
What is an Inpt & How to get it right The Challenges of Coverage and Compliance Why is it so hard? 1 From the pt: AARP Jan-Feb 2010 issue Hospital Stays are Under Observation Ruth Way fell, was admitted
Appeals and Grievances
 Appeals and Grievances Community HealthFirst MA Special Needs Plan (HMO SNP) As a Community HealthFirst Medicare Advantage Special Needs Plan enrollee, you have the right to voice a complaint if you have
Appeals and Grievances Community HealthFirst MA Special Needs Plan (HMO SNP) As a Community HealthFirst Medicare Advantage Special Needs Plan enrollee, you have the right to voice a complaint if you have
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services.
 907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
Annual Leadership Institute August 25, Triple Check: A Process for Preventing False Claims
 Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Learning Objectives. It Starts With an Order and an Expectation
 1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
Mental Health Fee-for-Service Program Provider Manual Version 3.1 February 2018
 New Jersey Department of Health Division of Mental Health and Addiction Services http://nj.gov/health/integratedhealth Mental Health Fee-for-Service Program Provider Manual Version 3.1 February 2018 1.
New Jersey Department of Health Division of Mental Health and Addiction Services http://nj.gov/health/integratedhealth Mental Health Fee-for-Service Program Provider Manual Version 3.1 February 2018 1.
September 2, Dear Mr. Slavitt:
 Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W., Room 445-G Washington, DC 20201 RE: CMS-1656-P, Medicare Program;
Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W., Room 445-G Washington, DC 20201 RE: CMS-1656-P, Medicare Program;
December 21, 2012 BY ELECTRONIC DELIVERY
 BY ELECTRONIC DELIVERY CDR Krista M. Pedley, PharmD, MS, USPHS Director Office of Pharmacy Affairs Healthcare Systems Bureau Health Resources and Services Administration 5600 Fishers Lane Parklawn Building,
BY ELECTRONIC DELIVERY CDR Krista M. Pedley, PharmD, MS, USPHS Director Office of Pharmacy Affairs Healthcare Systems Bureau Health Resources and Services Administration 5600 Fishers Lane Parklawn Building,
ABOUT AHCA AND FLORIDA MEDICAID
 Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
DEPARTMENT OF HEALTH AND HUMAN SERVICES. Permanent Certification Program for Health Information Technology; Revisions to
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary 45 CFR Part 170 RIN 0991-AB77 Permanent Certification Program for Health Information Technology; Revisions to ONC-Approved Accreditor Processes
DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary 45 CFR Part 170 RIN 0991-AB77 Permanent Certification Program for Health Information Technology; Revisions to ONC-Approved Accreditor Processes
Medicare Regulations and Rules Update What Should You Know?
 Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor. NJHFMA Finance for Clinicians Session March 24, 2016
 1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
Appeals and Grievances
 Appeals and Grievances Community HealthFirst MA Special Needs Plan (HMO SNP) Community HealthFirst MA Plan (HMO) Community HealthFirst Medicare MA Pharmacy Plan (HMO) Community HealthFirst MA Extra Plan
Appeals and Grievances Community HealthFirst MA Special Needs Plan (HMO SNP) Community HealthFirst MA Plan (HMO) Community HealthFirst Medicare MA Pharmacy Plan (HMO) Community HealthFirst MA Extra Plan
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Modernizing TRICARE Payment Policies (Resolution -A-) Jack McIntyre, MD, Chair Reference Committee J (Melissa
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Modernizing TRICARE Payment Policies (Resolution -A-) Jack McIntyre, MD, Chair Reference Committee J (Melissa
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
The In and Out of the Medicare Two Midnight Rule. Disclaimer. Objectives 3/31/2014
 The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Mobile Medical Review Team Observation Services & the 2 Midnight Rule. The Audio and/or Video Recording of this Educational Session is Prohibited
 Mobile Medical Review Team Observation Services & the 2 Midnight Rule The Audio and/or Video Recording of this Educational Session is Prohibited National Government Services, Inc. Medicare Part A & Part
Mobile Medical Review Team Observation Services & the 2 Midnight Rule The Audio and/or Video Recording of this Educational Session is Prohibited National Government Services, Inc. Medicare Part A & Part
American Health Information Management Association Standards of Ethical Coding
 American Health Information Management Association Standards of Ethical Coding Introduction The Standards of Ethical Coding are based on the American Health Information Management Association's (AHIMA's)
American Health Information Management Association Standards of Ethical Coding Introduction The Standards of Ethical Coding are based on the American Health Information Management Association's (AHIMA's)
Diane Meyer, CHC (650) Agenda
 Agenda") The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
Documentation Updates for Physicians
 Documentation Updates for Physicians CMS IPPS 2014 Final Rule AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
Documentation Updates for Physicians CMS IPPS 2014 Final Rule AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
CDx ANNUAL PHYSICIAN CLIENT NOTICE
 CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
Medicaid Managed Specialty Supports and Services Concurrent 1915(b)/(c) Waiver Program FY 17 Attachment P7.9.1
/(c) Waiver Program FY 17 Attachment P7.9.1") QUALITY ASSESSMENT AND PERFORMANCE IMPROVEMENT PROGRAMS FOR SPECIALTY PRE-PAID INPATIENT HEALTH PLANS FY 2017 The State requires that each specialty Prepaid Inpatient Health Plan (PIHP) have a quality
QUALITY ASSESSMENT AND PERFORMANCE IMPROVEMENT PROGRAMS FOR SPECIALTY PRE-PAID INPATIENT HEALTH PLANS FY 2017 The State requires that each specialty Prepaid Inpatient Health Plan (PIHP) have a quality
Topics. Overview of the Medicare Recovery Audit Contractor (RAC) Understanding Medicaid Integrity Contractor
 Understanding Medicaid Integrity Contractor") RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
Toolkit. Medicare Skilled Nursing Facility Coverage And Jimmo v. Sebelius. 1. Introduction
 1. Introduction Toolkit Medicare Skilled Nursing Facility Coverage And Jimmo v. Sebelius Jimmo v. Sebelius, No. 11-cv-17 (D. VT), is a nationwide class-action lawsuit brought on behalf of Medicare beneficiaries
1. Introduction Toolkit Medicare Skilled Nursing Facility Coverage And Jimmo v. Sebelius Jimmo v. Sebelius, No. 11-cv-17 (D. VT), is a nationwide class-action lawsuit brought on behalf of Medicare beneficiaries
Instructions for Implementing the Centers for Medicare & Medicaid (CMS) Ruling CMS 1536-R; Astigmatism-Correcting Intraocular Lens (A-C IOLs)
 Ruling CMS 1536-R; Astigmatism-Correcting Intraocular Lens (A-C IOLs)") News Flash - An Overview of Medicare Preventive Services for Physicians, Providers, Suppliers, and Other Health Care Professionals educational video program, provides information on Medicare-covered preventive
News Flash - An Overview of Medicare Preventive Services for Physicians, Providers, Suppliers, and Other Health Care Professionals educational video program, provides information on Medicare-covered preventive
RE: CMS-1631-PM Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016
 September 8, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-2333-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Main Office
September 8, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-2333-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Main Office
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings
 Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings Provider Dispute/Appeal Procedures; Member Complaints, Grievances and Fair Hearings 138 Provider Dispute/Appeal
Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings Provider Dispute/Appeal Procedures; Member Complaints, Grievances and Fair Hearings 138 Provider Dispute/Appeal
OIG Opines On Propriety Of ED On-Call Coverage Arrangements By Michael Paddock and Lauren Kim, Crowell & Moring LLP*
 OIG Opines On Propriety Of ED On-Call Coverage Arrangements By Michael Paddock and Lauren Kim, Crowell & Moring LLP* Over the last several years, due in part to the growing financial burden on both physicians
OIG Opines On Propriety Of ED On-Call Coverage Arrangements By Michael Paddock and Lauren Kim, Crowell & Moring LLP* Over the last several years, due in part to the growing financial burden on both physicians
Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules
 Ohio Hospital Association Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules Christa Nordlund cfn1@fuse.net Jeri Rose West Chester Hospital 7700 University Drive West
Ohio Hospital Association Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules Christa Nordlund cfn1@fuse.net Jeri Rose West Chester Hospital 7700 University Drive West
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Net Revenue Matters. Risk Mitigation in Today s Healthcare Environment. The Critical Role of Analytics in Managing the Strategic Decision Process
 Net Revenue Matters February 2014 Risk Mitigation in Today s Healthcare Environment The Critical Role of Analytics in Managing the Strategic Decision Process By Jack Duffy, EVP We have all heard the expression
Net Revenue Matters February 2014 Risk Mitigation in Today s Healthcare Environment The Critical Role of Analytics in Managing the Strategic Decision Process By Jack Duffy, EVP We have all heard the expression
Department of Health and Human Services
 Monday, November 27, 2006 Part IV Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 405, 412, 422, and 489 Medicare Program; Notification of Hospital Discharge
Monday, November 27, 2006 Part IV Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 405, 412, 422, and 489 Medicare Program; Notification of Hospital Discharge