Rapid Cycle Improvement Tucson Nurses Week May 2012
|
|
|
- Michael Malone
- 5 years ago
- Views:
Transcription

1 Rapid Cycle Improvement Tucson Nurses Week May 2012 Diana Lopez, RN, MSN & Jennifer Qualls, RN, MSN Knowledge Management Carondelet Health Network Page 1
2 Presentation Objectives Define RCI (Rapid Cycle Improvement) Model for Improvement Describe Plan, Do, Study, Act Discuss how to set up RCI teams Review the change process & common barriers & resistance to change Provide 2 examples of RCI Projects & lessons learned Page 2
3 What is RCI? Applying the recurring sequence of PDSA (Plan, Do, Study, Act) in a short period of time to solve a problem or issue facing the team in order to achieve a breakthrough or continuous improvement and realize results more quickly Page 3
4 PDSA Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? Goal Statement Measures What change can we make that will result in improvement? Ideas Act Act Plan Plan Study Study Do Do From: Associates in Process Improvement Page 4
5 Setting a Goal Answers and clarifies What do we want to accomplish? Creates a shared language for communicating to others about the project Facilitates conversations & understanding about the project within your organization Page 5
6 How Do You Know If Your Changes Result in Improvements? MEASURES! Types of Measures: Outcome Measures Have we improved the outcomes for our patients? Are the patients having a better experience? Process Measures Is our work improving outcomes? Balancing Measures What impact is our improvement work having on the rest of the system? Page 6
7 Ideas What changes can we make that will lead to improvement? What will lead us to accomplishing our goal? Page 7
8 Determining if the Change is an Improvement This work focuses on making changes to systems rather than on measurement but measurement plays a critical role. Key measures are required to assess progress toward the aim Specific measures can be used for learning during PDSA cycles Data from the system (including from patients and staff) can be used to focus improvement and refine changes. Page 8
9 The PDSA Cycle for Improvement Act - What changes are to be made? - Next cycle? Study - Complete the analysis of the data - Compare data to predictions - Summarize what was learned Plan - Objective - Questions and predictions (Why?) - Plan to carry out the cycle (who, what, where, when) Do - Carry out the plan - Document problems and unexpected observations - Begin analysis of the data Page 9
10 REPEATED USE OF THE PDSA CYCLE Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? Hunches Theories Ideas A P S D Very Small Scale Test Follow-up Tests A P S D Wide-Scale Tests of Change Changes That Result in Improvement Implementation of Change Hold the Gains Knowledge & Experience Rapi d Cycle P R O J E C T D I F F I C Y U L T Y

11 Find Your Champion! Page 11
 Track progress & celebrate small successes Clarify roles & responsibilities Handle conflict constructively & quickly Maintain core group for consistency Page")
12 Assemble Your Team Composition Team Leader/ Champion Facilitator Team member(s) Helpful hints Multidisciplinary Assure leadership support Include hands-on expertise & variety of skills (example: bedside nurses) Track progress & celebrate small successes Clarify roles & responsibilities Handle conflict constructively & quickly Maintain core group for consistency Page 12

13 Identify a Problem! 1 Page 13
14 Where do you start? Determine what you want to change Examples: Improve patient satisfaction Improve Core Measure Outcomes Change the work environment Improve work flow Manage time Decrease variation Eliminate wastes Improve systems to eliminate errors Page 14
15 Tools to Use with Rapid Cycle Improvement Brainstorming generating a large number of ideas about factors contributing to the problem or issue Affinity Diagram organizing the ideas from brainstorming into categories/groupings Cause & Effect Diagram (Fishbone) graphic display of ideas related to the problem or issue Generally helps in identifying leverage points Flowchart graphic display of the sequence of events in a process Creating an Actual and Desired flowchart may help in further defining the Rapid Cycle Improvement objective Page 15
16 Page 16
17 Fishbone Diagram Page 17
18 Tips for Success Improvement occurs in small steps Repeated attempts are needed to test and implement new ideas Assess regularly & improve plan as you go Start with changes that are easy to test & likely to be successful Collect and study useful data during each test Failed changes = learning opportunities Test fast, fail fast, adjust fast (Tom Peters) Eventually test over a wide range of conditions Page 18

19 Barriers & Resistance Barrier - Problems with Teams Is your leader available and empowered? Are you meeting weekly? Does everyone know their role and responsibilities? If you have conflicts, who can help to resolve them? Page 19

20 Address Conflicts Early Page 20
21 Barriers & Resistance Barrier - Problems with Resources Suggestions: Keep your team small at first Use volunteers and champions Collect just enough data Set a dedicated meeting time Huddle if needed (15 minutes is all you need!) Involve senior leadership if resources are a problem Page 21
22 Barriers & Resistance Barrier - Resistance : No one thinks there is a problem Take the high ground... We re different Share information and challenge assumptions... It s too difficult Look at others (internally & externally) that have successfully made a change Break ideas for change into small components Present changes as a test - that can be accepted, refined, or abandoned Use just enough data Post results of the small test from the outset as proof that it can happen Engage senior leadership Page 22

23 Adapting to Change Innovators 2.5% Early Adopters 13.5% Early Majority 34% Late Majority 34% Laggards 15% Identify your Early Adopters & engage their help Page 23
24 Barriers & Resistance Barrier - Problems with Ownership Be sure to include all affected areas Collaborate with staff at all levels Involve the people that DO the work Find champions in several disciplines Keep leaders informed and involved Page 24
25 Examples of CHN RCI Projects Glycemic Control: Managing blood sugars in the ICU CAP: Administering the correct antibiotics to pneumonia patients in a timely fashion SCIP: Giving surgery patients correct antibiotic & VTE prophylaxis and removing Foley catheters promptly CHF: Completing discharge education for heart failure patients Infection Control: Improving environmental cleaning in the OR Palliative Care: Providing comfort care to patients at end of life Falls: Preventing patient falls Customer Service: Improving patient satisfaction in the Emergency Center Quality: Decreasing the time it takes to gather Core Measure data Page 25
26 Glycemic Control in the ICU Facility A. Team Members: ICU, lab, pharmacy, IT, and physician members at Facility A. Specific Aim: Of all ICU blood glucose values, 80% or more will be in the optimal range of 60 to 180 mg/dl by Sept 15 th, Measure: % ICU blood glucose values mg/dl Page 26
27 Page 27




28 Facility A Pilot Blood Glucose Range Unit education, Hyperglycemia Audit started Pilot Approved as new Hospital A. order set 10 patient trial, 1:1 RN education D10W removed, pt criteria identified Baseline Period Mean: 77.35%


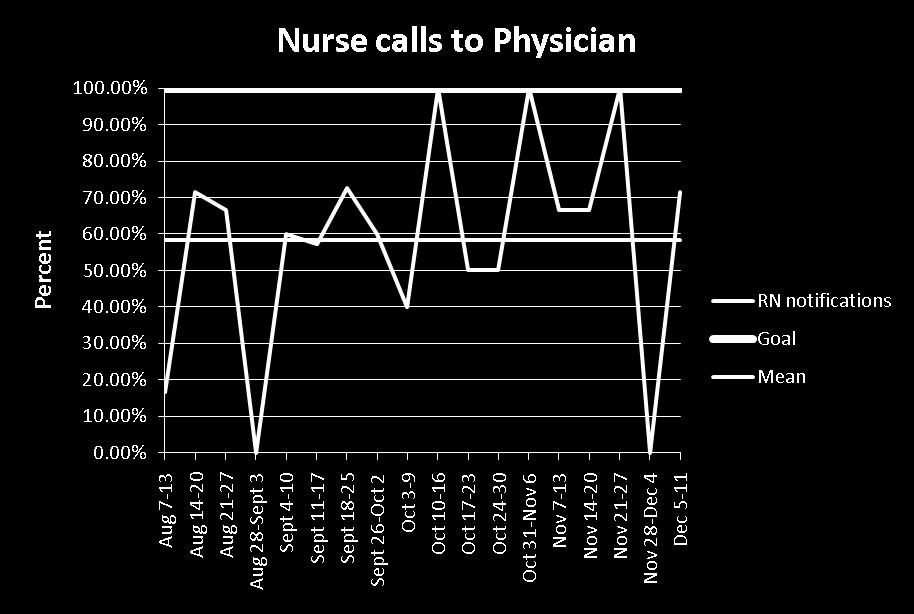
29 Nurse Call Compliance
30 Barriers and Resistance Facility A, Team leader leaving institution Identify new team leader before current team leader is gone Physicians (hospitalists) resistant to using insulin drips Encourage use by demonstrating reduced hypoglycemia with new orders Define patient population ideal for insulin drip use Revise subq insulin orders Page 30
31 Sustainability Plan Facility A Nursing Education: one-to-one remediation for noncompliance on hyperglycemia audit, reminders at safety briefs before each shift Data Monitoring: blood sugar reports reviewed weekly with team, posted weekly in ICU, reported monthly to administration Coaching: designated coaches on each shift for assistance and reinforcement of education Page 31
32 Glycemic Control Facility B Team Members: ICU, infection prevention, and physician members at Facility B. Specific Aim: For ICU patients undergoing cardiothoracic surgery, 80% or more of their blood glucose values will be in the optimal range of 60 to 180 mg/dl by Sept 15 th, Measure: % ICU blood glucose values mg/dl for ICU patients undergoing cardiothoracic surgery Page 32
33

34 Optimal Blood Glucose Range Facility B Auditing resumed Unit education completed, new protocol implemented

35 CHVI Blood Glucose Check Compliance Data Auditing stopped for protocol revision Concurrent, 100% auditing began Auditing resumed
36 Barriers and Resistance Facility B. Maintain high level of compliance while reducing audit frequency Continue to engage glycemic coaches Continue providing feedback (data) to staff Educate new RNs on insulin drip protocol Include in unit orientation before RN s first shift Glycemic coaches provide guidance during first few shifts to ensure understanding Page 36
37 Sustainability Plan Facility B Nursing Education: one-to-one remediation for noncompliance on insulin drip audit, insulin drip education update quarterly Data Monitoring: compliance reports reviewed monthly with team, posted biweekly in ICU, reported biweekly to administration Coaching: designated coaches on each shift for assistance and reinforcement of education Page 37
38 Lessons Learned Buy-in from physicians as well as nurses is key Anticipating and planning for barriers will help with implementation in the long run Obtaining accurate, timely data can be an unforeseen barrier Page 38
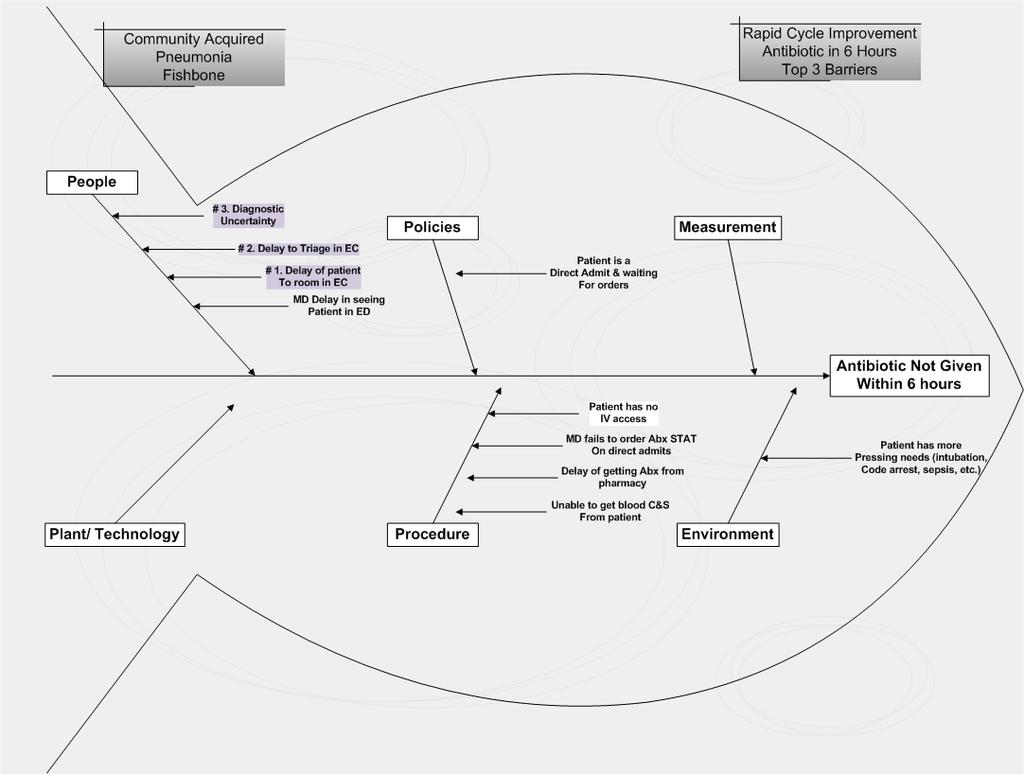
39 Community Acquired Pneumonia Antibiotic Selection Leverage Point: Physician use of pneumonia order sets Test of Change: Improve ease of access to order sets. Weekly feed back of order set use to CMO & physician champions. Robust review of charts that fall out for antibiotic selection by physician peers. Antibiotic in 6 Hours Leverage Point: Delay in identification of pneumonia patients entering the EC to the administration of antibiotic Test of Change: Weekly feedback to managers & nursing staff on antibiotic administered within 6 hours. Education & 1:1 counseling to nursing staff as needed. Page 39
40 Specific Aim & Measures AIM - 100% of Community Acquired Pneumonia patients will have appropriate selection & timely administration of antibiotics by September 15, 2011 Measures - Percentage of pneumonia patients with appropriate selection & timely administration of antibiotics Page 40
41 Team members From Two Facilities Infectious disease physician Primary care physicians Emergency department physicians Staff nurses Nurse managers Pneumonia core measure abstractors Pharmacist IT representative Page 41
42
43
44 Baseline Data Hospital A. Best Practice = 94.8% (Dec 2011)
45 Hosp A. Antibiotic Selection = 100% (Dec 2011) Hosp A. Antibiotic in 6 Hours = 100% (Dec 2011)
46 Baseline Data Hospital B. Best Practice = 100% (Dec 2011)
47 Hosp B. Antibiotic Selection = 100% (Dec 2011) Hosp B. Antibiotic in 6 hr = 100% (Dec 2011)
 Emergency Center")
48 Hospital A. Percent of Patients in Whom CAP Order Sets are Used (weekly) Emergency Center Use Admissions Use Meaningful Use Began Data not collected after 8/2011
49 Hosp B. Percent of Patients in Whom CAP Order Sets are Used (weekly) Emergency Center Use Admissions Use Initiated Robust Review of Fallouts 4/18/11 Meaningful Use Began 7/4/11
 Improve listing of order sets")
50 Ease of Access to Pneumonia Order Set for Physicians Place ICON on all hospital computer desktops for easier access to order sets (Completed Sept 2011) Improve listing of order sets Page 50
51 Barriers and Resistance EC Providers & Admitting Physicians Barriers: Physicians do not like using preprinted cook book order sets. They report there are barriers to locating order sets on line. Solution: Provide evidence via data demonstrating the use of order sets improves patient outcomes Provide education & coaching Remove barriers for locating electronic orders Page 51
52 Barriers and Resistance EC Nursing Staff & Unit Nursing Staff Barriers: Nurses worry about additional tasks but value change when they understand the benefits. Solution: Improve communication through timely feedback of information & data Provide education & coaching Web based training CE packet Page 52
53 Sustainability Education For physicians, nurses, & unit clerks on how to access preprinted order sets & components of core measures. Data Monitoring Monthly reporting of physician use of preprinted order sets. Reported to CMO s Weekly report to nursing departments on compliance with antibiotics within 6 hours Coaching 1:1 Coaching for all physician or nurses involved in fallouts Page 53




54 Pneumonia STATS: How Are We Doing? Hospital A For the week of September 26, 2011 Goal is 100%
55 Lessons Learned Getting someone to collect data is a challenge Weekly feedback to all nursing staff & managers 1:1 follow-up for fallouts by physicians & nursing managers Recognizing early adopters & shining stars Celebrating small victories Page 55

56 Questions? Page 56
57 References Kendrick, K. et al. Implementing projects using the rapid cycle approach; JONA; 3/2010; 20 (3): Valente, S. Rapid cycle change projects improve quality care; Journal of Nursing Care Quality; 4/2010; 26 (1) ASQ Quality Press; The public health quality improvement handbook; Berwick DM. A primer on leading the improvement of systems.bmj. 1996;312(9): Kotter JP. Leading change. Harvard Business Review 2007;85(1): Page 57
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Strategy/Driver Prevention Strategies Action Strategies
 I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Regenstrief Center for Healthcare Engineering
 Purdue University Purdue e-pubs RCHE Publications Regenstrief Center for Healthcare Engineering 3-31-2007 All Bundled Out - Application of Lean Six Sigma techniques to reduce workload impact during implementation
Purdue University Purdue e-pubs RCHE Publications Regenstrief Center for Healthcare Engineering 3-31-2007 All Bundled Out - Application of Lean Six Sigma techniques to reduce workload impact during implementation
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Quality/Performance Improvement Fundamentals
 Quality/Performance Improvement Fundamentals What to do and how to do it Skill Building Session May 29, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways
Quality/Performance Improvement Fundamentals What to do and how to do it Skill Building Session May 29, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways
3/30/2015. Objectives. Rationale for QAPI. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
Management and Culture
 Case Study Series on Surgical Care Improvement Measures: Improvement Strategies of Top-Performing Hospitals The following synthesis of performance improvement strategies is based on a case study series
Case Study Series on Surgical Care Improvement Measures: Improvement Strategies of Top-Performing Hospitals The following synthesis of performance improvement strategies is based on a case study series
SCIP. Surgical Care Improvement Project. Making Surgeries Safer. By: Roshini Mathew, RN
 SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
Change is Good: You Go First
 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE
 CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Quality Improvement (QI)
") Quality Improvement (QI) HOW DOES IT WORK? Dr S Narayanan Neonatal Consultant Watford General Hospital Outline of the talk Background Definitions QI What? Why? When? Where? How? Case study Discussion
Quality Improvement (QI) HOW DOES IT WORK? Dr S Narayanan Neonatal Consultant Watford General Hospital Outline of the talk Background Definitions QI What? Why? When? Where? How? Case study Discussion
Face to Face Nursing the Bedside
 Face to Face Nursing Report @ the Bedside Contact: Mary Kunkel, RN kunkelme@upmc.edu Campus: Shadyside "Patient Safety First...Care Always..." Project Aim Statement Improve Press Ganey survey scores from
Face to Face Nursing Report @ the Bedside Contact: Mary Kunkel, RN kunkelme@upmc.edu Campus: Shadyside "Patient Safety First...Care Always..." Project Aim Statement Improve Press Ganey survey scores from
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems. OHSU Performance Excellence
 Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems OHSU Performance Excellence DATE : April 1 8, 2 0 1 6 PRE SENTE D B Y: Nancy McCully MSN, MBA, RN, CCRN, Marge Willis
Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems OHSU Performance Excellence DATE : April 1 8, 2 0 1 6 PRE SENTE D B Y: Nancy McCully MSN, MBA, RN, CCRN, Marge Willis
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Value of HIT. Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017
 Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Engaging Learners Across Health Professions in Improving Care Together
 Session A17 / B17 These presenters have nothing to disclose Engaging Learners Across Health Professions in Improving Care Together Tuesday December 11, 2012 Objectives After this session, participants
Session A17 / B17 These presenters have nothing to disclose Engaging Learners Across Health Professions in Improving Care Together Tuesday December 11, 2012 Objectives After this session, participants
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Rapid Cycle Improvement
 Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Indiana Pressure Ulcer Reduction Initiative
 Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Fee: The fee for the 12-month renewal is $10,000.
 CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
Master of Science in Nursing (MSN) Concluding Graduate Experience (CGE) Handbook
 Concluding Graduate Experience (CGE) Handbook") CHAMBERLAIN UNIVERSITY Master of Science in Nursing (MSN) Concluding Graduate Experience (CGE) Handbook Welcome to your MSN Concluding Graduate Experience (CGE). All your previous graduate courses have
CHAMBERLAIN UNIVERSITY Master of Science in Nursing (MSN) Concluding Graduate Experience (CGE) Handbook Welcome to your MSN Concluding Graduate Experience (CGE). All your previous graduate courses have
Continuous Value Improvement in Health Care
 webinar summary Continuous Value Improvement in Health Care Featuring Kedar Mate Chief Innovation and Education Officer Institute for Healthcare Improvement October 26, 2017 sponsored by webinar summary
webinar summary Continuous Value Improvement in Health Care Featuring Kedar Mate Chief Innovation and Education Officer Institute for Healthcare Improvement October 26, 2017 sponsored by webinar summary
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
D Masina 1, J Ndirangu 1, I Choge 2, L Dayanund 3, C Bonnecwe 3, E Njeuhmeli 4, D Jacobs 1. Abstract no. WEPEE489
 Abstract no. WEPEE489 Improving client follow up in Voluntary Medical Male Circumcision (VMMC) programs through Continuous Quality Improvement (CQI): Experiences from South Africa D Masina 1, J Ndirangu
Abstract no. WEPEE489 Improving client follow up in Voluntary Medical Male Circumcision (VMMC) programs through Continuous Quality Improvement (CQI): Experiences from South Africa D Masina 1, J Ndirangu
Value Based Purchasing
 Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Improving Compliance
 Improving Compliance * The following planners, speakers, moderators, and/or panelists of this CME activity have no relevant financial relationships with commercial interests to disclose: Mary B. Johnson
Improving Compliance * The following planners, speakers, moderators, and/or panelists of this CME activity have no relevant financial relationships with commercial interests to disclose: Mary B. Johnson
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Tips and Tools for Learning Improvement. Developing Changes
 Tips and Tools for Learning Improvement Developing Changes What are changes in improvement? Making improvement requires change. Changes are any possible solutions to problems identified by improvement
Tips and Tools for Learning Improvement Developing Changes What are changes in improvement? Making improvement requires change. Changes are any possible solutions to problems identified by improvement
Transforming Care at the Bedside: Climbing the Clinical Ladder
 Transforming Care at the Bedside: Climbing the Clinical Ladder Rebecca Springer, MSN, RN Chief Nursing Officer, Nurse Executive Temiela Blackman, MA Quality Manager Hendry Regional Medical Center April
Transforming Care at the Bedside: Climbing the Clinical Ladder Rebecca Springer, MSN, RN Chief Nursing Officer, Nurse Executive Temiela Blackman, MA Quality Manager Hendry Regional Medical Center April
Learning Objectives. QAPI at a Glance: 8/22/16. Achieving Success with QAPI. Participants will be able to describe:
 Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
Quest for Excellence. Award Application. Bergan Mercy Medical Center Mercy Road. Omaha, Nebraska Contact:
 Quest for Excellence Award Application Bergan Mercy Medical Center 7500 Mercy Road Omaha, Nebraska 68124 Contact: Gail Brondum, Operations Director Quality Management Services gail.brondum@alegent.org
Quest for Excellence Award Application Bergan Mercy Medical Center 7500 Mercy Road Omaha, Nebraska 68124 Contact: Gail Brondum, Operations Director Quality Management Services gail.brondum@alegent.org
EMRAM Cases of Success
 EMRAM Cases of Success John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics @JohnHDaniels Why should we become a Stage 7 organization? NUMBER ONE QUESTION Why Use a Maturity
EMRAM Cases of Success John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics @JohnHDaniels Why should we become a Stage 7 organization? NUMBER ONE QUESTION Why Use a Maturity
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013
 Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
Preventing Health Care Associated Infections. PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011.
 Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Real Time Pressure Ulcer Data Drives Quality
 Real Time Pressure Ulcer Data Drives Quality Lisa Q. Corbett APRN ACNS-BC CWOCN Carol Strycharz RN BSN MPH Jamie A Curley RN BSN Nancy Ough LPN Rebecca Morton RN BSN CWCN Catherine Yavinsky RN MS NEA-BC
Real Time Pressure Ulcer Data Drives Quality Lisa Q. Corbett APRN ACNS-BC CWOCN Carol Strycharz RN BSN MPH Jamie A Curley RN BSN Nancy Ough LPN Rebecca Morton RN BSN CWCN Catherine Yavinsky RN MS NEA-BC
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
Quality/Performance Improvement Fundamentals
 Quality/Performance Improvement Fundamentals Getting Started Skill Building Session May 1, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways to strengthen
Quality/Performance Improvement Fundamentals Getting Started Skill Building Session May 1, 2013 Pat Teske, RN,MHA pteske@cynosurehealth.org (661)755-5317 Today Agenda for Today Review ways to strengthen
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Our Journey Towards CAUTI Freedom. Johnson City Medical Center
 Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
Clinical Safety & Effectiveness Cohort # 8
 Clinical Safety & Effectiveness Cohort # 8 Improvement of the Quality of Patient Messages DATE Educating for Quality Improvement & Patient Safety 1 FINANCIAL DISCLOSURE Muhammad Akram, MD has no relevant
Clinical Safety & Effectiveness Cohort # 8 Improvement of the Quality of Patient Messages DATE Educating for Quality Improvement & Patient Safety 1 FINANCIAL DISCLOSURE Muhammad Akram, MD has no relevant
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned
 On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
Lab Quality Confab Process Improvement Institute. New Orleans, LA. John Waugh 11/3/2015
 Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
DELAYED GASTRO EMPTYING
 DELAYED GASTRO EMPTYING Quality Improvement in Patient Discharge Dr Victoria Knott CT1 Context Two, thirty bed combined Gastroenterology wards at Northern General Hospital, Sheffield. There are four medical
DELAYED GASTRO EMPTYING Quality Improvement in Patient Discharge Dr Victoria Knott CT1 Context Two, thirty bed combined Gastroenterology wards at Northern General Hospital, Sheffield. There are four medical
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation. PADONA 2017 Annual Convention Hershey, PA.
 PADONA Annual Convention 2017 QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation PADONA 2017 Annual Convention Hershey, PA March 29, 2017 Your presenter today is:
PADONA Annual Convention 2017 QAPI: Quality Assurance Performance Improvement - Meeting the Requirements of Participation PADONA 2017 Annual Convention Hershey, PA March 29, 2017 Your presenter today is:
Grey Bruce Health Network Administrative Policies and Procedures
 Grey Bruce Health Network Administrative Policies and Procedures Policy Covering: Evidence-Based Effective Date: June 2006 Prepared by: Evidence- Based Coordinator Category: Patient Administration Policy
Grey Bruce Health Network Administrative Policies and Procedures Policy Covering: Evidence-Based Effective Date: June 2006 Prepared by: Evidence- Based Coordinator Category: Patient Administration Policy
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Title: Quality/Safety Education Physician Champion Phone:
 TeamSTEPPS 101: Know The Plan, Share The Plan Implementing A Customized Surgical Safety Checklist Team Communication Tool In Ambulatory And Inpatient Operating Rooms Organization Name: Christiana Care
TeamSTEPPS 101: Know The Plan, Share The Plan Implementing A Customized Surgical Safety Checklist Team Communication Tool In Ambulatory And Inpatient Operating Rooms Organization Name: Christiana Care
The LDL Challenge: Using Health Information Technology to Drive Clinical Quality Improvement
 The LDL Challenge: Using Health Information Technology to Drive Clinical Quality Improvement Tricia Lee Wilkins, Pharm D, PhD Kathy Reims, MD Cory Sevin, RN, MSN, NP March 11, 2014 Session C4 Financial
The LDL Challenge: Using Health Information Technology to Drive Clinical Quality Improvement Tricia Lee Wilkins, Pharm D, PhD Kathy Reims, MD Cory Sevin, RN, MSN, NP March 11, 2014 Session C4 Financial
Passage to Excellence Our Sepsis Journey
 Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Increased situational awareness to reduce undetected deterioration
 Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
ICAP Project: Introduction to Quality Improvement, Change Package, & Antibiotic Stewardship
 ICAP Project: Introduction to Quality Improvement, Change Package, & Antibiotic Stewardship AUGUST 28, 2014 Agenda Agenda Item Speaker Time Welcome and Introductions Faiza Khan 5 min Orientation to Quality
ICAP Project: Introduction to Quality Improvement, Change Package, & Antibiotic Stewardship AUGUST 28, 2014 Agenda Agenda Item Speaker Time Welcome and Introductions Faiza Khan 5 min Orientation to Quality
An economic - quality business case for infection control & Prof. dr. Dominique Vandijck
 An economic - quality business case for infection control & prevention @VandijckD Prof. dr. Dominique Vandijck What you/we all know, (hopefully) but do our healthcare executives, and politicians know this?
An economic - quality business case for infection control & prevention @VandijckD Prof. dr. Dominique Vandijck What you/we all know, (hopefully) but do our healthcare executives, and politicians know this?
Current Performance as stated on QIP2016/17
 Excellent Care for All Quality Improvement Plans (): Progress Report for The Progress Report is a tool that will help organizations make linkages between change ideas and improvement, and gain insight
Excellent Care for All Quality Improvement Plans (): Progress Report for The Progress Report is a tool that will help organizations make linkages between change ideas and improvement, and gain insight
When going Lean, Waste is the Enemy
 When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION
 ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative
 MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative Place picture here Sept. 12, 2017 Reminders For best sound quality, dial in at 1-800-791-2345 and enter code 11076 Please use the chat box to ask
MHA/OHA HIIN Antibiotic Stewardship/MDRO Collaborative Place picture here Sept. 12, 2017 Reminders For best sound quality, dial in at 1-800-791-2345 and enter code 11076 Please use the chat box to ask
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
PFAC as Consultant to Hospital Initiatives
 4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
Case Study High-Performing Health Care Organization March November
 Case Study High-Performing Health Care Organization March November 2009 2009 Kettering and Sycamore Medical Centers: Committing Resources to Surgical Quality Jennifer N. Edwards, Dr.P.H., and Ai m e e
Case Study High-Performing Health Care Organization March November 2009 2009 Kettering and Sycamore Medical Centers: Committing Resources to Surgical Quality Jennifer N. Edwards, Dr.P.H., and Ai m e e
COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL. Sepsis Treatment Order Sets Sepsis Treatment Order Sets
 Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
Agenda 2/10/2012. Project AIM. Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative
 Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative Marilyn A. Kacica, MD, MPH Chair Medical Director Division of Family Health NYSDOH Pat Heinrich, RN, MSN
Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative Marilyn A. Kacica, MD, MPH Chair Medical Director Division of Family Health NYSDOH Pat Heinrich, RN, MSN
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes
 Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes Presented by: VIRGINIA FLINTOFT, Manager, Central Measurement Team, Canadian Patient Safety Institute NARDIA BROWN, Clinical
Value of Safety Improvement Collaboratives for Home Care: Strategies and Outcomes Presented by: VIRGINIA FLINTOFT, Manager, Central Measurement Team, Canadian Patient Safety Institute NARDIA BROWN, Clinical
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Renfrew Victoria Hospital
 Renfrew Victoria Hospital Implementation of a Functional Abilities Measurement Tool TEAM MEMBER NAMES: Randy Penney, Executive Sponsor Charlene Hanniman, Team Lead Stefanie Coughlin, Team Member Chris
Renfrew Victoria Hospital Implementation of a Functional Abilities Measurement Tool TEAM MEMBER NAMES: Randy Penney, Executive Sponsor Charlene Hanniman, Team Lead Stefanie Coughlin, Team Member Chris
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing
 AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail: