Change is Good: You Go First
|
|
|
- Damon Wheeler
- 5 years ago
- Views:
Transcription
1 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009
2 Foundation s goals Support organizations that: Strengthen shared collaboration and partnership among relevant stakeholders, primary care agencies, faith-based organizations, community health organizations, social service agencies and community resources such as exercise and nutrition programs and medication/medical supply provides or other alternative community resources; Practice evidenced-based interventions that improve patient clinical outcomes; Are ready to make permanent changes to integrate diabetes self-management support throughout their care delivery systems; View self-management as an agency-wide, comprehensive approach to chronic illnesses Leverage resources (dollars, talent, shared responsibilities, services, etc) that improve patient care and their selfmanagement

3 Collaborative Partnership




4 Other Activated Patients The Patient Integrated plan Medical & SMG The Provider The Medical Assistant



5 Organizational Partnerships Community based peer support Primary Care Clinicians Patient Education Classes
6 Chronic Care Model Community Resources and Policies Self- Management Support Health System Health Care Organization Delivery System Design Decision Support Clinical Information Systems Informed, Activated Patient Productive Interactions Prepared, Proactive Practice Team Improved Outcomes
7 Planned Care Model Community Resources and Policies Self- Management Support Emphasize the patient's central role. Delivery System Design Health System Organization of Health Care Decision Support Clinical Information Systems Use effective selfmanagement support strategies that include Informed, Activated Patient assessment, goalsetting, action planning, problemsolving and follow-up. Productive Interactions Prepared, Proactive Practice Team Organize resources to provide support Functional and Clinical Outcomes
8 Three Key Components Patients with confidence and skills Health care team prepared and organized System with necessary supports
9 Current Practice What strategies or tools are you currently using to engage patients in managing their conditions?
10 Site Reviews - Teams Jordan Valley Short meaningful encounters Woven into flow of visit Optimal use of team esp nurses Should have engaged entire staff Provider buy in Right fit in hiring/tasking
11 Site Reviews - Teams CoxHealth Diabetes Center Multidisc Case Mgmt team Nurse, dietitian, counselor Cross training, scripting, MI skills Sustainability? Group visits?
12 PCRS and surveys PCRS lowest org. score Integration of SMS into primary care < 50% PCP s believe in the benefit of SMS PCRS lowest patient score emotional support
13 Site Reviews Teams/PCP Connection Barton County Mem. Hospital Group visits How to integrate more with office staff? Goals not always in front of PCP Eliciting barriers and follow up with tell us how you ve been doing relapse prevention
14 Site Reviews Teams/PCP Connection Morgan County Consult and referral, community supports Contracts signed by client and physician explain what we expect Consult notes Monitor progress every 3 months phone
15 Site Reviews Teams/PCP Connection Mississippi County Health Department Onsite educ session but still disconnect from PCP Best Flow Educ. visit before PCP? Some offices full day booked, others not Patients move from provider to provider
16
17 Who should be on your TEAM? How does a patient experience the flow of care before, during and after a visit with me or my team? How can I expand thinking about who could be on your team and how do you engage those folks to form a team? What could I do to increase information flow and coordination between parts of this team? Who are we not using?

18 Defining Tasks
19 Visit Flow RN reviews MD s upcoming schedule for patients with Hypertension and sends letters MD recruits patient during visit for SMS Patient declines Ask again at next visit Patient accepts MD/ RN huddle SMS with RN



20 SMS Flow RN provides SMS Patient s folder Action Plan Negotiate follow up My Care brochure Living Well Workshop brochure Patient Survey
21 Taking Perspective How can your work save others time? Protocols? Agreements? Can you offload tasks? What coordination efforts would help? Reimbursement issues? How to collaborate on follow up?
22 A Broader Definition of System Community what are the functions and what needs to happen. How do I do what I do best and help make sure we cover all of these things for patients.? Coordination of care and reducing waste Relationship building among parts of the system.
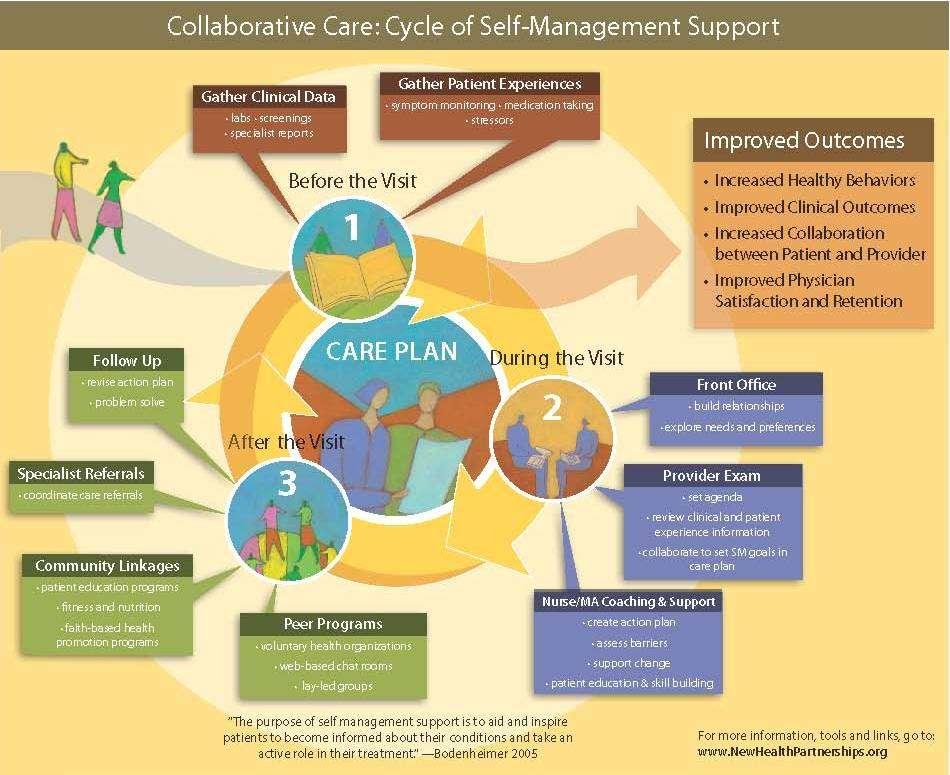
23 Two Views of SMS Portfolio of Tools and Techniques to help patients change behavior A fundamental transformation of the patient caregiver relationship into a collaborative partnership. Bodenheimer, CHCF.org 2007
24 Pt Education to SMS Not a Sage on the Stage, but a Guide on the Side Information is necessary, but not sufficient Patient should know what to do and feel confident they can do it
25 Site Reviews Partnering with patients and community U Miss Fam Medicine Expert, top down advice based vs Grass roots, bottom up cmty based CAB s/comm outreach-ongoing access to patient feedback Why are you not at the table? Nothing about me without me
26 Site Reviews Partnering with patients and community Missouri Highlands Healthcare Building Relationships lower the intimidation level Resource list, but real creative partnering community action agencies Relationships last after the funding ends sustainability Governing board and senior leader support
27 PCRS Patient supports PCRS lowest patient score emotional support Functional view of self management
28 Differences between Acute and Chronic Conditions ACUTE CHRONIC Beginning Rapid Gradual Cause Usually one Many Duration Short Indefinite Diagnosis Diagnostic tests Commonly accurate Often decisive Often uncertain Often limited value Treatment Cure common Cure rare
29 Differences Between Acute and Chronic Care Roles Role of Professional Role of Patient Lorig 2000 ACUTE Select and conduct therapy Follow orders CHRONIC Teacher/coach and partner Partner of health professionals responsible for daily management

30 Symptom Cycle Disease Fatigue Tense muscles Vicious Cycle Depression Stress/Anxiety Anger/Frustration/Fear
31
32 Dancing vs. Wrestling Tips on succeeding with SMS competencies Open the conversation in a positive way Offer a menu of options Ask what is important to the patient Make a plan Specify to make changes clear Support small changes Ask about confidence Adjust the plan until success is likely
33 My Health Choices Here are the things we have talked about. Which one is most important to work on right now? Irritating foods (write in others here) Testing Blood Sugar Walking Managing stress
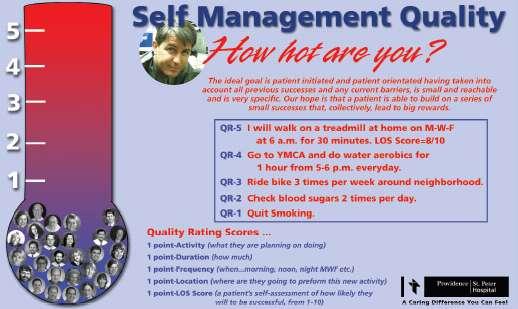
34 Partner Exercise Using an Action Plan Something you WANT to do Behavior specific What When How much How often Confidence level Follow-up plan
35
36 Change is Good: YOU go first Making small, incremental changes in practice Making changes that we WANT to do Embedding changes in routine practice activities Engaging a multidisciplinary team Finding new ways to connect practice and patients in the community
37 Moving from a Perfect Change to the Next Test PDSA or PPPP Plan Do Study Act or Plan Plan Plan Panic! How can we get away from drive to be "perfect" and instead use the Model for Improvement to start with small tests of change? A Question: What kind of challenges are you having testing change ideas using PDSA cycles?
38 Model for Improvement Setting Aims Establishing Measures Developing Changes What are we trying to accomplish? How will we know that a change is an improvement? What changes can we make that will result in improvement? Act Study Plan Do Adapted from Langley et al The Improvement Guide: A Practical Approach to Enhancing Organizational Performance 1996
39 The Plan-Do-Study-Act Cycle Plan: Do: Study: Act State the objective Predict what will happen and why Develop a plan (who, what, when, where, data to collect) Carry out the test. Document problems and unexpected observations Analyze the data Complete the analysis of the data Compare the data to your predictions Summarize what was learned What modifications should be made? What will happen in the next cycle?
40 What is a small PDSA? MODEL FOR IMPROVEMENT Cycle: Date: Objective(s) for this PDSA Cycle: Test new procedure getting patient s agenda for the visit: send out agenda form, front desk will check for form at check in and MA will provide additional form and explanation if patient hasn t brought it.. PLAN: QUESTIONS: (1) Will front desk remember to send form? (2) Will patient bring in completed form? (3) Will front desk check and MA provide? PREDICITONS: (1) Patients will complete the forms if they are provided by mail and in the office (2) Completed forms will give the physician time to introduce goal setting (3) Physician may still not introduce goal setting (4) Patients will like the forms and be more ready for the visit PLAN FOR CHANGE OR TEST: WHO, WHAT, WHEN, WHERE Who: physician, MA and front desk staff with 5 patients What: Use new agenda form with patients When: Week of November 28 Where: Five or more patients coming in for diabetes check back visits PLAN FOR COLLECTION OF DATA: WHO, WHAT, WHEN, WHERE MA will develop task list and place at front desk. review schedule will be reviewed to find
41 PDSA (Cont.) DO: CARRY OUT THE CHANGE OR TEST; COLLECT DATA AND BEGIN ANALYSIS. We planned to test the new form in five cases; however, two patients didn t fill in the form so we were able to test the change only three times. STUDY: COMPLETE ANALYSIS OF DATA; COMPARE TO PREDICTION, SUMMARIZE WHAT WAS LEARNED. The PCR remembered to send out the form and two patients brought them in. The MA gave the forms to the three other patients, but one refused it. One patient completed it in the room, the other read it but did not complete it. The physician did start the goalsetting conversation with four of the five patients, even though one patient had not filled it in. ACT: ARE WE READY TO MAKE A CHANGE? PLAN FOR NEXT CYCLE. Based on the initial test, the new plan is working pretty well. We plan to test again next week on five more patients with the PCR explaining the form a little more.


42 Repeated Use of the PDSA Cycle Improve Goal Setting Number of Goals Documented in Charts SMS Toolkit Changes That Result in Improvement Implementation of Change Wide-Scale Tests of Change Hunches Theories Ideas Very Small Scale Test Follow-up Tests
43 Series of PDSA Cycles to Improve Goal Setting Increased Goal Setting A P S D Cycle 5: Implement standards and monitor their use Use of Agenda setting tool will increase Goal Setting A P S D Cycle 4: Standardize process and agenda setting tool for best changes Cycle 3 Test best change with 1-3 MDs patients Cycle 2: Compare changes tes for one week Cycle 1: Define a small number of changes and test with staff
44 Why Test-Why Not Just Implement??
45 Why Test? Possible Objectives of PDSA Cycles for Testing Increase your belief that the change will result in improvement Opportunity for learning from failures without impacting performance Document how much improvement can be expected from the change Learn how to adapt the change to conditions in the local environment Evaluate costs and side-effects of the change Minimize resistance upon implementation
46 Current Situation Low Confidence that change idea will lead to Improvement High Confidence that change idea will lead to Improvement Appropriate Scope for a PDSA Cycle Cost of failure large Cost of failure small Cost of failure large Cost of failure small Staff/Physician Readiness to Make Change Resistant Indifferent Ready Very Small Scale Test Very Small Scale Test Very Small Scale Test Small Scale Test Very Small Scale Test Very Small Scale Test Small Scale Test Large Scale Test Very Small Scale Test Small Scale Test Large Scale Test Implement
47 Thought Provoking Questions What changes have you tested using effective PDSA cycles?
48 DRAFT DELIVERY SYSTEM DESIGN Assure the delivery of effective, efficient clinical care and self-management support. New tests are in italics and highlighted. CHANGE CONCEPT KEY CHANGES EXAMPLES YOU CAN TEST Define roles and distribute tasks among team members Define and develop the team as a unit. Determine process for care and assign team members to tasks. Match the work to the individual s licensure and capability. Cross train staff. Use protocols and standing orders for care. See also, decision support. Have receptionist obtain history, recent health info and VS, MD examines, RN does self-management and follow-up. Determine back-up staff for each task. Use protocols. Discuss everyone s planned care tasks as a unit. WHAT OUR TEAMS ARE TESTING: DIABETES PCAs assist Pts with PHQ9 at time of vitals (Cumberland) System implemented to ensure transitional flow (from Health Educator to Nutritionist to SW to MD) resulting in Pt receiving comprehensive care from all team members (East NY) Social Worker added to Team for planned visit days (Woodhull) Team Meetings prior to planned visits (Woodhull) Psychologist joined care team (Woodhull) Using team huddles to deliver care as team (Coney Island, Harlem) Providing care as a team consisting of PCP, PCA, dietary staff, clerical staff (Lincoln. Gouverneur)

49 Change Concepts, Theories, Ideas

50 Multiple PDSA Cycle Ramps Agenda Setting Goal setting Use of a Care Plan Standard follow up procedures Change Concepts
51 Team roles And Tasks Tools It Takes Work in Multiple Areas: Testing in Parallel Office Flow Cross Training Sr Leader Support A P S A P S D A P S A P S D D D A P S A P S A P S A P S D D A P S D D D A P S A P S D A P S A P S D D D A P S D A P S A P S A P D A P S D D A P S A P S D A P S D D A P S A P S A P Testing.Implementation.Spread S D A P S D S D A P S D D D Aim: Increase SMS Goals by 80%
52 Principles for Testing on a Small Scale Have others possessing some knowledge about the change review and comment on its feasibility Test the new product or the new process on the members of the team that developed the change before introducing it to others Incorporate redundancy in the test by making the change side-by-side with the existing process or product Develop a plan to simulate the change in some way Conduct the test in one facility or office in the organization, or with one customer Conduct the test over a short time period
53 Tips to Accelerate the Rate of Improvement Plan multiple cycles to test and adapt change Think a couple of cycles ahead Scale down size of initial test (# of patients, # of locations, time period, etc.) Test with volunteers Do not try to get buy-in or consensus for the test Be innovative to make the test feasible Collect useful data during each test In later cycles, include a wide range of conditions

54 Promotoras/Community Health Workers

55 Peer Led Workshops

56 Outreach

57 Organizations
58 Partnering Relationships involvement collaborating cooperating commitment resources coordinating networking

59 Environment and Policy

60 Walkable Neighborhoods/ Cyclovia

61 It Takes a Region
62 Online Resources
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Rapid Cycle Improvement
 Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Implementing Health Coaching
 Implementing Health Coaching Presented by: Amireh Ghorob, MPH Adriana Najmabadi Camille Prado UCSF Center for Excellence in Primary Care IHI Summit 2014, Washington DC March 10, 2014 Session: L9 These
Implementing Health Coaching Presented by: Amireh Ghorob, MPH Adriana Najmabadi Camille Prado UCSF Center for Excellence in Primary Care IHI Summit 2014, Washington DC March 10, 2014 Session: L9 These
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Learning Objectives. QAPI at a Glance: 8/22/16. Achieving Success with QAPI. Participants will be able to describe:
 Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
Achieving Success with QAPI John Leon, RN, MPH Nursing Homes Projects Specialist, OFMQ Learning Objectives Participants will be able to describe: QAPI Process Review Data/ Identify Priorities Set Improvement
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Team Integration Strategies
 Team Integration Strategies Making the Change to Team-Based Care Melissa Schoen, Schoen Consulting Cindy Barr, Capital Link Advancing the Financial Strength of L.A. County Clinics February 10, 2017 1 Dividing
Team Integration Strategies Making the Change to Team-Based Care Melissa Schoen, Schoen Consulting Cindy Barr, Capital Link Advancing the Financial Strength of L.A. County Clinics February 10, 2017 1 Dividing
NATIONAL STANDARDS, ESSENTIAL ELEMENTS AND INTERPRETIVE GUIDANCE
 Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Blending Behavioral Health and Primary Care. Applying the Model. Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist
 Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers. Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW
 Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Tools for Better Health. Referral Toolkit. Health Care Providers
 Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Assessment of Chronic Illness Care Version 3
 Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Working at Top of License How do you reallocate work among a team? January 28, 2015
 Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Assessment of Chronic Illness Care Version 3.5
 Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
EVOLENT HEALTH, LLC. Asthma Program Description 2018
 EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Using Innovation to Maximize Behavioral Health Accommodations. Regions Hospital Case Study
 Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Example 1: Self-Management: Development of a Self-Management form, Part 1
 PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
PDSA examples Example 1 We have concentrated on a collection of PDSA cycles that are relatively small in focus and time span, to emphasise the importance of small, rapid tests of change. Many of these
A8/B8: Self-Management: Critical to Chronic Care
 A8/B8: Self-Management: Critical to Chronic Care Brian Sandoval, Psy.D. Erin Wnorowski, MPH, PCMH CCE IHI 2015 Summit March 2015 Disclosures Erin Wnorowski is an employee of Arcadia Healthcare Solutions
A8/B8: Self-Management: Critical to Chronic Care Brian Sandoval, Psy.D. Erin Wnorowski, MPH, PCMH CCE IHI 2015 Summit March 2015 Disclosures Erin Wnorowski is an employee of Arcadia Healthcare Solutions
Arizona Living Well Institute
 HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
5A s Model for Self Management
 5A s Model for Self Management 5A s Model for Self Management The Five A s is a counseling approach that entails a series of sequential steps to facilitate patient selfmanagement and behavior change (World
5A s Model for Self Management 5A s Model for Self Management The Five A s is a counseling approach that entails a series of sequential steps to facilitate patient selfmanagement and behavior change (World
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Central Oregon Integrated Care Collaborative: Operational Strategies for Success
 Central Oregon Integrated Care Collaborative: Operational Strategies for Success 1 May 8, 2018 2 Welcome! Mike Franz, MD, DFAACAP, FAPA Medical Director, Behavioral Health, PacificSource Thanks to the
Central Oregon Integrated Care Collaborative: Operational Strategies for Success 1 May 8, 2018 2 Welcome! Mike Franz, MD, DFAACAP, FAPA Medical Director, Behavioral Health, PacificSource Thanks to the
EVOLENT HEALTH, LLC. Asthma Program Description 2017
 EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
Patient Referrals to Self-Management Programs
 October 26, 2016 Patient Referrals to Self-Management Programs Janet Tennison PhD, MSW, LCSW Senior Project Manager HealthInsight Quality Innovation Network (QIN) Quality Improvement Organization (QIO)
October 26, 2016 Patient Referrals to Self-Management Programs Janet Tennison PhD, MSW, LCSW Senior Project Manager HealthInsight Quality Innovation Network (QIN) Quality Improvement Organization (QIO)
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
INVESTING IN INTEGRATED CARE
 INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
Table of Contents for CCC Toolkit
 Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION
 ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
Integrated Behavioral Health
 1, Core Competencies, Chapter 16 Integrated Behavioral Health Contributor: Michael Mabanglo and Elizabeth Morrison Edited by Marc Avery Revision Date: 2/6/17 Definition and Why Supporting Integrated Behavioral
1, Core Competencies, Chapter 16 Integrated Behavioral Health Contributor: Michael Mabanglo and Elizabeth Morrison Edited by Marc Avery Revision Date: 2/6/17 Definition and Why Supporting Integrated Behavioral
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
Family Practice Clinic
 Family Practice Clinic FNP Job Description (Hospital Privileges) General: The Family Nurse Practitioner (FNP) assesses, plans and provides comprehensive patient care independently or in autonomous collaboration
Family Practice Clinic FNP Job Description (Hospital Privileges) General: The Family Nurse Practitioner (FNP) assesses, plans and provides comprehensive patient care independently or in autonomous collaboration
Patient Centered Medical Home Clinician Assessment
 Patient Centered Medical Home Clinician Assessment Please answer the following questions based on the procedures and approaches used by you and your immediate care team (e.g. those nurses and office staff
Patient Centered Medical Home Clinician Assessment Please answer the following questions based on the procedures and approaches used by you and your immediate care team (e.g. those nurses and office staff
MAKING PROGRESS, SEEING RESULTS
 MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Healthcare 9/15/2017. Learning Outcomes. Transforming Clinical and Fiscal Outcomes through Staff Nurse Driven Change
 Transforming Clinical and Fiscal Outcomes through Staff Nurse Driven Change Marian Altman RN, MS, CNS-BC, CCRN-K,ANP American Association of Critical Care Nurses Clinical Practice Specialist Learning Outcomes
Transforming Clinical and Fiscal Outcomes through Staff Nurse Driven Change Marian Altman RN, MS, CNS-BC, CCRN-K,ANP American Association of Critical Care Nurses Clinical Practice Specialist Learning Outcomes
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
A M.A.P. for improving blood pressure: Application within the QIN-QIO community
 A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health
 PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Using a Patient-Centered Care Plan and Teamwork to Support Self-Management
 Using a Patient-Centered Care Plan and Teamwork to Support Self-Management Speakers: Larry Mauksch, MEd, Senior lecturer and licensed mental health counselor, UW Department of Family Medicine; and Berdi
Using a Patient-Centered Care Plan and Teamwork to Support Self-Management Speakers: Larry Mauksch, MEd, Senior lecturer and licensed mental health counselor, UW Department of Family Medicine; and Berdi
The Palliative Care Quality Network s Quality Improvement Collaborative. Kara Bischoff, MD PCQN Spring Conference May 13, 2015
 The Palliative Care Quality Network s Quality Improvement Collaborative Kara Bischoff, MD PCQN Spring Conference May 13, 2015 Agenda: Session 1 The QI landscape in PC How the PCQN can help you excel The
The Palliative Care Quality Network s Quality Improvement Collaborative Kara Bischoff, MD PCQN Spring Conference May 13, 2015 Agenda: Session 1 The QI landscape in PC How the PCQN can help you excel The
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Team Based Care Assessment & Action Plan
 Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI
 COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Anthem Blue Cross and Blue Shield is the trade name of: In Colorado: Rocky Mountain Hospital and Medical
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Anthem Blue Cross and Blue Shield is the trade name of: In Colorado: Rocky Mountain Hospital and Medical
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI,
 Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI, aeslan@jsi.com CO Team-Based Care Initiative Change Package
Colorado Team-Based Care Initiative Change Package Tool Made possible with funding from the Colorado Health Foundation Contact: Alexia Eslan, JSI, aeslan@jsi.com CO Team-Based Care Initiative Change Package
Discussion Board in Learning Community Site
 Discussion Board in Learning Community Site The Discussion Board feature allows you to start discussion threads, share resources, and ask questions or seek input from the Care Partners community. Make
Discussion Board in Learning Community Site The Discussion Board feature allows you to start discussion threads, share resources, and ask questions or seek input from the Care Partners community. Make
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System
 Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Clinical Nurse Leader (CNL ) Certification Exam. Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012)
 Certification Exam. Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012)") Clinical Nurse Leader (CNL ) Certification Exam Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012) Subdomain Weight (%) Nursing Leadership Horizontal Leadership
Clinical Nurse Leader (CNL ) Certification Exam Subdomain Weights for the CNL Certification Examination Blueprint (effective February 2012) Subdomain Weight (%) Nursing Leadership Horizontal Leadership
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Patient and Provider Perspectives of Self-Management of Ulcers in SCI/D
 OFFICE of RESEARCH & DEVELOPMENT Patient and Provider Perspectives of Self-Management of Ulcers in SCI/D Dawn Ehde, PhD 1 Marylou Guihan, PhD 2 August 28, 2013 VETERANS HEALTH ADMINISTRATION Disclaimer
OFFICE of RESEARCH & DEVELOPMENT Patient and Provider Perspectives of Self-Management of Ulcers in SCI/D Dawn Ehde, PhD 1 Marylou Guihan, PhD 2 August 28, 2013 VETERANS HEALTH ADMINISTRATION Disclaimer
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Agenda 2/10/2012. Project AIM. Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative
 Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative Marilyn A. Kacica, MD, MPH Chair Medical Director Division of Family Health NYSDOH Pat Heinrich, RN, MSN
Improving Perinatal Health Outcomes: New York State Obstetric and Neonatal Quality Collaborative Marilyn A. Kacica, MD, MPH Chair Medical Director Division of Family Health NYSDOH Pat Heinrich, RN, MSN
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
NICU Graduates: Using the Model for Improvement and Learning from Data
 NICU Graduates: Using the Model for Improvement and Learning from Data Kristin Voos, MD and Dan Benscoter, DO Learning Session May 10, 2016 Through collaborative use of improvement science methods, reduce
NICU Graduates: Using the Model for Improvement and Learning from Data Kristin Voos, MD and Dan Benscoter, DO Learning Session May 10, 2016 Through collaborative use of improvement science methods, reduce
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.