Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
|
|
|
- Abel Randall
- 5 years ago
- Views:
Transcription
1 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1
2 ARE OUR OPERATING ROOMS SAFE? Not as safe as they could be. 2
3 Evidence for danger in the O.R. 3
4 Evidence for danger in the O.R. Orthopedic Surgeons 25% chance of performing wrong side surgery during their career. 4
5 Evidence for danger in the O.R. Hand surgeons -20% revealed that they had operated on the wrong side at least once. 16% had prepared to operate on the wrong side but were caught at the last minute by a colleague. Wachter, Robert M.D., Kaveh A. Shejania, M.D. Internal Bleeding, page 131. Meinberg, E.G., Stern, P.J., Incidence of wrong-site surgery among hand surgeons, Journal of Bones and Joint Surgery 85-A (2003). Pp
6 Evidence for danger in the O.R. Surgeons with the highest workloads reported the highest incident of operating on the wrong side. Wachter, Robert M.D., Kaveh A. Shejania, M.D. Internal Bleeding, page 131. Meinberg, E.G., Stern, P.J., Incidence of wrong-site surgery among hand surgeons, Journal of Bones and Joint Surgery 85-A (2003). Pp
7 Wall Street Journal Wed., Nov. 16, incidents [were reported] thirtythree percent of incidents resulted in permanent disability and 13% in patient death. Seventy-seven percent involved injuries related to an operation or other invasive intervention (visceral injuries, bleeding, and would infection/dehiscence were the most common subtypes) 7
8 Major complications occur in 3-20% of cases Gawande, AA, et al. Surgery 1999; 126:
9 Potential Patient Harm Occurs everyday in operating rooms Incorrect timing of antibiotics No DVT prophylaxis Case delays Communication failures Incorrect sponge counts Mislabeled specimens 9
10 10

11 Safety in Surgery 11
12 Safety in Surgery In 75% of wrong side surgeries, or sentinel events, someone knew something and did not speak up. 12
13 Errors can occur because of the intense atmosphere of the OR, where surgeons are the captains of the ship, treated with deference because of their unique skills. As a result, nurses, prep technicians and other aides can be afraid to speak up if they spot a problem. Now, some hospitals are taking new steps to combat this fearful atmosphere. They are putting programs in place to improve surgeons attitudes about teamwork Surgery, Vol.133, No. 6 p , June
14
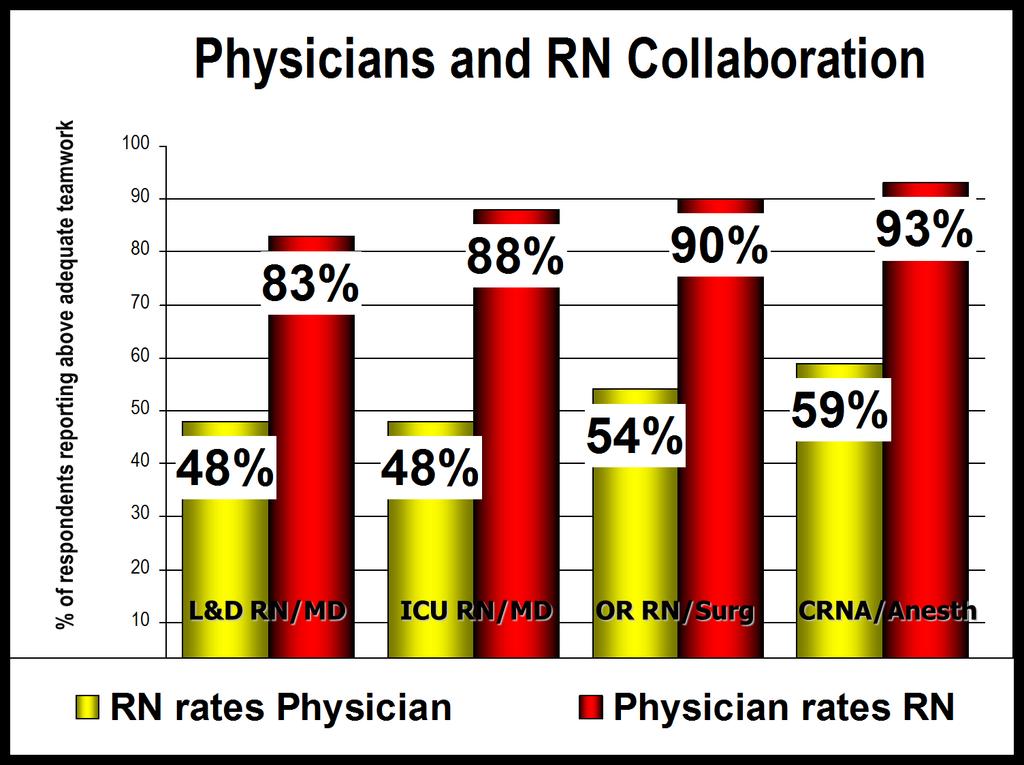
15 Safety in Surgery A survey of surgical team members attitudes about communication 40% of surgeons believe that junior team members should not question decisions of senior team members 40% of surgical nurses rated the quality of teamwork and collaboration with surgeons as low Sexton JB, et al. BMJ. 2000; 320:
16 Teamwork Disconnect RN: Good teamwork means I am asked for my input Physician: Good teamwork means the nurse does what I say 16
17 System Failures Leading to Communication Breakdown Differences between team members goals Differences between team members interpretation or events Knowledge that did not make it into the team consciousness Due to fear of speaking up or assumption that others already know Environmental features Noise, lighting, new equipment or technology Dekker S. The field guide to human error investigations,
18 Our Clinical Work Environment No ability to control or predict workload Incomplete, conflicting information Rapidly changing, evolving scenarios Fatigue, sustained operations Performance pressure, life/death outcome Operational pressure Distractions & auditory overload 18
19 19
20 Improving Communication Standardized work processes, creating independent checks, and learning from adverse events and strategies to reduce errors in teamwork. Pronovost, P.J. Health Serv. Res 41: , Aug Pronovost, P.J. Berenholtz, S.M. BMJ 337: Oct
21 Improving Communication Briefings and Debriefings are strategies to improve communication in the O.R. Makary, M.A. Jt. Comm. J Qual Patient Saf 32: , Jun Makary, M.A. Jt. Comm. J Qual Patient Saf 32: , Jul
22 Improving Communication Surgical checklists have been shown to decrease death and complication rates Haynes, A.B. et al. NEJM 2009 Jan. 29; 360(5):
23 Improving Communication Implementations of a medical team training program can reduce surgical mortality Neily, J. et al. JAMA 2010 Oct. 20; 304 (15):
24 Improving Communication Utilizing briefings and debriefings are associated with reductions in or delays Nundy, S. Arch Surg. 2008;143(11):
25 Improving Communication Teamwork and communication in O.R. s can be improved by using briefings and debriefings Berenholtz, S.M. et al. 2009;35(8): Jt. Comm. J Quality Patient Saf. Makary, M.A. et al. J Am Coll Surg. 2007; 204(2):
26 BEAUMONT HOSPITAL ROYAL OAK 26
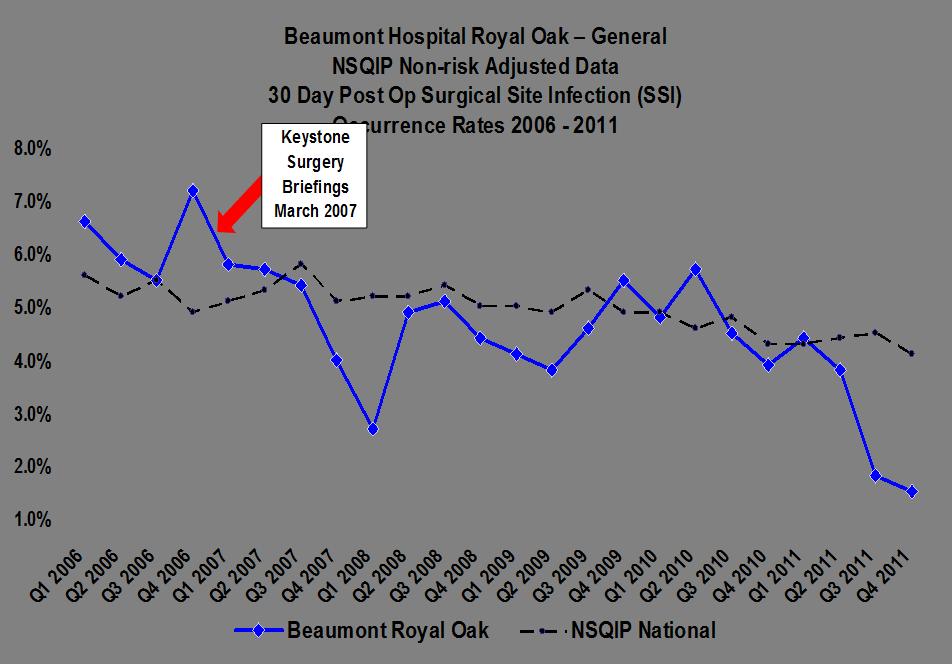
27 Initial Steps Program developed in conjunction with Johns Hopkins Quality and Safety Research Group, and the Michigan Health and Hospital Association (2006) Baseline culture assessment taken (April 2006) Developed Science of Safety education (CUSP), and briefing/debriefing tool (May-Sept 2006) Staff education on the Science of Safety (assertion, situational awareness, team communication, and conflict resolution) (September 2006) Roll-out briefings/debriefings (October 2006) Pilot Teams (thoracic and selected orthopedics) A step approach was taken to expand to all operating rooms (Oct 2006-Sept 2007) Over 100,000 briefings/debriefings performed to date Compliance to date average 92% 27
28 Initial Steps 1. Safety Culture Assessment 2. Educate staff and leadership on Science of Safety - assertion - communication - decision making - embedded into orientation - situational awareness 3. Executive partnership 4. Implement teamwork tools - Surgical briefings/debriefings - Culture debriefing tool 5. Learn from Defects - Tracking/reporting of defects in surgery 28
29 Initial Steps Keystone Surgery is combination of technical and adaptive methods to implement sustainable change in surgery that ultimately improved patient safety and outcomes Improved teamwork communication (briefings and debriefings) Elimination of mislabeled specimens 29
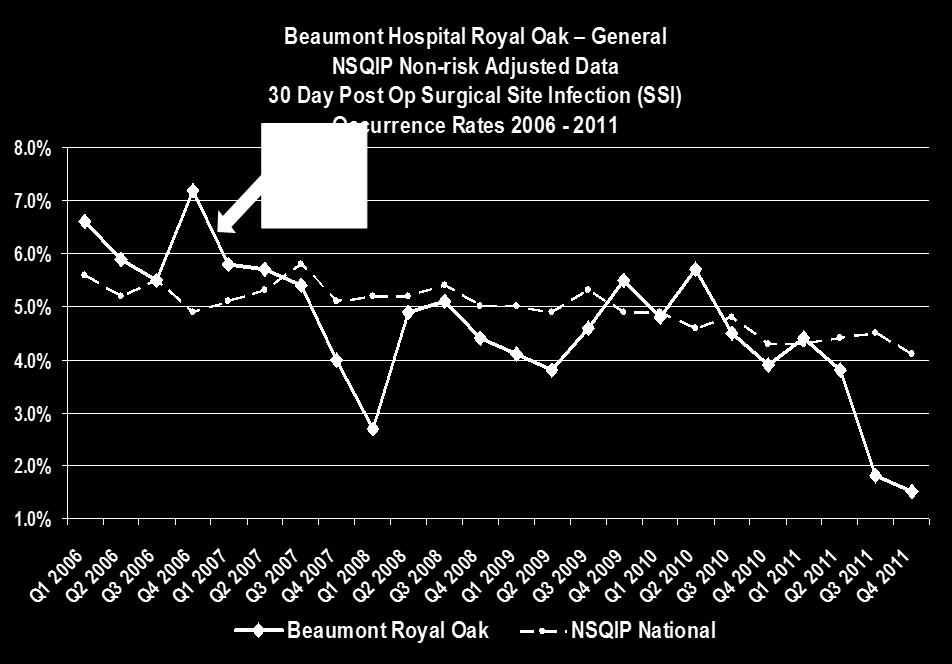
30 Initial Steps Reduction in surgical site infections Elimination of retained foreign objects Improved culture of safety 30
31 Briefing OR teams are comprised of a group of multidisciplinary providers who may or may not know each other Each team member has specific priorities and roles No one is aware of every detail involved in the case Many things happen before the patient arrives in the OR, briefing is the time to share this information 31
32 Briefing A discussion between the OR team, using succinct information pertinent to the present case. Increases situational awareness through clear and effective communication 32
33 Briefing Identifies the roles and responsibilities of each team member Key considerations relating to the case Heightens awareness of the situation Allows the team to plan for the unexpected Team members needs and expectations are met 33
34 Briefing Situational awareness is the ability of the team to have the same understanding of what is occurring during the procedure; the big picture. Focus is on: Preparation and planning Patient care Distraction avoidance 34
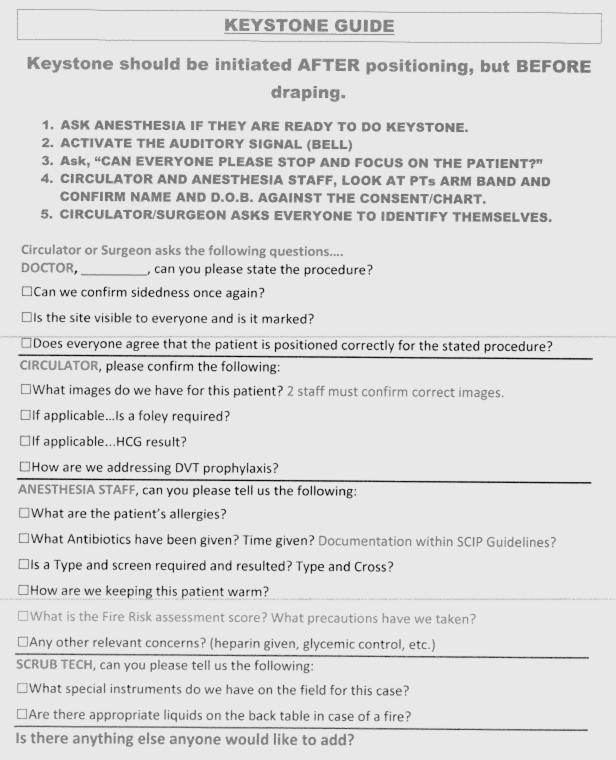
35 Briefing Template 1. ASK ANESTHESIA IF THEY ARE READY TO DO KEYSTONE. 2. ACTIVATE THE AUDITORY SIGNAL (BELL) 3. Ask, CAN EVERYONE PLEAST STOP AND FOCUS ON THE PATIENT? 4. CIRUCLATOR AND ANESTHESIA STAFF, LOOK AT PTs ARM BAND AND CONFIRM NAME AND D.O.B. AGAINST THE CONSENT/CHART. 5. CIRUCULATOR/SURGEON ASKS EVERYONE TO IDENTIFY THEMSELVES. Circulator or Surgeon asks the following questions.. DOCTOR,, can you please state the procedure? Can we confirm sidedness once again? Is the site visible to everyone and is it marked? Does everyone agree that the patient is positioned correctly for the stated procedure? CIRCULATOR, please confirm the following: What images do we have for this patient? 2 staff must confirm correct images. If applicable Is a foley required? If applicable..hcg result? How are we addressing DVT prophylaxis? ANESTHESIA STAFF, can you please tell us the following: What are the patient s allergies? What Antibiotics have been given? Time given? Documentation within SCIP Guidelines? Is a Type and screen required and resulted? Type and Cross? How are we keeping this patient warm? Anything other relevant concerns? (heparin given, glycemic control, etc.) SCRUB TECH, can you please tell us the following: What special instruments do we have on the field for this case? Are there appropriate liquids on the back table in case of a fire? Is there anything else anyone would like to add? In Accordance with Beaumont Policy #463 and Mandatory Keystone Computer Module March
36 Role of the Nurse Initiates briefing process by beginning introductions and verifying information on the white board Are all necessary instruments available? Will any special equipment be considered? Are correct films available Review allergies Plan for breaks Staff that relieve for breaks or at the end of the shift to introduce themselves when switching. 36
37 Role of Surgeon Discuss risks associated with procedure Provide team with pertinent information, including any anticipated problems Encourages participation from all team members Assures that everyone is familiar with the equipment to be used Any anticipated changes from standard preferences Expected blood loss and length of case At the end of the briefing surgeon states: If anyone has a concern now or during the case, please let me know. 37
38 Role of Anesthesia Discuss co-morbidities that increase patient s risk Aspects of surgery that increase risk Availability of blood products Abnormal test results impacting the case Discuss position and warming considerations DNR status Interventions to prevent complications 38
39 Time Out/Final Verification Review Critical Information Is this the correct patient? Is the correct site or side marked? Has the procedure been agreed upon? Have antibiotics been given? 39
40 Debriefing A process to enhance patient safety that gives the team the opportunity to learn from a shared experience, or significant event that has occurred. A review of pertinent issues at the end of the case. 40
41 Debriefing An opportunity to discuss what went well and what could be done differently to improve patient care in the future. Identifies barriers to the effective and efficient delivery of care. May define follow up responsibilities of team members 41
42 Who, when All team members should participate in the debriefing Complete at an appropriate time after first counts have been performed 42
43 Debriefing Guidelines Remind staff of the purpose and stay focused Reinforce goal: improvement not blame Listen to what others have to say Remember everyone is human! Assign follow up as needed How can information be disseminated to those not present? 43
44 Review of Critical Information Were counts correct? Are specimens all labeled properly? Post-op diagnosis Verification of procedure completed EBL Any special post-op considerations? (ICU bed, vent etc) 44
45 Debriefing Questions Did anything occur during the case with the patient or equipment that may have negatively impacted patient care? Were there any breakdowns in team communication that could have been improved? Is there anything that could have been done differently to improve patient care? If so, what follow up is required to correct these situations in the future? Who will be responsible for this follow up? 45
46 Debriefing Debriefing can lead to: Change in process, more effective future performance Revised or new procedures Improved teamwork Staff satisfaction All of these lead to enhanced patient safety 46
47 47
48 Briefings/Debriefings Results Findings included: Inappropriate timing of antibiotics Blood not available prior to case starting Equipment not available or unusable Inappropriate timing of DVT prophylaxis Lab results not available Insufficient number of supplies Consent not signed; consent not completed correctly Wrong surgery side marked AICD not being turned off in pre-op 48
49 What Is In It For the Surgeon? Better patient outcomes! Reduces ill-timed breaks by staff Reduces interruptions and distractions Early resolution of equipment issues Reduced delays in receiving equipment Reduced case delay or cancellations Nundy, S. Arch. Surg. 2008; 143(11):
50 50
51 51
52 Beaumont s Findings Effective communication and teamwork are critical in many health care settings, particularly the operating room (OR). Several studies have implicated failures of communication and teamwork as the root cause in a high proportion of sentinel events in the OR. Implementation of a standardized briefing and debriefing tool was a practical and feasible strategy to improve perceptions of interdisciplinary communication and teamwork in the OR. Berneholtz, S.M. et al. Implementing standardized operating room briefings and debriefings at a large regional medical center. Jt Comm Jt Qual Patient Saf. 2009;35(8):
53 Beaumont s Findings Briefings and debriefings are a practical and effective strategy to surface potential surgical defects in the operating rooms. Further research is needed to evaluate the impact of mitigating defects on clinical and economic outcomes. Bandari J., et al. Surfacing Safety Hazards using Standardized Operating Room Briefings and Debriefings at a Large Regional Medical Center. Jt Comm J Qual Patient Saf. 2012;38(4):
54 54
55 55
56 Contact Information William Beaumont Hospital Robert J. Welsh, MD Phone: (248)
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Failure Mode and Effects Analysis (FMEA) for the Surgical Patient
 for the Surgical Patient") How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
Crew Resource Management for Trauma Resuscitation. Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation
 Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Enhancing Patient Safety through Team Work and Communication Strategies
 Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Title: Learning from Defects Learning from and Preventing adverse events
 Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
"Using Simulation to Improve Operating Room Efficiency and Safety"
 "Using Simulation to Improve Operating Room Efficiency and Safety" Phyllis A. Toor RN BSN United States Army Medical Command Nurse Consultant/TeamSTEPPS Program Manager Patient Safety Program 1 Objective
"Using Simulation to Improve Operating Room Efficiency and Safety" Phyllis A. Toor RN BSN United States Army Medical Command Nurse Consultant/TeamSTEPPS Program Manager Patient Safety Program 1 Objective
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
SAMPLE Perioperative Self-Assessment Questionnaire
 SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Organizational Culture Change Results in Improvement in Outcomes, Value and Experience. Elizabeth C. Wick, M.D.
 Organizational Culture Change Results in Improvement in Outcomes, Value and Experience Elizabeth C. Wick, M.D. Objectives To describe the burden and complexity of surgical site infections To outline the
Organizational Culture Change Results in Improvement in Outcomes, Value and Experience Elizabeth C. Wick, M.D. Objectives To describe the burden and complexity of surgical site infections To outline the
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Communication failure in the operating room
 Communication failure in the operating room Amy L. Halverson, MD, a Jessica T. Casey, MD, b Jennifer Andersson, RN, c Karen Anderson, RN, d Christine Park, MD, e Alfred W. Rademaker, PhD, f and Don Moorman,
Communication failure in the operating room Amy L. Halverson, MD, a Jessica T. Casey, MD, b Jennifer Andersson, RN, c Karen Anderson, RN, d Christine Park, MD, e Alfred W. Rademaker, PhD, f and Don Moorman,
Take ACTION: A Collaborative Approach to Creating a Culture of Safety
 Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
A Practical Tool to Learn From Defects in Patient Care
 Tool Tutorial A Practical Tool to Learn From Defects in Patient Care Peter J. Pronovost, M.D., Ph.D. Christine G. Holzmueller Elizabeth Martinez, M.D., M.H.S. Christina L. Cafeo, R.N., M.S.N. David Hunt,
Tool Tutorial A Practical Tool to Learn From Defects in Patient Care Peter J. Pronovost, M.D., Ph.D. Christine G. Holzmueller Elizabeth Martinez, M.D., M.H.S. Christina L. Cafeo, R.N., M.S.N. David Hunt,
Wrong Site, Wrong Procedure, Wrong Person Surgery
 Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
The Clinician s Impact on the Patient Experience
 The Clinician s Impact on the Patient Experience Michelle George MSN RN CASC 1 Objectives Achieving desired clinical outcomes through safety initiatives and clinical best practices Communication and engagement
The Clinician s Impact on the Patient Experience Michelle George MSN RN CASC 1 Objectives Achieving desired clinical outcomes through safety initiatives and clinical best practices Communication and engagement
NoCVA SSI/VTE Safe Surgery Collaborative
 NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs
 Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
The Reliable Design of Obstetric and Gynecologic Care
 VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
Surgery Road Map. General practices. Road map sections
 Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Raising the bar for safety in the handling of surgical specimens Is this specimen fresh or frozen? Is it routine, or does it require a lung protocol?
 Patient safety Raising the bar for safety in the handling of surgical specimens Is this specimen fresh or frozen? Is it routine, or does it require a lung protocol? Does it go to the frozen section lab
Patient safety Raising the bar for safety in the handling of surgical specimens Is this specimen fresh or frozen? Is it routine, or does it require a lung protocol? Does it go to the frozen section lab
Multi disciplinary Team Communication and Effective Handoffs
 Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Electronic Surgical Scheduling Improves Patient Safety and Productivity
 Electronic Surgical Scheduling Improves Patient Safety and Productivity Katrina Spears, MA, Manager Business & Informatics Surgical Services Lina Munoz, BSN, RN, CPAN Manger Presurgical Testing, PACU,
Electronic Surgical Scheduling Improves Patient Safety and Productivity Katrina Spears, MA, Manager Business & Informatics Surgical Services Lina Munoz, BSN, RN, CPAN Manger Presurgical Testing, PACU,
Development and assessment of a Patient Safety Culture Dr Alice Oborne
 Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
To err is human. When things go wrong: apology and communication. Apology and communication position statement
 When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
Ruth Melville - QLD ACORN Director & Chair Standards Committee NUM ORS Clinical Services NGH
 Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
If you experience any problems, please call Marilyn Nichols at the MOCPS office at , ext 221 or The Basics of CUSP
 Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Assessing Non-Technical Skills. A Guide to the NOTSS Tool Adapted for the Labour Ward
 Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Simulation. Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N.
 Simulation Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N. Contributors to Maternal M&M from Obstetrical Hemorrhage DELAY IN DIAGNOSIS DELAY IN BLOOD TRANSFUSION
Simulation Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N. Contributors to Maternal M&M from Obstetrical Hemorrhage DELAY IN DIAGNOSIS DELAY IN BLOOD TRANSFUSION
Title: Quality/Safety Education Physician Champion Phone:
 TeamSTEPPS 101: Know The Plan, Share The Plan Implementing A Customized Surgical Safety Checklist Team Communication Tool In Ambulatory And Inpatient Operating Rooms Organization Name: Christiana Care
TeamSTEPPS 101: Know The Plan, Share The Plan Implementing A Customized Surgical Safety Checklist Team Communication Tool In Ambulatory And Inpatient Operating Rooms Organization Name: Christiana Care
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
POLICY. The purpose of this policy is to establish Saskatoon Health Region s (SHR s) communication requirements for all surgical patients.
 communication requirements for all surgical patients.") POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
What does safe surgery look like? Jonathan Beard Professor of Surgical Education
 What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
Sentinel Events and S Patient Patient entinel Event Alerts Safety Act Safety Ac Revised: BW/September 2010
 Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
SCIP. Surgical Care Improvement Project. Making Surgeries Safer. By: Roshini Mathew, RN
 SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
Safe Surgery The Checklist Experience
 Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital
 Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Teamwork and Communication for Quality & Safety: It s More Than Checklists
 Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
These incidents, reported by the Pennsylvania Patient Safety Authority, are
 Patient safety Taking steps to protect patients from specimen-handling errors An OR specimen was transported to the laboratory. The lab called to say there was no specimen in the container. The specimen
Patient safety Taking steps to protect patients from specimen-handling errors An OR specimen was transported to the laboratory. The lab called to say there was no specimen in the container. The specimen
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Cognitive Aids to Improve Crisis Management
 Cognitive Aids to Improve Crisis Management Alexander A. Hannenberg, M.D. Council on Surgical & Perioperative Safety Emergency Manual Implementation Collaborative Past President American Society of Anesthesiologists
Cognitive Aids to Improve Crisis Management Alexander A. Hannenberg, M.D. Council on Surgical & Perioperative Safety Emergency Manual Implementation Collaborative Past President American Society of Anesthesiologists
QUESTIONS PERTINENT TO PRODUCT SELECTION:
 QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
Walk through a QAPI Project
 Walk through a QAPI Project Quality Assessment to Performance Improvement Sandra Jones, CASC, CHPRM, LHRM, CHCQM, FHFMA Sjones@aboutascs.com 1 Types of Quality Measures Outcomes Measures results of care
Walk through a QAPI Project Quality Assessment to Performance Improvement Sandra Jones, CASC, CHPRM, LHRM, CHCQM, FHFMA Sjones@aboutascs.com 1 Types of Quality Measures Outcomes Measures results of care
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
When words and actions matter most: The Case for CANDOR
 January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Running head: ROOT CAUSE ANALYSIS 1
 Running head: ROOT CAUSE ANALYSIS 1 Death by Running: Root Cause Analysis Kristen Carey Angelo State University ROOT CAUSE ANALYSIS 2 Long QT Syndrome Over a decade ago the Institute of Medicine estimated
Running head: ROOT CAUSE ANALYSIS 1 Death by Running: Root Cause Analysis Kristen Carey Angelo State University ROOT CAUSE ANALYSIS 2 Long QT Syndrome Over a decade ago the Institute of Medicine estimated
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Prevention of Retained Foreign Objects
 Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Waiting for a family member who is having surgery
 Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
High 5s Project: Action on Patient Safety. SOP Flow Charts. 20 th International Forum on Quality and Safety in Healthcare April 2015 London, UK
 High 5s Project: Action on Patient Safety SOP Flow Charts 20 th International Forum on Quality and Safety in Healthcare 21-24 April 2015 London, UK Performance of Correct Procedure at Correct Body Site
High 5s Project: Action on Patient Safety SOP Flow Charts 20 th International Forum on Quality and Safety in Healthcare 21-24 April 2015 London, UK Performance of Correct Procedure at Correct Body Site
2012 WEBINAR SERIES. ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT.
 2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
Surgical Technology Patient Care Skills Preop Routine Objectives:
 Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Bridging the communication gap in the operating room with medical team training
 The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Washington Patient Safety Coalition & Surgical Public Health:
 Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
ORIGINAL ARTICLE. Incorrect Surgical Procedures Within and Outside of the Operating Room
 ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
In 2002 Ascension Health, the largest Catholic and
 Clinical Excellence Series Eliminating Preventable Death at Ascension Health Sanford Tolchin, M.D. Robert Brush, M.D. Paul Lange, M.D. Phyllis Bates, R.N., M.S., C.P.H.Q. John J. Garbo, R.N., M.A. In 2002
Clinical Excellence Series Eliminating Preventable Death at Ascension Health Sanford Tolchin, M.D. Robert Brush, M.D. Paul Lange, M.D. Phyllis Bates, R.N., M.S., C.P.H.Q. John J. Garbo, R.N., M.A. In 2002
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
2011 The International Conference on Residency Education La Conference Internationale sur la Formation de Residents
 2011 The International Conference on Residency Education La Conference Internationale sur la Formation de Residents Royal College of Physicians and Surgeons of Canada College Royale de Medecins et Chrurgiens
2011 The International Conference on Residency Education La Conference Internationale sur la Formation de Residents Royal College of Physicians and Surgeons of Canada College Royale de Medecins et Chrurgiens
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm. Kendra Folh, BSN, RNC-OB
 How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
Reducing Medical Errors
 Reducing Medical Errors 1403 19 Team Training (Crew Resource Management) System Failures & Human Factors Excessive number of handoffs Long work hours Excessive workload Variable information availability
Reducing Medical Errors 1403 19 Team Training (Crew Resource Management) System Failures & Human Factors Excessive number of handoffs Long work hours Excessive workload Variable information availability
Patient Safety in Ambulatory Care: Why Reporting Counts. August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH
 Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents