Translating Evidence to Safer Care
|
|
|
- Jasper Brown
- 5 years ago
- Views:
Transcription

1 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health Professor of Medicine, School of Medicine, Johns Hopkins University Your picture is also welcome
2 Overview To provide understand and provide strategies on how research findings can be translated into practice.

3 Components
4 1. In the IHI model for Improvement, what does PDSA stand for? a. Process, Delivery, Study, Activation b. Plan, Do, Study, Act c. Position, Deploy, Steady, Aim d. Patient, Doctor, Student, Administrator 2. In forming a quality improvement team, which of the following members does NOT necessarily need to be represented a. Leaders of the health care organization b. Physicians c. Technical expertise with the clinical problem d. Day-to-day leadership of units
5 3. After summarizing the evidence for effective interventions, what steps are need to translate evidence to safer care? a. Identify local barriers to implementing the intervention b. Measure performance c. Ensure all patients get the intervention d. All of the above 4. What is true about identifying local barriers to implementing interventions? a. Intervention is part of a work process b. It can be helpful to walk-through the steps to implement the intervention c. Compliance can be improved by targeting failure points in implementation d. All of the above 5. The 4 Es of implementing an intervention include a. Educate, Estimate, Eradicate, Evaluate b. Estimate, Educate, Execute, Eradicate c. Engage, Educate, Execute, Evaluate d. None of the above
6 Introduction Despite good evidence, difficult to get into practice changes that improve safety Knowledge translation needs to occur within systems of care
7 Integrated Approach to Translating Evidence to Practice A focus on systems (how we organise work) rather than care of individual patients Engagement of local interdisciplinary teams to assume ownership of the improvement project Creation of centralised support for the technical work Encouraging local adaptation of the intervention Creating a collaborative culture within the local unit and larger system.
 Model for")
8 Institute for Healthcare Improvement (IHI) Model for Improvement
9 Forming the Team Effective teams include members representing three different kinds of expertise within the organization system leadership technical expertise day-to-day leadership There may be one or more individuals on the team with each kind of expertise, or one individual may have expertise in more than one area, but all three areas should be represented in order to drive improvement successfully
10 Team Aim: Reduce adverse drug events (ADEs) on all medical and surgical units by 75 percent within 11 months. Team: Team Leader:, MD, Chair, Pharmacy and Therapeutics Committee, Patient Safety Officer Technical Expertise:, RPh, Director, Clinical Pharmacist Day-to-Day Leadership:, RN, Manager, Medical/Surgical Nursing Additional Team Members: Risk Manager, Quality Improvement Specialist, Staff Nurse, Staff Education, and Information Technology
11 Setting Aims Reduce adverse drug events (ADEs) in critical care by 75 percent within 1 year. Improve medication reconciliation at transition points by 75 percent within 1 year. Achieve > 95 percent compliance with on-time prophylactic antibiotic administration within 1 year.

12 Strategy for Translating Evidence to Practice Pronovost, BMJ 2008
13 Summarize the Evidence For interventions to improve a specific outcome Interdisciplinary team of researchers and clinicians reviews literature using to identify interventions with greatest benefit lowest barriers to use Agree on the top interventions (maximum of seven) and convert them into behaviors
14 Identify Local Barriers to Implementation The intervention will be part of a work process What is the context surrounding this work? Walk through steps with clinician to observe what is required to implement intervention Where are the failure points? What could be done to improve compliance?
15 Understanding Context To help understand the context in which the intervention will be implemented, ask all stakeholders why it is difficult or easy for them to comply with recommended practices Listen carefully and learn what staff may gain or lose from implementing the intervention
16 Measure Performance Need performance measures to evaluate How often patients actually receive the recommended therapy (process measures) Whether patient outcomes improve (outcome measures) Outcome measures are preferred if valid and feasible
17 Measures Teams use quantitative measures to determine if a specific change actually leads to an improvement. Many sequential, observable tests Gather "just enough" data to learn and complete another cycle "Small tests of significant changes" accelerates the rate of improvement
18 Ensure All Patients Receive the Intervention Final and most complex stage is to ensure that all patients reliably receive the intervention Interventions must fit each hospital s current system, including local culture and resources 4 Es Engage Educate Execute Evaluate
19 Engage Share real life stories of patients Estimate the harm attributable to omitting the intervention in their unit or hospital given their baseline data Informed each unit of its annual number of infections and patient deaths attributed to the infections
20 Educate All levels of staff Original scientific literature supporting the proposed interventions Concise summaries Checklist of the evidence
21 Execute Designed an implementation "toolkit" based on identified barriers to implementation Based on 3 principles for redesigning care standardize care processes create independent checks (such as checklists) learn from mistakes


22 Pronovost P, et. al. An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. The New England Journal of Medicine, 2006, 355: Link to Abstract (HTML) Link to Full Text (PDF)
23 Translating Evidence to Practice Summarize the evidence Identify local barriers to implementing the intervention Measure performance Ensure all patients get the intervention
24 Summarize the Evidence for Preventing Central Line Infection: 5 Best Practices Remove Unnecessary Lines Hand Hygiene Use of Maximal Barrier Precautions Chlorhexidine for Skin Antisepsis Avoid femoral lines MMWR. 2002;51:RR-10
25 Central Line Cart Observed insertion of central lines Clinicians gathered equipment essential for complying with recommended practice (sterile gloves, full sterile drape, etc) from up to eight different locations! To make compliance easier for clinicians introduced a central line cart storing all the necessary supplies.
26 Identify and Address Local Barriers Nurses reluctant to question or challenge doctors who failed to follow recommended practice Physicians did not like being questioned by nurses in front of patients or other staff Clinicians agreed with the recommended practices, but cultural barriers prevented reliable delivery To address barriers, implemented a comprehensive safety programme that includes methods to improve culture, teamwork, and communication
27 Comprehensive Unit Based Safety Program (CUSP) 1. Safety Culture Assessment 2. Science of Safety Training 3. Staff Identify Safety Hazards 4. Senior Executive Partnership 5. Learn from Safety Defects/Apply Tools to Improve 6. Reassess Safety Culture
28 ICUs also implemented A daily goals sheet to improve clinician-to-clinician communication within the ICU An intervention to reduce the incidence of ventilator-associated pneumonia A comprehensive unit-based safety program to improve the safety culture
29 Measures Performance Chose infection rates (an outcome measure) because Centers for Disease Control provides standardised, scientifically rigorous definitions Hospitals already collect data on infections Could not develop a valid and feasible measure of compliance with evidence based practices for central line insertion because lines are placed randomly Coordination of independent observation difficult Self reported compliance likely to overestimate performance
30 4 E s Engage Educate Execute Evaluate
31 Execute: Converted 5 evidence based behaviors to a Checklist Before the procedure, did they: Wash hands Sterilize procedure site with chlorhexadine Drape entire patient in a sterile fashion During the procedure, did they: Use sterile gloves, mask and sterile gown Maintain a sterile field Did all personnel assisting with procedure follow the above precautions
32 Evaluate: ICU catheter-related blood stream infections Education Line Cart Checklist NNIS Mean Rate/1,000 Catheter days Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar April May June July August
33 Evaluate and Feedback
34 Your To Do List Establish team; include executive Pick area and outcome Measure performance Implement intervention Protocol, independent check, failure modes Document improvements

35 The 2 nd Global Patient Safety Challenge 234 M surgeries globally Death % Complications 3-16% 1 million deaths 7 million disabling complications
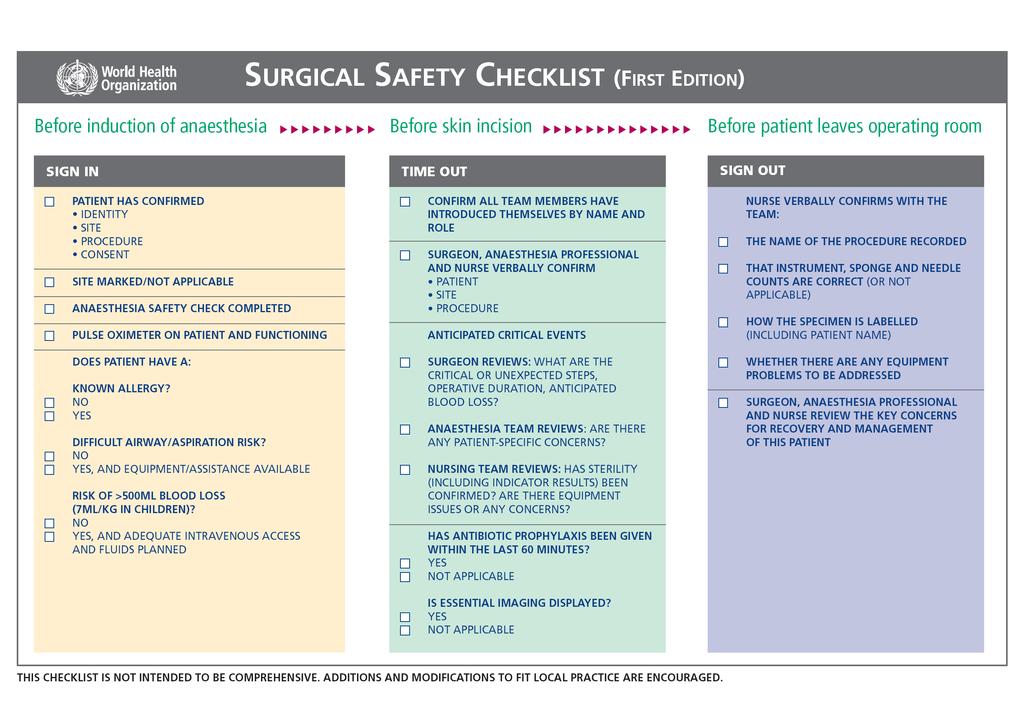
36 Ten Objectives of Safe Surgery Saves Lives 1. Correct patient / correct site 2. Prevent harm from anaesthetics 3. Prepare for airway emergencies 4. Prepare for high blood loss 5. Avoid allergies 6. Minimize surgical site infections 7. Prevent retention of instruments/ sponges 8. Accurately secure and identify specimens 9. Effectively communicate critical information 10. Establish surveillance of capacity/ volume/ results
37
38 Concluding remarks Understanding context, evidence, culture change, rigorous measurement, evaluation and feedback needed Sustainability also important
39 References Grol R, Crimshaw J. From best evidence to best practice: effective implementation of change in patients care. Lancet 2003;362: Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, Herbosa T, Joseph S, Kibatala PL, Lapitan MC, Merry AF, Moorthy K, Reznick RK, Taylor B, Gawande AA; Safe Surgery Saves Lives Study Group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med Jan 29;360(5): Pittet D, Allegranzi B, Boyce J; World Health Organization World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts. The World Health Organization Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infect Control Hosp Epidemiol Jul;30(7): Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. BMJ Oct 6;337:a1714. How to Improve: Improvement Methods. Institute for Healthcare Improvement.
40 1. In the IHI model for Improvement, what does PDSA stand for? a. Process, Delivery, Study, Activation b. Plan, Do, Study, Act c. Position, Deploy, Steady, Aim d. Patient, Doctor, Student, Administrator 2. In forming a quality improvement team, which of the following members does NOT necessarily need to be represented a. Leaders of the health care organization b. Physicians c. Technical expertise with the clinical problem d. Day-to-day leadership of units
41 3. After summarizing the evidence for effective interventions, what steps are need to translate evidence to safer care? a. Identify local barriers to implementing the intervention b. Measure performance c. Ensure all patients get the intervention d. All of the above 4. What is true about identifying local barriers to implementing interventions? a. Intervention is part of a work process b. It can be helpful to walk-through the steps to implement the intervention c. Compliance can be improved by targeting failure points in implementation d. All of the above The 4 Es of implementing an intervention include a. Educate, Estimate, Eradicate, Evaluate b. Estimate, Educate, Execute, Eradicate c. Engage, Educate, Execute, Evaluate d. None of the above
42 Interactive Participants identify local barriers to implementation of safe surgery guidelines
43 Questions?
44
Stasis and VTE Is lack of order putting patients at risk?
 Stasis and VTE Is lack of order putting patients at risk? Professor Cliff Hughes AO 29March 2012 Safe Driving - NSW (435) 376 CF Hughes 29 th March 2012 NSW Heavy Vehicle Statistics 2011 General fatalities
Stasis and VTE Is lack of order putting patients at risk? Professor Cliff Hughes AO 29March 2012 Safe Driving - NSW (435) 376 CF Hughes 29 th March 2012 NSW Heavy Vehicle Statistics 2011 General fatalities
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs
 Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Infection Control in Hospital Accreditation. Paul Ananth Tambyah
 Infection Control in Hospital Accreditation Paul Ananth Tambyah Are Hospitals Dangerous??? Hospitals were originally set up for the sick and dying among the poor The wealthy had physicians go to their
Infection Control in Hospital Accreditation Paul Ananth Tambyah Are Hospitals Dangerous??? Hospitals were originally set up for the sick and dying among the poor The wealthy had physicians go to their
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU. Dr David Ng Paediatric Medical Officer Sarawak General Hospital
 Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Identifying Solutions / Implementation
 Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Infection Prevention & Control Prof. Benedetta Allegranzi & the IPC Global Unit team SDS/HIS, WHO HQ
 Infection Prevention & Control Prof. Benedetta Allegranzi & the IPC Global Unit team SDS/HIS, WHO HQ 20 ottobre 2017, II convention nazionale dei clinical risk managers Outline The burden of health care-associated
Infection Prevention & Control Prof. Benedetta Allegranzi & the IPC Global Unit team SDS/HIS, WHO HQ 20 ottobre 2017, II convention nazionale dei clinical risk managers Outline The burden of health care-associated
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Implementation Guide for Central Line Associated Blood Stream Infection
 Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
Central Vascular Catheter Insertion Checklist Standard Operating Procedure. Perform optimal care
 Central Vascular Catheter Insertion Checklist Standard Operating Procedure Perform optimal care Improving process to improve outcome This checklist is adapted with kind permission from the checklist devised
Central Vascular Catheter Insertion Checklist Standard Operating Procedure Perform optimal care Improving process to improve outcome This checklist is adapted with kind permission from the checklist devised
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
A3/B3: Improvement in the Intensive Care Unit
 A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Ensuring quality outcomes
 Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Central Line Bundle Education. National Patient Safety Goal Preventing Central Line Infections 2010
 Central Line Bundle Education National Patient Safety Goal 07.04.01 Preventing Central Line Infections 2010 Central Line Associated Bloodstream Infections CAN and DO kill our patients. THE GOOD NEWS They
Central Line Bundle Education National Patient Safety Goal 07.04.01 Preventing Central Line Infections 2010 Central Line Associated Bloodstream Infections CAN and DO kill our patients. THE GOOD NEWS They
Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene 3. Isolation Precau
 Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
Erlanger Infection Prevention Resident and df Fellow Orientation June 2011 1 Outline 1. Infection Prevention Program Bloodborne Pathogens/Exposure Prevention & Management Standard Precautions 2. Hand Hygiene
Conflict of Interest Disclaimer. The Affordable Care Act. The Affordable Care Act. Caring for the Critically Ill. The Affordable Care Act
 Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Cognitive Aids to Improve Crisis Management
 Cognitive Aids to Improve Crisis Management Alexander A. Hannenberg, M.D. Council on Surgical & Perioperative Safety Emergency Manual Implementation Collaborative Past President American Society of Anesthesiologists
Cognitive Aids to Improve Crisis Management Alexander A. Hannenberg, M.D. Council on Surgical & Perioperative Safety Emergency Manual Implementation Collaborative Past President American Society of Anesthesiologists
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES
 WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Ensuring Patient Safety and Quality Measures for RRT in AKI 2. Eileen Lischer MA, BSN, RN, CNN University of California, San Diego
 Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN
 Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
In 2002 Ascension Health, the largest Catholic and
 Clinical Excellence Series Eliminating Preventable Death at Ascension Health Sanford Tolchin, M.D. Robert Brush, M.D. Paul Lange, M.D. Phyllis Bates, R.N., M.S., C.P.H.Q. John J. Garbo, R.N., M.A. In 2002
Clinical Excellence Series Eliminating Preventable Death at Ascension Health Sanford Tolchin, M.D. Robert Brush, M.D. Paul Lange, M.D. Phyllis Bates, R.N., M.S., C.P.H.Q. John J. Garbo, R.N., M.A. In 2002
Preventing Health Care Associated Infections. PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011.
 Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Title: Learning from Defects Learning from and Preventing adverse events
 Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Joint Commission NPSG 7: 2011 Update and 2012 Preview
 Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
To Dip or Not To Dip
 To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
Implementation Model. Levels of Evidence 3/9/2011. Strategies to get Evidence into Practice EXTRACTING. Elizabeth Bridges PhD RN CCNS, FCCM, FAAN
 Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU. A thesis presented by. Shelby L. Holden
 Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital.
 An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
A Practical Tool to Learn From Defects in Patient Care
 Tool Tutorial A Practical Tool to Learn From Defects in Patient Care Peter J. Pronovost, M.D., Ph.D. Christine G. Holzmueller Elizabeth Martinez, M.D., M.H.S. Christina L. Cafeo, R.N., M.S.N. David Hunt,
Tool Tutorial A Practical Tool to Learn From Defects in Patient Care Peter J. Pronovost, M.D., Ph.D. Christine G. Holzmueller Elizabeth Martinez, M.D., M.H.S. Christina L. Cafeo, R.N., M.S.N. David Hunt,
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
ORIGINAL ARTICLE. Surgical Safety Practices in Pakistan
 76 Surgical Safety Practices in Pakistan Asad Ali Toor, 1 Seema Nigh-e-Mumtaz, 2 Rasheedullah Syed, 3 Mahmood Yousuf, 4 Ameena Syeda 5 ORIGINAL ARTICLE Abstract Objectives: To evaluate the current practices
76 Surgical Safety Practices in Pakistan Asad Ali Toor, 1 Seema Nigh-e-Mumtaz, 2 Rasheedullah Syed, 3 Mahmood Yousuf, 4 Ameena Syeda 5 ORIGINAL ARTICLE Abstract Objectives: To evaluate the current practices
2017 Nicolas E. Davies Enterprise Award of Excellence
 2017 Nicolas E. Davies Enterprise Award of Excellence Agenda Memorial Hermann Health System Overview Journey to High Reliability Case study review CLABSI Prevention 2 Memorial Hermann Health System Woodlands
2017 Nicolas E. Davies Enterprise Award of Excellence Agenda Memorial Hermann Health System Overview Journey to High Reliability Case study review CLABSI Prevention 2 Memorial Hermann Health System Woodlands
Ambitious Goals to Reduce Harm: Why Has Progress Been Slow and What Can We Do to Bend the Curve?
 Ambitious Goals to Reduce Harm: Why Has Progress Been Slow and What Can We Do to Bend the Curve? Don Goldmann, M.D. Senior Vice President Institute for Healthcare Improvement Professor of Pediatrics Harvard
Ambitious Goals to Reduce Harm: Why Has Progress Been Slow and What Can We Do to Bend the Curve? Don Goldmann, M.D. Senior Vice President Institute for Healthcare Improvement Professor of Pediatrics Harvard
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
EMR Adoption: Benefits Realization
 EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Prairie North Regional Health Authority: Hospital-acquired infections
 Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Reducing Ventilator Associated Pneumonia (V.A.P) System and Patient Tracer
 System and Patient Tracer") Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
MRSA: National developments, Progress, Challenges and Targets
 MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Multi disciplinary Team Communication and Effective Handoffs
 Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Medication Reconciliation Bundle of Care. Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013
 Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Key prevention strategies for MRSA bacteraemia: a case study. Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta
 Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
The PIIQI Versus Research Debate
 MILITARY MEDICINE, 175,4:289,2010 Performance Improvement/Research Advisory Panel: A Model for Determining Whether a Project Is a Performance or Quality Improvement Activity or Research Lynn S. Platteborze,
MILITARY MEDICINE, 175,4:289,2010 Performance Improvement/Research Advisory Panel: A Model for Determining Whether a Project Is a Performance or Quality Improvement Activity or Research Lynn S. Platteborze,
Northern Health - Acute Services. Evidence Based Practice Venous Thromboembolism Prevention
 Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Establishing a Culture of Quality and Safety and the Journey to High Reliability
 Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Hospital-Acquired Infections Prevention is in Your Hands. Rachel L. Stricof
 Hospital-Acquired Infections Prevention is in Your Hands Rachel L. Stricof rstricof@gmail.com Morbidity 1.7 Million infections per year (estimate 2002) Mortality 99,000 deaths per year (estimate 2002)
Hospital-Acquired Infections Prevention is in Your Hands Rachel L. Stricof rstricof@gmail.com Morbidity 1.7 Million infections per year (estimate 2002) Mortality 99,000 deaths per year (estimate 2002)
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
By Marcus E. Semel, Stephen Resch, Alex B. Haynes, Luke M. Funk, Angela Bader, William R. Berry, Thomas G. Weiser, and Atul A.
 By Marcus E. Semel, Stephen Resch, Alex B. Haynes, Luke M. Funk, Angela Bader, William R. Berry, Thomas G. Weiser, and Atul A. Gawande Adopting A Surgical Safety Checklist Could Save Money And Improve
By Marcus E. Semel, Stephen Resch, Alex B. Haynes, Luke M. Funk, Angela Bader, William R. Berry, Thomas G. Weiser, and Atul A. Gawande Adopting A Surgical Safety Checklist Could Save Money And Improve
New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration
: Improving Perinatal Health through Partnerships and Collaboration") New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration Marilyn Kacica, MD, MPH Kristen Farina, MS New York State Department of Health
New York State Perinatal Quality Collaborative (NYSPQC): Improving Perinatal Health through Partnerships and Collaboration Marilyn Kacica, MD, MPH Kristen Farina, MS New York State Department of Health
SBAR: Use of gloves for environmental cleaning
 SBAR: Use of gloves for environmental cleaning Situation The National Infection Prevention and Control Manual for NHSScotland Chapter 1: Standard Infection Control Precautions (SICPs) Policy 1 was published
SBAR: Use of gloves for environmental cleaning Situation The National Infection Prevention and Control Manual for NHSScotland Chapter 1: Standard Infection Control Precautions (SICPs) Policy 1 was published
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success
 Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Enhancing Patient Safety through Team Work and Communication Strategies
 Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Hand Hygiene Toolkit
 Hand Hygiene Toolkit 1. Why ACT NOW to improve hand hygiene? 2. How can you improve hand hygiene (HH) compliance? 3. Unit/service leader checklist 1. The Hand Hygiene Data Reporting Tool : Bring relevant
Hand Hygiene Toolkit 1. Why ACT NOW to improve hand hygiene? 2. How can you improve hand hygiene (HH) compliance? 3. Unit/service leader checklist 1. The Hand Hygiene Data Reporting Tool : Bring relevant
30% 20% 10% -10% -20% -30% -40% 3 Haley Am J Epidemiol 1985
 Outline "INNOVATION AND IMPLEMENTATION STRATEGIC APPROACHES TO REDUCE CATHETER-RELATED BACTERAEMIA: THE RESULTS OF A EUROPEAN MULTICENTRE STUDY (PROHBIT)" Dr. Walter Zingg University of Geneva Hospitals
Outline "INNOVATION AND IMPLEMENTATION STRATEGIC APPROACHES TO REDUCE CATHETER-RELATED BACTERAEMIA: THE RESULTS OF A EUROPEAN MULTICENTRE STUDY (PROHBIT)" Dr. Walter Zingg University of Geneva Hospitals
QUALITY ACCOUNTS 2013/2014
 QUALITY ACCOUNTS 2013/2014 Northland District Health Board Quality Accounts 2013/2014 Quality is important to us all and we are making steady progress against each of our nominated priorities. We have
QUALITY ACCOUNTS 2013/2014 Northland District Health Board Quality Accounts 2013/2014 Quality is important to us all and we are making steady progress against each of our nominated priorities. We have
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Disposable, Non-Sterile Gloves for Minor Surgical Procedures: A Review of Clinical Evidence
 CADTH RAPID RESPONSE REPORT: SUMMARY WITH CRITICAL APPRAISAL Disposable, Non-Sterile Gloves for Minor Surgical Procedures: A Review of Clinical Evidence Service Line: Rapid Response Service Version: 1.0
CADTH RAPID RESPONSE REPORT: SUMMARY WITH CRITICAL APPRAISAL Disposable, Non-Sterile Gloves for Minor Surgical Procedures: A Review of Clinical Evidence Service Line: Rapid Response Service Version: 1.0
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Central Line Associated Bloodstream Infections: Is achieving zero possible?
 Mary-Louise McLaws Professor of Epidemiology Healthcare Associated Infection and Infectious Diseases Control Epidemiology Advisor to Clinical Excellence Commission School of Public Health and Community
Mary-Louise McLaws Professor of Epidemiology Healthcare Associated Infection and Infectious Diseases Control Epidemiology Advisor to Clinical Excellence Commission School of Public Health and Community
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Bundle Me Up! Using Central Line Bundles to Decrease Infection
 Bundle Me Up! Using Central Line Bundles to Decrease Infection Organization Name: Peninsula Regional : Acute Care Hospital Medical Center Contact Person: Regina Kundell Title: Dir, Women s and Children
Bundle Me Up! Using Central Line Bundles to Decrease Infection Organization Name: Peninsula Regional : Acute Care Hospital Medical Center Contact Person: Regina Kundell Title: Dir, Women s and Children
Prevention of Hospital Infection by Intervention and Training (PROHIBIT) Dr Walter Zingg
 Dr Walter Zingg") Prevention of Hospital Infection by Intervention and Training (PROHIBIT) Dr Walter Zingg 1. Objectives The aim of the Prevention of hospital infection by intervention and training (PROHIBIT) project was
Prevention of Hospital Infection by Intervention and Training (PROHIBIT) Dr Walter Zingg 1. Objectives The aim of the Prevention of hospital infection by intervention and training (PROHIBIT) project was
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
Safe Surgery Checklist to Brief and De brief
 afe urgery Checklist to Brief and De brief Limerick 29 th March 2014 James Clarke Consultant Anaesthetist London World Health Organisation 1 The question Why go to a 5 step process? when some of us we
afe urgery Checklist to Brief and De brief Limerick 29 th March 2014 James Clarke Consultant Anaesthetist London World Health Organisation 1 The question Why go to a 5 step process? when some of us we
NHSN: Information for Action
 NHSN: Information for Action Reducing Healthcare Associated Infections: Tennessee Marion A. Kainer MD, MPH Director, Hospital Infections Program Tennessee Department of Health marion.kainer@tn.gov 1 Outline
NHSN: Information for Action Reducing Healthcare Associated Infections: Tennessee Marion A. Kainer MD, MPH Director, Hospital Infections Program Tennessee Department of Health marion.kainer@tn.gov 1 Outline
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory