Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
|
|
|
- Clementine Woods
- 5 years ago
- Views:
Transcription
1 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for Geriatric Education University of Miami Miller School of Medicine (UMMSM) at Florida Atlantic University Alice Bonner, PhD, RN Executive Director Massachusetts Senior Care Foundation Assistant Professor University of Massachusetts Graduate School of Nursing Worcester, MA
2 Background Hospitalizations of NH residents are common, frequently result in morbid complications, and are expensive in terms of: DRG payments to hospitals Costs of complications Medicare Part A Skilled Nursing Facility stays Previous research suggests many such hospitalizations are inappropriate and/or related to ambulatory care sensitive diagnoses
3 Background 45% of admissions of 100 residents from 7 Los Angeles nursing homes to acute hospitals were rated as inappropriate Saliba et al, J Amer Geriatr Soc 48: , 2000 Medicare spent close to $200 million on hospitalizations related to Ambulatory Care Sensitive Diagnoses among longstay NH residents in New York state in 2004 This figure does not include residents on the Part A skilled benefit, who get hospitalized frequently Grabowski et al, Health Affairs 26: , 2007
4 The Opportunity Reducing potentially avoidable hospitalizations of NH residents represents an opportunity to both: Improve quality of care; and Reduce overall Medicare expenditures on this population
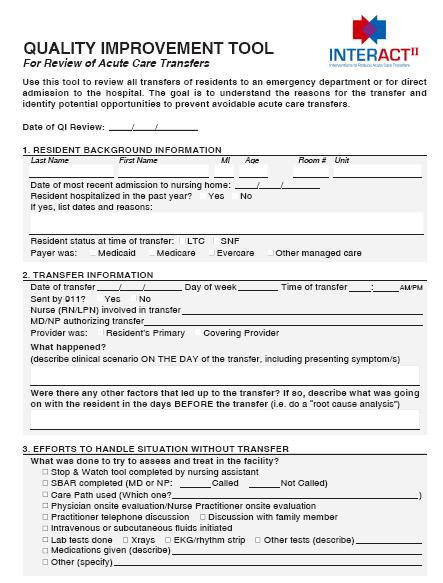
5 CMS Special Study Awarded to Georgia Medical Care Foundation Objectives July 2006 January Identify NHs in Georgia with high and low hospitalization rates 2. Compare characteristics of these homes and their residents 3. Conduct interviews with NH and hospital staff 4. Rate potential avoidability of 200 hospitalizations 5. Develop intervention strategies and tools 6. Conduct a pilot test in 2-4 NHs with high hospitalization rates 7. Disseminate results and intervention strategies
6 CMS NH Special Study Conclusions (1) 1. Rates of hospitalization of NH residents in Georgia varied considerably, and were related to several characteristics of the NHs and residents 2. 2/3 of 200 hospitalizations were rated as potentially avoidable by experts in NH care 3. Implementation of a toolkit addressing conditions commonly causing hospitalization, communication, and advance care planning was associated with: a. A 50% reduction of hospitalization in 3 NHs with high baseline rates b. A 36% reduction in hospitalizations rated as potentially avoidable
7 CMS NH Special Study Conclusions (2) 1. Reducing potentially avoidable hospitalizations by 1/3 could save Medicare over $1 billion annually 2. In order to safely reduce hospitalizations, NHs will need: a. Support for infrastructure: more trained RNs, on-site availability of primary care providers, better capabilities for lab tests and administration of IV or subcutaneous fluids b. Improved communication and adherence to evidence or consensus-based care paths c. More attention to advance care planning and avoidance of futile care
8 Next Steps (1) 1. Evaluate the new INTERACT II tools and implementation strategies in a collaborative quality improvement project in 30 NHs in 3 states (FL, NY, MA) 1. Explore the incorporation of elements of the INTERACT II toolkit into Health Information Technology 1. Estimate the costs to NHs of using the tools Supported by a grant from the Commonwealth Fund MA Nursing Homes selected Implementation 5/2009-1/2010
9 Next Steps (2) 1. Further disseminate the INTERACT II tools via the Advancing Excellence Campaign, Emergency Nurse s Association, AHCA and other organizations Supported by a grant from the Commonwealth Fund 18 Month Study beginning 5/2009

10 A Toolkit to Improve Nursing Home Care by Reducing Avoidable Acute Care Transfers and Hospitalizations Developed based on interviews and ratings of avoidability, and Expert Panel ratings of importance and feasibility Clinical Care Paths Communication Tools Advance Care Planning Tools
11 Interventions to Reduce Acute Care Transfers (INTERACT II) Institute of Medicine/CMS STEEEP Goals for Quality Care (Safe, Timely, Effective, Efficient, Equitable, Person-Centered) INTERACT II Tools Healthcare Organizational Characteristics and Infrastructure Reduced Avoidable Acute Care Transfers Morbidity Costs Infrastructure Support and Incentives Healthcare Organizational Culture Quality
12 Development of INTERACT Tools Evidence or consensus-based (and/or consistent with CPGs) Simple Feasible and efficient to use Acceptable to NH staff
13 Current Versions of the Tools are available on the Quality Net website at: Revised tools soon to be available on
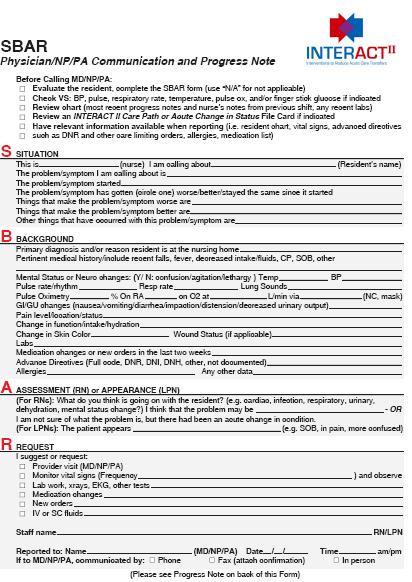
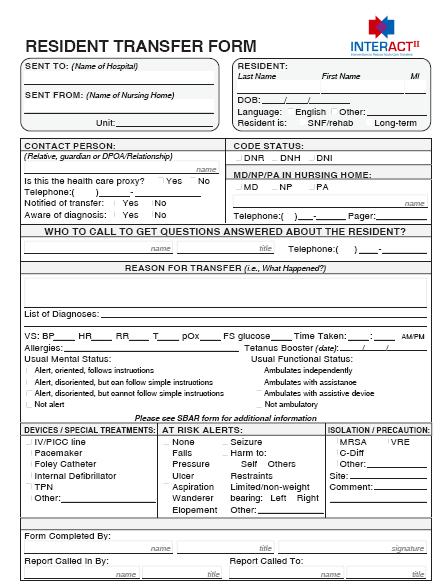
14 Early Warning Tool Stop and Watch SBAR Communication (Nurse to Physician and/or ER) Acute Change in Condition Guidance for Communication Resident Transfer Form Nursing Home Capabilities Acute Care Transfer Documents Communication Tools Pocket Cards and Report Forms Form and Progress Note File Cards Form completed on transfer Pre- populated Checklist Envelope with Checklist
15
16
17
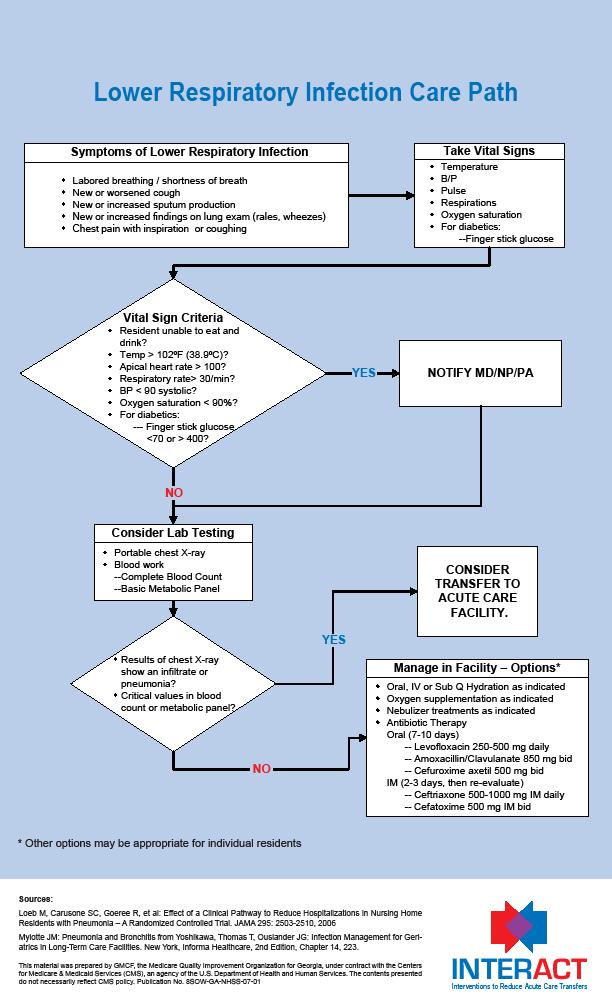
18 Care Paths Fever Acute mental status change Symptoms of Lower Respiratory Illness Symptoms of CHF Symptoms of UTI Dehydration Posters
19

20 Advance Care Planning Tools Identifying Residents to Consider for Palliative Care and Hospice Pocket Card Advance Care Planning Communication Guide Comfort Care Order Set Educational Information for Families File Cards File Cards Reprints
21
22 It s not about the tools It s about the process It s about the conversations and the relationships among providers and institutions
23 Commonwealth Fund Grant Principal Investigator: Co-Principal Investigator: Joseph G. Ouslander, M.D. Gerri Lamb, PhD, RN Independence Foundation and Wesley Woods Chair Associate Professor of Nursing, Emory University Collaborators: Laurie Herndon, MSN, GNP/ANP Senior Project Manager Alice Bonner, PhD, RN Co-Investigator Massachusetts Senior Care Foundation Multidisciplinary teams from FL, NY, and MA Support: ~ $390,000 over 2 years
24 Commonwealth Fund Grant Methods 1. Obtain input from national thought leaders in innovative models of long-term and transitional care and NH health care professionals from a nationally representative sample of NHs on the design, content, and implementation strategies for the toolkit 1. Refine the toolkit based on this input 1. Implement and evaluate the refined toolkit in a representative sample of NHs using a quality improvement project incorporating principles of an Institute for Healthcare Improvement (IHI) Collaborative 30 NHs will be involved: 10 in FL, 10 in NY, and 10 in MA
25 Methods 1. Collect data during the Collaborative that will be used to: Understand factors and strategies that are important for successful implementation and sustained use of the toolkit Estimate the costs of implementing the toolkit to inform P4P initiatives 2. Explore incorporating key elements of the toolkit into health information technology (HIT) using web-based formats and/ or an electronic health record
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
An Innovative Approach to Identifying and Communicating Change of Condition
 An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum
 Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum Mary Jane Koren, M.D., M.P.H. Vice President, Delivery System Reform The Commonwealth Fund Grantmakers in Aging Annual Conference
Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum Mary Jane Koren, M.D., M.P.H. Vice President, Delivery System Reform The Commonwealth Fund Grantmakers in Aging Annual Conference
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
INTERACT INSIGHTS. Greater New York Hospital Association Continuing Care Leadership Coalition
 INTERACT INSIGHTS A GUIDE OF INSIGHTS AND LESSONS LEARNED FOLLOWING EXPERIENCES WITH THE INTERVENTIONS TO REDUCE PREVENTABLE ACUTE CARE TRANSFERS IN NEW YORK (INTERACT NY) PROGRAM. Greater New York Hospital
INTERACT INSIGHTS A GUIDE OF INSIGHTS AND LESSONS LEARNED FOLLOWING EXPERIENCES WITH THE INTERVENTIONS TO REDUCE PREVENTABLE ACUTE CARE TRANSFERS IN NEW YORK (INTERACT NY) PROGRAM. Greater New York Hospital
Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers
 Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers Edith G Walsh, PhD Joshua Wiener, PhD Marc Freiman, PhD Susan Haber, PhD Arnold
Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers Edith G Walsh, PhD Joshua Wiener, PhD Marc Freiman, PhD Susan Haber, PhD Arnold
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative
 Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
NDNQI Rhythms in Quality 2010 Data Use Conference
 NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
Overview of Presentation
 End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings
 Early Findings") Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings Researchers: Martin, Thomas R. PhD, Assistant Professor St. Joseph s University Department of Health Services;
Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings Researchers: Martin, Thomas R. PhD, Assistant Professor St. Joseph s University Department of Health Services;
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Health Literacy & Palliative Care: Nurse Training
 Health Literacy & Palliative Care: Nurse Training Elaine Wittenberg, PhD Associate Professor, Nursing Research & Education City of Hope Presented at: Institute of Medicine Roundtable on Health Literacy
Health Literacy & Palliative Care: Nurse Training Elaine Wittenberg, PhD Associate Professor, Nursing Research & Education City of Hope Presented at: Institute of Medicine Roundtable on Health Literacy
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Engaging Residents and Families in HAIs/CAUTI Prevention. Presenters
 AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Better Ending. A Guide. for a A SSURE Y OUR F INAL W ISHES. Conversations Before the Crisis
 A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
Defining and Driving Value: Provider and Payer Perspectives
 Defining and Driving Value: Provider and Payer Perspectives NAHC Financial Managers Meeting June 2013 Serving the Midcoast of Maine in Knox Waldo Lincoln Counties 1 Who we are... Medicare Certified & State
Defining and Driving Value: Provider and Payer Perspectives NAHC Financial Managers Meeting June 2013 Serving the Midcoast of Maine in Knox Waldo Lincoln Counties 1 Who we are... Medicare Certified & State
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
ED Care Triage: Linkage to Primary Care
 ED Care Triage: Linkage to Primary Care BEST PRACTICES SUMMARY Updated 4/17/2017 ONECITY HEALTH SERVICES 199 Water Street, 31st Floor, New York, NY 10038 EXECUTIVE SUMMARY The goal of the ED Care Triage
ED Care Triage: Linkage to Primary Care BEST PRACTICES SUMMARY Updated 4/17/2017 ONECITY HEALTH SERVICES 199 Water Street, 31st Floor, New York, NY 10038 EXECUTIVE SUMMARY The goal of the ED Care Triage
2014 MASTER PROJECT LIST
 Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Quality Circles. Nursing as a Revenue Center NDNQI
 IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Hospital Funding Policy in Canada
 An Update Dublin, Ireland January 26 th 2011 Jason Sutherland, PhD Assistant t Professor Responsibility for health care funding, delivery and policy is a provincial issue Re-distribution ib ti of income
An Update Dublin, Ireland January 26 th 2011 Jason Sutherland, PhD Assistant t Professor Responsibility for health care funding, delivery and policy is a provincial issue Re-distribution ib ti of income
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care
 Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Heart Failure Nurse Practitioner Role Development and Proposal. Anita M. Wilson, BSN, RN. ACNP, DNP Student Creighton University
 1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 The Afterlife: Mortality in the Post Apocalyptic World of ICD 10 Debbie Malick, RN, BSN, MBA, CNML Clinical Nurse Specialist Cone Health at Alamance Regional Medical Center Burlington, NC 1 Background
The Afterlife: Mortality in the Post Apocalyptic World of ICD 10 Debbie Malick, RN, BSN, MBA, CNML Clinical Nurse Specialist Cone Health at Alamance Regional Medical Center Burlington, NC 1 Background
The long and winding road to Accountable Care
 The long and winding road to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute John E. Wennberg Distinguished Professor Geisel School of Medicine The long and winding road Past
The long and winding road to Accountable Care Elliott Fisher, MD, MPH Director, The Dartmouth Institute John E. Wennberg Distinguished Professor Geisel School of Medicine The long and winding road Past
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Infection Prevention and Control Training
 National Center for Emerging and Zoonotic Infectious Diseases Infection Prevention and Control Training Abimbola (Bola) Ogundimu, DrPH, RN, CIC Infection Preventionist for LTC CDC Division of Healthcare
National Center for Emerging and Zoonotic Infectious Diseases Infection Prevention and Control Training Abimbola (Bola) Ogundimu, DrPH, RN, CIC Infection Preventionist for LTC CDC Division of Healthcare
Clinical Nurse Specialist (CNS)
") Clinical Nurse Specialist (CNS) Paula Halcomb, MSN, DNP, APRN, ACNS-BC paula.halcomb@uky.edu Jill Dobias, MSN, APRN, ACCNS-AG, OCN, AOCNS jill.dobias@uky.edu Dee Sawyer, MS, APRN, MLDE, AGCNS-BC, BC-ADM,
Clinical Nurse Specialist (CNS) Paula Halcomb, MSN, DNP, APRN, ACNS-BC paula.halcomb@uky.edu Jill Dobias, MSN, APRN, ACCNS-AG, OCN, AOCNS jill.dobias@uky.edu Dee Sawyer, MS, APRN, MLDE, AGCNS-BC, BC-ADM,
MH LHIN Palliative Care Initiative. Dr. Robert Sauls September 2010
 MH LHIN Palliative Care Initiative Dr. Robert Sauls September 2010 1 BACKGROUND Mississauga Halton LHIN: 2008-09 Acute care LOS for palliative care 17, 722 days ALC palliative care 1,992 days 19, 714 days
MH LHIN Palliative Care Initiative Dr. Robert Sauls September 2010 1 BACKGROUND Mississauga Halton LHIN: 2008-09 Acute care LOS for palliative care 17, 722 days ALC palliative care 1,992 days 19, 714 days
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Patient Protection and Affordable Care Act
 Patient Protection and Affordable Care Act BY UCHECHI OKANI POLICIES, POWER, AND POLITICS TEXAS WOMAN S UNIVERSITY March 25, 2011 Introduction MANY IN THE HEALTH CARE PROFESSION ARE WONDERING HOW THE NEW
Patient Protection and Affordable Care Act BY UCHECHI OKANI POLICIES, POWER, AND POLITICS TEXAS WOMAN S UNIVERSITY March 25, 2011 Introduction MANY IN THE HEALTH CARE PROFESSION ARE WONDERING HOW THE NEW
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance. Our Story. What s So Special About Specialty Care?
 Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Accountable Care A path toward accountability for health and health care
 1 Accountable Care A path toward accountability for health and health care Managing Health System Capacity: Market and Policy Solutions December 1, 2008 Elliott Fisher, MD, MPH The Dartmouth Institute
1 Accountable Care A path toward accountability for health and health care Managing Health System Capacity: Market and Policy Solutions December 1, 2008 Elliott Fisher, MD, MPH The Dartmouth Institute
We Honor Veterans Conference March 29, 2018
 VA PANEL What s it Like to Work at the VA? We Honor Veterans Conference March 29, 2018 VA OUTPATIENT PROGRAMS We Honor Veterans Conference March 29, 2018 Heather Rood, RN 1 Objectives Become familiar with
VA PANEL What s it Like to Work at the VA? We Honor Veterans Conference March 29, 2018 VA OUTPATIENT PROGRAMS We Honor Veterans Conference March 29, 2018 Heather Rood, RN 1 Objectives Become familiar with
LICENSES AND CERTIFICATIONS Dates Type License Number Registered Nurse, Georgia RN Present-2019 Registered Nurse, Maryland RN115593
 MICHAEL E. CONTI, CRNA, PHD Assistant Professor Assistant Program, Nurse Anesthesia Program Nell Hodgson Woodruff School of Nursing Emory University Telephone: (404) 727-6540 Email: mconti@emory.edu EDUCATION
MICHAEL E. CONTI, CRNA, PHD Assistant Professor Assistant Program, Nurse Anesthesia Program Nell Hodgson Woodruff School of Nursing Emory University Telephone: (404) 727-6540 Email: mconti@emory.edu EDUCATION
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Postacute care (PAC) cost variation explains a large part
 cost variation explains a large part") INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
IMPROVING THE QUALITY OF LIFE AND CARE FOR PERSONS RECEIVING LONG-TERM SERVICES AND SUPPORTS
 IMPROVING THE QUALITY OF LIFE AND CARE FOR PERSONS RECEIVING LONG-TERM SERVICES AND SUPPORTS Join colleagues as they hear about: Activities and recommendations of LTQA s Quality Measurement and Quality
IMPROVING THE QUALITY OF LIFE AND CARE FOR PERSONS RECEIVING LONG-TERM SERVICES AND SUPPORTS Join colleagues as they hear about: Activities and recommendations of LTQA s Quality Measurement and Quality
21 st Century Health Care: The Promise and Potential of a Learning Health System
 21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
Nursing Home Labor Market Issues. Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans
 UCSF Nursing Home Labor Market Issues Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans Charlene Harrington, Ph.D., R.N., FAAN Professor of Nursing
UCSF Nursing Home Labor Market Issues Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans Charlene Harrington, Ph.D., R.N., FAAN Professor of Nursing
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
COPE Intervention for Cancer Caregivers
 COPE Intervention for Cancer Caregivers Susan C. McMillan, PhD, ARNP, FAAN Distinguished University Health Professor University of South Florida Tampa smcmilla@health.usf.edu COPE Intervention for Cancer
COPE Intervention for Cancer Caregivers Susan C. McMillan, PhD, ARNP, FAAN Distinguished University Health Professor University of South Florida Tampa smcmilla@health.usf.edu COPE Intervention for Cancer