INTERACT for Assisted Living
|
|
|
- Anastasia Carson
- 6 years ago
- Views:
Transcription
1 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20,
2 Bio/Disclosures LuAnne Leistner MS,RN,BC,NE,BC,CALN is the Director of Clinical Services for Assisted Living with Brookdale. She is a graduate of Wright State University, Bluffton University, Sinclair Community College with 38 years of varied nursing experience. She completed course work toward a post graduate certificate with the University of Toledo-Center for Successful Aging and is a member of the National Gerontological Academic Honor and Professional Society of Sigma Phi Omega. She currently holds 2 national certifications from the American Nurses Credentialing Center (ANCC) in gerontological nursing and nursing administration as a nurse executive. She is also a Certified Assisted Living Nurse (CALN) with NADONA/NALNA and has been an Ohio Assisted Living Association (OALA) Board member since 2006 and just completed the Chairperson position from She is a member of the Quality Committee with the National Center for Assisted Living-NCAL and a recently elected Board member to the American Assisted Living Nurse Association (AALNA). She has been with Brookdale since 2005.
3 Acknowledgements of Contributions to this Presentation Kevin O Neil, M.D. Chief Medical Officer Brookdale Senior Living Practiced and taught geriatric medicine for over 30 years. Clinical Professor in the Department of Aging Studies at the University of South Florida. Certified by the American Board of Internal Medicine in both Internal Medicine and Geriatric Medicine. Co-Director for the Center for Medicare Services (CMS) Health Innovations Challenge Grant for application of INTERACT in IL, AL, and HH settings. Joseph G. Ouslander, M.D. Professor /Senior Associate Dean for Geriatric Programs Interim Chair, Department of Integrated Medical Sciences Charles E. Schmidt College of Medicine Professor (Courtesy), Christine E. Lynn College of Nursing Florida Atlantic University Executive Editor, Journal of the American Geriatrics Society 3
4 OBJECTIVES Describe the development of the INTERACT QI program for Assisted Living as it relates to the CMS Innovations Challenge grant Identify the goals of the INTERACT Quality Improvement program and the 4 categories of INTERACT tools ( Identify strategies to prevent avoidable hospitalizations & improve the quality of resident care Describe the role of direct care staff in identifying/reporting acute changes in resident condition Describe how this program could be beneficial in the care of your AL residents & community Apply select INTERACT tools using clinical case scenarios 4
5 The Changing Landscape..HELP! ACA Higher Acuity..ACO.Bundled Payments Pay for Performance.Hospital Readmission Penalties.. Employer Mandates O Bama Care..Satisfaction. Medicare Shared Savings Plan New Medicare Tax Outcomes The Triple Aim Transition of Care BOOST Project Red.. INTERACT CMS Shared Responsibility Quality. Care Transition Partners..National Transitions of Care Coalition Reducing Hospital Admissions.Advanced Care Planning. Accountability EMR Avoidable Re-hospitalizations Post Hospital Syndrome Acute COC.Performance Metrics Medical versus Social Model Safety.State Surveys CNL s The Silver Tsunami.Growing Cost of Dementia Care.. 5
6 Assisted Living Landscape Fastest growing segment of elder care Over 31,000 ALFs 971,900 beds Acuity level has increased* 86% need assistance with taking meds 72% with bathing 57% with dressing 41% with toileting 36% with transferring 23% with eating *Source: National Center for Health Statistics, 2010
7 Triple Aim of CMS Better health of populations Better care for individuals while lowering the per-capita costs of care over time Improve the care experience 7


8 Costs of Care are Unsustainable Total Medicare Expenditures Courtesy: Advisory Board Company 8 Source: Thorpe K and Howard D, The Rise in Spending Among Medicare Beneficiaries: The Role of Chronic Disease Prevalence and Changes in Treatment Intensity, Health Affairs, 379, August 2006; Innovations Center Futures Database; Health Care Advisory Board interviews and analysis.

9 Functional Limitations Exacerbate the Challenge Average Annual Medicare Spending per person in 2006 $15,833 $7,926 $3,559 $2,245 Chronic Disease & Functional Limitations 3 or More Chronic Conditions Only 1-2 Chronic Conditions Only No Chronic Conditions 9 Source: Avalere Health, LLC analysis of the 2006 Medicare Current Beneficiary Survey, Cost and Use File
10 Why it matters - Going to the Hospital Disrupts our resident s/patient s life May cause health complications Is difficult for families and friends Costs billions of dollars to Medicare and Medicaid each year 10 INTERACT Program Overview and Stop and Watch June 2013

11 Benefits for Associates Knowledge to identify and manage acute changes in the community when it is safe and practical Identify residents/patients who require acute care transfers more rapidly Maintain connections and provide support to residents/patients and families Improve resident/patient care using clinical practice tools 11 INTERACT Program Overview and Stop and Watch June 2013

12 Benefits to the Community Better outcomes for our residents/patients Improved resident/patient and family satisfaction Increased reputation for quality care Reduced time associated with transfers Complying with advance care wishes 12 INTERACT Program Overview and Stop and Watch June 2013
13 Impact on Hospitals More than 2000 hospitals have received readmission penalties Penalties: >$280 million Impact on reputation: Hospital Compare website Revisions to CMS Guidelines for Discharge Planning 40% of Medicare beneficiaries admitted to PAC settings Skilled nursing, assisted living, and home care become critical to reducing readmissions 13
14 Definition Transition of Care refers to the movement of patients/residents between healthcare locations, providers or different levels of care within the same location as their conditions and care needs change. A transition of care can occur within settings (hospital ICU to medical unit) between settings( clinic to senior day care center) across health states( personal residence to Assisted Living) Inbetween providers( generalist to specialist) **Taken from AMDA TOC LTC Practice Guideline 14
15 Why Focus on Care Transitions? 20% of Medicare beneficiaries readmitted within 30 days 25% admitted to SNF readmitted within 30 days Negative physical, emotional, psychological impact Costs Medicare billions of dollars 1 $26 billion annually $17.5 billion on in-patient spending Avoidable hospitalizations/readmissions a key strategy 25-42% of readmissions are avoidable 2 1. Jordan Rau. Medicare Revises Hospitals Readmissions Penalties, Kaiser Health News. Oct. 2, Long-Term Quality Alliance. Improving Care Transitions: how quality improvement organizations and innovative communities can work together to reduce hospitalizations among at-risk populations. June 2012.
16 Ineffective Transitions Lead to Poor Outcomes Wrong treatment Delay in diagnosis Severe adverse events Resident complaints Litigation Increased healthcare costs Increased length of stay Australian Council for Safety and Quality in Health Care. Clinical hand-over and Patient Safety literature Review Report. March

17 Post-Hospital Syndrome An Acquired transient period of vulnerability 30 day post hospital risk period (stress/sleep/nutrition/inactivity/ deconditioning/weight loss/pain/medications 20% of Medicare patients discharged experience acute medical problem within 30 days Focus on Stressors that Contribute to Vulnerability Reduce disruption of sleep Minimize pain and stress Promote good nutrition Optimize use of sedatives (reduce risk of delirium and confusion) Emphasize physical activity and strength Enhance cognitive function 17

18 Post-Hospital Syndrome Harlan M Krumholz, M.D. & 30-day period following transition 18
19 Overview of QI Programs BOOST (Better Outcomes for Older Adults Through Safe Transitions) Project RED (Re-Engineered Discharge) Enhanced hospital discharge planning Care Transition Program Transition coach Trained volunteers Empowered patients and caregivers POLST (or MOLST ) (Physician (or Medical) Orders For life Sustaining Treatment) Advance care planning Courtesy: Joseph Ouslander, MD High Quality Care Transitions for Older Adults & Caregivers Bridge Model Social Worker coordinating Aging Resource Center Services at hospital discharge Transitional Care Model APN coordinates care during and after discharge Home, SNF, and clinic visits INTERACT (Interventions to Reduce Acute Care Transfers) Communication Tools, Care Paths, Advance Care Planning Tools, and QI tools for nursing homes and SNFs Slide used with permission of Dr. Joseph Ouslander

20 Geriatrics is a TEAM Sport! It s a lot easier if we all pull together! 20
21 The Solution Acknowledge and empower direct care staff as an integral part of the team. Educate and help direct care staff to recognize and report the not-normal. Learning how to give information can be taught. Provide tools, guidelines and protocols. Improve team communication
22 CMS Health Innovation Challenge Grant 3-Year $7.3 million Grant - Awarded July 1, 2012 to University of North Texas Health Science Center in partnership with Brookdale Senior Living Goal is to revise and implement the INTERACT Program in skilled nursing, assisted living, and home care settings to reduce avoidable readmissions and emergency room transfers Quality Nurse Leaders will evaluate data and guide quality improvement programs Implementing electronic health record to share data between healthcare providers Implementing in 67 Brookdale Communities (Florida/Texas/KS/Denver) during grant period and share lessons learned with acute and post-acute care partners Expected savings of more than $9 million 22
23 PROCESS Organization of the CMS Grant Team Summer 2012 October to December 2012: Began a Review of the INTERACT version 2 tools & made recommendations for changes for AL and HH. External survey of tools conducted with NCAL/AALNA/ through December 2012 Stop & Watch tool SBAR for AL Nurses SBAR for Caregivers-AL December 2012: External survey conducted to gather additional feedback on toolsgoal of survey participants for AL Internal experts: Brookdale Senior Living External experts: National organizations-ncal, AALNA, CEAL, ALFA, The Greenhouse Project, AMDA, Leading Age, Pioneer Network, AARP, and Advanced Practice Nurses (APN s). Pilot tools finalized Spring 2013 & training initiated August 2013 Training of approx. 71 communities (Skilled/AL) completed in June May 2014: Initiated use of select Interact tools for Independent Living NCAL= National Center for Assisted Living AALNA= American Assisted Living Nurse Association

24 All of us have a role in resident care & service. Working as one team to manage subtle changes in condition effectively and safely preventing unnecessary resident transfers Care Associates Dining Services Housekeeping Maintenance Administrative Therapy Nursing Activities/Program Staff
25 3 key strategies to help safely reduce hospital transfers by: 1. Preventing conditions from becoming severe enough to require hospitalization through early identification and assessment of changes in resident condition 2. Managing some conditions without transfer when this is feasible and safe 3. Improving advance care planning and the use of palliative care plans when appropriate as an alternative to hospitalization for some residents

26 Overview of the INTERACT Quality Improvement Program The goal of INTERACT is to improve care, not to prevent all hospital transfers In fact, INTERACT can help with more rapid transfer of residents who need hospital care

27
28 Interact Tools Communication Tools Decision Support Tools Quality Improvement Tools Advanced Care Planning Tools 28
29 Communication Tools Stop and Watch Early Warning Tool SBAR Communication Form and Progress Note for RN/LPN/LVN SBAR Communication Form and Progress Note for Caregiver 29


30 What is STOP and WATCH? Each letter in STOP and WATCH stands for a symptom 12 early warning signs 30 INTERACT Program Overview and Stop and Watch June 2013
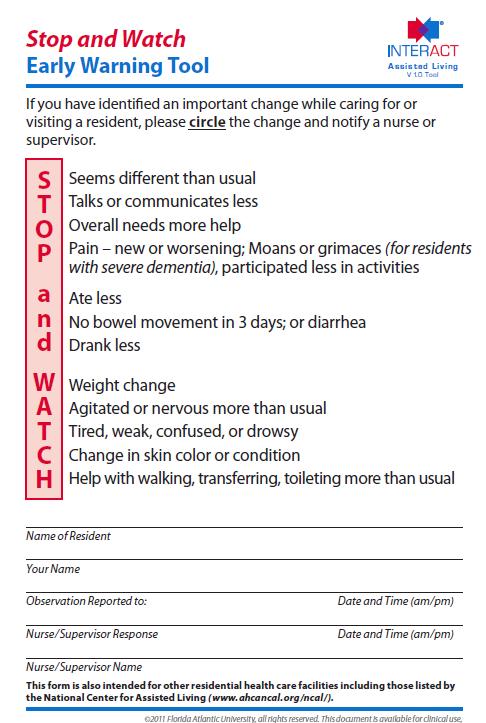
31
32 SBAR 2 SBAR Types for AL Nurse: Situation/Background/Assessment/Request Caregiver or Supervisor: Situation/Background/Appearance/Ready to Call Situation: What is going on with the resident? Background: What is the clinical background or context? Assessment/Appearance: What do I think the problem is? Request/Ready to Call: What do I think needs to be done for the resident?
33
34
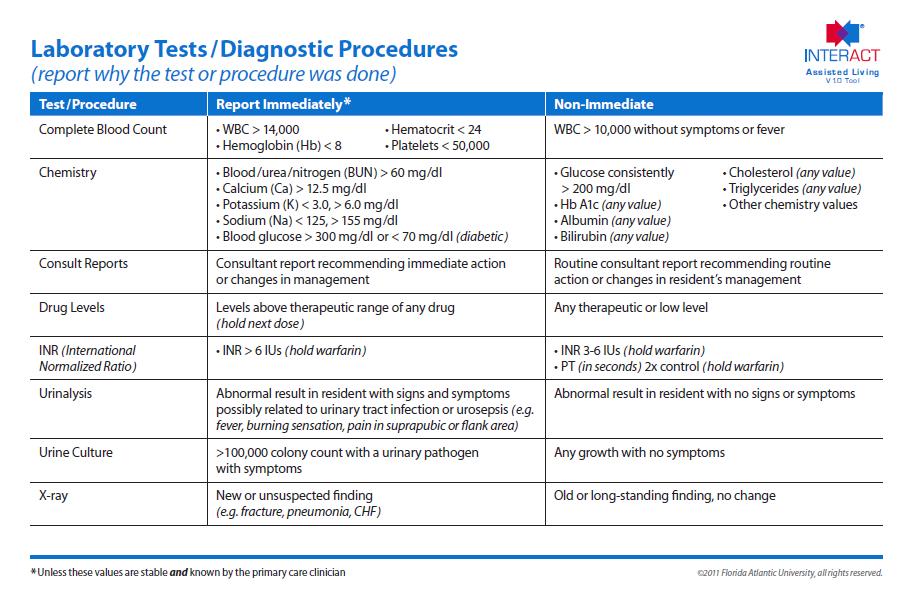
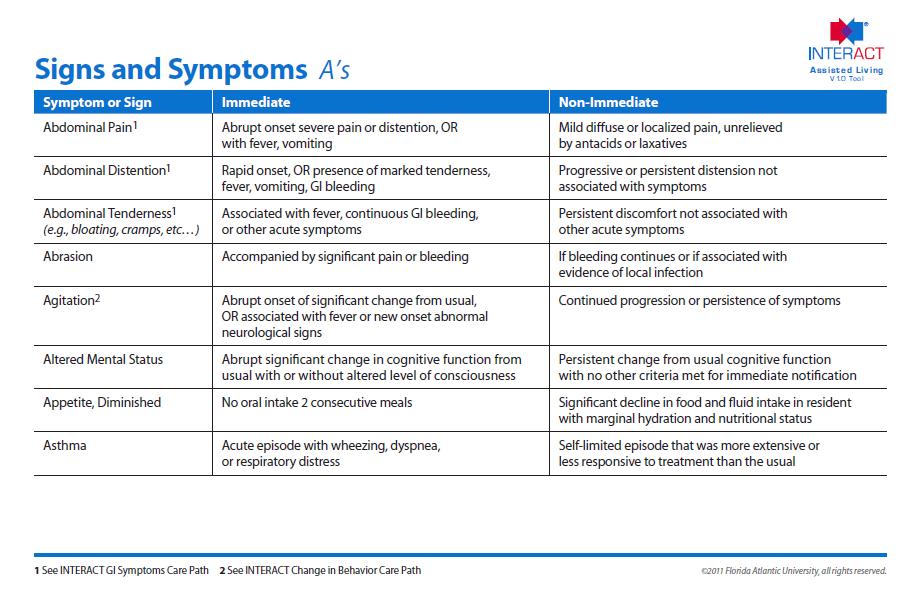
35 Decision Support Tools Change of Condition File Cards Care Paths: Version 4 for NH to be released soon (AL and HH to follow) 9 Care Paths: Lower Respiratory Illness, Acute MS Change, Change in Behavior, Dehydration, Fever, GI Symptoms(N-V-D), SOB, Symptoms of CHF, UTI 35
36
37
38
39
40

41 INTERACT Decision Support Tools: Change in Condition File Cards and Care Paths INTERACT Care Paths All structured the same way Provide guidance on when to notify the MD/NP/PA consistent with File Cards Suggest evaluation strategies Provide recommendations for management and monitoring in the facility Educational tools Recommended as posters Use for case-based learning

42

43 Continuous Improvement On-going review of processes and practices Evaluating the Process/Outcomes Plan Act Do Study 43 INTERACT Continuous Quality Improvement August 2013
44
45
46

47 Advanced Care Planning Advance Care Planning Tracking Form Advance Care Planning Communication Guide Identifying Residents Who May be Appropriate for Hospice or Palliative/Comfort Care Orders Comfort Care Order Set 47 INTERACT Continuous Quality Improvement August 2013

48 ADVANCE CARE PLANNING Advance Care Planning ACP should occur at some time shortly after admission Decisions should be reviewed regularly and at times of acute changes in condition 48
49
50
51 14.00 AL/MC 30 Day Readmission Trend 30-day Readmission Rates for Residents in Assisted Living Communities (n = 41) Readmission Rate Readmission rate Median Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Calendar Month 51
52 AL/MC Hospitalization Trend Hospitalization Rate of Residents in Assisted Living Communities (n = 41) Rate per 1,000 resident days Rate per 1,000 resident days Median Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Calendar Month 52
53 What We Have Learned Importance of Leadership & Communication in quality of care Role of Champions/Co-Champions is critical Sustaining gains & training new associates Integrating QI/tools into the culture Challenges with turnover Family education on Interact is important Advanced Care Planning discussions make a difference Involve all associates in quality improvement Role of a Transition Team 53
54 Transition Team Evaluate market dynamics Engagement of HCP s Evaluating clinical programs Developing effective communication Track and Measure results 54
55 Additional Resources or (Training/Education/Management Strategies) (printed materials-stop & Watch & SBARS) Advancing Excellence in Long Term Care Collaborative 55
56 Interact.fau.edu View web site 56
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
North Carolina Division of Medical Assistance
 North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards
 Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
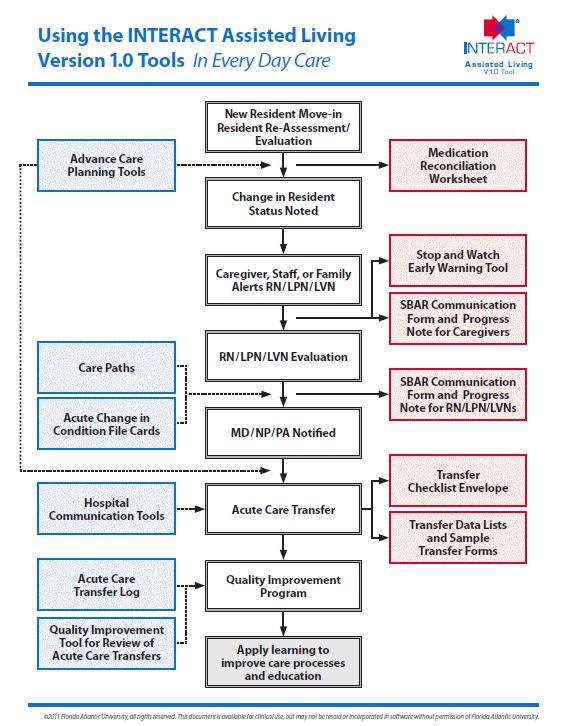
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral)
") Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Telligen. Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016
 Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
with Food, Nutrition, and Dining
 by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going?
 Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going? David Rogers Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration 2016
Lessons Learned from MLTSS Implementation in Florida Where Have We Been and Where Are We Going? David Rogers Assistant Deputy Secretary for Medicaid Operations Agency for Health Care Administration 2016
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative
 Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
The Cost of Care: Understanding the Next Generation of Payment Models
 The Cost of Care: Understanding the Next Generation of Payment Models Presented by: Debbie Welle Powell, MPA, Vice President Sisters of Charity Health System and Exempla Healthcare September 27 th, 2012
The Cost of Care: Understanding the Next Generation of Payment Models Presented by: Debbie Welle Powell, MPA, Vice President Sisters of Charity Health System and Exempla Healthcare September 27 th, 2012
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Overview of a new study to assess the impact of hospice led interventions on acute use. Jonathan Ellis, Director of Policy & Advocacy
 Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
THE BRIDGE MODEL. Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging
 THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
thequalitypost in this issue Get Out of Your Comfort Zone Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone
 thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Case Study: Cass Regional Medical Center
 Case Study: Cass Regional Medical Center CASS REGIONAL MEDICAL CENTER, A COUNTY HOSPITAL SERVING BOTH SUBURBAN AND RURAL COMMUNITIES, PURCHASED A NEW NURSE CALL PLATFORM TO SUPPORT THEIR GOALS TO IMPROVE
Case Study: Cass Regional Medical Center CASS REGIONAL MEDICAL CENTER, A COUNTY HOSPITAL SERVING BOTH SUBURBAN AND RURAL COMMUNITIES, PURCHASED A NEW NURSE CALL PLATFORM TO SUPPORT THEIR GOALS TO IMPROVE
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
The Case for Optimal Staffing: A Call to Action
 The Case for Optimal Staffing: A Call to Action 2015 ANCC National Magnet Conference October 7, 2015 2:30 3:30pm Session C721 Mary Jo Assi, DNP, RN, NEA BC, FNP BC Director of Nursing Practice and Work
The Case for Optimal Staffing: A Call to Action 2015 ANCC National Magnet Conference October 7, 2015 2:30 3:30pm Session C721 Mary Jo Assi, DNP, RN, NEA BC, FNP BC Director of Nursing Practice and Work
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Early Recognition of Sepsis in Long-Term Care
 Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
OhioHealth s Mission: To Improve the Health of Those We Serve
 Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Navigating the ROP Changes: Are You in Compliance? 1 1
 Navigating the ROP Changes: Are You in Compliance? 1 1 Track Your Progress Over Time 25 Antipsychotic PIP Project 20 Antipsychotic Rate 15 10 Sunshine NH Rate National Average 5 0 Jan Feb Mar Apr May Jun
Navigating the ROP Changes: Are You in Compliance? 1 1 Track Your Progress Over Time 25 Antipsychotic PIP Project 20 Antipsychotic Rate 15 10 Sunshine NH Rate National Average 5 0 Jan Feb Mar Apr May Jun
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality
 And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
Improving Collaboration With Palliative Care (PC): Nurse Driven Screenings for PC Consults (C833) Oct 8, 2015 at 2pm
: Nurse Driven Screenings for PC Consults (C833) Oct 8, 2015 at 2pm") 2015 ANCC National Magnet Conference Week 4 of 5 Improving Collaboration With Palliative Care (PC): Nurse Driven Screenings for PC Consults (C833) Oct 8, 2015 at 2pm Melissa Browning, DNP, ARPN, CCNS Ann
2015 ANCC National Magnet Conference Week 4 of 5 Improving Collaboration With Palliative Care (PC): Nurse Driven Screenings for PC Consults (C833) Oct 8, 2015 at 2pm Melissa Browning, DNP, ARPN, CCNS Ann
Overview of Home Health Star Ratings
 Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
Reducing Hospital Acquired Pressure Ulcers in the ICU
 Reducing Hospital Acquired Pressure Ulcers in the ICU Joanne Matukaitis, MSN, RN, NE-BC Christiana Care Health System Newark, Delaware 1 Christiana Care Health System 2 Title goes here 1 Opportunity for
Reducing Hospital Acquired Pressure Ulcers in the ICU Joanne Matukaitis, MSN, RN, NE-BC Christiana Care Health System Newark, Delaware 1 Christiana Care Health System 2 Title goes here 1 Opportunity for
Integrating Community and Primary Care: the eyes and ears of general practice
 re Integrating Community and Primary Care: the eyes and ears of general practice Context and Evidence Increasing numbers of people over 65 with chronic conditions being managed in primary care. Acute exacerbations
re Integrating Community and Primary Care: the eyes and ears of general practice Context and Evidence Increasing numbers of people over 65 with chronic conditions being managed in primary care. Acute exacerbations
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
Long Term Care. Lecture for HS200 Nov 14, 2006
 Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Low Acuity Emergency Department Visits. Joanna Cohen, MD June 2018
 Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Outcomes Reporting: Be Ready to Negotiate with a Hospital
 Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,
Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,