Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
|
|
|
- Daisy Booth
- 6 years ago
- Views:
Transcription
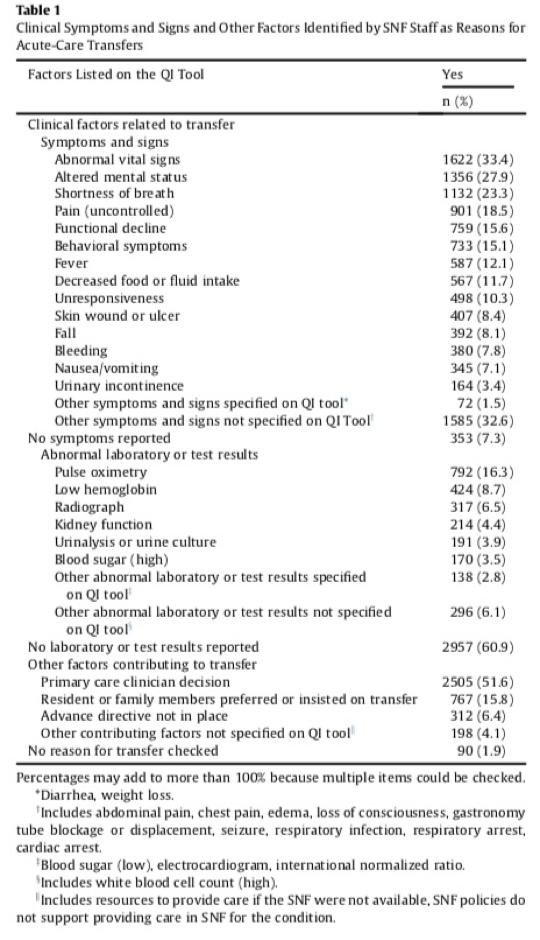
1 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital readmissions and RTAs is a top national priority. Reasons are multifold, but include: Rising Costs Increased risk of complications Especially risky for geriatric populations As many as 68% of readmissions are not considered medically necessary Skilled Nursing Facilities (SNFs) are one of the most significant points of initiation for 30-day hospital readmissions and Return to Acute care settings (RTAs), where 25% of patients nationwide are readmitted within 30 days. While SNFs by definition provide care for patients who are comparatively sicker or require more physical assistance and rehabilitation than those discharged straight to home, this alone does not explain SNFs readmission rates. In order to fix the problems associated with SNF readmissions, it is important to examine the reasons those readmissions occur. Frequently, they are associated with lower staffing rates, lower access to physician advice, inadequate communication between SNFs and the hospitals that discharge patients to them, and a variety of other factors. SNF Readmissions: Root Causes In a recent study examining SNF readmission rates using the IMPACT model of Quality Improvement, staff at participating SNFs conducted root-cause analyses (RCA) of each readmission to determine medical causes, preventability, and any organizational issues exacerbated the need to ride turn to acute. Clinically, the leading reasons staff gave for transferring care included abnormal vitals (33.4%), altered mental state (27.9%), shortness of breath (23.3%), uncontrolled pain (18.5%), functional decline (15.6%), behavioral symptoms (15.1%), fever (12.1%), and decreased food or fluid intake (11.7%). In 60.9% of readmission cases, no laboratory or test results were reported or none were conducted. Where results were reported, the highest percentage of these were abnormal pulse oximetry readings, which occurred in 16.3% of RTA patients. (Full table at bottom of paper). When asked to examine each readmission, staff members at the various SNFs were asked the following question: In retrospect, does your team think this transfer might have been prevented? Their answers were surprising: 23% of readmissions were identified as potentially preventable. The most common opportunities for improvement identified were (1) staff recognized that the condition might have been managed in the facility with existing resources (36%), (2) discussion of care preferences could have occurred earlier and/or advance directives could have been in place (27%), (3) resources necessary to manage the condition were not available
2 (25%), (4) the change could have been detected earlier (23%), and (5) communication could have been better (18%). (Ouslander et al. 259) This speaks to broader themes in geriatric care and the SNF setting nationwide. Problems associated with readmissions include limited training and protocols for responding to changes in patients conditions, inadequate communication between hospitals and SNFs during transfers of care, and most significantly, SNF staff not having adequate access to physicians. Telemedicine in the SNF setting Early adopting skilled nursing facilities have recently started implementing telemedicine partnerships allowing off-site providers to conduct virtual exams and provide medical services alongside nursing staff. With this implementation, participating SNFs have seen a reduction in readmissions. The most successful care model uses telehospitalists, who have the training and experience to determine the difference between a situation that needs ongoing monitoring and treating in place in the SNF setting versus a true medical emergency requiring RTA. Offering SNF staff support during evening and weekend hours when in-house providers are not available, telemedicine allows real-time, video examination, consultation, and supervised monitoring of potential rises in acuity. Telehospitalists also have the ability to order any tests that a facility is capable of providing, and have ongoing communication with staff when managing a patient s condition. Given their hospital experience, they also know what techniques can be used safely given each facility s capabilities. Even when an RTA cannot be avoided, telehospitalist physicians can communicate with Emergency Departments and hospitals directly and clearly, reducing numbers of cases requiring full readmission, helping patients receive needed services more quickly, and avoiding lost information during care transfer. This translates to more patients being able to remain in at the SNF setting while receiving appropriate treatment for a change in acuity, and more patients returning quickly to a SNF setting instead of requiring readmission for monitoring. Notes from the Emerging Field To understand how telehospitalist support can be so effective at avoiding unnecessary hospital admissions, it s helpful to consider some clinical cases stemming from a telemedicine partnership with Skilled Nursing Facility in Ohio. In the eight months between August 2017 and April 2018, the nursing staff at the SNF made 452 total calls to telehospitalists at TeleHealth Solution, a Charlotte, NC based telemedicine company. During these phone calls, nursing staff and the telehospitalist speak over the phone for a consultation, discussing symptoms, lab and test results, and other details of the patient s history and case. If needed, the physician elevates the phone call to a more intensive, real-time video examination, which includes EKGs, physicianguided physical exam, or other monitoring. This elevation in care was required in 39 total cases. Each of these would have resulted in a likely emergent admission without the intervention of the telehospitalist team. Instead, in 32 cases, the partnership allowed patients to be managed on-site and avoided the risks and costs associated with transferring care. 1 Ouslander, J; Naharci, I; et al. Root Cause Analyses of Transfers of Skilled Nursing Facility Patients to Acute Hospitals: Lessons Learned for Reducing Unnecessary Hospitalizations. JAMDA 17 (2016) 256e262 2 Numbers may add up to more than 100% as multiple causes could be checked.
3 Here are some examples of cases where admission was avoided: Case 1: Problem: Respiratory Failure Exacerbated by COPD Solution: Partnership to Counsel Family, Maintain Comfort, Implement Hospice A patient was experiencing respiratory failure exacerbated by COPD. Facility staff reached out to the telehospitals because the patient s saturation levels were down to 82%. The telehospitalists were able to work with staff to titrate oxygen levels, add additional medications to manage the respiratory failure, and to keep the patient comfortable until the family could arrive at bedside. Despite the patient reaching 5 liters of oxygen with only a saturation rate of 90%, the telehospitalists were able to avoid admission by consulting with staff and the family, providing hospice orders, and allowing the patient to remain comfortably in the SNF setting. Case 2 Problem: Memory Care Patient s Accidental Ingestion of Interactive Medications Solution: Telehospitalist s Acute Care Expertise Allowed On-Site Treatment & Monitoring Memory care unit nursing staff called telehospitalists after a patient ingested a large quantity of her roommate s medications that were spilled in their room. These were a combination of anti-psychotics, mood stabilizers, benzodiazepenes and anti-epileptic drugs, and interacted with the patient s own medications. Rather than requiring emergency treatment, working with the telehospitalist allowed appropriate management on-site. The doctor spoke with poison control and confirmed that the majority of the ingested medications had risks of cardiac side effects and interactions. He ran an EKG and evaluated all her cardiac intervals. Working with staff, the physician administered a significant amount of IV fluids, checked labs and routinely checked the patient s EKG to ensure there were no adverse side effects. The patient returned to her baseline with no long term sequelae. Without this coverage, the patient would have required immediate hospital admission for observation. Case 3 Problem: Foley Catheter Bleeding, Hematuria, Hypotension Solution: On-Site Management and Observation, Physician Follow-Up with ED Allowing Return to SNF Nursing staff called telehospitalist to evaluate a patient with hypotension and pure blood coming from foley catheter. Staff had removed the foley before speaking with the physician. The patient complained of being tired but had no specific complaints, and stated he was not pulling at the foley. The patient had hypotension (88/42), and acute hematuria confirmed by labs. The telehospitalist ordered a 1L bolus of IV fluids, a stat CBC, and saw quick improvement in the bleeding and the hypotension. Since the Foley was already pulled, the doctor instructed nursing to obtain a bladder scan in one hour and monitor closely for urine output, seek out a urology appointment for the patient in the morning, and added an extra dose of Flomax in case of obstructive uropathy. Although the patient requested ER evaluation due to feeling weak, the telehospitalist suspected he had acute blood loss anemia. The doctor communicated with the ER to discuss the ongoing patient care and goals. The ER physician was able to reinsert a catheter. Bladder irrigation showed clearing of the urine with a stable hemoglobin. The telehospitalist then worked with the ER for transfer back to the facility for continued care and the requisite urology consult. Without that telehospitalist support, the patient would have had to be admitted for monitoring and further intervention.
4 In the 32 cases where hospital admission was avoided, average costs would estimate that the partnership saved $76,704 in lost revenue, not including PAMA Penalties, reduced star ratings, and credibility among referring hospitals. When Admission is Necessary: Telehospitalist-Verified Need for RTA Although SNFs adapting to new CMS policies are certainly aiming for reduced admissions and RTAs, the entire SNF community and the mandate of care reforms maintain a shared goal of providing top-quality patient care. Therefore, it is critical to examine not only the cases where a potentially costly, traumatic, and risky unnecessary admission can be avoided, but also cases where patients have an escalation in acuity that absolutely requires treatment in an acute care setting. Without adequate physician support, nursing staff who are aware of the problems associated with transfers of care and attempts at facilities to reduce readmissions run into a bind. They do not want readmission, but their primary commitment has to be to the patients, and they do not have the training to judge a patient s acuity on their own. Although the above clinical encounters demonstrate situations where admissions were avoided, telehospitalist partnerships are useful in helping staff have confidence that they are providing the treatment a patient needs while also working on readmission-related quality improvement. In order for these partnerships to be effective, both telehospitalists and staff have to feel comfortable implementing a RTA when necessary, and nursing staff should not have to fear blowback over such decisions. IN THE SEVEN CASES IN THIS PARTNERSHIP WHERE HOSPITAL ADMISSION OCCURRED, CIRCUMSTANCES WERE AS FOLLOWS: 1. Patient was septic, required admission to the ICU. 2. Patient had acute neurological symptoms that required ER evaluation. The Telehospitalist worked with the Emergency Department and planned to transition the patient back to the SNF. Ultimately, the family had safety concerns and requested readmission instead. 3. Patient needed an emergency endoscopy due to an active GI bleed confirmed by telehospitalist with testing. 4. Patient had respiratory failure and required ICU admission. 5. Patient was hypoxic and hypotensive, likely aspiration pneumonia, required hospitalization. 6. Patient had acute hypoxic respiratory failure, with saturations dropping to the mid 80s despite an NRB mask. 7. Patient had fall with head trauma and lacerations. In all of these cases, an on-site physician would have been extremely unlikely to avoid an admission, given the facility s available equipment and the level of care provided. Nursing staff working alone or with an offsite but local on-call physician could certainly not have avoided readmission because of the time it would require for an on-site physician to arrive. In fact, although telehospitalists provided coverage during evenings, nights, weekends and holidays, making them the physicians responsible for patient outcomes during more than half of each week, the cases they managed accounted for only 5.9% of the 117 hospital inpatient admissions from this SNF during the study period. 3 Method of calculation is average Length of Stay (5.1 days) multiplied by Medicare reimbursement ($470/day) multiplied by number of admissions avoided.
5 Conclusion: If Skilled Nursing Facilities are to follow the standard quality improvement mandate of providing better care for every patient every day while lowering costs, they must be able to provide the services and expertise needed to manage their patients changes in acuity without resorting to unnecessary admissions. Yet nationally, they have not proven ability to do so, usually through no fault of their own. Although nursing staff have amazing capabilities and knowledge bases and should be providing services at the top of their licenses, the medical and payer community needs to recognize that it cannot expect those staff members to make decisions about acuity beyond their training. In order for treating-in-place to become the standard of care, with reduced risks and improved patient outcomes, SNFs require physician support at all hours. With today s technology, however, that support does not have to include in-person and on-site physician staffing. Telemedicine offers physician availability to nursing staff and immediate access to evaluation if required. This increases the chances for each SNF resident to get the care they deserve in the appropriate setting, avoiding the risks and costs of unnecessary hospitalization while escalating care when needed. As the data from this partnership demonstrates, nursing staff working together with acute care experts like hospitalists through telemedicine can make excellent decisions about the necessity of RTAs. When they do, the result is improved patient experiences and outcomes, lowered risks, and lowered costs.
6 APPENDIX:
Telehealth Program. Presenter: Colin Ward, VP Population Health & Clinical Integration. University of Maryland Upper Chesapeake Health
 Telehealth Program Presenter: Colin Ward, VP Population Health & Clinical Integration University of Maryland Upper Chesapeake Health 2 Problem 1 in 6 hospital admissions result in a readmission within
Telehealth Program Presenter: Colin Ward, VP Population Health & Clinical Integration University of Maryland Upper Chesapeake Health 2 Problem 1 in 6 hospital admissions result in a readmission within
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Assessment and Reassessment of Patients
 Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
EMERGENCY MEDICINE CLINICAL ROTATION COMPETENCY BASED CURRICULUM
 CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Amended Date: October 1, Table of Contents
 Amended Date: October 1, Table of Contents") Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Subject: Skilled Nursing Facilities (Page 1 of 6)
") Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Recognizing and Reporting Acute Change of Condition
 Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
MDS Language Impacts CAHs
 MDS Language Impacts CAHs April 2014 Kerry Dunning, MHA, MSH, CPAR, RAC-CT Sr VP, Long Term Care Division GPS Healthcare Consultants Objectives To Sufficiently Understand: Medicare intent for documentation
MDS Language Impacts CAHs April 2014 Kerry Dunning, MHA, MSH, CPAR, RAC-CT Sr VP, Long Term Care Division GPS Healthcare Consultants Objectives To Sufficiently Understand: Medicare intent for documentation
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Tube Feeding Status Critical Element Pathway
 Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview:
 Overview:") Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview: In 1986, Congress enacted EMTALA as part of the Consolidated Omnibus Budget Reconciliation Act (COBRA). Often
Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview: In 1986, Congress enacted EMTALA as part of the Consolidated Omnibus Budget Reconciliation Act (COBRA). Often
HEALTHCARE: Academic Medical Center & Health System
 HEALTHCARE: Academic Medical Center & Health System BEFORE Results ED Time in Dept (minutes) Each data point is the weekly average. Volume was relatively flat during the shown time period. [Academic Medical
HEALTHCARE: Academic Medical Center & Health System BEFORE Results ED Time in Dept (minutes) Each data point is the weekly average. Volume was relatively flat during the shown time period. [Academic Medical
Guidelines for Kuakini Medical Center General Surgery Rotation (Formulated by a previous Chief Surgical Resident)
") Guidelines for Kuakini Medical Center General Surgery Rotation (Formulated by a previous Chief Surgical Resident) Welcome to Kuakini Medical Center! The typical patient is in the Geriatric age group. As
Guidelines for Kuakini Medical Center General Surgery Rotation (Formulated by a previous Chief Surgical Resident) Welcome to Kuakini Medical Center! The typical patient is in the Geriatric age group. As
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Skilled Nursing Facility Admission Orders
 Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010)
") Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
General information. Hospital type : Acute Care Hospitals. Provides emergency services : Yes. electronically between visits : Yes
 General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
The new role of hospitalists. Keeping patients out of the hospital. Cynthia Litt, MPH Eugene Kim, MD
 The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Creating Laboratory Value for a Competitive Advantage
 Creating Laboratory Value for a Competitive Advantage LEO SERRANO FIRSTPATH LABORATORY SERVICES 1 2018 Cardinal Health. All Rights Reserved. Learning objectives After this webinar, you will be able to:
Creating Laboratory Value for a Competitive Advantage LEO SERRANO FIRSTPATH LABORATORY SERVICES 1 2018 Cardinal Health. All Rights Reserved. Learning objectives After this webinar, you will be able to:
Patient Selection and Education. (Allison + Zurlo)
") 2 Patient Selection and Education (Allison + Zurlo) There are some fundamental medical and non-medical questions to answer in determining whether a patient is a candidate for OPAT: Is the patient clinically
2 Patient Selection and Education (Allison + Zurlo) There are some fundamental medical and non-medical questions to answer in determining whether a patient is a candidate for OPAT: Is the patient clinically
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care
 Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare
 Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals
 Rural Hospitals under 100 Beds and Critical Access Hospitals") SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
SWING BED (SWB) Rural Hospitals under 100 Beds and Critical Access Hospitals Federal Regulations Hospitals under 100 Beds Critical Access Hospitals CMS State Operations Manual Appendix T Regulations and
The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances
 WHITE PAPER The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances The OB-ED model fundamentally changes how hospitals care for expectant mothers in a way that improves
WHITE PAPER The OB-ED: Redefining the Standard of Women s Care and Strengthening Hospital Finances The OB-ED model fundamentally changes how hospitals care for expectant mothers in a way that improves
RAPID RESPONSE TEAM & E-ICU ROBOT. Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health
 RAPID RESPONSE TEAM & E-ICU ROBOT Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health Kelly J. Green, R.N., J.D. Krieg DeVault LLP 12800 N. Meridian Suite 300
RAPID RESPONSE TEAM & E-ICU ROBOT Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health Kelly J. Green, R.N., J.D. Krieg DeVault LLP 12800 N. Meridian Suite 300
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Emergency Department Facility Coding and Billing
 Emergency Department Facility Coding and Billing The Basics of Facility Coding A Historical View of Hospital Coding and Reimbursement for ED Services E/M Visit Level Coding ED Procedure Coding Payment
Emergency Department Facility Coding and Billing The Basics of Facility Coding A Historical View of Hospital Coding and Reimbursement for ED Services E/M Visit Level Coding ED Procedure Coding Payment
Bundled Payment Primer
 Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Why Shepherd? Shepherd Center Patients. Here s How We Measure Up: Shepherd Patient Population
 Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
A Guide to CDI. AAPC National Conference Salud! HEALTHCARE SOLUTIONS
 A Guide to CDI AAPC National Conference 2013 Salud! HEALTHCARE SOLUTIONS Let patient centric, patient driven, patient quality of care guide needs Objectives Identify the Purpose of an effective CDI program
A Guide to CDI AAPC National Conference 2013 Salud! HEALTHCARE SOLUTIONS Let patient centric, patient driven, patient quality of care guide needs Objectives Identify the Purpose of an effective CDI program
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
Running head: FAILURE TO RESCUE 1
 Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT
 April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
2017 LEAPFROG TOP HOSPITALS
 2017 LEAPFROG TOP HOSPITALS METHODOLOGY AND DESCRIPTION In order to compare hospitals to their peers, Leapfrog first placed each reporting hospital in one of the following categories: Children s, Rural,
2017 LEAPFROG TOP HOSPITALS METHODOLOGY AND DESCRIPTION In order to compare hospitals to their peers, Leapfrog first placed each reporting hospital in one of the following categories: Children s, Rural,
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH
 WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Final Report. January 12, Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek
 Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Administrators. Medical Directors. 61% The negative impact on our hospital-based program s. 44% We will need to consider the most appropriate or most
 2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
EarlySense InSight. Integrating Acute and Community Care
 EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration