QIO Care Transitions Activity: the Good News so far
|
|
|
- Daisy Watts
- 5 years ago
- Views:
Transcription
1 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; Senior Project Director Colorado Foundation for Medical Care This material was prepared by CFMC (PM CO 2012), the Medicare Quality Improvement Organization for Colorado under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy.
2 Objectives Why we know it worked JAMA publication Describe the need for better transitions Discuss leading interventions in this work Outline current and future work and implications National and Alabama data 2


3 ork.com/article.aspx? articleid= It Worked!!

4 August 2008-July 2011: 14 QIOs working in 14 Communities AL: Tuscaloosa CO: Northwest Denver FL: Miami GA: Metro Atlanta East IN: Evansville LA: Baton Rouge MI: Greater Lansing area NE: Omaha NJ: Southwestern NJ NY: Upper capital PA: Western PA RI: Providence TX: Harlingen HRR WA: Whatcom county 4
5 Totals among Communities 70 Hospitals 277 Skilled Nursing Facilities 316 Home Health Agencies 89 Other types of Providers (Dialysis, Hospice, etc.) 666 ZIP Codes 1,125,649 Fee-for-Service Medicare Beneficiaries 5
6 The Strategy Define a community Identify service patterns associated with readmission Recruit and convene providers/partners To reduce unplanned 30d hospital readmissions for the community Using evidence based interventions and tools 6
7 Interim Quarterly Results Baseline Quarter Readmissions = 12,926 First quarter after intervention readmissions = 12, % 19.80% 19.60% 19.68% 19.40% 19.48% 19.20% p= % 18.80% Jan07- Mar07 N = Apr07- Jul07-Sep07 Jun07 N = N = Oct07- Dec07 N = Jan08- Mar08 N = A Apr08- Jun08 N = Jul08-Sep08 N = B Oct08- Dec08 N = Jan09- Mar09 N = C Apr09- Jul09-Sep09 Jun09 N = N = Oct09- Dec09 N = Jan10- Mar10 N = D Apr10- Jul10-Sep10 Jun10 N = N = Oct10- Dec10 N = 59630
8 5,000 10,000 15,000 20,000 25,000 30,000 Numerator and Denominator Quarterly 68,000 Numerator (readmissions) Denominator (admissions) 63,000 58,000 53,000 48,000 43,000 Jan07-Mar07 N = Apr07-Jun07 N = Jul07-Sep07 N = Oct07-Dec07 N = Jan08-Mar08 N = A Apr08-Jun08 N = Jul08-Sep08 N = B Oct08-Dec08 N = Jan09-Mar09 N = C Apr09-Jun09 N = Jul09-Sep09 N = Oct09-Dec09 N = Jan10-Mar10 N = D Apr10-Jun10 N = Jul10-Sep10 N = Oct10-Dec10 N = Quarter The unit N represents target community eligible beneficiaries. MIlestones: A) baseline quarter; B) Care Transitions theme initiation (Aug 2008); C) intervention implementation (Jan 2009); and D) 28-month follow up quarter.
9 Rehospitalization Trends, Intervention and Comparison Communities -5.7% (p<.001) -2.1% (p=.08) P=.03 (difference)
10 Hospitalization Trends, Intervention and Comparison Communities -5.7% (p<.001) -3.1% (p<.001) P=.01 (difference)
11 Statistical process control Assesses variation in an outcome presumed to be related to system functioning A change worth investigating: Reduced variation (increased control) Significant change in the value of the outcome Process control limits = 3sd from the mean variation during baseline Significant : 8 points in a row above/below the mean with at least one point in the during intervention time period OR A single point above/below the process control limit in the during intervention time period
12 Community Results Rehospitalizations Intervention Comparison Special cause decrease 10/14 (71%) 22/50 (44%) Special cause increase 2/14 (14%) 13/50 (26%) Hospitalizations Intervention Comparison Special cause decrease 13/14 (93%) 31/50 (63%) Special cause increase 0/14 (0%) 8/50 (16%)
13 Control Charts an innovative way to measure progress in healthcare
14
15 Readmissions per 1000 Benes Target Community - AL_0 Readmissions per 1000 Benes 24 3s Limits For n=2: 22 UCL=22.01 The Test1 Test1Test1 Test1 Test1 Test1 Test1 Test1 X=20.08 LCL=18.14 Improvement continues Target Community - TX_0 22 3s Limits For n=2: 20 UCL= X= Test2 Test2 Test1 Test1 Test1 Test1 Test1 Test1 Test1 Test LCL=16.42
16 What s important about this publication? Intervention communities avoided twice as many rehospitalizations (1 hospitalization for every 1000 Medicare beneficiaries) and hospitalizations (5 for every 1000 beneficiaries) as comparison communities Improvement for whole communities is a promising strategy Providers engaged based on relevance QIOs in the role of convener/supporter Included community and social services Unadjusted geographic population data allows easy data display/sharing
17 What Else was Important? Allowing flexibility leverages local resources/context Shewhart control charts published in a major peer-reviewed journal Rehospitalizations/1000 and hospitalizations/1000 metrics proved useful for improvement work
18 Why are people readmitted? Provider-Patient interface Unmanaged condition worsening; Use of suboptimal medication regimens; Return to an emergency department
19 Why are people readmitted? Provider-Patient interface Unmanaged condition worsening; Use of suboptimal medication regimens; Return to an emergency department Unreliable system support Lack of standard and known processes; Unreliable information transfer; Unsupported patient activation during transfers
20 Why are people readmitted? Provider-Patient interface Unmanaged condition worsening; Use of suboptimal medication regimens; Return to an emergency department Unreliable system support Lack of standard and known processes; Unreliable information transfer; Unsupported patient activation during transfers No Community infrastructure for achieving common goals
21 Why are people readmitted? Provider-Patient interface Unmanaged condition worsening; Use of suboptimal medication regimens; Return to an emergency department Unreliable system support Lack of standard and known processes; Unreliable information transfer; Unsupported patient activation during transfers No Community infrastructure for achieving common goals
22 Why Engage a Community? Every readmission begins with hospital discharge Every transition has 2 sides Isolated information is not safe medical management Inevitably need to share The problem of home Patients are people too Visibility to drive improvement and mission Providers are people too


23 It s not a hospital project

24 It s a Community Problem HHA SNF
25 Ways to Convene a Community

26
27 System-Level Drivers of Readmissions Provider-Patient interface Unmanaged condition worsening; Use of suboptimal medication regimens; Return to an emergency department Unreliable system support Lack of standard and known processes; Unreliable information transfer; Unsupported patient activation during transfers No Community infrastructure for achieving common goals
28 Interventions and Drivers Intervention Patient Activation Standard Process Information Transfer Care Transitions Intervention Transitional Care Model INTERACT II HHQI Best Practices Project BOOST Bridge model Project RED GRACE Model STAAR Initiative

29 CMS Table of Interventions Available at:
30 Hospital discharge standardization protocols RED 11 item checklist BOOST QI support for hospitalists and discharge planners Evidence: weak for readmissions; insufficient but probably necessary Driver: standard known process, information transfer Setting: Hospital

31 The CMS Discharge Planning Checklist Description: CMS developed checklist for patients and families to prepare for care capability after transition Resource: ations/pubs/pdf/11376.pdf
32 Care Transitions Intervention SM (CTI) Description: Transitions coaches support selfmanagement capacity Personal Health Record Medication discrepancy tool 5 contacts Evidence: RCTs and the Care Transitions Theme (30-50% 30d; 50% 180d) Driver: patient activation, information transfer Setting: hospital to home
33 Transitional Care Nursing Model Description: Transitional Care Nurses follow patients from the hospital into the home; work with a multidisciplinary team to develop and deliver comprehensive care plan; risk assessment tool(s) Evidence: RCTs (45% 90d) Driver: information transfer, creates a new standard process that individualizes services Setting: hospital to home health
34 Interventions to Reduce Acute Care Transfers (INTERACT) Description: Toolkit for SNF personnel to reduce avoidable hospital admission. Three types of tools: 1) communication; 2) clinical care paths; 3) advance care planning. Evidence: Ouslander (2008): Higher hospitalization rates associated with larger facilities, more Medicaid and Medicare skilled care residents, lower percentage of Caucasian residents and higher percentage of residents with impaired decision making; 68% of hospitalizations were avoidable, per expert panel record review.


35 In Reality Adapted models/components of models 2 tracks: activation plus provider process

36 What s he saying? I sure hope my wife is getting this.. No I m good to go. Whatever you say is what we ll do Doctor Blah blah blah, blah blah. Any questions? 1. Patient activation trumps all


37 The PAM is very helpful to guide interventions

38 2. Local adaptation is inevitable Adapt gold standard models Do not adapt others adaptations

39 3. Ask the community to help Brought to you by your Community Partners

40 Organize a Community Tie participation to values Include personal narratives Develop flexible tactics Community champion Align with other federal and local initiatives Develop a leadership team/advisory group
41 4. Measuring is important p= Insist on a population based measure of progress 41
42 Recurring Themes in Successful Communities Community cohesiveness Provider activation/will Strategic Partners Cross-setting Work Coaching as an intervention Strong community leadership (e.g., physician champions)
43 QIO Care Transitions: Good News continues Integrate Care for Populations & Communities August 2011-present
44 August 2011 Integrating Care for Populations & Communities Aims: Improve the quality of care for Medicare beneficiaries as they transition between providers Reduce 30 day hospital readmissions (nationally) by 20% within 3 years 44
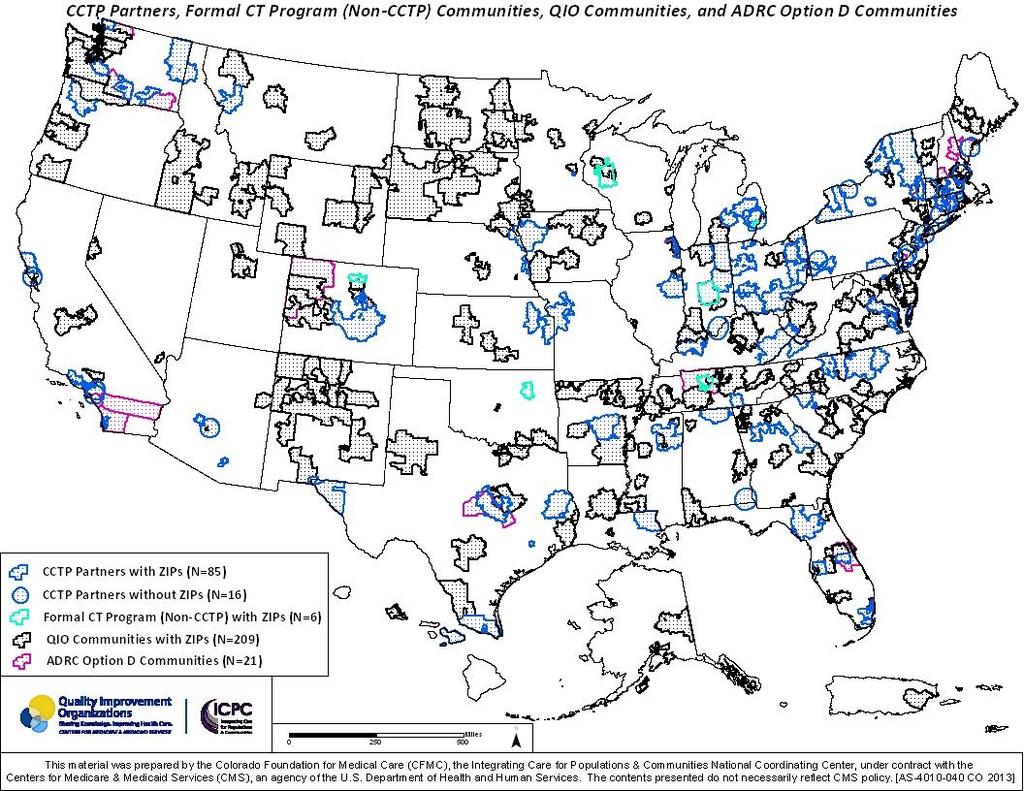
45 QIO assistance Toolkit Root cause analysis Learning and Action Networks Learning Sessions Community Convening Social Network Analysis Diagrams Hot-spotting maps Data, data, data (e.g., readmission/admission metrics; reach/intervention effectiveness measures) 45
46 QIO Accomplishments as of March 31, 2013 # of Engaged Communities 375 # of Beneficiaries Living there 12,455,368 # Formally Recruited Communities 227 # Communities with Signed Coalition Charter 221 # Applications Submitted 125 # Communities Receiving Formal Funding 81 # Recruited Hospitals 859 # Recruited Nursing Homes 1,533 # Recruited Home Health Agencies 901 # Recruited Hospice Facilities 342 # Recruited Dialysis Facilities 91 # Recruited Outpatient Physicians > 1900
47
48 National Coalition of QIO-recruited Communities Early Progress 6.8%
49 National Coalition of QIO-recruited Communities Early Progress 9.1%
50 50
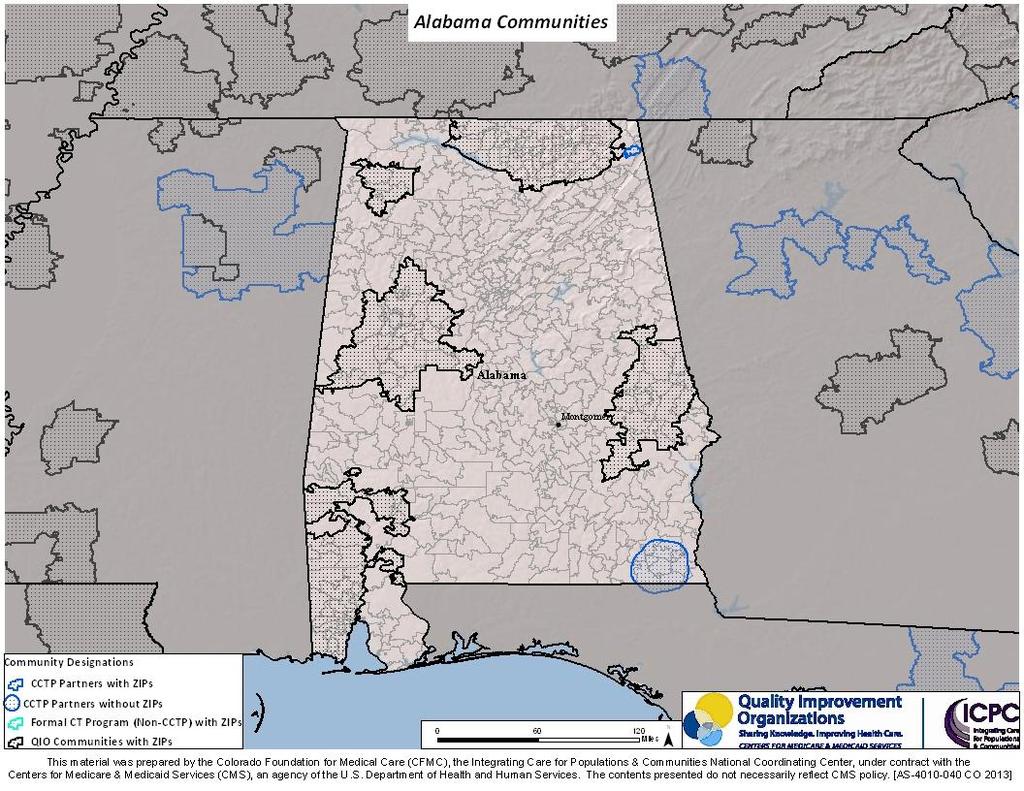
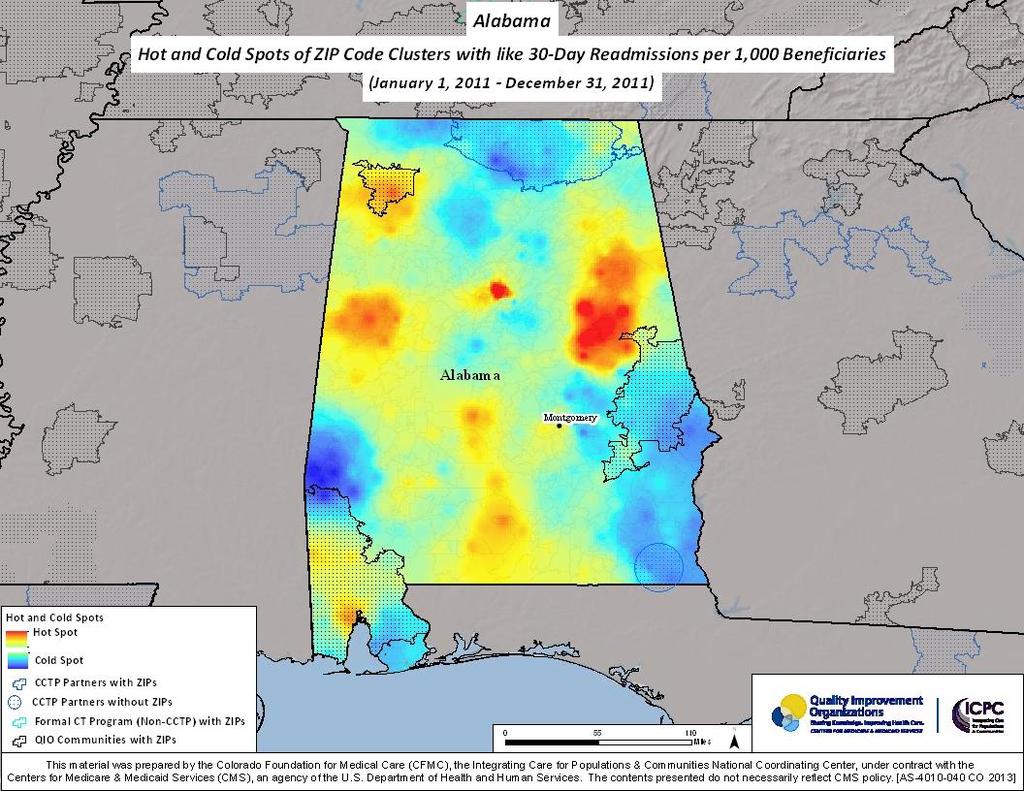
51 Alabama Data Tied for 3 rd highest number of recruited communities over LOE; 5 th highest number of engaged communities over LOE Among 17 states having ALL interventions showing improvement 38 th in readmissions reduction 41 st in admissions reduction
52
53 Interim Reductions!!! 10/1/10-3/31/11 compared to 10/1/11-3/31/12 Community Readmissions Admissions Statewide 2.9% 2.8% Community Care Coalition of East Alabama Top of Alabama Care Transitions Innovation Coalition Healthy Gulf Coast Care Transitions 14.9% 9.4% 13.1% 5.2% 7.2% 6.5% 53


54 Alabama
55 Top of Alabama Care Transitions Innovation Coalition CCTP Partner as of March 2013 Intervention # Beneficiaries Touched PCP follow-up appointments arranged 600 CHF program readmission rates 1500 INTERACT II 42
56 Percent of those contacted Patients Contacted Who Had Hospital Arranged Follow-up Appointments 100% 90% 80% 70% 60% 50% 40% R² = Median 41% 30% 20% <-Intervention 10% 0% Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Month
57 Readmission Rate Monthly CHF Readmission Rates 35.00% 30.00% 25.00% 20.00% CHF Program Median 18.67% 15.00% 10.00% R² = % 0.00% Month
58 Rate Rate of Unplanned ER Visit + Hospitalization 0.45% 0.40% 0.35% 0.30% 0.25% 0.20% 0.15% 0.10% 0.05% 0.00% R² = Median 0.25% Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Month
59 October 1, 2010-March 31, 2011 compared to October 1, 2011-March 31, % Relative Improvement in Admissions/1000 Medicare FFS Beneficiaries 13.1% Relative Improvement in Readmissions/1000 Medicare FFS Beneficiaries
60 Community Care Coalition of East Alabama Intervention # Beneficiaries Touched PCP follow-up appointment scheduled by patient 256
61 Compliance Percent of Patients Who Made Their PCP Appointment 100% 90% 80% R² = Mean 92% 70% 60% 50% <-Intervention 40% 30% 20% 10% 0% March 26-31, 2012 Apr-12 May-12 Jun-12 Jul-12 Month
62 October 1, 2010-March 31, 2011 compared to October 1, 2011-March 31, % Relative Improvement in Admissions/1000 Medicare FFS Beneficiaries 14.9% Relative Improvement in Readmissions/1000 Medicare FFS Beneficiaries
63





64 Seeing Ourselves in the System First image of the entire Earth Each of us is a system citizen in that we are (potential) change agents in the systems of which we are a part.
65 How to Get Started Contact your QIO Join (and listen to archived) Care Transitions Learning Sessions Browse our Toolkit 65
66 Additional Resources Medicaring an independent website for improving care transitions Partnership for Patients Community-based Care Transitions Program The AoA Toolkit 66
67 Thank You & Questions NCC website Kim Irby
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Care Transitions in Michigan
 Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Telligen. Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016
 Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
THE BRIDGE MODEL. Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging
 THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
THE BRIDGE MODEL Walter Rosenberg, MSW, LCSW Manager of Transitional Care Rush University Medical Center Health and Aging "If patient engagement were a drug, it would be the blockbuster drug of the century,
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Analysis of Incurred Claims Trend and Provider Payments
 Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Medicare & Medicaid EHR Incentive Programs Robert Tagalicod, Robert Anthony, and Jessica Kahn HIT Policy Committee January 10, 2012
 Medicare & Medicaid EHR Incentive Programs Robert Tagalicod, Robert Anthony, and Jessica Kahn HIT Policy Committee January 10, 2012 Medica re Active Registrations December 2011 December-11 YTD Eligible
Medicare & Medicaid EHR Incentive Programs Robert Tagalicod, Robert Anthony, and Jessica Kahn HIT Policy Committee January 10, 2012 Medica re Active Registrations December 2011 December-11 YTD Eligible
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Driving Quality Improvement in Managed Care. Toby Douglas, Director California Department of Health Care Services
 1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
CHC-A Continuity Dashboard. All Sites Continuity - Asthma. 2nd Qtr-03. 2nd Qtr-04. 2nd Qtr-06. 4th Qtr-03. 4th Qtr-06. 3rd Qtr-04.
 PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
3/24/2016. Value of Quality Management. Quality Management in Senior Housing: Back to the Basics. Objectives. Defining Quality
 Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Best Practices for Safety & Care Coordination
 Best Practices for Safety & Care Coordination Thursday, February 23, 2016 Nicole Skyer-Brandwene MS, RPh, BCPS, CCP Adverse Drug Events Network Task Lead Andrew Miller, MD, MPH Care Coordination Network
Best Practices for Safety & Care Coordination Thursday, February 23, 2016 Nicole Skyer-Brandwene MS, RPh, BCPS, CCP Adverse Drug Events Network Task Lead Andrew Miller, MD, MPH Care Coordination Network
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Patient Safety in Ambulatory Care: Why Reporting Counts. August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH
 Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
DSRIP Programs: Delivery System Reform Incentive Payment The Current Situation
 DSRIP Programs: Delivery System Reform Incentive Payment The Current Situation Claudia Gourdon 203-580-5408 cgourdon@hfgusa.com DSRIP What it Is and Isn t Drivers Behind DSRIP State Programs Commonalities
DSRIP Programs: Delivery System Reform Incentive Payment The Current Situation Claudia Gourdon 203-580-5408 cgourdon@hfgusa.com DSRIP What it Is and Isn t Drivers Behind DSRIP State Programs Commonalities
University of West Georgia. University Web Advisory Committee Fiscal Year 2015
 University of West Georgia University Web Advisory Committee Fiscal Year October 7, 2014 o bold. dvance and Reinvent University of West Georgia 2 oday s Agenda. Agenda, Web Advisory Committee, charge,
University of West Georgia University Web Advisory Committee Fiscal Year October 7, 2014 o bold. dvance and Reinvent University of West Georgia 2 oday s Agenda. Agenda, Web Advisory Committee, charge,
DoD-State Liaison Update NCSL August 2015
 UNITED STATES DEPARTMENT OF DEFENSE DoD-State Liaison Update NCSL August 2015 Mr. Thomas Hinton On Behalf of Dr. Tom Langdon Director, State Liaison and Educational Opportunity Office of the Deputy Assistant
UNITED STATES DEPARTMENT OF DEFENSE DoD-State Liaison Update NCSL August 2015 Mr. Thomas Hinton On Behalf of Dr. Tom Langdon Director, State Liaison and Educational Opportunity Office of the Deputy Assistant
Episode Payment Models:
 Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY Introduction
 COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Avoiding the Cap Trap What Every Hospice Needs to Know. Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc.
 Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Hospitalization Patterns for All Causes, CV Disease and Infections under the Old and New Bundled Payment System
 Hospitalization Patterns for All Causes, CV Disease and Infections under the Old and New Bundled Payment System Robert N Foley, MB, FRCPI, FRCPS United States Renal Data System Data Coordinating Center
Hospitalization Patterns for All Causes, CV Disease and Infections under the Old and New Bundled Payment System Robert N Foley, MB, FRCPI, FRCPS United States Renal Data System Data Coordinating Center
Ohio SIM: Episode-based payment updates. Webinar June 29, 2017
 Ohio SIM: Episode-based payment updates Webinar June 29, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ UT
Ohio SIM: Episode-based payment updates Webinar June 29, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ UT
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events
 Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
2016 Edition. Upper Payment Limits and Medicaid Capitation Rates for Programs of All-Inclusive Care for the Elderly (PACE )
") 2016 Edition Upper Payment Limits and Medicaid Capitation Rates for Programs of All-Inclusive Care for the Elderly (PACE ) R ABSTRACT The Program of All-Inclusive Care for the Elderly (PACE ) is a federal
2016 Edition Upper Payment Limits and Medicaid Capitation Rates for Programs of All-Inclusive Care for the Elderly (PACE ) R ABSTRACT The Program of All-Inclusive Care for the Elderly (PACE ) is a federal
D. Fistula First (FF) Initiative.
 Initiative.") D. Fistula First (FF) Initiative. The development of Quality Improvement Projects (QIP) is mandated in the ESRD Network contracts with CMS. The QIPs are developed and directed by the MRB, then reviewed,
D. Fistula First (FF) Initiative. The development of Quality Improvement Projects (QIP) is mandated in the ESRD Network contracts with CMS. The QIPs are developed and directed by the MRB, then reviewed,
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes
 Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Overview of Home Health Star Ratings
 Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
Overview of Home Health Star Ratings September 23, 2015 Presented by: Liz Silva Deyta Analytics, a division of HEALTHCAREfirst Agenda Home Health Star Ratings Quality of Patient Care Star Rating Patient
Program Overview. Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series. June 12, 2018
 Series. June 12, 2018") Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series Program Overview June 12, 2018 2017 New York State, Department Of Health, Office of Health Insurance Programs.
Medicaid Accelerated exchange Series and Medicaid Accelerated exchange New York (MAXny) Series Program Overview June 12, 2018 2017 New York State, Department Of Health, Office of Health Insurance Programs.
National Trends Winter 2016
 National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Using the BaldrigeCriteria to Achieve High Reliability
 Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Cardinal Bank & George Mason University
 Cardinal Bank & George Mason University 2th Annual Economic Conference Friday, January 13, 212 cra.gmu.edu Cardinal Bank/George Mason University 2 th Annual Economic Conference Is This a Recovery or What?
Cardinal Bank & George Mason University 2th Annual Economic Conference Friday, January 13, 212 cra.gmu.edu Cardinal Bank/George Mason University 2 th Annual Economic Conference Is This a Recovery or What?
Introducing the Discharge to Community Quality Measure
 Introducing the Discharge to Community Quality Measure Rachel Delavan, Director of Research Dawn Murr-Davidson, RN BSN, Director of Quality Initiatives October 20, 2015 1 Objectives Define the discharge
Introducing the Discharge to Community Quality Measure Rachel Delavan, Director of Research Dawn Murr-Davidson, RN BSN, Director of Quality Initiatives October 20, 2015 1 Objectives Define the discharge
The Cost of Care: Understanding the Next Generation of Payment Models
 The Cost of Care: Understanding the Next Generation of Payment Models Presented by: Debbie Welle Powell, MPA, Vice President Sisters of Charity Health System and Exempla Healthcare September 27 th, 2012
The Cost of Care: Understanding the Next Generation of Payment Models Presented by: Debbie Welle Powell, MPA, Vice President Sisters of Charity Health System and Exempla Healthcare September 27 th, 2012
Poverty and Health. Frank Belmonte, D.O., MPH Vice President Pediatric Population Health and Care Modeling
 Poverty and Health Frank Belmonte, D.O., MPH Vice President Pediatric Population Health and Care Modeling An iconic image of child poverty Children Living in Poverty 4 Healthcare Services Account for $19.2
Poverty and Health Frank Belmonte, D.O., MPH Vice President Pediatric Population Health and Care Modeling An iconic image of child poverty Children Living in Poverty 4 Healthcare Services Account for $19.2
HSAG the QIN-QIO NHQCC II and CDI Initiative Kick-off
 (HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
(HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH The aim of this report is to provide NHS Borders Board with a thematic review of:-
 Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Westchester Medical Center PPS Project Advisory Committee. April 15, 2015 Via Webinar: 10:00 am 11:30 am
 Westchester Medical Center PPS Project Advisory Committee April 15, 2015 Via Webinar: 10:00 am 11:30 am Agenda Discussion Topic Welcome & Status Update Finalizing the Implementation Plan DSRIP Year 1:
Westchester Medical Center PPS Project Advisory Committee April 15, 2015 Via Webinar: 10:00 am 11:30 am Agenda Discussion Topic Welcome & Status Update Finalizing the Implementation Plan DSRIP Year 1:
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Combining Nursing Power and Quality Metrics to Influence Policy Development
 Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO.
 CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO. THE TEAM UTAH VALLEY HOSPITAL John Mitchell, MD January 16, 2016 Centers for Medicare and Medicaid Services Federally funded inpatient
CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO. THE TEAM UTAH VALLEY HOSPITAL John Mitchell, MD January 16, 2016 Centers for Medicare and Medicaid Services Federally funded inpatient
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population