Embracing a Culture of Safety and Learning
|
|
|
- Dylan Peters
- 5 years ago
- Views:
Transcription

1 Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes
2 Outline Adverse Events (AEs) Understanding Adverse Events Reason s Person vs System ( swiss cheese ) model Creating a Culture of Safety Safety Policies Managing an Adverse Event

3 Adverse Events
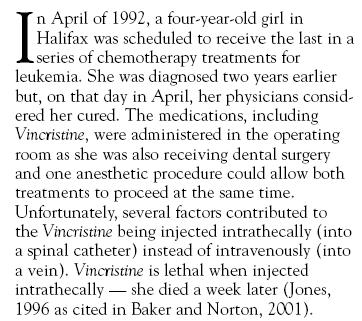
 Betsy s chemotherapy designed to be delivered over a 4 day protocol Instead she was given the protocol dose each day for 4 days Four fold overdose")
4 Adverse Events Dana Farber Cancer Institute Boston MA 1995 Betsy Lehman, young mother of three Healthcare reporter for the Boston Globe Undergoing experimental chemotherapy regimen for breast cancer One of the agents cardiotoxicity (dose dependent) Betsy s chemotherapy designed to be delivered over a 4 day protocol Instead she was given the protocol dose each day for 4 days Four fold overdose She died suddenly five days later of cardiac failure One other patient same overdose intensive care Error was not detected for 2 months

5 Adverse Events
6 Jim Conway Transforming an organization

7 Patient Safety Issue is not new Not unique to Calgary To Err is Human 1999 Canadian Adverse Events Study % of hospitalized patients 2.8% - preventable 6 to 7 extra days in hospital 1.6% of patients died and had an adverse event
8 Understanding Adverse Events Why do bad things happen? Designing Safer Systems Managing Adverse Events Patients / Families Healthcare Providers Stakeholders the people the healthcare system serves

9 Understanding Adverse Events
10 Two Models Why do bad things happen? 1. Person Model 2. System Model James Reason, Managing the Risks of Organizational Accidents, 1997
11 Why bad things happen A better explanation Man - a creature made at the end of the week when God was tired. Mark Twain
12 Person Model
13 The pweor of the hmuan mnid Aoccdrnig to a rscheearch at Cmabrigde Uinervtisy,, it deosn't mttaer in what oredr the ltteers in a wrod are. The olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae.. The rset can be a total mses and you can sitll raed it wouthit porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef,, but the wrod as a wlohe. Amzanig huh?
14 Approximations of system performance and potential performance Nominal error rates developed by specialists in human factors Activity* Probability of human error General error of commission for example, misreading a label General error of omission in the absence of reminders 0.01 General error of omission when items are embedded in a procedure for example, cash card is returned from cash machine before money is dispensed Simple arithmetic errors with self checking but without repeating the calculation 0.03 on another sheet of paper Monitor or inspector fails to recognise an error 0.1 Staff on different shifts fail to check hardware condition unless required by 0.1 checklist or written directive General error rate given very high stress levels where dangerous activities 0.25 are occurring rapidly Thomas W Nolan BMJ 2000;320: * Unless otherwise indicated, assumes the activities are performed under no undue time pressures or stress.

15 Avoid the Error Myth That Bad People Make Bad Errors!


16 Person Model Reaction SHAME & BLAME


17 Person Model Reaction BLAME & PUNISH
18 Two Models Why do bad things happen? 1. Person Model 2. System Model James Reason, Managing the Risks of Organizational Accidents, 1997
19 James Reason Why bad things happen

20 System Model
21 Understanding adverse events Causes Investigation
22 Unsafe Acts Errors Non-Compliance (Violations) Willful Intent to Harm (Sabotage) Errors do occur (all the time) Easiest cause to see Easiest cause to deal with Punishing people for committing errors does not lead to a safer system (probably the opposite)

23 Look alike packaging

24 Look alike labeling
25 System Model (#2) Safety Should be Engineered into the System Human Errors Poor Human Engineering Failure to Design Systems According to Cognitive Strengths / Weaknesses of Front-Line Workers Making a safer system Redesign Systems Make it Hard to Make Mistakes Reminders Alerts Forcing Functions Continual process improvement Measure Key Process Indicators James Reason, Managing the Risks of Organizational Accidents, 1997

26 System Design Every system is perfectly designed to achieve the results that it gets. Don Berwick
27 Patient Safety Strategy Creating a Culture of Safety


28 Patient Safety Strategy PATIENT SAFETY Provider Error Safety Culture High Reliability Human Factors System Factors


29 Why a focus on culture? I came to see, in my time at IBM, that culture isn't just one aspect of the game; it is the game. Lou Gerstner Jr. Chairman & CEO (Retired )

30 National Quality Forum

31 Top Five NQF 30 Safe Practices *

32 Making Healthcare Systems Safer Organizational Safety Culture J Reason & A Hobbs. Managing Maintenance Error. 2003
33 Making Healthcare Systems Safer HAZARD IDENTIFICATION ANALYSIS RECOMMENDATIONS PERFORMANCE MEASUREMENT EVALUATION RESEARCH SYSTEM IMPROVEMENT STRATEGIES / DESIGN TESTING IMPLEMENTATION
34 Safety Policies a Contract Between the Region / Providers AND Patients DISCLOSURE (Harm) Between Providers AND the Region REPORTING (Hazards / Close Calls / Harm) Between the Region AND its Providers JUST & TRUSTING Between the Region AND its Principal Healthcare Partners / Stakeholders INFORMING
35 Safety Policies
36 Just & Trusting Culture Two types of Evaluations (Separate) Safety Analysis Focus on systems Structured analytical approach ( RCA like ) Administrative Review Evaluates the actions of healthcare providers Roles, responsibilities, competencies In the context of the safety evaluation
37 Errors Just & Trusting Culture Region s Response to Provider s Actions The failure of a planned action to be completed as intended The Region will not discipline Non-compliance Deviations from established policies / standards The Region will evaluate the appropriateness of i) the policies & standards and ii) the circumstances leading to the non-compliance Willful Intent to Harm The Region will not tolerate disciplinary action will be taken & criminal investigations may result









38 Reporting where is the focus?

39 WHO Reporting Systems
40 Reporting - Key Concepts Focus is on LEARNING Safety Hazards (Hazardous situations) not Incidents or Errors Safety Learning Reports not Incident Reports

41 Safety Learning Reporting System March 11, 2008 Focus Hazards Close Calls Adverse Events Confidential Easy to use Each report is reviewed Status of reports can be tracked

42 Safety Learning Reporting System

43 Disclosure a risky business?
44 Disclosure Policy The Disclosure Process includes: 1.Acknowledging the harm to the patient 2.Providing an apology for the harm 3.Disclosing factual information about how the harm occurred
45 Level of harm Disclosure Policy Determines who will be involved in disclosure Coordination / communication vital Discretion For close calls (nearly harmed) Support for Health Partners For patients and their families For staff, physicians, health professionals involved
46 Managing Risks to: Managing Adverse Events Patients / Families Other Patients Healthcare Providers The Organization (reputation)



































47 Managing Adverse Events Adverse Event
48 Managing Serious* (Potential) Adverse Events SERIOUS* (POTENTIAL) ADVERSE EVENT IMMEDIATE MANAGEMENT RESPOND Resuscitate patient Ensure environment safe Secure equipment Protect other patients Offer initial support Notify Disclosure (Acknowledgment) Clinical Safety Evaluation Initial Timeline INITIAL ASSESSMENT CONTINUING MANAGEMENT ADVOCATE COMMUNICATE EVALUATE ASSIGN A PATIENT ADVOCATE DISCLOSURE TO PATIENT & FAMILY SAFETY ANALYSIS ONGOING SUPPORT FOR PATIENT & FAMILY SAFETY LEARNING REPORT ADMINISTRATIVE REVIEW ONGOING SUPPORT FOR HEALTHCARE PROVIDERS INFORMING * Serious Fatal or Severe (loss of limb or organ function or resuscitation required to sustain life) or substantial risk thereof (close call)
49 Person or System Model?
50 Managing Adverse Events Informing Sending a Strong Message of Transparency Opening the Possibility for Healing
51 Managing Serious* (Potential) Adverse Events SERIOUS* (POTENTIAL) ADVERSE EVENT IMMEDIATE MANAGEMENT RESPOND Resuscitate patient Ensure environment safe Secure equipment Protect other patients Offer initial support Notify Disclosure (Acknowledgment) Clinical Safety Evaluation Initial Timeline INITIAL ASSESSMENT CONTINUING MANAGEMENT ADVOCATE COMMUNICATE EVALUATE ASSIGN A PATIENT ADVOCATE DISCLOSURE TO PATIENT & FAMILY SAFETY ANALYSIS ONGOING SUPPORT FOR PATIENT & FAMILY SAFETY LEARNING REPORT ADMINISTRATIVE REVIEW ONGOING SUPPORT FOR HEALTHCARE PROVIDERS INFORMING * Serious Fatal or Severe (loss of limb or organ function or resuscitation required to sustain life) or substantial risk thereof (close call)
52

53


54 We learned..... to listen and speak publicly with more families
55 Public Forum October 2005 Canadian Healthcare Safety Symposium Halifax 5




56 A healing journey for individuals
57 A healing journey as a group Patient / Family Safety Council 13 patients / family members & Regional support






















58 Trust / Transparency Safety Agencies Healthcare Organizations Public Regional HC Providers
Human Factor and Patient Safety. Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA)
") Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Applying Human Factors to Healthcare Systems Safety
 April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation
 TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
Medication Safety: Lessons Learned
 Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
Systems Thinking & Human Factors Engineering in Healthcare
 Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
What s the data telling you? Using evidence-based stories for health planning and decision-making
 MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
2017 Pharmacy Education Series
 2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
Care of the Caregiver STARTS and ENDS with full leadership support and involvement!
 Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Provincial Forum on Adverse Health Events: Summary of Proceedings
 Provincial Forum on Adverse Health Events: Summary of Proceedings May 26, 2008 The Fairmont Newfoundland Prepared by: Loretta Chard-Kean 267 Task Force on Adverse Health Events Background Documents Volume
Provincial Forum on Adverse Health Events: Summary of Proceedings May 26, 2008 The Fairmont Newfoundland Prepared by: Loretta Chard-Kean 267 Task Force on Adverse Health Events Background Documents Volume
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE. FBI/UCR Report of Officers Killed and Assaulted. Officers Killed and Assaulted
 Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
Training. Agenda. Date / Tim Location: The Birc. Responsible. Action Plan. 5 Members Update. 6 Grant. Update 9 CECA. Kevin Bennett (Chairman)
") Training & Developmentt Forum Date / Tim Location: The Birc Agenda me: Wednesday 24 th May at 10.30am ches Conference Centre, National N Construction College, Bircham Newton, Kings Lynn, Norfolk Refreshments
Training & Developmentt Forum Date / Tim Location: The Birc Agenda me: Wednesday 24 th May at 10.30am ches Conference Centre, National N Construction College, Bircham Newton, Kings Lynn, Norfolk Refreshments
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Disclosures. Medication Incident. Objectives 4/23/2015. No conflicts to disclose
 Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Disclosure of Adverse Patient Safety Events and Harm Kitty Grant Beth Kiley Risk Management/ Patient Safety Consultants Performance Excellence
 Disclosure of Adverse Patient Safety Events and Harm Kitty Grant Beth Kiley Risk Management/ Patient Safety Consultants Performance Excellence Definitions: Adverse Patient Safety Event: A patient safety
Disclosure of Adverse Patient Safety Events and Harm Kitty Grant Beth Kiley Risk Management/ Patient Safety Consultants Performance Excellence Definitions: Adverse Patient Safety Event: A patient safety
Building a Just Culture
 Approved by: Building a Just Culture President and Chief Executive Officer Corporate Policy & Procedures Manual Policy No. III-35 Date Approved September 13, 2011 Next Review October 2014 Purpose The purpose
Approved by: Building a Just Culture President and Chief Executive Officer Corporate Policy & Procedures Manual Policy No. III-35 Date Approved September 13, 2011 Next Review October 2014 Purpose The purpose
Response to a Medication Error Tragedy and the Development of a Patient Safety Program. Dana-Farber Cancer Institute
 Response to a Medication Error Tragedy and the Development of a Patient Safety Program Dana-Farber Cancer Institute Institute of Medicine December 2010 Lawrence N Shulman, MD Chief Medical Officer and
Response to a Medication Error Tragedy and the Development of a Patient Safety Program Dana-Farber Cancer Institute Institute of Medicine December 2010 Lawrence N Shulman, MD Chief Medical Officer and
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016
 Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
National Agenda for Action: Patients and Families in Patient Safety Nothing About Me, Without Me *
 The National Patient Safety Foundation National Agenda for Action: Patients and Families in Patient Safety Nothing About Me, Without Me * Executive Summary This summary (and complete document) is a report
The National Patient Safety Foundation National Agenda for Action: Patients and Families in Patient Safety Nothing About Me, Without Me * Executive Summary This summary (and complete document) is a report
Critical Incident Reporting
 Critical Incident Reporting Sven Staender, MD Chairman EBA/ESA Task Force Patient Safety Department of Anaesthesia and Intensive Care, Regional Hospital, Maennedorf/ Zuerich, Switzerland; s.staender@spitalmaennedorf.ch
Critical Incident Reporting Sven Staender, MD Chairman EBA/ESA Task Force Patient Safety Department of Anaesthesia and Intensive Care, Regional Hospital, Maennedorf/ Zuerich, Switzerland; s.staender@spitalmaennedorf.ch
Hallmarks of Patient Safety and Quality Improvement Programs in Pharmacy Practice
 Hallmarks of Patient Safety and Quality Improvement Programs in Pharmacy Practice Jordan T. Daniel, PharmD Wednesday, May 10, 2017 Kimberly McDonough Spring Seminar Rhode Island Pharmacy Foundation Disclosure
Hallmarks of Patient Safety and Quality Improvement Programs in Pharmacy Practice Jordan T. Daniel, PharmD Wednesday, May 10, 2017 Kimberly McDonough Spring Seminar Rhode Island Pharmacy Foundation Disclosure
Innovative Techniques for Residents to Improve Safety
 Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
Reducing Risk: Mental health team discussion framework May Contents
 Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital
 Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital A report commissioned by the Vancouver Island Health Authority The System Review of
Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital A report commissioned by the Vancouver Island Health Authority The System Review of
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Creating a Highly Reliable Health System: the Leadership Challenge. 6 th Annual Patient Safety Symposium Rick Foster, MD
 Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
SPE III: Pharmacy 403W Preceptor s Evaluation of Student
 SPE III: Pharmacy 403W Preceptor s Evaluation of Student School of Pharmacy Student: Site: Preceptor: As a preceptor, you play a vital role in the education of our students and in assessing their competency
SPE III: Pharmacy 403W Preceptor s Evaluation of Student School of Pharmacy Student: Site: Preceptor: As a preceptor, you play a vital role in the education of our students and in assessing their competency
WHAT HAVE WE MISSED IN ACHIEVING SAFER HEALTHCARE??
 BMJ-IHI International Healthcare Forum, Singapore September 27-28, 2016 WHAT HAVE WE MISSED IN ACHIEVING SAFER HEALTHCARE?? Dr. / Akhil Sangal CEO Indian Confederation for Healthcare Accreditation Dr.
BMJ-IHI International Healthcare Forum, Singapore September 27-28, 2016 WHAT HAVE WE MISSED IN ACHIEVING SAFER HEALTHCARE?? Dr. / Akhil Sangal CEO Indian Confederation for Healthcare Accreditation Dr.
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
1875 Connecticut Ave. NW / Suite 650 / Washington, D.C / / fax /
 Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Understanding the Causes of Events. Objectives
 Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
SPE IV: Pharmacy 500X Preceptor s Evaluation of Student 2018
 School of Pharmacy SPE IV: Pharmacy 500X Preceptor s Evaluation of Student 2018 Student: Site: Preceptor: Rotation: First Second As a preceptor, you play a vital role in the education of our students and
School of Pharmacy SPE IV: Pharmacy 500X Preceptor s Evaluation of Student 2018 Student: Site: Preceptor: Rotation: First Second As a preceptor, you play a vital role in the education of our students and
How can the labelling and the packaging of drugs impact on drug safety? Prof. Pascal BONNABRY. Head of pharmacy. Swissmedic, Bern, June 19, 2007
 How can the labelling and the packaging of drugs impact on drug safety? Head of pharmacy Swissmedic, To err is human (USA) Serious adverse events in 3% [2.9-3.7%] of hospitalizations 10% [8.8-13.6%] of
How can the labelling and the packaging of drugs impact on drug safety? Head of pharmacy Swissmedic, To err is human (USA) Serious adverse events in 3% [2.9-3.7%] of hospitalizations 10% [8.8-13.6%] of
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1
 FORUM FOR EXCHANGE OF INFORMATION ON ENFORCEMENT Adopted at the 9 th meeting of the Forum on 1-3 March 2011 MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1 MARCH 2011 1 First edition adopted at the 6
FORUM FOR EXCHANGE OF INFORMATION ON ENFORCEMENT Adopted at the 9 th meeting of the Forum on 1-3 March 2011 MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1 MARCH 2011 1 First edition adopted at the 6
Department of Defense INSTRUCTION. SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP)
 Patient Safety Program (PSP) (MHSPSP)") Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Various Views on Adverse Events: a collection of definitions.
 Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Disclosure of Adverse Events and Medical Errors. Albert W. Wu, MD, MPH
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Human Factors Engineering in Health Care. Awatef O. Ergai, PhD Post-Doctoral Research Associate Healthcare Systems Engineering Institute
 Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Translational Safety Through Immersive Learning: Practice What you Preach
 Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
Running head: MEDICATION ERRORS 1. Medications Errors and Their Impact on Nurses. Kristi R. Rittenhouse. Kent State University College of Nursing
 Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant
 Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Understanding the High Reliability Organization and Why It's Important to Your Lab
 Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals
 Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
POLICY & PROCEDURE FOR INCIDENT REPORTING
 POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
Patient Safety Incident Report Form
 Page 1 This form is not meant to be a substitute to the health region s incident reporting. The purpose of this form is to assist with the identification and management of adverse events and near misses;
Page 1 This form is not meant to be a substitute to the health region s incident reporting. The purpose of this form is to assist with the identification and management of adverse events and near misses;
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
Patient Safety Case Study. Clara K. Terral. Angelo State University
 Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Compliance Program Updated August 2017
 Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Competition Guidelines Competition Overview Artificial Intelligence Grand Challenges
 IBM WATSON ARTIFICIAL INTELLIGENCE XPRIZE COMPETITION GUIDELINES Version 3 January 4, 2018 THE IBM WATSON AI XPRIZE IS GOVERNED BY THESE COMPETITION GUIDELINES. PLEASE SEND QUESTIONS TO ai@xprize.org AND
IBM WATSON ARTIFICIAL INTELLIGENCE XPRIZE COMPETITION GUIDELINES Version 3 January 4, 2018 THE IBM WATSON AI XPRIZE IS GOVERNED BY THESE COMPETITION GUIDELINES. PLEASE SEND QUESTIONS TO ai@xprize.org AND
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Standard Approaches to Adverse Event Reporting. Jonathan Deutsch, M.D.
 Standard Approaches to Adverse Event Reporting Jonathan Deutsch, M.D. 1 DISCLAIMER The opinions contained in this presentation are those of the presenter and do not necessarily reflect those of BMS 2 Scope
Standard Approaches to Adverse Event Reporting Jonathan Deutsch, M.D. 1 DISCLAIMER The opinions contained in this presentation are those of the presenter and do not necessarily reflect those of BMS 2 Scope
Incident Reporting Systems and Future Strategies for Patient Safety Improvement
 WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Zukunftsperspektiven der Qualitatssicherung in Deutschland
 Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Re-Engineering Medication Processes to Capitalize on Technology. Jane Englebright, PhD, RN Vice President, Quality HCA
 Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Patient Risk (Safety) in Radiation Therapy
 in Radiation Therapy") Patient Risk (Safety) in Radiation Therapy Michael G. Herman, Ph.D. Professor and Chair, Medical Physics Mayo Clinic Patient Safety 10/18/11 Herman # 1 Outline Radiation Therapy What Can/Did Happen? Is
Patient Risk (Safety) in Radiation Therapy Michael G. Herman, Ph.D. Professor and Chair, Medical Physics Mayo Clinic Patient Safety 10/18/11 Herman # 1 Outline Radiation Therapy What Can/Did Happen? Is
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS
 PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
Using a SYSTEMS APPROACH to address patient safety a case of MEDICATION ERROR.
 Using a SYSTEMS APPROACH to address patient safety a case of MEDICATION ERROR. By: George Kumi Kyeremeh. Director Nursing & Midwifery. Ghana. Presenter: Josephine Kyei BA NURSING,MPHIL HEALTH SER ADM FWACN
Using a SYSTEMS APPROACH to address patient safety a case of MEDICATION ERROR. By: George Kumi Kyeremeh. Director Nursing & Midwifery. Ghana. Presenter: Josephine Kyei BA NURSING,MPHIL HEALTH SER ADM FWACN
Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI
 Reflections: Ten Months and Where to From Here Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI 1 Presentation Overview Nature of the Problem Safer Healthcare Now Campaign Systems vs.
Reflections: Ten Months and Where to From Here Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI 1 Presentation Overview Nature of the Problem Safer Healthcare Now Campaign Systems vs.
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS
 APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
Sharps Safety Awareness
 Sharps Safety Awareness American University of Beirut 14 June 2013 Role of JCI to Improve Safety Culture and Quality of Health Care in the Middle East Khalil Rizk, BSN, MPH, MA, CPHQ JCI Consultant 0 What
Sharps Safety Awareness American University of Beirut 14 June 2013 Role of JCI to Improve Safety Culture and Quality of Health Care in the Middle East Khalil Rizk, BSN, MPH, MA, CPHQ JCI Consultant 0 What
Guidelines for Disclosure Process. 1) Patient disclosure does not include:
 Patient disclosure does not include:") Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Sunnybrook Policy: Disclosure of Adverse Medical Events and Unanticipated Outcomes of Care
 Sunnybrook Policy: Disclosure of Adverse Medical Events and Unanticipated Outcomes of Care POLICY STATEMENT: It is Sunnybrook & Women's Policy, in keeping with our Mission, Vision, Values and philosophy
Sunnybrook Policy: Disclosure of Adverse Medical Events and Unanticipated Outcomes of Care POLICY STATEMENT: It is Sunnybrook & Women's Policy, in keeping with our Mission, Vision, Values and philosophy
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors
 Transparency & Accountability are Critical to Reducing Medical Errors") Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is