Working with trainees to turn quality improvement into scholarship and dissemination
|
|
|
- Annabella Morgan
- 5 years ago
- Views:
Transcription
1 Working with trainees to turn quality improvement into scholarship and dissemination James Moses, MD, MPH Chief Quality Officer, Boston Medical Center Academic Advisor, Institute for Healthcare Improvement s Open School
2 Objectives Describe the growing imperative of including GME trainees in efforts to improve patient care Provide attendees an organizing framework for engaging GME trainees in efforts to improve quality and patient safety at the point of care Review the process of publication and dissemination for trainee-led faculty mentored quality improvement initiatives


 in")
3 Background Houston, we have a problem And the 6 Quality Aims are? Deeper alignment of engaging GME learners (residents and fellows) in Quality and Patient Safety
4 Educational reform has led to the direct assimilation of Quality and Patient Safety competencies into Medical Education at all levels Undergraduate Medical Education LCME requirements now include Quality and Safety, Interprofessional competencies Graduate Medical Education ACGME Outcomes Project Continuing Medical Education and Board Certification Maintenance of Certification-Part IV
5 Educational reform has led to the direct assimilation of Quality and Patient Safety competencies into Medical Education at all levels Undergraduate Medical Education LCME requirements now include Quality and Safety, Interprofessional competencies Graduate Medical Education ACGME Outcomes Project Continuing Medical Education and Board Certification Maintenance of Certification-Part IV
6 ACGME Outcomes Project: The Good and the Bad Better doctors Improved Quality and Safety Competency Domains Improved Educational Outcomes Creation of QI as requirement (PBLI and SBP) Last decade: Key Quality and Patient Safety Attributes Focus on getting residents to be better providers (PBLI>SBP) and Keeping patients safe duty hours


7 CLER: A New ACGME Focus Lack of clear patient outcomes related to GME Meaningful engagement of GME learners in Quality and Patient Safety in institutions across the country is lacking To move away from over emphasis on duty hours and ACGME s role as educational police Instead: ACGME as driver of fostering the right environment for institutions to more centrally engage and involve GME learners in their Quality and Patient Safety priorities
8 Focus Area: Patient Safety Preliminary Analyses, January Patient Safety Events (Housestaff ARS) Experienced event (%) Experienced and Reported through system (%) All PGY PGY PGY PGY For those Clinical Learning Environments where information was available: A median of 1.2% of patient safety events were reported by residents ( ~60% CLEs did not or could not track) Based on interviews with nurses and other clinical staff, residents infrequently report events; it was not unusual that the CLE s system was used to report on individual behaviors DRAFT January 31, 2015, copyrighted ACGME Do Not Cite or Reproduce

9 Shift in the healthcare landscape is necessitating a change in our approach to training To ensure that the healthcare workforce has the necessary knowledge and skills And seeing the trainees, in their role at the point of care, as actual drivers of health care quality

10 Moving beyond CLER-ACGME Common Requirements 2017
11 Is ACGME Right? Should Housestaff play a key role in Quality & Safety?
12 Benefits to both the training institution and to the housestaff Training Institution Frontline staff involvement and input into solutions Housestaff become faculty Housestaff engagement QPS culture Trainee QPS as an institutional priority QPS as part of every day work(identity) in taking care of patients Learn skills of QPS improvement work With Patient Outcomes as the True North trainee integration becomes necessity
13 GME Learners as Key Stakeholders Opportunity to create change Delivery of Patient Care Fellows and Residents Faculty Department/Division Chiefs CMO/Physician-In-Chief CEO Board MD Power Structure Board CEO CMO/Physician-In-Chief Department/Division Chiefs Faculty Fellows and Residents
14 Addressing current state gaps means addressing historical norms in the training environment Resident/fellows as transitory Trainee QI efforts not linked to system priorities Input as frontline staff not incorporated into hospital QI efforts Care improvement occurs in organizations despite housestaff as opposed to because of housestaff
15 A foundational paradigm shift
16 Developing a Framework Workforce QI/PS Competence Inter- Professional Team-Based Care Hearing the Patients Voice Experience and Engagement Quality and Patient Safety Data on Performance GME Engagement and Activation Leadership Prioritization Culture of Patient Safety and Quality Improvement

17 Barriers to address Time Lack of role models Resource and support allocation Competing priorities
18 So how to best to integrate trainees into QPS activities? Moving from in vitro to in vivo experiential learning at the point of care
19 Three Different Models Getting QI to be facilitated by anyone, everywhere
20
21 Model 1: Short-term, Team-based Definition: Focused on behavior change and/or process change within control of interdisciplinary medical team Scenario: Inpatient team spends 2-4 weeks together, integrating QI/PS into daily clinical care routines Improvement Objective: To solve a proximal workflow issue or gap in care that a team identifies Educational Objective: Motivate trainees to incorporate improvement principles and systems based thinking into daily clinical routines versus thinking of QI/PS as separate activity Example: Team prioritizes ensuring that 100% of patients admitted to the service have a completed VTE Risk Assessment completed by admitting resident prior to initiation of DVT prophylaxis
22 Model 2: Medium-term, Unit-based Definition: Focused on a workflow in a particular unit or clinic with aims that are tied to institutional priorities Scenario: Trainees who rotate through an unit (or clinic) and work on a QI project developed by the unit (or clinic) Improvement Objective: To develop new practice or implement an evidencebased intervention for the unit or clinic Educational Objective: To demonstrate to the trainee that even with limited period of time spent in one particular unit, he or she can play a vital role in accelerating that unit s improvement initiatives Example: Trainees who have weekly continuity clinic, participate as part of the clinic s QI team working to improve flu vaccination rates
23 Model 3: Long-term, Systems-based Definition: Focused on a workflow(s) that crosses multiple units/clinics with an aim to improve systems at departmental/institutional level Scenario: Trainees who join a hospital taskforce related to improving a corporate quality goal prioritize ensuring interventions are adopted locally as they rotate through a unit (or clinic) Improvement Objective: To make system-level change that helps achieve institutional QI/PS objectives Educational Objective: To integrate trainees into a larger institutional objectives for quality and safety; to make robust connections between clinical care at the bedside and institutional quality and safety aims Example: Trainees on a hospital readmissions taskforce join multidisciplinary rounds when on an inpatient rotation to ensure all patients have follow-up with PCP scheduled by the unit coordinator within 2 weeks of discharge
24 Selecting a Model Intentionally flexible Factors to consider from faculty perspective: Role in GME education Location within the QPS infrastructure of the institution Comfort with QPS principles and practice Factors to consider from a trainee perspective: Current QPS knowledge, skills and behaviors Motivation and time availability Interest in QPS as potential career
25 Putting the 3 Different Models to Action Sharing of Best Practice Examples #IHI27FORUM
26 Model 1 Short-term, Team-based #IHI27FORUM

27
28 Aim & approach Teach trainees how to improve (and how not to hate QI) What could we improve in 2 weeks? Team-based approach Start with a question: What s something you think we can do better? And then wait

29 What Christine told me
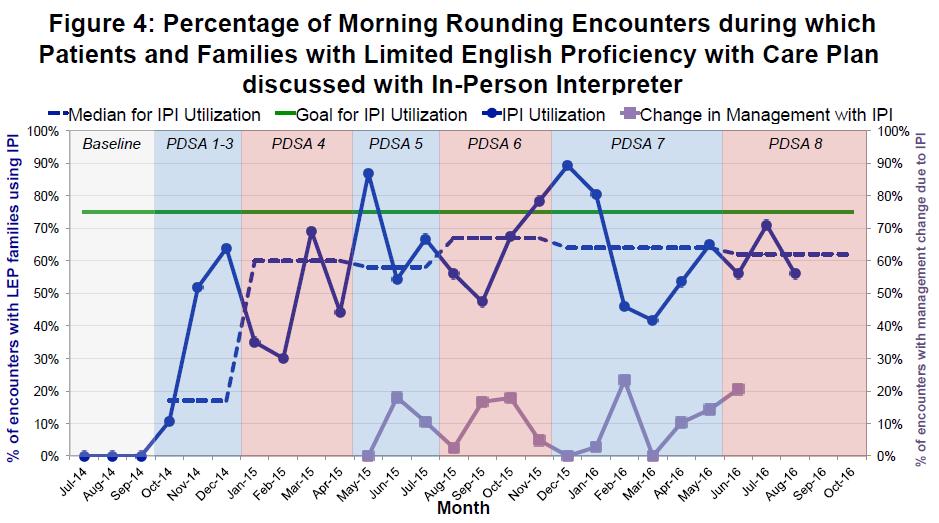
30 Simple measurement So, I asked how many of our patients needed interpreters? Our Day 2 measure: Total # patients not English Speaking Data collection plan: MS III to note from morning signout patients not English Proficient Plot number on workroom whiteboard Our Day 4 measure (final measure): Interpreters used on rounds/# of LEP patients
31 What changes did we make? Supervisor communicated with night team to capture language preference and communicate in morning signout Supervisor have ward assistant call for interpreters for rounds Created form for tracking to be used by MSIII Realized we should reach out to interpreter office and see if ok with to ensure interpreter involvement on rounds Ensure LEP patients prioritized due to interpreter arrival
32 What I didn t do Teach the Model for Improvement, PDSA, run charts, variation analysis, systems thinking Mention Juran, Deming or Shewhart Use acronyms Work on an abstract idea Work on something they didn t feel was important
33 Your role: Before rounds: 1) Fill out form for each non-english speaking patient on YOUR ROUNDING TEAM. 2) Make a copy of the form. 3) Give copy to unit coordinator (Pam) before 7:15am lecture. Hold onto original form. During rounds: 4) Complete starred (*) fields on original form. 5) At the end of rounds, write Huddle time, and give both team s completed sheets to Marjorie before huddles.
34 Hey Team! Another 10/10 on interpreter rounding forms! We really appreciate the work you've put into this project, and hope you know that your patients appreciate it too! Sometimes it's not easy to round in the room and schedule interpreters, but here are a few highlights from the surveys Lizzeth and I do on the floor weekly: "They all came in at once, talking about everything in front of me so I know what's going on." "I liked that it was a team, it was very interactive. There was opportunity to see different opinions and viewpoints. They were nice, concerned, and supportive." Way to go! Julio and Lizzeth
35 Model 2 Medium-term, Unit-based #IHI27FORUM

36 Residents take on CDI in our ICU C. diff rate higher than national average Routine infection control precautions are not always in place Hospital epidemiologist looking for pilot project #IHI27FORUM

37 ICU focused initiative Single unit, small 12-bed ICU Staff and leadership aware and on board Flexible scheduling No funding initially #IHI27FORUM
38 Aim Statement Improve adherence to basic infection control measures in the 9N ICU by 15% by January 31, #IHI27FORUM
39 Team membership Led by resident MS and SPH Students brought on board to track adherence Mentorship from hospital epidemiologist Collaboration with RN and MD leaders, unit RNs #IHI27FORUM

40 Measurement Healthcare workers observed with checklist Observations at irregular intervals given duty schedule Baseline data taken Process analyzed by traditional QI techniques #IHI27FORUM
41 Hand hygiene: Not so simple All healthcare workers had trouble adhering to basic hand hygiene & special precautions Multiple common failure points identified #IHI27FORUM

42 Solutions tested Install more hand sanitizer dispensers Create a campaign with infection control characters Make new alert signs featuring characters #IHI27FORUM

43 Resident Project $1,600 QI grant from Resident Union s BMC HS QI Council jointly supported by BMC s Malpractice Captive Work orders for new hand sanitizers Printed up signs and posters Measuring for change currently #IHI27FORUM
44 Resident Project Lessons learned Duty schedule often not compatible with project schedule Do project in manageable chunks Observations are more difficult than chart-based measurements Resident/student QI programs can work Trainees and students want to take leadership roles Unit based project Unit was engaged and interested in improvement Leadership comfortable with resident-run project Smaller is better; easier to make changes Less funding needed Unit-based pilots are the gateway to larger projects
45 Model 3 Long-term, Systems-based #IHI27FORUM


46 Housestaff Reporting Habits Residents experience errors But do not report them.
47 Objectives Increase physician (trainee and faculty) reporting of adverse events via Hospital-based taskforce with housestaff and faculty representatives Key intervention: Department specific didactic/discussion based STARS sessions
48 Participating Departments Psychiatry Orthopedics Medicine OB/GYN Emergency Department Surgery Pediatrics ENT Family Medicine Cardiology
49 Aim Statement Primary Drivers Secondary Drivers Change Strategies Knowing How To File a STARs Regular STARs related Educational Sessions Education on STARs Faculty Development Programming Knowing Why to File a STARs Increase by 50% the number of STARs filed by GME trainees across the organization per month Role Modeling by Faculty STARs Dashboard Belief that filing a STARs will improve care for patients Actions taken to effectively improve care and communicated back to GME Trainees Collection and reporting out of Action Steps taken by HS QI council and Risk Management Team Rewarding Environment for filing STARs by Trainees
50 # of STARS Reports STARS Incident Reporting Total Reported FY Total number of STARs filed continues to go up, demonstrating improved engagement by staff in raising awareness to safety issues across our clinical areas ` FY 2007 FY 2008 FY 2009 FY 2010 FY 2011 FY 2012 FY 2013 FY 2014
51 # STARS Filed STARS Incident Reporting Volume By Reporter Nursing continues to be group that files the most STARS but other staff are making meaningful contributions to the number of STARs filed as well Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month Resident Attending Nurse Pharmacy Other
 CY")
52 Though nursing makes up the majority of staff that file STARs, the total number of STARs filed by Attendings and Residents has risen steadily over the last year, largely as a result of a STARs initiative being lead by key faculty and the Housestaff Quality Improvement Council Stars Incident Reporting Attending/Resident (All Services) CY 2014
53 Conferences and Publications A Win-Win #IHI27FORUM
54 Can QI be published? Of course

55 SQUIRE Guidelines
56 Academic Products Opportunities Posters/Abstracts Local: Research Day/Quality Day Regional/National: Discipline specific society meetings, IHI, AHI, AAMC Integrating Quality Journals dedicated to QI American Journal of Medical Quality BMJ Quality and Safety Journal Journal of Healthcare Quality Joint Commission Journal on Quality and Safety Many major journals with dedicated quality forum NEJM/JAMA Society specific (Pediatrics, Hospital Medicine)

57 Where QI and Research Should Play Together
58 Why they need each other: QI Evolves interventions based on learning Fits into the local system Uses data over time to guide improvement Improvement realized is sustained intentionally in the system Does not control for confounding/bias Measures what is necessary for improvement (no controls) Data technique not intended for null hypothesis testing Research Controls for confounding/bias Formalizes hypothesis testing of differences between populations Interventions are decided apriori Adherence to intervention is formalized Does not allow for rapid improvement of an intervention Does not leverage data for learning purposes Heavy in resources/takes a long time Adherence to intervention only during study period
59



60
")


61 To create and support a culture of healthcare quality improvement (QI) engagement for BMC, the Boston HealthNet Community Health Centers and Boston University through accredited education, mentorship and administrative oversight.
62 Summary Changing landscape of medicine requires a change in the learning environment of trainees ACGME is calling for better integration and active participation of the trainees by hospital leaders in achieving meaningful quality and safety improvements for training institutions Lessons learned from CLER s initial round of site visits demonstrates a clear gap of where we are currently and where we need to get to at a national level Locally, many barriers exist in integrating trainees into Quality and Patient safety initiatives in a meaningful way Solutions do exist by integrating trainee improvement work at the point of care Which can be done in team based, unit based and system based efforts in which trainees play a central role to realizing improvement #IHI27FORUM
Engaging Learners Across Health Professions in Improving Care Together
 Session A17 / B17 These presenters have nothing to disclose Engaging Learners Across Health Professions in Improving Care Together Tuesday December 11, 2012 Objectives After this session, participants
Session A17 / B17 These presenters have nothing to disclose Engaging Learners Across Health Professions in Improving Care Together Tuesday December 11, 2012 Objectives After this session, participants
A Quiz. I am comfortable going to any healthcare provider or hospital in my city/town.
 A Quiz I am comfortable going to any healthcare provider or hospital anywhere in the country. I am comfortable going to any healthcare provider or hospital in my city/town. I am comfortable going to my
A Quiz I am comfortable going to any healthcare provider or hospital anywhere in the country. I am comfortable going to any healthcare provider or hospital in my city/town. I am comfortable going to my
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Northern Health - Acute Services. Evidence Based Practice Venous Thromboembolism Prevention
 Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound)
") Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Telligen. Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016
 Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Telligen Making BIG Changes Attainable with Affinity Group Outreach June 3, 2016 1 Telligen QIN-QIO 2 For today Assess the landscape Evaluate how your projects align with affinity group interests Tell
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Improving Children s Health Together
 Improving Children s Health Together Improvement is our business. Committed professionals and organizations across the U.S. are working hard every day to make it easier for children and families to live
Improving Children s Health Together Improvement is our business. Committed professionals and organizations across the U.S. are working hard every day to make it easier for children and families to live
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
The Digital ICU: Return On Innovation
 The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
A Comprehensive Framework for Patient Safety
 These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
The Clinical Learning Environment Review (CLER) Program. Background
 Program. Background") Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program November 2013 Background 2009-2010 ACGME Task Force Linked adherence to duty hours policies
Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program November 2013 Background 2009-2010 ACGME Task Force Linked adherence to duty hours policies
Imprinting Safety and Quality Practices on Residents and Fellows. John Szymusiak, MD Gregory M. Bump, MD
 Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
From Competition to Collaboration: Aligning institutions to improve quality
 From Competition to Collaboration: Aligning institutions to improve quality Meghan M Walsh MD MPH Hennepin County Medical Center Minneapolis, MN October 13, 2015 Disclosures None Objectives Recognize the
From Competition to Collaboration: Aligning institutions to improve quality Meghan M Walsh MD MPH Hennepin County Medical Center Minneapolis, MN October 13, 2015 Disclosures None Objectives Recognize the
Criteria Led Discharge Pilot NHS Ayrshire and Arran Lorna Loudon, Linsey Stobo, Fraser Doris Implementing CLD in Scotland
 Criteria Led Discharge Pilot NHS Ayrshire and Arran Lorna Loudon, Linsey Stobo, Fraser Doris Implementing CLD in Scotland 18.3.15 Whole System Patient Flow Improvement Programme 1 Background Project Team
Criteria Led Discharge Pilot NHS Ayrshire and Arran Lorna Loudon, Linsey Stobo, Fraser Doris Implementing CLD in Scotland 18.3.15 Whole System Patient Flow Improvement Programme 1 Background Project Team
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
Case: Comparing Two Scenarios
 The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
A Blueprint for Alignment
 A Blueprint for Alignment Engaging Residents in the Quality and Safety Mission of Penn Medicine PJ Brennan, MD Chief Medical Officer, UPHS Jennifer S. Myers, MD Director of Quality and Safety Education
A Blueprint for Alignment Engaging Residents in the Quality and Safety Mission of Penn Medicine PJ Brennan, MD Chief Medical Officer, UPHS Jennifer S. Myers, MD Director of Quality and Safety Education
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO
 Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Multi disciplinary Team Communication and Effective Handoffs
 Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment
 Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
COMBINED INTERNAL MEDICINE & PEDIATRICS Department of Medicine, Department of Pediatrics SCOPE OF PRACTICE PGY-1 PGY-4
 Definition and Scope of Specialty The Internal Medicine/Pediatrics residency program is a voluntary component in the continuum of the educational process of physician training; such training may take place
Definition and Scope of Specialty The Internal Medicine/Pediatrics residency program is a voluntary component in the continuum of the educational process of physician training; such training may take place
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
COMMITTEE REPORTS TO THE BOARD
 Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Preventing Health Care Associated Infections. PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011.
 Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Surgical Critical Care Sub I
 Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
OHSU SoM UME Competencies YourMD
 Preamble: In August, 2014, Oregon Health & Science University (OHSU) School of Medicine (SoM) launched a new curriculum for its entering medical school class. This curriculum transformation was the result
Preamble: In August, 2014, Oregon Health & Science University (OHSU) School of Medicine (SoM) launched a new curriculum for its entering medical school class. This curriculum transformation was the result
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
The Clinical Learning Environment Review (CLER) Program Update
 Program Update") Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program Update October 10, 2013 Updates CLER program development Early observations CLER Evaluation
Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program Update October 10, 2013 Updates CLER program development Early observations CLER Evaluation
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Reducing opioid-related harm and building quality improvement capability in New Zealand: a national formative collaborative
 Session Code: M3 The presenters have nothing to disclose Reducing opioid-related harm and building quality improvement capability in New Zealand: a national formative collaborative John Kristiansen Prem
Session Code: M3 The presenters have nothing to disclose Reducing opioid-related harm and building quality improvement capability in New Zealand: a national formative collaborative John Kristiansen Prem
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
From Implementation to Optimization: Moving Beyond Operations
 From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
CME Disclosure. Accreditation Statement. Designation of Credit. Disclosure Policy
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
Sutton Homes of Care Vanguard Programme
 Sutton Homes of Care Vanguard Programme An Innovative End of Life Care model for care homes Kings Fund Conference 6 th December 2016 Corinne Campion, Clinical Nurse Specialist, Supportive Care Home Team
Sutton Homes of Care Vanguard Programme An Innovative End of Life Care model for care homes Kings Fund Conference 6 th December 2016 Corinne Campion, Clinical Nurse Specialist, Supportive Care Home Team
Compliance Division Staff Report
 Compliance Division Staff Report Polygraph Advisory Board Meeting Tuesday, September 26, 2017 Public Outreach Compliance Division routinely attends annual industry meetings held by TALEPI (Texas Association
Compliance Division Staff Report Polygraph Advisory Board Meeting Tuesday, September 26, 2017 Public Outreach Compliance Division routinely attends annual industry meetings held by TALEPI (Texas Association
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Tina Nelson, MBA, BSN Lisa Stepp, BSN, RN Rebecca Fyffe, BSN, RN Jessica Coughenour, LPN
 Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Fall Prevention Program. St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer
 Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Ensuring quality outcomes
 Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Elaine Andrews, Assistant Director of Nursing & Safety and Caroline Booton Quality Analyst Jill Asbury, Acting Director of Nursing
 Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Report to: Board of Directors Date of Meeting: 26 th October 2016 Report Title: Inpatient Falls Report Status: Mark relevant box with X Prepared by: Executive Sponsor (presenting): For information x Discussion
Complexities & Progress in Graduate Medical Education
 Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
A Million Little Pieces: Developing a Controlled Substance Diversion Program. Tanya Y. Barnhart, PharmD, BCPS
 A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer,
 Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Decreasing Nosocomial C. diff
 Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Milestones Ready or not.here they come! SIU SOM March 6, 2013
 Milestones Ready or not.here they come! SIU SOM March 6, 2013 A Word of Thanks Donald Brady Susan Guralnick Justin Held Eric Holmboe Tom Nasca John Mellinger Julie Rhodes Jennifer Rodgers Hilary Sanfey
Milestones Ready or not.here they come! SIU SOM March 6, 2013 A Word of Thanks Donald Brady Susan Guralnick Justin Held Eric Holmboe Tom Nasca John Mellinger Julie Rhodes Jennifer Rodgers Hilary Sanfey
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Health Sciences North Horizon Santé-Nord (QIP) Quality Improvement Plan
 Quality Improvement Plan") Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
The Milestones provide a framework for the assessment
 The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year
 A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
of the respiratory checklist from July1, April 30, Measures were evaluated monthly. Primary measures:
 Surfactant Administration and Respiratory Care During the Golden Hour Adia Stokes MD, Bushra Saleem, MD, Melissa Oh, MD, Natalie Davis, MD and Sara Mola, MD University of Maryland Medical Center Primary
Surfactant Administration and Respiratory Care During the Golden Hour Adia Stokes MD, Bushra Saleem, MD, Melissa Oh, MD, Natalie Davis, MD and Sara Mola, MD University of Maryland Medical Center Primary
HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016
 HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016 Objectives: 1. Gain an in-depth understanding of four Core Leadership Competencies 2. Apply practical insights to developing
HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016 Objectives: 1. Gain an in-depth understanding of four Core Leadership Competencies 2. Apply practical insights to developing
Enhancing Patient Care through Effective and Efficient Nursing Documentation
 Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
TCLHIN Standardized Discharge Summary
 TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
Quality Improvement Plans (QIP): Progress Report for QIP
: Progress Report for QIP") Excellent Care for All Act Quality Improvement Plans (QIP): Progress Report for 2013-14 QIP This document uses the standard Health Quality Ontario (HQO) template for reporting on the progress as of April
Excellent Care for All Act Quality Improvement Plans (QIP): Progress Report for 2013-14 QIP This document uses the standard Health Quality Ontario (HQO) template for reporting on the progress as of April
3/24/2016. Value of Quality Management. Quality Management in Senior Housing: Back to the Basics. Objectives. Defining Quality
 Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH The aim of this report is to provide NHS Borders Board with a thematic review of:-
 Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
Appendix-15-35 Borders NHS Board PRESSURE ULCER THEMATIC ADVERSE EVENT REPORT - MARCH 15 Aim The aim of this report is to provide NHS Borders Board with a thematic review of:- Avoidable hospital developed
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
Patient Experience: Good to Great!
 Patient Experience: Good to Great! April, 2016 Angela Kramer & Nancy Burden FSASC Quality & Risk Management Conference April 2016 Renaissance Orlando at SeaWorld OBJECTIVES Upon completion of this presentation
Patient Experience: Good to Great! April, 2016 Angela Kramer & Nancy Burden FSASC Quality & Risk Management Conference April 2016 Renaissance Orlando at SeaWorld OBJECTIVES Upon completion of this presentation
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing August 2017 (July 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important