NoCVA HEN CAUTI Campaign Learning from Defects
|
|
|
- Ginger Wells
- 5 years ago
- Views:
Transcription
1 NoCVA HEN CAUTI Campaign Learning from Defects Shelby Lassiter, BSN, RN, CPHQ, CIC Kathy Steele, BSN, RN October 11, 2012
2 Polling Question 1 I am experienced in doing defect analyses (root cause analyses) and am confident analyzing CAUTI events to learn from individual events as well as several events in aggregate. TRUE FALSE
3 Polling Question 2 I know what CUSP is and am experienced in applying CUSP principles in my unit. TRUE FALSE
4 Objectives Participants will be able to: Define CUSP and list the five steps Define defect. Describe at least one concept about why defects occur. Describe the first step in analyzing a CAUTI as a defect. Define psychological safety and describe why it is important for a thorough defect analysis.
5 The Five Steps of CUSP 1. Educate on the Science of Safety 2. Identify defects (today) 3. Engage leadership (now and future) 4. Continue to learn from defects (today) 5. Teamwork and communication (now and future)
6 What is CUSP? Comprehensive Unit-based Safety Program Strategic framework for safety improvement that integrates communication, teamwork, and leadership to create and support a culture of patient safety that can prevent harms. It features: evidence-based safety practices, staff training tools, standards for consistently measuring harms (infection rates such as CLABSI), engagement of leadership, and, tools to improve teamwork among health care team members.

7 New CUSP Toolkit and Location «Now on AHRQ website «Added tools, resources such as videos cusptoolkit/

8 CUSP: Identifying and Learning from Defects Tap into the website tools to enhance your LfD process.
9 What is a Defect? Defect: Any clinical or operational event or situation that you would not want to happen again. May include events that you believe actually caused harm or put patients at risk for significant harm. Johns Hopkins s Learning from Defects tool from CUSP Toolkit at Accessed Oct 8, 2012.
10 Definitions Defect Analysis: -the process of analyzing a defect to determine its root cause. Defect Prevention: -the process of addressing root causes of defects to prevent their future occurrence. Lanier K. Experiences In Root Cause Analysis and Defect Prevention Methods. Presentation publically available at Accessed April 2010.
11 Basic steps in the L-from-D Process 1. What happened? 2. Why did it happen? 3. How will you reduce the likelihood of it happening again? 4. How will you know the risk is reduced? 5. With whom should you share the learning?
12 Why bother? Reimbursement systems are being reengineered to reward the best performers (no margin, no mission, no salary, no job ) Growing transparency of outcomes Defects are expensive in many ways Excellence in care provided - learning from each defect is the best way to prevent it from happening again The Golden Rule-it s what we d want done for us or the person we love most!
13 It s All About Prevention Learning from defects reduces the likelihood of event occurring again and causing harm. Learning may occur in two areas: o System design o Human behavior Using a tool to aid learning provides structure and consistency Learning from each CAUTI (or any type of harm) allows learning from common cause variations. Learning from defects that might contribute to CAUTIs (any type of harm) allows prevention further upstream from the harm to make care even safer.
14 Background Concept #1 Normalized deviance: (Workarounds, short-cuts) Long-term phenomenon in which individuals or teams repeatedly accept a lower standard of performance until that lower standard becomes the norm. I.e. what starts out as a deviation from SOP becomes routine practice and is normalized. It becomes acceptable and may no longer even be recognized as deviation. (Just Culture terms for this: behavioral drift, at-risk behavior) Allowed because we get away with it most of the time
15 A Famous Example: Challenger Tragedy NASA team accepted a lower standard of performance on solid rocket booster O-rings. Got comfortable with seeing occasional O-ring damage. By the time Challenger launched, O-ring damage was considered a marginal problem. In 1986, O-ring damage had become an accepted normalized deviance. On 1/28/86, Challenger exploded soon after take-off, killing all 7 crew members.
16 What are some common healthcare normalized deviances? Inconsistent hand hygiene practices. Not disinfecting aspiration ports on Foleys when obtaining specimens. Using the same container to empty urine collection bags in semi-private rooms. Hanging the Foley bag on the walker or gait belt when ambulating the patient or throwing it up on the stretcher during transport or hanging it from the side-rail. Diapering patients with diarrhea. What else?
17 Excuses to Deviate The rule(s) is stupid May not appear to have value Rule or reason for it is unknown Not valued New technology Complexity of work Rule does not apply to this patient Rule(s) doesn t apply to me I know a better way Healthcare worker is not the one at risk in most situations. Competing priorities: o Cost and time, o Culture (politics, hierarchy, lack of communication openness, etc.) It won t hurt anything this one time Assumed or minimal consequences.

18 Background Concept 2: Errors in Complex Systems
19 Active Failures Active failures: errors that occur at the point of contact between a human and some aspect of a larger system (e.g., a humanmachine interface). They are generally readily apparent (e.g., pushing an incorrect button, not securing a Foley) and almost always involve someone at the frontline or sharp end.
20 Latent Failures Latent Failures: less apparent failures of organization or design that contribute to the occurrence of errors or allowed them to cause harm to patients. Occurrences are at the blunt end but may result in active failures on the sharp end. AKA: Accidents waiting to happen. Reason JT. Human Error. New York, NY: Cambridge University Press; 1990.

21 Swiss Cheese Model
22 Background Concept 3: Analysis of a defect should occur as soon as possible after the defect is recognized. The best light is often that from a burning bridge. ~Don Henley
23 A Review: The 5 Steps in the LfD Process 1. What happened? 2. Why did it happen? 3. How will you reduce the likelihood of it happening again? 4. How will you know the risk is reduced? 5. With whom should you share the learning?
24 Tips For HAI LfDs It is rare to find the exact source in a nonoutbreak-related infection. HAIs are usually the culmination of many infection prevention breaches. (More than one hole lined up in the Swiss cheese ) Your job in a defect analysis is to search for the contributing factors that were most likely to have culminated in the infection in this particular patient.

25 Learn about the organism and how it s typically transmitted, if there has been an organism identified. Tap into your Infection Preventionist to help the group process through the chain of infection to help in search for contributing factors. Tip for HAIs
26 Need to learn: What is organism? Is this particular organism a MDRO? Where is it commonly found in nature? How is it transmitted? How common is it in your organization? How long can it live in the environment?
27 Step 1: What Happened? Use a standard event investigation format. No perfect form so use what is familiar and accepted that accomplishes the goal. Must establish a chronological order of events and data related to the event. Usually requires some research and walking the process. The same person should not do all the research/walking the process. Include assessment for active and latent failures.
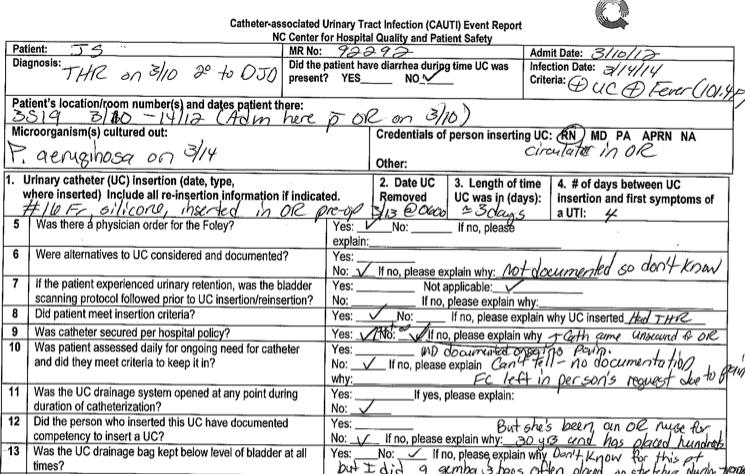
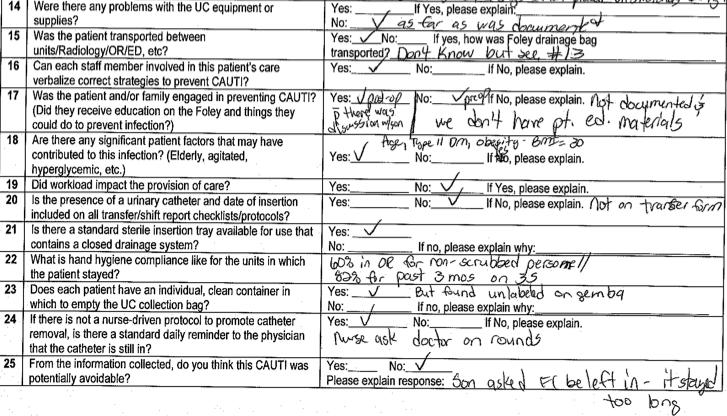
28 Case Study Jerri, a 72 yo female was admitted for THR on 3/10/11. A #16 Fr. Foley was placed in OR just before surgery. On 3/10 post-op, she experienced quite a bit of pain but was otherwise stable. Foley was due to come out on a.m. of 3/11, but her son requested it be left in to avoid having her get up to go to the BR. The Foley remained in until 3/13 a.m. On 3/14, the patient spiked a fever to F and was pancultured. UA was + for LE, nitrites, and 4+ bacteria in a cathed specimen. All cultures were negative except for urine, which grew out >100,000 CFU of Pseudomonas aeruginosa. CXR was negative.
29 Pseudomonas aeruginosa Gram negative rod. Commonly found in soil and water. Is frequently found on surfaces of plants and occasionally on animals. Favors moist environments and is often found in biofilm in faucets and sink drains. Opportunistic pathogen in humans: it exploits some type of break in host defenses to infect and rarely causes infection in healthy humans. It is primarily a nosocomial pathogen Reportedly colonizes more than 50% of humans. May be highly resistant to antibiotics. Transmitted by direct contact with a contaminated object, surface, solution, or hands. Studies have shown it can survive on inanimate objects for up to 16 months. In our organization, about 10% of our HAIs last year were with this organism.
30
31
32 Additional questions to consider, based on organism (examples) A. What are potential sources of organism in this case? B. Based on answer to A., devise rest of questions, e.g.: a. Given that P. aeruginosa is found in over 50% of humans normally and it s an opportunistic pathogen, placing a Foley put Jerri at risk of getting infected as that compromised her host defenses. Did the need for the Foley outweigh the risk of catheter-related complications, such as this CAUTI? Why do we put Foleys in all THR patients? b. Were there other sources of P. aeruginosa in Jerri s environment we need to consider? Plants? Sink? How was bathing carried out? Are bath basins used? If so, how are they cleaned after/before use? Are sinks being used as a bath basin? How is room cleaning done? Any caregivers wearing long or artificial nails? c. Could it have been transmitted from another patient via healthcare workers? From the patient in the room prior to Jerri s being there? C. Etc.
33 What have we learned? 72 yo Jerri experienced a symptomatic CAUTI 4 days after FC inserted from P. aeruginosa. FC inserted in the OR prior to surgery for THR per the circulating RN. FC in for 3 days despite routine to remove it the day after surgery: kept in per son s request due to patient being in pain from surgery. No alternatives to FC considered pre-op that are documented. Assumed pt. met insertion criteria due to type of surgery. But why do we put Foleys in all THR patients? What is the evidence to support that? Securement device not placed in the OR. Found out it does not come in Foley kits. No documentation of RN competency for FC insertion. RN has nursed for 30+ years and has great experience placing urinary catheters in OR but how do we know she puts them in correctly?
34 What we ve learned so far continued Observed practice shows transporters are raising collection bag above level of bladder. Found they get no training in how to handle collection bags. Pt/family engagement about FC occurred only post-op when there was deviation. Found we do not have any patient-family education materials on pre-op topics for post-op review/reiteration. Transfer form includes only presence of FC, not date of insertion. Hand hygiene compliance issues in OR and on unit. Urine measurement containers are not labeled with patient name/ room #. System for reminding MDs about FCs dependent on nurse being present on rounds. Pt. diabetic and BMI is 30.
35 Step 2: Why Did It Happen? Review events from event report with multidisciplinary team Further research/lit review may be necessary to determine why it happened and if there were any gaps with best practice. Question all practices and compare to best practice defined in the literature. Don t be afraid to really challenge practice. For each gap identified, ask Why five times or until the group feels the root cause has been found. (Keep pushing to the 5 Whys to ensure root cause is determined and latent failures are recognized if present.) Identify and list all contributing factors. Prioritize contributing factors.
36 The Five Whys One Example Gap: Foley remained in 2 days longer than protocol called for. Why 1: Son requested: He felt it was too painful for her to get OOB Why 2: Son was not aware of pain management protocol nor need for pt. to be up and moving. Why 3: Son could not be w/his mother during pre-op visits and there is no patient education on this post-op. Why 4: No process in place to reinforce critical aspects of post-op care with patients and families. Why 5: We ve assumed patients & families remember what they were taught pre-op. Why 1: Surgeon agreed to keep Foley in. Why 2: Surgeon felt risk of developing pneumonia greater if pt. in pain and not coughing/deep breathing post-op compared to developing CAUTI. Why 3: Surgeon did not operate here often and was not familiar with our pain management protocols. Why 4: We don t have processes to communicate new protocols effectively. Why 5: Such communication processes are not part of protocol development.
37 How to prioritize contributing factors an example Contributing Factors No process to reinforce pre-op education postop with patients and families Communication of new/revised protocols to MDs is not a formal step of protocol development/review. Foley insertion criteria are not used with THR patients as community practice is to place a Foley in all of these patients, but w/o scientific evidence. Daily review of Foley necessity is dependent upon nurses rounding with surgeons to remind them. No process in place to assess RN competency for Foley insertion upon hire or periodically thereafter. Importance to current event, 1 (low) to 5 (high) Importance to future events 1 (low) to 5 (high) Ease of Resolution 3 =easy, 2 = fairly easy 1=hard Total Score
38 Step 3: How can we reduce the chances of it happening again? 1. Develop interventions (countermeasures) to defend against the most important contributing factors. 2. Then, rate each countermeasure on its ability to mitigate the root cause and on the team s belief that the countermeasure will be executed. 3. Make an action plan for 2-5 of the highest scoring countermeasure. Must have many different perspectives. Must engage leadership.
39 Countermeasures Consider safe design principles: Standardize eliminate steps when possible Create independent checklists Learn when things go wrong (analyze defects) Safe designs apply to technical and team work. Brainstorm strategies and consider: 1. Ability to mitigate error. 2. Strength of countermeasures to prevent error. 3. Ease of implementation. (Resources and will necessary to implement.)
 Source: VA Center for Patient")
40 Strength of Countermeasures (Your Defensive Systems) Source: VA Center for Patient Safety
41 Rank Order: Strength of Error Reduction Strategies 7. Forcing functions and constraints Designed so that errors are virtually impossible or very difficult to make. Example: removing potassium chloride for injection from all patient care areas. Lessons human fallibility by limiting reliance on memory. 6. Automation and Computerization Example: Placing alcohol wipe in each Pyxis drawer with IV medications so wipe issued with each dose of medication. Standardizes processes/materials/resources to promote awareness of evidence-based practice and increase consistency between providers. It makes defect detection possible also. 5. Standardization and Protocols Example: Standardized CL insertion kit/cart. Standardized CL dressing change kits. Creates redundancies in system to look for errors 4. Checklists and double-check systems Example: Checklist to guide central line dressing changes. Requirement for an RN to recalculate doses of heparin in pediatrics behind pharmacist. Sets standards and expectations. Helps define what defects are. 3. Rules and policies Example: CL maintenance policy based on current science to prevent CL complications such as infection. 2. Education/Information Education and sharing of information Example: Staff education on CL maintenance policy. 1. Instructions to be more careful, vigilant. Admonitions to be more careful to prevent error. This is very traditional in the mental model where individuals have total control of their actions. Example: Management counsels an individual to be more careful after staff member has made a med error.
42 Countermeasures (interventions to reduce the risk of the defect) Daily review of Foley necessity is dependent upon nurses rounding with surgeons to remind them. Ability to mitigate the contributing factor, 1 (low) to 5 (high) Team believes the countermeasure will be implemented and executed, 1 (low) to 5 (high) Strength of Strategy, 1 (low) to 7 (high) Total Score Develop medical protocol giving nursing the ability to remove the Foley when certain criteria are met. (Nurse-driven protocol for Foley removal) Include patient and family in daily assessment for need. Place a reminder sticker on front of patient s chart For all patients with a Foley in, create a pop-up reminder on MD s CPOE screen
43 Step 4: How will we know the risk is reduced? Assess outcome and process data (CAUTI rates, compliance to catheter maintenance protocols, monitoring of specific process changes, etc.) Talk to staff to get their perspectives. Talk to patients/families to get their perspectives. Do gemba walks for direct observation. Feedback from patient safety rounds.
44 Step 5: How do we communicate our findings and to whom? Internal communications Other units Quality committee Risk Manager Staff and physicians External communications PSO Collaboratives, CAUTI Campaign
45 Common Pitfalls in LfD A systematic, scientific approach is not used. Only one person does the investigation. The medical record is the only source of information of what happened or may have happened. Direct care providers that cared for the specific patient are not involved. Active errors are identified but no work to push upstream and find the latent errors contributing to them. Physicians and patients/families are often left out. Team or individuals get caught in analysis paralysis. Primary countermeasures stop at re-educate and admonishments to providers to Be more careful. Learning stops at the individual defect. Information goes no further than the team involved.
46 Carteret General Hospital

47 Carteret General Hospital
48 Carteret General Hospital
49 Your Charge Within the next two months, use the Event Investigation tool (or your own tool) to investigate a CAUTI or a defect that may lead to a CAUTI. Go through each of the five steps of defect analysis. Call Shelby or Jan if you have any questions, need to talk through anything, etc.
50 Resources campaigncauti.lasso (CLABSI toolkit - Chapter 6 Hygiene) NC Participants: Shelby Lassiter slassiter@ncha.org VA Participants: Jan Mangun jmangun@vhha.org
CUSP: Learning from Defects. CUSP Boot Camp March 2013
 CUSP: Learning from Defects CUSP Boot Camp March 2013 Objectives Participants will be able to: 1. Describe how defect analysis is a foundational element of CUSP. 2. Discuss latent and active failures and
CUSP: Learning from Defects CUSP Boot Camp March 2013 Objectives Participants will be able to: 1. Describe how defect analysis is a foundational element of CUSP. 2. Discuss latent and active failures and
Real Time CLABSI Case Reviews at HCMC. Mary Ellen Bennett Steph Laskowski
 Real Time CLABSI Case Reviews at HCMC Mary Ellen Bennett Steph Laskowski RCA vs Real Time Case Review Similar: event review with stakeholders, no blame, gives ideas on what could be done better, focus
Real Time CLABSI Case Reviews at HCMC Mary Ellen Bennett Steph Laskowski RCA vs Real Time Case Review Similar: event review with stakeholders, no blame, gives ideas on what could be done better, focus
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Healthcare- associated Infections in North Carolina: A Statewide Discussion
 Healthcare- associated Infections in North Carolina: A Statewide Discussion 1 State Stakeholders 2 Agenda Background Data limitations Data review Prevention activities Q&A 3 Goal To discuss HAI prevention
Healthcare- associated Infections in North Carolina: A Statewide Discussion 1 State Stakeholders 2 Agenda Background Data limitations Data review Prevention activities Q&A 3 Goal To discuss HAI prevention
Infection Prevention and Control
 Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
BUGS BE GONE: Reducing HAIs and Streamlining Care!
 BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Joint Commission NPSG 7: 2011 Update and 2012 Preview
 Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
Surgical Technology Patient Care Skills Preop Routine Objectives:
 Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri
 Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Infection Control: You are the Expert
 Infection Control: You are the Expert The engaged participant will be able to: List Recognize Identify Three most frequently cited deficiencies Two ways to make hand washing safer Most important practice
Infection Control: You are the Expert The engaged participant will be able to: List Recognize Identify Three most frequently cited deficiencies Two ways to make hand washing safer Most important practice
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Is It Really a UTI? Do You Know It When You See It?
 Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
Infection Prevention Isolation Precautions Toolkit
 Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Training Your Caregiver: Hand Hygiene
 Infections are a serious threat to fragile patients. They are often spread by healthcare workers and family members who are providing frontline care. In fact, one of the major contributors to infections
Infections are a serious threat to fragile patients. They are often spread by healthcare workers and family members who are providing frontline care. In fact, one of the major contributors to infections
The Clatterbridge Cancer Centre. NHS Foundation Trust MRSA. Infection Control. A guide for patients and visitors
 The Clatterbridge Cancer Centre NHS Foundation Trust MRSA Infection Control A guide for patients and visitors Contents Information... 1 Symptoms... 1 Diagnosis... 2 Treatment... 2 Prevention of spread...
The Clatterbridge Cancer Centre NHS Foundation Trust MRSA Infection Control A guide for patients and visitors Contents Information... 1 Symptoms... 1 Diagnosis... 2 Treatment... 2 Prevention of spread...
Patient & Family Guide. VRE (Vancomycinresistant. Enterococcus)
") Patient & Family Guide VRE (Vancomycinresistant Enterococcus) 2017 www.nshealth.ca VRE (Vancomycin-resistant Enterococcus) What is VRE? Enterococci (plural of enterococcus) are bacteria that are commonly
Patient & Family Guide VRE (Vancomycinresistant Enterococcus) 2017 www.nshealth.ca VRE (Vancomycin-resistant Enterococcus) What is VRE? Enterococci (plural of enterococcus) are bacteria that are commonly
Why Does Hand Hygiene Matter? 1/26/2015 1
 Why Does Hand Hygiene Matter? 1/26/2015 1 This presentation will Explain why hand hygiene matters Explain how to perform hand hygiene Describe how and when to perform a crucial conversation regarding Hand
Why Does Hand Hygiene Matter? 1/26/2015 1 This presentation will Explain why hand hygiene matters Explain how to perform hand hygiene Describe how and when to perform a crucial conversation regarding Hand
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Understanding Health Care in America An introduction for immigrant patients
 Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
Patient Education Understanding Health Care in America An introduction for immigrant patients The health care system in the United States is complex. Some parts of the system are different in different
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013
 Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
Willamette Valley Medical Center Carla Galbraith RN, BSN, CIC Manager Patient Safety/Infection Control November 1, 2013 About Us Willamette Valley Medical Center McMinnville, Oregon Acute Care Facility
Hospitals Face Challenges Implementing Evidence-Based Practices
 United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Title: Learning from Defects Learning from and Preventing adverse events
 Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters
 Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters Pat Posa RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI patposa@gmail.com Objectives Understand
Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters Pat Posa RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI patposa@gmail.com Objectives Understand
Welcome to the Cooper Infection Prevention Team
 Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
CMS and NHSN: What s New for Infection Preventionists in 2013 Part II
 CMS and NHSN: What s New for Infection Preventionists in 2013 Part II Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the two major
CMS and NHSN: What s New for Infection Preventionists in 2013 Part II Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the two major
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
Proactively prevent HAIs with infection surveillance software
 Proactively prevent HAIs with infection surveillance software NIP HAIs IN THE BUD Redirect your time to proactively preventing infections instead of just reacting. RL s automated infection surveillance
Proactively prevent HAIs with infection surveillance software NIP HAIs IN THE BUD Redirect your time to proactively preventing infections instead of just reacting. RL s automated infection surveillance
World Health Organization Male Circumcision Quality Assurance Workshop 2010
 Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned
 On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
On the Road to Eliminating CAUTI at a Community Hospital Lessons Learned Getting Started CDC guidelines LeverageIT Capabilities Ordering, documenting and tracking Develop education SimLab observations
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
HAI Prevention. Beyond the Bundle. March 18, 2016
 HAI Prevention Beyond the Bundle March 18, 2016 Krystyna Strozewski Director of Quality Lake Health System Karen Mrazik Infection Preventionist Tripoint Medical Center Elizabeth Reed Infection Preventionist
HAI Prevention Beyond the Bundle March 18, 2016 Krystyna Strozewski Director of Quality Lake Health System Karen Mrazik Infection Preventionist Tripoint Medical Center Elizabeth Reed Infection Preventionist
Technical Bulletin. Summary...5. Background...2. Study Commissioned...2. Methodology...2. Results...3. Discussion...3. Cost Comparison...
 The Use of Medication Drawer Bin Liners As An Infection Control Strategy Technical Bulletin Health Care Logistics, Inc. 2005 Printed in the U.S.A. Background...2 Summary...5 Study Commissioned...2 Methodology...2
The Use of Medication Drawer Bin Liners As An Infection Control Strategy Technical Bulletin Health Care Logistics, Inc. 2005 Printed in the U.S.A. Background...2 Summary...5 Study Commissioned...2 Methodology...2
APIC Questions with Answers. NHSN FAQ Webinar. Wednesday, September 9, :00-3:00 PM EST
 APIC Questions with Answers NHSN FAQ Webinar Wednesday, September 9, 2015 2:00-3:00 PM EST General Questions We are an acute general hospital - psych, do we need to be reporting anything to NSHN? Yes,
APIC Questions with Answers NHSN FAQ Webinar Wednesday, September 9, 2015 2:00-3:00 PM EST General Questions We are an acute general hospital - psych, do we need to be reporting anything to NSHN? Yes,
Learning Objectives. Successful Antibiotic Stewardship. Byron Health Center & GrandView Pharmacy
 Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN
 Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety
 AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
Efficacy of Tympanostomy Tubes for Children with Recurrent Acute Otitis Media Randomization Phase
 CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
CONSENT FOR A CHILD TO BE A SUBJECT IN MEDICAL RESEARCH AND AUTHORIZATION TO PERMIT THE USE AND SHARING OF IDENTIFIABLE MEDICAL INFORMATION FOR RESEARCH PURPOSES TITLE Efficacy of Tympanostomy Tubes for
2016 Quality Management. Sandra Webb BSN RN CIC
 2016 Quality Management Sandra Webb BSN RN CIC Quality Management Department Functions: Core Measures Infection Prevention Patient Safety Officer Performance Improvement Performance Improvement Data is
2016 Quality Management Sandra Webb BSN RN CIC Quality Management Department Functions: Core Measures Infection Prevention Patient Safety Officer Performance Improvement Performance Improvement Data is
MRSA. Information for patients Infection Prevention and Control. Large Print
 MRSA Information for patients Infection Prevention and Control Large Print page 2 of 16 What is MRSA? MRSA is a bacterium (germ), which can be found living on the skin of healthy individuals, particularly
MRSA Information for patients Infection Prevention and Control Large Print page 2 of 16 What is MRSA? MRSA is a bacterium (germ), which can be found living on the skin of healthy individuals, particularly
Learning from Defects: Surgical Site Infection
 Learning from Defects: Surgical Site Infection 7/15/13 Sometimes you get the best light from a burning bridge From the song My Thanksgiving by Don Henley Shelby Lassiter, BSN, RN, CPHQ, CIC Performance
Learning from Defects: Surgical Site Infection 7/15/13 Sometimes you get the best light from a burning bridge From the song My Thanksgiving by Don Henley Shelby Lassiter, BSN, RN, CPHQ, CIC Performance
HEN 2.0 CLABSI WEBINAR NAILING CLABSI PREVENTION! February 11, :00 a.m. 12:30 p.m. CT
 HEN 2.0 CLABSI WEBINAR NAILING CLABSI PREVENTION! February 11, 2016 11:00 a.m. 12:30 p.m. CT 1 WELCOME AND INTRODUCTIONS Kimberly King, Program Specialist, HRET 11:00 11:05 2 WEBINAR PLATFORM QUICK REFERENCE
HEN 2.0 CLABSI WEBINAR NAILING CLABSI PREVENTION! February 11, 2016 11:00 a.m. 12:30 p.m. CT 1 WELCOME AND INTRODUCTIONS Kimberly King, Program Specialist, HRET 11:00 11:05 2 WEBINAR PLATFORM QUICK REFERENCE
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use
 Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures. Today s Presenters
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
High Reliability Organizations Healing Without Harm by 2014
 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Indwelling Urinary Catheters: A One- Point Restraint?
 Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
MRSA. Information for patients Infection Prevention and Control
 MRSA Information for patients Infection Prevention and Control What is MRSA? MRSA is a bacterium (germ), which can be found living on the skin of healthy individuals, particularly in the lining of the
MRSA Information for patients Infection Prevention and Control What is MRSA? MRSA is a bacterium (germ), which can be found living on the skin of healthy individuals, particularly in the lining of the
42 CFR Infection Control
 42 CFR 482.42 Infection Control Dodjie B. Guioa, MBA Hospital/ASC Program Lead Region VI Dallas dodjie.guioa@cms.hhs.gov Condition of Participation Infection Control The hospital must provide a sanitary
42 CFR 482.42 Infection Control Dodjie B. Guioa, MBA Hospital/ASC Program Lead Region VI Dallas dodjie.guioa@cms.hhs.gov Condition of Participation Infection Control The hospital must provide a sanitary
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
LESSON ASSIGNMENT. After completing this lesson, you should be able to: 2-3. Distinguish between medical and surgical aseptic technique.
 LESSON ASSIGNMENT LESSON 2 Medical Asepsis. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Identify the meaning of aseptic technique. 2-2. Identify the measures treatment personnel
LESSON ASSIGNMENT LESSON 2 Medical Asepsis. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Identify the meaning of aseptic technique. 2-2. Identify the measures treatment personnel
Major Oral Surgery: Composite Resection with Free Flap
 Major Oral Surgery: Composite Resection with Free Flap Information for patients diagnosed with oral cancer and their families Read this booklet to learn: how to prepare for oral surgery what you can expect
Major Oral Surgery: Composite Resection with Free Flap Information for patients diagnosed with oral cancer and their families Read this booklet to learn: how to prepare for oral surgery what you can expect
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
While Your Child Is on the BMT Unit
 Page 1 of 5 While Your Child Is on the BMT Unit A Guide for Patients, Family and Visitors Your child s care Your child s health care team provides familycentered care. Our goal is to get to know you and
Page 1 of 5 While Your Child Is on the BMT Unit A Guide for Patients, Family and Visitors Your child s care Your child s health care team provides familycentered care. Our goal is to get to know you and
4/30/2012. Disclosure. Housekeeping. The Role of the Infection Preventionist on the Value Analysis Committee. Boyd Wilson
 3M Infection Prevention Learning Connection The Role of the Infection Preventionist on the Value Analysis Committee Making a Business Case for Evaluating New Products May 8, 2012 Disclosure Boyd Wilson
3M Infection Prevention Learning Connection The Role of the Infection Preventionist on the Value Analysis Committee Making a Business Case for Evaluating New Products May 8, 2012 Disclosure Boyd Wilson
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success
 Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Toolbox Talks. Access
 Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Erlanger Infection Control Program. Resident Resident Orientation and. and
 Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Changing ICU culture to reduce catheter-associated urinary tract infections
 QI IN IPAC Changing ICU culture to reduce catheter-associated urinary tract infections Marcia Maxwell RN, MS, CNS, CCNS, CCRN, Kristy Murphy RN, BSN, MSc & Maude McGettigan RN, BA, CIC SCL Health Good
QI IN IPAC Changing ICU culture to reduce catheter-associated urinary tract infections Marcia Maxwell RN, MS, CNS, CCNS, CCRN, Kristy Murphy RN, BSN, MSc & Maude McGettigan RN, BA, CIC SCL Health Good
Device Utilization and CAUTI Prevention. Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016
 Device Utilization and CAUTI Prevention Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016 DISCLOSURES Nothing to disclose OBJECTIVES Explain relationship between catheterassociated
Device Utilization and CAUTI Prevention Lori Fornwalt, RN, CIC Infection Prevention Coordinator October 4, 2016 DISCLOSURES Nothing to disclose OBJECTIVES Explain relationship between catheterassociated
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Clostridium difficile Infections (CDI): Opportunities for Prevention. Linda Savage, RN, BSN, CDONA/LTC QI Specialist, Telligen March 23, 2016
: Opportunities for Prevention. Linda Savage, RN, BSN, CDONA/LTC QI Specialist, Telligen March 23, 2016") Clostridium difficile Infections (CDI): Opportunities for Prevention Christine LaRocca, MD Medical Director, Telligen Linda Savage, RN, BSN, CDONA/LTC QI Specialist, Telligen March 23, 2016 Deanna Curry,
Clostridium difficile Infections (CDI): Opportunities for Prevention Christine LaRocca, MD Medical Director, Telligen Linda Savage, RN, BSN, CDONA/LTC QI Specialist, Telligen March 23, 2016 Deanna Curry,
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
Department of Public Health Infection Control Survey
 Patient Care Services, uality and Safety Being Ready for Every Patient Every Day Department of Public Health Infection Control Survey Resource Guide for Patient Care ssociates Excellence Every Day The
Patient Care Services, uality and Safety Being Ready for Every Patient Every Day Department of Public Health Infection Control Survey Resource Guide for Patient Care ssociates Excellence Every Day The
Strategy/Driver Prevention Strategies Action Strategies
 I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
Decreasing Nosocomial C. diff
 Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Decreasing Nosocomial C. diff Our journey to decreasing nosocomial C. diff Jennifer Conti BSN, RN, CIC Nicole Rabic MSN, RN, CIC 4.21.2016 Nosocomial C. diff Use of the CDC standardized definition Review
Navigating through Frontline Competencies, Training and Audits
 Navigating through Frontline Competencies, Training and Audits Carol Vance MSN, RN, CIC Multi-site Director, Infection Prevention Advocate Children s Hospital Objectives Discuss the relationship between
Navigating through Frontline Competencies, Training and Audits Carol Vance MSN, RN, CIC Multi-site Director, Infection Prevention Advocate Children s Hospital Objectives Discuss the relationship between
Carbapenamase Producing Enterobacteriaceae: A Draining Concern
 Carbapenamase Producing Enterobacteriaceae: A Draining Concern Heather Candon, B.Sc., M.Sc., MHM, CIC Lorraine Maze dit Mieusement, RN, MN, CIC Natasha Salt, B.Sc., B.A.Sc., CPHI (C), CIC Introduction
Carbapenamase Producing Enterobacteriaceae: A Draining Concern Heather Candon, B.Sc., M.Sc., MHM, CIC Lorraine Maze dit Mieusement, RN, MN, CIC Natasha Salt, B.Sc., B.A.Sc., CPHI (C), CIC Introduction
Health Care Associated Infections in 2017 Acute Care Hospitals
 Health Care Associated Infections in 2017 Acute Care Hospitals Christina Brandeburg, MPH Epidemiologist Katherine T. Fillo, Ph.D, RN-BC Director of Clinical Quality Improvement Eileen McHale, RN, BSN Healthcare
Health Care Associated Infections in 2017 Acute Care Hospitals Christina Brandeburg, MPH Epidemiologist Katherine T. Fillo, Ph.D, RN-BC Director of Clinical Quality Improvement Eileen McHale, RN, BSN Healthcare
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Identify patients with Active Surveillance Cultures (ASC)
") MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
Patient Safety Case Study. Clara K. Terral. Angelo State University
 Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental