Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters
|
|
|
- Brittany Hicks
- 6 years ago
- Views:
Transcription
1 Creating Sustainable Change to Prevent Harm in the ICU: Culture Matters Pat Posa RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI
2 Objectives Understand the importance of leadership engagement and strategies to attain it Review strategies to create a culture of safety including safe design principles, communication and focusing on learning from defects Discuss the 4 E s framework to deal with both adaptive and technical change 2
3 It is Time to Change!! 44,00 to 98,000 preventable death in hospitals related to medical errors annually (IOM report, 1999) 92,888 deaths directly attributable to safety indicators between (HealthGrades 2009) Failure to rescue, pressure ulcers and post-op infections National Patient Safety Goals include prevention of Hospital Acquired Infections (HAIs) 1 out of 20 patient have HAI Lack of reimbursement for preventable injury 2013-lowest percent improvement/total Medicare cut $50 billion in total costs for preventable injury 3
4 What is Patient Safety? Patient safety was defined by the IOM as the prevention of harm to patients. Emphasis is placed on the system of care delivery that: 1. prevents errors 2. learns from the errors that do occur 3. is built on a culture of safety that involves health care professionals, organizations, and patients. Aspden P, Corrigan J, Wolcott J, et al., editors. Patient safety: achieving a new standard for care. Washington, DC: National Academies Press;

5 Value Sets Platform for Performance Improvement: The Vision of Health Care in the U.S. NOW 5
6 High Reliability Organizations High Reliability: consistent performance at high levels of safety over long periods of time Possess Collective mindfulness Means that everyone who works in these organizations, both individually and together, is acutely aware that even small failures in safety protocols or processes can lead to catastrophic adverse events, if some action is not taken to solve the problem Two other features: Eliminate deficiencies in safety processes through the use of powerful tools to improve their processes Create an organizational culture that focuses on safety, in which they remain constantly aware of the possibility of failure Chassin & Loeb, Health Affairs, April 2011; Chassin & Loeb, The Milbank Quarterly, Vol 91 No 3, 2013 pp
7 Key Components to Sustainable Change Leadership engagement Culture of safety Implementation framework that deals with both technical and adaptive change 7
8 Leadership Engagement
9 Leadership, get their interest It is the right thing to do patient stories their stories WIFM What s In it For Me (them) Cost avoidance estimation Patient Throughput Reduce turn-over Sources: 1. Duval-Arnould J, Mathews SC, Weeks K, Colantuoni E, Mukherjee A, Nundy S, Watson SR, Holzmueller CG, Lubomski LH, Goeschel CA, Pronovost PJ, Pham JC, Berenholtz SM. Using the Opportunity Estimator tool to improve engagement in a quality and safety intervention. Jt Comm J Qual Patient Saf Jan;38(1):41-7,1. 2. Waters HR, Korn R Jr, Colantuoni E, Berenholtz SM, Goeschel CA, Needham DM, Pham JC, Lipitz-Snyderman A, Watson SR, Posa P, Pronovost PJ. The business case for quality: economic analysis of the Michigan Keystone Patient Safety Program in ICUs. Am J Med Qual Sep-Oct;26(5):
10 Leadership Engagement Leadership support Vice President or higher Support the work of the team Round on unit be purposeful Script the rounds How will the next patient in this unit be harmed? How can I help to remove barriers, so that the safety defects you are most concerned about can be better addressed? How well does teamwork occur on this unit? What doesn t work well? If there is a learning board, use this as the meeting point on the unit. Source: Sexton, JB, Engaging Leaders Webinar,
11 Goals of Executive Safety Partnerships Near term goal: to build capacity for quality improvement within the unit Medium term goal: to have staff bring up solutions rather than problems Long term goal: for staff to say: We don t need to meet monthly with the executive I would feel safe being treated here as a patient I felt like I was heard today I made a difference today 11
12 Create a Culture of Safety Application of safe design principles Improve communication and teamwork Focusing on learning from defects
13 Medical errors most often result from a complex interplay of multiple factors. Only rarely are they due to the carelessness or misconduct of single individuals. Lucien L. Leape, MD Harvard School of Public Health 13
14 Why Mistakes Happen? Variable input (diff pts) Inconsistency/variation Complexity Too many/complicated steps Human intervention Tight time constraints Hierarchical culture Process Factors Fatigue Inattention/distraction Unfamiliar situations/new problem Using past solutions Equipment design flaws Communications errors Mislabeling/inadequate instructions People Factors 14
15 A Positive Culture of Safety..recognizes the inevitability of error and proactively seeks to identify latent threats Nieva, V F Qual Saf Health Care 2003;12(suppl) 15
16 Safe Design Principles Understand system determines performance Use strategies to improve system performance Standardize Create Independent checks for key process Learn from Mistakes Apply strategies to both technical work and team work Recognize that teams make wise decisions with diverse and independent input 16
17 Improve Communication and Teamwork

18 Communication Breakdowns Cause Treatment Delays Root Causes of Treatment Delays( ) 18

19 Communication Breakdowns Cause Infection-associated Events Root causes of infection-associated events (2005) 19

20 Effective Teamwork s Positive Impact on Health Care Reduced length of stay Lower nurse turnover Higher quality of care Greater ability to meet family member needs Better patient outcomes Better patient experience with care scores 20


21 % of respondents within an ICU reporting good teamwork climate Teamwork Climate Across Michigan ICUs The strongest predictor of clinical excellence: caregivers feel comfortable speaking up if they perceive a problem with patient care No BSI = 5 months or more w/ zero 10 0 No BSI 21% No BSI 44% No BSI 31%
22 Learn from a defect SBAR (Team STEPPS) Daily rounds/goals Pre-procedure briefing (Team STEPPS) Morning briefing (Team STEPPS) Huddles Shadowing Crucial Conversations Executive Safety Rounds/Partnership Handoff standardization (Team STEPPS) 22
23 SBAR provides A framework for team members to effectively communicate information to one another Communicate the following information: Situation what is the situation? Background what is the clinical background? Assessment what is the problem? Recommendation what do I recommend/request be done? Remember to introduce yourself 23
24 Multidisciplinary Rounds with Daily Goals What is it? A strategy to assemble the patient care team members to review important patient care and safety issues and improve collaboration on the overall plan of care for the patient Improve communication among care team and family members regarding the patient s plan of care Goals should be specific and measurable Documented where all care team members have access Checklist used during rounds prompts caregivers to focus on what needs to be accomplished that day to safely move the patient closer to transfer out of the ICU or discharge home Measure effectiveness of rounds team dynamics, communication, quality measure compliance, LOS 24
25 Evidence For Impact Of MDR Rounds Research studies on the effect of structured interdisciplinary rounds show: Earlier identification of clinical issues More timely referrals Improved ratings by nurses and physicians on teamwork, communication and collaboration. Research also indicates variable effects on LOS and cost, with some studies showing improvement and others having no impact. Improving teamwork: impact of structured interdisciplinary rounds on a medical teaching unit. O'Leary KJ, et. al, Journal Of General Internal Medicine [J Gen Intern Med], ISSN: , 2010 Aug; Vol. 25 (8), pp ; PMID:
26 Multidisciplinary Rounds with Daily Goals Challenges and Opportunities Should be done in ICUs and all units in hospital Hard initiative to implement, especially if you have an open unit and/or no intensivists or in non-icu area Standardize the structure and process for all units Benefits seen even if physician can not attend consistently or at all Second rounds should be done in afternoon include at least physician and bedside nurse Evaluate if goals for day have been met; readjust if necessary Identify if patient can be discharged (or transferred ) the next day and if so, what needs to be accomplished 26
27 Multidisciplinary Rounds with Daily Goals Challenges and Opportunities (continued) Focused first on defining daily goals and recording those either on the white board in the room or on a sheet of paper Then standardize rounds who should attend and what is discussed Implemented nursing objective card to clearly define role of nurse in multidisciplinary rounds 27

28 Interdisciplinary Rounds: Nursing Objective Card Pain, Agitation and Delirium Mobility VAE SEPSIS CAUTI/CLABSI
29 Why Checklists? Levels of cognitive function are often compromised with increasing levels of stress and fatigue in certain fields of work. Aviation, aeronautics, and product manufacturing have come to rely heavily on checklists to aid in reducing human error. The checklist is an important tool in error management across all these fields, contributing significantly to reductions in the risk of costly mistakes and improving overall outcomes. Such benefits also translate to improving the delivery of patient care. Despite demonstrated benefits of checklists in medicine and critical care, the integration of checklists into practice has not been as rapid and widespread as with other fields. J Crit Care 2003;21:
30 Huddles Enable teams to have frequent but short briefings so they can stay informed, review work, make plans, and move ahead rapidly. Allow fuller participation of front-line staff and bedside caregivers, who often find it impossible to get away for the conventional hour-long improvement team meetings. They keep momentum going, as teams are able to meet more frequently. Use this strategy to begin to recover immediately from defects---ie: falls, sepsis. Use daily to focus on unit outcomes 30

31 Components Metric 1: Quality/Safety Metric 2: Patient Satisfaction Metric 3: Operations Daily Critical Communications Information Ideas in Motion How to do it? Beginning or mid shift 5-10 minutes Lead by member of unit leadership team 31

32 SICU Huddle Board 32
33 Focus on Learn from Defects

34 What Is a Defect? Anything that you do not want to happen again. 34

35 Errors Provide Useful Information We can learn more from our failures than from success Our processes can be improved when studied Give me a fruitful error anytime, full of seeds, bursting with its own corrections. You can keep your sterile truth to yourself. Vilfred Pareto copyright 2008 by the Trustees of Columbia University in the City of New York Rights Reserved 35
36 Learn from a Defect Designed to rigorously analyze the various components and conditions that contributed to an adverse event and is likely to be successful in the elimination of future occurrences. Tool can serve to organize factors that may have contributed to the defect and provides a logical approach to breaking down faulty system issues Patient, team, task, caregiver factors Training, education, technology factors Local or institutional environment 36
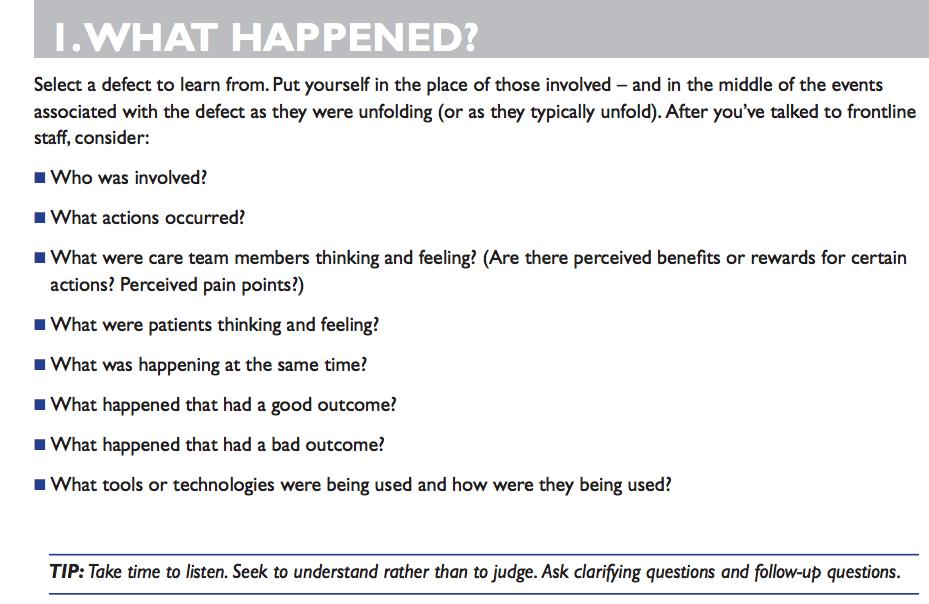
37 Learning From Defects What happened? From view of person involved Why did it happen? How will you reduce it happening again? How will you know the risk is reduce? With whom will you share the learnings? 37
38 Brainstorm #1 38

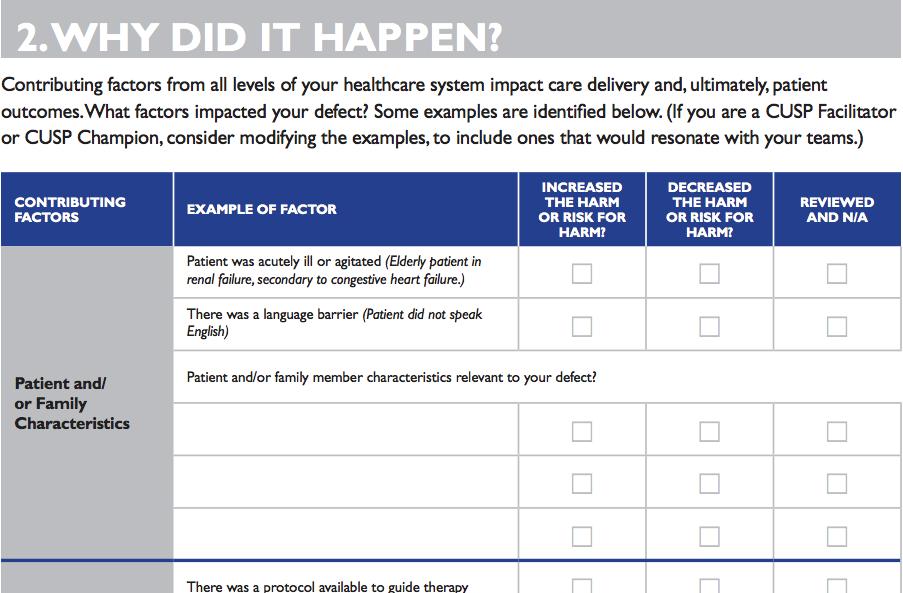
39 Brainstorm # 2 Why Did It Happen? 339


40 Brainstorm # 3 Solution Finding.All ideas are Welcome Necessary 40
41 Start with Low Hanging Fruit 41

42 A Good Solution Must Be Clear in how we measure the success Trialable and easy to test Compatible with or improve existing workflows Low cost, low fidelity 42

43 Building Resiliency Into Interventions Forcing functions and constraints Automation and computerization Standardization and protocols Strongest Checklists and independent check systems Rules and policies Education and information Vague warnings Be more careful! STRENGTH OF INTERVENTION 43 Weakest 43
44 LFD: CLABSI 44
45 LFD: CAUTI 45
46 4E s Implementation Framework CLABSI CAUTI
47 Technical and Adaptive Change One of the most common leadership mistakes is expecting technical solutions to solve adaptive problems." Ron Heifetz 1 Leadership Without Easy Answers (Cambridge: Harvard University Press, 1994) 47
48 Key concepts: Adaptive and Technical Work Technical Work CAUTI Prevention Appropriate Indication Insertion Maintenance CLABSI Prevention Insertion Maintenance Review daily if necessary Adaptive Work Work that shapes the attitudes, beliefs, and values of clinicians, so they consistently perform tasks the way they know they should The intangible components of work, like ensuring an ICU team holds each other accountable Work that lends itself to standardization (e.g., checklists and protocols) Culture change is not a checklist 48
49 4 E s for Implementing Change Executive Leaders Team Leaders Staff Engage adaptive How Do I Make the World a Better Place? How do I create an organization that is safe for patients and rewarding for staff? How does this strategy fit our mission? How Do I Make the World a Better Place? How do I create a unit that is safe for patients and rewarding for staff? How do I touch their hearts? How Do I Make the World a Better Place? Do I believe I can change the world, starting with my unit? Can I help make my unit safer for patients and a better place to work? Educate technical What Do I Need to Know? What is the business case? How do I engage the Board and Medical Staff? How can I monitor progress? What Do I Need to Know? What is the evidence? Do I have executive and medical staff support? Are there tools to help me develop a plan? What Do I Need to Know? Why is this change important? How are patient outcomes likely to improve? How does my daily work need to change? Where do I go for support? Execute adaptive What Do I Need to Do? Do the Board and Medical Staff support the plan and have the skills and vision to implement? How do I know the team has sufficient resources, incentives and organizational support? What Do I Need to Do? Do the Staff Know the plan and do they have the skills and commitment to implement? Have we tailored this to our environment? What Do I Need to Do? Can I be a better team member and team leader? How can I share what I know to make care better? Am I learning from defects? Evaluate technical How Will I Know I Made a Difference? Have resources been allocated to collect and use safety data? Is the work climate better? Are patients safer? How do I know? How Will I Know I Made a Difference? Have I created a system for data collection, unit level reporting, and using data to improve? Is the work climate better? Are patients safer? How do I know? How Will I Know I Made a Difference? What is our unit level report card? Is the unit a better place to work? Is teamwork better? Are patients safer? How do I know? Quality and Safety Research Group, Johns Hopkins University
50 Technical Adaptive Technical Adaptive 4E s Preventing CAUTI Frontline Staff CAUTI Prevention Engage Ask, how will CAUTI prevention make the world a better place? -Help staff understand preventable harm -Share stories about patients affected -Develop a business care -Include execute champion/physician leadership Define evidence related to preventing CAUTI Share CAUTI rate, number of patients harmed, Share patient stories Create business case related to the impact of CAUTI prevention--decreased hospital LOS and decreased ICU LOS, improved reimbursement--vbp Share business case with executive champion/ physician leadership Educate What do we need to do to prevent CAUTI in critically ill patients? -Convert evidence into behaviors -Evaluate awareness and agreement Review the literature Identify barriers to getting the catheter out Ensure appropriate insertion technique-who and how Adopt recommended indications for insertion of catheter Define appropriate catheter care Bladder Bundle Define your education plan (utilizing workshops, hands-on trainings, conferences, slides, presentations and interactive discussions via multiple modalities to cater to different learning styles) -Identify support through outreach to the leadership team Do you have a nurse driven catheter removal policy Implement an insertion checklist Who should be involved? On your unit and beyond Do we have all the equipment? Discuss as part of interdisciplinary rounds/daily goals -Learn from defects Execute How will we implement CAUTI prevention at our hospital give local culture and resources? -Listen to resisters -Standardize care and create independent checks -Make it easy to do the right thing -Learn from mistakes Evaluate How will we know that our efforts to prevent CAUTI in our patients made a difference? -Define measures -Regularly assess measures -Provide feedback to staff and celebrate success Audit compliance with components of the bladder bundle and insertion indication and technique Collect CAUTI rates and device utilization Define data collection plan
51 Technical Adaptive Technical Adaptive 4E s Preventing CLABSI Frontline Staff CLABSI Prevention Engage Educate Execute Evaluate Ask, how will CLABSI prevention make the world a better place? -Help staff understand preventable harm -Share stories about patients affected -Develop a business care -Include execute champion/physician leadership What do we need to do to prevent CLABSI in critically ill patients? -Convert evidence into behaviors -Evaluate awareness and agreement How will we implement CLABSI prevention at our hospital give local culture and resources? -Listen to resisters -Standardize care and create independent checks -Make it easy to do the right thing -Learn from mistakes How will we know that our efforts to prevent CLABIS in our patients made a difference? -Define measures -Regularly assess measures -Provide feedback to staff and celebrate success Define evidence related to preventing CLABSI Share CLABSI rate, number of patients harmed, Share patient stories Create business case related to the impact of CLABSI prevention-- decreased hospital LOS and decreased ICU LOS, improved reimbursement--vbp Share business case with executive champion/ physician leadership Review the literature Ensure appropriate insertion technique-who and how Identify barriers to getting the catheter out Avoid femoral line insertion Define appropriate catheter care Maintenance Bundle Define your education plan (utilizing workshops, hands-on trainings, conferences, slides, presentations and interactive discussions via multiple modalities to cater to different learning styles) -Identify support through outreach to the leadership team Do you have a policy related to care of the central line Implement an insertion checklist, and a line cart or line bag Do we have all the equipment? Dressings, disinfection caps Discuss as part of interdisciplinary rounds/daily goals Learn from defects Audit compliance with components of the insertion and maintenance bundles Collect CLABSI rates, SIR and device utilization Define data collection plan
52 CAUTI Prevention in the ICU Challenges High prevalence of urinary catheter High prevalence of fever Approach Focus on removing devices Clear consensus on when a urinary catheter is necessary in the critically ill patient are you going to do anything different each hour based on the urinary output? Provide alternatives to indwelling catheters Nurse driven removal protocols Improve urinary culture practices 52
53 CLABSI Prevention in the ICU Challenges Competing priorities Drift by staff in implementing evidence based practices Approach Team/champions identified to continue to focus on this work Educate new staff in standard practices/expectations Audit compliance with both insertion and maintenance of central lines Learn from each defect 53
54 Key Components to Sustainable Change Leadership engagement Culture of safety Implementation framework that deals with both technical and adaptive change 54
55 Top Strategies to hardwire prevention of CLABSI and CAUTI Identify local physician and nurse champions Standardize care based on the evidence Tap into the wisdom of frontline staff Partner with senior executive who sets expectations related to infection prevention Learn from defects 55
56 Top Strategies to hardwire prevention of CLABSI and CAUTI Track CLABSI and CAUTI prevention practices Interdisciplinary rounds on all units that reviews/ensures compliance with key prevention strategies Harness the power of local data to drive improvement efforts Train new staff in evidence-based care 56
57 THANK YOU
If you experience any problems, please call Marilyn Nichols at the MOCPS office at , ext 221 or The Basics of CUSP
 Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Title: Learning from Defects Learning from and Preventing adverse events
 Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Title: Learning from Defects Learning from and Preventing adverse events Armstrong Institute for Patient Safety and Quality Presented by: David A. Thompson DNSc, MS, RN Title: Associate Professor The Johns
Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN
 Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
Beyond the Bundle: Strategies to Prevent Catheter Related Blood Stream Infections in a Pediatric Oncology In- Patient Unit Patricia Church, MSN, RN, PCNS-BC, CPON Bernice Mowery, PhD, PNP, RN Objectives
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
21 st Century Health Care: The Promise and Potential of a Learning Health System
 21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
Implementation Model. Levels of Evidence 3/9/2011. Strategies to get Evidence into Practice EXTRACTING. Elizabeth Bridges PhD RN CCNS, FCCM, FAAN
 Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
FY 13 Pillar Goal Update and FY 14 Pillar Goals
 FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on
FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of
 Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model
 Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Physician Engagement
 On the CUSP: STOP CAUTI Physician Engagement Mohamad Fakih, MD, MPH St John Hospital and Medical Center Detroit, MI February 7, 2012 Acknowledgments Special thanks to Drs Sanjay Saint and Sarah Krein for
On the CUSP: STOP CAUTI Physician Engagement Mohamad Fakih, MD, MPH St John Hospital and Medical Center Detroit, MI February 7, 2012 Acknowledgments Special thanks to Drs Sanjay Saint and Sarah Krein for
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
St. Joseph Mercy Health System Keystone ICU Collaborative: Making your ICUs safer
 St. Joseph Mercy Health System Keystone ICU Collaborative: Making your ICUs safer The secret ingredients are culture and team Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy
St. Joseph Mercy Health System Keystone ICU Collaborative: Making your ICUs safer The secret ingredients are culture and team Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy
Strategies to Address All Types of Harm. Objectives. Share implementation process for a successful large scale harm reduction campaign
 C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
Implementing and Validating a Comprehensive Unit-Based Safety Program
 JOBNAME: jops 1#1 2005 PAGE: 1 OUTPUT: Tue March 15 15:21:54 2005 ORIGINAL ARTICLE Implementing and Validating a Comprehensive Unit-Based Safety Program Peter Pronovost, MD, PhD,* Brad Weast, MHA, Beryl
JOBNAME: jops 1#1 2005 PAGE: 1 OUTPUT: Tue March 15 15:21:54 2005 ORIGINAL ARTICLE Implementing and Validating a Comprehensive Unit-Based Safety Program Peter Pronovost, MD, PhD,* Brad Weast, MHA, Beryl
Wednesday, April 22, :00 a.m. Eastern
 Wednesday, April 22, 2015 11:00 a.m. Eastern Dial In: 888.863.0985 Conference ID: 5358648 Slide 1 Speakers Karen Harris, MD, MPH, FACOG President, North Florida Women's Physicians Medical Director of Patient
Wednesday, April 22, 2015 11:00 a.m. Eastern Dial In: 888.863.0985 Conference ID: 5358648 Slide 1 Speakers Karen Harris, MD, MPH, FACOG President, North Florida Women's Physicians Medical Director of Patient
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
High Reliability and Robust Process Improvement
 High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
Michael Andrew Basinger University of Nevada, Las Vegas, UNLV Theses, Dissertations, Professional Papers, and Capstones
 UNLV Theses, Dissertations, Professional Papers, and Capstones 5-1-2014 The Reduction of Central Line-Associated Bloodstream Infections in Intensive Care Units through the Implementation of the Comprehensive
UNLV Theses, Dissertations, Professional Papers, and Capstones 5-1-2014 The Reduction of Central Line-Associated Bloodstream Infections in Intensive Care Units through the Implementation of the Comprehensive
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Getting Better at Getting Better V O L U M E 1, I S S U E 1
 Getting Better at Getting Better V O L U M E 1, I S S U E 1 A quarterly newsletter from the Office of the Chief Quality & Patient Safety Officer IN THIS ISSUE VPH Workshop Accelerates Change Letters From
Getting Better at Getting Better V O L U M E 1, I S S U E 1 A quarterly newsletter from the Office of the Chief Quality & Patient Safety Officer IN THIS ISSUE VPH Workshop Accelerates Change Letters From
Thinking Differently Acting Differently. Higher staff satisfaction = better patient outcomes & better patient experience
 Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri
 Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Kathleen S. Hall-Meyer, RN, MBA, CIC Saint Luke s Health System Kansas City, Missouri Nothing to disclose At the conclusion of this program, the learner will be able to: -Describe how a partnership with
Impacting quality outcomes: Utilizing an innovative unit-based nursing role. Kaitlin Lindner, BSN, RN, CCRN Stacey Trotman, MSN, RN, CMSRN, RN-BC
 Impacting quality outcomes: Utilizing an innovative unit-based nursing role Kaitlin Lindner, BSN, RN, CCRN Stacey Trotman, MSN, RN, CMSRN, RN-BC Outcomes Identify opportunities for improving quality outcomes
Impacting quality outcomes: Utilizing an innovative unit-based nursing role Kaitlin Lindner, BSN, RN, CCRN Stacey Trotman, MSN, RN, CMSRN, RN-BC Outcomes Identify opportunities for improving quality outcomes
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success
 Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs
 Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
Describe the impact of CLABSI on patients and their families. Discuss three methods of reducing CLABSIs Explore the essential elements of maintaining decreased CLABSIs 1 2001-43,000 CLABSIs In ICUs 2009-18,000
INFECTION of the urinary tract caused
 J Nurs Care Qual Vol. 00, No. 00, pp. 1 6 Copyright c 2016 Wolters Kluwer Health, Inc. All rights reserved. Incorporation of Leadership Rounds in CAUTI Prevention Efforts Suzanne Purvis, DNP, RN, GCNS-BC;
J Nurs Care Qual Vol. 00, No. 00, pp. 1 6 Copyright c 2016 Wolters Kluwer Health, Inc. All rights reserved. Incorporation of Leadership Rounds in CAUTI Prevention Efforts Suzanne Purvis, DNP, RN, GCNS-BC;
TRANSFORMING CARE DELIVERY
 APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
IMPROVING HEALTH OUTCOMES: BLOOD PRESSURE ADAPTIVE CHANGE IN AMBULATORY PRACTICE
 IMPROVING HEALTH OUTCOMES: BLOOD PRESSURE ADAPTIVE CHANGE IN AMBULATORY PRACTICE 2015 American Medical Association and Introduction Despite their best intentions, many ambulatory care practices struggle
IMPROVING HEALTH OUTCOMES: BLOOD PRESSURE ADAPTIVE CHANGE IN AMBULATORY PRACTICE 2015 American Medical Association and Introduction Despite their best intentions, many ambulatory care practices struggle
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations.
 ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
Hospitals Face Challenges Implementing Evidence-Based Practices
 United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Value-Based Purchasing: A Rural Hospital Perspective
 Value-Based Purchasing: A Rural Hospital Perspective Stratis Health & MHA Quality & Patient Safety PPS Hospital Learning Action Network Day Glen Kegley, Hutchinson Health Tuesday, May 3, 2016 Mall of America-
Value-Based Purchasing: A Rural Hospital Perspective Stratis Health & MHA Quality & Patient Safety PPS Hospital Learning Action Network Day Glen Kegley, Hutchinson Health Tuesday, May 3, 2016 Mall of America-
Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0
 2.0") Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0 Hospital NHSN Workshop February 22, 2017 Greg Vasse Anne Diefendorf Our charge is clear:
Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0 Hospital NHSN Workshop February 22, 2017 Greg Vasse Anne Diefendorf Our charge is clear:
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
Room of Horrors : Engaging Interprofessional Students in a Hazards of Hospitalization Simulation. Margie Molloy, DNP, RN, CNE, CHSE Alison Clay, MD
 Room of Horrors : Engaging Interprofessional Students in a Hazards of Hospitalization Simulation Margie Molloy, DNP, RN, CNE, CHSE Alison Clay, MD ANCC Continuing Nursing Education International Nursing
Room of Horrors : Engaging Interprofessional Students in a Hazards of Hospitalization Simulation Margie Molloy, DNP, RN, CNE, CHSE Alison Clay, MD ANCC Continuing Nursing Education International Nursing
Implementation Assessment: Quantitative Interview
 CUSP 4 MVP VAP Improving Care for Mechancially Ventilated Patients Implementation Assessment: Quantitative Interview ICU Unit Type: Hospital Name: Interview Date: Interviewer Name: Section 1: Staff Safety
CUSP 4 MVP VAP Improving Care for Mechancially Ventilated Patients Implementation Assessment: Quantitative Interview ICU Unit Type: Hospital Name: Interview Date: Interviewer Name: Section 1: Staff Safety
HROs and the Role of Finance South Carolina HFMA Annual Institute
 HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
Running head: EBN & CAUTIS 1
 Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
STEER YOUR MAGNET JOURNEY LET PROPHECY ASSESSMENTS BE YOUR GPS
 Prophecy Predicting Employee Success STEER YOUR MAGNET JOURNEY LET PROPHECY ASSESSMENTS BE YOUR GPS www.prophecyhealth.com www.aps-web.com 617.275.7300 The journey to Magnet is both exhilarating and challenging!
Prophecy Predicting Employee Success STEER YOUR MAGNET JOURNEY LET PROPHECY ASSESSMENTS BE YOUR GPS www.prophecyhealth.com www.aps-web.com 617.275.7300 The journey to Magnet is both exhilarating and challenging!
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
LEADERSHIP CHALLENGES IN PATIENT SAFETY
 LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
A3/B3: Improvement in the Intensive Care Unit
 A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU. A thesis presented by. Shelby L. Holden
 Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
The Business Case for Patient Safety
 The Business Case for Patient Safety Janet Corrigan, PhD, MBA Distinguished Fellow Dartmouth Institute for Health Policy and Clinical Practice Gary Kaplan, MD, FACP, FACMPE, FACPE Chairman and CEO Virginia
The Business Case for Patient Safety Janet Corrigan, PhD, MBA Distinguished Fellow Dartmouth Institute for Health Policy and Clinical Practice Gary Kaplan, MD, FACP, FACMPE, FACPE Chairman and CEO Virginia
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Incentives and Penalties
 Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
These Things (Don t Have to) Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013
 Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013") These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
HIMSS Davies Award Enterprise Application. --- Cover Page --- IT Projects and Operations Consultant Submitter s Address: and whenever possible
 HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
The High-Reliability Clinical Enterprise: Part 1
 Nursing Executive Center The High-Reliability Clinical Enterprise: Part 1 Best Practices for Ensuring Every Patient Receives the Known Standard of Care Every Time Phoebe Draper Analyst draperp@advisory.com
Nursing Executive Center The High-Reliability Clinical Enterprise: Part 1 Best Practices for Ensuring Every Patient Receives the Known Standard of Care Every Time Phoebe Draper Analyst draperp@advisory.com
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
School of Nursing Applying Evidence to Improve Quality
 Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
4/30/2012. Disclosure. Housekeeping. The Role of the Infection Preventionist on the Value Analysis Committee. Boyd Wilson
 3M Infection Prevention Learning Connection The Role of the Infection Preventionist on the Value Analysis Committee Making a Business Case for Evaluating New Products May 8, 2012 Disclosure Boyd Wilson
3M Infection Prevention Learning Connection The Role of the Infection Preventionist on the Value Analysis Committee Making a Business Case for Evaluating New Products May 8, 2012 Disclosure Boyd Wilson
Indwelling Urinary Catheters: A One- Point Restraint?
 Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Conflict of Interest Disclaimer. The Affordable Care Act. The Affordable Care Act. Caring for the Critically Ill. The Affordable Care Act
 Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
Get UP to Drive Harm Down. ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health
 Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
CCHS: Quality and Patient Safety. J Michael Henderson, MD Guido Bergomi
 CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
Reducing CAUTI by Decreasing Inappropriate Catheter Utilization
 Reducing CAUTI by Decreasing Inappropriate Catheter Utilization Reducing HAIs in Hospitals E. Eve Esslinger Jane Ehrhardt Heather Banker Debby Fosson Roddy Summers QIN-QIO Map HAIs Central Line-Associated
Reducing CAUTI by Decreasing Inappropriate Catheter Utilization Reducing HAIs in Hospitals E. Eve Esslinger Jane Ehrhardt Heather Banker Debby Fosson Roddy Summers QIN-QIO Map HAIs Central Line-Associated
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
Communication Among Caregivers
 Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Building a Culture That Lasts
 Building a Culture That Lasts Establishing a Leadership Legacy Quality Texas Foundation June 28, 2016 M. Michael Shabot, MD, FACS, FCCM, FACMI Executive Vice President System Chief Clinical Officer V2
Building a Culture That Lasts Establishing a Leadership Legacy Quality Texas Foundation June 28, 2016 M. Michael Shabot, MD, FACS, FCCM, FACMI Executive Vice President System Chief Clinical Officer V2
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Leveraging Clinical Communications Technology to Prevent Missed Nursing Care
 Leveraging Clinical Communications Technology to Prevent Missed Nursing Care Maintaining a competitive edge in the value-based purchasing era Patricia Smith MBA, BSN, RN Preventing Missed Nursing Care
Leveraging Clinical Communications Technology to Prevent Missed Nursing Care Maintaining a competitive edge in the value-based purchasing era Patricia Smith MBA, BSN, RN Preventing Missed Nursing Care
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc.
 Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
Engaging Leaders: From Turf Wars to Appreciative Inquiry
 Engaging Leaders: From Turf Wars to Appreciative Inquiry Principles of Leadership for a Quality and Safety Culture Harvard Safety Certificate Program 2010 Gwen Sherwood, PhD, RN, FAAN Gwen Sherwood, PhD,
Engaging Leaders: From Turf Wars to Appreciative Inquiry Principles of Leadership for a Quality and Safety Culture Harvard Safety Certificate Program 2010 Gwen Sherwood, PhD, RN, FAAN Gwen Sherwood, PhD,