Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017
|
|
|
- Kelly Bryan
- 6 years ago
- Views:
Transcription
1 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October pm-3.00pm Conference Room 1, Trafalgar House, King Street, Dudley
2 PUBLIC MEETING OF THE TRUST BOARD 1.00pm, Thursday, 5 th October 2017 Conference Room 1, Trafalgar House AGENDA Culture and Conduct Protocol We are a values-led Board. We place quality of care and safeguarding the needs of our patients at the heart of everything we do. We work consciously as a team to support and constructively challenge each other in the best interests of service users, their carers and families. We champion the interests of staff and acknowledge that they are working well in challenging times. We seek to ensure value for money at all times through efficient use of our resources in the delivery of services and achievement of standards. We welcome the rigour of debate with fellow Board members, drawing upon a range of different experiences and perspectives and applying the Nolan principles of Selflessness, Integrity, Objectivity, Accountability, Openness, Honesty and Leadership. ITEM Purpose Board Lead Format Timings 1 Apologies Mr Reid Oral 1.00pm 2 Declarations of Interest For Board members to declare any relevant interests in items on the agenda Mr Reid Oral 3 Minutes of the Previous Meeting To approve the minutes of the Board meeting held on 7 September 2017 Approval Mr Reid Enc 1 4 Matters Arising/Action Schedule Continuity Mr Reid Enc 2 5 Summary Report of Confidential session of Trust Board held on 7 September Chief Executive Officer s Overview (including written summary of strategic publications and headlines) 7. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS Information Mr Reid Enc 3 Information Mr Axcell Enc pm 7.1 OnBoard Visits Governance Arrangements Assurance Mr Axcell Enc pm Trust Integrated Performance Report (Month 5) including the Performance Dashboard and Contract Performance Dashboard Assurance Mr Davies Enc pm a Quality Quality & Safety Committee Chair s Report Assurance Dr Murphy Enc pm b Quality Report Assurance Dr Murphy Enc 8
3 7.1.3 a ITEM Purpose Board Lead Format Timings Finance & Performance Finance & Performance Chair s Report from meeting held on 25 th September 2017 Assurance Mr Turner Enc pm b Finance & Performance Committee Minutes from meeting held on 30 August 2017 Assurance Mr Turner Enc 10 c Audit Committee Chair s Report from meeting held on 19 th September Assurance Mr Lancaster Enc 11 d Audit Committee Minutes from meeting held on 19 th September Assurance Mr Lancaster Enc 12 e Finance Report Assurance Mr Davies Enc 13 f Cost Improvement Programme (CIP) Progress Report Assurance Mr Davies Enc a Workforce Workforce Committee Chair s Report (report from meeting held on 25 September 2017 Assurance Mr Turner Enc pm b c Workforce Committee Minutes from the Extraordinary meeting held on 4 th September 2017 (Ratified) Workforce Performance Report Assurance Assurance Mr Turner Mrs Williams Enc 16 Enc Medical Directors Report Assurance Dr Gingell /Dr Weaver Enc pm 7.3 Director of Nursing Report Assurance Ms Musson Enc pm 7.4 Quality Improvement Priorities & CQUINN Quarterly Progress Report Assurance Ms Musson Enc pm 7.5 Enhancing Quality through Safer Staffing Levels - Monthly Exception Report Assurance Ms Musson Enc pm 7.6 Director of Operations Report Assurance Mrs Writtle Enc pm 7.7 High Level Operational Risk Register Assurance Mrs Musson Enc pm 8. STRATEGIC DEVELOPMENT & DIRECTION 8.1 MERIT Progress Report Assurance Mr Axcell Enc pm 9. FOR ASSURANCE 9.1 MExT Chair s Report from 26 th September 2017 Assurance Mr Davies Enc pm 10. ANY OTHER BUSINESS

4 ITEM Purpose Board Lead Format Timings 11. QUESTIONS FROM MEMBERS OF THE PUBLIC Questions from members of the public pertaining to agenda items. Oral 12. DATE AND TIME OF THE NEXT MEETING Thursday, 2 November 2017 at 1.00om, The Board Room, Canalside, Bloxwich
5 Enc 1 MINUTES OF THE TRUST BOARD MEETING OF DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST Present Mr B Reid Mr M Axcell Mr J Burbeck Mr R Davies Dr K Gingell Mr J Lancaster Dr S Murphy Mrs R Musson Mr H Turner Dr M Weaver Mrs A Williams Mrs L Writtle Held at 1.00pm on Thursday, 7 th September 2017 The Board Room, Canalside, Bloxwich PUBLIC SESSION Chair Chief Executive Officer Associate Non-Executive Director Interim Director of Finance, Performance and IM&T Joint Medical Director Non-Executive Director Non-Executive Director Acting Director of Nursing Non-Executive Director Joint Medical Director Acting Director of People Interim Director of Operations In Attendance Mr P Lewis-Grundy Mrs L Wix Mrs T Cross Mr K Parsons Company Secretary Corporate Governance Support Officer (minutes) Patient Experience Officer (for item 103 only) Service User ITEM 103. PATIENT STORY ACTION The Chair welcomed everyone to the meeting. Mr Axcell welcomed and introduced Mrs Cross and Mr Parsons, to the meeting advising members that Mr Parsons would share his experience as a Service User. Mr Parsons told the Board that his symptoms had started in 2010 although it had taken sometime before he was diagnosed and offered appropriate treatment. He was deemed unsuitable for psychological treatment on the basis that he was receiving treatment for a gambling addiction from a charitable organisation, although he had contested this as he was not receiving treatment for his mental well-being. Mr Parsons advised that he had received treatment at Woodside and was referred to a psychologist at Halesview. He had applied for a Personal Independent Payment and the Trust had written to the Department for Work and Pensions in support of this application, although Mr Parsons hadn t been in total agreement with some of the content and these issues had since been addressed. Page 1 of 22
6 The Chair sought confirmation that Mr Parsons was content with the treatment he was currently receiving and Mr Parsons confirmed this to be the case, although there had been some communication issues between the Trust and his GP and he was fearful that he would be discharged from the service and would need to be re-referred as his mental health would deteriorate under those circumstances. Dr Gingell confirmed that she was aware of the issues Mr Parsons had raised and was working towards resolving them with him. Mrs Cross advised the Board that Mr Parsons intended to stay for the remainder of the public session. Mrs Cross left the meeting APOLOGIES & WELCOME Apologies had been received from Mr P Rana, Non- Executive Director. The Chair welcomed Mr Burbeck, a recently appointed Associate Non-Executive Director, to his inaugural Board meeting of the Trust DECLARATIONS OF INTEREST Members were asked to disclose any interest they may have, direct or indirect, in any of the items being considered during the course of the meeting and to note that those members declaring an interest would not be allowed to participate in the consideration, discussion or vote on any issue relating to that item. Dr Murphy reminded the meeting that he was also a Non- Executive Director at Birmingham Community Healthcare NHS Foundation Trust. Mrs Writtle declared an interest being the Director of Operations at Black Country Partnership Foundation Trust as well as interim Director of Operations at Dudley & Walsall Mental Health NHS Trust. There were no other interests declared in addition to those already recorded on the Register of Interests MINUTES OF THE PREVIOUS MEETING To approve the minutes of the meeting held on 3 rd August Minute 88.1 Matters Arising Dr Weaver requested that the third paragraph be amended Page 2 of 22
7 to read Dr Weaver expected that the proposed locality based model would generate CIP savings and the complex care based model might generate income. RESOLVED: That the minutes of the meeting held on 3 rd August 2017 be approved and signed by the Chair, subject to the amendment above being made MATTERS ARISING/ACTION SCHEDULE All items were either complete or had a future completion date. The Chief Executive made reference to the ongoing action 24.1 On Board visits. The Chair suggested and it was agreed that this be discussed at the forthcoming Board Development Session on 18 September 2017, revisiting the purpose of on Board visits and thereby developing an appropriate Protocol and process for the visits. During the ensuing discussion a number of suggests were made to include in a process which would feed into the discussion on 18 September ACTION: Include discussion on the On Board Visit Protocol and Process on the Agenda for the Board Development Session on 18 th September RESOLVED: That the matters arising and the assurance given where those actions have been completed be noted SUMMARY REPORT OF THE CONFIDENTIAL SESSION OF TRUST BOARD HELD ON 3 rd AUGUST Members noted the content of the confidential summary of the meeting held on 3 rd August RESOLVED: That the Board received the report for information CHIEF EXECUTIVE OFFICER S OVERVIEW The Chief Executive presented his report and gave an update on the following: Transforming Care Together Mr Axcell advised that the proposed date of 1 October 2017 for the acquisition of the Page 3 of 22
8 Trust by Birmingham Community Healthcare NHS Trust under the TCT Partnership had been delayed. This had been communicated to staff across the three organisations. NHSI were reviewing the TCT Full Business Case and an update on the anticipated timeframe for integration would be advised once it had been clarified. Mrs Williams confirmed that the TUPE consultation process would be unaffected by the change in timescales and the work already undertaken would remain valid. MERIT Vanguard The MERIT Vanguard continued to make excellent progress in developing a consistent approach to Crisis and Recovery. The programme was in discussion with NHS Improvement and NHS England regarding the level of funding available to continue the Vanguard during 2017/18 A new website was available for those in crisis to identify the resources available across the West Midlands. Walsall CCG Healthy Walsall Partnership Board Walsall Together had not met during the month although it was progressing and discussion continued around an alliance approach to place based care. Dudley MCP - During August Dudley CCG announced the decision on the bidders that would go through to the next stage of the MCP Procurement process. Following an initial evaluation, the CCG in partnership with Dudley Council, would enter into a dialogue process with a consortium involving four local NHS Trusts and local GPs. Mr Axcell advised that the four trusts were Birmingham Community Healthcare NHS Foundation Trust, The Dudley Group NHS Foundation Trust, Dudley and Walsall Mental Health Partnership NHS Trust and Black Country Partnership NHS Foundation Trust and noted that the proposed contributors were listed as individual organisations. Mr Axcell added that he had attended the Dawn Jones Art prize event. Over Thirty entries had been received for the prize all of which he commended. Two winners had been selected; one being a painting and the other a piece of poetry. Mr Axcell reminded the Board that the Mental Health Forum and the AGM were taking place on Friday 22 September 2017 at the New Walsall Art Gallery. The Forum Healthy Mind, Healthy You would commence at 10.00am, followed by a light lunch and the AGM at 1.00pm. The Staff Awards would take place at 6.30pm at Bescot Stadium Walsall. The Chair encouraged the Board to support the events. RESOLVED: That the Board Page 4 of 22
9 Considered and discussed the information contained within the report, and noted for assurance the actions identified throughout the report. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS 110. Trust Integrated performance Dashboard & Contract Performance (Month 4) Mr Davies presented the report advising that it made reference to performance across the four domains, Quality and Safety, Service User Experience, Efficiency and Resources and summarised the main points. The Performance Dashboard included Trust wide and individual service line data with green RAG rating against those targets that were being achieved. He noted that there had been an increase in the level of incidents reported which may have demonstrated an improvement in the reporting culture within the Trust. The vacancy rate was 12.4% and RAG rated red this was explored further in the Workforce Performance Report. Referring to the Contract Performance report, Mr Davies advised that the Acute Adult Inpatient Stays of 40 days or more stood at 76% against a target of 95% of patients and activity was performing 4% above the block contract figures. The Chair questioned the correlation between the achievement of the CIP included in this report and those included in the detailed CIP update report. Mr Turner commented that the CIP shortfall had been debated at the Finance Committee and that he would provide further detail when as Chair of the Committee he would report on the meeting of the Finance and Performance Committee. RESOLVED: That the Board noted the content of the report Quality & Safety Committee Minutes from the meeting held on 18 th July The Chair of the Committee presented the minutes of the meeting. RESOLVED: That the Board received the minutes for information and assurance. Quality Report Mrs Musson presented the Quality report for month 4 which made reference to: Page 5 of 22
10 A summary of incidents Operational Service Line Reports Safety Alert Broadcasts (SABs) Safeguarding Performance Framework The Quality and Safety Committee had not met in August and therefore the Committee would review the Quality Report for months 4 and 5 when it met on 13 September Mrs Musson advised that there had been a significant increase in the number of incidents reported on inpatient wards over the month and a deep dive had been undertaken to identify underlying reasons for this. There had been stress in the system on Ambleside Ward. The team on the Ward had been provided with additional support and the outcome of this had been positive. In Urgent Care there a number of patients had self-harmed, this would be monitored and any appropriate action taken to address the position. Mrs Musson confirmed that there had been three under 18 admissions through early intervention services. The Trust continued to report and discuss Under 18 admissions with both NHSE and NHSI and the Quality & Safety Committee would undertake a deep dive in this regard at the meeting in November. Mrs Musson advised that there was pressure on Tier 4 beds nationally and Dr Murphy suggested that the increased reporting at a national level would highlight the issues faced by Trusts nationally. Mr Burbeck queried whether there was a process in place with regard to reviewing the delayed discharge of patients. Mrs Writtle confirmed that each delay was reviewed and work undertaken with clinicians to identify appropriate placements, at that stage if a placement was not available there was an escalation process through to the relevant Local Authority and or CCG. Whilst Mr Burbeck acknowledged that the process was robust there had still been a deterioration in month in Dudley. Mrs Writtle advised that the figures were based on a 3 month average, and that there were a few patients that were having an impact on reported figures The Chair queried whether the Trust was financed appropriately by CCGs for delayed transfers and what the operational implications were. Mrs Writtle advised that the Trust was paid on a block contract, although there were occasional case by case agreements but these were very infrequent. Mrs Writtle referred to the contract review discussions with CCGs that she had reported to Board on previous occasions and as part of that dialogue she was sharing information on the acuity of patients. Referring to delayed transfers from an operational perspective Mrs Writtle Page 6 of 22
11 confirmed that there were beds available, although a patient in Dudley may be admitted to a Walsall bed and vice versa Mr Axcell advised that the graph evidenced an increase in delayed transfers some 10 months previously - it had been identified that the instances of delayed transfers were not being recorded accurately with inconsistency across the Trust regarding this. Mrs Writtle advised that since that time the Bed Management policy had been implemented which had impacted positively on staff reporting delayed transfer of care cases and which was reflecting in the reported figures. RESOLVED: That the Board received the report for information and assurance Mental Health Act Scrutiny Committee Chair s Report In presenting the report, Mr Reid provided an overview of the topics discussed and drew particular attention to candid and positive contribution of the Committee members. The Chair sought to ensure that the Committee would continue to function during the delay in proposed integration of the TCT partner Trusts. RESOLVED: That the Board received the report for information and assurance Mental Health Act Scrutiny Committee minutes from meeting held on 10 August The Chair of the Committee presented the draft minutes of the meeting and advised that they were for information rather than approval as they had yet to be ratified by Committee members. RESOLVED: That the Board received the minutes for information and assurance Finance & Performance Committee Chair s Report In presenting the report Mr Turner referred to the following: Finance Report - The financial position to the end of July 2017 showed a 779,000 surplus which was 47k ahead of the plan to date (based on the planned annual surplus of Page 7 of 22
12 1,839,000). It was noted that both Dudley and Walsall contracts were over-performing to the value of 130k and 447k respectively to Month 4 and the Director of Operations had undertaken a review of contract delivery in order to identify areas that could be focused upon with a view to stemming demand and/or placing challenge back to commissioners around demand management. It was proposed to undertake a joint Trust/Commissioner mid-year contract review to highlight issues, concerns and risks and an internal meeting between finance, operations, the contract team and Director of Nursing was scheduled to gather evidence to present to the CCGs in support of additional financing to fund the over performance. In response to the Chairs question Mrs Writtle advised that the Trust was in a strong position on contract performance and that, together with data from the acuity tool, it would be possible to demonstrate that patients were more challenging. Additionally, the Trust was performing to targets on community lines and there had been improvements to the transformational work and that overall there was a strong evidence base to present to the Trust s commissioners Mr Turner confirmed that the Committee had reviewed year end projected forecasts and it was highlighted that there were financial pressures within Corporate and Inpatient service lines and the protocol of the Workforce Committee would be replicated with budget holders being invited to the next Finance & Performance Committee meeting to outline their proposals to reduce the deficit. Mr Turner confirmed that the Committee had received a paper outlining the risks and required mitigations in order to achieve the 1.839m surplus control total in year. The potential risks highlighted ranged from 0.8m through to 2.4m with a potential impact of around 1.4m and members requested that these risks be reviewed in light of the financial assumptions included in the forecast. Mr Turner advised that despite these financial pressures, there was an increased level of confidence that delivery of the financial plans to the 1.8m surplus control total would be achieved. Referring to CIPs, Mr Turner advised that performance had improved during August following the release of vacancies the position now reflected a delivery of 2.8m against the 3.8m target for the year. Even though progress was positive it was highlighted to the Finance and Performance Committee that there was still a reliance on non-recurrent means of delivery against the CIP target which would have an impact on next financial years CIP target. Mrs Williams advised that the Workforce Performance Report reflected Page 8 of 22
13 this position. Mrs Writtle confirmed that the release of vacancies which had generated 1m CIP was a one off and whilst ongoing vacancies in the normal cause of business would make some savings for the Trust savings on a similar scale would not be realised again. Mr Turner reiterated that there remained a CIP shortfall of 1m. Mr Davies advised that further work undertaken by the finance team had identified an additional 500, ,000 reducing the CIP shortfall further to 400,000. The Chair sought clarification that were the due diligence process in preparing the TCT Full Business Case be repeated it would confirm the position that the Board were being advised, i.e. a CIP shortfall of 400,000 and evidence that 3.3m of CIP had been identified and would be delivered. Mr Davies confirmed this to be the case. Referring to the CIP shortfall for 2018/19, Mr Turner advised that this may be in the region of 4m next year, the Committee recommended a different bottom up approach to encourage ownership of CIPs at all levels. In light of the delay in thetct transaction there was a need to put in place a plan for next year that would have a financial impact from 1 April The Chair queried whether any development had been made in relation to the review of the use of the Trust s estate. Mr Davies confirmed that a presentation was proposed on the estates utilisation to the Private Board meeting however with the Boards agreement this was deferred to the Board Development session being held on 18 th September. Mrs Writtle commented that a mapping exercise had been undertaken as part of the TCT clinical workstream and this intelligence could be reviewed at the Board Development session and Mrs Musson concurred, adding that any resulting actions had to be Quality Impact Assessed. RESOLVED: That the Board received the report for assurance and information and noted the content and endorsed the decisions taken by the Finance & Performance Committee Finance & Performance Committee DRAFT Minutes from the meeting held on 24 th July The Chair of the Committee presented the draft minutes of the meeting advising that they were for information only as they had yet to be ratified by Committee members. RESOLVED: That the Board received the minutes for information and assurance. Page 9 of 22
14 110.7 Finance Report Mr Davies presented the report and referred to the following in support of the Finance & Performance Committee Chairs report earlier in the minutes: The Trust had delivered a month 4 surplus of 779,000 and this represented a favourable variance of 47,000 against the planned Year to Date (YTD) surplus of 732,000. This planned YTD figure forms part of the plan to deliver a month 06 surplus of 1.068m and a full year surplus of 1.839m. Pay expenditure was 160,000 in surplus against budget to date, which had been driven by vacancies across the Trust. Bank & Agency spend equated to 502,000 in month and despite the increase in costs within the month, agency spend was still currently ahead of plan by 199,000 in relation to the overall 4.05m Agency target for the year. RESOLVED: That the Board received the report for assurance and noted the content Cost Improvement Programme (CIP) Progress Report In presenting the report, Mr Davies advised that 19 schemes were identified in 2017/18 to achieve the CIP target of 3,780,000. Of these 19 schemes, three had delivered and had been closed, one had delivered and risks were being monitored, and nine were progressing with a further six schemes being delivered. RESOLVED: That the Board received the report for assurance and information and noted the content Workforce Committee Chair s Report In presenting the report Mr Turner advised that Mrs Williams had chaired a meeting of members of the Workforce Committee held on Monday 4 th September and she confirmed that the focus had primary been on mandatory training and appraisals. There had been an improvement and appraisal compliance was at 86% which was above the target of 85% and mandatory training was also above the 90% target at 92.6%. Mrs Williams confirmed that the meeting had also considered the Memorandum of Understanding for the training passport Page 10 of 22
15 which enabled staff to move between Trusts with any mandatory training transferring with them. This would be ratified at the next meeting Mr Turner confirmed that the focus of the next Workforce Committee meeting would be to review the potential for sustained performance against targets going forward. RESOLVED: That the Board received the report of the meeting for assurance and information and noted the content Workforce Committee Minutes from the meeting held on 24 th July The Chair of the Committee presented the draft minutes of the meeting advising that they were for information only as they had yet to be ratified by members of the Committee. RESOLVED: That the Board received the minutes for information and assurance Workforce Performance Report Mrs Williams presented the report and advised that the Workforce Committee Chair s report had covered the pertinent points of the Workforce Performance Report. RESOLVED: That the Board noted the updates on key current workforce agenda items 111. Medical Directors Report In presenting the Medical Directors report, Dr Gingell referred to the following: General Data Protection Regulations Dr Gingell referred to the changes that would come into force in May 2018 and the potential financial implications for Trusts across the country and the issues would be discussed in the relevant committees to identify any issues for the Trust Mr Lewis- Grundy advised that these regulations would supersede elements of the Data Protection Act 1998 and he would work with the Information Governance team to provide Board with the assurance that the Trust would be compliant with the provisions in the new regulations Expansion of medical student intakes Dr Gingell advised that the Secretary of State for Health had announced an Page 11 of 22
16 increase of 1,500 medical school places from 2018/19, and this had been welcomed by Health Education England (HEE) and other stakeholders as a key opportunity to expand the medical workforce to meet future needs whilst reducing the reliance on overseas doctors. Dr Gingell advised that Psychiatry was less popular than other disciplines and questioned the impact that the expansion of medical student intakes would have in the short term. Recruitment Dr Gingell stated that Psychiatry is currently the specialty with the highest number of unfilled medical training posts at 35%, followed by histopathology (28%) and general practice (16%). The Trust continued to experience difficulties with recruitment and had been unable to recruit to three Specialty and Associate Specialist (SAS) grades in the Dudley locality. Mr Lancaster queried whether the Trust had feedback from candidates and in response Dr Gingell advised that there had been positive feedback following interviews with people keen to join organisation and the Trust had a high staff retention rate. Dr Weaver concurred, adding that in some service models, especially locality based teams, this risk could be mitigated through appropriately trained nursing staff undertaking some duties previously carried out by clinicians. Dr Gingell confirmed that there had been three occasions where under 18 s had been admitted to the adult in-patient wards in the last four weeks and one patient had been waiting for a Tier 4 bed for 9 weeks on the paediatric ward and had required intense support from the icamhs team and this had been escalated to the CCG, the acute hospital and NHSI and had been raised as a serious incident. The Chair queried whether the Trust could have refused to admit the patient as the environment was inappropriate and Mrs Musson advised that the Board had previously reviewed a risk assessment outlining the issues in admitting Under 18s and had concluded that the Trust had a duty of care. Dr Gingell advised that this was not unusual situation and other Trusts admitted Under 18s to cover the gap in care for adolescents, that the nurses took very good care of the individuals and it was appropriate for brief periods. Mrs Writtle advised that other Trust s admitted Under 18s however they were managed differently through the 136 suite and with community support. Mr Axcell queried whether in managing Under 18 admissions Trusts were understating the shortage of Tier 4 beds nationally and whilst there were beds in Birmingham there were no Tier 4 beds in the Black Country. Dr Murphy reiterated that the Quality & Safety Committee had a deep dive in Under 18 admissions scheduled for November and would report the findings to the Board via the Committee Chair s report to the Board in December. Page 12 of 22
17 ACTION: Report the findings of the Quality & Safety Committee deep dive into under 18 admissions via the Committee Chair s to the Board in December. Mrs Musson Referring to the mortality report, Dr Gingell advised that there were 12 cases falling inside the scope of the report two unexpected and one incident was being investigated as a Serious Incident. There had been one case where the individual had died of natural causes at a young age and the mortality tool was being utilised to identify whether this related to the patient s mental health issues. Dr Gingell advised that the report included the quarterly update on the Guardian of Safe Working and this was provided for information. RESOLVED: That the Board: Received the report for assurance and information and noted the content Received and noted the content of the Guardian for Safe Working Report 112. Mortality Review Policy In presenting the report, Dr Gingell advised that from September 2017 the Trust was required to have a policy outlining how deaths are investigated within the organisation. The policy had been influenced heavily by a number of national publications, including: Mazars report into Southern Health NHS Foundation Trust (2016) Learning, Candour and Accountability (CQC 2016) National Guidance on Learning from Deaths (National Quality Board 2017) Subject to approval of the policy by the Board it would be published on the Trust s website in accordance with the requirements of national guidance. Dr Gingell confirmed that the policy had been reviewed by the Mortality Surveillance Group Mr Turner queried who was the nominated Non-Executive Lead. Following confirmation that Dr Murphy was happy to take on this role from the Chair this was endorsed by the Board. RESOLVED: That the Board approved the Mortality Review Policy and agreed to its publication on the Trust s website and endorsed Dr Murphy as the Non-Executive Lead for Page 13 of 22
18 Mortality Director of Nursing Report In presenting the Director of Nursing Report, Mrs Musson advised that as previously stated in the Joint Medical Directors report, there had been three under 18s admissions onto adult in-patient wards and the Trust s Quality and Safety Committee would be conducting a deep dive looking at the impact of the CAMHS 3.5 services and also any lessons learnt regarding the under 18 admissions. In all cases there had not been timely availability of a Tier 4 CAMHS bed. Mrs Musson made reference to: Safer staffing the acuity of patients was having an impact on rostering and consideration was being given to adopting the measure utilised by acute hospitals Peer support Funding had been secured for a 6 month pilot scheme and this initiative had been well received and approved at MExT Annual report on Practice placements for Student Nurses the Trust was working closely with feeder universities and was planning a recruitment day in September to encourage student nurses to apply in time for the January 2018 intake. RESOLVED: That the Board received the report for assurance and information and noted the content CQC Action Plan In presenting the report Mrs Musson advised that the Trust s CQC Action Plan addresses all of the identified areas of concern and provided detailed assurance to the Trust, public, CQC and partners that appropriate action was being taken in the relevant areas. The report provided a summary of the current position and identified current risks, mitigations and perceived residual risks that may remain upon completion of the agreed actions. She confirmed that the red RAG rating for rapid tranquilisation would be downgraded to amber due to staff undertaking training. Mr Burbeck queried how the risks identified through the CQC Action Plan were reflected in the Operational Risk Register elsewhere on the Agenda. Mrs Musson advised that the CQC Action Plan had been formulated in response to concerns raised by the CQC, the operational risk register Page 14 of 22
19 presented elsewhere on the Agenda to Board reported only those high level risks rated Red. Mr Burbeck queried the RAG rating of the Action Plan. In response Mr Axcell advised that amber was used in some cases to show actions which, whilst they were being progressed would not be RAG rated green until they had been completed and tested. Mr Burbeck suggested, and it was agreed, that the RAG rating of the Action Plan be amended in line with that used for Board and Committee actions incorporating an additional Blue rating for those actions that were progressing to schedule. ACTION: The RAG rating of the Action Plan be amended in line with that used for Board and Committee actions incorporating an additional Blue rating for those actions that were progressing to schedule. Mrs Musson Mr Lancaster commented that the Trust s aspiration was to be rated outstanding and to achieve this, the RAG ratings would have to be green against each action. The Chair concurred and asked when a further CQC inspection was likely to take place. Mrs Musson advised that in accordance with the revised inspection regime a well led review would take place annually, the timetable for more targeted inspections under the new regime would take place based on CQC rating. RESOLVED: That the Board acknowledged the current position and received assurance from the planned mitigating actions Health & Safety Annual Report In presenting the report, Mr Davies advised that the annual report highlighted action taken by the Trust to protect its employees, volunteers, contractors, clients and service users, from Health and Safety Risks and covered the period from 1 st April 2016 to 31 st March The Chair requested an update on fire safety and Mr Davies confirmed that every building across the estate had an annual fire risk assessment (FRA). The Chair queried further given that the FRAs had not highlighted the compartmentation issue. Mr Davies assured Board that action had been taken to resolve this issue at Bushey Fields Hospital and progress was being made at Dorothy Pattison Hospital. The FRAs for the Bloxwich site had highlighted some issues which it would be clarified were captured on the Trust s Operational Risk Register. ACTION: Clarify that the risks highlighted in the FRAs for Bloxwich were captured on the Operational Risk Mr Lewis- Grundy Page 15 of 22
20 Register. The Chair queried whether the water standards continued to be monitored and Mrs Musson confirmed that the Water Safety Group provided quarterly updates to the Quality & Safety Committee and that water testing results were consistent and there was confidence in the testing process. RESOLVED: That the Board received and approved the annual report to continue to support The Health and Safety Strategy Enhancing Quality through Safer Staffing Levels Monthly Exception Report In presenting the report Mrs Musson advised that the data included therein represented July 2017 and a monthly trend analysis for a 12 month period. Across the inpatient areas the overall fill rates were %, with 98.58% for registered staff and % for care staff which indicated the Trust was meeting the optimum level of fill rates. There was one ward (Kinver) to note as exceptions, whereby staff fill in part was within the lower category and an impact assessment had been completed that provided assurance that safe staffing levels had not been compromised. Where staff have concerns about staffing levels the reporting takes place through the Trusts incident reporting processes and Mrs Musson had a high degree of confidence in the escalation system when there was one qualified member of staff on night duty. In July no incidents were reported related to safer staffing in inpatient services. RESOLVED: The Board: Noted the monthly data return submitted, providing details of planned and actual staffing at ward level. Data represented July 2017 and a 12 month trend analysis. Noted the work underway to enable the most efficient safe and effective use of nurse staffing in inpatient service, which would focus on all professional groups, including therapists. Noted the data relating to internal Trust standard of two qualified staff per shift and received assurance on mitigations in place Director of Operations Report Mrs Writtle presented the report providing updates on the four service lines, Urgent & Access, Community, Early Intervention and Inpatients. Page 16 of 22
21 Referring to Inpatient Services, she advised that the recently revised Inpatient management structure had been fully recruited to, with post holders in place. The new structure would ensure adequate capacity to deliver safe services and also focus on CIP delivery and transformation project work. Mrs Writtle provided and update on the Instant Access to Psychological Therapies (IAPT) advising that the final report had been shared with the service, NHSI and Commissioners and a joint planning event was scheduled for 25 th September to discuss the recording data, staffing levels and accessing staff with appropriate training with stakeholders. An improvement implementation plan would be presented to the Quality & Safety Committee later in the year. Referring to the Section 75 agreement, Mrs Writtle had met with the new manager and was more positive about closer collaborative working going forward and would report key outcomes to the Board at the meeting in October via the Director of Operations report. ACTION: Section 75 outcomes to be reported to the Board in October via the Director of Operations report. Mrs Writtle RESOLVED: That the Board received the report for assurance and information and noted the content Emergency Preparedness, Resilience and Response (EPRR) Assurance In presenting the report, Mr Axcell advised that it had been compiled by an external provider who provide Emergency planning services to the Trust and that under the Health and Social Care Act 2012, all NHS Trusts must comply with the NHS England Core Standards for Emergency Preparedness, Resilience and Response (EPRR). The assurance process required NHS Trusts to undertake an annual self-assessed update on their progress against the Core Standards and this was appended to the report for approval. Referring to the Shelter and Evacuation Planning at Inpatient Sites whilst the Trust already had a comprehensive and robust suite of local evacuation plans for its inpatient facilities at Bushey Fields, Bloxwich and Dorothy Pattison Hospitals which had been successively and successfully tested by real incidents it was anticipated that a further practice would be conducted shortly. Mr Burbeck queried whether other buildings that were not managed by the Trust and were used by Trust patients to access services were similarly prepared and had evacuation plans in place. Mr Axcell confirmed that Page 17 of 22
22 he would clarify this point. ACTION: Clarify whether buildings that did not have inpatient capacity but were used by Trust patients to access services were similarly prepared and had evacuation plans in place. Mr Axcell RESOLVED: That the Board: Approved the contents of the update and associated EPRR Core Standards return. Agreed proposed next steps in maintaining ongoing compliance in the context of the TCT process Service Experience Desk Report (Q1) In presenting the report, Mr Axcell advised that during the reporting period the Trust had received 34 complaints, 84 concerns, 113 compliments, 2 claims, 30 enquiries and 4 suggestions. Compliments, suggestions and claims had risen slightly since Q4, whilst complaints, concerns and enquiries had marginally decreased. Compliments continued to make up the largest feedback category (113) stating that the Trust is particularly effective and responsive. The information had been shared with Heads of Service and teams, taken to Service Line meetings and examples and numbers included in team brief. Dr Murphy commented that there were identified themes within the report and the Net Promoter Score had dipped and he suggested, and it was agreed, that the Quality & Safety Committee would undertake a deep dive into the data provided in the report. ACTION: Quality & Safety Committee undertake a deep dive into the Net Promotor data provided in the SED report. Mrs Musson RESOLVED: That the Board received the report for assurance and information and noted the content High Level Operational Risk Register In presenting the Risk Register, Mrs Musson advised that the report provided the Board with the Red Operational risks held across the Trusts Risk Registers for the period 30 th August 2017 and provided information on: Page 18 of 22
23 Any new red risks being escalated to the High Level Operational Risk Register. Any red risks being downgraded from the High Level Operational Risk Register Any updates to red risks currently held on the High Level Operational Risk Register. There were currently 11 risks being presented as part of this report and the report remained unchanged in month. Risk 314 paper and electronic records. Mr Burbeck queried whether the TCT pause should be included on the register and whilst Mr Lewis-Grundy advised that there was a strategic risk defined in the Board the Chair commented that the delay may also generate operational risks and requested that the existing TCT operational risks received by the Board in private at is meeting in June 2017 be reviewed again in light of the delay. ACTION: Existing TCT operational risks received by the Board in private at is meeting in June 2017 to be reviewed again by the Quality & Safety Committee in light of the delay. Mrs Musson Referring to the red RAG rated Risk EF002 fire safety management within the Trust, Mr Turner stated that there were no corresponding completion dates for the actions and Mr Davies advised that whilst some actions were being progressed in relation to electricity at work, a programme of mattress replacement introduced and fire marshal training this did not mitigate the risk sufficiently to reduce the overall risk rating to Green. RESOLVED: That the Board approved the content of the High Level Operational Risk Register STRATEGIC DEVELOPMENT & DIRECTION Annual Plan Quarterly Review Mr Axcell advised the Board that the Trust s priority activities for 2017/18 had been agreed through a number of workshops with Executives and Non-Executives and the plans were shared with staff through Team Brief for comment and were agreed and ratified by the Board in April The report included an update on actions taken and progress made in Quarter /18 and he confirmed that there were no red RAG rated actions. The Annual Plan would be reviewed in light of the TCT development. Page 19 of 22
24 RESOLVED: That the Board received the report for assurance and information and noted the content LEADERSHIP, CULTURE & WORKFORCE Quarterly Update Report on Staff Engagement Process In presenting the report, Mrs Williams advised that the report provided assurance and updates on the ongoing actions arising from the 2017 Staff Survey, preparations for the 2017 Staff Survey and of TCT collaborative work being undertaken in terms of impact on staff engagement. A number of Resilience events were plan for staff in relation to the TCT which offered general advice and coping strategies during the consultation period following integration. Mr Burbeck queried whether there were mechanisms in place to communicate changes to staff given the TCT development and Mrs Williams confirmed that Change Champions and Engagement Champions were available to address staff concerns. The Chair queried the number of shared posts there were under the TCT umbrella and whilst Mrs Writtle was unaware of the precise figure she believed that there were a number of shared clinical and support posts and it was unlikely that these would continue in the longer term given the additional work involved for individuals that they had been agreed on a short term basis. RESOLVED: That the Board received the report for assurance and information and noted the content FOR ASSURANCE MExT Chair s report from 29 th August In presenting the report Mr Axcell advised that MExT had received the following items: Chief Executive s Update Emergency Preparedness, Resilience and Response (EPRR) Assurance, which was agreed for consideration by the Board and is a separate item on the Agenda for Board A Business Case to pilot a peer review project which MExT agreed Service Line Reviews Verbal updates from the Joint Medical Directors, the Nursing Director, the Operations Director the HR Director and the Freedom to Speak Up Guardian Written reports from the Director of People regarding Page 20 of 22
25 the TCT Management of Change Briefing and the Director of Finance on the Month 4 Financial position. Service Development/Changes Social Inclusion/S75 and POG update Communications update He confirmed that the Committee had also received a presentation and updates on the Walsall Mental Health Transformation Programme and Transforming Care Together (TCT) Partnership Integration. RESOLVED: That the Board noted the content of the report for information and assurance ANY OTHER BUSINESS Mr Parsons asked why the TCT integration had been delayed and the Chair advised that the regulators had asked for more time to review the assumptions included in the business case. Mr Parsons advised that following integration the TCT would need to work with a lot more councils and each council operated differently and the decisions they take would affect the income of the new Trust. Mr Axcell advised that there was already collaborative working with councils and work was ongoing to ensure that this was maintained. Mr Parsons referred to the paper based and electronic patient record and whether information was synchronised between the two and Dr Gingell confirmed this to be the case advising that the Trust only had to be notified once of any changes to contact information. Mr Parsons queried whether the Trust s financial position affected recruitment and Dr Gingell advised that the Trust s financial position was robust with the ability to pay doctors but that there was a shortage of doctors nationally, particularly in psychiatry. In response to Mr Parsons query related to adverse publicity, Mr Axcell confirmed that the Trust had a Communications Team who monitored local and national press bulletins and provided quarterly reports to the Board DATE AND TIME OF NEXT MEETING The next Trust Board meeting would take place at 1.00pm on 5 th October, Conference Room 1, Trafalgar House, King Street, Dudley. Meeting closed at 3.32pm Page 21 of 22
26 Signature.. Date. Mr B Reid, on behalf of the Dudley and Walsall Mental Health Partnership NHS Trust Board Page 22 of 22
27 MATTERS ARISING FROM PUBLIC MEETINGS Enc 2 RAG Action Outstanding Completion date in the future Action Completed Item No Date Added 7 September July September September June 2017 Action Responsibility Due Date Update High Level Operational Risk Register Existing TCT operational risks received by the Board in private at its meeting in June 2017 to be reviewed again by the Quality & Safety Committee in light of the delay. Workforce Committee Chair s report Following completion of the Nurse Establishment Review, review the Safer Staffing Policy and Standard in August Service Experience Desk Report Q1 Quality & Safety Committee undertake a deep dive into the Net Promotor data provided in the SED report. Medical Directors Report Report the findings of the Quality & Safety Committee deep dive into under 18 admissions via the Committee Chair s to the Board in December. Quality & Safety Committee Chair s Report Undertake a scoping exercise related to the fire issues to be reviewed by the Mrs Musson Mrs Musson/Mrs Writtle Mrs Musson Mrs Musson Mr Davies November 2017 November 2017 November 2017 December 2017 December 2017 The Quality & Safety Committee reviewed the SED report in September although a deep dive into the Net Promoter data was not undertaken. Item deferred to November. 1
28 Item No. Date Added Action Responsibility Due Date Update Audit Committee with a report back to Board via the Audit Committee Chair s Report 48 1 June 2017 Chief Executive s Overview Report Audit Committee to review the report on the cyber-attack in September to include assurance that there is a robust process in place with Terrafirma keeping the Trust s IT department appraised of any issues. Mr Davies October 2017 Audit Committee agenda item at the meeting on 19 September The Committee was assured that the IT provider TeraFirma was ISO registered and that they had robust systems was in place to prevent the Trust being the victim of any future cyber attacks. Completed. Closed September 2017 Matters Arising Include discussion on the On Board Visit Protocol and Process on the Agenda for the Board Development Session on 18 th September Mr Lewis- Grundy October 2017 Discussion had at the Board Development session on 18 th September. Completed. Closed May 2017 Quality & Safety Committee Chair s Report Approach Engagement Champions for input on potential improvements to the Board Walkabout process for capturing actions taken. Mr Lewis- Grundy October 2017 Discussion had during the Board Development session on 18 October. Completed. Closed. 2
29 Item No. 117 Date Added 7 September 2017 Action Responsibility Due Date Update Director of Operations Report Section 75 outcomes to be reported to the Board in October via the Director of Operations report. Mrs Writtle October 2017 Update included in Director of Ops report to the October Board. Completed. Closed September 2017 Health & Safety Annual Report Clarify that the risks highlighted in the FRAs for Bloxwich were captured on the Operational Risk Register. Mr Davies October 2017 The risks have been captured on the Operational Risk Register. Completed. Closed July 2017 Quality Report Quality & Safety Committee to review the ligature incidents and provide assurance to the Board via the Quality & Safety Committee Chair s Report. Mrs Musson October 2017 Reviewed by Quality & Safety Committee in September and referenced in the Quality & Safety Committee Chair s report to Board in October. Completed. Closed September September 2017 CQC Action Plan The RAG rating of the Action Plan be amended in line with that used for Board and Committee actions incorporating an additional Blue rating for those actions that were progressing to schedule. Emergency Preparedness, Resilience & Response (EPRR) Assurance Clarify whether buildings that did not have inpatient capacity but were used by Trust patients to access services were similarly prepared and had evacuation Mrs Musson Mr Axcell October 2017 October 2017 Action discussed at CQC Steering Group Action plan has been amended and the blue RAG rating included in the Board report. Completed. Closed. Mr Axcell had received confirmation that the EPRR process covers all buildings in which the Trust provides services. Completed. Closed. 3
30 Item No. Date Added Action Responsibility Due Date Update plans in place. 4
31 Board meeting date: 5 October 2017 Agenda Item number: 5 Enclosure: 3 Report Title: Summary Report of Confidential Session of Trust Board held on 7 September 2017 Accountable Director: Author (name & title): Purpose of the report: Ben Reid, Chair Paul Lewis-Grundy, Company Secretary Best practice in corporate governance requires that business considered in private session is reported into the public session as soon as possible. Given the arrangement of the Board meetings, the earliest opportunity is at the public session of the following month. This report outlines the business considered in private at the meeting of the Board held on 7 September Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: None Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Please give brief details: Best practice in corporate governance requires that business considered in private session is reported into the public session. Effective Well-led Safe Enc 3 confidential session Page 1 of 2
32 Title Summary Report of Confidential Session of Trust Board held on 7 September 2017 Introduction This report outlines the business considered at the meeting of the Board held in private on 7 September Summary of key points, issues and risks On 7 September 2017 the Board received the following reports: Chief Executive s Update Report Transforming Care Together (TCT) Progress Report The finalised Memorandum of Understand for the Black Country Sustainability & Transformation Plan which Board agreed. Plan (STP) Service Development & Growth Progress Report The Medical Revalidation Annual Report, which Board approved for the appropriate sign off and submission The Final Construction Costs for Clee Ward refurbishment, which Board approved Ratified minutes of the MExT meeting held on 25 th July Recommendation The Board is invited to note the business transacted in the private session held on 7 September Board action required The Board is asked to receive this report for information. Enc 3 confidential session Page 2 of 2
33 Board meeting date: 5 October 2017 Agenda Item number: 6 Enclosure: 4 Report Title: Chief Executive Officer s Overview (including written summary of strategic publications and headlines) Accountable Director: Author (name & title): Purpose of the report: Mark Axcell, Chief Executive Paul Lewis-Grundy, Company Secretary This report summarises recent reports, publications and information, which are of relevance or interest to the Trust. It sets out the key points of each item and identifies the officer accountable for any action required and appraising the Board where appropriate. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: None Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Accountable workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: The report provides information regarding latest news and relevant strategic developments that may impact all 5 CREWS domains. Enc 4 CEO StrategicBrief-October2017-(Final) Page 1 of 7
34 Title: Chief Executive Officer s Overview (including written summary of strategic publications and headlines) Introduction This report provides a summary of internal news from the Chief Executive and recently announced legislation, publications and information that is of interest and relevance to the Board. It identifies the Trust officer accountable for any action the Trust may be required to take and for appraising the Board where appropriate. Summary of key points, issues and risks CHIEF EXECUTIVE UPDATE Transforming Care Together As the Board will be aware the transaction date for TCT was originally planned to be the 1st October During the month NHS Improvement paused the process. They have now asked for more information regarding the Full Business Case for the 3 Trusts coming together. The revised anticipated date for the transaction, subject to the necessary approvals, is the 1st December MERIT Vanguard An update on MERIT is included later on the agenda. NHS Improvement have now agreed to release ¾ of the funding for the programme for the year. Developments of particular note are as follows: MERIT Crisis Care webpages launched The MERIT Vanguard partnership has launched a dedicated Crisis Care section on its website allowing anyone to find out which services are available to provide care to someone during a mental health crisis, regardless of where in the West Midlands they live. It can be a challenge to provide the right care for service users who experience a mental health crisis whilst travelling outside the area covered by the Mental Health Trust which covers their home address. MERIT Electronic Health Record Viewer Tuesday 28 November will see the launch of the MERIT Electronic Health Record Viewer. It represents a major step forward for clinicians who sometimes see and treat inpatients or outpatients who live in the area covered by another of the partner Trusts, and will allow shared access to specific but crucial information from the patient s mental health record subject to obtaining informed consent. MERIT Bed Finder The MERIT Bed Finder will be launched on 28 November. It will offer staff in each of the partner Trusts the opportunity to view the status of beds at each other s organisations. Dudley MCP The Trust continues to engage positively with the MCP development. Clinical and Operational representatives have been identified for all of the key workstreams to support the development of the clinical model. Flu Campaign 2017: GET A JAB, GIVE A JAB HELP UNICEF October marks the launch of our staff flu campaign We will again be encouraging all staff to have a flu vaccination. This year as well as the monthly prize draws the Trust will be supporting UNICEF and for every member of staff that has a flu jab we will be donating to UNICEF to buy 10 Tetanus jabs for developing countries. Enc 4 CEO StrategicBrief-October2017-(Final) Page 2 of 7
35 Exercise of Delegated Authority In accordance with the authority delegated to me in consultation with the Chair, I have exercised that authority in consultation with the Chair with regard to the submission of a commercial tender. Board, in private session due to the commercial nature of the decision, will receive further detail of this tender within the Service Development & Growth Report. Action: To note the exercise of this delegated authority NATIONAL POLICIES & STRATEGIES The following national strategies and policies have recently been issued. They are potentially relevant to the future strategic, planning and operational management of the Trust and the implications should be taken into account. Each document has been considered with the respective executive directors. This summary is not intended to incorporate all national publications, for instance those issued by National Patient Safety Agency, National Institute for Clinical Excellence or every operational directive issued by Department of Health which should be considered within the Trust by the appropriate department and necessary action taken. 1. Stepping forward to 2020/21: The mental health workforce plan for England Published by: Health Education England Date Published: 31 July 2017 The plan to expand the mental health Workforce sets out measures to tackle the historic imbalance in workforce capacity and fulfil ambitions to improve mental health services. The government had announced that it is committing 1.3 billion to transform mental health services, with a pledge to treat an extra 1 million patients by 2020 to 2021, provide services 7 days a week, 24 hours a day and integrate mental and physical health services for the first time The plan has been developed by Health Education England (HEE) together with NHS Improvement, NHS England, the Royal College of Psychiatrists and other key mental health experts. It shows how the health service will dramatically increase the number of trained nurses, therapists, psychiatrists, peer support workers and other mental health professionals to deliver on this commitment and tackle the burning injustice of mental illness and inadequate treatment. By 2020 to 2021 local areas will need to create 21,000 new posts in priority growth areas to deliver the improvements in services and support set out in the NHS s Five Year Forward View for Mental Health. The strategy recommends each STP area appoint a chief executive or executive director to lead the development and delivery of a mental health workforce strategy. Action: Recruitment into mental health specialties remains a great challenge for all disciplines. This is being considered in the Trust s workforce planning and is being progressed via the Workforce Committee and also the STP Mental Health Workstream Web-link Executive Director: Medical Director / Acting Director of People Board Committee: Workforce Committee Enc 4 CEO StrategicBrief-October2017-(Final) Page 3 of 7
36 2. Integrating Care: contracting for accountable models Published by: NHS England Date Published: 7 August 2017 This guidance provides support for early accountable care organisations (ACOs) and outlines the new contractual framework for ACOs and how to establish the care model in practice. Action: Included in consideration of the models of care in Dudley and Walsall Web-link Executive Director: Chief Executive Board Committee: Board 3. Integrating Support and Assurance Process (ISAP); new guidance Published by: NHS Improvement Date Published: 17 August 2017 Working with NHS England, NHS Improvement has designed a consistent, streamlined process for supporting and assuring the successful delivery of complex contracts. The Integrated Support and Assurance Process (ISAP) has been designed to ensure NHS England and NHS Improvement have a co-ordinated approach to supporting the transactions for complex contracts. The guidance details the integrated process that they ll be using to help providers and commissioners looking to complete procurements for complex contracts. The guidance includes lessons learnt from past complex contracts, key risk management questions for providers, commissioners, NHS Improvement and NHS England, the stages of the ISAP, when to apply the ISAP, information on the submissions and evidence expected from commissioners and providers at each stage, how to feed back on the ISAP and the next steps for those working on complex contracts The resource replaces the introductory document published in November Action: For information Web-link Executive Director: Chief Executive Board Committee: Board 4. NHS Property Services Charging Policy 2017/18 Published by: NHS Property Services Date Published: August 2017 NHS Property Services (NHSPS), in conjunction with NHS England and the Department of Health, has published a refreshed Charging Policy for 2017/18. It provides clarity to NHSPS customers on the charges payable for occupation of NHSPS properties and is relevant to customers with signed leases in place as well as those who are currently occupying premises on an undocumented basis. The policy also includes details about the vacant space hand back scheme and sessional space policy. Action: To be considered by the Estates and Capital Planning Group. Web-link Executive Director: Director of Finance, Performance and IM&T Board Committee: Finance & Performance Committee Enc 4 CEO StrategicBrief-October2017-(Final) Page 4 of 7
37 5. Prevention concordat for better mental health: planning resource Published by: Public Health England Date Published: 30 August 2017 The Prevention Concordat for Better Mental Health is underpinned by an understanding that taking a prevention-focused approach to improving the public s mental health is shown to make a valuable contribution to achieving a fairer and more equitable society. This resource has been developed to help local areas put in place effective arrangements to promote good mental health and prevent mental health problems, offering a 5-part framework of focus for effective planning for better mental health. It also highlights a range of actions and interventions that local areas can take to improve mental health and tailor their approach. This includes illustration through practice examples and links to further supporting resources. This concordat has been informed by the findings of a stocktake of local mental health mental health prevention planning arrangements, which itself is based primarily on a content analysis of key planning documents in 35 local areas and published by Public Health England on 30 August 2017 Action: Joint meeting and discussion between our medical and nursing leads and colleagues in public health to arrive at collaborative local strategies and initiatives Web-link 158_NEWSL_HMP% &dm_i=21A8,54RCU,M5T16P,JPGIG,1 Executive Director: Medical Director Board Committee: Quality & Safety Committee 6. Managing risk in health and care this winter Published by: NHS Providers Date Published: 3 September 2017 This report assesses NHS planning for the upcoming winter season and finds whilst the level of planning and support is more developed than last year, the system still requires emergency funding to ensure patient safety. NHS Providers warns that a failure to make an emergency investment of million will lead to longer patient waiting times and increased patient safety risks Action: To note for information. Web-link _NEWSL_HMP% &dm_i=21A8,552GW,M5T16P,JQZK2,1 Executive Director: Interim Director of Operations Board Committee: Quality & Safety Committee 7. Updated employment check standards Published by: NHS Employers Date Published: 7 September 2017 NHS Employers has updated the employment check standards for While the legal requirements have remained largely unchanged, this year s review has responded to requests for additional clarity on certain elements of the requirements. In particular, the check standards reinforce the importance of the relationship between employers, agencies and third party staffing providers to ensure they understand the type of checks required for all temporary workers. Enc 4 CEO StrategicBrief-October2017-(Final) Page 5 of 7
38 The standards have also been formatted with contents and introductory pages to help employers access information more easily and explain what the check is and why it s important. The standards are subject to periodic review to ensure they take into consideration any changes to legal requirements and policy direction. Action: The updated standards will be reviewed by the workforce development team Web-link Executive Director: Acting Director of People Board Committee: Workforce Committee 8. Practical guide for large scale change Published by: NHS England Date Published: 13 September 2017 The guide provides a comprehensive round-up of all the latest thinking and practical approaches and tools that can be used in advancing large scale change programmes, including updates on the leading models that will enable leaders to address the challenges in achieving large scale change and the latest thinking from national and global improvement experts and change leaders. It outlines New tools, techniques and tips to help leaders effectively progress large scale change programmes and includes content that will help system leaders successfully take forward STP, vanguard, new care model, accountable care system or other large scale change programmes signposting to a host of new online resources Action: For Information Web-link ngland%29 Executive Director: Chief Executive Board Committee: Board 9. Draft Health Service Safety Investigations Bill Published by: Department of Health Date Published: 14 September 2017 The draft bill proposes setting up the Health Service Safety Investigations Body (HSSIB). The HSSIB will conduct investigations which focus on learning from patient safety incidents in the NHS, to reduce health care harm and improve patient care. The draft bill allows the HSSIB to conduct investigations using safe space. Safe space is a set of legal powers that prevent the HSSIB from disclosing the information it gathers in the course of an investigation. Action: To note and keep Board informed of the Bill s progress and future implications for the Trust. Web-link EWSL_HMP% &dm_i=21A8,55SCL,M5T16P,JTPMY,1 Executive Director: Acting Director of Nursing Board Committee: Quality & Safety Committee Enc 4 CEO StrategicBrief-October2017-(Final) Page 6 of 7
39 10. The future of the mental health workforce Published by: Centre for Mental Health on behalf of the Mental Health Network, part of the NHS Confederation Date Published: September 2017 This report calls for reform of mental health services in order to develop a workforce that is able to meet people's needs in the future. The report describes commissioning of mental health services as in crisis with a diminishing workforce, growing expectations and increasing demand putting pressure on staff across the country. It recommends that all GPs should have significant and wide-ranging mental health training, and that mental health professionals should be given the time and training to consult with GPs and other public service staff to help them to respond to more people s mental health needs. Action: This is being progressed as part of the Black Country Local Workforce Action Board (LWAB) and a bid is being submitted for Mental Health First Aid training. The Trust also has a robust Health & Wellbeing action plan in place to support staff s Mental Health needs. Web-link = _NEWSL_HMP% &dm_i=21A8,5601G,M5T16P,JVYXV,1 Executive Director: Acting Director of People Board Committee: Workforce Committee 11. The State of pre and post graduate medical recruitment in England Published by: British Medical Association (BMA) Date Published: September 2017 This briefing examines the current state of medical recruitment in England, with additional UK-wide data for the foundation programme. Looking at data from 2013 onward, it identifies some of the ongoing issues facing medical recruitment, and recommends how some of these key concerns can be addressed. Action: Recommendations to be reviewed by the medical management team and strategies discussed to mitigate the shortfall locally in the shorter and longer term. Web-link Executive Director: Medical Director Board Committee: Workforce Committee Recommendation It is recommended that the Board: Considers and discuss the information contained within this report, and note for assurance the actions identified throughout the report. Board action required The Board is asked to: Note the information and actions contained within the report. Identify any further specific action required and agreed timeframe for completion. Enc 4 CEO StrategicBrief-October2017-(Final) Page 7 of 7
40 Meeting date: 5 October 2017 Report Title: Agenda Item number: 7.1 Enclosure: 5 OnBoard Visits Governance Framework Accountable Director: Author (name & title): Purpose of the report: Mark Axcell, Chief Executive Paul Lewis-Grundy, Company Secretary To present Board with the proposed developments in the governance of OnBoard visits Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Board Development Session Date reviewed: 18 September 2017 The report incorporates the outcome of discussions at the Board Development Session. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Please give brief details: OnBoard Visits by members of the Board may variously cover any of the domains. Safe Enc 5 OnBoard Visits Governance Arrangements Page 1 of 4
41 Title OnBoard Visits Governance Framework Introduction Board members have been doing OnBoard visits for a number of years and they are widely recognised across NHS Provider Boards as an important element of the role of Board members, to meet and discuss matters with staff and patients and to triangulate information that Board receive through Management reports to the Board and its various Committees. The arrangements for these visits have not changed since their inception and there is currently a lack of a documented process to ensure that the OnBoard visits add value to the work of the Trust. There is also an outstanding action against the Trust s own self- assessment against the CQC Well-Led Framework to develop a more structured process around OnBoard Visits. A more documented approach to OnBoard visits was discussed at a Development Session with Board members on 18 September The governance arrangements presented in this report have been formulated taking account of those discussions. Following that Session the CQC assessment of the two outstanding mental health trusts have been reviewed. Reference was specifically made to the high quality of the questions, challenge and debate at Board meetings and board members appropriately holding executive staff to account to ensure the trust was meeting the needs of people using the services. CQC report of East London NHS Foundation Trust and Northumberland & Tyne and Wear NHS Foundation Trust also highlighted positively under the well-led domain the significant time that Board members spend visiting services and talking to staff and patients relating this to strong leadership within the Trusts. Board members are encouraged to visit services as and when they are able to as part of their role within the Trust not limiting these to On Board visits. A protocol for visiting wards outside of On Board visits will be developed by the Acting Director of Nursing to ensure the approach of the Board minimises any risks to staff and patients. Summary of key points, issues and risks This report confirms the purpose of OnBoard visits and documents how the wards / teams and services that will be visited will be determined. It also strengthens where and how the feedback from visits will be co-ordinated within the Trust s existing governance arrangements. Members of the Board are undertaking OnBoard visits before the Board meeting on 5 October 2017 and can use the opportunity of this report to feedback any high level themes from those visits. Subject to Board agreeing the framework outlined in this report it will be implemented for the following round on OnBoard visits. Enc 5 OnBoard Visits Governance Arrangements Page 2 of 4
42 Further detail 1. Purpose of OnBoard Visits 1.1 The purpose is To engage and Learn from Staff To talk to patient s to hear about their experience in receiving services from the Trust To triangulate information that Board members receive from other sources as a form of assurance 1.2 OnBoard visits are important to the wider Leadership role of the Board and to promote the Trust s culture and Values across the organisation 1.3 The stated purpose on the visits should also support the quality of the questions, challenge and debate at Board meetings and board members appropriately holding executive staff to account to ensure the Trust is meeting the needs of people using the services. 2. Frequency and location 2.1 On Board visits will continue to be scheduled in a two month block to align with the venue of the Board meeting 3 times a year. 3. How the Areas to visit will be determined 3.1 Data from Incidents, Complaints, Patient Experience metrics Performance Reports, Audits and CQC Action Plans, including areas of good practice and performance will be used to assess which areas / services to visit. 3.2 The work of the Board Committees may also identify areas to visit and will be informed through the Committee Chairs report to Board. 4. Before the Visit 4.1 Board members will receive a short briefing note from the relevant Executive Director in advance of the visit to assist in the enquiries that the Board members may wish to make. 4.2 The areas to be visited will receive a short note explaining the purpose of the OnBoard visits and how the themes identified during the visit will be incorporated back into the governance of the Trust. 5. During the Visit 5.1 At the start of the visit, Members of the Board will receive a brief on any issues that they need to be aware of during the visit. 5.2 Members of the Board should make a note of any issues to help feedback on any overarching themes from the visit. Enc 5 OnBoard Visits Governance Arrangements Page 3 of 4
43 6. Where and how Feedback will be incorporated into the existing Governance Arrangements 6.1 An item will be included on the Agenda for the Public Board meeting in the afternoon of the visit to enable feedback and discussion on the general themes of the visit and any referral as necessary to the relevant Committee of Board. 6.2 The Themes will be referred to the Triangulation and embedding lessons group to inform shared practice across the Trust. 6.3 Board members undertaking a visit that have a significant clinical concern as a result of the visit should raise this immediately after the visit with the relevant Executive Director, or Chief Executive, or Executive Director On Call. 7. Administration 7.1 OnBoard visits will be administered by the Corporate PA Team / Corporate Governance Support Office. Recommendation That the Governance arrangements for OnBoard Visits outlined in this report be adopted. Board action required As recommended Enc 5 OnBoard Visits Governance Arrangements Page 4 of 4
44 Board meeting date: 5 October 2017 Agenda Item number: Enclosure: 6 Report Title: Trust Integrated Performance Report (Month 5) including the Performance Dashboard and Contract Performance Dashboard Accountable Director: Author (name & title): Purpose of the report: Rupert Davies Interim Director of Finance, Performance and IM&T Makhan Singh (Principal Consultant, Information & Performance) To update the Board on all aspects of Trust performance at month 5 of 2017/18 Quality and Safety Service User Experience Efficiency Resources Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality and Safety Committee considered elements from within the Quality and Safety domain, and the Service User Experience domain. Finance and Performance Committee considered elements from the Efficiency, Resource and Quality and Safety Domains Workforce Committee considered elements from the Resource and Quality and Safety Domains Date reviewed Quality and Safety Committee met on 13 September 2017 Finance & Performance Committee and the Workforce Committee met on 25 September 2017 The key points are addressed through the separate reports from the Chair of the respective Committees. Enc 6 17_18 IPD Month 5 Page 1 of 5
45 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources What impact or implications does this report have on any of the following: Caring Responsive Please give brief details: The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources Effective Well-led Safe Enc 6 17_18 IPD Month 5 Page 2 of 5
46 Title Trust Integrated Performance Report (Month 5) including the Performance Dashboard and Contract Performance Dashboard Introduction This paper presents the Trust s performance at the end of month five 2017/18 financial year. The 2017/18 Integrated Dashboard allows comparison and triangulation across Quality and Safety, Service User Experience, Efficiency, and Resources to give a comprehensive picture of the performance of the Trust. The 2017/18 Integrated Dashboard also includes performance, and exception commentary, by service line, so that the Board is better able to see achievements as well as any adverse performance within the overall aggregate level. Summary of key points, issues and risks For 2017/18 the Trust Integrated Performance Dashboard (IPD) has been reviewed by Operational and Corporate Teams. The IPD has been amended in accordance with the changes to the service lines. Where appropriate the 18 month trends are shown in the IPD and for any new KPI s under a service line, the in-month position is reported. Quality and Safety Domain In August the Trust reported 484 incidents. This represents a decrease of 17% compared to July (583). Although this is a considerable decrease, particularly in the Disruptive/Aggressive Behaviour category, reported incidents still remain high. A patient on Holyrood, referred to in previous reports, has had their medication reviewed and as a result incidents relating to this patient have significantly reduced. Inpatient Services (Acute) continues to report high levels of Disruptive/Aggressive Behaviour despite a decrease on the previous month. Care provided to mitigate the risks posed to other patients and staff is appropriate with any restraints being independently scrutinised by Trust MAPA Leads. Kinver Ward has reported a high number of incidents in August due to a patient who is pregnant and refusing to take medication. The MAPA team has been involved and there is an appropriate care plan in place. Older Adults Inpatient Services has seen a decrease in reported incidents, particularly Disruptive/Aggressive Behaviour with Clinical Care, Quality and Treatment being their highest reported category for August. Linden Ward has continued to report high numbers of incidents, with one particular patient being involved in 68 incidents. The Psychology Team have provided support to the ward and have assisted with the development of a Positive Behavioural Support Plan. Community Services continue to have low levels of reported incidents. The Trust reported seven Serious Incidents during August (By service: 2 Inpatients, 2 Urgent Care, 2 Early Intervention and 1 Dudley Outpatients). The Duty of Candour was Enc 6 17_18 IPD Month 5 Page 3 of 5
47 considered for all Serious Incidents with one meeting the specific criteria. All the investigations have now commenced and support mechanisms for patients, relatives and staff are in place. Any identified areas for improvement will be managed through the Trust Embedding lessons procedures. CPA Performance at month five: Trust is above target for both CPA indicators, Copies of Care Plan at 95.44% and CPA Formal Reviews at 95.56%. In August the Trust is non-compliant for the 5 day follow-up on inpatient discharge KPI at 94.90% (93/98), and the five breaches were reviewed and verified by operational leads. There were 18 Safety Alert Broadcasts received by the organisation via the Central Alerts System. One has been circulated for information, 1 requires action and 1 is being assessed for relevance. Efficiency Domain The Trust s Cost Improvement Target for the year is 2,500k, however, in order to ensure the required level of funding to support in year Cost Pressures schemes have been developed to the value of 3,765k. As at month five 2,906k worth of schemes have been delivered against the target of 3,765k. Based on the agreed Agency Cap ceiling of 4.05m for the financial year this equates to an overall target of 8.24% based on the Trust s planned annual pay costs. Current position to date is reflecting a favourable position to plan of 7.37%. Total agency spend in financial terms has out turned at a spend level of 1,558k across the Trust against a planned spend of 1,706k (giving a position of 148k ahead of plan). Vacancies There are currently 100 Full Time Equivalent contracted vacancies across the Trust meaning the vacancy rate has reduced to 9.11% in month five from the 12.40% reported in month four. The TRAC recruitment system is currently being used within the Trust giving increased control and oversight to recruiting managers and allows the Trust to performance manage against recruitment KPIs. Turnover The 12 Month Turnover rate has increased from 11.21% to 11.97%. The Trust s percentage turnover rate (excluding Junior Medical Staff) is average compared with other Mental Health organisations in the NHS. Sickness Absence The rolling 12 month sickness rate has decreased from 4.05% in month four to 3.93% in month five, this is within the Trusts target and the tenth consecutive month of being so. In month sickness has decreased from 4.02% in month four to 3.35% in month five. Appraisal Compliance has increased from 84.77% to 87.93%, this is above the Trust target of 85%. There are 110 employees in the Trust that have not had an appraisal recorded in the last 12 months, an improvement on the 223 reported in September Bi Weekly reports are now being produced in order to support managers in highlighting with low compliance and future requirements. Mandatory Training - Mandatory Training compliance increased from 90.60% in month four to 91.97% in month five and is above the agreed target of 90% for all mandatory training. As with the Appraisal, new reports are being distributed to Enc 6 17_18 IPD Month 5 Page 4 of 5
48 Further detail Service leads to assist with what training individuals need to undertake in order to remain compliant. Further detail is in the appended Integrated Performance Dashboard (Appendix 1), Contact Dashboard (Appendix 2) and the following underpinning reports for finance, quality and workforce. Recommendation It is recommended that the Board note the performance of the Trust as at month five and debate accordingly. Board action required Debate the content of the reports accordingly. Enc 6 17_18 IPD Month 5 Page 5 of 5
49 Enc 6 Appendix 1 Trust Integrated Performance Dashboard Month /18
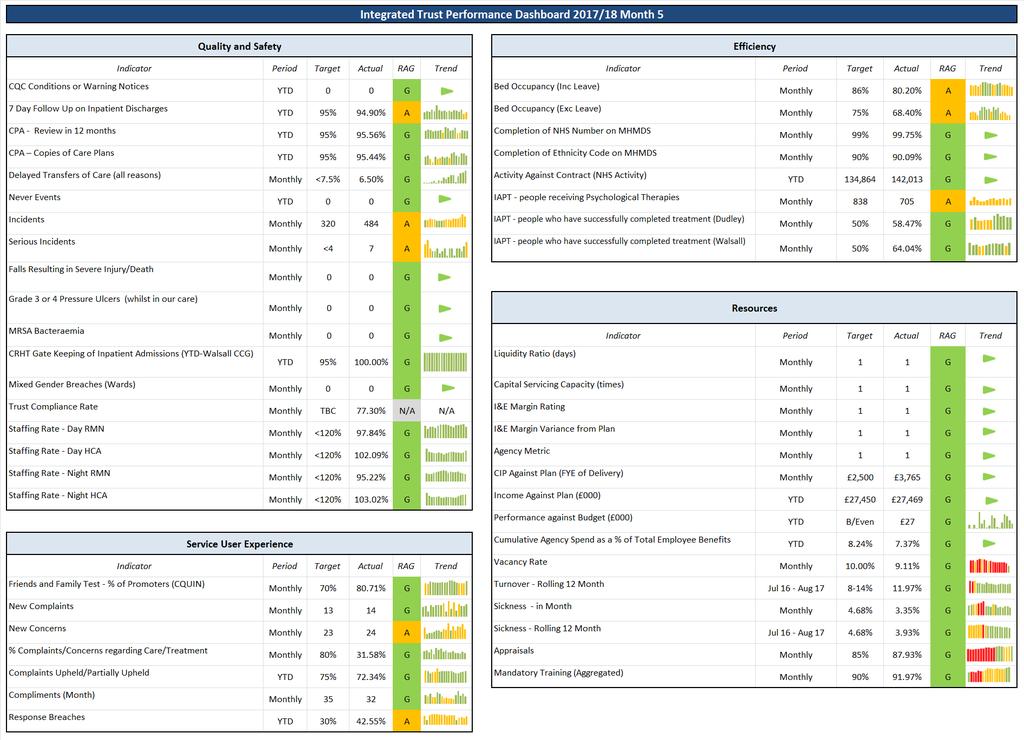
50 2

51 Inpatients Service Line Summary In month five, there are 11 Dudley CCG patients reported as Delayed Transfer of Care (DToC) resulting in a rate of 6.50%. Operational leads have prepared an exception report, which will be shared with Dudley CCG and further discussions to be held at Contract Quality Review meetings. 2 Serious Incidents reported in month five; 1 Older Adult Inpatients, 1 Walsall Home Treatment. This service line has overspent by 199k to month five, including a 104k overspend in month five itself, this included an overspend of 45k on Ambleside (in response to an incident and to separate safeguarding concerns), and of 61k on Holyrood (due to the challenging behaviour of several DToC patients). There has been a slight decrease in month five sickness to 5.50% (5.71% in month four). Performance for Mandatory Training has increased slighlty (86.31% in month four to 87.65% in month five). 3

52 Community Service Line Summary CPA Performance Community service (CRS, Older Adult CMHT s) is performing at 95.12% for Copies of Care Plan given and 95.55% for CPA Formal Reviews within 12 months. Community & Recovery Services position at month five is 78k overspent. This is being driven by costs around anticipated NHS Property Services charges for properties such as Poplars and Brace Street within Community Estates. There has been a decrease in sickness levels for month five to 1.86% (3.12% reported in month four). Mandatory training performance has increased to 92.48% in month five compared to 90% in month four. 4

53 Urgent Care & Access Summary IAPT Project team is in place to review and take action on the needs of delivering an IAPT service, where the Trust needed to increase the target for IAPT KPI s during the year in order to meet the end of year target that now only applies to IAPT and can only be met by IAPT recognised staff and IAPT therapies for depression and anxiety only. The thresholds are extremely difficult for an element of the service to meet compared with the previous position where the service met their KPI s and also measured against the prevalence for depression and anxiety in the local communities. There is a robust communication campaign on going to encourage more people to access the service. This service line has underspent by 30k to month five. This is being driven by vacancies across a number of Primary Care and Access teams. There has been a decrease in sickness performance for month five to 5.11% from 6.39% in month four. There has been an increase in performance for mandatory training to 93.51% in month five (91.30% in month four). Appraisals performance has fallen below agreed threshold to 84.69% in month five (86.32% in month four). 5

54 Early Intervention Service Line Summary Early intervention service is reporting EI Teams and CAMHS Services. CPA Performance this service is performing above Target for both CPA indicators; 98.88% for Copies of Care Plan given and 97.78% for CPA Formal Reviews within 12 months. The Early Intervention service line is underspent by 98k at month five, which is due to slippages against new funding streams. Drawdown on the slippage is expected to meet the expectations set out by commissioners in terms of training, etc. Early Intervention sickness has seen a slight increase to 3.17% in month five (2.79% in month four). Performance for appraisals has decreased at 87.72% in month five (91.60% reported in month four). Mandatory training has increased to 92.31% in month five (91.60% in month four). 6
55 Enc 6 Appendix 2 Trust Contract Performance Dashboard Month /18
56 2 Contractual Quality Requirements Trust and CCGs (In month performance and monthly trends) KPI No KPI Detail and Target Trust Dudley CCG Walsall CCG Trust Monthly Trend Dudley CCG Trend Walsall CCG Trend 1 Percentage of Service Users on incomplete RTT pathways (yet to start treatment) waiting no more than 18 weeks from Referral. (Target: Above 92%) 98.88% % 98.16% 2 Zero tolerance RTT waits over 52 weeks for incomplete pathways Care Programme Approach (CPA): The percentage of Service Users under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care. (Target: Above 95%) Completion of a valid NHS Number field in mental health and acute commissioning data sets submitted via SUS (Target: Above 99%) Completion of Mental Health Minimum Data Set ethnicity coding for all detained and informal Service Users. (Target: Above 90%) 94.90% 93.88% 95.00% 99.75% 99.89% 99.97% 90.09% 90.79% 93.07% 6 Sleeping Accommodation Breach Percentage of people experiencing a first episode of psychosis will be treated with a NICE approved care package within two weeks of referral. (Target: Above 50%) Completion of IAPT Minimum Data Set outcome data for all appropriate Service Users. (Target: Above 90%) The proportion of people that wait 6 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period. (Target: Above 75%) The proportion of people that wait 18 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period. (Target: Above 95%) % % % 99.24% 98.73% % 94.44% 91.33% 99.11% 99.60% 99.74% % 11a IAPT - number of people who receive psychological therapies. (Target Dudley: 477 per month) b IAPT - number of people who receive psychological therapies. (Target Walsall: 361 per month) IAPT - Proportion of people who complete treatment who are moving to recovery. (Target Walsall: Above 50%) 58.47% 64.04% 13 Percentage of patients who are provided a copy of their care plan. (Target: Walsall - Above 95%) 95.44% 96.74%
57 3 Contractual Quality Requirements Trust and CCGs (In month performance and monthly trends) KPI No KPI Detail and Target Trust Dudley CCG Walsall CCG Trust Monthly Trend Dudley CCG Trend Walsall CCG Trend 14 Delayed Transfer of Care (All Reasons). (Target: Below 7.5%; Walsall - TBC) 6.50% 9.50% 4.00% 15 Inpatient Admissions Gate kept by CRHT. (Target: Walsall - Above 95%) % 16 Acute Adult Inpatient stays less than 40 Days. (Target: Dudley - Above 95%) 77.55% 17 Proportion of in-scope patients assigned to a cluster. (Target: (Dudley - Above 95%) 95.49% Proportion of patients within cluster review periods. (Target: Dudley M1 >80%;M2>82%;M3>84%;M4>86%;M5>88%;M6>90%;M7>92%;M8>94%;M9-12>95%) Dudley and Walsall Recovery Outcome Measure - Number of CPA patients assessed using DWROM (Target: Dudley Only: Q1 - >85%; Q2 - >90%; Q3 & Q4 - >95%) 88.50% 90.75% Eating Disorders - % of children & young people who receive treatment within four weeks of referral for routine cases. (Target: Walsall - Above 95%) Eating Disorders - % of children & young people who receive treatment within one week of referral for urgent cases. (Target: Walsall - Above 95%) % % 22 PLT - number of patients seen on the wards within 24 hours. (Target: Dudley - Above 85%) % 23 PLT - number of patients seen in A&E assessed within 4 hours. (Target: Dudley - Above 95%) % 24 CRS - proportion of patients seen within 6 weeks. (Target: Dudley - Above 75%) % 25 PT Hub - proportion of patients seen within 18 weeks. (Target: Dudley - Above 95%) % 26 Duty of Candour
58 Board meeting date: 5 October 2017 Agenda Item number: 7.1.2a Enclosure: 7 Report Title: Quality and Safety Committee Chair s Report Committee: Author: Quality and Safety Committee Simon Murphy Non Executive Director Rosie Musson Acting Director of Nursing Action required from the Board Decision / Gain assurance Approval Introduction Discussion Information The Quality and Safety Committee met on 13 September Summary of key points, issues and risks Deep Dive Review of Ligature Incidents The Committee received a presentation on the number of ligature incidents over the last two years: an analysis of the incidents: their severity and mitigations in place. Key discussion points at the Committee related to: The importance of minimising risk, whilst still providing a therapeutic environment including garden areas. The use of door sensors on the wards. The Committee will be reviewing a for and against appraisal of their usage at the October meeting. High incident reporting on Ambleside Ward. The Committee will receive a deep dive regarding Ambleside at the October meeting led by the Joint Medical Director and Acting Director of Nursing. Further information to be circulated to the committee regarding bench marking with other trusts in relation to incidents. Quality and Safety Report The Quality Report was presented to the Committee for information and assurance. The following points were noted: 484 incidents reported, which represents a decrease of 17% from July. The Committee discussed the decrease in reported incidents across the Trust and how the management and placement of a small number of patients had affected this decrease, Enc 7 Q and S Committee Chair's Report-(Final) Page 1 of 3
59 although incident reporting levels still remain high. The main decrease was in the Disruptive/ Aggressive category and has been reflected in the number of staff injuries recorded.clinical Care, Quality and Treatment incidents have increased, however the Committee were assured that this is mainly attributed to the recording of clinical holds relating to personal care, which is reflected in the physical intervention figures. Acute services report high levels of disruptive and aggressive behavior that can be attributed to a small number of patients. The Committee asked further information regarding patient and Staff injuries to understand any variations. Seven serious incidents were reported, of which, having carried out the initial review of our transfer processes and care delivery, the 2 Serious Incidents relating to Under 18 admissions will be transferred from the Trust s reported figures to specialist commissioning. One other will be transferred as the patient is from Wolverhampton and therefore the investigation will be undertaken by Black Country Partnership NHS Foundation Trust The Committee will have a spotlight session on Under 18 admissions in November. Compliance against safeguarding training continues to be monitored. Quality and Safety High Level Risk register The Committee was advised that there are currently ten operational red risks. Detailed discussions took place regarding their current status in light of the number of actions already taken to mitigate. It was agreed that work should be undertaken to review the risks with the Executive Leads and for the review to be presented to the next Committee to receive Service Experience Desk Quarter 1 Report The Committee reviewed the report. The key discussions were as follows The decrease in Friends and Family Test results. The Committee received assurance that Heads of Service are being advised of the issue and asked to raise at service line meetings. Concerns regarding poor communication category to be discussed further by Executive Directors and outcome feedback to next Committee Concerns relating to staff attitude and the importance training for staff in customer care. Category to be monitored through quarterly embedding lessons report. Clinical Audit and Effectiveness Annual Report The Committee receive the report for assurance. The report provided an overview of Clinical Audit activity during 2016/17. The Committee noted the progress made and that the report will be sent to Audit Committee for assurance. CQC Action Plan Update The Committee received an update on the CQC Action plan. Good progress continues to be made and the next steps will be to look at how the Trust can move from Good to Outstanding. To maintain progress an assurance plan will be developed including Supportive Visits and audits. This will be monitored through the CQC Steering Group and update reports to the Quality and safety Committee. Enc 7 Q and S Committee Chair's Report-(Final) Page 2 of 3
60 Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees/Groups: Audit Committee Finance and Performance Committee MExT CARM / CQR Clinical Audit and Effectiveness Committee Embedding Lessons Group Regulation and Risk Working Group Safeguarding Strategic Group Suicide Prevention Group Equality and Diversity Steering Group R&D Committee Health & Safety Committee Infection Prevention Control Committee Medicines Management Committee Mental Health Forum Policy & Procedures Group Resuscitation Committee Recommendation The Trust Board is asked to: Accept this report for assurance about the exercise of delegated authority by the Quality and Safety Committee. Board Action Required As recommended. Enc 7 Q and S Committee Chair's Report-(Final) Page 3 of 3
61 1 Meeting date: 5 October 2017 Agenda Item number: 7.1.2b Enclosure: 8 QUALITY REPORT (MONTH 5) 1
62 2 Section 1 Summary of Trust Incidents and Serious Incidents 2





 Under 18 Admission Medication Health & Safety Security / Cyber Security Equipment Documentation & Electronic Records Management Fire Information Governance And")

63 Section 1 3 Summary of Trust Incidents and Serious Incidents August 2017 Trust Incidents 484 Serious Incidents Patient Safety Incidents Security Incidents Reports 99 High Low 12 months incident data 12 months SI data 12 months PSI 12 months SIRS Top 5 Cause Groups & top 3 Incident Causes August 2017 Incidents by Serviceline Inpatient UCAS Community E.I. CSD August 2017 Incidents by Category Disruptive / Aggressive Behaviour Behavioural - Aggressive Physical Assault - Pt On Pt Physical Assault - Pt On Staff Clinical Care, Quality And Treatment Clinical - Treatment / Care Related Clinical - Difficulty In Obtaining Treatment Staffing - Agency Staff Usage Serious Harming Behaviour Self Harm - Medication Overdose Self Harm - Cut Self Harm - Self Injury Patient Accident Patient - Faint/ Fit / Unwell Found With Injury Fall - Unobserved Fall Mobilising Alone Access, Admission, Transfer Discharge Delay In Admission/ Assessment Absconded (Sectioned Patient) Under 18 Admission Medication Health & Safety Security / Cyber Security Equipment Documentation & Electronic Records Management Fire Information Governance And Confidentiality Skin Integrity Infection Control Mental Health Act Other 16 Active Serious Incident Investigations 15 August 2017 PSI incidents 3 Benchmarking 1 No Harm Low Harm Death DWMH Previous Year 3 Moderate Harm Severe Harm 0 Severe DWMH Previous month 9 5 Death Mental Health Organisations -12 mth Moderate 4 Duty of Candour 4 Low None 0.0% 50.0% 100.0% PSI - Harm Serious Incidents category in the last 12 months Serious Harming Behaviour Patient Accident Access, Admission, Transfer Discharge Disruptive / Aggressive Behaviour Infection Control Clinical Care, Quality And Treatment 100% 50% 0% PSI Incidents level of Harm Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug of the patient safety incidents reported for August were reviewed and 1 meets the criteria for Duty of Candour. The remaining incidents have had support processes applied where appropriate. Please see section 3 for further information. Top 3 Incident Categories Physical Assault - Pt On Staff Clinical - Treatment / Care Rel Verbal Abuse - Pt On Staff No Harm Low Mod Severe Section 1 - This section looks to provide a summary of all of the Incidents and Serious Incidents occuring within the Trust. Trust Incidents - there have been 484 incidents reported within the Trust during the month of August. This represents a 17% decrease when compared to the previous month, however still rmeains high. Distruptive / Aggressive Behaviour remains the highest reported category with 176 incidents reported, despite a 35% decrease on last month. Further breakdown by service lines and Analysis can be found in Section 2 Serious Incidents - 7 Incidents have been reported during the month of August and are currently under investigation. There are currently 15 Active Investigations open to the Trust. A further summary of the Serious Incident cases can be found in Section 3 3
64 4 Section 2 Individual Operational Service line Reports 4
65 Section 2 - Service Line Reports 5 2.1a Inpatient Service Line Top 5 Cause Groups & top 3 Incident Causes August 2017 All Inpatient Incidents 402 Adult Inpatients Older Adults Inpatient Dudley Walsall Dudley Walsall month All - Dud - Wal Adult Inpatients Disruptive / Aggressive Behaviour Physical Assault - Pt On Pt Behavioural - Destructive / Damage To Property Physical Assault - Pt On Staff Clinical Care, Quality And Treatment Clinical - Treatment / Care Related Insufficent Communication - Internal Staffing - Agency Staff Usage Serious Harming Behaviour Self Harm - Medication Overdose Self Harm - Cut Self Harm - Self Injury Patient Accident Patient - Faint/ Fit / Unwell Fall - Unobserved Fall Mobilising Alone Found With Injury Access, Admission, Transfer Discharge Under 18 Admission Absconded (Sectioned Patient) Medication Security / Cyber Security Fire Health & Safety Infection Control IG And Confidentiality Equipment Skin Integrity Mental Health Act Wal Dud Dud Dud Wal Dud Wal Wal Wal Dud Dud Older Adults Inpatient F F mix M M Func Org Func Org Ambleside Kinver Wrekin Clent Langdale Home Treatment Home Treatment Total Clinical Care, Quality And Treatment Clinical - Treatment / Care Related Staffing - Agency Staff Usage Insufficent Communication - Internal Disruptive / Aggressive Behaviour Behavioural - Aggressive Physical Assault - Pt On Staff Physical Assault - Pt On Pt Patient Accident Fall - Observed Fall Mobilising Alone Fall - Observed Fall Chair/Toilet Found With Injury Serious Harming Behaviour Self Harm - Asphyxiation Self Harm - Ligature Self Harm - Self Injury Health & Safety Skin Integrity Security / Cyber Security Medication Documentation & Electronic Records Mgmt Access, Admission, Transfer Discharge IG And Confidentiality Equipment Fire Mental Health Act Infection Control Top 5 Cause Groups & top 3 Incident Causes % 80.00% 60.00% Acute Bed Occupancy Older Adults Bed Occupancy Cedars Linden Malvern Holyrood Total 5

 and Trust Incidents resulting in the use of Physical Interventions.")
66 Section 2 - Service Line Reports 6 2.1b Inpatient Service Line Section 2.1 This section is focused on Inpatient services and looks to show the number of incidents reported during the previous month against a comparison for the last 12 months. This section also looks to provide information in relation to the types of incidents reported, and their risk and impact. This section also shows high level information in relation to Incidents reported to the NHS Safety Thermometer, HSE (RIDDOR) and Trust Incidents resulting in the use of Physical Interventions. Commentary on Section 2.1a There has been an 18% decrease in incidents reported for August 2017 in comparison to the previous month, however numbers still remain high. Adult Inpatient Wards Kinver- There has been a 60% rise in the Disruptive/Aggressive Behaviour category. Of the 32 incidents reported 26 can be attributed to patient A. The patient is pregnant and a known trigger for her is that she refuses to have her medication, which leads to increased agitation. The MAPA team have been involved in supporting staff to administer her IM PRN medications due to her escalating behaviour. There is a care plan in place to assist with her administering the patient s medications. Clent- There has been a 29% decrease in reported incidents. Patient B and C are involved in 13 of 22 incidents which are mainly altercations between the two patients. Therefore, Patient B has been transferred to a PICU due to increased challenging and disinhibited behaviour. Patient C was subsequently transferred to Langdale Ward. Langdale- Patient C was responsible for 7 of the 14 Disruptive/Aggressive Behaviour incidents, these are mainly towards staff. However due to the high level of aggression, the patient has now been placed at a PICU. Ambleside- There has been a 74% decrease in Disruptive/Aggressive Behaviour incidents from the previous month. This is mainly attributed to a patient that was displaying sexually inhibited behaviour, who has since been discharged to an appropriate placement. All Inpatient Incidents August % 95.00% Patient Injuires 12 month trend Staff Injuries 40 Minor 46 2 Moderate 0 1 Injury Major Benchmarking NHS Safety Thermometer - Harm Free Care 0 Physical Intervention Older Adults Inpatient Wards Linden has seen a sustained number of reported incidents when compared to other wards. This is mainly attributed to Patient D, who is responsible for 53 out of 60 of the Clinical Care, Quality and Treatment incidents and 15 of 37 Disruptive/Aggressive Behaviour incidents. This is mainly due to clinical holding having to be used to support their personal care which is a known trigger a positive behaviour plan has been formulated with input from the Psychology Team. They have reviewed the patient s documentation and have formulated a robust plan which is broken down into sections to identify early warning signs for the patient detailing exactly how they can respond to each scenario without further provoking or distressing the patient. Patient E is also responsible for 15 Disruptive/Aggressive incidents. This patient suffers from severe cognitive impairment and short term memory loss and is an imminent risk of falls, requiring a crash mat in her room. The patient requires support with mobility and this escalates her behaviour. Therefore, a clinical decision has been made to use clinical holding in the patient s best interests to assist the patient. This has been fully incorporated into her care plans. Holyrood- There has been a 59% reduction in incidents under the Disruptive/Aggressive Behaviour category. This is mainly attributable to a reduction in the number of incidents in relation to 1 patient who has now had a full medication review, resulting in improvements in their presentation and this is reflected in the incident numbers % DWMH DWMH 12 month Average National 12 month Average Health & Safety Excetive 0 Patients Involved 20 Adult 43 Inpatients 161 Older injury was reported as a result of Physical Intervention but this was low harm Patients Involved 16 6
67 Section 2 - Service Line Reports Urgent Care & Access Services August 2017 All Urgent Care & Access Services 22 Dudley Locality 15 Walsall Locality 7 Department & Incident Category Aug Dudley Talking Therapy Service 7 Serious Harming Behaviour 3 Disruptive / Aggressive Behaviour 2 Patient Accident 1 Equipment 1 EAS (Dudley) Sandringham 6 Access, Admission, Transfer Discharge 2 Clinical Care, Quality And Treatment 2 Serious Harming Behaviour 1 Equipment 1 Psychiatric Liaison Team - Dudley 2 Serious Harming Behaviour 2 PC MH & TTS 2 Serious Harming Behaviour 1 Clinical Care, Quality And Treatment 1 Psychiatric Liaison Team - Walsall 2 Serious Harming Behaviour 2 Crisis Resolution - Walsall 2 Mental Health Act 1 Clinical Care, Quality And Treatment 1 EAS (Walsall) 1 Clinical Care, Quality And Treatment 1 Grand Total 22 Reported Injuries 1 Injuries Patient Staff Minor Injury 0 1 Moderate Injury 0 0 Major Injury 0 0 Commentary Section 2.2 This section is focused on the Urgent Care & Access Servies and looks to show the number of incidents reported during the previous month against a comparision for the last 12 months. This section also gives a break down of the incidents by Locality, and also shows the number of Injuries. The monthly (mean) average for incidents relating to Urgent Care & Access Services (calculated using data from the last 12 months, and as a combination of the previous individual Services) is 25. Serious Harming behaviour continues to be highest reported category within this service, totalling 9 in August. No trends were identified as this was distributed across the departments. 7
68 Section 2 - Service Line Reports Community Services August 2017 All Community Services Dudley Locality Walsall Locality Aug CMHTOP Walsall 3 Clinical Care, Quality And Treatment 2 Equipment 1 CRS South (Dudley - Hales) 3 Clinical Care, Quality And Treatment 2 Information Governance And Confidentiality 1 Memory Services (BVC) 2 Clinical Care, Quality And Treatment 2 Woodside (CMHTOP) 2 Disruptive / Aggressive Behaviour 1 Clinical Care, Quality And Treatment 1 CRS South (Dudley - HH) 2 Disruptive / Aggressive Behaviour 1 Clinical Care, Quality And Treatment 1 CRS North (Walsall - Moss) 1 Clinical Care, Quality And Treatment 1 CRS South (Walsall AM) 1 Access, Admission, Transfer Discharge 1 Psychological Therapies Hub (HH) 1 Clinical Care, Quality And Treatment 1 Grand Total 15 Injuries Minor Injury Moderate Injury Major Injury Commentary Reported Injuries 0 Patient Staff Section 2.3 This section is focused on the Community Services and looks to show the number of incidents reported during the previous month against a comparision for the last 12 months. This section also gives a break down of the incidents by Locality, and also shows the number of Injuries. The monthly (mean) average for incidents relating to Community Services (calculated using data from the last 12 months, and as a combination of the previous individual Services) is of the incidents reported under the category of Clinical Care, Quality And Treatment, are deaths where patients have been known to our service however passed away from Natural Causes. All Deaths are reviewed by the Trust's Mortality Review Group. There are no further trends or significant incidents relating to this service. 8
69 Section 2 - Service Line Reports Early Intervention Services August 2017 All Early Intervention Services Dudley Locality Walsall Locality Department & Incident Category ICAMHS Dudley (Elms) 13 Serious Harming Behaviour 12 Clinical Care, Quality And Treatment 1 ICAMHS Walsall (Canalside) 7 Serious Harming Behaviour 7 CAMHS Dudley (Elms) 6 Serious Harming Behaviour 2 Disruptive / Aggressive Behaviour 1 Security / Cyber Security 1 Documentation & Electronic Records Management 1 Equipment 1 CAMHS Walsall (Canalside) 1 Serious Harming Behaviour 1 Positive Steps (Tier 2) (D) 1 Equipment 1 Early Intervention In Psychosis (Dudley) 1 Disruptive / Aggressive Behaviour 1 Grand Total 29 Aug Injuries Minor Injury Moderate Injury Major Injury Commentary Reported Injuries 3 Patient Staff 2 Section 2.4 This section is focused on the Early Intervention Services and looks to show the number of incidents reported during the previous month against a comparison for the last 12 months. This section also gives a break down of the incidents by Locality, and also shows the number of Injuries. The monthly (mean) average for incidents relating to Early Intervention Services (calculated using data from the last 12 months, and as a combination of the previous individual Services) is 40. There was 1 case of Serious Harming Behaviour which has been recorded as moderate harm by Walsall ICAMHS. This was an overdose requiring treatment, patient had previously been seen by ICAMHS and is open to Sandwell CAMHS. There were 2 cases of Serious Harming Behaviour recorded as moderate harm by Dudley CAMHS. 1 resulted in a safeguarding referral to Childrens' Services and 1 was an overdose requiring treatment by a patient not open to services. All other Incidents have been recorded as Low or No Harm 0 0 9
70 10 Section 3 Serious Incidents 10
71 Section Serious Incidents and Duty of Candour 11 Table List of Serious Incident raised during the month of August 2017 SI Number Date of Incident Service Line Incident Description Level of Risk DoC applicable Family Engagement Level of response 2017/ Dudley Outpatients Completed Suicide - Medication Overdose High No Yes Comprehensive Dudley 2017/ Bloxwich Hospital Linden Ward Fall - Observed Fall Mobilising Alone Moderate Yes Yes Concise Walsall 2017/ Dudley ICAMHS Under 18 Admission Low No No Concise Dudley 2017/ Walsall Early Intervention Under 18 Admission Low No No Concise Dudley 2017/ Dudley MHAS Completed Suicide - Asphyxiation High No Yes Comprehensive Dudley 2017/ Dudley PLT Completed Suicide - Ligature High No No Concise Dudley 2017/ Home Treatment Walsall Completed Suicide - Substance Overdose High No Yes Comprehensive Walsall Locailty Commentary The monthly (mean) average for Serious Incidents across the Trust (calculated using data from the last 12 months) is 3.5. Table 3.1 shows a list of the Serious Incidents logged on STEIS during the previous month, this includes details of the service line and nature of the incident. There have been 7 Serious Incidents reported for the month of August 2017, 4 suicides, 2 under 18 admissions and 1 fall. Chart 3.1 illustrates the types of the Serious Incidents that have been reported over the previous 12 months. Details of all active Serious Incidents can be found in the section below. Chart Summary of the Serious Incident types during the last 12 months 7% 9% 14% 5% 5% Serious Harming Behaviour 60% Patient Accident Access, Admission, Transfer Discharge Disruptive / Aggressive Behaviour Chart Total number of Serious Incidents during the last 12 months Infection Control Clinical Care, Quality And Treatment Serious Incidents Average Mean + S.D. Mean - S.D. 11
72 Section Serious Incidents and Duty of Candour 12 Serious Incident Case Summaries - Reported Previous Month SI Number Date of Service Line Incident Description Status Current Status Incident 2017/ Dudley Outpatients Patient was found at home with an empty packet of tablets next to her, and a message to her children was left on the mirror in lipstick Investigation remains on-going, to date no concerns or themes have been identified from the initial information. The investigation has highlighted the patient was accessing her GP, Summit House and Social Services were involved, we are currently liaising with this to gain further information. 2017/ Bloxwich Hospital Linden Ward Patient unfortunately lost his balance and experienced a fall. Patient was transferred to the Manor Hospital, however, no fracture was evident. Further x-rays carried out, which showed that the patient had a relatively undisplaced intertrochanteric fracture. 2017/ Under 18's admission (turned 17 January 17). Patient was admitted to Clent Ward under Section 2 of the Mental Health Act, due to no Tier 4 beds being available. Patient is currently on 1:1 obs. Safeguarding Lead and Designated Nurse informed. 2017/ Under 18's admission (turned 17 on 01 September 16). Patient was admitted to Wrekin Ward under Section 2 of the Mental Health Act, due to no Tier 4 beds being available. Safeguarding Lead and Designated Nurse informed. Unable to contact the family Investigation remains on-going, to date no concerns or themes have been identified from the initial information Review remains on-going Review remains on-going 12
73 13 Section Serious Incidents and Duty of Candour 2017/ Dudley Mental Health Assessment Service 2017/ Dudley Psychiatric Liaison Team Patient took his own life in the family home, using chloroform and a plastic bag. Patient was found hanged at his home address on 15/08/17. Patient was previously seen in A&E by our Psychiatric Liaison Team on 8th April 2017, following an episode of self-harm - patient was also intoxicated at the time Investigation remains on-going, to date no concerns or themes have been identified from the initial information. Internal independent clinicians have been allocated Family have been engaged in the investigation process Investigation remains on-going, to date no concerns or themes have been identified from the initial information. Internal independent clinicians have been allocated. 13
74 Section Serious Incidents and Duty of Candour 14 Serious Incident Case Summaries - Ongoing / Open Cases SI Number Date of Incident Service Line 2017/ Crisis Dudley 2017/ Bloxwich Hospital Cedars 2017/ Community Recovery Service Dudley North Incident Description Status Current Status Patient was open to CRHT in August 2011, however, was discharged back to the care of her GP in September Patient s family made contact with the Crisis Team in April 2017, to say that their Mother's mental health had deteriorated since Christmas Reported by Street Triage that patient had been found deceased, allegedly by hanging. Upon admission on 02/07/2017, the patient was placed on level 2 observations, however, this was reduced to level 1 on the morning of 03/07/17. The patient was also assessed as medium risk of falls. At around 22:50 on the 03/07/2017, the patient was observed to get out of his chair and fall to the floor when attempting to mobilise with his walking stick, by the time staff were able to intervene he had already fallen to the floor. Phone call received from patient s son to say that he had not been able to get in touch with his mother, and was concerned. Team carried out a safe and well check, however, unfortunately, upon arrival patient could be seen through window, and was unresponsive to staffs calls. Staff called an ambulance, who attended and pronounced the patient dead at the scene. Patient had reportedly taken a large dose of Tramadol and Amitriptyline. STOP CLOCK No further updates since the Potential SCR/DHR meeting held on 26 June have been received. It was agreed that a safeguarding enquiry would take place led by social care and followed up with a case conference to review and make a decision as to whether it meets the criteria for a DHR Investigation has been completed, no care or services delivery issues have been identified. Awaiting final approval Investigation remains on-going, to date no concerns have been identified. The investigation is due to conclude the 28 th September 17, this is due to clinicians involved being on annual leave. Coroners Reports has been completed and submitted no medical concerns identified. 2017/ BFH Wrekin Ward Under 18's admission (17, but due to turn 18 in October). Patient was admitted to Wrekin Ward under Section 3 of the Mental Health Act, due to no Tier 4 beds being available. Patient was on 1:1 obs. Safeguarding Lead and Designated Nurse informed. Family have been engaged in the investigation process Awaiting final approval availability of a Tier 4 bed at the time has been identified as the root cause. 14
75 15 Section Serious Incidents and Duty of Candour 2017/ BFH Malvern Ward 2017/ DPH Ambleside Ward Patient was being escorted from Birch Day Hospital to Malvern Ward. Patient unfortunately tripped on a curb falling heavily on to her left side. X-rays showed that patient has broken two bones in her elbow, which is currently in a cast. Staff were alerted to the patient bathroom where material was seen on top of the door. Staff entered, pushing the door open. Staff reported that it sounded like the patient fell, emergency alarms were then pressed. Patient was found with her jumper used as a ligature around her neck, member of staff removed this. Blood was observed to patient s nose, and she appeared to be grey in colour. Patient was responding to pain stimuli only, but not responsive to voice or touch prior to transfer to Walsall Manor Hospital Investigation has been completed, no care issues have been identified. The investigation has highlighted the parked car obstructing the pathway as the root cause. Awaiting final approval Table Top Review has been undertaken with attendance from the clinical staff involved in the patient s care, Medical Director, Acting Director of Nursing, Health and Safety and Internal Independent Clinicians. The root cause has been identified as the patient s attempted severe self-harm with the intention of ending her life as a result of a persistent fluctuations in her mood driven by elements of a depressive illness, long standing personality behavioural traits and more recent personal conflicts which she had disclosed to the multidisciplinary team. The investigation has highlighted learning points which will be shared once the investigation is completed. Family have been engaged in the investigation process. The investigation has also highlighted the excellent response from the ward staff and medic responding to the incident. 15


76 16 Section 4 National Guidance Central Alerting System 16
77 17 Section 4: CAS Alerts Table 4.1 Summary of Alerts received during August 2017 Number of Alerts in August Action not Assessing Action Type of Alert Required Relevance Required MDA MHRA CMO DDL EFN DH EFA DH SDA NHS PSA Total Circulated for Information During August 2017 there were 18 alerts issued via the Central Alerting System, of these 18 alerts: o The Trust is assessing the relevance of 1 alert o 15 alerts required no action taking o 1 alert has been circulated for information. o 1 Alert in relation anti-barricade devices requires action from the Trust The table below (4.2) outlines a summary of the alerts issues and any action taken. Alert Number EFN/2017/15 (U) EFN/2017/26 Table 4.2 Alerts issued during August via the Central Alerting System EFN/2017/26R Alert Date Description of Alert Status Notes / action taken / assurance 04-Aug- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - UPDATE - Schneider Electric Action not The Trusts authorising officer acknowledged RN6c - Ring Main Unit required receipt of the alert and that no action was required 07-Aug Aug High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - ABB - Series 2 SDAF - Ring Main Unit High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - ABB - Series 2 SDAF - Ring Main Unit Action not required Action not required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust 17
78 18 Section 4: CAS Alerts Alert Number CEM/CMO/20 17/004 NHS/PSA/RE/ 2017/004 EFN/2017/27 EFN/2017/28 EFN/2017/29 MDA/2017/021 MDA/2017/022 MDA/2017/023 EFA/2017/002 Alert Date Description of Alert Status Notes / action taken / assurance 07-Aug- Shortage of adult Hepatitis B vaccine Circulated for The alert was circulated in line with the 2017 There is a global shortage of hepatitis B vaccine which is currently impacting severely on the UK supply. The information requirements of the alert situation particularly critical during August but there is likely to still be some limitations on supply until early 11-Aug Aug Aug Aug Aug Aug Aug Aug Resources to support safe transition from the Luer connector to NRFit for intrathecal and epidural procedures, and delivery of regional blocks This Alert supports providers with the safe transition from the Luer connector to NRFit for intrathecal and epidural procedures, and delivery of regional blocks. The Alert signposts providers to the supporting information to help them recognise the risks to patients and to manage the process as safely as possible. High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Hawker Siddeley Switchgear Ltd - URV12 - Circuit Breaker High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Schneider Electric - Genie Evo - Circuit Breaker High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - Hawker Siddeley Switchgear Ltd - Eclipse - Circuit Breaker VITEK 2 Identification (ID) / Antimicrobial Susceptibility Test (AST) Cards potential false resistance for antibiotics on the AST panel, leading to false negative ESBL test or false positive urea (URE) reaction on ID cards. DePuy Synthes Impactor for PFNA (Proximal Femoral Nail Anti-rotation) Blade: risk of infection Shoulder system: Comprehensive Nano Humeral Components increased risk of revision when used in reverse configuration Anti-Barricade Devices: risk of ineffectivity in certain circumstances The purpose of this Alert is to advise that in certain circumstances some anti-barricade devices, that may have been fitted to doors to manage the risk of barricade situations occurring, may be rendered ineffective. This increases the risk of avoidable harm and self-harm until the room can be accessed. Action not required Action not required Action not required Action not required Action not required Action not required Action not required Action required The Trust does not conduct epidural and intrathecal procedures The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trust does not have a laboratory service where such devices would be used These are used in trauma care. The Trust does not provide services where such a device would be used The Trust does not undertake surgery, as such no action was required in relation to this particular alert The Trust is currently undertaking a piece of work to look at its compliance against the requirements of the alert. Full details of the alert is outlined below. Anti-barricade devices include mechanical fittings such as latches, hinges and special locks used to prevent doors being used as barricades. 18
79 19 Section 4: CAS Alerts Alert Number MDA/2017/024 MDA/2017/025 MDA/2017/026 MDA/2017/027 MDA/2017/028 MDA/2017/028 (R) Alert Date Description of Alert Status Notes / action taken / assurance 24-Aug- Insulin pens: NovoPen Echo and NovoPen 5 (certain batches) risk of hyperglycaemia due to cartridge Action not The Trust would not be issuing these devices, as 2017 holder weakening when exposed to certain household chemicals required such no formal action is required in relation to this alert. The alert has however been circulated to 24-Aug Aug Aug Aug Aug Nail intramedullary fixation system: Trauma guide wires 70cm risk of infection Manufactured by Zimmer Biomet Recall due to risk of infection if the wire breaks through the packaging Overhead hoist: Freeway Easy Fit system with a swivelling trolley risk of fixing pin moving or splaying Manufactured by Prism splayed or misplaced pins may lead to the hoop detaching and dropping the sling. Intra-aortic balloon pump (IABP): CS100, CS100i and CS300 risk of haemodynamic instability to patients with critical conditions due to a delay in or sudden interruption of therapy Replacement bileaflet mechanical heart valves risk of inverted implantation Specific manufacturers measures to prevent inverted valve implantation resulting from incorrect mounting of the valve on its valve holder Replacement bileaflet mechanical heart valves - risk of inverted implantation Specific manufacturers measures to prevent inverted valve implantation resulting from incorrect mounting of the valve on its valve holder Action not required Assessing Relevance Action not required Action not required Action not required staff for information These are used in trauma care. The Trust does not provide services where such a device would be used The Trust is currently assessing whether it uses any of these devices The Trust does not use these devices The alert was superseded by alert MDA/2017/028(R) The Trust does not use these devices Summary of alert EFA/2017/002 The alert requires the Trust to: 1) Bring this alert to the attention of all appropriate managers, staff and specialist advisors 2) Identify rooms where aggressive situations are likely to occur and review the effectiveness of existing anti-barricade protection, e.g. mechanical fittings including latches, hinges, and special locks which are used to prevent doors being used as barricades. Evaluation criteria for anti-barricade devices should include tamper resistance. 3) Where anti-barricade devices are found to be missing or ineffective: a) Carry out a collaborative multi-disciplinary risk assessment in-situ at department level. b) Identify and implement suitable mitigation measures, e.g. alternative means of gaining access to the identified rooms. c) Ensure violence and aggression risks work together with all other key performance needs, e.g. therapeutic, fire, privacy, equality, infection control. If any compromises are necessary, these and their mitigations should be recorded by the multi-disciplinary group. d) Test a range of likely circumstances in-situ. 19
80 20 Section 4: CAS Alerts 4) Arrange a schedule of periodic collaborative multi-disciplinary reviews of procedures, devices and environments for managing risk. Identify and implement suitable risk assessment and risk management plans for individual patients and ensure that they are treated in the most appropriate environment. Include the suitability of existing mitigation measures, e.g. anti-barricade devices, taking account of any changes to safe systems of working as well as to each space s purpose or layout. 5) Collaborative multi-disciplinary reviews should also be carried out if there is a significant change, e.g. clinical or service modifications, physical alterations, refurbishment and maintenance activities. 6) Schedule and carry out routine testing and maintenance in accordance with manufacturer s instructions. The compliance and Safety Team are in the process of arranging a meeting to take forward the requirements of the alert and agree a work plan in relation to this alert. The alert has a completion deadline of 19 th February
81 21 DWMHT Safeguarding Performance Framework 2017/18 Section 1 Safeguarding Training Compliance (to follow) Section 2 Deprivation of Liberty (DoL s) Domestic Violence Section 3 Safeguarding Children (including CAMH s LAC) Vulnerable Adults 21
82 Safeguarding 22 Training Compliance Training Data Month 4 DWMH 12 month Trend Corporate / Pan Trust Compliance Target Compliant Required Compliant % High point Compliant Required Compliant % Compliant Required Compliant % Compliant Required Compliant % compliance Low point compliance compliance compliance Safeguarding Induction 100% % % % % Safeguarding Adults Lvl 1 90% % % % % Safeguarding Adults Lvl 2 90% % % % % Safeguarding Adults Lvl 3 90% % % % % Safeguarding Adults Lvl 4 90% % % Safeguarding Children Lvl 1 90% % % % % Safeguarding Children Lvl 2 90% % % % % Safeguarding Children Lvl 3 90% % % % % Safeguarding Children Lvl 4 90% % % Mental Capacity Act 90% % % % % PREVENT 90% % % % % Domestic abuse & Violence 60% % % % % Dudley Walsall Exceptions / Commentary This section shows the latest Training requirement and compliance levels as set out in the Commissioner Contract for 2017/18, related to Safeguarding and Vulnerable Adults. Within the contract there are agreed trajectory requirements. Adult Safeguard Training - Children's Safeguarding Training - Q1-90% Q1-90%Compliance as detailed in the table above. Q2-90% Q2-90% Q % Q % Q % Q % Mental Capacity Act (MCA) and Deprivation Of Liberty (DOL s) Prevent Domestic Abuse Q1 90% Q % Q1-60% Q2 90% Q % Q2-70% Q % Q % Q3-80% Q % Q % Q4-90% 22
 - This shows the total number of active cases of DOL's, broken down by Locality DOL's Closed 6 1 5 1 2 5 2 1 NHS Walsall 5 6 7 4 3 11 5 3 13 3 1 DOL's Applied For 2")

83 23 Safeguarding Performance Framework for August 2017 Section 2 - DoL's and Domestic Violence 2.1 Deprivation Of Liberties (DOL's) - This shows the total number of active cases of DOL's, broken down by Locality DOL's Closed NHS Walsall DOL's Applied For DOL's Closed Out of Borough 1 2 DOL's Applied For 1 1 DOL's Closed 1 Grand Total Active DoL's Linden Cedars Grand Holyrood Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Total Malvern NHS Dudley Adult Langdale DOL's Applied For Total Commentary Table 2.1 This table shows the activity in relation to cases of Deprivation Of Liberties (DOL's). This information is broken down by locality and shows the current number of Active cases, and activity for the last 12 months. There were 10 new DoLS applications during the month of August 8 in Dudley, 1 in Walsall and 1 Out of Borough which has since been discontinued following admission to the local acute hospital. There are currently 21 DoLS cases active 7 in Walsall and 14 in Dudley. The is one active DoLS case on Langdale Ward. There are 3 DoLS case that have been active prior to the 12 month period shown. Table 2.2 Domestic abuse cases are reported as separate figures to display the prevalence within the service. Case figures are also sh own for MARAC (multi agency risk assessment conference), these figures demonstrate how many cases are heard at MARAC where the victim, perpetrator or children are open cases to mental health. The first table provides information on Cases reported Externally of the Trust which are then checked to see if these Patient s are open to Dudley and Walsall Mental Health. The second table provides information on Domestic Abuse cases which have been reported internally into our Trust *3 DoL's cases have been active prior to the 12 month period shown above Older Adult 2.2 Domestic Abuse NHS Dudley Dudley NHS Walsall Out of Borough Total number of cases of Domestic Violence for the current month, these include cases reported within the Trust and Externally notified by MARAC (Multi-Agency Risk Assessment Conference) Walsall Open To Mental Health Referred into MARAC MARAC Safeguarding Cases Internally reported as Domestic Abuse Alert Only Referral Open To Mental Health Referred into MARAC Jul
84 Safeguarding Children Safeguarding Performance Framework for August 2017 Graph This graph provides information relating to the last 12 months and shows a breakdown of Safeguarding cases which are just for alert only and those which have been progressed to be continued under Safeguarding Table 3.1 -This shows that the number of Safeguarding cases broken down by case type and showing the locality. This also shows information on whether the case is for alert only or if it has been referred for further investigation to another agency. Table This table provides information in relation to Looked after Children (LAC), who have been referred or in receipt of our services. During the month of August there were 3 under 18 admissions incidents. Two of the admissions related to one person who was re-admitted following discharge to an appropriate placement. Both service users were Walsall residents but admitted to Dudley wards. Each admission was managed and documented appropriately as per the Under 18 Admission Policy and they have now been discharged. There have been 3 Prevent notifications received from Channel for services users known to the Trust. All cases have been reviewed and appropriate information shared. There were 4 child protection notifications received this month, however work is ongoing with CAMHS to ensure that the agreed indicators are included in their data collection. The SCR scoping event scheduled for last month in Walsall has been completed and meets the criteria for a Serious Case Review. Table 3.1 Total number of Safeguarding Children cases for the current month Child Safeguarding Case Patient considered High Risk Position of Trust Internal Position of Trust External Under 18 Admission Under 18 Death FGM Prevent Serious Case Review (Child) Grand Total Dudley Walsall Grand Referral Alert Only Referral Alert Only Total Table Looked after Children (LAC) Total number of cases of Looked after Children Dudley Walsall Number of Looked after Children Total Grand Total Graph Total number of Safeguarding Children incidents reported during the last 12 months 0 New Performance indicators /18 As part of the new Commissioner Contract for 17/18 additional indicators have been introduced (shown below) for which the trajectors have yet to be agreed, and will be based on the data set in Q1. 4 notifications have been received regarding Child Protection Cases during Month 5 Number of invitations to Initial Child Protection Conferences Rate of attendance at Initial Child Protection Conferences Rate of report submission to Initial Child Protection Conferences Rate of report-sharing with parent/child prior to Initial Child Protection Conferences Number of invitations to Review Child Protection Conferences Rate of attendance at Review Child Protection Conferences Rate of report submission to Review Child Protection Conference Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Alerts 2017 Referral 24

85 Vulnerable Adults Safeguarding Performance Framework for August 2017 Graph 3.2 -This graph provides information relating to the last 12 months and shows a breakdown of Vulnerable Adults Cases which are just for alert only and those which have been progressed to be continued under Safeguarding. Table 3.2 This shows that the number of Vulnerable Adults cases broken down by case type and showing the locality. This also shows information on whether the case is for alert only or if it has been referred for further investigation to another agency. It is to be noted that the Position of Trust incident reported last month on Ambleside was substantiated. However there has been a further two incidents reported from the ward this month of which 1 was not substantiated and 1 is ongoing. These incidents involve bank and agency staff only. There have been 4 Prevent notifications during the month of August in Dudley which were reviewed and monitored appropriately. There has been 1 FGM concern which did not require mandatory reporting duty as it related to concerns around the risks for the service users children following their unsuccessful application to remain in the UK. Safeguarding procedures were followed and a referral made to children s services. Table Total number of Vulnerable Adults incidents for the current month Graph 3.2 Total number of Vulnerable Adults incidents reported during the Last 12 Months Adult Patient Considered High Risk Position Of Trust Internal Position Of Trust External Prevent Case Serious Adult Review DHR FGM Grand Total Dudley Walsall Grand Referral Alert Only Referral Alert Only Total Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug 2017 Alerts Referral 25
86 Board meeting date: 5 October 2017 Report Title: Agenda Item number: 7.1.3a Enclosure: 9 Finance and Performance Committee Chair Report Committee: Finance and Performance Committee (F&P) Author (name & title): Harry Turner Non Executive Director Action required from the Board Decision / Approval Gain assurance Key issues & risks Discussion Information The Finance and Performance committee met on the 25 th September to consider the Finance and CIP information for August (Month 5). The Committee reviewed the following items of business: Performance The report tabled was accepted and the following areas were noted: Activity overall is 5.3% above contract KPIs Under-performance against 4 of the agreed 27 KPI s, namely achievement of adult inpatient length of stay within Dudley of less than 40 days (red), CPA within 7 days (amber), Delayed Transfer of Care for Dudley (amber) and the number of patients receiving IAPT therapy (both localities both amber) Data Quality Improvement Plan The report was tabled and accepted. PbR & Clustering Report The report was tabled and accepted. Finance Report & Income/Activity Report The finance report was presented. The financial position to the end of August 2017 showed a 933k surplus which was 27k ahead of the plan to date (based on the planned annual surplus of 1,839k). Enc 9 FandP Chairs report (M05) Page 1 of 3
87 In August Contracted Income reflected an adverse variance of 69k. This has been driven in part by the additional CIP of 200k Full Year Equivalent placed on Non Contract activity which has been slow to start at the beginning of the year, as well as the shortfall in Detox bed use. Income overall is in surplus by 13k which is being driven by education and training income, offsetting the adverse contracted income position mentioned above. It was noted that both Dudley and Walsall contracts were indeed over-performing in their true sense to the value of 100k and 460k respectively to Month 5. Agency spend was discussed in light of the NHSI agency cap of 4.05m. The position year to date as of month 05 is reporting an underspend of 148k and has been good progress so far during the financial year. Overall Pay spending is in surplus and is continuing to follow the trend of underspends as experienced throughout the previous financial year Year-end projected forecasts were reviewed and it was highlighted that there is still an expectation to deliver a balance FOT position and thus achieve the 1.8m surplus control total. The initial view from Finance based on service line knowledge was suggesting a risk of around 600k to the forecast outturn and as a result a further 500k risk around payment of 500k STF funding. The potential surplus position for the Trust could therefore be as low as 739k. CIP performance now reflects a delivery of 2.9m against the 3.8m target for the year. Even though progress is positive it was highlighted to the committee that there is still a reliance on non-recurrent means of delivery against the CIP target which would have an impact on next financial years CIP target. Finance Outturn Following the update to the forecast outturn position above an additional paper was discussed which reviewed the 12 risk areas that had been identified in a similar paper presented to the Committee last month. The Committee was updated in relation to these 12 risks in relation to those that had been taken account of in terms of the 600k risk identified by the Finance team within the Finance report above. The committee agreed that of the 12 identified risks (totaling around 1.4m potential risk) the risks should be assessed, rag-rated and a plan put in place to minimize and/or mitigate the risk. A proposed forecast outturn position was discussed for each service line that would ensure the 1.8m surplus control total could be delivered It was requested by the Committee that management action be taken to ensure delivery of the forecast outturn targets mentioned above. Operational leads along with the support of Finance need to have sight on the risks and the actions required to deliver against financial pressure and, ensure that a balanced forecast outturn is achieved for the Trust as a whole. The Director of Finance, Performance and IM&T and Interim Director of Operations agreed to raise this urgently at MExT with a view to progressing this at pace. Enc 9 FandP Chairs report (M05) Page 2 of 3
88 CIPs The Committee reviewed a paper that detailed the potential shortfalls against the in year CIP target of 3.7m. The Committee agreed the need to update and close off the outstanding 2016/17 schemes and looking forward to 2018/19, requested clarity around the approach going forward to CIP monitoring and delivery. Contractual Delivery Against Service Lines The Interim Director of Operations tabled and led the committee through the paper which will serve as the basis for discussions with commissioners at the upcoming contract negotiation rounds for 2018/19 contracts. The paper was noted and accepted. Risk Registers Risk registers for both Finance/Performance and Estates/Capital were tabled. They were accepted by the Committee. E&CPG Minutes The minutes from the Estates & Capital Planning Group were tabled and accepted. Reference Costs It was agreed that this would be circulated to Committee members for the next meeting. Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees/Groups: MEXT Audit Committee Governance & Quality Committee CARM CQR Recommendations and requests for direction Trust Board is asked to:- Accept this report for assurance about the exercise of delegated authority by the Finance and Performance Committee Endorse the decisions and recommendations made by the Finance and Performance Committee. Enc 9 FandP Chairs report (M05) Page 3 of 3
89 Board meeting date: 5 October 2017 Agenda Item number: 7.1.3b Enclosure: 10 FINANCE & PERFORMANCE COMMITTEE MEETING Minutes of a Meeting Held on Wednesday 30 th August 2017 Conference Room 2, Trafalgar House, Dudley START TIME 10:00 HOURS Present: Harry Turner Rupert Davies Dr Mark Weaver Ashi Williams In Attendance: John Burbeck James Parker Mark Banks Jeanette Rooke Apologies: Mark Axcell Dr Kate Gingell Lesley Writtle John Lancaster Pawiter Rana Dan Howard Rosie Musson Makhan Singh Paul Chamberlain Non Executive Director (Chair) Interim Director of Finance Joint Medical Director Acting Director of People Associate Non Executive Director Commissioner Liaison Manager Deputy Director of Finance Note Taker Chief Executive Officer Joint Medical Director Acting Director of Operations Non Executive Director Non Executive Director Head of Business Intelligence and IM&T Acting Director of Nursing Principal Consultant, Information & Performance Head of Financial Planning Enc 10 FP Minutes (Final) Page 1 of 6
90 42 Apologies For Absence ACTION 42.1 Apologies noted as above. 43 FINANCE 43.1 Finance Report Month 4 Mr Turner explained the reason for the extraordinary meeting being called with regards to some concerns with in relation to finances presented to Trust Board from the previous meeting. Mr Turner introduced John Burbeck as one of the new nonexecutive directors. Mr Banks talked through the Month 4 finance report. The outturn positions 779k surplus, 47k ahead of the plan. Pay position is surplus of 160k. Vacancy CIP position was explained. Mrs Williams collaborated vacancies to be confirmed with Mr Banks at a later date ready for Trust Board report next week. Mrs Williams Bank and agency spend 200k below forecast. Good performance expected to continue. Non-pay expenditure indicates some overspends showing a 122k impact. CCG Contracts on block so no financial impact. Underspend due to detox beds and NCA s. Other income Category B training and Category C. Income generation reflecting a surplus of 31k. CCG contracts if paid for actual activity would reflect an over performance of 130k for Dudley and 450k for Walsall. 1.5 to 2m expected at year-end. Mr Parker mentioned a recovery plan was in place and this will be presented to September s F&P committee. Mr Parker Mr Turner asked for this to be brought to the F&P report with regards progress making to give Board assurance though we may not have the figures. Mr Burbeck questioned as to Walsall s perception this was alleviated with other bigger concerns with other contracts include Walsall Acute and their own financial pressures. Risk share agreement needs to be implemented and is the way forward and this was agreed or a more generous block Mr Davies/Mr Banks Enc 10 FP Minutes (Final) Page 2 of 6
91 payment. 3 or 4 CIP schemes at risk. Schemes are guaranteed to deliver to that forecast re. 2.8m certainty. Capital slow pace 139k awaiting various invoices (Sandringham). Business case re. Clee for a 400k capital requirement. Mr Turner expressed concerns on this figure. Mr Davies explained this is not a committed figure and an explanation will be presented to the Trust Board. Mr Davies/Mr Banks Mr Banks explained the summary Income and Expenditure statement highlighting key areas. Mr Burbeck queried the surplus within early intervention of 122k the assumption being that by year-end this will be spent. Mr Turner raised concerns in regards to Inpatient Services showing a 394k forecast overspend against budget. Mr Banks explained that this was being looked at with regards to possibly recovering costs from Commissionaire re. special observations. Dr Weaver clarified the issues being faced within the in-patient group. Drill down has been implemented. Mr Turner stressed the importance of giving Trust Board assurance that this committee is scrutinizing figures presented to ensure effective commentary is fed back. It was agreed that budget holders should be asked to present to the committee in order to clarify large over-spends. This was agreed to be a positive move but was not for discussion at this meeting. Mr Burbeck queried interventions implemented, whereby Dr Weaver gave some examples of interventions. Mr Davies explained how acuity is dealt with on hospital wards. Mr Turner queried the year-end zero position the aim should be to show a surplus at year-end. Mr Banks explained the STF funding is built into the overall 1.8m control total. By securing a surplus this would secure 500k. Mr Burbeck queried the figures on various enclosures which do not appear to tally. Mr Davies clarified the budget analysis which shows some of the operational budgets but also includes some income lines. Mr Banks clarified Slide 6 (income). Slide 9 (forecast) was explained in more detail some of the service lines were analysed. These figures are lifted via Slide 5. A zero position means that we achieve the 1.8m and we are loading this through the 900k reserves. Enc 10 FP Minutes (Final) Page 3 of 6
92 Mr Banks service lines could be manipulated by working more closely with the managers. Mr Turner reiterated that the figures need to be analysed and budget holders accountable. Mr Turner explained that he would find it useful to have year on year analysis in future and more detail around margins. Mr Banks Mr Davies explained the main issue is around in-patients expenditure. The current levels of bank and agency staffing is a concern. Dr Weaver gave further details with regards to existing staffing arrangements across the wards, particularly female wards and having not had a Head of Service for some time which has had an impact on other leaders/ managers. Mr Parker explained that Debbie Cooper would welcome further scrutiny and this would be agreed with Lesley Writtle (LW) and brought to the next meeting. Mr Parker explained that outcharging work in progress with Mrs Writtle. Mr Banks explained Slide 11 (CIP) in more detail highlighting additional funds shown within the cost improvement programme re. CIP 12 and CIP 14. This shows a potential carry forward deficit issue with CIP into next year Year-End Forecast Mr Davies moved on to the forecast. Calculation of the run rate for was explained in more detail. The figures presented are based on the current ledger showing 2.343m at year-end. Adjusting the run rate for expected profiling issues was then explained that adjustments for profiling shows 1.988m at yearend. Financial risks in the system were clarified over the run rate. 12 risks were highlighted. At worst 2.4m but expected was shown as 1.4m. Mr Turner asked for clarification re. the 1.4m could this have an impact to Mr Banks s figures the answer was yes. Mr Davies explained that this is nothing to do with reserves. Mr Turner asked for clarification on the year-end position in order to report back to the Board in an accurate fashion. Mr Davies explained that these risks were likely if we did not manage them. Mr Burbeck highlighted that the best case risk is 872k that should then be taken out of Mr Banks s forecast figures. Mr Turner clarified that Mr Banks s figures show a break even Enc 10 FP Minutes (Final) Page 4 of 6
93 position at year-end but the forecast is not showing the same position. Trust Board to see the real position from forecast to outturn. Mr Davies/Mr Banks 43.3 CIP Status Mr Turner requested that this paper needs to be simplified for the Trust Board. Mr Davies explained the summary of adjusted profiled run rate against the forecast outturn. Outstanding issues/mitigations need to be addressed. Mr Turner expressed his concern that this needs to be shop floor led in future years i.e. a whole service approach for accountability. Mr Davies explained Enc. 3 position after the CIP, Improvement and Growth Programme Board meeting on 22 nd August. Mr Turner requested that this report goes through MEXT for approval. Mr Parker explained the step down beds value of 178k but an expected? was shown on the spread sheet. There are now additional funds to support this initiative via CCG. Dr Weaver explained details behind the Walsall new urgent care pathway. Mr Turner queried the establishment review of 125k compared to expected 10k. Much better position than previously outlined of 1m budget Mr Turner queried the figures which do not include 3% increment in that year. Mr Davies explained that the CIP target would be approximately 4.2m. Cost pressures are not known. This could change dramatically once the new Trust is established. The CIP Status report will be presented to the next MExT committee. Mr Davies 43.4 Mitigation Plans Issues mentioned around Black Country Partnership financial position. The Trust is in a much better financial position. The challenge is to explain the financial situation to Trust Board. Mr Banks and Mr Davies to produce this report comparing like for like and will run this past member of Mr Davies/Mr Banks Enc 10 FP Minutes (Final) Page 5 of 6
94 this committee prior to submitting to Trust Board. Mr Turner thanked the presenters and requested that Mrs Musson and Mrs Cooper be asked to present, but check with Mr Axcell if this is appropriate. Mr Parker advised that Mrs Cooper would welcome the opportunity to present her strategies. Mr Davies 44 Any Other Business No other items were discussed. 45 Date, Time and Venue of Next Meeting Monday 25 th September :00 to 17:00 hours Board Room, Canalside House, Walsall END TIME 12:00 HOURS Enc 10 FP Minutes (Final) Page 6 of 6
95 Board meeting date: 5 October 2017 Report Title: Agenda Item number: 7.1.3c Enclosure: 11 Audit Committee Chair s Report Committee: Audit Committee Author (name & title): John Lancaster, Non-Executive Director Annalee Russell, Finance Manager Audit & Assurance Action required from the Board Decision / Approval Gain assurance Discussion Information This report provides details of the work undertaken by Audit Committee during its meeting held on 19 th September Key issues and Risks NEDs Review of Work Undertaken by Other Sub-Committees The Chair of the Finance and Performance Committee provided a detailed update of the work being undertaken by the Committee. The Chair explained that he had only recently undertaken the role in an attempt to provide continuity through and beyond the TCT transaction date. He explained that the Committee were focused on reviewing the Trust s year to date financial position, CIPs, 2017/18 forecast outturn and contract over performance. Significant discussions were held around the CIP processes in place at the Trust particularly the need for CIP s to be transformational and the process to be driven from within the Service Lines rather than top down. In addition, the Chair of Finance & Performance Committee stressed how work needs to begin immediately on identifying CIP schemes for 2018/19 if they are to deliver a full year effect from 1 st April The Committee also discussed the risks that the delay in the integration date under the TCT partnership posed. The update was well received by the Committee. Internal Audit Internal Audit presented the following documents to the Committee Progress Report Outstanding Recommendations Report - No overdue recommendations - One deferred recommendation was reported relating to recruitment KPIs. Internal Audit confirmed that they had recently undertaken addition review work in this area and that the recommendation could likely be closed down as a result. - Updates will be chased for all outstanding recommendations (whether due or not) in the final weeks of the Trust to present a clean handover to the new organisation. Enc 11 Audit Committee Chair's Report - September 2017 Page 1 of 3
96 The following Internal Audit Reports were presented to the Committee Partnership Mental Health Alliance, Resilience, Innovation and Training (MERIT) Vanguard Significant Assurance Care Records Least Restrictive Practice Significant Assurance Care Records General Review Significant Assurance, although there were some inconsistencies in practice across the three hospital sites and therefore the Quality and Safety Committee would be asked to review this Audit. The Chair expressed that he was pleased with the progress made in this area over the last 12 months but was disappointed that the progress was not consistent across all sites and areas audited and noted how in some areas deterioration had been recorded Care Records Mental Capacity Act and Deprivation of Liberties Moderate Assurance Workforce Race Equality Standard (WRES) Moderate Assurance TRAC Recruitment System-Benefit Realisation Significant Assurance In addition, Internal Audit also presented the following documents to the Committee Performance Outcome Measures and Key Performance Indicators 2016/17 the Trust received a Good rating CW Audit Annual Satisfaction Survey Results of the Well Led Review (Advisory Work) Internal Audit reported that the Trust were performing well across the selected domains but that a number of recommendations had been made to strengthen existing governance arrangements. External Audit External Audit presented the following documents to the Committee External Audit Update Report External Audit advised that the report contained progress to date against the plan that had been prepared on the assumption that the Trust would be acquired by Birmingham Community Healthcare NHS Foundation Trust on 1 st October The delay was acknowledged and External Audit confirmed that the plan would be revised when [at that time] the revised acquisition date was known. External Audit confirmed that the following documents would not be required part year for the Trust if it were acquired. Quality Account and Value for Money Conclusion and as a result these would not need to form part of the audit plan (dependent on acquisition date). The report also contained a number of embedded reports relevant to the Trust. Annual Audit Letter 2016/17 This report provided a summary of the audit work undertaken and resulting findings for the financial year ended 31 st March Anti-Fraud Anti-Fraud presented the following documents to the Committee Anti-Fraud Progress Report - No new referrals have been made since the last Audit Committee meeting National Fraud Initiative Report - 29 matches identified, investigated and closed no further work required Update re: NHS Protect - NHS Protect are being replaced by NHS Counter Fraud Authority - Little expected impact on the Trust In addition, the following documents were presented to the Committee for information Enc 11 Audit Committee Chair's Report - September 2017 Page 2 of 3
97 Update from NHS Protect Investigation Guidance for Anti-Fraud Specialists Guidance from Crown Prosecution Service Trust Business The following issues were discussed under Trust Business Management Papers The regular updates on the number and value of waivers, purchase invoices with no orders and losses and special compensations were provided for the 2017/18 financial year to date. Use of waivers within the Trust was discussed in some detail. The Chair requested that the Waivers listing be taken to Executive Directors and sign off to be undertaken by the responsible Executive Director rather than the Director of Finance. Review of Board Assurance Framework (BAF) The report was reviewed and noted. IR35 Compliance Update The report was reviewed and noted. Cyber Attack Report The report was reviewed and noted. Deaf CAMHS Update Report The report was reviewed and noted. Members of the Audit Committee commented that the Trust may find it more cost effective to employ BSL interpreters. The Chair of the Committee requested that the Director of Operations be asked to formulate an action plan to reduce spend on cancellation charges for interpreters. Any Other Business No items of other business were raised. Interfaces with other Committees Quality and Safety Committee are asked to review the inconsistencies between performance at sites across the Trust in attempt to ascertain if there are any management issues that need to be addressed in relation to them. Workforce Committee to receive the Workforce Race Equality Standard (WRES) and TRAC Recruitment System-Benefits Realisation Internal Audit Reports for review and follow-up as appropriate. Executive Directors to receive Waiver list for review. Recommendations and requests for direction The Board is asked to receive and note this report from Audit Committee. Enc 11 Audit Committee Chair's Report - September 2017 Page 3 of 3
98 Board meeting date: 5 October 2017 Agenda Item number: 7.1.3d Enclosure: 12 Audit Committee Minutes of meeting held on Tuesday 19 September 2017 Conference Room 1, Trafalgar House Start time: 11:00 hours Present: Mr John Lancaster Mr John Burbeck In Attendance: Mr Rupert Davies Ms Annalee Russell Ms Joan Barnett Ms Sarah Swan Mr Harry Turner Mr Lewis-Grundy Mrs Linda Wix Apologies: Mr Mark Stocks Mr Paul Westwood Mr Paul Dudfield Non-Executive Director (Chair) Associate Non-Executive Director Interim Director of Finance, Performance & IM&T Finance Manager Manager Grant Thornton Assistant Director, CW Audit Services Non-Executive Director & Chair of the Finance & Performance Committee (Minute only) Company Secretary Corporate Governance Support Officer (Minutes) Engagement Lead, Grant Thornton Head of Anti-Fraud Services Consortium Director, CW Audit Services Minute Item Action 20. Welcome The Chair welcomed everyone to the meeting. 21. Apologies Apologies were noted as above. 22. Minutes 22.1 The Minutes from the meeting held on 22 May 2017 and 21 June 2017 were noted as a true and accurate record. Minute 4.3 Matters Arising The Chair sought assurance that the TCT Operational Risk Register was following due process. Mr Lewis-Grundy advised that the document would be updated by Clinical Governance colleagues in light of discussions had during the Board Development Session on 18 th September and would be reviewed by the Board in October The Chair queried whether final audit arrangements were Audit Committee Minutes (Final) Page 1 of 15
99 in place and Ms Russell confirmed that initial plans were in discussion, although these would have to be re-scheduled due to the pause in the TCT process. Mr Davies confirmed that it would be prudent to hold a final Audit Committee prior to the transaction date once this date was confirmed and the Chair requested that this be captured on the Action Schedule. ACTION: Arrange a final Audit Committee prior to the TCT transaction date once this date had been announced. PLG 23. Matters Arising 23.1 The following items were discussed: Minute 3.2 Action Schedule Mr Davies advised that this action had been partly completed and the policy had been taken through due process. The introduction of an electronic systems to support job planning and appraisals was unlikely to be realised due to the TCT Integration. The Chair confirmed that although the action was incomplete he was content for it to be closed as it would be resolved post integration. Completed. Closed. Minute /16 ISA260 Governance Report Whilst this action had been concluded, the Chair sought confirmation that the matter was resolved and Mr Davies confirmed that the Trust had been credited with 400,000. There may be a recurrence of the issue in 2017/18 although the invoices were available and this had not been the case previously which had led to the dispute. All other items were either complete or had a future completion date. 24. Review of work undertaken by the Finance & Performance Committee Mr Turner advised that he had only recently been appointed as Chair of the Finance & Performance Committee for continuity purposes as post TCT transaction he would remain on the Board of the new organisation for an interim period. He stated that the transitional arrangements were unclear, although the Finance & Performance Committee would become a management committee reporting to an overarching Finance and Perfornance Committee of the Board of the enlarged Trust. The membership of the management committee and the Terms of Reference had yet to be confirmed. In the Audit Committee Minutes (Final) Page 2 of 15
100 intervening pre-transaction period the Committee was focussed on gaining clarity around the Trust s financial position and had reviewed CIPs, end of year position, finance and contract over-performance. There were a number of emerging risks as a result of the pause in the TCT process that would have financial implications and these had been raised at TCT Integration Board. The Chair queried whether the CIP target would be achieved by year end and Mr Davies confirmed this to be the case with the use of non-recurrent funding. Mr Turner advised that three CIPs were red RAG rated, Step down beds, CRS pathway in Walsall and the establishment review and concurred with Mr Davies that there were nonrecurrent mitigations to close the CIP gap. He confirmed that the Finance & Performance Committee would review the CIPs at the meeting to be held in September. Whilst it was not within the remit of the Audit Committee to review the financial position in detail, the Chair commented that it was clear that there would be CIP challenges in the next financial year. Mr Turner concurred, adding that next year CIPs should be transformational and a bottom up exercise and that given the uncertainties around the TCT Integration, work should begin on identifying 2018/19 CIPs with plans in place ready for 1 April 2018 in line with procedures that had been implemented earlier in the current financial year. The Chair advised that he would highlight the CIP challenges in his report to the Board and Mr Turner confirmed that he would do the same. ACTION: Audit Committee and Finance & Performance Committee Chair s reports to highlight the 2018/19 CIP challenges to ensure that work commenced on CIPs so that plans were in place for 1 April Mr Burbeck reiterated the Chair s concerns that the delay with the TCT integration would impact on the Trust s finances and the Chair commented that decisions and actions should be made on the basis that the Trust was an ongoing concern. The Committee noted the content of the verbal report. Mr Turner left the meeting. 25. INTERNAL AUDIT 25.1 Internal Audit Progress Report Ms Swan drew attention to the audits undertaken and that the reports were agenda items. She advised the Committee that the work had commenced on Unexpected Deaths and premises assurance with regard to fire prevention. An audit of the Trust s financial systems had Audit Committee Minutes (Final) Page 3 of 15
101 commenced in September and was due to conclude in October. The Chair commented that the IG toolkit audit would be undertaken by the new TCT organisation and Mr Davies agreed, adding that a fire safety audit had replaced the IG toolkit audit and findings of the latter would be presented to the next Audit Committee in December and as it may highlight some gaps in fire safety procedures it would in the interim be reviewed by the Quality & Safety Committee. The Chair queried whether the Board Assurance Framework included fire safety risks and Mr Lewis-Grundy confirmed that the BAF reflected the strategic risks for the Trust as sovereign body and the TCT Full Business Case had reviewed the BAFs of the three TCT organisations to identify the strategic risks for the new organisation. Ms Swan advised that the report included a considerable number of publications given the length of time since the last Audit Committee, some of which may impact on the Trust, and Mr Lewis-Grundy confirmed that there was some overlap with those publications already included in the CEO s monthly report to the Board providing assurance that the Executive Team were up to date with the latest publications. The Committee noted the report Outstanding Recommendations Report Ms Swan advised that there were no outstanding or overdue recommendations and there was one recommendation that was not yet due related to introduction of KPIs for the recruitment process and as this had been completed this recommendation could now be closed. The Committee noted the report Partnership Mental Health Alliance, Resilience, Innovation & Training (MERIT) Vanguard Report Ms Swan took the Committee through the report advising that the overall opinion was that significant assurance could be given and that there was a generally sound system of internal control, designed to meet the organisation s objectives, and that controls were generally being applied consistently. The Chair advised that the success of MERIT was difficult to measure and Ms Swan concurred adding that evidence of delivery would be robust work plans with partners realising benefits of partnership working. The audit had concluded in February and had reviewed the status of the Audit Committee Minutes (Final) Page 4 of 15
102 project in Quarter /17 and MERIT would have moved on since that time. Mr Davies advised that funding for MERIT was at risk as it was dependent on the every member Trust agreement to their individual control totals. The Committee noted the report Performance Outcome Measures and Key Performance Indicators 2016/17 Ms Swan advised that the report demonstrated how CW Audit complied with standards and any particular outcome measures. She highlighted the positive responses of the main contact within the organisation to the post-audit questionnaire resulting in a score of 9 which gave an overall rating of good. The Committee noted the content of the report Care Records Least Restrictive Practice In presenting the report, Ms Swan advised that the Trust had a formally documented Search Policy and Locked Door Policy in place and the review noted that compliance with policy requirements had strengthened since previous reviews. It should also be noted that there were improvements made to care record documentation held in support of access and exit arrangements for informal patients and the management of blanket restrictions. Nonetheless, some further improvements could be made in recording patients consent for conducting the searches. The overall opinion was that significant assurance could be given. The Chair queried whether the overall management was consistent across the Trust and Ms Swan confirmed this to be the case although there was some evidence that managers applied individual processes. The Committee noted the content of the report Care Records General Review Ms Swan took the Committee through the report advising that improvements had been noted in the completion and maintenance of general care records, and in particular the quality of the care plan documentation had improved and no exceptions were noted in relation to the sample and criteria tested. The overall opinion was therefore that significant assurance could be given. She commended staff for the outcome, although there were still some areas Audit Committee Minutes (Final) Page 5 of 15
103 for the Trust to work on in order to reach full compliance against the Trust s Care Record Criteria. The Chair commented that completion of care records would remain a risk to the Trust until the introduction of an electronic patient record (EPR) and although Ms Swan concurred she added that the EPRs were not without their own issues. Mr Burbeck queried the disparity between Bloxwich, Dorothy Pattison and Bushey Fields Hospitals in compliance related to identifiable data displayed on the front cover of care records, Ms Swan advised that staff at Bushey Fields Hospital had been provided with incorrect guidance. Mr Burbeck stated that there had also been a deterioration in the insertion of the authors name and designation in the care records on Holyrood Ward. Ms Swan advised that the Care Records Audit report had been shared with Ward Managers at Bushey Fields Hospital in order to correct the inconsistencies. Ms Russell advised that these inconsistencies should be reported to the Board via the Committee Chair s report. ACTION: Audit Committee Chair s report to Board to make reference to the disparity in compliance between sites related to identifiable data displayed on the front cover of care records and the reason for this. The Chair advised that the inconsistencies across the trust were disappointing and Mr Davies suggested, and it was agreed, that the care records audit report would be reviewed by the Quality & Safety Committee as the inconsistencies may be linked to management issues. ACTION: Care records audit report to be reviewed by the Quality & Safety Committee as the inconsistencies may be linked to management issues. The Committee noted the content of the report Care Records Mental Capacity Act (MCA) and Deprivation of Liberty (DoLs) In presenting the report Ms Swan advised that the overall opinion was that significant assurance could be given and asked members to note that there had been considerable improvements in all areas since the previous review undertaken a year ago when the opinion given at that time was moderate. The review had noted a small number of instances where forms were not on medical records at the time of review and there were some gaps within completed documentation. The Committee noted the content of the report. Audit Committee Minutes (Final) Page 6 of 15
104 25.8 CW Audit Annual Satisfaction Survey Ms Swan advised that the survey had been distributed to the CW Audit client base and overall satisfaction was rated 7 or above by 97% of respondents and this was an improvement of 2% on last year s results. The contribution of our Heads of Internal Audit/Chief Internal Auditors and Audit Managers was scored 7 or above by 97% and 94% of respondents respectively. Areas for improvement had been identified and the response and any related actions for CW Audit were included in the report. The Committee noted the content of the report Workforce Race Equality Standard (WRES) Ms Swan advised that the Trust was required to complete a mandatory NHS data return on the Workforce Race Equality Standard. The outcome from the 2015/16 return had raised some action areas for the Trust to help ensure that the risk of any bias was reduced. The auditors had been unable to fully validate the data in the return due to the availability of information although some limited testing on more recent data had been completed. A number of potential areas for further consideration within the WRES Action Plan had been identified along with improvements to the Trust policy on Recruitment and Selection. The Trust should also ensure that all relevant documentation following appointment is passed on to the recruitment team. She confirmed that the overall opinion was moderate assurance. The Chair queried whether employment of people from the BME community was disproportionate. Mr Lewis-Grundy advised that the Board had received the Annual WRES report in August which reflected positively on the Trust s employment of people from the BME community as a proportion of the overall population that the Trust serves The Committee noted the content of the report TRAC Recruitment System Benefit Realisation In presenting the report Ms Swan advised that the overall opinion was significant assurance. The review noted the introduction of the TRAC Recruitment system in February 2017 and recommendations from the previous audit had resulted in the strengthening of a number of controls within the Trust s recruitment process. Eight out of ten staff who responded to the survey expressed that they thought the TRAC system had led to improvements. The calculation of Audit Committee Minutes (Final) Page 7 of 15
105 time at each key stage of the recruitment process in comparison to the results in July 2016 showed improvements in performance at all stages with a net average decrease in time to recruit of 41 days. In order for further benefits to be realised, focus should now be placed on finalising and reporting recruitment KPI s to support the ongoing performance management process. Mr Lewis-Grundy advised that the report would be presented to the Workforce Committee. The Committee noted the content of the report Well Led Summary Ms Swan advised that the Trust was performing well in the selected domain areas Strategy & Planning and Capability & Culture. Board members were able to comprehensively describe the strategic risks that were facing the Trust. There was a clear strategic risk register in place, supported by a service level risk register and there was also a robust Board Assurance Framework in place, which was assessed on a quarterly basis and reflected risks to the initiatives included in the Trust s strategic plan. The Board regularly assessed and considered current and future risks to quality and performance and took steps to address and mitigate these risks. The report included suggestions for strengthening governance arrangements, which could potentially help to improve overall arrangements and there were no significant weaknesses to report. Mr Burbeck made reference to the lack of timescales within the action schedule and Mr Lewis-Grundy advised that as the audit was an advisory piece of work the suggested developments were not added to the recommendations tracker. Mr Burbeck stated that as the Trust was inspected by the CQC under the well led domain there should be agreed completion dates for the recommended actions, and Mr Lewis-Grundy agreed to populate the completion dates for the recommended actions to improve the process. ACTION: Populate the completion dates for the recommended actions to improve the process. The Committee noted the content of the report Hand-over of outstanding reports to TCT Trust Audit Committee Minutes (Final) Page 8 of 15
106 Given the pause in the TCT integration process, Mr Davies confirmed that arrangements had been made with CW audit to continue with the internal audit programme and reports submitted to the Audit Committee. Ms Russell confirmed that any resulting outstanding actions from the audits would be reported to the Audit Committee and Mr Lewis-Grundy advised that he had received a request from BCHC to provide an Audit Committee position statement to ensure that anything outstanding was reported to Audit Committee in the enlargeled organisation post transaction. Mr Davies confirmed that the Finance team had received a similar request. The Committee noted the verbal update. 26. EXTERNAL AUDIT UPDATE 26.1 External Audit Update Report Ms Barnet took members through the report, advising that the report included an update on progress and the plan had been prepared on the assumption that the Trust would be acquired on 1 October 2017 by Birmingham Community Healthcare NHS FT. As the formal transaction date had been delayed, the plan would now be issued when the transaction date was confirmed as the audit work was dependent on the date of acquisition. The report also included a summary of emerging national issues and developments that may be relevant to NHS Trusts: NHS Companies: An enterprising approach to health Shaping a vibrant economy: A blueprint for the UK NHSI Quarterly Monitoring Report Mental Health in Prisons The Kings Fund Reports on the Capped Expenditure Process and Quality Improvement in Mental Health Department of Health accounting guidance for NHS bodies 2017/18 NHSE had announced new sites to test new approaches for delivering mental health services Ms Barnett referred to the progress report and specifically the Addendum letter advising that under the new contract awarded under Eastern Shires Purchasing Organisation (ESPO) Consultancy Services framework agreement (664) September 2017 external auditors were required to issue an addendum letter which sets out respective roles and responsibilities Referring to the Accounts Audit Plan, Ms Barnett advised that the plan was based on the assumption that the Trust Audit Committee Minutes (Final) Page 9 of 15
107 would be acquired on 1 October 2017 by Birmingham Community Healthcare NHS FT. Now that the formal transaction date will be later the plan would be issued once the date is confirmed as the audit work was dependent upon the date of acquisition. Ms Barnett confirmed that the Value for Money conclusion would not be required due to the integration and similarly the review of the Quality Account would not be undertaken. Ms Barnett commended the finance team for their contribution and co-operation in the completion of the external auditors work. The Committee noted the report Annual Audit Letter Ms Barnett advised that the Annual Audit Letter summarised the key findings arising from the work that had been carried out at Dudley and Walsall Mental Health Partnership NHS Trust (the Trust) for the year ended 31 March The letter was intended to provide a commentary on the results of the work to the Trust and its external stakeholders, and to highlight issues that that auditors wished to draw to the attention of the public. The detailed findings of the audit were reported to the Audit Committee on 22 May The Committee noted the report. 27. ANTI-FRAUD 27.1 Anti-fraud Progress Report Ms Swan advised that the report summarised the work undertaken to date against the 2017/18 anti-fraud work plan and demonstrated progress against planned activities, providing details of new or on-going fraud investigations and those that had been closed since the previous Audit Committee update. She advised that one case relating to water testing had been brought forward since the last report and this had now been closed. There were no new referrals to report. The Committee noted the report National Fraud Initiative Referring to the report Ms Swan advised that a data matching process had been conducted which compared computer records held by one public sector body against other computer records held by the same or another body to see how far they match. When a match was found it may indicate that there is an inconsistency which requires Audit Committee Minutes (Final) Page 10 of 15
108 further investigation. There had been 29 recommended matches identified and each match had been reviewed and closed as in each case the inconsistency had not required further investigation. The Committee noted the content of the report Update from NHS Protect Ms Swan advised that the circular was provided for information only and gave an update on the creation of NHS Counter Fraud Authority which was a new special health authority which began in shadow form in April 2017 to provide a clear focus for both the prevention and investigation of fraud and would work with key stakeholders to tackle fraud, bribery and corruption within the health service. She confirmed that the impact for the Trust was minimal. The Committee noted the content of the report Investigation guidance for Anti-Fraud Specialists Ms Swan advised that this circular was also for information and provided an update on CPS file submissions and how to use NHS Protect s Forensic Computing Unit and financial investigators. The Committee noted the content of the report Guidance from Crown Prosecution Service Ms Swan advised that the circular presented guidance from the Crown Prosecution Service following a review they had undertaken on the standards of NHS investigation files and was provided for information only. The Committee noted the content of the report. 28. TRUST BUSINESS 28.1 Management Papers Mr Davies referred to the key messages: Waivers There were 53 waivers that had been authorised with a Audit Committee Minutes (Final) Page 11 of 15
109 value of 712k in the first five months of the 2017/18 financial year and Mr Davies gave an explanation on the largest amounts: The largest amount was related to a company who provided a data transfer service under a long term contract which had been extended and would terminate shortly. There were also considerable amounts for interpreting services and these issues were covered in a separate report on the agenda. The MERIT evaluation of 46,000 would be funded by central resources. The facilities energy review could have been put out to tender but as Kier were already on site the decision had been taken to utilise their services. The call off order for ACR related to a disciplinary investigation. The Chair stated that given the significant sums of money involved tighter control was needed and he suggested, and it was agreed, that the waivers subject to Standing Financial Instructions should be reported to Executive Directors and the responsible Executive Director should sign off waiver within their remit before the Director of Finance, Performance and IM&T exercised his delegated authority under the Standing Financial Instructions. ACTION: waivers to be reported to Executive Directors and the sign off of waivers subject to Standing Financial Instructions be undertaken by the responsible Executive Director prior to the Director of Finance, Performance and IM&T exercised his delegated authority under the Standing Financial Instructions. No Orders There had been 45 instances of invoices being received without orders having been raised since the last Audit Committee meeting. These invoices had a total value of 71k. Mr Davies confirmed that the glass repairs were related to damage on Kinver ward caused by a cohort of patients and the damage would have been repaired and an order placed retrospectively as the Trust did not have an ongoing contract with a glazing company. Losses and Special Compensations There had been 14 losses and special compensations reported with a value of 4, Mr Davies advised that the fruitless payments related to interpreting services in deaf CAMHS which was the subject of a later report on the Audit Committee Minutes (Final) Page 12 of 15
110 agenda. The Committee noted the report. 29 Review of Board Assurance Framework (BAF) Mr Lewis-Grundy advised that BAF had been reviewed and revised through discussion at Board Development Session on 30 March 2017 and the risks included in the Board Assurance Framework had been agreed through the Board Development Session as those strategic risks to the delivery of the Trusts overarching priorities. Within the reporting process the Committees of the Board had a significant role in monitoring the strategic risks within their Terms of Reference to ensure that they are being managed effectively and provide assurance through that work to the Board. Mr Lewis-Grundy confirmed that the Board had received the BAF in August and was being presented to the Audit Committee for assurance on the Committee review process in Quarter 1. He confirmed that the BAF would follow the same process in Quarter 2. There were 6 strategic risks, 5 rolled over from last year and the sixth related to TCT integration. The Committee noted the report. 30 IR 35 Compliance Update Mr Davies presented the reporting, advising that the Trust had undertaken a High level audit early in financial year 2017/18 that had identified workers coded to agency lines on Trust s financial ledger and there had been less than 10 potential individuals at risk, each staff member had been reviewed and arrangements agreed. Those workers had been identified as IR35-compliant or outside of IR 35 with one exception and this resulted in termination of their contract. The Chair concluded that the Trust was able to demonstrate to the Inland Revenue that it was taking the relevant action in line with the legislation. The Committee noted the report. 31. Cyber Attack Report In presenting the report, Mr Davies made reference to the national ransomware cyber attack which occurred In May 2017 affecting many parts of the NHS. Whilst devices Audit Committee Minutes (Final) Page 13 of 15
111 within the DWMH network were not directly affected by the ransomware, the Trust took precautionary measures in isolating systems which led to unavailability between Friday 12th May and Monday 15th May. Key patients systems, such as Oasis, were unavailable for short periods during the weekend while patching was undertaken. It was subsequently agreed to undertake a Cyber Security audit to ensure appropriate controls were in place and are effective and TeraFirma confirmed that they were complaint with the necessary information security standards, although they had stated that they would charge the Trust on a time cost basis if they were to be audited. The Chair advised that as they were ISO registered they would have had to provide evidence as to the security measures they had in place. He advised that Birmingham Community Healthcare was significantly impacted by the cyber attack resulting in the unavailability of information held within key IT systems and significant quantities of appointments were cancelled which would have had significant cost implications for the Trust. It was expected that an enlarged in-house BCHC IT function will service the new Trust. The Committee noted the report. 32. Deaf CAMHS Update Report Mr Davies advised that Losses in respect of interpreters used by Deaf CAMHS have been reported to Audit Committee regularly over the last 12 months or so and It should also be noted that cancellation charges appear to be levied at 100% of actual cost of the service even when cancelled within 7 days and these cancellation charges totalled 10, since April Mr Davies advised that there was no evidence that there had been a breakdown in process, although there may be some poor practice and the Chair advised that as the amounts were significant the Director of Operations should be asked to produce an action plan to reduce the spend on cancellation charges for interpreters. Action: Interim Director of Operations should be asked to produce an action plan to reduce the spend on cancellation charges for interpreters. Mr Burbeck commented that it might be more cost effective for the Trust to employ interpreters rather than pay agency fees. 33. Any Other Business Audit Committee Minutes (Final) Page 14 of 15
112 There were no items of any other business. 34. Date of next meeting: Tuesday, 12 December 2017 at 11.00am, Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS Meeting closed at Audit Committee Minutes (Final) Page 15 of 15
113 Board Meeting date: 5 October 2017 Agenda Item number: 7.1.3e Enclosure: 13 Finance Report, Month /18
114 Finance Report Month /18 Page Key Messages: Current Performance 1 Single Oversight Framework (NHS Improvement) 2 Overall Summary and RAG Assessment 3-4 Trust Summary Income & Expenditure Statement: Functional Analysis 5-8 Cost Improvement Programme 9 Agency Cap / Agency Spend by Staff Group / Reported Shift Breaches (weekly) Capital Programme 13 Payables Performance & Aged Debt 14 Cash Flow Statement 15 Statement of Financial Position (Balance Sheet) 16
115 Key Messages : Current Performance Financial Position Expenditure Pay 933k surplus at M05 27k Favourable variance 50k Favourable variance The Trust has delivered a month 5 surplus of 993k. This represents a favourable variance of 27k against the planned Year To Date (YTD) surplus of 907k. This planned YTD figure forms part of the plan to deliver a month 06 surplus of 1.068m and a full year surplus of 1.839m. Pay expenditure is 50k in surplus against budget to date, which has been driven by vacancies across the Trust. Bank & Agency spend equates to 642k in month (split 389k for Agency and 253k for Bank) which is up on the previous months spend of 502k (split 297k for Agency and 205k for Bank). Despite this increase in costs within the month, agency spend is still currently ahead of plan by 148k in relation to the overall 4.05m Agency target for the year (actual spend of 1,558k against 1,706k plan). Expenditure Non Pay Income & Activity 2017/18 outturn 37k Adverse variance 13k Favourable variance (incl 69k noncontracted activity underperformance) Non-Pay expenditure is 37k in deficit against budget to date: 531k of this is driven by over-spending by budget holders against their non-pay lines and non delivered devolved CIP. Offset in part by a surplus on budget reserves less non-delivered CIP held centrally of 398k. The Trustwide Contracted Activity position at month end is reflecting an under-performance of 69k and is explained as: Both Dudley CCG and Walsall CCG are now on block and as such are reflecting a breakeven position. Other smaller CCG contracts in total (such as Worcester) have under-performed by 2k Non-Contract Activity (NCA)s have under-performed against plan by 24k The activity in the Detox beds at Bushey Fields has under performed by 43k Non-contracted Income such as SLA s and Education Income are ahead of expected plan and are mitigating against the current under-performance in contracted income mentioned above, giving an overall favourable income position for the year to date of 13k (which includes Interest Receivable shortfall of 5k). CIP plans delivered for 2017/18 Expenditure - Capital 2,906k delivered against target 376k spend YTD In order to meet in year cost pressures the Trust has identified CIP schemes equating to 3,776k. At month 05 schemes have delivered 2,906k. The four schemes held centrally are being phased into the finance position each month to the tune of 19.0k ( 95.3k YTD / 228.7k FYE) and could be deemed to being met non-recurrently through the overall favourable (surplus) finance position to date. Executive focus is particularly on those schemes rated as red The Capital Programme has been agreed at 3.8m for the year. Of this 2.4m relates to the replacement EPR system which includes 1.0m carried over from last years Capital plan. At month 5 376k has been spent to date. 1


116 Single Oversight Framework Trust Performance subcode Q1 M04 M05 Forecast Outturn Plan Actual Plan Actual Plan Actual Plan Actual Liquidity Rating PRR Capital Service Cover Rating PRR I&E Margin Rating PRR Distance from Financial Plan PRR Agency Rating PRR Overall Use of Resources PRR Commentary The Single Oversight Framework is designed to help NHS providers attain, and maintain, Care Quality Commission ratings of Good or Outstanding. The Framework doesn't give a performance assessment in its own right. The Framework will help NHSI identify NHS providers' potential support needs across five themes: - quality of care - finance and use of resources - operational performance - strategic change - leadership and improvement capability NHSI will segment individual trusts according to the level of support each trust needs. NHSI can then signpost, offer or mandate tailored support as appropriate. Scoring a 4 on any finance metric will mean the overall rating is at least a 3, triggering a concern. Current month position and position for the Trust to date is giving a maximum rating of 1. 2
117 Overall Summary and RAG Assessment Statement of Comprehensive Income - Financial Position to 31st August 2017 Annual In Month Year To Date Plan Plan Actual Variance Plan Actual Variance Income Revenue From Activities Revenue-NHS Clinical 60,829 5,088 5, ,366 25,339 (27) Revenue-Non NHS Clinical (47) Total Revenue From Activities 61,569 5,149 5, ,675 25,601 (74) Other Operating Revenue Revenue-Employee Benefits Revenue-Education & Training 1, Revenue NHS Non-Clinical 1, Other Revenue (4) (48) (15) Total Other Operating Revenue 3, (22) 1,776 1, Total Revenue 65,356 5,499 5,485 (13) 27,450 27, Expenditure Pay (51,230) (4,289) (4,376) (87) (21,219) (21,146) 73 Non Pay (9,842) (866) (989) (123) (4,303) (4,834) (531) Trustwide Reserves Total Operating Expenditure (60,962) (5,112) (5,149) (37) (25,480) (25,539) (59) Commentary Revenue Position The plan for the year currently reflects a planned surplus position of 1.839m, as per the agreed Control total with NHSI. As at month 05 the Trust has delivered a surplus of 933k, which is 27k ahead of plan. Total Income is reflecting an over-recovery of 13k year to date which includes a current level of under-performing contracted income with CCG s of 69k. It should also be noted that it is assumed that the Trust will receive 166k in relation to the Merit Vanguard. At present this is being withheld by NHSI & NHSE as a result of other organisations not agreeing their control totals. CIP 2017/18 Delivery The Trust has a declared an internal plan of 3,776k for 2017/18 and has schemes in place totalling 3,765k. At month 5 there is a balance of 228k non-delivered CIP held centrally. It is important that this balance is addressed on a recurring basis as soon as possible. EBITDA 4, (51) 1,972 1,930 (41) Depreciation (1,475) (123) (104) 19 (615) (519) 95 Amortisation (256) (21) (30) (9) (106) (149) (43) Net Operating Surplus 2, (42) 1,251 1, PDC (865) (72) (51) 21 (360) (339) 21 Interest Receivable (1) (5) P/L Disposal Net Surplus /(Deficit) 1, (21) Budgetary Reserves Gross budget reserves at month 5 is 1.3 million, supported by non recurrent credit budgets of over 1 million. There are recurring commitments against the budgets of around 400k for Older Adults Primary Care and Complex Care teams Technical Adj - Impairment Technical Surplus 1, (21)
118 Overall Summary and RAG Assessment Continued Run Rate 2017/18 Capital Programme 2017/18 2,000 1,750 1,500 1,839 Cumulative Planned Run Rate (Surplus) 4,000 3,500 3,000 3,800 Planned Spend '000 1,250 1, Actual Run Rate '000 2,500 2,000 1,500 1, Revised Planned Spend Cumulat ive Actual Spend CIP 2017/18 Forecast vs Actual Cash Balance 2017/18 CIP Target as per NHS Improvement 2,500 17,000 16,500 Identified Schemes (PYE) 3,765 '000 16,000 15,500 Identified Schemes (FYE) 4,778 15,000 14, ,000 2,000 3,000 4,000 5,000 6,000 '000 14,000 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Revised Plan 14,047 15,304 15,575 16,073 16,416 16,169 16,386 16,626 16,840 16,691 16,355 15,402 Original Plan 14,697 14,682 14,702 14,985 14,966 14,531 14,862 14,887 14,885 15,210 15,230 14,791 Actual 16,161 16,501 15,674 16,220 16,643 4
119 Trust Summary Income & Expenditure Statement Including Functional Analysis Annual Plan In Month Year to Date FOT M /18 Plan Actual Var Plan Actual Var Var '000 '000 '000 '000 '000 '000 '000 '000 NHS Revenue-Activities 61,329 5,129 5, ,575 25,547 (27) (100) Revenue from LAs (10) (42) (97) Total Revenue from Activities 62,009 5,186 5,181 (5) 25,858 25,789 (69) (197) Corporate Functions Corporate Departments (13,585) (1,143) (1,223) (81) (5,725) (5,963) (238) (430) Central Reserves Total Corporate Functions (13,475) (1,098) (1,005) 93 (5,682) (5,522) Operational Services Urgent Care & Access (5,447) (460) (464) (4) (2,297) (2,267) 30 (40) Hospital Support (604) (50) (52) (1) (252) (258) (7) (10) Inpatient Services (Acute & OA) (11,750) (1,008) (1,112) (104) (4,926) (5,125) (199) (450) Community Services (8,089) (675) (682) (7) (3,294) (3,372) (78) 0 Early Intervention (6,215) (521) (545) (24) (2,601) (2,503) 98 0 Medical Services (12,037) (986) (985) 1 (4,835) (4,812) Total Operational Services (55,288) (3,700) (3,839) (139) (18,206) (18,337) (132) (350) Total Expenditure (68,763) (4,798) (4,844) (46) (23,887) (23,860) Sub Total (6,753) (51) 1,972 1,931 (41) (77) Interest Receivable (1) (5) (12) PDC Dividend (865) (72) (51) 21 (360) (339) Depreciation (1,729) (144) (134) 10 (720) (669) Net Surplus/(Deficit) (9,307) (21) Commentary The Trust is showing a 69k under-performance position against contracted activity levels. This is due to under-recovery on Non-Contract Activity to date coupled with a shortfall against Detox bed activity. Corporate areas have overspent in month due to additional costs incurred in relation to the Transforming Care Together (TCT) Partnership staffing support, Legal Fees, Bid writing and Membership costs. Central Reserves have improved in the month in order to mitigate the deterioration in the overall financial position. There still remains a balance of 228k CIP still to be devolved/delivered. The Inpatients service line overspend for August includes: Acute inpatient overspend of 62k (including 45k Ambleside), Older Adults inpatients overspent of 64k ( 61k for Holyrood), due to patient acuity and associated observation levels. This has been offset slightly by HT and psychology vacancies. Community areas remain in surplus due to slippages within CRS vacancy slippage and the decommissioning of Walsall Carer s Team. Early Intervention area has deteriorated in month due to expected drawdown on early vacancy slippage from continued agency usage on WLI some of which will be used to support commissioner commitments already made. Medical services have generated a small underspend year to date, mainly against non pay budgets (e.g. training not spent in equal twelfths). The Trust is currently reflecting a surplus position of 27k ahead of the trajectory to deliver the 1.839m planned surplus at year end. 5
120 Trust Income Statement Income Annual Plan In Month Year to Date FOT M /18 Plan Actual Var Plan Actual Var Var '000 '000 '000 '000 '000 '000 '000 '000 Revenue From NHS Activities Dudley CCG 28,208 2,351 2, ,753 11, Walsall CCG 27,257 2,290 2, ,378 11, Sandwell & West Birmingham CCG 1, Wolverhampton CCG Birmingham Cross City CCG Birmingham South Central CCG South East Staffs & Seisdon CCG Stafford & Surrounds & E Staffs CCGs Cannock Chase CCG East Staffs CCG (0) Redditch & Bromsgrove CCG Wyre Forrest CCG (1) NHS South Worcester CCG NCA - Adult Neuro Income Generation CIP NCAs (13) (77) (100) CAMHs Deaf 1, (0) (1) 0 Total NHS Revenue-Activities 60,829 5,088 5, ,366 25,339 (27) (100) Revenue - Local Authorities Walsall MBC (0) 0 0 (0) 0 Dudley MBC Sandwell MBC Wolverhampton MBC Stafford MBC Detox Beds (10) (43) (97) Dudley CRI NCA - Other HC Total Revenue from LAs (10) (42) (97) STF Funding Income - DoH Total Revenue from Activies 62,009 5,186 5,181 (5) 25,858 25,789 (69) (197) Commentary The Trust is now operating on a block contract with Dudley CCG and Walsall CCG across all service lines. NCA s reflect an under-performance of 24k to date, which indicates a slow start to the expected additional 200k CIP target (based on actual performance delivered last financial year). In patient detox service at Bushey Fields is currently 43k adrift against the annual target. Overall the Trust is under-performing by 69k against its target to date. If the Trust were to report actual activity undertaken under a shadow reporting arrangement then the Trust would actually be over-performing by 418.7k (was reported as 611.1k in month 4) This level of over-performance would primarily be reflected as: Walsall CCG 459.8k over Dudley CCG 100.3k under (significant deterioration from an over-performing position of 129.6k last month) Sandwell & West Birmingham CCG 131.9k over Wolverhampton CCG 48.1k over Birmingham Cross City CCG 14.9k over Remaining CCGs 68.7k under = Total CCG over-performance of 485.7k Offset by under-performance on NCAs and Detox beds mentioned above ( 67.0k) Overall, we have seen a deterioration in the position by around 192k in the month, primarily within Dudley Community Services, Inpatients and CAMHs. 6
121 Trust Income & Expenditure Statement - Corporate Functions Annual Plan In Month Year to Date FOT M /18 Plan Actual Var Plan Actual Var Var '000 '000 '000 '000 '000 '000 '000 '000 Corporate Functions Chief Executive (986) (82) (100) (18) (413) (534) (121) (235) Corporate Affairs (497) (44) (69) (25) (202) (224) (22) (15) Corporate Human Resources & Dev. & People (1,139) (95) (86) 9 (475) (460) 14 0 Corporate Medical (1,135) (95) (91) 3 (473) (482) (10) 10 Estates - Acute (1,592) (133) (125) 8 (663) (634) Estates - Corporate (1,268) (110) (121) (11) (549) (553) (4) (80) Corporate Operations (3,400) (281) (310) (29) (1,424) (1,504) (80) (20) Corporate Finance (1,159) (99) (114) (15) (500) (527) (27) (70) Corporate Performance & IT (2,410) (205) (207) (1) (1,027) (1,045) (18) (30) Total Corporate Functions (13,585) (1,143) (1,223) (81) (5,725) (5,963) (238) (430) Commentary CEO We now have 3 staff members who have been aligned with the TCT workstream which is a significant cost pressure. We have also started seeing costs for the IAPT review and further investigative costs hit the position in month. Awaiting confirmation of MERIT funding to ease the position. L&D continues to support the position with vacancy slippage. Corporate Affairs Additional bid writing costs for Employment Support have swung the position in month. Corporate HR Agency for the DBS project continues but is being mitigated by non-rec income from the LDA along with a benefit from the movement of staff to TCT work. Additional costs have hit from a grievance investigation (16k). No progress has been made on the Apprentice CIP so far. Corporate Medical Agency usage in Pharmacy has ceased in month and they are now fully recruited. Corporate Estates Additional costs for the Energy Review and the Security Management 85 day plan along with agency costs have been offset by low Water Management costs. Acute Estates Utility costs continue to be low but are expecting them to increase in the second half of the year. Corporate Operations E-rostering project costs & s.75 income deficiency has been partly offset by gains in Psychology/QI/Infection Control. Corporate Finance Membership Cost pressures and additional costs for part year audit. Corporate IT/Performance Additional storage on Records Management along with high telephone charges are the drivers for the overspend. 7
122 Trust Income & Expenditure Statement - Operational Services Annual Plan In Month Year to Date FOT M05 Commentary Operational Services 2017/18 Plan Actual Var Plan Actual Var Var '000 '000 '000 '000 '000 '000 '000 '000 The Inpatients service line overspend for August includes: Acute inpatient overspend of 62k (including 45k Ambleside), Older Adults inpatients overspent of 64k ( 61k for Holyrood), due to patient acuity and associated observation levels. This has been offset slightly by HT and psychology vacancies. Urgent Care & Access (5,447) (460) (464) (4) (2,297) (2,267) 30 (40) Hospital Support (604) (50) (52) (1) (252) (258) (7) (10) Inpatient Services (Acute & OA) (11,750) (1,008) (1,112) (104) (4,926) (5,125) (199) (450) Community Services Community Estates (556) (46) (64) (17) (232) (308) (76) (150) Community Management (CIP) (16) (30) Community & Recovery Services (7,580) (632) (622) 10 (3,085) (3,072) Total Community Services (8,089) (675) (682) (7) (3,294) (3,372) (78) 0 Early Intervention (6,215) (521) (545) (24) (2,601) (2,503) 98 0 Medical Services (12,037) (986) (985) 1 (4,835) (4,812) Total Operational Services (44,142) (3,700) (3,839) (139) (18,206) (18,337) (132) (350) Medical services have generated a small underspend in year to date, mainly against non pay budgets (e.g. training not spent in equal twelfths). Community Estates We are anticipating a larger bill for against our NHS Property Service buildings in 2017/18 after settling on the historical charges with them. We anticipate the additional cost to be in the region of 200k. This is being reflected within the position. Community Services & Recovery Psychological Therapies Hub & Community Recovery Service Vacancy slippage along with gaps within Older Adults have been supplemented by agency causing an overspend. Walsall Carer's Team has now finished and has released an underspend which will go to QIPP. Community Older Adults CIPs still have to be met. Community Management The old year CIP element has now been transacted and we remain with the NP Travel CIP of 49k to be met. Early Intervention (EI) Continued usage of agency within CAMHS is supporting the prolonged WLI program (Agency 66k in month/ 223k Year To Date). This is offset by other areas of new developmental money where services are not yet up to speed (Overall CAMHS 62k). EI and Deaf CAMHS continue to have some pay slippage. 8
123 Cost Improvement Programme Annual Of Which Schemes CIP Delivery to Date Likely Achievement Recurrent 17/18 Commentary Devolved to Still Held Cost Improvement Programmes (by POD) Ref Plan Service Lines Centrally Achieved Outstanding (excl. mitigations) Plans Outstanding 4 Step Down Beds from DGoH CIP , , , ,500 Walsall QIPP Access Pathway (Urgent Care) CIP ,000 75, , ,000 Dudley Primary Care & IAPT Decommissioning CIP , , , ,000 - Operational Budget Reserves CIP , , , ,000 - Increase NCAs CIP , , , , ,000 - Corporate Operations CIP , , ,879 1, ,000 1,121 Shift Pattern review CIP , , , ,882 10, ,882 Estates Review CIP ,000 50, ,000 50,000 - Efficient Recovery Pathway Review CIP , , , ,000 MEA Revaluation of Fixed Assets CIP , , , , ,000 Inflation Topslice CIP , , , ,000 - Vacancy Review CIP , , , , ,281 - Apprenticeship Levy CIP ,000 60, ,000 60,000 - TCT Back Office Review CIP , ,000 54,000-4,000 54,000 - Non Recurrent Savings CIP , , , , ,000 Non Pay Review (Travel savings) CIP , , ,384 23, ,000 - Budgetary Reserves CIP , , , ,000 - Casual Vacancy Deductions (Non Recurrent) CIP , , , , , ,000 Walsall Carers Service CIP ,250 56, ,250 56,250 - Total CIPs 3,764,750 2,836, ,500 2,906, ,286 3,238,621 1,894,503 Current RAG The Trust had initially declared a plan to NHSI of 2,500k in order to deliver the planned surplus of 1,839k However, internally in order to deliver the required plan in year (meeting requirements around cost pressures, etc) the Trust has had to identify CIP schemes of 3,776k In total 19 separate schemes have been identified in order to deliver the 3,776k CIP target. The table opposite identifies these schemes and the current expectations and performance to date. At the beginning of the new financial year all but four schemes had been devolved down to service lines. CIP schemes 12, 14 and 18 in relation to vacancies have now all but been delivered, with a total of 228k remaining against central funds. This is effectively scheme CIP01 at 179k plus a residual balance on the three vacancy CIPs mentioned above, still to be delivered. As of Month 5 a total of 2,906k has been delivered out of the overall 3,776k target. Annual Target 17/18 3,776,246 3,776,246 (Deficit) / Excess of Schemes Above Plan -11, ,625 9
124 NHS Improvement Agency Expenditure Cap 2017/18 Agency Analysis 17/18 - Performance by Service Line Annual Profile Agency Agency Distance Service Line To Meet Cap Actuals M1-M5 Plan M1-M5 from Target 000s 000s 000s 000s Urgent Care & Access InPatient Services 1, , ahead of plan Community Services Early Intervention 1, , ahead of plan Dudley Medical Walsall Medical , behind plan Corp IT Services Corporate Affairs Corporate Estates Corporate Operations Corporate-CEO Corporate-Finance Corporate-HR Corporate-Medical Corporate-Performance Corporate-Reserves ahead of plan Grand Total 4,050 1,558 1, ahead of plan Commentary For 2017/18 the Trust has been tasked with working within an overall agency expenditure cap of 4.05m for the year. The planned spend across the year has been profiled across the new service lines based on the spend patterns from the previous year with an assumed level of reduction in spend in order to meet the required cap. The Trust has also been tasked with further reducing its Medical Locum spending by 86,760 in year in order to support the national drive to reduce locum spending this expectation is embedded within the 4.05m cap but will be monitored against last financial years Medical Locum spend of 1.284m. If the Trust is able to work within the Medical Locum spend plan of 1.1m it will more than deliver the required spending reduction expected. In month the Trust has spent 389k on Agency (up from 297k last month) and Year To Date the spend equates to 1,558k, which is below the planned spend position and is therefore 148k ahead of the cap. for 2017/18 there is an embedded expectation that Medical locum spending would reduce compared to 2016/17 levels in order to support the national delivery of a 150m Medical locum reduction. For the Trust we have been tasked with reducing our Medical locum spend by 86,760 over our 2016/17 levels of 1.284m The 'plan' above of 1.1m would ensure that this target is fully achieved 10
125 Agency Spend by Staff Group In Mth ( 000) Year End ( 000) Plan Act Variance Plan Act Variance Agency Staffing Qualified Nursing Medical Other (Incl. Admin, Estates, HCA's, AHP's) ,705 1, Other' represented by: Unqualified Nursing note 1 Admin & Clerical / Maint & Works note 2 Scientific & Technical note note 1 note 2 note 3 Malvern 4.4 Estates 65.9 Walsall CAMHs 61.5 Wrekin 5.3 E-Rostering 44.3 Pharmacy 0.0 Clent 6.0 IM&T 0.4 Dudley CAMHs 28.7 Kinver 8.7 DPH / BF Med Secs 22.2 Dudley Primary Care Langdale 9.1 Finance / HR / PA's 33.4 Walsall IAPT 0.0 Cedars 7.8 ANS 1.4 PT Hub 0.0 Linden 14.8 Walsall IAPT 7.9 OA Malvern / OT / 26.7 Ambleside 17.8 Walsall CAMHs 5.7 Mgmt / EAS Holyrood 34.8 Dudley CAMHs 13.7 Adult In-Pats 62.6 Birch Day 0.1 Dudley Primary Care 13.6 Criminal Justice 17.7 Dudley Access 4.4 Dudley CRS Dudley EI 36.4 Old Year Accruals w/o Commentary This view of the agency spending looks at the staff groups categories that are reported to NHSI on a monthly basis. A further breakdown is provided around the other staff category which identifies the main service line / budget areas that contribute to this category. As experienced last financial year some of the spending in month has been the result of additional support needed to cover areas such as: observations Support for one-off project works, such as E-rostering and Water Management Delivery of in year waiting list schemes funded non-recurrently by commissioners, for example, CAMHs. These additional costs will continue to be a pressure to the Trust in terms of delivery against the agency cap target. 11
126 Agency Reported Shift Breaches to NHSI (weekly) No of Shift Breaches by Week/Staff Group 40 No of Shifts Apr 10-Apr 17-Apr 24-Apr 01-May 08-May 15-May 22-May 29-May 05-Jun 12-Jun 19-Jun 26-Jun 03-Jul 10-Jul 17-Jul 24-Jul 31-Jul 07-Aug 14-Aug 21-Aug 28-Aug 03-Apr 10-Apr 17-Apr 24-Apr 01-May 08-May 15-May 22-May 29-May 05-Jun 12-Jun 19-Jun 26-Jun 03-Jul 10-Jul 17-Jul 24-Jul 31-Jul 07-Aug 14-Aug 21-Aug 28-Aug Medical (Price) Nursing (Price) HCAs (Price) Admin & Estates (Price) Total Shifts Commentary The above graph represents the reported shift breaches in terms of agency staff who are charging hourly prices above the mandated agency cap rates. The graph also represents the level of total shifts reported each week to NHSI as part of the revised agency returns this gives some indication therefore of the level of breaches as compared to total shifts worked. Reporting is reflective of staff groups as per TFIMS headings Medics do not appear on this analysis as they are covered under StaffFlow which ensures that agencies used and rates paid are in line with the mandated agency rules. 12


127 Capital Programme to Month 04 Commentary The budget for the Clinical Systems Development has been reduced in year by 1,700k. 1,200k of this has been used to fund additional Estates projects and to create a contingency for further capital works that may be required in year. The remaining 500k will be taken off the Trust s CRL for this financial year, as discussed at the Estates and Capital Planning Group in June
128 Payables Performance & Aged Debt Better Payment Practice Code Aged Debt as of August 2017 Current days days days 120+ days Agreed Tolerances Non-NHS <75% 75% - 95% >95% Commentary on Payables Transactions by Number Value Qtr % 98.02% Jul 96.75% 99.12% Aug 93.30% 97.53% Non-NHS YTD 95.12% 98.11% NHS <75% 75% - 95% >95% Qtr % 93.54% Jul 96.55% 93.05% Aug % % NHS YTD 96.22% 94.23% 39.1% 5.6% Commentary on Aged Debt 14.8% 15.3% Debt Profile and Value 25.2% Current days days days 121+ days Total ,122 Aged Debt Value % of Total Agreed 000 Tolerances Debt Over 91 days >20% 10% - 20% <10% % Over 120 days >10% 5% - 10% <5% % Better Payment Practice Code The Trust has achieved the required target for non-nhs invoices by value within the current month and by both number and value Year To Date (YTD). In terms of the NHS target there has been full delivery against both number and value within the current month and for numbers processed YTD, with a marginal under-performance against the NHS Value KPI.. The NHS metrics can vary dramatically in terms of percentage achievement as the number of NHS invoices processed each month is on average around 30 invoices in total. Thus a delay in payment of 2 invoices will cause the percentage to drop below the required 95%. Aged Debt Profile by Value 39.1% of debt was aged 91 days or older at the end of the period equating to 439k in total, and this is explained by: Debt between days (totalling 63k) relates in the main to: Dudley CCG 39.6k re Lion Health project Walsall Healthcare re Older Adults Psych iatric Liaison 14.0k Wolverhampton MBC 11.4k re IPS (Protect) project Debt over 120 days old (totalling 439k) relates in the main to: IMS Health 1.4k Merck study Various CCGs re 1617 NCAs of 16.5k Walsall MBC 132.6k re Q3/Q S.75 Dudley CCG 288.2k re a combination of 16/17 CQUIN settlement and IAPT 14
129 Cash Flow Statement '000 Cash Flows from Operating Activities Adjusted Operating Surplus/(Deficit) 1,260 Depreciation and Amortisation 670 (Increase)/Decrease in Trade and Other Receivables (213) Increase/(Decrease) in Trade and Other Payables (1,148) Increase/(Decrease) in Provisions 0 Dividend Paid 0 Net Cash Inflow/(Outflow) from Operating Activities 569 Cash Flows from Investing Activities Interest received 11 (Payments) for Property, Plant and Equipment (903) Proceeds from sale of assets 0 Net Cash Inflow/(Outflow)from Investing Activities (892) Net Cash Inflow/(Outflow) before Financing (323) Cash Flows from Financing Activities 0 Net Increase/(Decrease) in Cash (323) Cash at the Beginning of the Period 16,966 Cash at the End of the Period 16,643 Commentary Cash Flow The Trust has made an operating surplus of 1,260k in 2017/18 and received cash of 670k in respect of depreciation and amortisation Trade and Other Receivables have increased over the period (a negative impact on cash) Trade and Other Payables have decreased over the period (a negative impact on cash) The Trust has received 11k of interest, and spent 903k on capital (including on reducing capital payables from the 2016/17 year end). Total capital expenditure in cash terms was less than the cash received for depreciation and amortisation (a positive impact on cash) The impact of all these movements was to reduce the Trust s cash balance Year To Date by 323k EBITDA at 31 August 2017 as per Summary Slide 4 1,930 Deduct Depreciation and Amortisation (670) Add Back Fixed Asset Impairment Reversal 0 Adjusted Operating Surplus at 31 August ,260 Cash Benchmark (assuming no other working capital movements) Opening cash 16,967 Planned surplus 1,839 Release of Capital Payables (583) Capital Expenditure in excess of Depreciation and Amortisation (1,789) Realisation of PDC Receivable 14 Interest Received 30 Expected Cash at 31 March ,478 15


130 Statement of Financial Position as at 31 st August 2017 Commentary Non Current Assets Amortisation and depreciation exceeds capital expenditure for the year decreasing the value of the Trust s Non- Current Assets in year Final outturn against capital schemes is reviewed later in this report Current Assets Receivables have increased by 214k in 2017/18 Cash is 323k lower than the balance at 31 March 2017 An analysis of cash flows can be seen elsewhere in this report Current Liabilities Payables have reduced by 1,334k in the financial year There has been no movement in the value of provisions held since the start of the year Tax Payers Equity The Current Year I&E figure represents the surplus for the year to date of 933k This is 124k ahead of the plan for Month /18 16
131 Board meeting date: 5 October 2017 Agenda Item number: 7.1.3f Enclosure: 14 Report Title: Cost Improvement Programme (CIP) Progress Report Accountable Director: Author (name & title): Purpose of the report: Rupert Davies, Interim Director of Finance, Performance, IM&T and Estates Jacky O Sullivan, Clinical Development Director/Acting Associate Director of Operations To present to the Board a summary of the current status of the Cost Improvement Programme for 2017/18. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report CIP, Growth & Improvement Programme Board, 19 th September Finance and Performance Committee, 25 th September Key points or recommendations from Committee or Group: 19 schemes were identified in 2017/18 to achieve the CIP target of 3,778,000. Of these 19 schemes, 4 have delivered, 9 are being progressed, and 6 schemes are under development. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources Quality Impact Assessment Domain Patient Safety Patient Experience Clinical Effectiveness / Outcomes Workforce Experience Efficiency & Productivity Continuous Improvement in the Quality of Care Comment Will be considered as part of the Quality Impact Assessment for each scheme Will be considered as part of the Quality Impact Assessment for each scheme Will be considered as part of the Quality Impact Assessment for each scheme Will be considered as part of the Quality Impact Assessment for each scheme Will be considered as part of the Quality Impact Assessment for each scheme Enc 14 TB CIP update September 2017 v2page 1 of 14
132 The CQC domains that this report relates to are: Caring Plans use evidence based practice to ensure improvements in quality, outcomes and patient experience. Responsive Plans are developed to ensure responsiveness to service user needs. Effective Well-led Safe Plans represent best value to ensure CIP plans are met through efficiency and effectiveness All transformational and service development plans have a project team approach to both development and implementation. All plans are assessed for the need for a Quality Impact Assessment and where indicated a full assessment including risks and mitigations is undertaken and monitored. Enc 14 TB CIP update September 2017 v2page 2 of 14
133 CIP ideas brainstormed and scoped by Management Executive Team (MExT) and wider Review of all strategic themes by Trust Board to agree which proceed further within these parameters: High Quality Services Inclusive Partnerships Supporting Strategies Effective & Efficient Resources Leadership Culture Responsible Workforce No Idea archived Yes Idea developed and presented to MExT MExT approve/reject No Idea archived Summary of schemes including Quality Impact Assessment (QIA) & risks submitted to MExT and Trust Board Project Workbooks developed & submitted to CGI Programme Board for approval & sign off including QIA, EIA, PIA & risks All projects complete Workbook Completed workbooks & QIA signed off by Director of Nursing and Medical Directors and MExT Implementation Stage Final QIA and risks presented to MExT for project closure QIA & risks on delivered projects presented to CGI Programme Board for sign off including Director of Nursing & Medical Directors Final QIA and risks presented to Trust Board for final sign off Enc 14 TB CIP update September 2017 v2page 3 of 14
134 Title Cost Improvement Programme (CIP) Progress Report Introduction The purpose of this report is to present to the Board a summary of the current status of the Cost Improvement Programme for 2017/18. Executive Summary of key points, issues, financial impact and risks 19 schemes were identified in 2017/18 to achieve the CIP target of 3,778,000. Of these 19 schemes, 3 have delivered and closed, 1 has delivered and risks are being monitored, 9 are in progress and 6 schemes are under development. Summary of key points, issues and risks 1. CIP 2016/17 2 schemes were carried over from 2017/18 (appendix 1), these are: Dudley Older Adult Service Medical Services Establishment Review The Dudley Older Adult Service scheme is dependent on the implementation of the new service model, and is expected to deliver in quarter 4. The most recent delay to the project has been to return to the Overview and Scrutiny Committee; this has now taken place and will now be considered by the CCG Clinical Development Committee in October. It is expected that the final model will be signed off at this meeting and implementation will then commence with a completion date of March The Medical Services Establishment Review scheme delivered 200k recurrent savings in 2016/17; the remaining 150k is being delivered from income on the Adult Neurodevelopmental Service. The service has a monthly income target which is on plan at month 5 and forecast to achieve the full year effect by March These schemes are being monitored by the CIP, Growth and Improvement Programme Board. 2. CIP 2017/18 Target for 2017/18 3,778,000 Full year value of identified schemes 3,778,000 Planned part year effect of identified schemes 3,764,750 There are a total of 19 schemes for 2017/18. 3 schemes have delivered and are now closed. A fourth scheme, Operational Budget Reserves has delivered and will be monitored until the end of quarter 2. The quality impact assessment for the Dudley Primary Care & IAPT Decommissioning was presented to MExT in September 2017 for approval. Enc 14 TB CIP update September 2017 v2page 4 of 14
135 9 schemes are in progress of which 2 are red RAG rated, these schemes are: MEA Fixed Asset Revaluation Maximising Apprenticeship Levy The Walsall Carers Service scheme has delivered and was presented to MExT in September 2017 for closure. The remaining 5 schemes are under development and the quality impact assessments will be presented to the joint Medical Directors and Director of Nursing when completed before progressing to MExT and Quality and Safety Committee, these schemes are RAG rated red: Step down Beds Walsall New Urgent Care Pathway Corporate Operations Budget Establishment Review Efficient Recovery Pathway Review Recurrent savings have been identified for the Efficient Recovery Pathway Review scheme, which meet the part year effect value. The RAG ratings are being reviewed by the CIP, Growth and Improvement Board and MExT and will be reflected in the next report. A full list of projects can be found in appendix 2. The CIP, Growth and Improvement Programme Board will be monitoring and tracking the progress of these schemes to report risks, and mitigations to the Finance and Performance Committee and the Board. 3. CIP 2018/19 A list of potential schemes has been identified (appendix 3) and work is in progress to scope these. It is unlikely that any of these will be ready to deliver this financial year. Further detail (if required) Appendix 1, 2 and 3 contain further details of the schemes. Recommendation Trust Board members are asked to note the contents of this report and receive it for information and assurance. Board action required No action required. Enc 14 TB CIP update September 2017 v2page 5 of 14
136 Appendix /17 CIP schemes Division Type Ref. Project Title Exec Lead Balance to FYE Value ( ) Overall Project Status Implementation Plan Finance KPIs Risks QIA Progress Report Operations Transformational CIP Dudley Older Adult Service Medical Transformational CIP Medical Services Review LW 67,390 R A R N/A A A Implementation expected to commence in October with completion and delivery of CIP by March MW / KG 150,000 R A G N/A R A This is being achieved through income for the Adult Neurodevelopmental Service which is on target at month 5 and forecast to achieve the full amount by March The red risk is under review with potential to downgrade it. Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 6 of 14
137 Appendix /18 CIP schemes Project Status Red Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Step down Beds Income generation through the provision of step down beds. Discussions are being held with Dudley CCG. Lesley Writtle None 238,000 R R R R R No impact No impact N/A 238, ,500 Walsall New Urgent Care Pathway Remodeling of the urgent care pathway in Walsall as part of a QIPP will potentially deliver this scheme. Commissioner intentions of the future model are needed to progress the scheme. Lesley Writtle None 150,000 R R R R R No impact Yes N/A 150,000 75,000 Dudley Primary Care and IAPT Reduce expenditure on service by 200K in line with CCG reductions. The scheme is being transacted non recurrently. Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 7 of 14
138 Project Status Red Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Decommissioning Lesley Writtle None 200,000 R R G R R No impact No impact N/A 200, ,000 Corporate Operations Budget Establishment Review Savings to be realised from the Corporate Operations budget. Savings have been identified from vacancies which meets the PYE. Lesley Writtle None 300,000 R R A R R No impact No impact N/A 300, ,000 Rostering review or changing work patterns to deliver savings. The original plan will not be progressed. The scheme is under review. Rosie Musson None 250,000 R R R R R No impact No impact N/A 250, ,000 Efficient Recovery Pathway Review Savings to be realised from reduction in activity and new service model. Scoping for this scheme is ongoing. Recurrent savings have been identified which meet the PYE value. Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 8 of 14
139 Project Status Red Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Mark Weaver Urgent Care Outpatient Review 250,000 R R A R R No impact No impact N/A 250, ,000 MEA Revaluation of Fixed Assets Maximising Apprenticeship Levy PDC savings and IT depreciation moving to 7 years. The target is being met non-recurrently, the scheme is unlikely to deliver recurrently. Rupert Davies None 400,000 R R R G G No impact No impact N/A April , ,000 This project will look at opportunities to introduce apprenticeships with scope to generate non recurrent savings. It is unclear whether the scheme will deliver savings. Ashi Williams TCT Back Office review 240,000 R R R A G No impact No impact N/A 240,000 60,000 Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 9 of 14
140 Scheme Executive Lead Links to other projects Value Overall Project Status Project Status Amber Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Operational Budget Reserves Estates Review Removing an uncommitted reserves budget. The scheme has delivered and will be monitored until the end of quarter 2. Lesley Writtle None 150,000 A G G A A No impact No impact N/A April , ,000 Review the Trust s portfolio of properties across Dudley and Walsall with a view to minimising the use of leased properties and maximising the use of owned properties. Rupert Davies None 100,000 A A A A A No impact No impact N/A 100,000 50,000 Vacancy Review Long term vacant posts will be assessed for continued requirement and removal. The PYE figure has been met. Ashi Williams ECT project 400,000 A G A A A No impact No impact N/A April , ,000 TCT Back Office Review This project will reduce the requirement of redeployment/redundancy when the Transforming Care Together (TCT) Partnership Trusts merge in coming months/years. This will contribute to current and future cost saving schemes. Savings have been identified from vacancies and meet the Part Year Effect. Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 10 of 14
141 Scheme Executive Lead Links to other projects Value Overall Project Status Project Status Amber Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Rupert Davies / Ashi Williams None 100,000 A G G A A No impact Yes N/A April ,000 50,000 Non recurrent Savings A non-recurring contribution to the recurring shortfall of the 2016/17 QIPP. This relates to end of year provisions which may not be required in 2017/18, and can therefore be used to offset slippage on the QIPP. The scheme has delivered. Rupert Davies None 500,000 A G G G A No impact No impact N/A April ,000 Budgetary Reserves Savings from budgetary reserves. The scheme has delivered. Rupert Davies None 500,000 A G G A G No impact No impact N/A April , ,000 Casual Vacancy Reduction (Non recurrent) Non recurrent savings from vacancies. Savings are being identified on a monthly basis. Rupert Davies / Lesley Writtle None 500,000 A G G G A No impact No impact N/A April ,000 Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 11 of 14
142 Scheme Executive Lead Links to other projects Value Overall Project Status Project Status Amber Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Increase in NCA Activity Walsall Carers Service Income generation through non contracted activity. The scheme is behind schedule. Lesley Writtle / Rupert Davies None 200,000 A G A A A No impact No impact N/A April , ,000 Decommissioning of the carers service by the CCG will deliver savings. Savings have been realised and will be transacted. Lesley Writtle None 75,000 A G G A A No impact Yes N/A July ,000 56,250 Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 12 of 14
143 Scheme Executive Lead Links to other projects Value Overall Project Status Project Status Green Plan Finance Risks QIA EIA PIA KPIs Implementation Month Planned Recurrent FYE Value ( ) Planned PYE Value ( ) Inflation Topslice Topslice of inflation dependent on budget setting. The scheme has delivered. Rupert Davies None 125,000 G G G G G No impact No impact N/A April , ,000 Non Pay Review Deliver savings via a review of the travel expenditure. Savings are being transacted. Rupert Davies None 100,000 G G G G G No impact No impact N/A April , ,000 Key: QIA = Quality Impact Assessment KPIs = Key Performance Indicators PIA = Privacy Impact Assessment EIA = Equality Impact Assessment Enc 14 TB CIP update September 2017 v2page 13 of 14
144 Appendix /19 Potential CIP schemes Type Project Title FYE Value 18/19 ( ) FYE Value 19/20 ( ) Transformational Walsall QIPP Rehab Out of Area Savings 300,000 Transformational Bloxwich Cost Savings 0 312,000 Transformational Productivity Growth in Dudley Locality 500,000 Transformational Challenging Behaviour Unit 0 200,000 Transformational TMS 100,000 Transformational Female PICU 200,000 Transformational Review PD Pathway 0 Transformational Zero-base IP and Community Services 500,000 Transformational Inpatient CAMHS Ward Transactional Establish Complex Care Ward 300,000 Transactional CAMHS Overheads 200, ,000 Transactional Corporate CIP Target from TCT 250, ,000 Transactional Increase in Older Adults Inpatient Price 250, ,000 Transformational QIPP: Walsall Access pathway 150, ,000 Transformational QIPP: Walsall Medical Staffing 125, ,000 Transformational QIPP: Walsall Older Adults Nursing 0 250,000 Transformational QIPP: Walsall Older Adults Medical Staffing 0 150,000 Transformational QIPP: Walsall Older Adults Out of Area Income 376, ,000 2,751,000 2,763,000 Enc 14 TB CIP update September 2017 v2page 14 of 14
145 Board meeting date: 5 October 2017 Agenda Item number: 7.1.4a Enclosure: 15 Report Title: Workforce Committee Chair s Report Committee: Author: Workforce Committee Harry Turner Non Executive Director Action required from the Board Decision / Approval Gain assurance Introduction Discussion Information The Workforce Committee met on the 25 th September 2017 and considered and discussed key topics around the Trust s Workforce. The Workforce committee agenda is categorised under 4 main areas: - Workforce Performance - Staff Wellbeing - Organisational Development - Workforce Compliance Summary of key points, issues and risks WORKFORCE PERFORMANCE Workforce Performance Report Month 5 Key messages from the Workforce Performance Month 5 Report were: - There are currently 100 Full Time Equivalent contracted vacancies across the Trust meaning the vacancy rate has reduced to 9.1% in Month 5 from the 13.3% reported in Month 3. - The reason for the reduction in vacancies is the removal of budgeted 43 Whole Time Equivalent associated to CIPs for this financial year. It was agreed that assurance would be sought from the Quality and Safety committee that there were no adverse quality impacts on the removal of these roles. - The TRAC recruitment system is currently being used within the Trust giving increased control and oversight to recruiting managers and allows the Trust to performance manage against recruitment KPIs. Enc 15 WFC Chairs Report M5 17 Page 1 of 6
146 - The 12 Month Turnover rate has increased from 11.21% to 11.97% which in itself is not significant, however the committee is monitoring any increased turnover due to TCT particularly from Corporate services and the risks associated with any vacancies not being filled. - The rolling 12 month sickness rate has decreased from 4.05% in Month 4 to 3.93% in Month 5, this is within the Trusts target and the tenth consecutive month of being so. In month sickness has decreased from 4.02% in Month 4 to 3.35% in Month 5. - Appraisal Compliance has increased from 84.8% to 87.9%, this is above the Trust target of 85%. - Mandatory Training - Mandatory Training compliance increased from 90.6% in Month 4 to 92.0% in Month 5 and is above the target of 90% agreed at MEXT for all mandatory training. - An Essential Skills Spotlight was presented detailing the actions the ruts will take to improve Essential Skills Training compliance from 73% to the 90% target. Practice Placement annual report An evaluation carried out jointly between the Trust and The University of Wolverhamption of the Trusts placements for student nurses in 2016/17 was presented. The evaluation showed excellent results with 90% of students feeling supported by the Trust and its mentors. The work the Trusts Practice Placement Manager has done to support students was recognised by the Committee. TRAC Recruitment system Evaluation In February 2016 the Trust implemented the TRAC recruitment system, an evaluation has been conducted by CW Audit which has shown positive outcomes and strengthened a number of controls within the Trust s recruitment process. 8/10 of ten staff who responded to the survey expressed that they thought the TRAC system had led to improvements. Calculation of time at each key stage of the recruitment process in comparison to the results in July 2016 showed improvements in performance at all stages with a net average decrease in time to recruit of 41 days. In order for further benefits to be realised, focus should now be placed on finalising and reporting recruitment KPI s to support the ongoing performance management process. The CW Audit report details the recommendations made and agreed actions to include: Update Recruitment Policy and processes to refer to TRAC processes Agree final Recruitment KPIs to measure performance against Ensure training is available to managers TCT partners are also considering a business case to implement TRAC across TCT. Vacancy Position Following the star chamber meetings conducted by the Chief Executive officer and Director of Finance a report was presented detailing the 43 whole time equivalent vacancies which have been identified and removed from the budgeted establishment without any adverse impact on performance or patient safety/quality of case. Assurance will be provide to the Quality and Safety Committee Enc 15 WFC Chairs Report M5 17 Page 2 of 6
147 DBS Progress Update In October 2016 the Trust implemented sign up to the DBS Update service. Whist this is not a legal requirement in order to adequately safeguard the Trust s vulnerable groups, a decision was taken to implement the DBS Update Service and prioritise staff whose roles required an enhanced DBS check in the first instance. Consultation with the workforce has taken place making it a contractual requirement to be registered with the update service if the role required an enhanced DBS check 886 employees were identified as requiring a DBS check in order to register with the DBS Update service. The majority of checks have now been completed and there are 22 staff (2%) remaining to be checked from the original list. From December 2017 onwards; the Trust will be required to operate a monthly program of subscription updates which involves identifying forthcoming subscription lapses via ESR reporting and individually entering each of the DBS accounts and paying the 13 annual subscription fee on behalf of the employee. At the same time the certificate will be checked for validity and any staff identified with a change to their certificate will be required to undertake a new DBS check. E-Rostering Update Good progress has been made with the implementation of the E-Rostering system. 82 rosters are now attached to ESR interface, removing the need for timesheets or paper based turnarounds. There are 19 more active rosters which need to be attached to the interface and the team is working currently to get these services connected to ESR for the October and November turnaround periods All nursing, catering and admin bank staff are being paid via the system Paper timesheets going to payroll now reduced to annual leave claims only Roster performance dashboards are being produced monthly for consideration by Director of Nursing and the Roster Improvement Group. These will also be presented to the Workforce Committee on a quarterly basis We are now in the Improvement phase of the project with a view to entering the Sustainability phase to realise the benefits of the project. STAFF WELLBEING Health and Wellbeing Update The Trust is launching its Staff Health and Wellbeing week, week commencing 25 th September Following on from the success of the Health and Wellbeing days in January 2016 a range of support is being offered across Dudley and Walsall sites, including: Goody bags with informative literature, healthy snacks and drinks Health checks Healthy Food choice stands Training around stress management, resilience and mindfulness Physical activity support Stop Smoking support Flu Vaccination clinics It was agreed that more information on the benefits available to staff will be publicised and access to local gyms at a discounted rate. Enc 15 WFC Chairs Report M5 17 Page 3 of 6
148 The Trust is launching its Flu Campaign on 1 st October 2017 and is also working in partnership with TCT for a consistent approach. Following 2016 success the Trust is training up to 20 peer vaccinators to support the campaign, support will continue to be received by SWBH Occupational Health. Incentives will be offered to staff ie 1 days annual leave monthly prize draw and a donation to UNICEF for every vaccination, in order to help achieve the CQUIN target of 70% of frontline staff being vaccinated. ORGANISATIONAL DEVELOPMENT Staff Engagement Update 2017 Staff Survey Following the results priority was given to actions around 1. Bullying & Harassment, 2. Health & Well-being, 3. Appraisals and 4. Senior Management Communications, In a change we adopted a service line specific approach rather than a generic Trust wide one, enabling a more nuanced focus on specific areas e.g. bullying & harassment is more of an issue in inpatient settings than say community. In addition with responsibility for action planning sitting at service line level gives them ownership of initiatives is likely to result in them being followed up Staff Survey Due to the timing of the formation of the new Trust vis a vis the National Staff Survey the three TCT Trusts will undertake three separate 2018 Staff Surveys and receive three sets of results. We are proceeding as though already one organisation in terms of adopting full staff surveys, a mixed mode (electronic and paper copies), common communications promoting the survey and launch/close timings, to ensure a consistent and coherent message it is then anticipated that these will be reviewed and analysed together to produce one Trust wide set of proprieties. TCT Extensive engagement work is being undertaken collaboratively across all three Trusts to support staff through the period of transition and beyond, notably the creation of Change Champions (modelled on DWMH s existing Engagement Champions) to be local experts and lead on local communication, feedback and facilitation of organisational development (OD) especially beyond October 1 st. Staff Friends and Family Test Q1& Q2 results for 2017 showed a drop initially in Extremely Likely/Likely responses to DWMH as a place for Treatment / Place To Work over 2016/17 results but these appear to have stabilized in Q2; this probably indicative of additional anxieties during a period of change it should be noted that they remain comparable to 2016 results however. WORKFORCE COMPLIANCE Workforce Risk Register The Committee received the workforce risk register and the Committee was assured that the risks are being appropriately managed. Enc 15 WFC Chairs Report M5 17 Page 4 of 6
149 No new risks have been added to the register. It was agreed that a comprehensive review if the risks would be carried out as some risks can now be removed or downgraded in severity. This will be presented to the next Workforce Committee. WRES Update A quarterly update on the Trusts WRES scheme was presented. There has been a number actions delivered between 2016 / 2017 to address the barriers identified in the 2016 data submission. Key Headlines: Reviewed current development opportunities for BME staff and Promoted NHS Leadership Academy Stepping up Programme within the Trust. 5 BME members of staff applied with 3 accepted onto the programme. Programme commenced in May. Developed a MERIT WRES dashboard and share best practice case studies with partners. Links now made with Community and Voluntary organisations including the Centre for Equality & Diversity. Arrangements in place to advertise potential jobs within the Trust to a much wider and diverse range of communities Reviewed and refreshed the E&D Policy to include inclusion and equality of opportunities. Reviewed and refreshed the recruitment selection training for recruiting managers and training on unconscious bias for all recruiting managers In process of developing a BME Talent Management initiative through MERIT. This will be discussed further at the E&D Work stream in October 2017 Carried out an Audit on Recruitment campaigns: CW Audit report completed highlighting current picture regarding recruitment practice for BME staff. Report to be submitted to the Trust Workforce Committee. Further promoted support mechanisms available to staff and service users whom report bullying, harassment and discrimination, such as Cultural Ambassadors Programme and Work Place Advisors. Ensured that all managers and staff undertaking disciplinary Investigations, hearings and appeals undertake: Equality and Diversity training, Unconscious Bias training and Cultural Competence training. Revised and developed Bullying and Harassment Policy. Forward Thinking Leadership conference held in May and organising a masterclass in Inclusion going beyond the inclusion conversation on 26 th September The Trust is taking forward the 2017/18 plans and continuing to work with TCT and MERIT partners. Safe Staffing Levels The safe staffing level report was presented. Across the inpatient areas the overall fill rates are %, with 96.92% for registered staff and % for care staff. This indicates the Trust is meeting the optimum level of fill rates. Typically where our care staff rates exceed 100%, this is due to temporary staff being used to support patient observations, increases in acuity or changes in skill mix Enc 15 WFC Chairs Report M5 17 Page 5 of 6
150 A significant improvement has been made with the safe staffing levels on Night Shifts largely due to the additional and targeted recruitment to the night shifts. The following actions are being taken to ensure temporary staffing is used effectively and efficiently Vacancy review has been completed for inpatients; the Trust faces challenges in relation to the recruitment of Band 5 nurses and has a proactive recruitment campaign in place. Recent recruitment drives have been successful with new staff starting the end of September. Vacancy levels require ongoing monitoring. Optimising recruitment processes for bank staff a successful initial drive. Now a rolling programme supported by coms campaign. Implementation of best practice rostering metrics ward managers are working with rostering manager to maximize the efficiency of their rostering. Revised process for sign off of rosters through new inpatient manager allowing early detection of inefficiencies or concerns. Safer staffing report is being reviewed with TCT partners to enhance triangulation or metrics provide improved assurance to Trust Board. Revised format to be presented to Workforce Committee in October. Recommendation and requests for direction Trust Board is asked to: Accept this report for assurance about the exercise of delegated authority by the Workforce Committee Enc 15 WFC Chairs Report M5 17 Page 6 of 6
151 Board meeting date: 5 October 2017 Agenda Item number: 7.1.4b Enclosure: 16 EXTRAORDINARY WORKFORCE COMMITTEE MEETING Minutes of a Meeting Held on 4 th September 2017 Conference Room 1, Trafalgar House, Dudley START TIME 09:00 HOURS Present: Ashi Williams Acting Director of People (Chair) Debbie Cooper Vulnerable Adults and Children s Lead/Acting Head of Service Inpatients Nick Stephens Head of Service - Community Anne Marie Carey Head of Urgent Care and Access/Early Intervention Services Mark Banks Deputy Director of Finance Dr Kate Gingell Joint Medical Director Rosie Musson Acting Director of Nursing Becky Temple-Purcell Senior Workforce Development Manager Jeanette Rooke Apologies: Mark Axcell Michael Hirons Rupert Davies Paul Singh Lesley Writtle Hannah White Jacky O Sullivan Note Taker Chief Executive Officer Freedom to Speak Up Guardian & Staff Engagement Lead Interim Director of Finance Equality and Diversity Lead Manager Interim Director of Operations Senior HR Business Partner Clinical Development Director/Associate Director of Operations 43. Apologies for Absence ACTION Apologies noted as above. It was noted that the following members had been stood down from this meeting: Pete Hayward Consultant Occupational Therapist James Parker Commissioner Liaison Manager Hassan Omar Head of Social Care Andrew Campbell Chief Pharmacist Enc 16 Final WFC Minutes V1.0 Page 1 of 4
152 44. Minutes of the previous Extraordinary Workforce Committee meeting held on 3 rd August The minutes of the previous Extraordinary Workforce Committee were approved as an accurate record. 45. Matters Arising Action Point Mrs Musson one person s appraisal has been completed. An individual is due to return from sick leave today and the paperwork is still outstanding. Action carried forward. Action Point Gemma Peters appraisal paperwork has been completed. Action completed and closed. Action Point a Dr Gingell to update letter re. outstanding appraisals. Action carried forward. Action Point b Mr Peniket to update any appraisals still outstanding after meeting. Action completed and closed. Action Point an update to be provided during the meeting. Action Point Mrs Writtle was not present at the meeting and Mr Peniket was on annual leave, therefore this action point to establish whether an appraisal list was complete could not be established during the meeting. Action carried forward. Action Point a Mrs Carey sent the list of Early Interventions to L&D re. update for areas of compliance around appraisals. Action completed and closed. Action Point b Mrs Shaw s appraisal was queried as she had taken on a new internal role. Action carried forward. Action Point c Update for Early Intervention to Dan Peniket. Action carried forward. Action Point d after the appraisal the paperwork will be completed. Action carried forward. Action Point e EI list to be sent to Mrs Writtle. Action carried forward. Action Point a not sure if the in-patients planned appraisal timetable has been completed. Action carried forward. Action Point b implementation of ESR automatic reminders to managers and staff has not yet been actioned. Action carried forward. Mrs Musson Dr Gingell Mrs Writtle Mr Peniket Mark Axcell Mr Stephens Mr Peniket Mrs Writtle Mr Peniket Enc 16 Final WFC Minutes V1.0 Page 2 of 4
153 Action Point c the Heads of Service continue to reinforce message to managers and staff in terms of mandatory training and appraisal compliance. Action completed and closed. Action Point d COMMS work in progress. Mrs Temple-Purcell is leading on appraisals. Action completed and closed. Action Point Mr Stephens to provide an update during the meeting. Action Point Dr Gingell to ensure 7 medics are compliant with their mandatory training. Action carried forward. Action Point safer staffing/nursing establishment review. Action carried forward. Dr Gingell Mrs Musson 46. WORKFORCE PERFORMANCE 46.1 Appraisal and Mandatory Training Compliance The overall appraisal compliance rate is 86%. Still areas that are not compliant. Mr Banks gave a quick update. 2 specific in Mr Banks team Louise has been completed and signed. Dan Howard is leaving this Friday therefore non-compliance is not applicable. One further in the team and two within IG department. Operations Level Management 3 at 84% - Mrs Musson gave update of those outstanding but in-hand. Appraisal by team tab medical level 3. Dr Gingell gave update re. all medical secretary s up to date. Paperwork is due in. 5 medical staff need updating. Older Adults at 52% - anomalies Mrs Musson has queried the data. Mrs Williams to send anomalies for updating to Mrs Musson. Inpatients Mrs Cooper states these are not corresponding with her data. Has been on leave and will need to update. Kinver ward data not corresponding and Mrs Cooper will update this week. Mr Stephens raised concerns re. apprentice not receiving induction or appraisal. Mandatory training is currently 92.6% for in-patients and IG. Mrs Cooper to update Mrs Williams. Mrs Musson to provide Mrs Williams with update. Community services (amber and some red) Mr Stephens advised 5 outstanding currently. Apprentice (Mr Jones) has not received Dr Gingell Mrs Williams Mrs Cooper Mrs Musson Enc 16 Final WFC Minutes V1.0 Page 3 of 4
154 46.6 training. Mrs Williams mandatory training can be done on-line. Mr Banks provided update with regards to finance which were mostly compliant only two people outstanding. Dr Gingell to remove Dr Maumi as he has now left the organisation. The termination paperwork has not yet been completed. Dr Gingell 47. WORKFORCE COMPLIANCE 47.1 MOU Passport for MERIT The Workforce Committee agreed to sign off the MOU Passport for MERIT. Mrs Musson queried the quality of training. Mrs Temple-Purcell has asked those responsible in the areas to look at overall objectives. Mrs Temple- Purcell 48. Any other Business 48.1 Mr Banks TCT partners/targets re. mandatory training. Will there be a significant blip? Mrs Musson stated there would be some variations. Slightly different expectations in some areas re. mandatory training they exclude for 1 month re. new starters and then others are excluding for 3 or 6 months which creates anomalies. Mrs Temple- Purcell comparing across various trusts to develop a common standard/approach. Mrs Williams confirmed they would continue to produce reports as is until the merger of the ESR systems. 49. Date, Time and Venue of the next meeting 49.1 Monday 25 th September to 1300 hours Board Room Canalside House, Walsall END TIME: 09:40 HOURS Enc 16 Final WFC Minutes V1.0 Page 4 of 4
155 Trust Board Meeting date: 5 October 2017 Agenda Item number: 7.1.4c Enclosure: 17 Workforce Performance Report Month /18
156 Workforce Report - Contents Page Key Messages Workforce Dashboard Recruitment Turnover Sickness Appraisal Mandatory Training
157 Vacancies There are currently 100 Full Time Equivalent contracted vacancies across the Trust meaning the vacancy rate has not significantly changed at 9.1% in Month 5 from the 9.0% reported in Month 4. The TRAC recruitment system is currently being used within the Trust giving increased control and oversight to recruiting managers and allows the Trust to performance manage against recruitment KPIs. Turnover The 12 Month Turnover rate has increased from 11.21% to 11.97%. The Trust s percentage turnover rate (excluding Junior Medical Staff) is average compared with other Mental Health organisations in the NHS. 3
158 Sickness Absence The rolling 12 month sickness rate has decreased from 4.05% in Month 4 to 3.93% in Month 5, this is within the Trusts target and the tenth consecutive month of being so. In month sickness has decreased from 4.02% in Month 4 to 3.35% in Month 5. Appraisal Compliance has increased from 84.8% to 87.9%, this is above the Trust target of 85%. There are 110 employees in the Trust that have not had an appraisal recorded in the last 12 months, an improvement of the 223 reported in September Bi Weekly reports are now being produced in order to support managers in highlighting with low compliance and future requirements. Mandatory Training - Mandatory Training compliance increased from 90.6% in Month 4 to 92.0% in Month 5 and is above the target of 90% agreed at MEXT for all mandatory training. As with the Appraisal, new reports are being distributed to Service leads to assist with what training individuals need to undertake in order to remain compliant. 4
159 445 Dudley and Walsall Mental Health Partnership NHS Trust Aug-17 Staff in Post Target Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Headcount Funded Establishment Staff in Post FTE (Contracted) WTE Variance Vacancy % 10.0% 17.3% 15.5% 14.6% 15.4% 14.0% 13.8% 13.6% 13.5% 13.5% 13.3% 9.0% 9.1% Clinical Vacancy % 10.0% 11.6% 12.1% Worked FTE (Substantive) Worked FTE (Temp) Worked FTE (Total) 1, , , , , , , , , , , ,154.5 Turnover % (12 Months) 8-14% 10.71% 11.47% 11.62% 11.27% 10.72% 10.33% 10.53% 11.56% 11.40% 11.18% 11.21% 11.97% Pay Spend Target Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Funded 4.16m 3.91m 4.18m 4.16m 4.34m 4.39m 4.49m 4.16m 4.28m 4.35m 4.14m 4.29m Substantive Spend 3.64m 3.60m 3.63m 3.45m 3.63m 3.70m 3.60m 3.73m 3.68m 3.75m 3.68m 3.39m Temp Spend 0.46m 0.48m 0.56m 0.52m 0.54m 0.58m 0.58m 0.38m 0.49m 0.54m 0.50m 0.79m Total Pay Spend 4.10m 4.08m 4.18m 3.96m 4.16m 4.28m 4.18m 4.11m 4.17m 4.29m 4.19m 4.18m Varaince - Budget to Actual 58K - 173K K 200K 171K 111K 307K 52K 116K 55K - 45K 113K Absence Target Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sickness % (Month) 4.68% 4.92% 3.90% 3.72% 3.66% 4.89% 4.57% 3.34% 3.59% 3.40% 4.01% 4.02% 3.35% Sickness Days Lost FTE (Month) 1,391 1,152 1,071 1,095 1,476 1,263 1,030 1,069 1,049 1,196 1,244 1,030 No of Sickness Episodes (Month) Cost of Sickness (Month) 130K 95K 85K 82K 114K 102K 90K 90K 81K 100K 111K 76K Maternity % (Month) 1.45% 1.64% 1.61% 1.85% 2.12% 2.19% 2.23% 2.05% 2.23% 2.36% 2.42% 2.35% Sickness % (12 Months) 4.68% 4.85% 4.73% 4.57% 4.43% 4.42% 4.39% 4.31% 4.24% 4.14% 4.11% 4.05% 3.93% Long Term Sickness % (12 Months) 69.6% 68.3% 68.0% 66.3% 64.0% 63.2% 62.9% 62.6% 63.5% 61.6% 62.5% 60.0% Cost of Sickness (12 Months) 1,457K 1,418K 1,359K 1,303K 1,292K 1,271K 1,260K 1,249K 1,208K 1,198K 1,195K 1,140K Development Target Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Appriasals Completed Appraisals Outstanding Appraisals Required Appraisal % 85% 73.7% 80.0% 79.1% 77.6% 79.4% 86.0% 87.0% 85.5% 83.1% 82.9% 84.8% 87.9% Mandatory Training % 90% 83.8% 85.4% 89.3% 89.7% 88.9% 88.9% 89.8% 88.0% 88.6% 88.3% 90.6% 92.0% Essential Skills Training % 90% 61.3% 62.1% 64.6% 65.6% 58.3% 66.1% 66.9% 68.3% 70.2% 71.8% 72.1% 73.7% Number of Training DNAs Training DNA Rate % 14.1% 22.0% 19.4% 14.5% 19.4% 5

160 Application to advert view rate Avg no of days advertised Staff Group No of adverts WTE Advertised Advert views Applications Applications per WTE Additional Clinical Services Additional Professional Scientific & Technical % Administrative & Clerical % Allied Health Professionals % Estates & Ancillary Medical & Dental % Nursing & Midwifery Registered % Total % The table above shows the number of adverts published on NHS jobs in August and the associated Whole Time Equivalent (WTE) by Staff Group. 20 of the WTE advertised for Nursing & Midwifery Registered were for Band 5 Ward Staff Nurses, and therefore more than 20 WTE could be recruited to the position due to it being a rolling recruitment advert. 6
 (Month) (12 Months) 445 CAF")
161 15.0% 14.0% 13.0% 12.0% 11.0% 10.0% 9.0% 8.0% 7.0% 6.0% 5.0% DWMH Turnover % by Month 12.0% 11.5% 11.6% 11.3% 11.6% 11.4% 11.2% 11.2% 10.7% 10.7% 10.3% 10.5% Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Target Range Turnover % Service Starters FTE Leavers FTE Turnover % (Month) (Month) (12 Months) 445 CAF Corporate Affairs Level % 445 CDP Corporate Development and People Level % 445 CDS Clinical Development Level % 445 CHX Chief Executive Level % 445 FIN Finance Level % 445 HR Human Resources Level % 445 OPS Operations Level % 445 MED Medical Level % 445 AOMGT Acute & Older Adults Management Level % 445 COM Community Services Level % 445 EIN Early Intervention Level % 445 INP Inpatient Services Level % 445 UCA Urgent Care & Access Level % 445 Dudley and Walsall Mental Health Partnership NHS Trust % 12 Month Turnover has increased to 11.97% in Month 5. This is within the Trusts targeted range and could be considered a good indicator that the Trust in general retains its staff. 7
162 Sickness Absence % v Trust Target 5.50% 5.03% 5.00% 4.80% 4.59% 4.50% 4.00% 3.50% 3.81% 3.89% 3.62% 3.33% 3.59% 3.40% 4.01% 4.02% 3.35% 3.00% Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Target Sickness % Sickness % 12mth Service Jul-17 Aug-17 Sickness % (12 Months) 445 CAF Corporate Affairs Level % 1.33% 1.14% 445 CDP Corporate Development and People Level % 0.00% 0.37% 445 CDS Clinical Development Level % 6.42% 7.70% 445 CHX Chief Executive Level % 1.74% 1.96% 445 FIN Finance Level % 0.92% 1.79% 445 HR Human Resources Level % 0.76% 1.51% 445 OPS Operations Level % 2.35% 5.05% 445 MED Medical Level % 1.06% 4.02% 445 AOMGT Acute & Older Adults Management Level % 2.46% 4.13% 445 COM Community Services Level % 1.86% 3.79% 445 EIN Early Intervention Level % 3.17% 2.60% 445 INP Inpatient Services Level % 5.50% 4.65% 445 UCA Urgent Care & Access Level % 5.11% 4.04% 445 Dudley and Walsall Mental Health Partnership NHS Trust 4.02% 3.35% 3.93% The rolling 12 month sickness rate has decreased in Month 5 to 3.93% from 4.05% in Month 4. This within the trusts target 4.68%. In month sickness has decreased from 4.02% in Month 4 to 3.35% in Month 5. 8
 445 EIN Early Intervention Level 3 2.55% 2.")
163 5.00% 4.50% 4.00% 3.50% 3.00% 2.50% 2.00% 1.50% 1.00% 0.50% 0.00% 12.00% 10.00% 8.00% 6.00% 4.00% 2.00% 2.56% 2.44% 1.43% 1.3% 1.3% 1.2% 445 Corporate Level COM Community Services Level 3 Short Term/Long Term Sickness % (Rolling 12 Months) 445 EIN Early Intervention Level % 2.1% 445 INP Inpatient Services Level 3 ST% LT% 2.56% 2.38% 2.36% 1.5% 1.7% 1.6% 445 MED Medical Level 3 Sickness Absence Comparison by Staff Group 445 UCA Urgent Care & Access Level Dudley and Walsall Mental Health Partnership NHS Trust Long term sickness accounts for 60% of sickness for the rolling 12 month period to August The number of open Long Term sickness cases is 18 in Month 5. The top 3 reasons for sickness based on FTE days lost for Month 5 were: 1. Anxiety/Stress Gastro problems Injury, Fracture % Add Prof Scientific and Technic Additional Clinical Services Administrative and Clerical Allied Health Professionals Estates and Ancillary Medical and Dental Nursing and Midwifery Registered DWMH Jul % 5.29% 1.89% 9.74% 7.34% 2.53% 4.71% 4.02% Aug % 5.07% 2.02% 5.29% 4.33% 0.43% 4.27% 3.35% 9

164 100.0% Appraisal % v Trust Target 90.0% 80.0% 73.7% 80.0% 79.1% 77.6% 79.4% 86.0% 87.0% 85.5% 83.5% 82.9% 84.8% 87.9% 70.0% 60.0% 50.0% Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Target Appraisal % Service Appraisals Required 445 CAF Corporate Affairs Level CDP Corporate Development and People Level CDS Clinical Development Level CHX Chief Executive Level FIN Finance Level HR Human Resources Level OPS Operations Level MED Medical Level AOMGT Acute & Older Adults Management Level COM Community Services Level EIN Early Intervention Level INP Inpatient Services Level UCA Urgent Care & Access Level Dudley and Walsall Mental Health Partnership NHS Trust 911 Jul-17 Aug % 100.0% 100.0% 100.0% 100.0% 81.3% 100.0% 100.0% 91.9% 91.4% 94.1% 94.4% 85.5% 81.4% 83.7% 87.0% 52.4% 91.3% 92.7% 93.5% 80.7% 87.7% 79.9% 86.3% 86.3% 84.7% 84.8% 87.9% +/- Appraisal compliance is tracking at 87.9% at the end of August This is above the Trust target There are 110 employees in the Trust that haven't had an appraisal recorded on ESR in the last 12 months. 10
165 445 Dudley and Walsall Mental Health Partnership NHS Trust Aug-17 Training Compliance Jul-17 Aug-17 Competence Target Completed Required % +/- Completed Required % +/- Mandatory Training k 90% % % Mandatory Training Jul-17 Aug-17 Competence Target Completed Required % +/- Completed Required % +/- Equality, Diversity and Human Rights 90% % % Fire Safety 90% % % Health and Safety 90% % % Infection Control (Clinical) 90% % % Infection Control (Non Clinical) 90% % % Information Governance 95% % % Moving and Handling (Foundation) 90% % % Moving and Handling (Patient Handling) 90% % % Safeguarding Adults Level 1 90% % % Safeguarding Adults Level 2 90% % % Safeguarding Children Level 1 90% % % Safeguarding Children Level 2 90% % % 11
166 Board meeting date: 5 October 2017 Agenda Item number: 7.2 Enclosure: 18 Report Title: Medical Directors Report Accountable Director: Author (name & title): Dr Gingell and Dr Weaver, Joint Medical Directors Dr Gingell and Dr Weaver, Joint Medical Directors Purpose of the report: To update the Board on matters pertaining to the joint medical directors portfolio that are of relevance and interest to the Board. This will include, but is not limited to, strategic implications of national and regulatory guidance and publications, together with local matters including risk and governance issues. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Items in this report potentially and variously cut across all of the CQC domains. Enc 18 Joint Medical Directors Report Page 1 of 6
167 Title Medical Directors Report National and Regulatory guidance There is no new national or regulatory guidance this month to bring to the attention of Board Recent Publications and Hot Topics World suicide prevention day World Suicide Prevention Day (WSPD) is an awareness day observed on the 10 th September every year since The International Association for Suicide Prevention (IASP), collaborates with the World Health Organization (WHO) and the World Federation for Mental Health, to host World Suicide Prevention Day in order to support and promote a worldwide commitment and action to prevent suicides, with various activities in countries around the world. Every year more than 800,000 people die by suicide and up to 25 times as many make a suicide attempt. There is an annual theme which this year was take a minute, change a life which highlights the importance of connecting with those within communities who are vulnerable and socially isolated. The focus was to encourage people to identify those who may be struggling, to offer to talk listen and offer words of support. The 13 th Annual Black Country Suicide Prevention Symposium took place on the 8 th September and included a range of speakers and was well attended. A film was shown I jumped from the golden gate bridge and survived which describes the turmoil which can drive serious suicide attempts but also the importance of effective and timely intervention. The brief film has been circulated to Board members. RCPsych Recruitment Campaign In last month s MD report the current challenges in recruitment to psychiatry were highlighted, with the highest number of unfilled medical training posts being in the specialty. This has generated a need to focus on retention of staff and improving career pathways. This month the Royal College of Psychiatrists has launched a recruitment campaign #Choose Psychiatry. This is a six week campaign aimed to increase entry into the specialty. Central to this largely social media focused campaign is what is described as an empowering video which shows how working in psychiatry makes a difference and is a challenging and varied career. The key messages of the campaign are: With more psychiatrists needed in the NHS it s a perfect time to choose psychiatry as the career can offer diversity, work-life balance and broad opportunities As a psychiatrist, you will get to really know a patient, sometimes better than friends and family You treat the whole person, addressing their physical and mental health needs Enc 18 Joint Medical Directors Report Page 2 of 6
168 Every day presents different challenges, calling on your medical expertise and problemsolving skills In a recent NHS survey, the top three trusts where medical staff in training felt personally satisfied with the quality of work and care they delivered were from the mental health sector When you treat someone with a complex mental illness, such as perinatal psychosis you re helping them, their family, their friends and society the ripple effect is immense Psychiatry saves lives It is a job for the clinically curious who are fascinated by human behaviour. It is hoped the campaign will reach sixth formers, medical students and foundation doctors. ( Local Matters Recruitment of Locums We continue to experience difficulties with recruitment of agency locums which remains on our risk register. Although the vacancies are relatively few in number several locums whom we have initially identified through the agencies we currently use have been delaying acceptance of short term appointments in our Trust and have been trying to negotiate above capped rates. The impact of the gaps in medical cover has not been experienced in our out of hours cover but has resulted in some clinic cancellations in both localities which we are keeping under review. We are scoping the full impact of this in terms of delays in routine or follow up appointments. We have also been looking at alternatives to agency locum cover using our existing substantive and Trust locum staff. There has been no impact on new referrals and urgent assessments. TMS Board members will be aware of our Transcranial Magnetic Stimulation pilot project which began at the end of August. Some members of our executive and non-executive team have visited the clinic. The report which will evaluate the pilot project is due to be submitted at the end of October although we are looking if possible to extend the pilot period. Interest in the service locally has been positive with more referrals coming in than available treatment slots. Amongst those who have been receiving the treatment there have been initially encouraging responses although the outcome data has to be fully evaluated. There has also been some interest received in relation to providing the treatment on a privately commissioned basis though this will not be considered as part of the pilot. Currently, through the pilot project at this stage we have been the only NHS organisation in the Midlands to offer the treatment, although it is available in private clinics. Enc 18 Joint Medical Directors Report Page 3 of 6
169 Mortality Report Mortality Data for August 2017 There are 13 cases applicable for inclusion within this month s figures which are outlined within the table below. Information in respect to these cases has been collected from the Safeguard Reporting system and the Informatics and Performance Department. The information from each electronic system complements the other and through cross referencing within other clinical information on OASIS, information from the coroner s office and information from partner agencies, are aligned via the agreement of the Trusts mortality review group with one of the 13 following definitions: Natural deaths - ones from a recognisably incurable condition. Expected death - one where prognostic features have been identified leading to a reasonable expectation of death within an identified timescale Unexpected death - one occurs at a time that is sooner than may reasonably have been predicted from a non-natural cause or where the cause in unknown Preventable death - one that should not have occurred given current medical knowledge and technology 4 of the deaths falling under the scope of this report were identified as being a serious incident, however one of these is being transferred to services in Wolverhampton for investigation. There are 13 cases falling inside the scope of this report and can be summarised as follows: Age Team Diagnosis Summary DWMH Definition 59 Home Treatment (Dudley) Delusional disorder Telephone call received at 1610hrs from ex-husband of above patient. Ex-husband reported that above patient had been found dead at approximately 0930hrs. Ex-husband stated that no suspicious circumstances had been identified at this time. CoD:- 1a) Faecal Peritonitis, 1b) Stercoral Colonic Perforation, Natural Death 54 CRS Walsall North Paranoid schizophrenia 1c) Marked Faecal Loading Staff Member went to deliver medication in the morning however there was no answer at the door. She attempted another visit around 4pm to deliver medication but again no answer. Staff member called the office and informed me that there was no answer. Concerns that the kitchen door was not opened and neighbours had not seen patient either. Agreed to request a safe and well check from the police. Paramedics and Fire service arrived at property. They forced entry into the property and they found patients deceased body in bed. Paramedics confirmed time of death as 17.32pm. No information for next of kin was available. CoD:- 1a) Left Ventricular Hypertrophy, 1b) Hypertensive Heart Disease, Hypertension, 2) Chronic Kidney Disease, Diabetes Mellitus Natural Death Enc 18 Joint Medical Directors Report Page 4 of 6
170 Age Team Diagnosis Summary DWMH Definition 35 Medical outpatients Mixed Anxiety And Depressive Disorder received from Coroners on 02/08/2017, to advise that patient had been found deceased at home, following a potential drug overdose. Full packet of tablets found next to patient. Patient was diagnosed with mixed anxiety and depression, and also mental & behavioral problems associated with the use of alcohol. Patient was engaging with CRI, Atlantic House. Unexpected death Patient came into services in November 2016 via EAS, and was referred to Home Treatment. Patients main presenting problems were alcohol dependence, and an ongoing court case with her children. Patient was discharged in December 2016, and was happy with the discharge plan. Patient was then seen in A&E in March 2017, following an overdose, due to the ongoing stress she had trying to gain access to her children. Following this, patient agreed to be admitted to Kinver Ward. Patient was discharged from the ward, and remained under our Home Treatment Team until she was discharged in April Incident being investigated as Serious Incident 2017/ CoD Awaiting cause of death. However, toxicology results confirmed that JL was positive for alcohol, cocaine and benzodiazepines, 60 EAS Walsall Not Given Call received from a member of family reporting that the patient had died on July 27th at WMH and would therefore not be able to attend his appointment with Walsall EAS. Patient believed to have died from natural causes - cardiac related. According to Fusion patient died from physical health related issues. No further information provided from family member and call was terminated CoD:- 1a) Extensive Malignancy of unknown Primary 2) Severe Left Ventricular end-systolic Dimension (LVSD), Atrial Fibrillation, Ischemic heart 57 Primary Care Team Dudley Not Given disease received from Coroners on 15/08/17, to advise that patient had taken his own life in the family home. Natural Death Unexpected Death Patient was diagnosed with Mixed Anxiety and Depression in 2008, and was under services until No further contact until 28th July Patient was screened by EAS, and was offered a routine Outpatients appointment on 18th September In the meantime, patient accessed our Dudley Talking Therapies Service on 2nd August Psychiatric liaison Dudley Not Given Being investigated as Serious Incident 2017/ received from Coroners on 15/08/2017, to advise that patient had taken their own life at their home address Unexpected death The Trust has had one contact recorded for this patient, whereby he was seen in A&E by PLT on 8th April 2017, following an episode of self harm. 43 Home Treatment Walsall Not Given The Trust initially logged this as serious incident 2017/20470, however are in the process of transferring this to Walsall services. Call into home treatment from home treatment staff nurse who was out doing his daily visits. He informed us that when he arrived at the patient s home he was informed that the patient has been found dead that morning. Unexpected death 85 CMHTOP Dudley Dementia in Alzheimer disease with late onset Patient was under home treat and zoned Green. He had received a medical review on the 16th August by home treatment Doctor. At time of report cause unknown. However evidence of possible O/D. Incident has therefore been logged as a serious incident 2017/21147 Client passed away on 4 August 2017 at Russell Hall Hospital CoD:- 1a) Sepsis syndrome 1b) UTI 1c) Recurrent UTI 2) Dementia, Hypertension, Hypercholesterolemia, Thalamic infarct, Previous spontaneous intracerebral hemorrhage and Acute kidney injury. Natural Death Enc 18 Joint Medical Directors Report Page 5 of 6
 Hospital acquired pneumonia 1b) COPD, Advanced dementia 11)")
171 Age Team Diagnosis Summary DWMH Definition 84 CMHTOP Walsall Vascular dementia of acute onset Telephone call from patients who informed service user had passed away that morning whilst an inpatient at Walsall Manor Hospital Natural Death 92 CMHTOP Walsall 94 Memory Service Walsall Vascular dementia of acute onset Not Given CoD:- 1a) Hospital acquired pneumonia 1b) COPD, Advanced dementia 11) Fracture neck of femur, atrial fibrillatrion, gout, cerebrovascular disease, left ventricular systolic dysfunction Fusion identified death 20/08/2017 from sepsis CoD:- 1a) Sepsis b) Bronchopneumonia 2) Atrial fibrillation, Vascular dementia Patient.referred for a memory assessment. Part assessment carried out and patient referred for a CT scan. On checking Fusion, Walsall Manor Hospital's pt's records system, it was noted that scanning appointment had been cancelled. Rang MRI imaging (Rhianne) who informed me that they had a call from patients son who notified them that she had died. Call made to GP surgery to confirm patient died. Natural Death Unknown 77 CMHTOP Walsall Schizophrenia No cause of death ascertained at this moment in time Telephone enquiry from west midlands police). Who asked mhas if we had any next of kin details as regards the patient who was said to be deceased. Police were informed on a need to know basis that no next of kin details were available on oasis. Unknown 83 CMHTOP Walsall Unspecified dementia No cause of death ascertained at this moment in time Team became aware that the patient died following fall and admission to Walsall Manor Hospital. No cause of death ascertained at this moment in time, query stroke? Unknown Recommendation The Board is asked to accept the Medical Directors report for information and discussion. Board Action Required To receive the report. Enc 18 Joint Medical Directors Report Page 6 of 6
172 Board meeting date: 5 October 2017 Agenda Item number: 7.3 Enclosure: 19 Report Title: Director of Nursing Report Accountable Director: Author (name & title): Rosie Musson Acting Director of Nursing Rosie Musson Acting Director of Nursing Purpose of the report: To update the Board on matters pertaining to the Director of Nursing portfolio that are of relevance and interest to the Board. This will include, but is not limited to, strategic implications of national and regulatory guidance and publications, together with local matters including risk and governance issues. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources x The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: The report relates to all domains and supports the Trust in the delivery of the CQC Fundamental Standards of Care Enc 19 DoNs Board Briefing Paper Public - Oct 17 Pag
173 Title Director of Nursing Report Smoke Free Mental Health nurses are leading work to ensure that we improve our understanding of the inequalities and biases people with mental health conditions face if they want to give up smoking and assess where good practice is taking place to learn from each other. This is crucial if we are to narrow the gaps and have an impact on premature deaths. Eight mental health trusts are now working together on a number of improvement initiatives to improve their compliance with the NICE Guidance on smoking cessation. Leading Change Adding Value: Smoking in Mental Health Programme Around 15.5% of adults in England smoke. However, inequality remains and smoking prevalence is 40.5% in adults with a serious mental illness and can be up to 70% among patients in psychiatric units. This equates to one in three of all cigarettes smoked are smoked by people with a mental health condition. The Trust will be attending a conference led by the Mental Health and Learning Disability Director of Nursing Forum to learn from others to support the Trust going smoke free. This will be delivered in the context of the Trust recovery model. Introduction of Safe Care Acuity tool for inpatient services A pilot is near completion across the adult inpatient wards to trial an acuity tool (recommended through National Guidance). The tool is used at census points in the day to measure patient acuity. The pilot is being evaluated and has received positive feedback. It is hoped that this will be rolled out subject to pilot feedback in November The information from the acuity tool will be used to inform clinical decision making regarding daily staffing levels, but also be used to inform workforce planning and future establishment reviews and monitoring the impact of raised acuity. The process is supported by Allocate Safe Care software and will be supported through nurses using technology on the wards to compile the data. Acuity tools for older adult wards will also soon be piloted. Trip to the Netherlands Three nurses and the Trust Acting Professional Lead for Occupational Therapy have visited the Netherlands this month to learn about their model of delivery of mental health services. The visit followed the Trust s Clinical Development Director visiting the Netherlands two years ago as part of the HOPE European Health Exchange programme and last year some of their staff visiting the Trust to see how street triage operates. As a result of the visit they are now piloting street triage in the Netherlands. Enc 19 DoNs Board Briefing Paper Public - Oct 17 Pag
174 Trust staff who have just returned will be sharing their experience at various forums including at Board next month and agreeing with the Trust what they can take forward to implement. Revalidation Support continues to be provided by the Trust to enable nurses to revalidate. All nurses required to revalidate have successfully achieved this during the last year. Recommendation The Board is asked to receive the update from the Director of Nursing portfolio for assurance. Board Action Required As recommended. Enc 19 DoNs Board Briefing Paper Public - Oct 17 Pag
175 Board meeting date: 5 October 2017 Report Title: Accountable Director: Author (name & title): Purpose of the report: Agenda Item number: 7.4 Enclosure: 20 Quality Improvement Priorities and CQUIN Q1 Update Report 2017/18 Rosie Musson Acting Director of Nursing Rupert Davies Interim Director of Finance, Performance and IM&T Olive Hewitt Clinical Quality Improvement Manager The purpose of presenting this report to the Trust Board is to provide a quarterly update on: Progress against Trust Quality Improvement Priorities 2017/18 by exception Progress against CQUINs by exception Where appropriate recommend risks to the Finance and Performance Committee in terms of delivery of CQUINs Identify risks to delivery and mitigations Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report Quality and Safety Committee Key points or recommendations from Committee or Group: The Quality and Safety Committee received the Quarter 1 Quality and Improvement priorities and CQUINS report. The following areas were discussed and noted by the Committee.. CQUIN- Improving physical healthcare to reduce mortality in people with severe mental illness- This CQUIN was rated as amber in Q1 due to physical health care pathways being inconsistent across the Trust and completeness of the cardio metabolic risk factors recording. The committee discussed mitigations and areas for further action. The Committee noted the work that was ongoing to increase performance including increased checks for assurance. CQUIN- Improving health and wellbeing of NHS staff- this CQUIN was rated as amber in Q1 due to potential capacity of peer vaccinators to be released from substantive posts. Mitigations have been put in place to assist with this; details are outlined further in this report. Quality Improvement Priority Ensuring organisational learning is embedded and sustained - this is rated as amber/green due to difficulties operationalising an electronic system for managing recommendations and learning. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 1 of 22
176 Quality Impact Assessment Domain Patient Safety Patient Experience Comment Both CQUINS and Quality Improvement priorities impact on all domains of the CREWS model as they aim to demonstrate continuous quality improvement. Clinical Effectiveness / Outcomes Workforce Experience Efficiency & Productivity Continuous Improvement in the Quality of Care The CQC domains that this report relates to are: Caring Responsive Please give brief details: Both CQUINS and Quality Improvement priorities impact on all CQC domains as they aim to demonstrate continuous quality improvement. Effective Well-led Safe Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 2 of 22
177 Title Quality Improvement Priorities and CQUIN Q1 Update Report 2017/18 Introduction The purpose of this report to Trust Board is to provide a quarterly update by exception on: progress against Trust Quality Improvement Priorities 2017/18 progress against CQUINs 2017/18 identified risks and mitigations to delivery The Trust continues to implement the Quality Improvement Strategy and promote a culture of ongoing quality improvement throughout the services delivered. To ensure the quality priorities and CQUINs are mapped into the Trusts quality governance framework, a full quarterly update is provided to Trust Board, detailing progress and an overview of outcomes and exceptions. Where risks to delivery have been identified risk mitigations have been put in place. This report provides Trust Board with an overview of progress in Q1 and also provides assurance on the ongoing delivery of the Trusts Quality Improvement Strategy. Executive Summary of key points, issues, financial impact and risks All Priorities and CQUINs have made progress in Q1. Where risks have been identified to the delivery the project leads have put in mitigation plans. Table 1 and Table 2 provide an overall project risk score for the end of Q1. CQUIN- Improving physical healthcare to reduce mortality in people with severe mental illness The physical health CQUIN remains a risk for the Trust in terms of sufficient achievement against the requirements of the audit for cardio metabolic risk factor recording. In addition the milestones for patient pathways for interventions are inconsistent across the Trusts localities, are not easy to navigate and require further work to clarify and align with a changing health economy. For example, public health no longer has the same level of resource in smoking cessation. CQUIN- Improving health and wellbeing of NHS staff Part 1C of the health and wellbeing for staff CQUIN did not reach the required target of 75% uptake of flu vaccinations by frontline staff during 16/17. This year Providers are to evidence to commissioners that up to 70% of front line clinical staff have received the flu vaccine. The Trust is working closely with Transforming Care Together partners (TCT), have developed an implementation plan and meet as a flu planning group on a monthly basis. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 3 of 22
178 Further detail Information All quarterly updates for CQUINs and Quality Improvement Priorities are presented to the Quality and Safety Committee. In addition, the Clinical Audit and Effectiveness Committee provide an exception report to Quality and Safety Committee on a monthly basis for discussion and assurance. Quality Impact Both the CQUINS and Quality Improvement priorities impact on all domains of the CREWS model as they aim to demonstrate continuous quality improvement. Financial Impact A risk remains to the identified CQUINs outlined in this paper of failing to achieve the full requirements of the CQUINS and where completion is achieved there is a possibility that this may be at a lower level of compliance therefore full payment may not achieved. Legal Comment None Risk Assessment Risks surround failure to achieve full requirements of CQUIN milestones. Where risks to delivery have been identified risk mitigations have been put in place. Recommendation Trust Board to note the progress made in relation to the 2017/18 Quality Improvement Priorities and CQUINs and note the reported exceptions. Board Action Required Trust Board to note the progress made in relation to the 2017/18 Quality Improvement Priorities and CQUINs and note the reported exceptions. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 4 of 22


179 CQUIN & Quality Improvement Overview 2017/18 Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 5 of 22
180 1. Overall Project Risk This section provides an overview report of CQUINs and Quality Improvement Priorities. All projects have made progress and where risks to project delivery have been escalated project managers are putting in place risk mitigations plans. Table 1: Overall Project Risk Score (CQUINs) CQUIN Exception Project RAG rating Improving physical healthcare to reduce premature mortality in people with serious mental illness (PSMI) Improving staff health and wellbeing Improving services for people with mental health needs who present to A&E Preventing ill health by risky behaviours alcohol and tobacco Transitions out of Children and Young People s Mental Health Services (CYPMHS) Current pathways for interventions and signposting for all cardio-metabolic risk factors are inconsistent across the Trust. Total Value Risk remains in respect to low completion rates for cardio metabolic form. 285,329 Flu part 1C, potential risk of peer vaccinator s constraint s in terms of capacity to be released from substantive post. However two bank workers are currently being trained as peer vaccinators. 285,329 None None Joint report on current state of transition planning has commenced. 285, ,329 The implementation plan based of level of need is in development. 285,329 Table 2: Overall Project Risk Score (Quality Improvement Priorities) Quality Improvement Priority Person centred care planning/care planning Improving the quality of record keeping Ensuring organisational learning is embedded and sustained Becoming smoke free Refocus/recovery model Exception Project RAG rating Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 6 of 22
181 CQUIN 1: Improving physical healthcare to reduce premature mortality in people with serious mental illness (PSMI) Description of Indicator Indicator 3a) Cardio metabolic assessment and treatment for patients with psychoses. Indicator 3b) Collaboration with primary care clinicians. Year 1 (17/18) To demonstrate cardio metabolic assessment and treatment for patients with psychoses in the following areas: a) Inpatient wards. b) All community based mental health services for people with mental illness (patients on CPA), excluding EIP services. c) Early intervention in psychosis (EIP) services. Year 2 (18/19) To demonstrate positive outcomes in relation to BMI and smoking cessation for patients in early intervention in psychosis (EIP) services. Rationale for Inclusion People with severe mental illness (SMI) are at increased risk of poor physical health, and their lifeexpectancy is reduced by an average of years mainly due to preventable physical illness. Two thirds of these deaths are from avoidable physical illnesses including heart disease and cancer, mainly caused by smoking. There is also a lack of access to physical healthcare for people with mental health problems less than a third of people with schizophrenia in hospital receive the recommended assessment of cardiovascular risk in the previous 12 months. People with SMI are three times more likely to attend A&E with an urgent physical health need and almost five times more likely to be admitted as an emergency, suggesting deficiencies in the primary physical healthcare they are receiving. Project Milestones 2017/18 Mar 18 Feb 18 Jan 18 Dec 17 Nov 17 Oct 17 Sept 17 Aug 17 July 17 June 17 May 17 April 17 3a - Ensure sustainable and high quality training programme in place for all relevant clinical staff caring for people with SMI. 3a - Ensure clear pathways for interventions and signposting for all cardio-metabolic risk factors. 3a -.Ensure the electronic care record system has been developed and is being used effectively for collection of physical health assessment and interventions data. 3b Identify and develop clear plans for aligning and cross checking SMI QOF and CPA registers. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 7 of 22
182 3b Establish a clear shared protocol between secondary care provider and primary care regarding physical health checks for people with SMI and appropriate follow ups. Audit to be undertaken by provider 3a Results of national audit across inpatient and community mental health services and of EIP self-assessment scheme published. 3b Results of local audit to be reported to local commissioners. Progress Update Risks Identified Mitigation The Trust continues to enhance and strengthen training work undertaken in 2016/17 CQUIN. A review of current training needs is being undertaken to ensure all elements of physical care aspects are incorporated and not just the elements outlined by the CQUIN. Whilst there are patient pathways for interventions, these are inconsistent across the Trust, are not easy to navigate and require further work to clarify and align with a changing health economy. For example, public health no longer has the same level of resource in smoking cessation. The cardio-metabolic form is in the electronic records on Oasis for community teams and paper copies for inpatients. Overall Project Risk: Amber Inconsistent pathways across the Trust Low completion rates Internal /sub milestones have been formulated to address local actions required. Guidance and Communication sent out to all staff identifying what is required including roles and responsibility Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 8 of 22
183 CQUIN 2: Improving staff health and wellbeing Description of Indicator Indicator 1a) Improvement of health and wellbeing of NHS staff. Indicator 1b) Healthy food for NHS staff, visitors and patients. Indicator 1c) Improving the uptake of flu vaccinations for front line staff within providers. Rationale for Inclusion The Health & Wellbeing CQUIN introduced in 2016 encourages providers to improve their role as an employer in looking after employee s health and wellbeing. Part of this scheme provided the option to introduce schemes focussing on mental health, physical activity and MSK many of which are being introduced during the second half of The focus of this element of the CQUIN will shift from the introduction of schemes to measuring the impact that staff perceive from the changes via improvements to the health and wellbeing questions within the NHS staff survey. Estimates from Public Health England put the cost to the NHS of staff absence due to poor health at 2.4bn a year around 1 in every 40 of the total budget. This figure excludes the cost of agency staff to fill in gaps, as well as the cost of treatment. As well as the economic benefits that could be achieved, evidence from the staff survey and elsewhere shows that improving staff health and wellbeing will lead to higher staff engagement, better staff retention and better clinical outcomes for patients. The Five Year Forward View made a commitment to ensure the NHS as an employer sets a national example in the support it offers its own staff to stay healthy. A key part of improving health and wellbeing for staff is giving them the opportunity to access schemes and initiatives that promote physical activity, provide them with mental health support and rapid access to physiotherapy where required. The role of board and clinical leadership in creating an environment where health and wellbeing of staff is actively promoted and encouraged. Project Milestones 2017/18 Mar 18 Feb 18 Jan 18 Dec 17 Nov 17 Oct 17 Sept 17 Aug 17 July 17 June 17 May 17 April 17 Provider to evidence to commissioners a 5% increase in the answer Yes, definitely for Staff Survey questions 9a-9c. Provide evidence to commissioners showing that a substantive change has been made in shifting toward healthier products. Providers should also evidence to commissioners that they have maintained changes from 16/17 by providing at least the following evidence: A signed document between the NHS Trust and any external food supplier committing to keeping the changes. Evidence for improvements provided to a public facing board meeting. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 9 of 22
184 Provider to evidence to commissioners that up to 70% of front line clinical staff have received the flu vaccine. Progress Update Risks Identified Mitigation 1a Staff Survey results currently being worked through using service line breakdown reports to assess particular local/service line issues. None None required Service lines are in the process of drawing up action plans, which include addressing staff Health & Wellbeing issues. 1b There is no advertising of high SSF products throughout all catering area s within the Trust. To continue to promote healthier eating across the Trust. None None required 80% of confectionary does not exceed 250Kcal. To continue to reduce the amount of high sugared confectionary throughout vending and catering area s Promote healthy eating at all sites by providing healthy nutritional food 1c Provider to evidence to commissioners that up to 70% of front line clinical staff have received the flu vaccine. 1. Working in partnership with TCT Partners 2. TCT Flu planning Group set up in May 2017 and meets monthly see enclosed implementation plan 3. Incentives paper to be agreed with all TCT partners 4. Flu vaccines ordered with OH 5. Dates of clinics being agreed Peer Vaccinator volunteers, training to be agreed Overall Project Risk: Amber Peer vaccinators not released from substantive post Incentives may not be agreed across partnership 2 Bank workers also being trained as Peer vaccinators DWMH agreed through MEXT to continue with local Incentive approach CQUIN 3: Improving services for people with mental health problems who present to A&E Description of Indicator Year 1 (17/18) Reduce by 20% the number of attendances to A&E for those within a selected cohort of frequent attenders who would benefit from mental health and psychosocial interventions, and establish improved services to ensure this reduction is sustainable. Year 2 (18/19) Sustain the reduction in year 1 of attendances to A&E for those within the selected cohort of frequent attenders who would benefit from mental health and psychosocial interventions. Reduce total number of attendances to A&E by 10% for all people with primary mental health needs. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 10 of 22
185 Rationale for Inclusion People with mental ill health are 3 times more likely to present to A&E than the general population. More than 1 million presentations are currently recorded as being directly related to mental ill health. People with known mental ill health are 5 times more likely to be admitted to acute hospitals and 80% of these emergency admissions are recorded as being primarily for physical health reasons. This highlights the need for acute hospitals to be equipped to detect and treat urgent mental health needs that are cited as the primary reason for presentation as well as improving identification of underlying mental health conditions where the primary presenting reason may be a physical health one. The Quality Watch study also found that people with mental ill health had 3.6 times more potentially preventable emergency admissions than those without mental ill health in 2013/14, and that the high levels of emergency care use by people with mental ill health indicate that they are not having their care well managed and suggest that there are opportunities for planned care (inside and outside of the hospital) to do more. These people are well known to the healthcare system and are having many health encounters Project Milestones 2017/18 Mar 18 Feb 18 Jan 18 Dec 17 Nov 17 Oct 17 Sept 17 Aug 17 July 17 June 17 May 17 April 17 MH trust and acute trust to review most frequent A&E attenders who have attended times or more within the last 12 months. Identify subset of attenders who would benefit from assessment, review and care planning with MH staff. Identified subset of attenders to be recorded and set as baseline. MH trust and acute trust to assure commissioners that further work has been undertaken with partners (111, ambulance service, police substance misuse, primary care etc) to identify whether identified cohort also presenting frequently at other UEC system touch points. MH trust and acute trust to identify whether the presentation of the identified cohort were coded appropriately in A&E HES dataset. Conduct internal audit of A&E mental health coding and agree joint data quality improvement plan and arrangements for regular data sharing r.e. people attending A&E. MH trust and acute trust to establish joint governance arrangements to review progress against CQUIN and associated service development plans. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 11 of 22
186 MH trust and acute trust to work with other partners to ensure that: Care plans in place for each patient in the identified cohort of frequent attenders. System is in place to identify new frequent attenders and ensure care plans are put in place swiftly. Care plans are shared with other system partners (with patients permission) MH trust, acute trust to bring in partners, agree service development plan to support a sustained reduction in A&E frequent attendees by people with MH needs. MH trust, acute trust to review progress against data quality improvement plan and confirm that systems are in place to ensure that coding of MH need via A&E HES data submissions is complete and accurate. MH trust and acute trusts to assure CCG that a robust system for coding primary and secondary mental health needs is in place. 20% reduction in A&E attendances of those within the selected cohort of 2016/17 frequent attenders. Progress Update Risks Identified Mitigation There has been strong engagement from all parties, with joint meetings taking place throughout quarter 1 with both Dudley Group of Hospitals NHS FT, and Walsall Healthcare. That patients from the agreed cohort refuse to engage Personalised care plans and communications As per CQUIN requirements a cohort of patients for both Dudley and Walsall has been agreed. A joint letter has been sent from the Trust and Dudley Group of Hospitals NHS FT to DCCG outlining the progress against quarter 1 milestones and requesting approval for the proposed approach. The approach in Walsall is very much the same as in Dudley; however the CCG quality lead was present at the initial meeting in Walsall, who was satisfied with the approach and therefore removed the need of formal communication. Overall Project Risk: Green That A&E attendances do not decrease for the agreed cohort Process for newly identified patients to be added to the cohort Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 12 of 22
187 CQUIN 4: Preventing ill health by risky behaviours alcohol and tobacco Description of Indicator Indicator 9a) Percentage of unique adult patients who are screened for smoking status AND whose results are recorded. Indicator 9b) Percentage of unique patients who smoke AND are given very brief advice. Indicator 9c) Percentage of unique patients who are smokers AND are offered referral to stop smoking services AND offered stop smoking medication. Indicator 9d) Percentage of unique adult patients who are screened for drinking risk levels AND whose results are recorded in local data systems. Indicator 9e) Percentage of unique patients who drink alcohol above lower-risk levels AND are given brief advice OR offered a specialist referral. Rationale for Inclusion Context This CQUIN seeks to help deliver on the objectives set out in the Five Year Forward View (5YFV), particularly around the need for a radical upgrade in prevention and to incentivising and supporting healthier behaviour. The proposal also supports delivery against the FYFV efficiency target by generating a projected national net cost-saving to the NHS over the course of the CQUIN. The burden of smoking Smoking is estimated to cost 13.8bn to society ( 2bn on the NHS through hospital admissions, 7.5bn through lost productivity, 1.1bn in social care). Smoking is England s biggest killer, causing nearly 80,000 premature deaths a year and a heavy toll of illness, 33% of tobacco is consumed by people with mental health problems. Smoking is the single largest cause of health inequalities A Cochrane Review shows that smoking cessation interventions are effective for hospitalised patients regardless of admitting diagnosis. Inpatient smoking cessation leads to a reduced rate of wound infections, improved wound healing and increased rate of bone healing. Permanent smoking cessation reduces the risk of heart disease, stroke, cancer and premature death. The quit rates among patients who want to quit and take up a referral to stop smoking services are between 15% and 20%, compared to 3% to 4% amongst those without a referral. The burden of excessive alcohol consumption In England, 25% of the adult population (33% of men and 16% of women) consume alcohol at levels above the UK CMOs lower-risk guideline and increase their risk of alcohol-related ill health. Alcohol misuse contributes (wholly or partially) to 60 health conditions leading to hospital admission, due either to acute alcohol intoxication or to the toxic effect of alcohol misuse over time. Conditions include cardiovascular conditions, liver disease, cancers, depression and accidental injuries. There are nearly 22,500 alcohol-attributable deaths per year. Out of c3.7m admissions, c333,000 were admissions where an alcohol-related disease, injury or condition was the primary diagnosis or there was an alcohol-related external cause. These alcohol-related admissions are 32% higher than in 2004/05. Alcohol is estimated to cost the public purse 21bn per annum, of which 3.5bn are costs to the NHS. Around three quarters of the 3.5bn cost to the NHS is incurred by people who are not alcohol dependent, but whose alcohol misuse causes ill health this is the group for which IBA is the most effective. Identification and Brief Advice (IBA) results in recipients reducing their weekly drinking by c12%. Because alcohol health risk is dose dependent, reducing regular consumption by any amount reduces the risk of ill health. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 13 of 22
188 Project Milestones 2017/18 Mar 18 Feb 18 Jan 18 Dec 17 Nov 17 Oct 17 Sept 17 Aug 17 July 17 June 17 May 17 April 17 Complete information systems audit which sets out: Proposed mechanisms for collecting required data. Changes to data capturing arrangements. Approach for conducting quarterly case note audits. Complete brief advice training for relevant staff, including: Who will deliver training? Who will receive training? Contents of training. Review of training. Schedule of training. Collect relevant data to establish baseline for all indicators. Audit of new admissions Audit of new admissions Audit of new admissions Progress Update Risks Identified Mitigation Data Capturing mechanisms for collecting the data for this CQUIN have been identified and will be utilising a combination paper records and electronic. None None required Contacts have been made within Public Health England CQUIN representatives to establish the audit tool content All front line ward staff will require brief advice and intervention training Training will be delivered electronically via a PowerPoint presentation with an assessment and evaluation to be completed Baseline data continues to be gathered and stored on a Trust developed spreadsheet in preparation for inputting onto the strategic data collection portal Overall Project Risk: Green Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 14 of 22
189 CQUIN 5: Transitions out of Children and Young People s Mental Health Services (CYPMHS) Description of Indicator This CQUIN aims to incentivise improvements to the experience and outcomes for young people as they transition out of Children and Young People s Mental Health Services (CYPMHS). This CQUIN is constructed so as to encourage greater collaboration between providers spanning the care pathway. There are three components of this CQUIN: 1. a case note audit in order to assess the extent of Joint-Agency Transition Planning; and 2. a survey of young people s transition experiences ahead of the point of transition (Pre- Transition / Discharge Readiness); and 3. a survey of young people s transition experiences after the point of transition (Post-Transition Experience). This CQUIN does not prescribe the wording for surveys, nor does it require a particular method for taking this information such as online or telephone surveying. This is to be agreed at a local level and as appropriate for the young person, and signed off by the receiving service, commissioners, and young people. CCGs must be satisfied that the questionnaire wording and methods provide adequate evidence of young people s preparedness for, and experience of, transition. Rationale for Inclusion This CQUIN is intended to improve the outcomes for young people who transition out of CYPMHS; to improve young people s experience of transition; to improve young people, parent and carer involvement; and to incentivise the safe transfer of care for young people. The point of transition from CYPMHS is recognised as a point of potential upheaval for young people who may find it difficult to navigate new service settings, or to manage their mental health following discharge from CYPMHS, especially as the availability and offer of support can change dramatically from CYPMHS to AMHS, or voluntary sector services. Project Milestones 2017/18 Mar 18 Feb 18 Jan 18 Dec 17 Nov 17 Oct 17 Sept 17 Aug 17 July 17 June 17 May 17 April 17 Sending and receiving providers to jointly develop engagement plan across all local providers. Sending and receiving providers to map the current state of transition planning/level of need and to submit joint report on findings to commissioners. Sending and receiving providers to develop implementation plan to address identified needs and agree with approach with commissioners. Sending and receiving providers to update and assure commissioners as to implementation of joint plan to support better transition planning Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 15 of 22
190 Sending provider to undertake casenote audit assessing those who transitioned out of CYMPHS from Q4. Sending provider to undertake assessment of discharge questionnaires for those who transitioned out of CYPMHS in Q4. Receiving provider to undertake assessment of post-transition questionnaires of those who transitioned to AMHS from CYPMHS through Q4. Sending and receiving providers to present to commissioners a joint report outlining overall CQUIN progress to date. Results to be submitted to NHS England via Unify2 Collection. Progress Update Risks Identified Mitigation Project group established representation from nursing, medical, CRS, CRHT and CAMHS. Joint engagement plan formulated with sending and receiving providers. Draft needs/gap analysis completed to inform implementation plan. Waiting on responses from partners (CRS). Part 3 (implementation plan) of Quarter 1 milestone currently under draft development and collaborative working with Black Country Partnership to share best practice. Overall Project Risk: Green Implementation plan not fully developed Draft implementation plan is under development Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 16 of 22
191 Quality Priority 1: Improvement initiatives & Evaluation Rational & Objectives Project lead Project team Smoke Free (continued from 2016/17) Smoking is the largest single preventable cause of morbidity. People with mental health problems smoke significantly more, with levels of about three times those observed in the general public. The Trust is committed to supporting individuals to stop smoking whilst received NHS Care as this is seen as a significant opportunity to support individuals and reduce smoking. The Trust recognises that by prioritising smoking cessation it will be supporting people with mental health problems who are at greater risk of poor physical health get access to prevention and screening programmes. As part of this, NHS England and Public Health England should support all mental health inpatient units and facilities (for adults and children and young people) to be smoke-free by Rosie Musson, Interim Director of Nursing Olive Hewitt, Clinical Quality Improvement Manager Helena Allport, Quality Improvement Facilitator Project Milestones Timeline April 17 May 17 Jun 17 July 17 Aug 17 Sept 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18 A business case including was costings to be presented to the Trust s Management Executive Team Collaborative working with partners to share ideas and best practise Meet with Heads of Service to plan communication of smoke free changes to service users and visitors in preparation for launch Small supply of leaflets and posters to be printed for distribution across community and inpatient sites Quarter One Progress Update Risks Identified Mitigation A business case including was costings have been presented to the Trust s Management Executive Team May Collaborative working continues with partners to share ideas and best practise. Black Country Partnership Foundation Trust smoke free project team meeting attended in June. Posters and leaflets shared along with Smoke free Management Policy and training material Trust pharmacists working collaboratively with counterparts at BCPFT to develop a joint formulary of approved products for use across the Black Country health economy for smoking cessation. Overall Project Risk: Green None None required Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 17 of 22
192 Quality Priority 2: Improvement initiatives & Evaluation Rational & Objectives Project lead Project team Person Centered Care / Care Planning People who use mental health services should have the opportunity to make informed decisions about their care and treatment, in partnership with their health and social care practitioners. Putting person centered values into practice means that you are providing care that is focused on the individual. It demonstrates to the individual that you want to care for and support their recovery. The CQC report and internal monitoring show that whist progress continues to be made further work is required to improve the quality and consistency of person centered care planning. Kelly Plant, Inpatient Manager Vicky Gibbons, EAS Manager Rachael Payne, Clinical Lead, ECMHTOA Norma Ellis, CPN, Dudley CRS North Project Milestones Timeline April 17 May 17 Jun 17 July 17 Aug 17 Sept 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18 Trust Supportive Visits and feedback Targeted training Re-audit external to the ward managers/deputies Quarter One Progress Update Risks Identified Mitigation During Quarter one the person centred care planning action has remained a feature on all wards for their individual CQC plans, whereby they are producing their own self-assessment and assurance actions for progression. The Trust has undertaken supportive visits across all wards, which was an independent review and scrutiny of the embedding of the My Careplan document and each lead has feedback a detailed report to the ward managers. Targeted training for staff has been made available and led by 2 ward managers across the acute wards. MHA CQC visit has taken place at Bloxwich hospital that has evidenced robust person centred care plans. Further work is being planned to look at a training resource as part of nurse development. Overall Project Risk: Green None None required Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 18 of 22
193 Quality Priority 3: Improvement initiatives & Evaluation Rational & Objectives Project lead Project team Improving the quality of our record keeping Through feedback from the CQC, internal clinical audits and feedback from service users it has been identified that improvements need to be made to the quality of record keeping to enable greater consistency. The Trust currently has a mix of electronic and paper records, which creates challenges to consistency, however as the trust moves towards an electronic single patient record further work is required to ensure the quality of record keeping is maintained and improved. Kelly Plant - Inpatient Manager Debbie Gall Home Treatment Manager Dr Ahmad/Deputy Rachael Payne, Clinical Lead, ECMHTOA Norma Ellis, CPN, Dudley CRS North Project Milestones Timeline April 17 May 17 Jun 17 July 17 Aug 17 Sept 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18 Re-issuing of guidance to staff re historical risks Clear guidance to be given to managers and included in ward audit activity Trust supportive visits Review and guidance of standards to be examined for electronic recording of review dates when no changes are required Revised guidance to be delivered to all staff Quarter One Progress Update Risks Identified Mitigation This QIP focuses on risk assessments in relation to record keeping. All ward staff are completing electronic risk assessments on the inpatient wards. Training has been delivered and managers/deputies monitor these through their regular documentation audits. This also formed part of the Trust supportive visit process. Guidance to be reviewed and sent out again to all ward areas. Standards of how often electronic risk assessments are to be updated to be reviewed to ensure the document evidences regular reviews Overall Project Risk: Amber/Green Further issues have been identified with some staff not pulling through all historical risks to enable accurate formulation of current risk assessments. Inpatient HOS has discussed at the SLM with managers to raise awareness with staff to address this. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 19 of 22
194 Quality Priority 4: Ensure organisational learning is embedded and sustained Improvement initiatives & Evaluation Rational & Objectives Project lead Project team Ensure organisational learning is embedded and sustained Learning is identified through complaints, claims, audit and third party inspections. If learning is embedded in practice and sustained over time, the likelihood of repeated incidents and other events which can cause harm are reduced. Through feedback from the CQC Inspection and internal quality governance processes it has been identified further work is required to improve embedding lessons process to ensure effective triangulation of information, monitoring of actions taken and ensuring improvements are embedded in practice. Margaret Barnsley, Serious Incident Co-ordinator Tom Jinks, Compliance and Safety Manager, Dave Miles, Quality Improvement Facilitator Debbie Cooper, Vulnerable Adults and Children s Lead/Acting Head of Inpatient Services Project Milestones Timeline April 17 May 17 Jun 17 July 17 Aug 17 Sept 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18 Updates made to Embedding Lessons and Triangulation To R and a full review of group membership undertaken. Design a central database for logging actions from the work streams within the group. Produce quarterly Lessons Learnt Bulletin. Develop a SharePoint network so that actions database can be centrally accessed. Create and Embedding Lessons and Triangulation reporting template which can be shared with committees. Develop assurance programme for stress testing actions. Produce quarterly Lessons Learnt Bulletin Establish a schedule for attending medic meetings to share learnings with front line staff. Identify Lessons Learnt Champions for each service line Develop content and present at the Patient Safety Roadshows. Carry out assurance testing for evidence of completed actions. Review and evaluate group ToR and membership. Carry out assurance testing for evidence of completed actions. Produce annual summary for actions and lessons learnt. Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 20 of 22
195 Quarter One Progress Update Risks Identified Mitigation New Terms of Reference have been published and membership reviewed to gain wider medical involvement. Process flowchart has been developed alongside the ToR to demonstrate group s vision and reporting structures to members. To appropriately triangulate actions and learning. None Ensure attendance from all members is as regular as possible None required Database for collating actions from different work streams has been developed. Agreement of use of SharePoint to be discussed and finalised in meeting 23 rd August. Overall Project Risk: Amber/Green Amendments are required to ensure that it is suitable for all group members. Amendments are required for access to SharePoint. Agreement reached that SED will continue to use their current reporting structures to log actions. Ensure that members are still using the shared drive for saving files before SharePoint is operational. Quality Goal 5: Improvement initiatives & Evaluation Rational & Objectives Project lead Project team Refocus / Recovery Model Recovery is a concept that recognises people can be in control of their lives despite mental health problems, and can regain a meaningful life despite a mental illness. Refocus is a specific approach to recovery that works with both individual and team attitudes towards recovery practices. Peter Hayward, Consultant Occupational Therapist Steve Byng, Clinical Lead for Care Cluster & Tariff Development Project Milestones Timeline April 17 May 17 Jun 17 July 17 Aug 17 Sept 17 Oct 17 Nov 17 Dec 17 Jan 18 Feb 18 Mar 18 1st Round of Refocus training TRIP self-assessment. Team assessment of current Recovery Practises Training for Wrekin staff in use of DWROM TRIP Service user assessment 2nd Refocus event Facilitated team and Individual assessment of recovery attitudes and Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 21 of 22
196 practices (Sep) Wrekin staff will conduct pilot of use with DWROM on selected service users DWROM version specifically for OA to be developed 3rd Refocus event Skills training in Refocus coaching method DWROM implemented fully to assessment and care planning in Wrekin 4th Refocus team self-assessment TRIP team assessment post Refocus events DWROM Pilot on OA ward to be arranged TRIP service user assessment post Refocus training. Quarter One Progress Update Risks Identified Mitigation Refocus -The first round of Refocus training took place on June 9th in conjunction with BSMHPT. 30 people from DWMH attended, including EBEs. Speaker was Mike Slade from Nottingham University TRIP The three pilot teams for the 2nd round of Refocus training have completed the Team Recovery Implementation plan (TRIP). This has been completed as a pre Refocus training assessment of team functioning with respect to Recovery. DWROM Adult Occupational Therapy and Head of Clinical Service Development have provided training on the use of the DWROM to all staff on Wrekin in June. The team are currently piloting the service user portion with new users of the service. Staff are also asking for feedback from service users regarding how they find the experience of using the DWROM as an assessment. Overall Project Risk: Green None None required Enc 20 Trust BoardQ1 CQUIN and QIP (3) Page 22 of 22
197 Board meeting date: 5 October 2017 Agenda Item number: 7.5 Enclosure: 21 Report Title: Enhancing Quality through Safer Staffing Levels Monthly Exception Report Accountable Director: Author (name & title): Purpose of the report: Rosie Musson Acting Director of Nursing Rosie Musson Acting Director of Nursing Makhan Singh Principal Consultant, Informatics and Performance This report provides the Trust Committee with: A summary report of planned and actual staffing for August 2017, which has been submitted to NHS Choices as part of a national staffing return and is available on the Trust s website. Exception reporting for variances and any concerns relating to safer staffing Trend analysis monthly average fill rate Bank and agency actual hours analysis against substantive hours Number of qualified staff per shift Action required from the Committee Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Workforce Committee Date reviewed: 25 th September 2017 Any points will be reported through the Workforce Chair s Report Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources Enc 21TB Safer Staffing Oct 2017 Page 1 of 14
198 Quality Impact Assessment Domain Patient Safety Comment Ensuring safer staffing in inpatient services. Patient Experience Clinical Effectiveness / Outcomes Workforce Experience Efficiency & Productivity Continuous Improvement in the Quality of Care The CQC domains that this report relates to are: Caring Responsive Effective Efficient use of staffing resource to deliver quality care. Please give brief details: Ensuring staffing levels are responsive to meeting patient need Well-led Safe Ensuring staffing levels are adequate to deliver safe care Enc 21TB Safer Staffing Oct 2017 Page 2 of 14
199 Title Enhancing Quality through Safer Staffing Levels - Monthly Exception Report Introduction This report provides the Trust Board with: A summary report of planned and actual staffing which has been submitted to NHS Choices as part of a national staffing return and is available on the Trust s website. Exception reporting for variances and any concerns relating to safer staffing. Trend analysis monthly average fill rate. Bank and agency actual hours analysis against substantive hours. Data relating to trust standard of minimum of two registered RMNs on duty by shift. Update on the integration of safer staffing data into the Trusts integrated dashboard. Summary of key points, issues and risks The Data represents August 2017 and a monthly trend analysis for a 12 month period. Across the inpatient areas the overall fill rates are %, with 96.92% for registered staff and % for care staff. This indicates the Trust is meeting the optimum level of fill rates. Typically where our care staff rates exceed 100%, this is due to temporary staff being used to support patient observations, increases in acuity or changes in skill mix. Ward managers and Clinical Leads are empowered to be responsive and flex staffing to meet patient acuity. There is one ward to note as exceptions, whereby staff fill in part is within the lower category (Kinver). An impact assessment has been completed that provides assurance safe staffing levels have not been compromised. Where staff have concerns about staffing levels the reporting takes place through the Trusts incident reporting processes. In August there was 2 incident reported related to safer staffing in inpatient services. As reported in last month s report this information is collected manually however, from September the data will be automated and linked to the electronic rostering system. The Trust has in place a locally agreed standard of the minimum of 2 qualified members of staff per shift. Due to inpatient vacancies the Director of Nursing and has sought further assurance that when the ward plans to drop below this standard, mitigations are in place to maintain patient safety. Assurance has been provided that full consideration is given to skill mix when using temporary staff especially on night shifts when this has resulted in with one qualified member of staff being on duty with back up from the night coordinator as a qualified senior nurse and experienced HCAs. Enc 21TB Safer Staffing Oct 2017 Page 3 of 14
200 Update on Actions being taken and timelines The following actions are being taken to ensure temporary staffing is used effectively and efficiently Vacancy review has been completed for inpatients; the Trust faces challenges in relation to the recruitment of Band 5 nurses and has a proactive recruitment campaign in place. Recent recruitment drives have been successful with new staff starting the end of September. Vacancy levels require ongoing monitoring. Optimising recruitment processes for bank staff a successful initial drive. Now a rolling programme supported by coms campaign. Implementation of best practice rostering metrics ward managers are working with rostering manager to maximize the efficiency of their rostering. Revised process for sign off of rosters through new inpatient manager allowing early detection of inefficiencies or concerns. Safer staffing report is being reviewed with TCT partners to enhance triangulation or metrics provide improved assurance to Trust Board. Revised format to be presented to Workforce Committee in October. Recommendation 1. To note and discuss the monthly data return submitted providing details of planned and actual staffing at ward level. 2. To note the work underway to enable to most efficient safe and effective use of nurse staffing in inpatient service, this will focus on all professional groups, including therapists. 3. To Note and discuss the data relating to internal Trust standard of two qualified staff per shift and to discuss and receive assurance on mitigations in place. Board action required As recommended. Enc 21TB Safer Staffing Oct 2017 Page 4 of 14
201 1. Nursing and healthcare staffing fill rates August 2017 The data submission was made on 12 th September 2017 of August data. The following table provides a summary of the planned verses actual staffing levels on the inpatient wards. Ward Return Aug-17 5ay Night 5ay Night RMN Care Staff RMN Care Staff Average fill rate - registered Planned Actual Planned Actual Planned Actual Planned Actual nurses/midwives (%) Average fill rate - care staff (%) Average fill rate - registered nurses/midwives (%) Average fill rate - care staff (%) Cedars % % % 97.92% Linden % % % % Ambleside % % % % Langdale % % 94.05% % Clent % % % % Kinver % % 74.64% % Wrekin % % 99.87% % Holyrood , , , , % % % 99.83% Malvern % % % % Grand Total % % 95.22% % Lowest range less than 80% Highest range greater than 150% Low range greater than 80% but less than 90% High range greater than 120% but less than 150% Greater than 90% but less than 120% Comments Across the inpatient areas the overall fill rates are %, with 96.92% for registered staff and % for care staff. This demonstrates an optimum range of fill rate for qualified and care staff for the demand (number of staff identified as required by the ward to meet patient acuity). Where our care staff rates exceed 100% on Wrekin Ward, this is due to Enc 21TB Safer Staffing Oct 2017 Page 5 of 14
202 temporary staff being used to support patient observations, increases in acuity or changes in skill mix. Ward managers and Clinical Leads are empowered to be responsive and flex staffing to meet patient acuity. 2. Exception Report on Variance August 2017 Exceptions Rationale Impact Remedial Actions Kinver Ward Bushey Fields Hospital 74.64% Night Average fill rate Registered Nursing (Low range) The deficit relates to non-availability of bank/agency RMN cover. HCA was used instead of a planned second trained on the night shift. On each occasion mitigations were put in place to maintain safety. Safe staffing levels maintained, no reported incidents Incidents reported through safer staffing escalation process. There were two incidents reported in August In both instances patient safety was not compromised. Continue recruitment to vacancies. Review on monthly basis. Incident Number Date of Incident Location/ service area Incident Summary (taken from report submitted) /08/2017 Kinver Incident Type: Staffing Insufficient Levels Incident: An agency staff member was booked as second qualified, but did not attend for their shift. This was filled with a HCA leaving only one qualified /08/2017 Wrekin Incident Type: Staffing Insufficient Levels Incident: Staffing levels at night on Wrekin Ward had been increased from 3 to 4 due to a patient with complex needs being transferred from Malvern Ward. A member of staff had to be re-deployed by the senior Actions/Outcome / Assurance Outcome: There was no negative impact or noted risk on patient care or incidents reported. Action: As the shift could not be covered with a qualified staff member a HCA filled the shift. Assurance: There was a total of 5 staff on shift which was more than required. Outcome: There was no negative impact or noted risk on patient care or incidents reported. Action: The re-deployed staff member was later returned to Wrekin Ward. Assurance: Support given by Senior Nurse and the re-deployed staff member was returned to Wrekin Ward Enc 21TB Safer Staffing Oct 2017 Page 6 of 14

203 Incident Number Date of Incident Location/ service area Incident Summary (taken from report submitted) nurse to support another ward. Wrekin also received a new admission during the evening. Actions/Outcome / Assurance 3. Trend Analysis average fill rate The following table shows a monthly trend of the total average fill rates planned verses actual for the Trust. This demonstrates that staffing levels are flexed to meet the increases and decreases in patient acuity, which is currently informed by clinical expertise. Enc 21TB Safer Staffing Oct 2017 Page 7 of 14

204 4. Registered Nurse Hours Substantive Against Temporary Staff fill rates The below table shows percentage of hours from April 2016 split by bank hours, agency hours and substantive hours for all registered nurses. Further work is being undertaken to enable this data to be triangulated and ensure we are utilising temporary staffing in the most effective and efficient way. Enc 21TB Safer Staffing Oct 2017 Page 8 of 14

205 5. Registered Nurse Hours Substantive Against Temporary Staff Fill Rate The below table shows percentage of Registered Nurse Hours Substantive V s Temp Staff Fill Rate for individual wards. Further work is being undertaken to enable this data to be triangulated and ensure we are utilising temporary staffing in the most effective and efficient way. Vacancy rates and sickness are impacting on fill rates alongside, increased patient acuity requiring increased observations. Enc 21TB Safer Staffing Oct 2017 Page 9 of 14

206 6. Care Staff Nurse Hours Substantive against Temporary Staff fill rates The below table shows percentage of hours from April 2016 to August 2017 split by bank hours, agency hours and substantive hours for all care staff. Vacancy levels and increased patient acuity requiring high level observations are impacting on use of temporary staff. There is a slight increase in use of agency staff, this was due to late requests due to changes in staff availability. Enc 21TB Safer Staffing Oct 2017 Page 10 of 14

207 7. Care Staff Nurse Hours Substantive Against Temporary Staff fill rates Further analysis of registered nurse hours by ward for August month is presented in the below table.vacancy levels and increased patient acuity requiring high level observations are impacting on use of temporary staff. During August there was a high level of additional staffing demand due to patient acuity. Enc 21TB Safer Staffing Oct 2017 Page 11 of 14
, with 96.")
208 8. Minimum of two qualified nurses per shift Standard The Trust has an internal standard, where there is a minimum of two qualified nurses per shift. The information sourced from HealthRoster shows that in August 2017 across the inpatient areas the overall day and night compliance rates are 77.3% (previous month 79.63%), with 96.06% (previous month 97.96%) for day shifts and 39.78% (previous month 42.96%) for night shifts. Vacancies continue to impact on the ability to have two RMNs on a night duty; however recruitment continues to occur to fill the vacancies. The Head of Service has reported that new starters are likely to impact from October. Sickness rates have also impacted on Holyrood and Wrekin during this reporting time. Enc 21TB Safer Staffing Oct 2017 Page 12 of 14

209 The below table shows the August 2017 Day shift compliance rate by ward: Where compliance falls below 100%, this is predominantly around short notice sickness. Where there are shortfalls, this is managed by support from the supernumerary Ward Managers, Band 6 who are on supervisory days or bleep holders. Enc 21TB Safer Staffing Oct 2017 Page 13 of 14
210 The below table shows the August 2017 Night shift compliance rate by ward: There is significant variance on the compliance. It is evident that the impact of vacancies and team skill base is leading to one qualified member of staff being rostered into the numbers for nights on wards, however assurance provided by the Head of Service and Ward Managers is that their preference to maintain a safe environment and continuity of care is to utilise experiences HCA staff in some instances. The Head of Service is working with Ward Managers to improve consistency. Enc 21TB Safer Staffing Oct 2017 Page 14 of 14
211 Board meeting date: 5 October 2017 Agenda Item number: 7.6 Enclosure: 22 Report Title: Director of Operations Report Accountable Director: Author (name & title): Purpose of the report: Lesley Writtle, Interim Director of Operations Lesley Writtle, Interim Director of Operations James Parker, Commissioner Liaison Manager To update the Trust Board on key issues pertaining to service delivery in the directorate of operations. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: None Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Please give brief details: Service delivery issues relate to all aspects of the CQC domains. Safe Enc 22 Director of Operations Report October v2 Pag
212 Title Director of Operations Report Introduction The report for the Directorate of Operations aims to update the Board on pertinent issues and challenges relating to operational service delivery. Summary of key points, issues and risks Urgent and Access: Early Access Service (EAS) Mental Health Assessment Service Crisis Resolution teams Psychiatric Liaison and Urgent Care Street Triage Section 136 Suites Early Intervention: Child and Adolescent MH Services, including i- CAMHS Eating Disorder services Regional Deaf CAMHS service Primary MH Services, including IAPT Early Intervention in Psychosis teams Community: Community Recovery Services Employment Services Psychological Therapies Hub Community MH Teams for Older People Older People Day Services Dudley Memory Assessment Service Walsall Carers Service TALCS Inpatients: All Inpatient Services (4 wards for Older People, 5 wards for working age Adults) Home Treatment Services Bed Management 1) Early Intervention Services IAPT: Mental Health Strategies (MHS) have now completed their review of both the Walsall and the Dudley IAPT services and have presented their report to the Trust. The following summarises their main findings: What we re achieving with the resources we ve got is comparable with the national picture. There are a number of data quality issues which include issues such as the electronic system being used Neither service has enough staff to meet the national targets. Insufficient training places available to develop our staff. Primary care mental health needs a clear service specification following the IAPT split The report has been shared with the Trust s commissioners and a mini summit took place on 25th September to jointly action plan. NHS England and the report author were present, Enc 22 Director of Operations Report October v2 Pag

213 it was a productive meeting and a first draft action plan will be in place in the middle of October CAMHS: The services have commenced the CYPIAPT project and have a full list of staff waiting to start training courses in October. Backfill is covered via the CAMHS Transformation Plan funding held by the local CCG s. CAMHS: Both Dudley and Walsall teams, held open days during September. Both days were particularly successful with local stakeholders, members of the public and the Mayors from Dudley and Walsall in attendance. 2) Community Services Section 75 The Director of Operations has met with the new project lead responsible for the dissolution of the section 75 agreement. This was a positive meeting with the project lead understanding the need to maintain strong partnership post separation. Timescales are awaited, a joint plan will be developed and led in partnership. This will be presented to the Board and Council Jointly. Dudley Older People Transformation - A 30 Day Public consultation hosted by Dudley CCG commenced on Monday 19 th June for the proposed redesign of Older People Mental Health services. The proposed changes were presented to the Health Oversight Scrutiny Committee in July, resulting in a request for further information from the CCG. This therefore is likely to delay the plans by at least a further month. Once the plans are approved it is expected the transformation will take up to 6 months. 3) Inpatient Services Bed Pressures: In August, the Trust overall bed occupancy including home leave decreased to 80.2% compared to the previous month (80.8%). However Older Adult Inpatient Services have seen a slight increase from 63.9% to 64.2%. Enc 22 Director of Operations Report October v2 Pag
214 Delayed Transfer of Care: As per the chart below, we have seen a steady increase in the number of Delayed Transfer of Care episodes since the start of the year. The services have been working very closely with the local commissioners, and it is expected that the current position will decrease in September. This portrays an accurate picture which is driven by strong process and monitoring Recommendation The Board is asked to note the updates within operation services. Board Action Required To receive the report. Enc 22 Director of Operations Report October v2 Pag
215 Trust Board Meeting: 5 October 2017 Agenda Item number: 7.7 Enclosure: 23 Report Title: High Level Operational Risk Register Accountable Director: Author (name & title): Rosie Musson (Acting Director of Nursing) Neil Tong (Patient Safety Facilitator) Purpose of the report: The purpose of this report is to provide the Trust Board with the Red Risks for the period ending 26 September 2017 and in doing so provides the committee with information on: o Any new red risks being escalated to the High Level Operational Risk Register o Any red risks being downgraded from the High Level Operational Risk Register. o Any updates to red risks currently held on the Trust High Level Operational Risk Register. Action required from the Committee Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: The detail within this report was reviewed by: Quality and Safety Committee Finance and Performance Committee Workforce Committee Date reviewed: 13/09/2017 Quality and Safety Committee 25/09/2017 Finance and Performance Committee 25/09/2017 Workforce Committee The risks enclosed within this risk register were approved by Quality and Safety Committee with a number of risks referred to Finance and Performance Committee, Mental Health Act Scrutiny Committee and Workforce Committee in line with the requirements of the Trusts risk management strategy. Enc 23 High Level Operational Risk Register Page 1 of 15
216 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Some of the risks held on the register have the ability to directly or indirectly impact upon the care/services offered The Trust Wide Risk Register Provides a representation of the Trusts Red Risks and the responses to managing/action planning these risks; some (due to the nature of the risk) provide a response to a short term or long term issue Some of the risks held on the Trust Wide Risk Register impact upon the future viability / effectiveness of the Trusts operations. Risk FINAN 1 specifically relates to the long term outlook in relation to CIP Some risks held on operational risk registers Pertain to issues around service redesign and may have impacts upon leadership and staffing issues The appropriate management of risk is central to the provision of a quality, safe service. In particular CQC Outcome 16 Assessing and monitoring the quality of service provision Enc 23 High Level Operational Risk Register Page 2 of 15
217 Title High Level Operational Risk Register Introduction It is the purpose of this report is to provide the Trust Board with the Red Operational risks held across the Trusts Risk Registers (for the period 28 th June 2017) and in doing so provides Trust Board with information on: Any new red risks being escalated to the High Level Operational Risk Register. Any red risks being downgraded from the High Level Operational Risk Register Any updates to red risks currently held on the High Level Operational Risk Register. There are currently 10 risks being presented as part of this report. This is being done in line with the Trusts risk management strategy and further details of these are included within table 1.1. The revised TCT Operational Risk register following the Board Development Session on 18 September 2017 is presented in full with the latest update report from the TCT Integration Board in Private Session. Summary of key points, issues and risks There are 10 risks included within this report which are applicable for presentation to the Trust Board. A summary of these risks are detailed within table 1.1. The full details of these risks are articulated in appendix 1 Table 1.1. Summary of risks Risk ID Risk Description Impacts Opaerationally (and updates) FINAN 1 Inability to meet the annual savings targets set for NHS Source Financially driven risk with quality implications. providers. Existing This covers both 'internal' cost improvement requirements and 'external' (QUIPP) requirements. Addition information Issues to note include:- This risk has been updated by the Acting Director of 1) 3-4% efficiency requirement has been in place for a Finance to include information in relation to MCP and number of years, and is likely to continue QIPP requirements 2) The Trust is increasingly reliant upon non-recurrent solutions 3) The Dudley MCP is likely to require similar levels of savings in the future 4) The Trust has exhausted the potential for 'transactional' solutions, but is finding 'transformative' solutions difficult to implement 5) CIP proposals tend to be 'top/down, rather than developed by individual services. HR 002 Reduction in Local Authority Funding for Mental Health Social Care Workforce. This has the potential to impact on service delivery and on the viability of the S75 agreements and has the potential to place operational pressures on clinical teams and operational viability of some services Source Risk to quality of service driven by a reduction in local authority funding. Existing risk already reported to Quality and Safety Committee Addition information Risk has been updated to include impact on service provision and additional required actions Enc 23 High Level Operational Risk Register Page 3 of 15 Status of risk = =
218 Risk ID Risk Description Impacts Opaerationally (and updates) 314 The Trust effectively operates two sets of clinical records - paper-based in wards and electronic in the community. This may lead to an inconsistent approach being taken to clinical risk management, having implications upon continuity of patient care planning and risk management Source Major project already enacted by the Trust to replace existing clinical system. CQC assessment highlighted that interface between electronic and paper system is a clinical risk and as such interim measures are being put in place to mitigate the risk along with long term measures (the replacement of OASIS) Status of risk = Furthermore, the decision as to which product is to be procured has been delayed as a result of TCT. The delay reflects an eventual desire to implement a single agreed solution across the TCT trust 315 An inconsistent approach is being taken to the management of clinical risk management and care plan development was identified by the CQC. This is likely to have implications upon continuity of patient care planning and risk management. 320 The Trust has a lack of clearly defined processes and policies in respect to the use of personal alarms, the provision of call alarms which allied to an additional need for personal safety training for staff has the ability to impact upon the health and safety of both staff and patients, especially when staff are working on their own. 322 The Trusts assessment by the CQC noted that there may be a lack of evidence to support that calls within the Trusts Crisis team are responded to in a timely manner Addition information / update Risk reviewed and updated by Acting Director of Finance and Performance. Risk description now better reflects current risk facing the Trust. Risk scored as 5x4 = 20 Whilst an IT solution will help there was however some discussion that an IT solution is not the cure all for the issues that have been picked up through the CQC inspection about our medical record keeping, so we should still be actioning what we can to strengthen our record keeping within the constraints of our existing systems. Source CQC visit highlighted that this is a recurrent issue Addition information Trust has purchased a license agreement for writing person centered care plans. The standards are supported by the CCA and NHS improvement. Trust supportive visits have noted that whilst the updating of risk assessments on OASIS has improved, there are still issues within inpatient areas of care plans not being patient centered. Source The Trusts CQC visit highlighted this as a risk to the Trust. Addition information Supportive visits noted that there are still issues with alarm protocols within certain inpatient areas, review of community areas is still ongoing. Source The Trusts CQC visit highlighted this as a risk to the Trust. Addition information As noted a new crisis call log has been established and a standard for incident reporting has been agreed Whilst no incident forms have been entered in relation to this issue since the CQC visit, there is at this stage audit results to indicate the number of calls which are being returned and the average response time for these. Audit has been completed and has been presented to Clinical Audit and Effectiveness Committee. A decision needs to be made in respect to any risks highlighted by the audit. = = = Enc 23 High Level Operational Risk Register Page 4 of 15
219 Risk ID Risk Description Impacts Opaerationally (and updates) 323 Failure of the Trust to achieve its mandatory and essential Source CQC highlighted that this was a risk to the training may result in staff not being appropriately skilled to Trust undertake their role and impact upon the Trust meeting Risk reviewed by Quality and Safety Committee. It was compliance with CQC standards and impact upon the noted that due to further work being required in relation quality of patient care to this (as identified by the Trusts November 2016 CQC visit and its associated action plan) it was felt that this risk should be upgraded to a red risk. This decision was further approved by the Trusts workforce committee and a decision was made to rescore the risk as a red risk. The Trust is currently compliant with its Mandatory Training target however this needs to be sustained for a number of months EF002 Fire Safety Management within the Trust and lack of assurances in respect to certain arrangement regarding fire safety 289 Changes to the local interagency 136 policy may leave to Trust open to reputational risks around its implementation. It is noted that only one doctors was required for a Section 12 and an AMHP. Should an instance arise where a second doctor was required they would be called. There were also noted issues documented as part of the Trusts November 2016 CQC Visit. Namely in relation processes around the safe operation of the Trusts 136 suites 379 Shortage of National Junior psychiatric trainees from August's rotation may impact on patient care due to reduced workforce capacity before this risk can be downgraded Source Gap analysis of assurances undertaken within estates. Issue escalated via Estates Risk Register Addition information Fire safety working group has now been convened and is meeting on a weekly basis to address the identified issues. Source Following discussion at the Trusts MHASC in light of the findings of the November 2016 CQC visit it was noted that this risk should be escalated to the status of a red risk. Addition information Following discussion at Quality and Safety it was felt that this risk should be referred to MHASC for review and further re-scoping Addition information / update Risk added following discussion at Trust Board and Quality and Safety Committee Status of risk = = = = Further detail (if required) Further details of the risks are outlined in appendix 1 Recommendation It is recommended that the Trust Board approve the enclosed copy of the High Level Operational Risk Register. Action required To approve the risks included within this report and note the action taken to date in managing these. Enc 23 High Level Operational Risk Register Page 5 of 15
220 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts F INAN 1 Inab ility to m ee t the annua l sav ings ta rge ts se t fo r NHS p rov ide rs. T h is cove rs bo th 'in te rna l' cos t im p r ove m e n t requ ire m en ts and 'ex te rna l' (Q U IP P ) requ ire m e n ts. Issues to no te inc lude :- 1) ) 3-4 % e ffic iency requ ire m en t has been in p lace fo r a nu m be r o f yea rs, and is like ly to con tinue 2) ) The T rus t is inc reas ing ly re lian t upon non -recu rren t s o lu tions 3) ) The D ud ley M CP is like ly to requ ire s im ila r leve ls o f sav ings in the fu tu re 4) ) The T rus t has exhausted the po ten tia l fo r 'tr ansac tiona l' so lu tions, bu t is fin d ing 'tr ans f o r m a ti v e ' so lu tions d ifficu lt to im p le m en t 5) ) C IP p roposa ls tend to be 'top /do w n, ra the r than deve loped by ind iv idua l se rv ices. F inance P ro jec tions / D a t a 28 /02 /2011 M a rk A xce ll Rupert Davies 5 4 R ed 20 D e ta iled deve lop m en t o f cos t im p rove m en t p rog ra m m e Investm en t in a C IP P M O p ro jec t t e a m 2016 /17 in te rna l aud it rev ie w o f the ope ra tion o f the then C IP P rog ra m m e B oa rd - T rus t im p le m en ted its reco m m enda tions rega rd ing te rm s o f re fe rence and m ode o f ope ra tion. E s tab lished C IP P rog ra m m e B oa rd (no w expanded re m it to cove r g ro w th - C IG P rog ra m m e B oa rd Q ua lity Im pac t A ssess m en ts ca rried ou t on a ll cos t im p rove m en t p ro jec ts A c tive in -yea r m on ito ring fac ilita tes inc reased sc ru tiny w he re C IP s a re n ot be ing im p le m en ted o r de live red o r w he re a lte rna tive m itiga tions requ ire deve lo p m e n t. 5 3 R ed 15 Q IA s shou ld be co m p le ted and s igned o ff be fo re the co m m ence m en t o f the financ ia l yea r to w h ich the C IP re la tes. B oa rd, M e X T, F&P, and C IP p rog ra m m e B oa rd a ll requ ired to focus upon sche m es no t de live ring /de layed de live ry. P rocesses shou ld be im p le m en ted so tha t C IP sche m es a re deve loped 'loca lly ' ra the r than im posed upon se rv ice lines by the D irec to r o f F inance as pa rt o f the budge t se tting p rocess A tten tion and m u tua l executive suppo rt shou ld focus upon trans fo rm a tiona l sche m es 5 1 G reen 5 V a rious F inance and P e rfo rm ance repo rts inc lud ing : R epo rts to B oa rd R epo rts to F&P C o m m itt e e inc lud ing ind iv idua l ac tion p lans on p ressure a reas. R epo rts to M EXT R ev ie w s by ex te rna l assessors inc lud ing T D A, HDD and M on ito r In te rna l aud it repo rts a round C IP g iv ing fu rthe r assu rance E x te rna l bench m a rk ing o f p lans 25 /09 /2017 R isk upda ted by A c ting D irec to r o f F inance and P e rfo rm ance. R isk to re m a in a red risk Enc 23 High Level Operational Risk Register Page 6 of 15
221 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts H R 002 R educ tion in Loca l A u tho rity Funding fo r M en ta l H ea lth S oc ia l C a re W o rk fo rce. T h is has the po ten tia l to im pac t on se rv ice de live ry and on the v iab ility o f the S 75 ag ree m en ts and has the po ten tia l to p lace ope ra tiona l p ressures on c lin ica l tea m s and ope ra tiona l v iab ility o f so m e se rv ices Feedback F ro m S takeho lde rs / P 30 /05 /2012 Les l e y W r ittl e Rosie Musson Hassan Omar 4 4 R ed 16 S ec tion 75 ag ree m en ts p rov ide fo rm a l p la tfo rm as the bas is fo r any fu rthe r nego tia tions in fund ing and resou rce changes Jo in t app roach ag reed w ith W a lsa ll M B C rega rd ing im p le m en ta tion o f fund ing reduc tions. R isk A ssess m en ts on loss o f pos ts has been co m p le ted R egu la r d iscuss ions be ing he ld a t P a rtne rsh ip O pe ra tions G roup. A dd itiona l sho rt te rm capac ity has been co m m iss ioned 4 4 R ed 16 D iscuss ions ongo ing a t P O G (M on th ly ) 4 2 A m be r 8 R epo rts to M EXT U pda tes to B oa rd 01 /02 /2017 R isk has been upda ted to inc lude im pac t on se rv ice p rov is ion and add itiona l requ ired ac tions Enc 23 High Level Operational Risk Register Page 7 of 15
222 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 314 The T rus t e ffec tive ly ope ra tes tw o se ts o f c lin ica l reco rds - pape r-based in w a rds and e lec tron ic in the c o m m u n it y. T h is m ay lead to an inconsis ten t app roach be ing taken to c lin ica l risk m anage m en t, hav ing im p lica tions upon con tinu ity o f pa tien t ca re p lann ing and risk m anage m en t F u rthe rm o re, the dec is ion as to w h ich p roduc t is to be p rocu red has been de layed as a resu lt o f T C T. The de lay re flec ts an even tua l des ire to im p le m en t a s ing le ag reed so lu tion ac ross the T C T trus t Feb 2016 CQC V is it 19 /05 /2016 R upe rt D a v i e s IM&T David Crook 4 4 R ed 16 R ev ie w o f risk assessm en t te m p la te has been co m p le ted in line w ith CPA requ ire m en ts to ensu re tha t s ta ff p rac tice is in line w ith bes t p rac tice T ra in ing needs ana lys is has been looked a t ac ross the T rus t to ensu re tha t inpa tien t s ta ff can upda te e lec tron ic risk assessm en ts on O A S I S C onsu lta tion w ith ove r 60 c lin ica l an c lin ica l ad m in s ta ff to deve lop the bus iness case and spec ifica tion fo r the ne w c lin ica l sys te m has been unde rtaken S upp lie rs have sub m itted responses to the Inv ita tion to Tender (ITT ) Inpa tien t a re be ing tra ined to upda te FA C E risk assessm en ts on the O A S IS sys te m, to ensu re tha t co m m un ity s ta ff a re a w a re o f risks w h ich m ay have e m e rged du ring the pa tien ts inpa tien t s tay R e fe rence S ite V is its have occured S ys te m D e m ons tra tions unde rtaken C lin ica l engage m en t is be ing pu rsue ac ross the T C T pa rtne rsh ip (by w ay o f the c lin ica l w o rks trea m s ) w ith a ne w p roposed ro ll-ou t p lanned fo r O c tobe r 2018 d d s5 4 R ed 20 F u ll bus iness case app roved and con trac t s igned R o ll ou t o f ne w c lin ica l sys te m c o m m ences Iden tifica tion o f p re fe rred supp lie r Q ua lity im p rove m en t p rio rity in re la tion to "Im p rov ing the Q ua lity o f reco rd keep ing " and P e rson C en tred C a re P lann ing " to be unde rtaken du ring the 2017 /18 yea r. 4 2 A m be r 8 R epo rts to M E x T R epo rts to IG IM & T co m m ittee 25 /09 /2017 R isk rev ie w ed and upda ted by A c ting D irec to r o f F inance and P e rfo rm ance. R isk descrip tion no w be tte r re flec ts cu rren t risk fac ing the T rus t. R isk sco red as 5x4 = 20 Enc 23 High Level Operational Risk Register Page 8 of 15
223 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 315 A n inconsis ten t app roach is be ing taken to the m anage m en t o f c lin ica l risk m anage m en t and ca re p lan deve lop m en t w as iden tified by the CQC. T h is is like ly to have im p lica tions upon con tinu ity o f pa tien t ca re p lann ing and risk m anage m e n t. Feb 2016 CQC V is it 19 /05 /2016 R ose m a r y M usson Dr Mark Weaver R ed Dr Kate Gingell Patient Safety and Compliance Team Bob Yardley R ev ie w o f risk assessm en t te m p la te has been co m p le ted in line w ith CPA requ ire m en ts T ra in ing needs ana lys is has been looked a t ac ross the T rus t S po t check o f ca re inpa tien t ca re p lans have been unde rtaken O u tco m e o f spo t checks in re la tion to risk assessm en ts has been p resen ted to M HASC s4 4 R ed 16 T a rge ted rev ie w o f eve ry pa tien ts risk assessm en t and m anage m en t p lan w ith in the Inpa tien t and C ris is / H o m e T rea tm en t se rv ice. (A ug 2017 ) A c tion find ings o f ta rge ted rev ie w in to pa tien ts risk assessm en ts (A ug 2016 ) W he re a tra in ing need is iden tified, spec ific suppo rt and ta rge ted ac tions and supe rv is ion im p le m en ted to m on ito r. (A ug 2017 ) T a rge ted rev ie w o f eve ry pa tien ts C a re P lan w ith in the Inpa tien t and C ris is / H o m e T rea tm en t se rv ice (A ug 2017 ) 4 1 G reen 4 R epo rts to M HASC C lin ica l A ud it o u tc o m es 01 /05 /2017 It w as ag reed by Q ua lity and S a fe ty C o m m ittee fo llo w ing a rev ie w as pa rt o f a risk deep d ive, tha t th is risk shou ld re m a in as a red risk to the T rus t. F u rthe r im p le m en ta tion o f M y C a re P lan (O ngo ing ) R egu la r spo t checks o f risk assessm en ts to be co m p le ted (S ep t 2016 and ongong ) Enc 23 High Level Operational Risk Register Page 9 of 15
224 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 320 The T rus t has a lack o f c lea rly de fined p rocesses and po lic ies in respect to the use o f pe rsona l a la rm s, the p rov is ion o f ca ll a la rm s w h ich a llied to an add itiona l need fo r pe rsona l sa fe ty tra in ing fo r s ta ff has the ab ility to im pac t upon the hea lth and sa fe ty o f bo th s ta ff and pa tien ts, especia lly w hen s ta ff a re w o rk ing on the ir o w n. Feb 2016 CQC V is it 19 /05 /2016 R upe rt D a v i e s Phil Clark (Head of Estates) Andrew Foley (Health and Safety Officer) Team Manager Tom Jinks 4 4 R ed 16 C o m m un ica tion has been issued to tea m m anage rs rega rd ing the use o f pe rsona l a la rm s w ith a reques t to deve lop an ind iv idua l loca l p ro toco l. A g ile w o rk ing po licy has been deve loped w h ich h igh ligh ts ro les and responsib ilities in respect to the use o f m ob ile dev ices w hen lone w o rk ing Lone w o rk ing po licy has been re -co m m un ica ted co m m un ica ted to s t a ff. P rov is ion o f ca ll a la rm s a t A ncho r M eado w and pop la rs has been rev ie w ed R ev ie w o f a ll trus t p re m ises to be co m p le ted and assessed aga ins t ag reed s tanda rds fo r a la rm sys te m s (co m p le ted ) A T NA has been co m p le ted in respect to iden tify ing w ha t s ta ff requ ire pe rsona l sa fe ty tra in ing, inc lud ing a rev ie w o f the con ten t o f such tra in ing Funding has been iden tified and tw o ne w sys te m s have been ins ta lled an d tw o sys te m s upg raded, a ll p rocedu re s have been rev ie w ed. R ev ie w has been co m p le ted ac ross the tw o co m m un ity s ites. P e rsona l S a fe ty tra in ing needs a re re flec ted in the T rus ts T NA m a trix. T h is has been rev ie w ed a longs ide M APA tra in ing. R epo rt on M HA and M APA tra in ing co m p liance sub m itted to the M HA S c ru tiny C o m m ittee m ee ting R ed 16 R isk to be tes ted by nex t round o f T rus ts suppo rtive v is its, w ith a focus upon co m m un ity se rv ices (S ep t 2017 ) 4 1 G reen 4 C o m p le tion o f loca l p ro toco ls A ud it resu lts E s ta tes and C ap ita l P lann ing P ape rs 01 /05 /2017 It w as ag reed as pa rt o f a deep d ive in to the T rus ts red risks tha t th is risk shou ld re m a in on as a red risk, bu t shou ld be s tress tes ted as pa rt o f the nex t round o f T rus ts suppo rtive v is its (w ith a focus upon co m m un ity se rv ices ) Enc 23 High Level Operational Risk Register Page 10 of 15
225 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 322 The T rus ts assessm en t by the CQC no ted tha t the re m ay be a lack o f ev idence to suppo rt tha t ca lls w ith in the T rus ts C ris is tea m a re responded to in a tim e ly m anne r Feb 2016 CQC V is it 19 /05 /2016 Les l e y W r ittl e Rosie Musson Crisis team 3 5 R ed 15 A ne w c ris is ca ll log has been deve loped A s tanda rd has been ag reed tha t if a R ed ca ll is no t re tu rned w ith in the hou r an inc iden t fo rm w ill be sub m itted P rocesses have been co m m un ica ted to s ta ff A ud it in to co m p liance has been c o m p le ted C a ll log to be re -aud ited and a risk deep d ive to be p resen ted to Q ua lity and S a fe ty C o m m ittee (A p ril 2017 ) R epo rt in to co m p liance to be p resen ted to C lin ica l A ud it and E ffec tiveness C o m m ittee 3 1 G reen 3 Inc iden t figu res C lin ica l A ud it R esu lt s 03 /04 /2017 A 2nd aud it has been co m m iss ioned in re la tion to assessing the response tim es a round c ris is ca lls. The ins ta lla tion o f a c ris is ca ll log is m en tioned w ith in the T rus ts CQC repo rt (fro m N ov 2016 v is it) as a pos itive s tep. W h ils t the in itia l issue a round a "lack o f log " has been add resse the d w ill need conc lude w he the r the response tim e is app rop ria te. T h is is to be fu rthe r rev ie w ed in ligh t o f the CQC repo rt by the CQC s tee ring g roup. Enc 23 High Level Operational Risk Register Page 11 of 15
226 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 323 F a ilu re o f the T rus t to ach ieve its m anda to ry and essentia l tra in ing m ay resu lt in s ta ff no t be ing app rop ria te ly sk illed to unde rtake the ir ro le and im pac t upon the T rus t m ee ting co m p liance w ith CQC s tanda rds and im pac t upon the qua lity o f pa tien t ca re Feb 2016 CQC V is it 19 /05 /2016 A sh i W illia m s Becky 3 3 Temple-Purcell A m be r 9 R ev ie w o f T ra in ing tra jec to ries and co m p liance leve ls to be co m p le ted fo r bo th m anda to ry and essentia l tra in ing has been co m p le ted P e rsona l S a fe ty T ra in ing and M HA T ra in ing a re no w inc luded as pa rt o f the T rus ts tra in ing ca lenda r P e rsona l S a fe ty tra in ing needs a re re flec ted in the T rus ts T NA m a trix. T h is has been rev ie w ed a longs ide M APA tra in ing. L R P gu idance cove red in recen t tra in ing sess ions de live red has been inco rpo ra ted w ith in M APA tra in ing fo r fu tu re sess ions ensu ring tha t a ll s ta ff tha t jo in the T rus t to w o rk w ith in Inpa tien ts w ill rece ive th is in fo rm a tio n T ra in ing needs ana lys is has been unde rtaken ac ross inpa tien t a reas. R ev ie w o f M HA tra in ing unde rtaken by M HA m anage r and W o rk fo rce D eve lo p m e n t. T ra in ing needs ana lys is has no w been co m p le ted and is be ing rev ie w ed ac ross O lde r A du lts S e rv ic line. C lose w o rk ing be tw een HR /L D and O pe ra tions F a ce to face tra in ing and e -lea rn ing ava ilab le T e lephone book ing sys te m ava ilab le fo r m anda to ry tra in ing W eek ly co m p liance repo rts sen t to M E x T e 4 4 R ed 16 E nsu re tha t co rrec t tra in ing p rov is ion and m e thods fo r essentia l tra in ing requ ire m en ts a re in p lace (Ju ly 2017 ) T ra jec to ries ag reed fo r each se rv ice a rea to m a in ta in a ll yea r round c o m p liance. S ta ff no t co m p lian t w ith 7-8 M T m odu les o be m anaged in accordance w ith the C apab ility P o licy E m a il is be ing sen t to H eads o f S e rv ice fro m CEO s ta ting tha t the ir a reas need to be co m p lian t by end o f Ju ly o the rw ise they w ill need to a ttend W F C to exp la in w hy the ta rge t has no t been ach ieved T o rev ie w and ag ree cu rren t essentia l tra in ing requ ire m en ts fo r s ta ff g roups inc lud ing co m p liance ta rge ts (Ju ly 2017 ) 4 1 G reen 4 T ra in ing repo rts to co m m ittees T ra in ing da ta on ESR 28 /06 /2017 R isk rev ie w ed and fu rthe r ac tions upda ted fo llo w ing d iscuss ion a t W o rk fo rce C o m m itt e e Enc 23 High Level Operational Risk Register Page 12 of 15
227 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts EF002 F ire S a fe ty M anage m en t w ith in the T rus t E x is ting R epo rting S y s t e m s 19 /05 /2016 R upe rt D a v i e s Phil Clark STK (Fire Safety Advisors) Marsha Ingram Rosie Musson Neil Tong R ed A ll s ites m a in ta ined by the T rus t have a spec ific F ire R isk A ssess m e nts in P lace. R ed P P M s a re in p lace as requ ired by H T M s A ll m a ttresses a re 5 and o r 7 C rib ra te d. M anda to ry tra in ing is in p lace. F ire S a fe ty P o licy has been upda ted and re -ra tified N u m be r o f fire requ ired fire m a rsha ls has been iden tified ADT and M id w es t F ire S e rv ices hav been co m m iss ioned to p rov ide a se rv ice w h ich add resses so m e o f th gaps in assurance. S u itab le and su ffic ien t assessm en t fire risk assessm en ts to be unde rtaken a long w ith an aud it o f docu m en ta tion. G rade 1 w o rks fro m fixed w ire tes tin has been co m p le ted. PAT tes ting p rog ra m in p lace E xa m ina tion o f ex te rna l (s truc tu ra l) and in te rna l (su rge p ro tec tion ) co m ponen ts ce rtified. R ou tine tes ting o f fire de tec tion and w a rn ing sys te m s in p lace. P o rtab le fire app liance inspection reg im e in p lace w ith A bbey fire C o m pa rtm en ta tion c o m p le ted su rveys A ud it tra il in p lace in re la tion to s m oke and fire da m pe rs. A ud it o f cu rta ins, d rapes and b linds have ensu red tha t ag reed s tanda rds a re be ing m e t in re la tion to fire s a f e t y. e e o f g P rog ra m o f m a ttress rep lace m en t to be co m p le ted to ensu re tha t a ll m a ttresses a re ra ted as C rib 7 ongo ing. E s ta tes cu rren tly w o rk ing w ith ope ra tiona l s ta ff to ensu re th is s tanda rd is be ing m e t w ith in acu te inpa tien t a reas. P rog ra m o f fire doo r rep lace m en t fo r the D o ro thy P a ttison S ite cu rren tly ongo ing. P rinc ip le fire doo rs a t DPH has been co m p le ted fu rthe r w o rk ongo ing w ith ope ra tiona l co lleagues to ensu re rep lace m en t o f bed roo m doo rs. PAT T e s ting po licy to be deve loped and ra tified (D ece m be r 2017 ) A n independen t rev ie w o f the T rus t's po lic ies and p rocedu res, ro les and responsib ilities, tra in ing and deve lop m en t, risk assessm en t, asset m a in tenance, res ilience, e m e rgency p lann ing and bus iness con tinu ity p lann ing in respect o f fire risks (N ove m be r 2017 ) A m be r STK F ire M anager F ir e c o m p a rtm e n ta tio n assess m e n ts F ire R isk assess m e n ts T ra in ing figu res 27 /09 /2017 R isk upda ted by F ire S a fe ty G roup Enc 23 High Level Operational Risk Register Page 13 of 15
228 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 289 C hanges to the loca l in te ragency 136 po licy m ay leave to T rus t open to repu ta tiona l risks a round its im p le m en ta tion. It is no ted tha t on ly one doc to rs w as requ ired fo r a S ec tion 12 and an A M HP. S hou ld an ins tance a rise w he re a second doc to r w as requ ired they w ou ld be c a lled. The re w e re a lso no ted issues docu m en ted as pa rt o f the T rus ts N ove m be r 2016 CQC V is it. N a m e ly in re la tion p rocesses a round the sa fe ope ra tion o f the T rus ts 136 su ites E x is ting R epo rting S y s t e m s 15 /10 /2015 Les l e y W r ittl e Rosie Musson, 4 4 Hassan Omar, Anne-Marie R ed Carey 16 A n in itia l ve rs ion o f the po licy has been d ra fted and is cu rren tly be ing consu lted upon.. It is the in ten tion tha t on ly 1 doc to r and an A M HP w ill be requ ired fo r a S ec tion 12 and an A M H P. P a rtne rsh ip G roup had s igned o ff the 136 po licy in the m a in 4 4 R ed 16 R ev ie w ing N a tiona l S tanda rds fo r 136 su ites to de te rm ine env iron m en ta l requ ire m en ts (Ju ly 2017 ) T o unde rtake a rev ie w o f the 136 su ite aga ins t requ ire m en ts (Ju ly 2017 ) T o m ake a lte ra tions to env iron m en t to ensu re su ite m ee ts the needs o f the requ ire m en ts (Ju ly 2017 ) T o unde rtake spo t checks o f env iron m en t on an on -go ing bas is (Ju ly 2017 ) It is no ted tha t a lthough the P a rtne rsh ip G roup had s igned o ff the 136 po licy in the m a in the re w e re s till so m e re m a in ing issued to be w o rked th rough. D irec to r o f O pe ra tions and N u rs ing to p rov ide inpu t in to the po licy 4 1 G reen 4 P a rtne rsh ip G roup M ins 26 /05 /2017 F o llo w ing d iscuss ion a t the T rus ts M HASC in ligh t o f the find ings o f the N ove m be r 2016 CQC v is it it w as no ted tha t th is risk shou ld be escala ted to the s ta tus o f a red risk. It is acknow ledged tha t the con tro ls w ill requ ire a lign ing w ith the T rus ts CQC ac tion p lan Enc 23 High Level Operational Risk Register Page 14 of 15
229 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie w Fu rthe r C o m m en ts 379 S ho rtage o f N a tiona l Jun io r psychia tric tra inees fro m A ugus t's ro ta tion m ay im pac t on pa tien t ca re due to reduced w o rk fo rce capac it y W o r k f o r c e S t a tis tic s 06 /06 /2017 A sh i W illia m s Dr Mark Weaver 4 4 R ed Dr Kate Gingell R ed 16 R ev ie w o f on ca ll a rrange m en ts U se o f agency/locu m s 4 2 A m be r 8 W o r k f o r c e c o m m itt e e 06 /06 /2017 R isk added as a red risk fo llo w ing d iscuss ion a t T rus t B oa rd, w he reby it w as sugges ted tha t th is risk w ou ld be added to the risk reg is te r as it w ou ld need be c lose ly m on ito red and it m ay be necessary t rev ie w the on ca ll a rrange m en ts if the sho rtfa ll w as no t add ressed. A dd itiona lly sou rc ing su itab le agency locu m cove r re m a ined cha lleng ing fo llo w ing the agency cap and o the r changes in locu m sho rt te rm e m p loy m en t a rrange m e n ts. Enc 23 High Level Operational Risk Register Page 15 of 15
230 Board meeting date: 5 October 2017 Agenda Item number: 8.1 Enclosure: 24 Report Title: MERIT Vanguard Overview Report Accountable Director: Author (name & title): Mark Axcell Chief Executive Mark Axcell Chief Executive Purpose of the report: The attached updates the Board on progress with the MERIT Vanguard as at September Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: N/A The Board is asked to note progress with the MERIT Vanguard. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Please give brief details: The MERIT Vanguard aims effect all CQC domains Responsive Effective Well-led Safe Enc 24 MERIT Vanguard Overview Report Page 1 of 3
231 Title MERIT Vanguard Overview Report Introduction MERIT alliance is an equal partnership between four trusts: Birmingham and Solihull Mental Health NHS Foundation Trust (BSMHFT) Black Country Partnership NHS Foundation Trust (BCPFT) Coventry and Warwickshire Partnership NHS Trust (CWPT) Dudley and Walsall Mental Health Partnership NHS Trust (DWMHT) The programme consists of two clinical workstreams (Crisis Care; and Recovery Culture) and five enabling workstreams (Information Technology; Workforce; Quality Governance; Equality & Diversity; and Research & Innovation). The report outlines the main achievements in the reporting period and that planned for the next along with the key risks and issues in the workstreams and their mitigations. The quarterly update report is dated 13 September 2017 and was agreed as at the last meeting of the MERIT Steering Group. Summary of key points, issues and risks Recovery Pathway Due to funding issues it is not possible to confirm training details which is impacting on timescales. If issues regarding funding continue then it is likely to change the status to RED. Crisis Pathway There has been slippage with the Crisis Care training competencies and pathways research element. Additional resource is being sought for R&I. Timescales and scope will need to be refreshed. There is a significant risk to the delivery of this activity due to the loss of project management resource which is likely to change the status to RED. ESHR Viewer Due to funds not being released, accessing technical resource which incurs costs had been adversely impacted. There is also slippage in the development of interface activity as a result of more time required to complete and engagement from appropriate stakeholders and also the loss of project management support. The new expected phased Go-Live date is November onwards. Co-Ordinated Bed Management Due to funds not being released, accessing technical resource which incurs costs has been adversely impacted. There is also slippage in the implementation of SOPs as a result of poor engagement from appropriate stakeholders (primarily, bed managers and clinicians) from each Trust and also the loss of project management support. Enc 24 MERIT Vanguard Overview Report Page 2 of 3
232 Temporary Staffing Activity currently on schedule, however there is a risk to the delivery of this activity due to the loss of project management and Workstream Lead resource. Training Passport There is some minimal slippage on timescales for the training passport to be delivered on schedule due to Trusts signing off MOU through their respective HR committees. There is also a risk to the delivery of this activity due to the loss of project management and Workstream Lead resource. Recommendation That the board receive this quarterly update on progress with the MERIT vanguard Board action required To receive the report for assurance. Enc 24 MERIT Vanguard Overview Report Page 3 of 3

233 Enc 4a SEPTEMBER 2017 Current RAG Forecasted RAG MERIT R ( ) A ( ) Main achievements this reporting period Evaluation dashboard for key metrics available Crisis Care website signed-off at CQOSG and all changes to the website to be completed by the developer Crisis Care website Go-Live and completion of associated comms and engagement Information Sharing Agreement signed-off Development of the Bed Management viewer commenced Training Passport scoping workshop finalise content R&I planned activity for Crisis Care pathway and competency framework confirmed Feasibility analysis and demand for cross trust cover temporary staffing to be carried out Commence software development for time to shine toolkit Scoping of ReQol technical solution web base and browser The BCPFT ReQol app will be piloted (paper or IT solution) Implementation plans for Recovery model for BSMHFT Progression of WMCA support for TimeBank HSJ article on Bed Management and ESHR MERIT Presentation to Birmingham and Solihull STP Mental Health Programme Delivery Group Main achievements planned for next reporting period MERIT Programme Financial impact assessment and review Training Passport MOU sign off by Workforce committees and go-live Completion of the referral form for Bed Management Implementation commencement of Bed Management SOPs Progression of ESHR viewer (Health Share) implementation Research questions confirmed for Crisis Care pathways and training competencies with outline plan agreed for delivery Delivery of initial awareness of Crisis Care deliverables (ESHR, Bed Management and Website) and associated communications tools (intro piece, Q&A, flow diagram and internal comms) Updating of MERIT website and Trust intranet sites Filming for Mental Health First Aid complete Recovery practices baseline complete for all four Trusts Confirmation of refocus skills development programme Confirmation of horizon change agents training and action learning sets TimeBank vision document completed Health Expo MERIT presentations and stand NHS Employers MERIT Presentation Royal College of Psychiatry - MERIT Presentation Key Risks/Issues 1. Funding for Q1 has not been released by NHS E 2. Continued Clinical and Operational engagement, input and buy-in from all four Trusts (Risk Ref 3) 3. There is a risk that all or part of the programme objectives may not be achieved, if one or more partners do not support all or part of the programme deliverables (Risk Ref 5) Mitigations 1. To work with NHS E to release funds 2. Steering group and Clinical Oversight group to support the continued engagement. Areas of low engagement to be identified and progressed by each Trust 3. Ensure leadership involvement and support remains in place from all organisations. Gain support and buy-in from Trust Boards. Page 1 of 16
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016 1.00pm-3.45pm Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS PUBLIC MEETING
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016 1.00pm-3.45pm Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS PUBLIC MEETING
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Wednesday 6 th August 2014 3:00 pm 5:00 pm Board Room, 1st Floor, Canalside House, Abbotts Street, Bloxwich, Walsall,
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Wednesday 6 th August 2014 3:00 pm 5:00 pm Board Room, 1st Floor, Canalside House, Abbotts Street, Bloxwich, Walsall,
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
Dudley & Walsall Mental Health Partnership NHS Trust Board
 Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Improvement and assessment framework for children and young people s health services
 Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Improvement Plan in response to recommendations outlined in the Independent Investigation into the Care and Treatment of P 14 June 2017
 Improvement Plan in response to recommendations outlined in the Independent Investigation into the Care and Treatment of P 14 June 2017 RAG key: Completed In progress Outstanding RECOMMENDATION 1 Black
Improvement Plan in response to recommendations outlined in the Independent Investigation into the Care and Treatment of P 14 June 2017 RAG key: Completed In progress Outstanding RECOMMENDATION 1 Black
Review of due diligence undertaken by PWC January 2014
 FOI615 FOI request concerning the due diligence undertaken on the acquisition of Oxfordshire Learning Disability Trust (OLDT) and the subsequent review of that due diligence. This response includes details
FOI615 FOI request concerning the due diligence undertaken on the acquisition of Oxfordshire Learning Disability Trust (OLDT) and the subsequent review of that due diligence. This response includes details
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Adults and Safeguarding Committee 19 March Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy.
 Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
NHS East and North Hertfordshire Clinical Commissioning Group. Quality Committee. Terms of Reference Version 4.0
 NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
The Board is asked to note the survey outcome as Substantial (green rag rating). Progress with action planning and delivery has commenced
. Progress with action planning and delivery has commenced") Item 13 Report title Report from Prepared by Previously discussed at Attachments Report to Board, 30 March 2017 NHS England emergency preparedness resilience and response (EPRR) annual assurance survey
Item 13 Report title Report from Prepared by Previously discussed at Attachments Report to Board, 30 March 2017 NHS England emergency preparedness resilience and response (EPRR) annual assurance survey
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Safeguarding review to assist Walsall Healthcare NHS Trust
 [Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
[Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011
 HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011 1. Purpose This paper provides an update on the outcome of the consultation to re-provide Intermediate Care Services
HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011 1. Purpose This paper provides an update on the outcome of the consultation to re-provide Intermediate Care Services
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
DR KUMAR CQC INSPECTION ACTION PLAN
 DR KUMAR CQC INSPECTION ACTION PLAN REVIEWED: 28 TH DECEMBER 2015 RED NOT COMPLETED AMBER STARTED TO COMPLETE or SUPPORT AGREED WITH OTHER PARTNERS/ AGENCIES GREEEN COMPLETED GENERAL CQC CONCERNS ASSURANCE
DR KUMAR CQC INSPECTION ACTION PLAN REVIEWED: 28 TH DECEMBER 2015 RED NOT COMPLETED AMBER STARTED TO COMPLETE or SUPPORT AGREED WITH OTHER PARTNERS/ AGENCIES GREEEN COMPLETED GENERAL CQC CONCERNS ASSURANCE
Why do we need this project? What is Mouth Care Matters? Why Does it Matter? Mary. Oral Health Champion Volunteers. August 2018
 This month, I am pleased to inform you about this important project, Mouth Care Matters, and am proud to support the Dental Service within the MaxilloFacial Department as the Executive Lead on this. 1
This month, I am pleased to inform you about this important project, Mouth Care Matters, and am proud to support the Dental Service within the MaxilloFacial Department as the Executive Lead on this. 1
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Present: Dr Stephen Bentley Specialist Doctor Assistant Director Integrated Commissioning Associate Director Health Services Commissioning
 Agenda Item No: C DRAFT Minutes of the Meeting of the Governing Body held on Wednesday at 1.30 p.m. in Jubilee Suite, Orford Jubilee Suite, Winwick Road, Warrington Present: In Attendance: Dr Andrew Davies
Agenda Item No: C DRAFT Minutes of the Meeting of the Governing Body held on Wednesday at 1.30 p.m. in Jubilee Suite, Orford Jubilee Suite, Winwick Road, Warrington Present: In Attendance: Dr Andrew Davies
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Present: Mr B Reid OBE Chair of the Board of Directors Mr N Summers CBE Vice Chair of the Board of Directors. Mr G McEvoy Non-executive Director
 ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
Personal Budgets and Direct Payments
 Personal Budgets/Direct Payments Date of resource : April 20 Page 1 of Learning Aims The learning aims of this briefing are to enable you to 1 Understand how personal budgets can be requested for special
Personal Budgets/Direct Payments Date of resource : April 20 Page 1 of Learning Aims The learning aims of this briefing are to enable you to 1 Understand how personal budgets can be requested for special
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session
 Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: Tuesday 23 September 2014 For: Decision Discussion Noting Agenda Item and title: Author:
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: Tuesday 23 September 2014 For: Decision Discussion Noting Agenda Item and title: Author:
Learning from Deaths Policy
 Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting
 Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
Integrating care: contracting for accountable models NHS England
 New care models Integrating care: contracting for accountable models NHS England Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement,
New care models Integrating care: contracting for accountable models NHS England Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement,
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
Apologies Lay Member Financial Management & Audit
 Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
Warrington CCG Operational Safeguarding Children Health Forum. Terms of Reference
 Warrington CCG Operational Safeguarding Children Health Forum 1 Introduction Terms of Reference 1.1 The Operational Safeguarding Children Health Forum (the Health Forum) is established within the Safety
Warrington CCG Operational Safeguarding Children Health Forum 1 Introduction Terms of Reference 1.1 The Operational Safeguarding Children Health Forum (the Health Forum) is established within the Safety
APPROVED CLINICIAN (AC) POLICY FOR MEDICAL STAFF
 POLICY FOR MEDICAL STAFF") APPROVED CLINICIAN (AC) POLICY FOR MEDICAL STAFF Version: 1 Ratified by: Date ratified: August 2015 Title of originator/author: Title of responsible committee/group: Date issued: August 2015 Review date:
APPROVED CLINICIAN (AC) POLICY FOR MEDICAL STAFF Version: 1 Ratified by: Date ratified: August 2015 Title of originator/author: Title of responsible committee/group: Date issued: August 2015 Review date:
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
(Committee Chair) Chair) Interim Board Secretary (MHSA/16/25 onwards) Head of CAMHS and Childrens Learning Disability (MHSA/16/24 only)
 Chair) Interim Board Secretary (MHSA/16/25 onwards) Head of CAMHS and Childrens Learning Disability (MHSA/16/24 only)") POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 03 MARCH 2016, AT 10.00AM, GROUND CONFERENCE ROOM, NEUADD BRYCHEINIOG, BRECON Present:
POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 03 MARCH 2016, AT 10.00AM, GROUND CONFERENCE ROOM, NEUADD BRYCHEINIOG, BRECON Present:
Minutes. Board of Directors meeting held in public. Wednesday, 27 September pm 3.00pm Board Room, St Nicholas Hospital
 Agenda item 3) Minutes Board of Directors meeting held in public Wednesday, 27 September 2017 1.00pm 3.00pm Board Room, St Nicholas Hospital Present: Alexis Cleveland Dr Leslie Boobis Martin Cocker James
Agenda item 3) Minutes Board of Directors meeting held in public Wednesday, 27 September 2017 1.00pm 3.00pm Board Room, St Nicholas Hospital Present: Alexis Cleveland Dr Leslie Boobis Martin Cocker James
Document Title Investigating Deaths (Mortality Review) Policy
 Policy") Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Workforce and Organisational Development Committee. Minutes of the meeting held on in the Board Room, Ysbyty Gwynedd and via videoconference
 Workforce and Organisational Development Committee Minutes of the meeting held on 13.3.14 in the Board Room, Ysbyty Gwynedd and via videoconference Present: Dr P Higson Ms J Dean Dr C Tillson Mr K McDonogh
Workforce and Organisational Development Committee Minutes of the meeting held on 13.3.14 in the Board Room, Ysbyty Gwynedd and via videoconference Present: Dr P Higson Ms J Dean Dr C Tillson Mr K McDonogh
NHS Cumbria CCG Transforming Care Programme Learning Disabilities
 NHS Cumbria CCG Governing Body Agenda Item 07 December 2016 8 NHS Cumbria CCG Transforming Care Programme Learning Disabilities Purpose of the Report To update the Governing Body on local progress with
NHS Cumbria CCG Governing Body Agenda Item 07 December 2016 8 NHS Cumbria CCG Transforming Care Programme Learning Disabilities Purpose of the Report To update the Governing Body on local progress with
ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS. To approve. This paper supports the standards
 BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Service Guide. together. Your guide to: for Walsall GPs. Services provided Referral pathways How to contact services
 Service Guide for Walsall GPs Your guide to: Services provided Referral pathways How to contact services together Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced
Service Guide for Walsall GPs Your guide to: Services provided Referral pathways How to contact services together Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Service Guide. Your guide to: for Dudley GPs. Services provided Referral pathways How to contact services
 Service Guide for Dudley GPs Your guide to: Services provided Referral pathways How to contact services Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced to help
Service Guide for Dudley GPs Your guide to: Services provided Referral pathways How to contact services Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced to help
Mental Health (Wales) Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities
 Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities") Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Minutes of a Corporation Meeting held on
 Minutes of a Corporation Meeting held on Wednesday 13 th July 2016 at 5.00pm Held in the Boardroom Present: In Attendance: Mr Stuart Brand Ms Di Crookes Mr Stewart Fergusson Ms Maggie Galliers (Chair)
Minutes of a Corporation Meeting held on Wednesday 13 th July 2016 at 5.00pm Held in the Boardroom Present: In Attendance: Mr Stuart Brand Ms Di Crookes Mr Stewart Fergusson Ms Maggie Galliers (Chair)
Under 18s Admission to Adult Mental Health Ward: Standard Operating Procedure
 Clinical Under 18s Admission to Adult Mental Health Ward: Standard Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: Replacement. Replaces: Policy on the formal or
Clinical Under 18s Admission to Adult Mental Health Ward: Standard Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: Replacement. Replaces: Policy on the formal or
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Unique Identifier: Review Date: November Issue Status: Approved Version No: 1.4 Issue Date: November 2017
 Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Visit report on Royal Cornwall Hospital NHS Trust
 South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Meeting of Governing Body
 Meeting of Governing Body Date: 7 August 2018 Time: 1.30pm Location: Clevedon Hall, Elton Rd, Clevedon, North Somerset, BS21 7RQ Agenda number: 10.3 Report title: Business Continuity Policy Report Author:
Meeting of Governing Body Date: 7 August 2018 Time: 1.30pm Location: Clevedon Hall, Elton Rd, Clevedon, North Somerset, BS21 7RQ Agenda number: 10.3 Report title: Business Continuity Policy Report Author:
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
Response to recommendations made in the Independent review into Liverpool Community Health NHS Trust
 To: The Board For meeting on: 22 March 2018 Agenda item: 8 Report by: Ian Dalton, Chief Executive Officer Report on: Response to recommendations made in the Independent review into Liverpool Community
To: The Board For meeting on: 22 March 2018 Agenda item: 8 Report by: Ian Dalton, Chief Executive Officer Report on: Response to recommendations made in the Independent review into Liverpool Community
Report from Quality Assurance Committee meeting held on 30 November 2017
 Report from Quality Assurance Committee meeting held on 30 November 2017 Governing Body meeting Item 18f 11 January 2018 Author(s) Sponsor Director Purpose of Paper Carol Henderson, Committee Secretary
Report from Quality Assurance Committee meeting held on 30 November 2017 Governing Body meeting Item 18f 11 January 2018 Author(s) Sponsor Director Purpose of Paper Carol Henderson, Committee Secretary
Stewart Mason, Emergency Planning and Resilience Officer Tom Jones, Clinical Programme Manager
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Shakeel Sabir Head of MERIT Vanguard
 MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
CLINICAL COMMISSIONING GROUP RESPONSIBILITIES TO ENSURE ROBUST SAFEGUARDING AND LOOKED AFTER CHILDREN ARRANGEMENTS
 MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
TRUST BOARD TB(16) 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals
 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals") TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
(Committee Chair) Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)
 Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)") POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
GOVERNING BOARD. Governing Board Assurance Framework. Date of Meeting 16 March 2016 Agenda Item No 6. Title
 GOVERNNG BOARD Date of Meeting 16 March 2016 Agenda tem No 6 Title Governing Board Assurance Framework Governing Board members reviewed the GBAF s and process at a development session on 10 February 2016.
GOVERNNG BOARD Date of Meeting 16 March 2016 Agenda tem No 6 Title Governing Board Assurance Framework Governing Board members reviewed the GBAF s and process at a development session on 10 February 2016.
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC
 Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality