Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting
|
|
|
- Hortense Cain
- 5 years ago
- Views:
Transcription
1 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Wednesday 6 th August :00 pm 5:00 pm Board Room, 1st Floor, Canalside House, Abbotts Street, Bloxwich, Walsall, WS3 3BW
2
3 PUBLIC MEETING OF THE TRUST BOARD 3pm, Wednesday 6 th August 2014 Boardroom, Canalside House, Walsall AGENDA ITEM Purpose Board Lead Format Timings 1. Apologies 3pm Minutes Of the Previous Meeting 2. To approve the minutes of the Board meetings held on Wednesday 2 nd July 2014 Approval Dr Hill, Interim Chair Enc 1 3. Summary Report of Confidential session of Trust Board held on Wednesday 2 nd July 2014 Information 4. Matters Arising Continuity 5. Notification of Items of Any Other Business Dr Hill Interim Chair Dr Hill Interim Chair Enc 2 Enc 3 6. Declarations of Interests For Board members to declare any relevant interests in items on the agenda. All Enc 4 7. Questions from Members of the Public 8. Chairman s Comments (including Chair recruitment process update) Information Dr Hill Interim Chair Oral 3.10pm 9. Chief Executive Officer s Overview (including written summary of strategic publications and headlines) Information Mr Graham Enc pm 10. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS 10.1 Trust Integrated Performance Dashboard (Month 3) Performance Report Quality Governance Report Finance Report Workforce Report 10.2 TDA PMR Report - Month 3 Assurance Approval (following Chair s action) 10.3 Governance and Quality Committee Chair s Report, Assurance Mr Axcell /Ms Pugh/Ms Ingram Mr Axcell Dr Gutteridge 10.4 Finance & Performance Committee Chair s Report Assurance Mr Higgs Enc 6 Enc 7 Enc 8 Oral 3.20pm 3.35pm 3.40pm 3.45pm
4 ITEM Purpose Board Lead Format Timings 10.5 Audit Committee Chair s Report Assurance Mr Matthews Oral 3.50pm 10.6 Management Executive Team Chair s Report Assurance Mr Graham Oral 3.55pm 10.7 Mental Health Act Scrutiny Chair s Report, including: - Mental Act Scrutiny Committee Annual Report Assurance Dr Hill Interim Chair Enc 9 4pm 10.8 Trust Wide Risk Register Approval Ms Pugh Enc pm 10.9 Quality Update Report and Francis Winterbourne Recommendations Update Assurance Ms Pugh (Ms Musson in attendance) Enc pm Service Experience Desk Annual Report Assurance Ms Ingram (Mrs Bytheway in attendance) Enc pm Full Picture and Proposals regarding changes to the Complaints Process Information /Approval Ms Ingram Enc pm 11. LEADERSHIP, CULTURE & WORKFORCE 11.1 Medical Directors Update Assurance Dr Weaver/Dr Gingell Oral 4.40pm 11.2 Nurse Director Update Assurance Ms Pugh Oral 4.45pm 11.3 Monthly Ward Staffing Report Assurance Ms Pugh Enc pm 12. STRATEGIC DEVELOPMENT & DIRECTION 12.1 Update to BAF report & framework presentation Approval Ms Edwards Enc 15 5pm 13. ANY OTHER BUSINESS 14. DATE AND TIME OF THE NEXT MEETING Wednesday 3 rd September 2014, 3pm, Dudley TBC
5 MINUTES OF THE TRUST BOARD MEETING OF DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST Held on Wednesday 2 nd July 2014 Village Hotel, Dudley PUBLIC SESSION Enc 1 Present Dr S Hill Mr Graham Mr M Axcell Dr K Gingell Mr D Matthews Dr R Gutteridge Mrs G Cooper Interim Chair/Non Executive Director Chief Executive Officer Director of Finance & Performance (up to item only) Joint Medical Director Non Executive Director Non Executive Director Non Executive Director In Attendance Ms M Edwards Ms R Musson Mr P Singh Miss H King FT Project/Company Secretary Consultant Head of Nursing, Quality and Innovation (items to only) Equality and Diversity Lead (item only) Minute Taker 248. APOLOGIES ACTION Apologies were received from Dr Weaver, Mr Higgs, Ms Ingram, and Ms Pugh. It was noted that Mr Axcell would need to leave the meeting early MINUTES OF THE PREVIOUS MEETING The minutes of the meeting held on 4 th June 2014 were agreed as an accurate record, with the exception of the following: - Item 243 end of 4 th paragraph to read Mr Graham informed the Board that he had been advised that the unions Day of Activity on pay planned for 5 th June would not affect us. - Item nd paragraph to read the growth PMO would be funded from the non-recurrent gains from MARS. - Item nd paragraph to read External Audit had been very positive about the way the Trust's accounts had been prepared and had commented that the Trust's financial position compares favourably with other Trusts they audit however, the sector faces continued pressures and the Trust needs to remain focused on achieving its CIP and its overall financial position. The Minutes of the Extraordinary Board meeting held on 24 th June 2014 were agreed as an accurate record. The Chair thanked Mrs Cooper for 1
6 chairing the meeting. The minutes were approved and would be signed by the Chair following the amendments requested being undertaken for those dated 4 th June SUMMARY REPORT OF CONFIDENTIAL SESSION OF TRUST BOARD The Board noted a summary of the business transacted in the confidential session of the Trust Board held on 4 th June MATTERS ARISING The schedule of matters outstanding was discussed and the following was noted: Regarding item it was noted that the Safer Staffing Levels Report had been published as required. Regarding item Mr Axcell advised that the redesign of the Performance Dashboard was ongoing. Dr Hill highlighted that as issues became more complex, enhanced triangulation would be very important. Regarding item Mr Axcell confirmed that the risks had been discussed and a full update was provided within the Risk Register report and Finance and Performance Committee Chair s Report. Regarding item a Board to Board meeting with Dudley CCG was still being arranged and Ms Edwards would keep the Board informed as progress was made. Regarding item it was explained that as there was no specific deadline for the work, the deferral of this item to August would not be an issue. Dr Hill was keen that the item should not be deferred again NOTIFICATIONS OF ITEMS OF ANY OTHER BUSINESS No items of any other business were noted DECLARATIONS OF INTEREST Members were asked to disclose any interest they may have, direct or indirect, in any of the items being considered during the course of the meeting and to note that those members declaring an interest would not be allowed to participate in the consideration, discussion or vote on any issue relating to that item. No interests were declared QUESTIONS FROM MEMBERS OF THE PUBLIC No members of the public were present. 2
7 255. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS Trust Integrated Performance Dashboard Month 2 Mr Axcell took the Board through the key points, issues, and risks, as set out within the report. He highlighted that - There had been 1 patient fall in the month which was reported on the Quality dashboard. - Ethnicity coding which was a new target was still posing a challenge. Mr Axcell advised that the target was 90% and that as at the end of May this target had been met. It was highlighted that there was potential for the CCGs to fine the Trust circa 14k if the target was not met for 2 months. - The Trust remained below its YTD activity target, which had been discussed at the Finance and Performance Committee. Work was being undertaken with the teams to see what the main drivers were, with a detailed report to be returned to the Committee. It was not an issue at present as the Trust was on a block contract, but would need to be resolved for the future. - IAPT people completed treatment (Dudley) was showing an amber RAG rating for month 2, this was considered to be a one off, with performance expected to be back on track for next month. Delayed Transfers of Care were discussed. The Dashboard was showing this at 0% which was good. It was highlighted however that this could be as a result of complex patients becoming poorlier no place of discharge that would be appropriate. It was noted that the average length of stay looked good. It was however, pointed out that as this figure was collected upon discharge Delayed Transfers of Care would not be included. Mr Axcell agreed to include a KPI on the Dashboard to show length of stay more accurately than at present, including Delayed Transfer of Care cases. Mr Axcell Mr Axcell proceeded to take the Board through the service line dashboards. It was highlighted that: - PDR figures in Acute Services were one of the lowest in the organisation at 56%. - 7 day follow up on inpatient discharges figures did not appear correct as they all read the same and mirrored the whole Trust Dashboard figure. Mr Axcell agreed to check this. - Copies of Care Plan within Early Intervention were being targeted for improvement. - The average length of stay within Older Adults was rising. - Sickness appeared to be an issue within most service lines, except recovery, with Older Adults being nearly double the target. This was affecting the delivery of activity against contract target. Mr Axcell 3
8 Mrs Cooper queried what was being done specifically about sickness levels within the Trust. At each meeting it had been advised that steps were being taken to improve the situation but for the 7 th consecutive month improvement had not been seen. Long term sickness was also increasing. Mr Graham reminded the Board of leadership issues that had been identified within Older Adults last year. Changes had been made and posts removed, the Head of Service post had been advertised, and the Clinical Director for the area had moved to Dudley to be more local to any issues. Older Adults had been flagged as an area of concern by the CQC. Punitive action would not be helpful and the impact of the new management structure should start to reduce. This would also be picked up through QPR. Finance and activity were generally under control. The Board expressed its concern, but noted Mr Graham s comments. The Board would keep a watching eye on the matter and improvement would be expected. Dr Gingell advised that once the new management structure was in place for Older Adults there would inevitably be a short period of destabilisation. The Older Adult Strategy and future service shape from commissioners were also awaited, and once in place would help. Mr Graham reminded the Board that the issues within the service were known. The quality indicators for the service were all green, and assurance should be taken from this. Mr Axcell advised that from a financial perspective all was fine, however the vacancies currently in the system were masking sickness and an overspend would show when vacancies were recruited to. Mr Axcell took the Board through the Performance Report and the following was noted: - KPI 1. new cases accepted to EI (Walsall) was showing as amber but the issue had now been resolved and this would return to green. - KPI 12. ethnicity codes had already been discussed under the Dashboard report. Mr Matthews queried whether of the 5% not followed up within 7 days of inpatient discharge did the Trust have assurance that these were still followed up. Dr Gingell confirmed that they were all followed up on an individual basis. Dr Gutteridge advised that there had been some discussion about KPI 14 IAPT people who had completed treatment metric not being useful. Mr Axcell advised that discussion around this had been incorporated within the report. Mr Axcell took the Board through the Finance report and the key 4
9 messages as set out on page 3 of the report. The Trust had delivered a surplus in month 2 of 224K, which was 107k ahead of the planned surplus for the year to date. Mrs Cooper queried why there had been a delay regarding the detox recovery beds at Bushey Fields Hospital. Dr Gingell explained that the Substance Misuse Service had ceased to be provided by the Trust and arrangements had not been in place immediately to continue with the detox beds. This had now been resolved. Mr Matthews queried whether it was an issue that pay was over spent. Mr Axcell advised that this was not an issue as pay had to be looked at in conjunction with other costs. Future reports would include netted-down pay and non-pay to show the true position better. The capital programme was on plan, and from a cash perspective the Trust was ahead of schedule. Mr Axcell advised that the funding arrangement for out of area placements was changing which may pose a risk. This was being looked in to further at the Finance and Performance Committee. The Chair highlighted the level of detail within the Finance Report and queried whether it should be condensed. Mr Graham advised that he had asked Mr Axcell to look at the detail of the report, but it was important that the Trust remained transparent. Mr Axcell explained that in the future he hoped to incorporate in to the Finance Report something similar to that of the summary report in the Workforce Report, including service line reporting on pay and non pay. The Finance Team were working on this at present. In summary it had been a good start to the year, the Board knew what the risks were early on and know what is being done to manage those risks. Mr Axcell left the meeting. Dr Gutteridge took the Board through the Quality Report. She advised that there were no major trends to note. Serious incidents were showing a downward trend and the Governance and Quality Committee were reviewing if this was due to a change in category. It was noted that incidents had decreased by 16.5% on the previous month. The Chair asked if the safeguarding section of the report could be changed to bring out the key points. Dr Gutteridge advised that the Governance and Quality Committee wanted to re-look at how it reported and collated its data in order to provide more intelligent information. The Board agreed that the Governance and Quality Committee 5
10 should look at how it reported and collated its information in order to produce different and more helpful reporting. Mr Graham took the Board through the key messages of the Workforce Report and it was noted that: - A full picture would be available on MARS by 12 th July The Trust s 5 year workforce plan had been submitted to Health Education England. There were thought to be significant changes afoot regarding their workforce plans and this would be kept an eye on. - The Trust had a new cohort of 9 Band 5 nurses. 25 had been recruited previously. The Trust had found it more successful to recruit via mass advert than to try and recruit to individual posts. - There had been a recruitment event for apprentices in partnership with Walsall College. Dr Gingell advised that difficulty was being experienced with regards to the recruitment of Junior Doctors as a result of the recruitment process now being managed at a national level. There appeared a general lack of interest in Psychiatry, resulting in vacancies which had cost implications as they had to be covered by locums. The Chair expressed his disappointment regarding this change in process. The dashboard showed sickness had slightly reduced (in month) but slightly increased year to date. PDRs stood at 68%. The Board noted the performance of the Trust as at month CHAIRMAN S COMMENTS The Chair advised that a Council of Governors Meeting had taken place on the 18 th June 2014, which had been well received. The Governors also receive monthly summaries of both confidential and public Trust Board meetings CHIEF EXECUTIVE OFFICER S OVERVIEW Mr Graham spoke through his strategic overview and horizon scan paper for the Board which was included within the papers. The Board discussed the paper and the following was highlighted: - The CQC had formally written to the TDA and Monitor saying that they had assessed that the Trust s quality was at an appropriate level to continue to progress towards becoming a Foundation Trust. The Trust now anticipated being reactivated with Monitor on 3 rd October It was pleasing to note that the Trust had therefore received an implicit good or outstanding rating from CQC. - The QGAF review was on the Board agenda for review today. - Monitor had committed to a view of what good leadership looked like. - The new NHS pension scheme employer contribution rate of 14.3% 6
11 was already included within the LTFM. The Board agreed that it was a useful report summarising important information in one place. The Chair asked that Ms Edwards separate the news items from items which needed to be actioned for future reports. Mrs Cooper highlighted the Equality and Diversity Award and asked whether this would be recognised in some way. Mr Graham asked that Ms Ingram include this in the staff recognition programme, perhaps recognising it at the staff awards. Ms Edwards Ms Ingram The Board received the CEO s overview for information and assurance QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS TDA PMR Report Month 2 The Board noted the contents of the report which summarised the Trust s performance as at the end of month /15. The Board declarations had already been signed off for submission to the TDA as a Chairman s action. The Board endorsed and ratified the PMR submission as at month Governance and Quality Committee Chair s Report Ms Musson joined the meeting. Dr Gutteridge took the Board through the Governance and Quality Committee Chair s report and highlighted the key points: - The daily safer staffing levels review continued. - A deep dive had been requested in to medicines management. It had been a very fruitful discussion about identifying risks and quality improvement. - Action had been agreed to facilitate continuous improvement in the quality of action plans relating to embedding lessons. Action plans would not be signed off if they were not using SMART objectives. - The Information Governance Committee needed to be added to the interfaces with other Committees section. - There were no new quality risks recommended to the Board for addition to the register this month. - The quality account had been ratified at the Extraordinary Board Meeting on 24 th June A key priority was the intelligent use of data; this would be worked upon by the Committee without compromising monthly reporting. Ms Pugh/Dr Gutteridge The Board accepted the report for assurance and endorsed the decisions and recommendations made by the Committee. The 7
12 Board approved the Quality Report for the period ending May 2014, and endorsed the Committee s activity around the intelligent use of data. Ms Musson presented the Board with the quarterly refresh of the QGAF. The Board discussed each domain in turn and debated what rating it considered appropriate currently. The following points were noted: In March the Trust had self-assessed and agreed a score of 2.5 (2 x A/G rating, plus1 x A/R regards data quality). It would be unlikely that a score of 0 would ever be achieved as this was a fluid process and there were always lessons to be learned and improvements to make. - 1A Does quality drive Trust strategy? The Trust would continue to improve in this area. The Quality Improvement Strategy would need to be refreshed before reactivation with Monitor. The Board agreed the rating should remain green. - 1B Is the Board aware of potential risks to quality? Significant progress had been made in this area which could be evidenced with regards to the embedding and effectiveness of the new PMO process. The risk escalation process was in place. At the recent Board Development Meeting it had been decided that MExT would be responsible for CIP delivery, and report to Trust Board by exception, with the Board delegating any issues to the Governance and Quality Committee or Finance and Performance Committee as required. Mr Graham also mentioned the recent CQC report and its comments, pointing out that the actions identified meant the rating should probably not be changed. It was also noted that the reports from the whistleblowing and staff engagement work would need to be complete to assure the Board that staff felt able to raise concerns before the Board could relook at this. The Board agreed the rating would remain amber/green. - 2A Does the Board have the necessary leadership, skills and knowledge to ensure delivery of the quality agenda? The narrative for this domain should be strengthened using the narrative from within the recent CQC report which was very positive about the strong NEDs and effective leadership. The Board agreed the rating should remain green. - 2B Does the Board promote a quality focused culture throughout the Trust? The Board agreed the rating should remain green - 3A Are there clear roles and responsibilities in relation to quality 8
13 governance? The Trust had received strong CQC feedback in this area. The Board agreed the rating should remain green - 3B Are there clear well defined processes for escalating and resolving issues and managing quality? Monitor had said previously that staff appraisals were not linked to the Trust s quality goals. The CQC had provided positive feedback on how the Trust had managed quality concerns in older adults. The Governance and Quality Committee had discussed the data quality work undertaken, the strengthening of the safeguarding system, and incident reporting work. Mrs Cooper highlighted the whistle blowing issues and low appraisal figures, querying that although a strong framework was in place, was this working effectively? The Board acknowledged that the Trust had addressed the original issues that led to an A/G rating, but was not confident that newly identified issues had yet been fully addressed. It was decided that the staff engagement work should come to fruition before any change was made to this rating. The Board agreed the rating should remain amber/green. - 3C Does the Board actively engage patients, staff and other key stakeholders on quality? Reference to the active engagement with staff and service users, plus EbE s needed to be added to the narrative. The Board agreed the rating should remain green. - 4A is appropriate quality information being analysed and challenged? The Board agreed the challenge was whether it was analysing the right quality metrics. There was a considerable amount of data available but it was whether it was analysed and challenged as intelligently as it might be. The Trust was on a journey of continuous improvement with this. Dr Gingell thought that for the domain to be rated green, data would need to be available more quickly and triangulated better with the people on the front line. Qualitative narrative could also be improved. It was agreed that Mental Health Strategies need to complete their work, present the finding to the Governance and Quality Task and Finish Group, and the relevant metrics to be signed off by Board, before this domain could be rated green. 9
14 The Board agreed the rating should remain as amber/green. - 4B Is the Board assured of the robustness of quality information? It was anticipated this domain would improve from an amber/red rating once the data quality internal audit was complete and provided positive assurance. Data Quality was currently a red rated risk on the risk register. Ms Edwards also advised that the outcome of the recent Clinical Coding Audit needed to be reported to the Board. Ms Pugh The Board agreed the rating should remain as amber/red. - 4C Is quality information used effectively? It was highlighted that the information was generally presented clearly and effectively, and was humanised. The green rating had been sustained and ongoing improvement work continued to improve benchmarking opportunities. The Board agreed that the rating should remain green. The outcome of the Board s review of the QGAF was that the total score should remain the same, at 2.5. Ms Musson would update the narrative for the QGAF domains as specified by the Board. Ms Musson Mrs Cooper queried whether the Board felt it was doing everything it could, as it had not predicted the 3 CQC compliance notices which it received. Quality issues at the point of care were raised by the CQC. Mr Graham advised that the severity of these notices, none of which were serious, should be borne in mind and that all had been addressed immediately. The Chair highlighted that the Board was making intelligent use of the QGAF. The Board asked the Governance and Quality Committee to oversee the actions identified and agree timescales Finance and Performance Committee Chair s Report The Board accepted the report for assurance and endorsed the decisions and recommendations made by the Committee Director of Infection Prevention and Control Annual Report Ms Musson explained that the report provided an overview of all aspects of the Trust s infection prevention and control programme for 2013/14, and was also a demonstration of assurance from the Director of Infection prevention and Control in relation to Trust compliance with the Health 10
15 and Social Care Act The report had been endorsed by the Governance and Quality Committee, and following Board approval would be published on the Trust s website. The Board approved the report and work programme for 2014/15. Ms Musson left the meeting Audit Committee Chair s Report Mr Matthews advised that there had been 2 Extraordinary Meetings, at which the Annual Accounts, and the Quality Accounts, had been approved by the Committee Management Executive Team Chair s Report There was nothing additional to report regarding the Management Executive Team Meetings Remuneration Committee Chair s Report The Chair advised that the Remuneration Committee had recently met and discussed the Chief Executive Officer s appraisal, and the VSM performance and remuneration for 2014/ Trust Wide Risk Register There had been no changes this month to the risks recommended by the Governance and Quality Committee or Finance and Performance Committee. Changes recommended at a recent Board Development meeting had been made to align the strategic risks with 2014/15 priorities: A new risk had been added, risk 225, with regard to insufficient resilience and skills in leadership, which may result in poorly engaged, de-motivated staff and poor service quality. 2 risks were merged, these were: - Risk STRAT 1 delay in clarity of current health care reforms and associated implementation leads to uncertainty with commissioners that affects the Trust s ability to deliver its agenda. - FT 14 inability to reactivate FT application, either due to local Trust issues, unsuccessful CQC assessment, or further unforeseen changes to the Monitor assessment process. Mr Matthews asked if the Board could be briefed on the mitigations and the timescales with regard to risk 225. Mr Graham advised that the independent investigation should be concluded during August and a report would be submitted to Trust Board. Dr Hill 11
16 The Chair requested that the Board also re-visit the fundamental criteria for risk scoring. It was agreed this would be carried out during a future Board Development meeting. Ms Edwards 259. LEADERSHIP, CULTURE, AND WORKFORCE Equality and Diversity Report Mr Singh entered the meeting. Mr Singh explained that equality and diversity work had been very successful over the past year. The Trust had been put on the map winning many awards. It had achieved NHS Employers Equality and Diversity Partners Programme Status 2013/14, and been awarded as an NHS Employers Personal, Fair, and Diverse Organisational Champion. The Trust were the only one in the West Midlands to get this award and other Trust s had been asking the organisation to share information regarding good practice with them. The Trust had also won the Gold Standard Award for Equality at the employer s network for equality and inclusion awards on 1 st July The Board congratulated Mr Singh on this achievement. The Trust was fully compliant with all legislation, and mandatory training compliance stood at 88%. Additional training had also been provided as requested by staff. The Trust had also achieved EDS 2 self assessment grading for 2014 and was fully complaint with quality objectives. Equality data for staff needed to be worked on. Confidence needed to be provided to staff that their data was secure and confidential. This was a problem for other organisations too. The Chair commended Mr Singh on behalf of the Board for his report and hard work, as well as the work of the Community Development Workers. He highlighted the star chart within the report as a good example of humanising data. The Board noted the progress made with equality and diversity within the Trust and approved the report. Mr Singh left the meeting Medical Directors Update Dr Gingell had no updates to provide to the Board STRATEGIC DEVELOPMENT AND DIRECTION Review of Annual Plan with BAF Quarter 4 Ms Edwards updated the Board on the report. All objectives were rated 12
17 green, with the exception of 2 which related to the Trust s Foundation Trust status. Ms Edwards apologised for the delay in submitting this report to Board, and advised that the quarter 1 report should come to Board in August. The BAF has previously always been reviewed at Finance and Performance Committee prior to submission to Board. However it had been proposed in future that it would be submitted directly to Board. It was agreed the BAF report would come directly to Trust Board in the future and actions directed back to Committees if required ANY OTHER BUSINESS No items of other business were raised DATE AND TIME OF NEXT MEETING Wednesday 6 th August 2014, 3pm, Canalside House, Walsall. Signature.. Date. Dr S Hill, on behalf of the Dudley and Walsall Mental Health Partnership NHS Trust Board 13
18

19 Board meeting date: 6 th August 2014 Agenda Item number: 3 Enclosure: 2 Title Summary of Confidential session of Trust Board held on 2 nd July 2014 Accountable Director: Author: Dr Hill, Interim Chairman Mandy Edwards, Interim Company Secretary CONTEXT AND BACKGROUND FOR REPORT Best practice in corporate governance requires that business considered in private session is reported into the public session as soon as possible. Given the arrangement of the Board meetings, the earliest opportunity is at the public session of the following month. This report outlines the business considered in private at the meeting of the Board held on 2 nd July KEY ISSUES FOR BOARD OF DIRECTORS CONSIDERATION AND DECISION Chair s Update The Chair commented on the Agile working pilot project and asked Board members for feedback. Despite some teething problems all members reported positively about the benefits. The Chief Executive Officer s (CEO s) overview The CEO provided an update to the Board which included: Foundation Trust Application Formal notification had yet to be received from Monitor/TDA, but a 1 st October 2014 re-activation was anticipated. Clinical Commissioning Group Partnerships Discussions had recently been held with Walsall CCG to raise the profile of mental health and a Board to Board meeting is arranged for September, with Executive pre-meeting beforehand. This forms part of the Board activities to enhance relationships with CCG s. Confidentiality Issue The Board were made aware that one of its commissioners had shared confidential contract information with competitor organisations. The concern had been raised with the commissioner and the Trust awaited a response. CIP and Service Transformation Report Mrs O Sullivan briefed the Board on the report, which included information on the following: The timing of CIP reports submitted to MExT had changed to a six weekly cycle therefore the Board would in future receive a written report on alternate
20 months and a verbal exception report for the intervening meetings, together with any relevant updates via Committee Chairs reports. No changes in finances or risks this month. Further work up of the next two years CIPs was being progressed. The MH Strategies Older Adults work and modelling of options will be discussed at MExT, then Board in September. Payment by Results Presentation The Board received a presentation on PbR timelines, milestones and the challenges faced prior to implementation. The following points were highlighted: Key risks identified included; potential for loss of income; accurate identification of active caseload; and MHMDS reporting of HONOS and Quality Indicator data from July. No definite date for implementation of PbR has been announced. An update will be provided to F&P Committee nearer September when there will more information regarding the future of PbR. Nurse Director Update It was noted that the Safe Staffing report had been presented at the extraordinary Board meeting the previous week. The approved report had been submitted and published on time and in accordance with the national directive. Medical Directors Update There were no updates to report to the Board by the Medical Directors this month. Occupational Health Future Service Provision The Board discussed options for the future provision of Occupational Health services but was not able to reach a final decision and requested additional information. An enhanced report was requested for presentation at the Board development session on 10 th July, where a decision would be made. Refresh of IT strategy and update on IT service provision Due to time constraints, this oral update was deferred to a future Board, as there were no decisions required and no urgent issues to bring to the Board s attention. For Assurance The Board noted the minutes of the Management Executive Team meeting held on 27 th May 2014, the Governance and Quality Committee meeting held on 14 th May 2014 and the Finance and Performance Committee held on 3 rd June Any Other Business No other business was raised. RECOMMENDATIONS The Board is invited to note the business transacted in the private session held on 2 nd July 2014.
21 Enc 3 MATTERS ARISING FROM PUBLIC MEETING Item No. Date Added Action Responsibility Due Date Update Integrated Dashboard nd July 2014 Mr Axcell to include a KPI on the Dashboard to show length of stay more accurately than at present, including Delayed Transfer of Care cases. Mr Axcell to check accuracy of 7 day follow up figures for inpatient discharges (figures did not appear correct as they all read the same and mirrored the whole Trust Dashboard figure). Mr Axcell Mr Axcell 6 th August th August 2014 In progress In progress Strategic Overview and Horizon Scan Paper nd July 2014 Ms Edwards to separate the news items from items which needed to be actioned for future reports. The Equality and Diversity Award to be acknowledged. Ms Ingram to include this in the staff recognition programme, perhaps recognising it at the staff awards. Ms Edwards Ms Ingram 6 th August th August 2014 Action complete nd July 2014 The Information Governance Committee to be added to the interfaces with other Committee s section within the Governance and Quality Committee Chair s Report. Ms Pugh/Dr Gutteridge 6 th August 2014 Action complete The outcome of the recent Clinical Coding Audit to be reported to the Board. Mr Axcell TBC
22 Ms Musson to update the narrative for the QGAF domains as specified by the Board. Ms Musson 6 th August 2014 Enc 3 Risk Register nd July 2014 Re: Risk 225 (insufficient resilience and skills in leadership, which may result in poorly engaged, demotivated staff and poor service quality). An independent investigation outcome to be submitted to a future Trust Board. Dr Hill TBC Fundamental criteria for risk scoring to be added to the Board Development Agenda for August. Ms Edwards 6 th August 2014 Action complete th June 2014 A report to be submitted to Trust board on the CQC Compliance Action Plan and the must, should and could do actions on a quarterly basis. Ms Pugh Sept th June 2014 Integrated Dashboard Mr Axcell to look in to benchmarking of reference costs against estates costs. Mr Axcell TBC 187 A Board to Board to be organised with the 2 CCG s to take place within the next 6 months. Ms Edwards Oct 2014 Walsall CCG B2B arranged for 16 th September Ms Edwards to keep the Board informed on progress th Nov 2013 A presentation to be given at a future Board Development meeting on research and development, including where the Trust is at present and where it intended to be in the future. Dr Gingell 25 th June th July 2014 Action complete. Update provided on the Research and Development position, including benchmarking against other Trusts, to the Non Executive Director s.
23 st July 2013 R&D investment and benchmarking against other Mental Health Trusts to be progressed via the Governance and Quality Committee once the R&D strategy has been presented to the R&D Committee. Dr Gingell 6 th August 2014 Enc 3 Action complete. Update provided on the Research and Development position, including benchmarking against other Trusts, to the Non Executive Director s. 160 A Review of the NHS Hospitals Complaints System, Putting Patients Back in the Picture Full picture and proposals regarding changes to the complaints process to be brought back to Trust Board in June. Ms Ingram 4 th June nd July th August 2014 On agenda for August.
24
25 Enc 4 REGISTER OF INTERESTS 6 th August 2014 CURRENT DIRECTORS Date of appointment to the Board Post Declared Interests Dr Stuart Hill Interim Chair/Non- Executive Director Michael Higgs Non-Executive Director David Matthews Non-Executive Director Dr Robin Gutteridge Non-Executive Director Lay Member Solicitors Disciplinary Tribunal Lay Member Chartered Institute of Management Accountants Disciplinary Committee Lay member - National Register of Public Service Interpreters Disciplinary Committee Independent Person Standards, Wolverhampton City Council Lay member RICS/IPA Fixed Charged Receivership Scheme Joint Regulation Committee Lay Member Financial Reporting Council Tribunals Panel Non-Executive Director of Extra Care Trust Nothing to declare Gill Cooper Non Executive Director Gary Graham Chief Executive Nothing to declare Consultant in Health and Wellbeing, Faculty of Education, Health and Wellbeing, University of Wolverhampton Chartered Psychologist: Full member Division of Teachers and Researchers Accredited Member of the British Association for Counselling and Psychotherapy (BACP) Member of the College of Sexual and Relationship Therapists (CoSRT) HCPC Registered Counselling Psychologist: Number PYL Trustee Frederick Pearson Fisher Charity Serving Justice of the Peace Dudley Bench Dr Kate Gingell Joint Medical Director Marsha Ingram Director of People and Corporate Development Wendy Pugh Director of Operations & Nursing Dr Mark Weaver Joint Medical Director Mark Axcell Director of Finance and Performance Nothing to declare Nothing to declare Nothing to declare Nothing to declare Trustee A Child of Mine Charity
26
27 Board meeting date: 6 th August 2014 Agenda Item number: 9 Enclosure: 5 Report Title: CEO Strategic Overview and Horizon Scan Accountable Director: Author (name & title): Purpose of the report: Gary Graham, Chief Executive Mandy Edwards, Interim Company Secretary This report summarises recent publications and information, which are of relevance or interest to the Trust. It sets out the key points in each publication and makes recommendations to the Board of any action the Trust plans to take. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources What impact or implications does this report have on any of the following: Quality & standards (inc. CQC/NHSLA) Patient safety & experience Financial (income, expenditure & CIP) Performance Workforce & Leadership Equality & Diversity Sustainability Risk Register/Board Assurance Framework Patient & Public Involvement Please give brief details:
28 Introduction This report provides a summary of recent information and news of interest and relevance to the Board making recommendations to the Board of any action the Trust has taken or plans to take. Summary of key points, issues and risks Summary of key areas for action: DWMH Mental Health Community Survey Management Report Monitor - NHS National Tariff Payment System 2015/16: engagement documents consultation Monitor - NHS Foundation Trusts: Code of Governance updated DoH - Changes to Mental Health Act (1983) Code of Practice consultation Requirements for Registration with the CQC - changes to standards for CQC registration and introduction of Duty of Candour and fit and proper persons requirement for directors. NHS England - Friends and Family Test to roll out to all NHS services NHS Workforce Bulletin - New staff engagement case studies NHS England - takes action to improve access to specialised mental health services for children & young people The Complainants Survey - Complainants User Survey developed to help organisations gain assurance about complaints handling process and improve how the service is delivered. NHS Benchmarking Network: Four new data collections - Learning disabilities for Commissioners; Older people in acute settings; Pharmacy Services; Corporate Functions. The Pursuit of Happiness: A new ambition for our mental health - aims to address issues within Mental Health and sets out values, principles and approaches to mental health. Recommendation for future Action Responsible person Presentation to MExT in September, Director of People & following which results and action plan Corporate Development will be reported to the Board as part of Q2 SED report. Feedback from Monitor consultation Director of Finance and event on 24 th July will be reported to Performance Board in September. Review Code of Governance and Company Secretary inform September Board of any changes which impact the Trust. Review implications and respond to Director of Operations, consultation if appropriate. Nursing & Estates Review guidance and bring report to Director of Operations, September Board outlining implications Nursing & Estates and and actions. Director of People & Corporate Development Review guidance and opportunities for improving current practice. Review and consider adoption of any new approaches. For information and consideration of any implications for the Trust regarding Tier 4 CAMHS. Consider whether to participate in project. Consider participation in and/or outcomes from relevant projects. Consider the impact on the Trust s strategy and objectives. Director of People & Corporate Development Director of People & Corporate Development Strategic Planning Manager Director of People & Corporate Development Director of Finance, Performance & IM&T All Directors
29 Recommendation It is recommended that the Board note and discuss the information contained within this report and consider the proposed actions. Board action required The Board is asked to: Agree the recommended actions and nominated leads identified within the report.
30
31 Strategic Overview and Horizon Scan Report July 2014 This report summarises recent important publications and information items, setting out the key points of each item and making recommendations to the Board of any action the Trust has taken or plans to take. Trust Internal News Evaluation of the financial impact of Seven Day Service NHS England have asked Deloittes to do a piece of work to evaluate the financial impact of Seven Day Service across number service areas including Urgent and Emergency Care, planned care, community and social care. This will include an appraisal of the impacts of increased service levels across different settings of care by identifying the clinical, reconfiguration, workforce and financial components related to increased access to care. The methodology will involve significant stakeholder engagement, service definitions, impact assessments as well as financial modeling Mental Health Community Survey Management Report The National Service User Survey was undertaken for Dudley and Walsall Mental Health Partnership NHS Trust between February and June The results will be presented to MExT in September and an action plan will then be reported to the Board. Monitor Website link: NHS National Tariff Payment System 2015/16: engagement documents Monitor and NHS England are in the process of developing the 2015/16 National Tariff Payment System. They are currently consulting on this which closes on 15 th August 2014 and would like views on the following The approach to setting prices for 2015/16 The impact of the proposed changes to the National Tariff The proposals for local payment arrangements The approach to enforcing the National Tariff Healthcare providers and commissioners are encouraged to respond to these proposals in order to influence the final national tariff which will be published later in the year. More information can be found at: Recommendation for future Action For information Presentation to MExT in September, following which results and action plan reported to the Board as part of Q2 SED report Recommendation for future Action Feedback from Monitor consultation event on 24 th July will be reported to Board in September. Responsible person Director of People & Corporate Development Responsible person Director of Finance and Performance
32 system engagement-documents Annual Plan 2014/15 Monitor published its 2014/15 annual plan on 20 th June and they state that: Monitor's annual plan encourages NHS providers to develop new ways of working and to take controlled risks in order to improve patient care. The full publication can be found at: NHS Foundation Trusts: Code of Governance Monitor updated its Code of Governance on 4 th July. The full publication can be found at: Annual Report and accounts for 2013/14 Monitor published its 2013/14 annual report & accounts on 14 th July. The full publication can be found at: NHS foundation Trusts: consolidated accounts 2013/14 Monitor published its NHS foundation trusts: consolidated accounts 2013/14 on 17 th July and the accounts presented in this report have been prepared from a consolidation of the audited accounts submitted by the 147 individual NHS foundation trusts which were authorised by Monitor prior to 31 March The full publication can be found at: Department of Health (DoH) Website link: The Dementia Challenge link on the website has news which includes: Slides from the Global Dementia Legacy Event A news article that research has concluded that 1 in 3 cases of Alzheimer s could potentially be prevented by addressing factors that increase the risk of developing the disease. Changes to Mental Health Act (1983) Code of Practice: Launch of Open Consultation. The DoH are seeking comments on proposed changes to legislation governing the treatment of people with mental health problems. The consultation closes on 12 th September 2014 The draft Code includes new chapters on: The Care Programme Approach Equality, human rights and parity of esteem For information Review Code of Governance and Board to be informed of any changes which impact the Trust For information For information Recommendation for future Action For Information Review implications and respond to consultation if appropriate. Company Secretary Responsible person Director of Operations, Nursing & Estates
33 Mental capacity and deprivation of liberty Victims More information can be found at: Requirements for Registration with the CQC In July 2014 the DH published their response to 3 separate consultations on changes to fundamental standards of CQC registration requirements, the Duty of Candour and the fit and proper persons requirement for directors. The DH state that CQC will "require providers to be taking steps to ensure that there is good organisational management and leadership in place to encourage and support staff to be open with service users and to drive a culture change towards more openness and transparency". The DH refers to the National Patient Safety Agency's 'Being Open' guidance which suggests providers should take the following steps to implement a policy, and culture, of candour: Create or review and strengthen local policies identifying how to communicate with patients where serious injury or death has occurred; and ensure this policy is embedded with the organisation s wider risk management processes Boards should make public commitments to implementing a policy of candour Providers should have named executive and non-executive leads responsible for candour Publicise the new policy with staff and provide advice and training to staff on managing patient safety incidents Publicise information on the support systems currently available for staff distressed by patient safety incidences It has been decided to introduce the measures in sequence: October 2014 Duty of Candour and fit and proper persons requirement introduced for NHS bodies only April 2015 fundamental standards introduced for all providers April 2015 Duty of Candour and fit and proper persons requirement extended to all CQC-registered providers The consultation response document can be found at: file/327561/consultation_response.pdf NHS England Website link: NHS England takes action to improve access to specialised mental health services for children & young people On 10 th July it was published that NHS England is taking urgent action to improve access to specialised inpatient mental health services for children and young people after publishing a frank and honest report on current provision. Review guidance and bring report to September Board outlining implications and actions. Recommendation for future Action For information and consideration of any implications for the Trust regarding Tier 4 CAMHS. Director of Operations, Nursing & Estates (fundamental standards) and Director of People & Corporate Development (Duty of Candour & fit and proper persons) Responsible person Strategic Planning Manager
34 For England as a whole, the report says it is impossible to conclude definitively whether the current level of bed provision is sufficient to meet the need. Further information can be found at: Friends and Family Test to roll out to all NHS services NHS England has published comprehensive updated guidance for use by hospital trusts in helping them to implement the Friends and Family Test most effectively. NHSE has decided to move away from a net promoter score and will test alternative presentation methods with the aim to have the new methodology in place during the autumn. The guidance can be found at: NHS Workforce Bulletin Issue July 2014 New staff engagement case studies NHS Employers has been working with three NHS organisations to profile particular aspects of their approaches to engagement. Some of the key outcomes include, major improvements in national staff survey results, reductions in sickness absence and staff feeling more valued. The full study can be found at: Foundation Trust Network (FTN) Full newsletters can be obtained from mandy.edwards@dwmh.nhs.uk June Issue 57 Main highlights: Patient safety campaign launched NHS rated as best healthcare system in the world July Issue 58 Main highlights: NHS England announce CAMHS beds increase (as mentioned in NHS England section) CQC publish their annual report and accounts Mental Health Foundation Website link: Social contact, peer support and self-help can positively benefit people with dementia. Review the guidance and consider any opportunities for improving current practice Recommendation for future Action Review and consider adoption of any new approaches Recommendation for future Action For information For Information Recommendation for future Action For Information Director of People & Corporate Development Responsible person Director of People & Corporate Development Responsible person Responsible person
35 The Mental Health Foundation have released its results and evaluation of their dementia self-help project. This found a positive impact of the peer support groups on participants wellbeing, social support and practical coping strategies. Participants improved in their communication abilities and in managing their memory and their lives. It also revealed benefits extending beyond group members to include staff, families, friends, other residents in the housing scheme and the housing provider. The full report and recommendations can be found at: dementia-selfhelp/ NHS Benchmarking Network Website link: National Association of PICU conference Takes place at the University of Birmingham, 4 September, 2014 The Benchmarking Network team will be presenting on 'How different is quality performance between PICUs'. The Complainants Survey NHS Benchmarking Network have launched a new partnership project with the Patients Association on complaints handling. The Patients Association has developed a Complainants User Survey which can help organisations gain assurance about their complaints handling process and also improve how the service is delivered. This project fee will be based on the number of complaints received per annum and will be in the range of 3-6,000 per participating organisation. Further information & registration details at - Four new data collections Learning disabilities for Commissioners - stock take of current provision, quality and access and will be a first strategic view for the NHS on how care is planned and delivered for people with a learning disability. Older people in acute settings - project will consider pathways for older people through secondary care from A&E through to short term assessment units, elderly care wards and supported discharge processes. Links with other sectors including primary care, community, mental health and social care particularly at the front and back end of hospitals will be of particular interest. Pharmacy Services - runs parallel to the Medicines Management project and will compare pharmacy services across acute, community and mental health settings. Initiation event held on 20th June. The content of the project is currently being finalised and is likely to include; workforce and skills, infrastructure, finance and activity, policies and procedures, quality, medicines optimisation, audit, integration with primary care, and good practice case studies. Recommendation for future Action For information Consider whether to participate in project Consider participation in and/or outcomes from relevant projects Responsible person Director of People & Corporate Development Director of Finance, Performance & IM&T
36 Corporate Functions - one of the longest running and most successful projects providing the most comprehensive dataset of NHS back-office and corporate activities available to the NHS. The project can be confidently used by members as a point of reference to make evidence based decisions of the effectiveness, value, and strategic fit of NHS corporate activities. Data collection will commence in September and run through October letters/newsletterjune2014.pdf CentreForum Commission Website link: The Pursuit of Happiness: A new ambition for our mental health. Published July 14 the aims of CentreForum Mental Health Commission are to address issues within Mental Health, specifically: Examine the current state of mental health in England; Set out values, principles and approaches to mental health; Evaluate the effectiveness and progress made in delivering the implementation framework for the government s mental health strategy, No Health Without Mental Health; and Identify, and provide effective solutions based upon key policy issues in this area, looking towards The document states that Following a year-long evidence-based commission, this report sets out the responses to the challenges faced in mental health over the next five years. The Commission believes that it is vital in the next Parliament that mental health policy includes a more ambitious objective for investing in the wellbeing and mental and social capital of the nation. In achieving this, there should be a focused agenda that recognises and enhances the strengths and assets of our communities. The report makes many recommendations in the following areas, with a dedicated chapter for each area: Communities Families Schools Workplace Health and Social Care Making it happen The report concludes that, The Commission goal was to set out a new ambition for the nation s mental health by A major change in approach is needed. The change goes well beyond the confines of the NHS. The full document, can be found at: Recommendation for future Action Consider the impact on the Trust s strategy and objectives. Responsible person All Directors
37 Board meeting date: 6 th August 2014 Agenda Item number: 10.1 Enclosure: 6 Report Title: Trust Integrated Performance Dashboard Month 3 (June 2014/15) Accountable Director: Author (name & title): Mark Axcell - Director of Finance and Performance James Parker Commissioner Liaison Manager Purpose of the report: To update the Board on all aspects of Trust performance at month 3 of 2014/15 Quality and Safety Service User Experience Efficiency Resources Monitor and Trust Development Authority Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Committee: Governance and Quality Committee considered elements from within the Quality and Safety domain, and the Service User Experience domain. Finance and Performance Committee considered elements from within the Quality and Safety domain, Efficiency Domain, Resource Domain and the Service User Experience domain. MExT members have reviewed the data and contributed to the supporting narrative. Date reviewed Governance and Quality Committee 9 th July 2014 Finance and Performance Committee 28 th July 2014 Key points or recommendations from Committee:
38 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources What impact or implications does this report have on any of the following: Caring Responsive Effective Well-led Safe Please give brief details: The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources
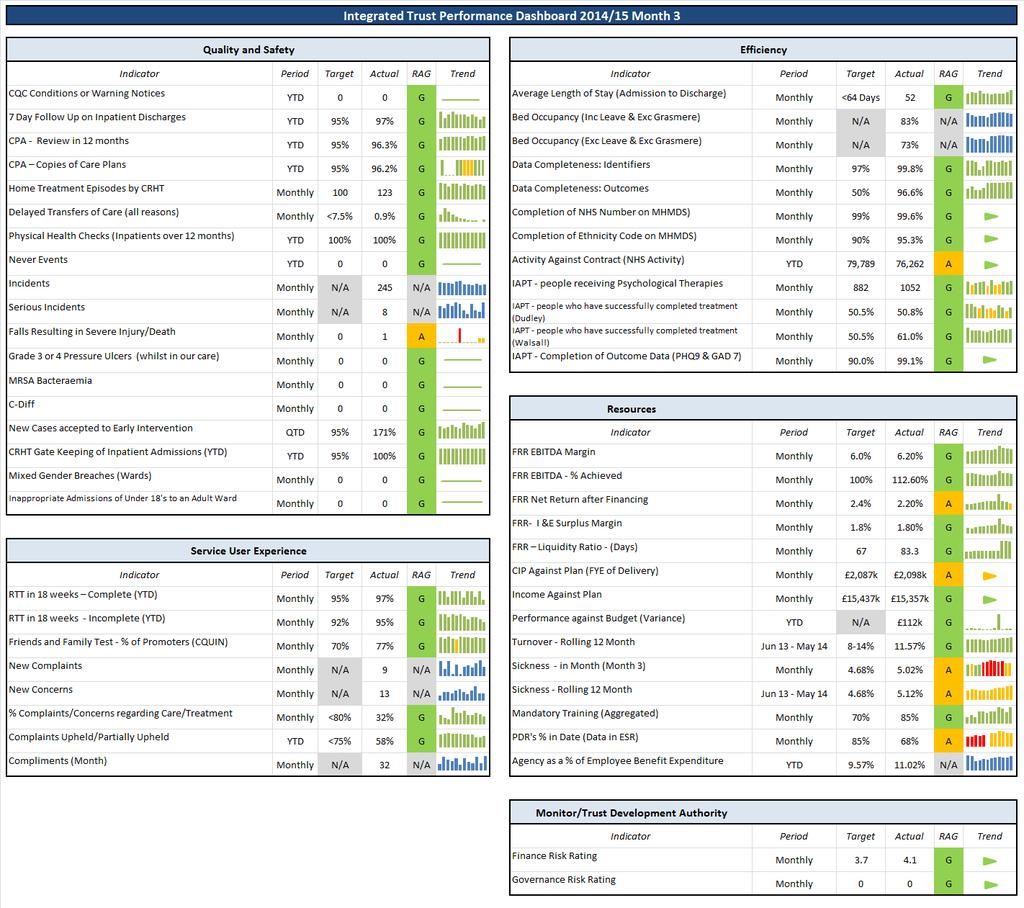
39 Title Trust Integrated Performance Dashboard Month 3 (June) 2014/15 Introduction This paper presents the Trust s performance at the end of month three 2014/15 financial year. The 2014/15 Integrated Dashboard allows comparison and triangulation across Quality and Safety, Service User Experience, Efficiency, and Resources to give a comprehensive picture of the performance of the Trust. The 2014/15 Integrated Dashboard also includes performance, and exception commentary, by service line, so that the Board is better able to see achievements as well as any adverse performance within the overall aggregate level. Summary of key points, issues and risks Sickness - The in-month Trust sickness absence rate for month three still remains above the threshold (4.68%) at 5.02%. This is an increase from month two of 0.01%. The overall finance risk rating for the month remains green with a score of 4.1. The overall governance risk rating for the month remains green with a score of 0. Further detail Please se attached Integrated Performance Dashboard and underpinning Performance, Finance, Quality Governance and Workforce reports. Recommendation It is recommended that the Board note the performance of the Trust as at month twelve and debate accordingly. Board action required The Board is asked to receive the report for information and assurance
40
41 Trust Integrated Performance Dashboard Month 3 (June) Presented at Trust Board on 6 th August2014
42
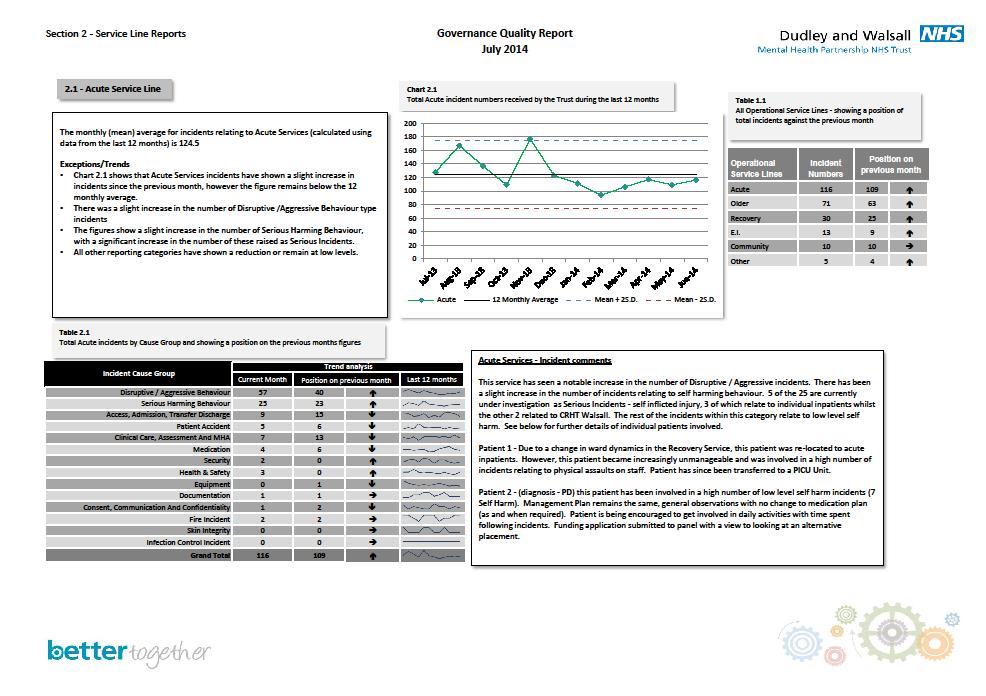
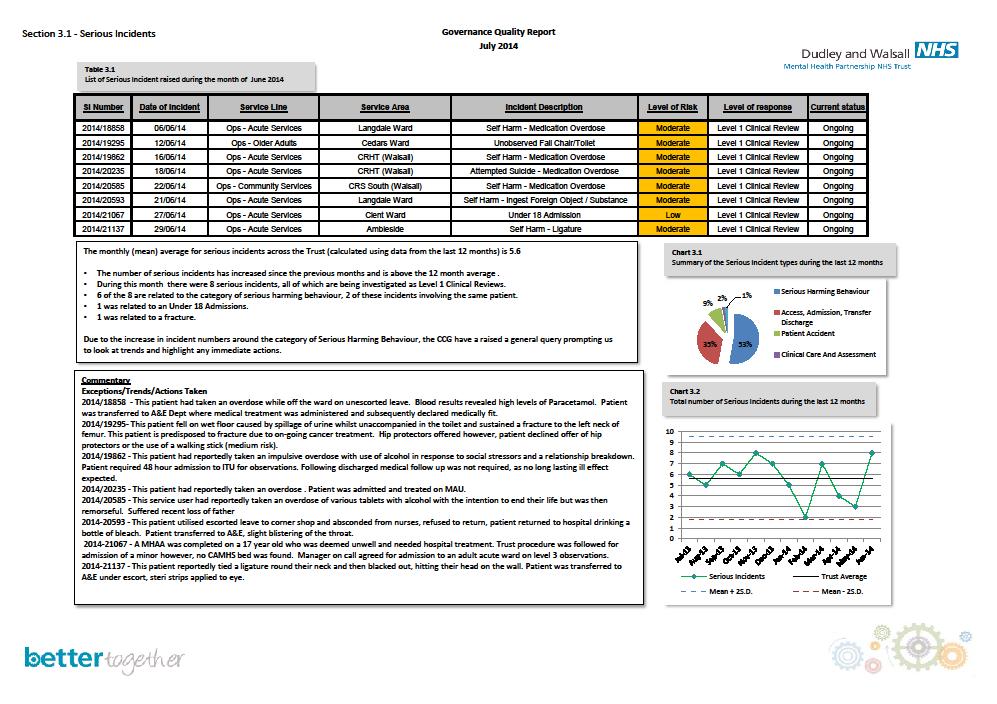
43 Trust Level Integrated Dashboard Exception Commentary Quality and Safety Domain Serious Incidents (SIs) - There have been eight Serious Incidents reported during month three, which is slightly above the 12 month average. All of the SIs are being investigated as Level 1 Clinical Review, with six being in relation to serious harming behaviour, one under 18 admission, and one fracture due following a fall. Copies of Care Plan During month three, the performance against this measure has improved and continues to achieve over the threshold. This continues to be closely monitored, to sustain compliance. Efficiency Domain Completion of Ethnicity Codes This indicator is a newly mandated requirement for the 2014/2015 Standard NHS Contract. At month two the Trust reported performance of 81.2% against a target of 90.0%. At month two plans were put in place to look at these exceptions and in month three we are now reporting 95.3%. Activity against contract (NHS Activity) For month three the Trust has reported 76,262 units of activity against a target of 79,789 year to date. It is worth noting that this figure is cumulative and the Trust over achieved within the month of June. However a watching brief is still advised going forward. Resources Domain Cost Improvement Programme (CIP) - The Trust s CIP target for the year is 2,087k. The in year achievement of CIP is forecast at 1,866k which leaves 221k to be managed centrally through uncommitted reserves. The full year recurrent effect of these schemes is 2,098k, representing a recurrent 11k planned overachievement. The indicator is rated amber as a reflection of the work on-going to deliver the full year effect of the 2,087k plan. Trust income has fallen to 80k below the plan at Month 3 relating to under achievement on out of area SMS activity and slippage on the establishment of the new detox bed provision at Bushey Fields. The Trust Reserves have an uncommitted balance of approximately 600k. Sickness - The in-month Trust sickness absence rate for month three still remains above the threshold (4.68%) at 5.02%. The in month sickness figure has been above the threshold for eight consecutive months, which is causing an increase in the rolling twelve month average, from 5.04% in month two to 5.12% in month three. Whilst all sickness levels and compliance with the policy continues to be closely monitored by managers across service lines, and supported by HR colleagues, a watching brief is advised, given that there has been an increase in long term episodes of sickness. Regular case review meetings have been arranged with Occupational Health for all of the long term episodes. Appraisal Data Capture has remained at 68% for months two and three and still remains below the threshold. A targeted approach has been used to ensure that the importance of staff appraisals and the capture of data is a priority. Executive Directors and Heads of Service have received reports on individual staff regarding appraisal compliance. A new data capture form has been made available to ensure all relevant data is captured and uploaded onto ESR.

44 Service Line Summary Activity against contract has seen underperformance during month three against the target. This service line has underspent against budget by 68k in June 2014, of which 46k relates to CRHT vacancies. Wards have underspent by 7k in the first Quarter, following a spike in ward costs in March (which had resulted from a temporary restriction of Kinver ward staff duties). Sickness levels have decreased for month three (5.19%) from 5.30% (month two). This was due to a lower number of short term sickness cases.
45 Community Performance Dashboard 2014/15 Month 3 Quality and Safety Efficiency Indicator Period Target Actual RAG Trend Indicator Period Target Actual RAG Trend CQC Compliance YTD 0 0 G Activity Against Contract (NHS Activity) YTD 18,145 15,491 A 7 Day Follow Up on Inpatient Discharges (YTD) YTD 95% 97% G CPA - Review in 12 months YTD 95% 96.2% G Resources CPA Copies of Care Plans YTD 95% 96.5% G Indicator Period Target Actual RAG Trend Never Events YTD 0 0 G Income Against Plan Monthly 2,191k 2,188k G Incidents Monthly N/A 10 N/A Performance against Budget (Variance) Monthly N/A 5k G Serious Incidents Monthly N/A 1 N/A Turnover - Rolling 12 Month Jun 13 - May % 8.57% G Falls Resulting in Severe Injury/Death Monthly 0 0 G Sickness - in Month (Month 3) Monthly 4.68% 4.50% G Grade 3 or 4 Pressure Ulcers (whilst in our care) Monthly 0 0 G Sickness - Rolling 12 Month Jun 13 - May % 5.08% A MRSA Bacteraemia Monthly 0 0 G Mandatory Training (Aggregated) Monthly 70% 91% G C-Diff Monthly 0 0 G PDR's % in Date (Data in ESR) Monthly 85% 84% A Agency as a % of Employee Benefit Expenditure YTD TBC 10.15% N/A Service User Experience Indicator Period Target Actual RAG Trend Friends and Family Test - % of Promoters (CQUIN) Monthly N/A 80% N/A New Complaints Monthly N/A 1 N/A New Concerns Monthly N/A 3 N/A % Complaints/Concerns regarding Care/Treatment Monthly <80% 50% G Complaints Upheld/Partially Upheld YTD <75% 100% A Compliments (Month) Monthly N/A 3 N/A Service Line Summary Whilst activity has seen an increase during month three, it still remains below the contracted target. Plans were put in place from month two to monitor this in greater detail and we expect to see an improvement. Community Services are close to break-even up to June There are 7 WTE agency workers within the CRS teams, to manage the existing caseloads. The part year CIP target of 281k, with effect from July 2014, is set to slip by 3 months until the structure is finalised, causing a forecast underspend of 95k for the service line at year end. Sickness levels within the community service line have seen an increase for month three (4.50%), from 2.87% (month two), this means the service line still remain within the threshold for sickness in month, and due to the improvement the service line is only slightly under the threshold for the rolling 12 month.

46 Service Line Summary CPA Copies of Care Plan Month three has seen an increase against this indicator for Early Intervention and are now above the threshold. It is important to note that the service carries a caseload of small numbers which distorts the percentage. However there will be a continued focus Trust wide to ensure we sustain compliance. Early Interventions had an underspend of 13k to June There are an existing number of vacancies within Walsall CAMHS LD which are progressing through the recruitment process. All old year CIP schemes for 13/14 have been delivered from April This service line has a full year CIP target of 80K for 14/15 which is expected to be met, pending the approval of the skill-mix changes within the CAMHS teams and removal of some vacant positions. Sickness levels have increased for Month three (7.34%) and this service is now above the threshold (4.68%) for the second consecutive month. This is driven by episodes of long term sickness within the service line.
.")
47 Service Line Summary This service line has overspent against budget by 26k in June This comprises an overspend of 44k on inpatient services, net of an underspend on community areas (the latter resulting from vacancies). The inpatient overspend results from the use of temporary staffing in excess of funded vacancy levels an increase in costs occurred on Linden ward for the last couple of months, due to a number of patients on high observation levels. Sickness levels within Older Adults service line have decreased for month three (8.09%), from 9.99% (month two) but still remain above the threshold and the rolling 12 month continues on an upward trend. CPA Copies of Care Plan This service line has improved recording and is now above the agreed threshold. Activity against contract has seen an increase in performance during month three against the target.

48 Service Line Summary Recovery is break-even for April-June Cost pressures remain from last year within EAS where there are 2.00 WTE agency workers unfunded to manage assessments. This has been offset by a number of vacancies within Walsall SMS. The high amount of turnover reported in month three, is driven by the TUPE of Dudley Substance Misuse employees. Month three has seen an increase in sickness and are now above the threshold but due to strong performance previously this service are still within the threshold for the rolling 12 month target.
49 Trust Performance Report Month /15 1
50 Contractual KPIs, month 3 KPI Target Loc Apr May Jun July Aug Sept YTD RAG 1. New cases Trust 89 accepted to EI - Target Cumulative Trust Trust Actual Target Dudley Actual Target Walsall Actual KPI Target Loc Apr May Jun July Aug Sept YTD Actual 2. Gate-keeping of 100% 100% 100% inpatient admission * 95% Trust 100% (67/67) (76/76) (65/65) 95% Dudley 100% 100% 100% 100% 95% Walsall 100% 100% 100% 100% 3. 7 day follow up on 97% 95% 97% Inpatient discharge * 95% Trust 96% (89/92) (99/104) (82/84) 4. DToCs (All reasons) <7.5% 5. Average length of stay * 95% Dudley 95% 95% 98% 96% 95% Walsall 100% 95% 97% 97% Trust 0.7% 0.0% 0.9% (30/4510) (1/4701) (42/4447) <7.5% Dudley 0.0% 0.0% 0.6% 0.2% <7.5% Walsall 1.5% 0.04% 1.3% 0.9% <64 days Trust <64 days Dudley % RAG <64 days Walsall Users with a copy of their care plans * 95% Trust 95% 95.4% 96.2% 95% 95% Dudley 95% 95.4% 96.2% 95% 95% Walsall 95% 95.4% 96.2% 95% 2
51 Contractual KPIs, month 3 KPI Target Loc Apr May Jun July Aug Sep YTD Actual 7. CRHT HT episodes * 1187 Trust Inappropriate admissions of under 18s to an adult ward* 8a. Appropriate admissions of Under 18s to Adult Ward 9. % of patients seen in 18 weeks Complete / incomplete 10. Physical health checks for inpatients more than 12 months 11. Completion of NHS number on MHMDS 12. Completion of ethnicity code on MHMDS (100/mth) 579 (49/mth) 608 (51/mth) Dudley Walsall 0 Trust Dudley Walsall No target Trust %/ 92% Trust 95% /92% Dudley 95%/ 92% Walsall 70 98% 100% 97% 98% 98% 97% 95% 97% 98% 100% 96% 98% 99% 96% 94% 96% 100% 100% 100% 100% 97% 98% 97% 97% 100% Trust 100% 100% 100% 100% 100% Dudley 100% 100% 100% 100% 100% Walsall 100% 100% 100% 100% 99% Trust % 99.6% 99.6% (8463/8502) (8848/8880) (9072/9108) 99% Dudley 99.5% 99.6% 99.6% 99.6% 99% Walsall 99.5% 99.6% 99.6% 99.6% 90% Trust 81.9% 90.1% 95.3% (6959/8502) (8078/8880) (8680/9108) 90% Dudley 81.9% 90.1% 95.3% 89.5% 90% Walsall 81.9% 90.1% 95.3% 89.5% % 89.5% RAG 3
52 Contractual KPIs, month 3 KPI Target Loc Apr May Jun July Aug Sept YTD Actual 13. IAPT - number of people who receive (882/mth) Trust psychological therapies - attending 4825 one session only (402/mth) Dudley (480/mth) Walsall IAPT - People who have successfully completed treatment 50.5% Dudley 50.8% 34.6% 50.8% 46.0% 50.5% Walsall 62.8% 59.2% 61.0% 61.1% RAG 15. IAPT - completion of outcome data PHQ9 and GAD7 90% 90% Trust 99.1% 99.1% 99.1% (334/337) (341/344) (328/331) 99.1% Dudley 100% 99% 99% 99.6% 90% Walsall 98.3% 98.9% 98.9% 98.7% 4
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69 2014/15 DWMHPT Finance Report Month 3 28
70 2014/15 DWMHPT Finance Report Month 3 Page Key Messages 3 Overall Summary and RAG Assessment 4-5 Trust Income Statement: Functional Analysis 6-9 Capital Programme 10 Activity and Income 11 Financial Performance Metrics 12 TDA Key Financial data: Month 3 13 Cash Flow Statement 14 Debtor and Creditor Performance 15 Workforce Cost Improvement Target Achievement 19 Statement of Financial Position (Balance Sheet) 20 29
71 Key Messages Financial Position The Trust has delivered a year to date surplus in Month 03 of 291k. This is 112k ahead of the planned surplus for the year to date. CIP plans delivered for 2014/15 The Trust s Cost Improvement Target for the year is 2,087k. As at Month 03 approximately 1.9 million of savings have been identified. The full year effect of the schemes being implemented is 2,098k. Income 2014/15 outturn There is still some initial slippage against the NCA target, but this expected to recover in future months. There has been a delay in re-establishing the detox beds in Bushey Fields Hospital, which has resulted in some slippage, but admissions have started and the Trust has achieved 10k income in the first two weeks. It is unlikely that the Trust will receive any income for cross border activity in relation to Dudley SMS. Bank, Agency and Locum spend continues to receive close management There is some overspending in Older Adults wards, but at present this is more than offset by underspending in Acute services. In Medical Services there are 7.90 high cost agency locums. This is planned to reduce over the coming year. 30
72 Overall Summary and RAG Assessment Statement of Comprehensive Income - Financial Position to 30th June 2014 Annual In Month Year To Date Plan Plan Actual Variance Plan Actual Variance Income Revenue From Activities Revenue-NHS Clinical 59,178 4,934 4, ,796 14,784 (12) Revenue-Non NHS Clinical 2, (16) (69) Total Revenue From Activities 61,740 5,147 5,144 (2) 15,437 15,357 (80) Other Operating Revenue Revenue-Education & Training 1, Revenue NHS Non-Clinical Other Revenue (2) (8) Revenue-Employee Benefits Total Other Operating Revenue 2, Total Revenue 64,352 5,389 5, ,097 16,090 (7) Expenditure Pay (46,795) (3,872) (3,719) 153 (11,559) (11,814) (255) Clinical Supplies and Services (1,985) (126) (113) 13 (464) (446) 18 Other Costs (11,263) (1,001) (1,131) (130) (2,945) (2,609) 336 Expenditure Reserves (666) (95) (148) (53) (242) (223) 19 Total Operating Expenditure (60,710) (5,093) (5,109) (18) (15,210) (15,091) 119 EBITDA 3, Depreciation (1,278) (108) (108) 0 (320) (320) 0 Amortisation (244) (23) (23) 0 (61) (61) 0 Net Operating Surplus 2, PDC (1,352) (113) (113) 0 (338) (338) 0 Interest Receivable Net Surplus /(Deficit) Technical Adjustment Technical Surplus Commentary Revenue Position The Trust is reporting a Month 03 surplus 291k, which is 112k ahead of plan. This achieves a Monitor metric of 4.10 for the year end position, against a plan for the year of Key message The Trust is ahead of plan to achieve its planned annual surplus of 808k. CIP 2014/15 Delivery Most CIP targets been devolved to the appropriate management levels. Cash The Trust s cash balance has seen a small reduction from 13,649k at the end of Month 02 to 14,376k at the end of Month 03. Capital Total capital expenditure to the end of month 03 was 148k. Budgetary Reserves Trust recurring reserves have been committed to meet non recurring cost pressures in 2014/15, 31
73 Overall Summary and RAG Assessment Continued 900 Run Rate 2014/15 3,000 Capital Programme 2014/15 ' Cumulative Budgeted Planned Run Rate Actual Run Rate '000 2,500 2,000 1,500 1, Cumulative Planned Spend Cumulative Actual Spend 0 0 CIP 2014/15 Actual vs Forecast Cash 2013/14 and Beyond 15,000 Transacted full year value 2,098 14,000 Transacted part year effect 1,820 13,000 12,000 CIP Target 2,087 11, ,000 2,000 3,000 '000 Actual Cash Forecast Cash Cash Benchmark 32
74 Trust Summary Income & Expenditure Statement Including Functional Analysis Annual Plan In Month Year to Date FOT M /15 Plan Actual Variance Plan Actual Variance Var '000 '000 '000 '000 '000 '000 '000 '000 NHS Revenue-Activities 59,178 4,934 4, ,796 14,784 (12) (26) Revenue from LAs 2, (16) (68) (119) Total Revenue from Activities 61,740 5,147 5,145 (3) 15,437 15,357 (80) (145) Commentary The Trust is reporting a surplus to Month 03 of 291k, which is 112k ahead of plan. There are risks around relating to non NHS income: slippage on detox beds, non recovery of out of areas SMS activity and under performance against NCAs. Corporate Functions Corporate Departments (12,290) (1,033) (1,077) (44) (3,034) (3,107) (73) (139) Central Reserves (666) (95) (148) (53) (242) (223) Total Corporate Functions (12,956) (1,128) (1,225) (97) (3,277) (3,330) (54) 30 Operational Services Total Acute & Older Adults (18,315) (1,531) (1,438) 93 (4,581) (4,373) Total Community Services (15,339) (1,302) (1,296) 5 (3,905) (3,883) 22 (45) Medical Services (13,010) (1,023) (1,010) 13 (3,169) (3,153) 16 0 Total Operational Services (46,664) (3,855) (3,744) 111 (11,654) (11,408) Total Expenditure (59,620) (4,982) (4,969) 13 (14,931) (14,738) Sub Total 2, Interest Receivable (0) PDC Dividend (1,352) (113) (113) 0 (338) (338) 0 0 There are corporate cost pressures in Estates and Performance and IT. The increased expenditure in Older Adults at the end of 2013/14 has not continued, and vacancies in Acute and Older Adults Community teams have resulted in an underspend of 115k in Acute and Older Adults Services. As at Month 03 the Trust s cash balance is higher than planned, even when MARS and PDC payments are factored into the forecasts. As a result of this it is likely that PDC will be approximately 50k less than planned, although this is not reflected in the forecast at present. The forecast outturn is in line with plan. Net Surplus/(deficit) (0) Technical Adjustment Technical Surplus (0) 33
75 Trust Income Statement Income Annual Plan In Month Year to Date FOT M /15 Plan Actual Variance Plan Actual Variance Var '000 '000 '000 '000 '000 '000 '000 '000 Revenue From NHS Activities Dudley CCG 27,048 2,254 2, ,762 6, Walsall CCG 27,378 2,282 2,282 (0) 6,845 6,845 (0) 0 NHS Walsall Sandwell & West Birmingham CCG 2, (0) 0 Wolverhampton CCG (0) (0) Birmingham Cross City CCG (0) (0) (0) Birmingham South Central CCG (0) South East Staffs & Seisdon CCG Cannock Chase CCG (0) (0) 0 Stafford & Surrounds & E Staffs CCGs (0) 1 1 (0) (0) Total Staffs CCGs (0) (0) (0) Redditch & Bromsgrove CCG Wyre Forrest CCG Total Worcester CCGs Budget for Under Recovery (30) (3) 0 3 (8) (7) 1 (2) NCAs (13) (24) CAMHs Deaf 1, (0) Total NHS Revenue-Activities 59,178 4,934 4, ,796 14,784 (12) (26) Revenue - Local Authorities Walsall MBC 2, Dudley MBC (0) (0) 0 Sandwell MBC (7) (12) (87) Wolverhampton MBC (2) 5 0 (5) (20) Stafford MBC (1) 3 0 (3) (12) Detox Beds (7) 51 2 (49) 0 Dudley CRI NCA - Other HC Total Revenue from LAs 2, (16) (68) (119) Commentary The Trust has negotiated block contract agreements with its host and neighbouring CCGs, which reduces the risk of in year loss of income, but equally limits the scope for over performance. There is normally a lag in receiving data on NCA activity, but this is expected to catch up in the coming months. The budget for income from Dudley MBC has been reduced to reflect the loss of the SMS contract. This has also resulted in an interruption in the provision of the detox. Service at Bushey Fields. The Trust experienced difficulties in 2013/14 in getting paid for out area patients accessing our SMS services. The loss of the SMS contract means that there will not be income against the non host Councils. Total Revenue from Activies 61,740 5,147 5,145 (3) 15,437 15,357 (80) (77) 34
76 Trust Income & Expenditure Statement- Corporate Functions Corporate Functions Annual Plan In Month Year to Date FOT M /15 Plan Actual Variance Plan Actual Variance Var '000 '000 '000 '000 '000 '000 '000 '000 Chief Executive (838) (70) (62) 8 (209) (184) Corporate Affairs (952) (65) (56) 9 (194) (185) Corporate Human Resources & Dev. & People (1,545) (129) (124) 5 (386) (374) Corporate Medical (974) (81) (87) (6) (243) (260) (17) (68) Corporate Estates (2,602) (217) (246) (30) (651) (714) (63) (87) Corporate Operations (2,029) (169) (159) 10 (507) (482) Corporate Finance (1,232) (127) (127) 1 (328) (297) Corporate Performance & IT (2,118) (175) (216) (41) (515) (611) (96) (171) Total Corporate Functions (12,290) (1,033) (1,077) (44) (3,034) (3,107) (73) (139) Commentary Corporate Estates The CIP target for POD055 and POD063 has slipped further but plans are in place to deliver from the renewal of contracts and efficiency within our current contracts. Pilots for cleaning services are anticipated to make efficiency but await confirmation of roll out across the Trust. CEO budget has an under spend due to slippage on recruitment to MH PbR posts. IT costs include ISDN Network costs which require additional work in order to transfer services into the contract and reduce costs with 3rd party providers. The expected date of transfer has passed which has caused a further cost pressure for IT services. 35
77 Trust Income & Expenditure Statement-Operational Services Operational Services Annual Plan In Month Year to Date FOT M /15 Plan Actual Varianc e Plan Actual Variance Var '000 '000 '000 '000 '000 '000 '000 '000 Acute and Older Adults Management and Administration (1,039) (87) (40) 47 (260) (184) Acute Services (8,395) (701) (634) 68 (2,099) (1,929) Acute Estates (2,686) (224) (220) 4 (672) (663) 8 (1) Older Adults (6,196) (519) (545) (26) (1,551) (1,596) (46) (306) Total Acute & Older Adults (18,315) (1,531) (1,438) 93 (4,581) (4,373) Community Services Community Estates (756) (63) (64) (1) (189) (196) (7) (16) Community Services (4,024) (359) (355) 4 (1,076) (1,071) 5 (95) Management and Administration (279) (23) (21) 2 (70) (61) 9 37 Early Intervention (7,242) (603) (599) 5 (1,811) (1,798) Recovery Services (3,037) (253) (258) (5) (759) (758) 1 9 Total Community Services (15,339) (1,302) (1,296) 5 (3,905) (3,883) 22 (45) Medical Services (13,010) (1,023) (1,010) 13 (3,169) (3,153) 16 0 Total Operating Services (46,664) (3,855) (3,744) 111 (11,654) (11,408) Commentary Within Acute & Older Adult services, Older Adult wards overspent by 42k on staffing, as temporary staff usage exceeded vacant posts, but vacancies in OA community services offset this, bringing the OA service line overspend down to 26k for the month. A&OA services as a whole underspent by 93k, due to vacancy savings in Acute services (mainly in CRHT). The impact of POD075 delivery slippage and the use of Agency staff to cover the demand within the service are causing the Community Services function to move from a breakeven position to a forecast outturn of 95k. Early Intervention is forecast to fully deliver the CIP target and underspend by 20k due to vacancies within the CAMHS and Primary Care services. There is a small variance from budget for medical services (mainly related to timing of training expenditure), and the uncommitted contingency funds remain at 176k for the year. 36
78 Capital Programme Plan YTD Expenditure YTD Capital Schemes 2013/14 Plan Adj. in Year Revised Plan Actual Accrued Total Variance '000 '000 '000 '000 '000 '000 '000 Schemes not completed Prior Years 2013/14 Schemes 'Mop Up' CQC Compliance Notices Service Transformation Halesview Perseverance House Site Rationalisation Anti-Ligature BFH (Malvern) - Anti Ligature Windows DPH (Langdale) - Anti Ligature Windows Other Anti Ligature Schemes Estates Backlog Maintenance Better Bedroom Project Blueprint Canalside - Temperature Controls BFH - Visitor Areas BLX (Linden & Cedars) - Ward Refreshes BLX DPH - LED Lighting BFH (Sandringham) - Drs, Training Rooms and Storage BFH - Ward Refreshes and Kitchens BLX DPH - Ward Level Laundry Equipment DPH (Langdale) - Bedroom Refresh inc. Fire Doors Hospital Fire Doors BLX - Fire Doors Other Hospital Fire Doors IT Oasis Licenses Wi-fi (Phase 1) Agile Working (to include Room Booking System) e-oasis Catering DPH - Main Catering Oven Green & Environment BFH Heating Controls Contingency Total Cost of Capital Schemes 2, , ,237 Commentary A small amount of expenditure has been incurred in respect of old year schemes 8k The balance of expenditure year to date relates to the Agile Working Pilot that was rolled out at the beginning of this financial year 37
79 Activity and Income Analysis Total Of Recorded Activity Total Of Contracted Activity Over/(Under) Performance (Activity) Over/(Under) Performance ( ) Service name Currency Qtr 1 Consultant Services : Outpatient Setting : Adult Other : First Attend Appointment Consultant Services : Outpatient Setting : Adult Other : Follow Up Attend Appointment 3,216 3,216 3,331 (115) (1,700) Consultant Services : Community Setting : Adult Other : First Appointment (1) 8 Consultant Services : Community Setting : Adult Other : Follow Up Attend Appointment (4) (374) Consultant Services : Outpatient Setting : Elderly : First Attend Appointment (14) (1,267) Consultant Services : Outpatient Setting : Elderly : Follow Up Attend Appointment ,558 Consultant Services : Community Setting : Elderley : First Attend Appointment (13) (1,243) Consultant Services : Community Setting : Elderley : Follow Up Attend Appointment (18) (744) Inpatients : Adult : Intensive Care ECA Bed Day ,372 Inpatients : Adult : Acute Care Bed Day 7,993 7,993 8,110 (117) (35,447) Inpatients : Elderly Bed Day 5,586 5,586 4, ,645 Inpatients : Rehab Bed Day ,347 Day Care Facilities : Regular Attendances : Elderly Day Rate 1,101 1,101 1,518 (417) (19,234) Memory Clinic Day Rate ,372 CRS Face To Face Contact 11,710 11,710 12,987 (1,277) (40,212) CRS Non Face To Face Contact 1,930 1,930 2,319 (389) (2,500) EAS Face To Face Contact ,096 (135) (7,415) EAS Non Face To Face Contact 1,919 1,919 1, ,721 TTT Face To Face Contact (237) (9,770) TTT Non Face To Face Contact (6) (31) Elderly Services Community Team Face To Face Contact 3,367 3,367 3,680 (313) (10,135) Elderly Services Community Team Non Face To Face Contact 1,588 1,588 1, ,293 Primary Care Team Face To Face Contact 12,110 12,110 12,781 (671) (24,693) Primary Care Team Non Face To Face Contact ,281 Recovery Intervention Service Face To Face Contact ,659 (701) (32,153) Recovery Intervention Service Non Face To Face Contact (46) (402) AMH Employment Services Face To Face Contact (27) (943) AMH Employment Services Non Face To Face Contact (123) (564) Adult Eating Disorder Community Team Face To Face Contact ,455 Adult Eating Disorder Community Team Non Face To Face Contact Crisis Resolution Home Treatment Team: Adult Face To Face Contact 5,070 5,070 5,911 (841) (51,474) Crisis Resolution Home Treatment Team: Adult Non Face To Face Contact 3,035 3,035 3, ,093 Early Intervention in Psychosis Service: Adult Face To Face Contact 2,235 2,235 1, ,094 Early Intervention in Psychosis Service: Adult Non Face To Face Contact Other Mental Health Specialist Teams: Child Face To Face Contact 4,650 4,650 5,318 (668) (40,155) Other Mental Health Specialist Teams: Child Non Face To Face Contact Criminal Justice Liason Team Face To Face Contact (37) (3,433) Criminal Justice Liason Team Non Face To Face Contact (49) (423) Psychiatric Liason Team Face To Face Contact ,974 Psychiatric Liason Team Non Face To Face Contact (130) (967) Unadjusted Total before CQUIN 76,268 76,268 79,793 (3,525) (73,671) CQUIN (1,535) mbc detox beds (48,866) mbc sms activity 5,903 5,903 (19,348) sth worc inpat older adult not recorded (6) (6) MTH 3 RECORDED ACTIVITY 82,187 82,187 Unadjusted Total (143,420) Adjustment for Walsall CCG Shadow as not on cost and volume 14,370 Adjustment for Dudley CCG Shadow as not on cost and volume 13,928 Adjustment for Wolverhampton CCG non obd Over Performance as not on cost and volume (3,548) Adjustment for Sandwell & West Birmingham CCG Shadow as not on cost and volume 44,577 Adjustment for B'ham Cross City CCG Shadow as not on cost and volume 6,876 Adjustment for B'ham South CCG Shadow as not on cost and volume 797 Adjustment for Redditch & Bromsgrove CCG Shadow as not on cost and volume 877 Adjustment for Wyre Forest CCG Shadow as not on cost and volume 2,267 Adjustment for South East Staffs & Seisdon CCG Shadow as not on cost and volume (14,471) Adjustment for Staffs & Surrounds CCG Shadow as not on cost and volume (511) Adjustment for Cannock Chase CCG Shadow as not on cost and volume (2,381) Adjustment for East Staffs CCG Shadow as not on cost and volume 164 Sub Total (80,475) Roundings (10) Over Performance As Per Ledger Month 3 (80,485) Commentary Traditional prices remain standard across all commissioners for 14/15 contracts. All contracts adopt a shadow cost and volume (block) arrangement, however improved activity recording throughout 13/14 has helped during 14/15 contract negotiations & will also help to safeguard income levels going forward. SMS commissioning remains with the Local Authority. There are no contracted activity targets for SMSwithin these LA contacts & therefore the actual activity count & financial performance is shown as a 'below the line' adjustment. Non Contracted Activity (NCA) doesn't have activity targets either, however the actual NCA activity is identified as over-performance (activity). The genuine NCA financial performance (budget to actual variance) however, is reflected within performance ( ). Trust definitions for eligible non face to face activity have been changed for 14/15. For contracting purposes prices & planned activity has been refreshed accordingly to ensure that these change have no negative financial impact on commissioners. Month 3 shows under-performance of 63k within shadow c & v contracts (an improvement of 52k from month 2). Major contracts contributing to the deficit are Walsall - 14k (crs,crht,camhs), Dudley - 14k (ris,primary care,crht) & Sandwell & West B'ham - 45k (inpats elderly, inpats acute). The 80k under-performance is a combination of the following: Under-performance to budget on NCAs by 12k (improving by 12k from month 2) Under-recovery of Local Authority SMS/detox beds income making a negative impact of 68k 38
80 Financial Performance Metrics Amended Monitor Financial Risk Rating Metric Plan Score - Plan Weighted FRR - Plan Actual - Month 3 Score - Actual Month 3 Weighted FRR - Actual Month 3 EBITDA margin 6.0% % EBITDA, % achieved 100.0% % Net Return after Financing 1.5% % I&E surplus margin 1.3% % Liquidity ratio Weighted Average Amended FRR Criteria Metric Weight EBITDA margin 25% 11% 9% 5% 1% <1% EBITDA, % achieved 10% 100% 85% 70% 50% <50% Net Return after Financing 20% 3% 2% -1% -5% < -5% I&E surplus margin 20% 3% 2% 1% -2% < -2% Liquid ratio (Days) 25% <10 Key Data Item 2013/14 Full Year Current Year to Date Forecast Outturn Accounts Plan Actual Variance Plan Forecast Variance (mc 01) (mc 02) (mc 03) (mc 04) (mc 05) (mc 06) (mc 07) 000s 000s 000s 000s 000s 000s 000s Continuity of Service Risk Ratings Liquidity Ratio (days) Capital Servicing Capacity (times) Overall Continuity of Service Risk Rating Commentary As detailed below Monitor have issued new Financial metrics, but the FRR will continue to be reported in order to provide a degree of consistency during the transition The reduced planned surplus for 2014/15 of 808k means that the planned FRR will reduce to 3.7 The underspending in Month 03 has resulted in an actual FRR of 4.10 Monitor have published in 2013 a new financial assessment tool, called the Continuity of Service Metric, which incorporates two metrics: Capital Service Capacity (Revenue available for Debt service and or Capital service) and Liquidity (Cash for Liquidity relative to turnover). The financial performance to month 03 gives an overall score of 4. 39
81 TDA Key Financial Data: Month 3 Key Metrics (A) Accountability Framework Sub Sign Plan Current Month Metrics Actual / Forecast Variance RAG Rating Previous Three Months (var) May Variance RAG by Month May RAG Rating Code (mc 01) (mc 02) (mc 03) (mc 04) (mc 05) (mc 16) 000s 000s 000s 000s NHS Financial Performance 1a) Forecast Outturn, Compared to Plan 100 +/ GREEN 0 GREEN 1b) Year to Date, Actual compared to Plan 150 +/ GREEN 106 GREEN Financial Efficiency 2a) Actual Efficiency recurring/non-recurring compared to plan - Year to date actual compared to plan 200 +/- GREEN GREEN - Total Efficiencies for Year to Date compared to Plan 210 +/ Recurrent Efficiencies for Year to Date compared to Plan 215 +/ b) Actual Efficiency recurring/non-recurring compared to plan - Forecast compared to plan 220 +/- GREEN GREEN - Total Efficiencies for Forecast Outturn compared to Plan 225 +/- 2,616 2, Recurrent Efficiencies for Forecast Outturn compared to Plan 230 +/- 2,616 2, Underlying Revenue Position 3) Forecast Underlying surplus / (deficit) compared to Plan 250 +/- 1,088 1, GREEN 0 GREEN Cash and Capital 4) Forecast Year End Charge to Capital Resource Limit 350 +/- 2,180 2,180 0 GREEN 0 GREEN 5) Permanent PDC accessed for liquidity purposes 400 +/- 0 GREEN GREEN Commentary The TDA return for Month 03 is shown in the table to the left. Planned efficiencies include 0.5 million delivered through lower costs compared to the national norms. The underlying position reflects the Trust reserves, approximately 500k in year, and the fact that 500k has been used to support nonrecurring cost pressures in 2014/15. Trust Overall RAG Rating 455 GREEN GREEN (B) Continuity of Service Risk Ratings Year to Date Rating 460 +/ GREEN 0.00 GREEN Forecast Outturn Rating 465 +/ GREEN 0.00 GREEN 40
82 Cash Flow Statement '000 Cash Flows from Operating Activities Adjusted Operating Surplus/(Deficit) 619 Depreciation and Amortisation 380 Fixed Asset Impairments Reversal 0 (Increase)/Decrease in Trade and Other Receivables 1,484 Increase/(Decrease) in Trade and Other Payables (329) Increase/(Decrease) in Provisions 10 Dividend Paid 0 Net Cash Inflow/(Outflow) from Operating Activities 2,164 Cash Flows from Investing Activities Interest received 11 (Payments) for Property, Plant and Equipment (547) Net Cash Inflow/(Outflow)from Investing Activities (536) Net Cash Inflow/(Outflow) before Financing 1,628 Cash Flows from Financing Activities 0 Net Increase/(Decrease) in Cash 1,628 Cash at the Beginning of the Period 12,748 Cash at the End of the Period 14,376 EBITDA at 30 June 2014 as per Summary Slide Deduct Depreciation and Amortisation (380) Operating Surplus at 30 June Fixed Asset Impairment Reversal 0 Adjusted Operating Surplus 619 Cash Benchmark Opening cash 12,748 Planned surplus 808 Release of Capital Payables (382) Planned cash to capital transfer (685) Realisation of PDC Receivable 33 Interest Received 48 MARS Payments (800) Forecast Cash 31 March ,770 Commentary Cash Flow The Trust made an operating surplus of 619k for the first quarter of 2014/15, and received cash of 380k in respect of depreciation and amortisation Trade and Other Receivables decreased over the period (a positive impact on cash) Trade and Other Payables decreased over the period (a negative impact on cash) The Trust has received 11k of interest, and spent 547k on capital ( 399k on reducing capital payables from the year end and 148k on 2014/15 capital expenditure). Total capital expenditure in cash terms was more than the cash received for depreciation and amortisation (a negative impact on cash) The impact of all these movements was to increase the Trust s cash balance YTD by 1,628k Cash Benchmark for March 2015 This is a useful figure to compare actual cash against as the year progresses It assumes no working capital movements other than those specifically listed 41
83 Payables Performance On Time Late Total Number Of Transactions Non-NHS Better Payment Practice Code On Time Late (%) On Time Late Total (%) On Time (%) Value Of Transactions Non-NHS Late (%) Mth 1 1, , % 3.72% 2,754,493 23,848 2,778, % 0.86% Mth 2 1, , % 11.50% 2,019, ,931 2,262, % 10.74% Mth 3 1, , % 12.55% 2,034, ,629 2,188, % 7.06% YTD 3, , % 9.43% 6,808, ,408 7,230, % 5.83% Number Of Transactions NHS Value Of Transactions NHS Mth % 0.00% 1,090, ,090, % 0.00% Mth % 5.00% 195,269 8, , % 4.20% Mth % 4.00% 219,933 1, , % 0.54% YTD % 1.69% 1,506,106 9,758 1,515, % 0.64% Av days Commentary Better Payment Practice Code The Trust meets the 95% target across both of the NHS indicators in June and YTD. The Trust did not meet the 95% target for either of the Non-NHS indicators in June or YTD. Non-compliance is as a result of IAS transactions not being approved on a timely basis by Managers and delays caused by requisitioners raising orders retrospectively. 3,500,000 Aged Receivables Profile by Value 3,000,000 2,500,000 2,000,000 1,500,000 1,000, ,000 0 Bal (120+) Bal (91-120) Bal (61-90) Bal (31-60) Bal (0-30) Aged Debt Profile by Value 77% of outstanding invoices were aged 60 days or less at the month end (this figure was 25% at the end of May). 19% of debt was aged 90 days or older at the end of June. This figure was 36% at the end of May. This is split between balances with Local Authorities relating to Drug and Alcohol Charges and balances with other NHS bodies relating to 2013/14. 42
84 Workforce NREC Funded WTE Actual Worked WTE (substantive staff) Actual Worked WTE (bank staff) EstimatedWTE (agency staff) Total Actual WTE Variance WTE Previous Month Variance (m2) WTE Function REC Funded WTE Acute & OA Management Acute Services Acute & OA Estates (0.24) Older Adult Services (9.58) (10.76) Medical Services (3.12) (3.02) Community Services Community Management Early Intervention Services Recovery Services CEO Development & People Corporate Affairs HR (4.06) (0.37) Corporate Medical Corporate Ops (incl Gov) Estates (0.01) (0.47) Finance IT (2.45) (1.58) Performance (0.48) (2.40) In Acute Services: vacancies exceeded bank and agency staff usage In Older Adult Services: ward overtime, bank and agency staff exceed funded ward vacancies In Medical Services there were 7.90 agency locums (3.40 in Dudley & 4.50 in Walsall) plus 4.00 agency medical secretaries. Staff numbers exceed budget, due to sickness cover and extra secretarial capacity funded from annual contingency. Early Intervention Service line holds a high number of vacancies resulting in high Agency usage; CAMHS teams are due to be restructured to enable the delivery of the 2014/15 CIP target. Both CAMHS and Primary Care teams have Agency cover for a number of Psychologist posts, who are providing sessions for out of hours services. Community Services Agency is unfunded but currently covered by vacancies until the service redesign is implemented. HR WTE includes posts working on externally funded projects with no funded establishment. IT budgets include posts that have been appointed on an interim basis, whilst the provision of IT Service is being explored in full detail. In addition to this, the department is funding a switchboard operator until a solution is arranged to mitigate the additional call triage since centralising the operator service. 43
85 Workforce Continued (1) 160, , , ,000 80,000 60,000 Expenditure on Agency Locum Doctors 2014/15 Actuals 2014/15 Original Forecast Commentary Current position Dudley funded 3 agency locums from contingency funds: 2 to cover vacant posts, 1 to cover long term sick leave Dudley also employed 0.40 wte agency locum for weekend A&E shifts, as funded from Dudley CCG for 24/7 PLS 40,000 20, Temporary Staffing Analysis - Adult Acute Wards 2014/15 Current Forecast Clent Kinver Wrekin Ambleside Langdale Walsall funded 4.5 agency locums from contingency funds: 3.5 to cover vacant posts, 1 to cover sick leave Locum costs are expected to rise in coming months, due to 5 new vacancies. The departures of these 3 staff / 2 vacancies on the rotation scheme were not known about in the original locum forecast, but contingency funds are sufficient to cover the extra forecast locum costs. Temporary staff usage on acute wards relates to cover of vacancies, long term sick and maternity leave cover There was a small underspend against the acute inpatient staffing budget inmonth Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 44
86 Workforce Continued (2) Temporary Staffing Analysis - Older Adult Wards Holyrood Malvern Cedars Linden Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Commentary Temporary staff usage on these wards relates to cover of vacancies, long term sick and maternity leave cover, high observation levels/ patient dependency. The sharp rise in costs on Linden in recent months relates to an increase in patient observation levels 45
87 Cost Improvement Target Achievement Headlines Target for 2014/15 = 2,087k 2014/15 Month 03 year to date = 1,799k. Current FYE value of those schemes transacted in Month 03 = 2,098k. TDA CIP target is 2,616k, but the Trust has reviewed its commitments for 2014/15, and agreed a internal target of 2,087k. Commentary Budgets for the 2014/15 target have been devolved to the appropriate budget areas. Work is ongoing to ensure that the FYE of all the 2014/15 schemes is realised and deliverable from 1st April Work is ongoing to ensure 2015/16 schemes begin to deliver cash reduction by 1st April
88 Statement of Financial Position 31 March June 2014 Movement Non-Current Assets Property, Plant and Equipment 43,153 42,981 (172) Intangible Fixed Assets (60) Total Non-Current Assets 43,753 43,521 (232) Current Assets Receivables less than one year 3,574 2,091 (1,483) Cash (OPG and Other) 12,748 14,376 1,628 Total Current Assets 16,322 16, Non Current Assets Held for Sale Total Current Assets 16,527 16, Current Liabilities NHS Payables less than one year (1,376) (582) 794 Payables less than one year (6,366) (6,772) (406) Provisions less than one year (334) (344) (10) Total Current Liabilities (8,076) (7,698) 378 Net Current Assets less Liabilities 8,451 8, Provisions greater than one year (459) (459) 0 Total Assets less Current Liabilities 51,745 52, Financed by Tax Payer Equity: Public Dividend Capital (48,321) (48,321) 0 Revaluation Reserve (57) (57) 0 I&E Reserve b/f 1,086 (3,367) (4,453) Current Year I&E (4,453) (291) 4,162 Total Taxpayers' Equity (51,745) (52,036) (291) Commentary Non Current Assets Capital expenditure exceeds depreciation and amortisation in 2014/15. This is to be expected at the beginning of the financial year as capital schemes get underway. Progress against capital schemes is reviewed elsewhere in this report Current Assets Receivables are 1,483k less than at 31 March 2014 Cash is 1,628k higher than the balance at 31 March 2014 An analysis of cash flows can be seen elsewhere in this report Current Liabilities Payables have decreased by 388k NHSLA Provisions have increased by 10k, provisions in relation to medical pay arrears and staff of fixed term contracts have remained constant. Provisions This provision is in respect of VAT over-recovered from HMRC. This has remained constant since the year end. Tax Payers Equity The Current Year I&E figure reflects the surplus YTD of 291k 47

89 Trust Board August 2014 Workforce report Month /15 48
90 Key Messages June Mutually Agreed Resignation Scheme (MARS) The majority of staff who were given the option to leave the Trust on the MAR Scheme have confirmed their intention to leave the Trust, and Settlement Agreements have been signed. Most will be leaving on 30 th September, though it has been agreed for five to leave early (July and August) and one to leave at the end of December. Five members of staff who had applications declined have confirmed their intention to retire. 2. Occupational Health Tender Following agreement by Trust Board earlier this month, the future Occupational Health Service provision will be managed by Sandwell and West Birmingham (SWBH). Meetings have been arranged with SWBH to confirm contractual terms, KPIs and contract management arrangements. Five members of our Occupational Health Services team will be TUPE d across to SWBH, with no current impact on their terms and conditions of service or location. 3. Five-year Workforce Plan Since the meeting in June, we have received a response from Health Education West Midlands (HEWM), following submission of our refreshed workforce plan, and have received partial assurance. From feedback, we have been advised that this year s focus was on Activity and Finance, whereas 2013 (when full assurance was given) was related to education commissioning. 30 Trusts submitted workforce plans with four receiving full assurance, 14 receiving partial assurance and the remainder awaiting a response. 4. Mandatory Training - Compliance remains above target as an aggregated total at 85%. Compliance with most areas of training has increased throughout June. Safeguarding and Information Governance have remained static along with recorded levels of appraisal activity. 5. Dementia Training - The Trust s dementia training plan continues to be implemented with further sessions of Dementia Capable Care: Behaviours training rolled out to staff working on Linden and Holyrood wards. The first dementia focused quarterly current awareness bulletin has been issued by Library and Knowledge Services. 6. Management of Potential and Actual Aggression (MAPA ) - The Trust s MAPA programme has been reviewed and consolidated to align with the most up to date standards set by the Crisis Intervention institute (CPI). Utilisation of workbooks and improved teaching methods has led to the programme being condensed from 10 to 5 days. 49
91 Workforce Dashboard Indicator Trust Target Corporate Medical Directorate Acute Services Community Services Early Intervention Older Adults Recovery Services Ops Management Trust (Previous Month) Trust (Current Month) Month On Month Trend Sickness % (YTD) <4.68% 3.16% 3.23% 6.45% 5.08% 4.61% 8.26% 4.24% 3.47% 5.04% 5.12% Sickness % (Month) <4.68% 3.39% 2.13% 5.19% 4.50% 7.34% 8.09% 5.71% 2.08% 5.01% 5.02% PDR's % 85% 78% 68% 56% 84% 87% 48% 75% 66% 68% 68% _ Turnover % (Exc Jnr Medics) 8-14% 15.27% 8.94% 10.61% 8.57% 7.72% 9.99% 28.73% 10.17% 11.45% 11.57% Headcount FTE in post Employment Relations Cases* Turnover for Medical Directorate excludes junior Trainee Doctors *Employee Relations cases includes disciplinary, grievance, performance management and harassment & bullying. 50

92 FTE Against Workforce plan as at 30 th June 2014 June 2014 saw a 4.49 FTE increase compared to May Since June 2013 we have seen a decrease of approximately FTE 51

93 Turnover as at 30 th June 2014 In June 2014 we saw an increase of 0.12% in the rolling turnover rate compared to May 2014; this is 2.00% higher than the same period last year. Recovery Services is showing a high turnover due to the TUPE transfer of Dudley SMS Services on 1 st April The turnover rate data excludes junior doctors due to the nature of their rotational contracts. 52
 which has resulted in absence rates above 8% on Birch Unit,")
94 Staff Absence Trust sickness for June 2014 was 5.02%, an increase of 0.01% on May s rate of 5.01%. The 12 month Rolling rate increased to 5.12% from 5.04%. Long term sickness episodes during the month have reduced from 33 to 32 episodes Older Adults had 7 staff on long-term sickness (June 2014) which has resulted in absence rates above 8% on Birch Unit, Linden and Cedar swards, CMHTs Walsall East and Dudley and OA Management. Early intervention services had 9 staff on long term sickness (June 2014) which has resulted in absence rates above 8% in the Deaf Service, Walsall CAHMs, Dudley Early Intervention Team and Dudley Primary Care The Human Resources team have been working closely with Operations over the last few months to focus on the absence issues within Older Adults and Acute Services, with particular emphasis on patterns of short term absence; sickness absence within both areas reduced In June. Regular case review meetings are taking place with the Occupational Health service. 53

95 Staff Absence National and Local Benchmarking Sickness National Benchmarking (I-view data March 2014) 12 Month Rolling April March 2014 Sickness Absence Ranking MH Trusts Dudley & W'sall MH Partners 4.94% 35/50 All Trusts 4.14% All MH Trusts 4.71% Local MH Trust % 32/50 Local MH Trust % 39/50 Local MH Trust % 13/50 Local MH Trust % 31/50 Figures from I-View may not match local figures due to a rounding effect to the nearest whole 5 Benchmarking figures for the 12 month period April 2013 March 2014 places the Trust 35/50 against MH Trusts nationally this is a deterioration on the last reported position (34/51). This information is taken from the I-View system hence the time delay of 12 weeks. The sickness absence percentage for Staff group benchmarking identifies that the Trust does not have a typical profile for sickness against either Mental Health Trusts or All Trusts for the period April 2013 March

96 PDR / Appraisals as at 30 th June 2014 The information held within the Electronic Staff Record database has remained static at 68% in June There has been a review of how appraisal data is submitted centrally and further guidance together with a revised form sent out to staff. A Pay Progression Policy linked to both appraisal and mandatory training activity was discussed at MExT. 55
97 Board meeting date: 6 th August 2014 Agenda Item number: 10.2 Enclosure: 7 Report Title: Trust Development Authority Self Certification Documents Monthly report (Month 3) Accountable Director: Author (name & title): Mark Axcell Director of Finance, Performance, and IM&T James Parker Commissioner Liaison Manager Purpose of the report: PMR was introduced by the SHA in late 2011/12. The regime was introduced to support NHS Trusts to operate in a Monitor like way, and support their preparation for the DH and Monitor Foundation Trust assessment. It was also intended to prepare Trusts for an environment in which they would be regulated by Monitor under their Compliance Framework. The regime has been continued by the successor organisation, the NHS Trust Development Authority (NTDA) and provides an opportunity for Trust s to earn autonomy from the TDA. Providers who can demonstrate consistent performance in governance, finance, quality and contract management will undergo a more light touch involvement from the TDA. There is also a clear escalation process for Trusts with persistently poor ratings or other issues. As part of the NHS Trust Development Authority Accountability Framework for NHS Trust Boards, a self-certification process has been set up. As a provider organisation we are required to provide the NHS Trust Development Authority with two monthly selfcertifications in relation to the Foundation Trust application process. The self-certification process consists of two forms as per 2013/14: Monitor Licensing Requirements Trust Board Statements Both submissions are included in this enclosure, and require the review, and recommendation for the Chief Executive Officer and the Trust Chairman to approve submission to the Trust Development Authority. It is recommended to approve submission of these self-certifications following the presentations of the Performance and Finance Reports which include the current Financial Risk Rating and the Governance Risk Rating.
98 Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Committee: Finance and Performance Committee Date reviewed: 28 th July 2014 Key points or recommendations from Committee: Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources What impact or implications does this report have on any of the following: Caring Responsive Effective Well-led Safe Please give brief details: The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources
99 Title Trust Development Authority Self Certification Documents Monthly report (Month 3) Introduction This paper presents the Trust s performance at the end of month three, 2014/15 financial year. Summary of key points, issues and risks Governance Risk Rating (GRR) remains 0 with 0 being the best rating possible. Monitor Financial Risk Rating (FRR) remains 4 with 5 being the best rating possible. The overall FRR is rating is therefore Green. The Board is required by the NHS TDA to provide and return the oversight self-certification governance declarations no later than close of play on 31 st July Late submissions will be over-ridden to a red governance risk rating. Recommendation It is recommended that the Trust Board take note of the overall Trust performance against the month three Performance Report and Finance Report and consider the Oversight Selfcertification statements. Board action required The Board is asked to ratify the submission made by the Chief Executive Officer and the Chairman.
100
101
102
103
104
105
106
107
108
109
110
111
112
113 Board meeting date: 6th August 2014 Agenda Item number: 10.3 Enclosure: 8 Report Title: Committee: Governance and Quality Committee Chair Report Governance & Quality Committee Author (name & title): Dr Robin Gutteridge NED and Chair of Governance and Quality Committee Wendy Pugh Director of Operations and Nursing Rosie Musson Head of Nursing and Quality Action required from the Board Decision / Approval Gain assurance Discussion Information Key issues and Risks At the Governance and Quality Committee meeting held on the 9th July 2014, key issues were discussed around three dimensions of risk: Quality and Safety, Experience and Effectiveness and Regulation and Compliance. Time was allocated to more detailed consideration of the following: In relation to Quality and Safety: The Committee discussed the scrutiny processes for staff incidents and assaults and trend analysis: alignment of data: Quality and Governance risk register: safe staffing levels: progress on the overarching Francis action plan: the Annual Health and Safety Report. In relation to Experience and Effectiveness: Experts by Experience Report, Service Experience Desk (SED) Annual Report. In relation to Regulation and Compliance: The committee discussed the latest Trust Performance Report; changes to CQC Quality Risk Profile; and held a spotlight session on Clinical Audit. 1.0 Quality and Safety 1.1 The Quality Report for May The report was scrutinised for assurance. The committee noted a possible increasing trend of overdose incidents. This was referred to the medicines management committee
114 for review of trends and there was agreement that this should be incorporated into the deep dive schedule for the committee in Q2. The committee discussed the process for scrutinising staff incidents and assaults. The committee received assurance that the system is sufficient and timely to convey confidence to staff that their health and safety is an important Trust consideration. It was agreed a trend analysis would be reviewed on a quarterly basis by the Committee as a new addition to the Quality Report. In addition, as a forthcoming Board Competency review is planned, the Committee agreed to ask for feedback from the Board about any identified gaps in information flows and data alignment to and from G&Q and the Board. This followed a discussion of a justifiable non-alignment of data in the Quality report and the Annual Quality Account: the Committee recognise that where non-alignment occurs for a known reason, this should be explained in a transparent and succinct way within the public report. The Quality Report is recommended to the Board for approval 1.2 The Quality and Governance Risk Register The Quality and Governance Risk Register was considered. The Committee agreed that one new risk should be added to the Risk Register Risk Ref The risk of insufficient resilience and skills in leadership, which may result in poorly engaged, demotivated staff and poor service quality. This is a new strategic risk identified at a recent Board Development session. The committee did not support the downgrading of financial risk Finan 1. The Committee asked for further guidance from the Finance and Performance Committee and Trust Board Finan 1 Inability to meet CIP targets and the impact on the viability of the Trust. The Trust Board is asked to provide further guidance on financial risk Finan 1 and approve the addition of risk ref Director of Operations and Nursing Update: Safe staffing levels Staffing levels reporting is in its second month Following the staffing levels report being presented to the Extraordinary Board meeting in June the Chair enquired if there were any outstanding questions. The NEDs agreed they were assured about the post Cummings staffing levels and that the Trust had maintained safe staffing levels pre Cummings. They also were assured that the Trust continues to adopt a rigorous and careful approach to ensuring safe staffing levels. It was agreed that data from the monthly reporting will be triangulated and scrutinised on a quarterly basis.
115 1.4 Medical Director & CD for G&Q Update: No items were raised 1.5 Overarching Francis, Winterbourne, Cavendish, Keogh and Berwick Action Plan Update Sustainable progress is being made in relation to the action plan, with 53% of actions completed and the remainder ongoing. Where slippage has occurred dates have been reviewed and new timescales set. The committee received assurance that currently no risks require escalation. A meeting has taken place with the TDA whereby it was recommended that the action plan be amalgamated into an overarching improvement plan including TIP and CQC plans. The TDA have supplied a template whose emphasis is on the measurement of impact. The Committee recommends the report to the Trust Board in August for assurance 1.6 Health and Safety Annual Report The Committee received and discussed the content the Health and Safety and Fire Safety Annual Reports and work plans. The Committee notably reiterated their intention to ensure that the Trust commitment to staff safety, health and wellbeing is visible and evident to all stakeholders endorsed work in progress to triangulate Health and Safety incidents to staff with data from the staff survey and workforce reports. thanked Mr Rowlands for a helpful report and for the discussion this generated Asked Mr Rowlands to convey the thanks of the G&Q Committee to the H&S teams for their work during the year The Committee recommends the Annual Report and work plan to the September Trust Board for ratification. 2.0 Experience and Effectiveness 2.1 Monthly Expert by Experience Report The monthly report from the Experts by Experience was accepted. Thanks were expressed to Mrs Jankowska who is taking a break from her EBE duties 2.2 Suicide Prevention Plan Update The Committee deferred the Suicide Prevention Plan progress update until the August meeting. 2.3 SED Annual Report
116 The SED Annual Report was presented to the Committee. The Committee discussed the report and noted the high number of compliments received. The Committee approved the report and recommends it to the Trust Board in August for ratification. 3. Regulation and Compliance 3.1 The Performance Report The performance report was received for information and assurance. Positive performance in relation to care plans was noted. 3.2 CQC Quality Risk Profile The Committee noted that the CQC will be changing the format for the Quality Risk Profiles. Currently there are no exceptions to report. 3.3 Spotlight Session A Clinical Audit presentation was given to the Committee that highlighted areas of good practice, areas for improvement and proposals for the future. The Committee agreed that further discussions regarding the proposed areas for improvement were required and requested an update report in September. 4. Committee Business, Reporting and Planning There were no matters of concern in the Exception reports which were received from the following Sub-groups: Infection Prevention Control Committee Health and Safety Committee Medicines Management Committee Policy and Procedures Focus Group Key action points and work in progress Clinical Audit To ensure clinical audit practice is in line with National Best Practice and to ensure clinical audit is effectively supporting quality monitoring and improvement in the Trust CQC Action Plans and alignment to overarching improvement plan the committee continues to take an active role in addressing the findings of the CQC Report and will continue to monitor progress in relation to the impact of implemented actions on quality outcomes. Intelligent use of data and data alignment the Committee will continue work to improve how data is collated, aligned and presented to facilitate effective quality monitoring, assist prioritisation of Committee activity and support continuous improvement.
117 Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees / Groups: Audit Committee CARM/ CQR Clinical Audit and Effectiveness Committee Embedding Lessons Group Equality and Diversity Steering Group Finance and Performance Committee Health & Safety Committee Infection Prevention Control Committee Information Governance Committee Medicines Management Committee Mental Health Forum MExT Policy & Procedures Group Regulation and Risk Working Group R&D Committee Resuscitation Committee Safeguarding Strategic Group Suicide Prevention Group Recommendations and requests for direction The Board is asked to: Accept this report for assurance about the exercise of delegated authority by the Governance and Quality Committee Endorse the decisions and recommendations made by the Governance and Quality Committee. In particular, the Board is asked to: Approve the Quality Report for July 2014 (period ending 30 June 2014) Discuss and agree the proposed management of the Quality risks detailed on the Trust Wide Risk Register as recommended by the Governance and Quality Committee Receive a quarterly update on the Francis overarching action plan for assurance Ratify the Health and Safety Report which will be presented to Trust Board in September Ratify the SED Annual Report
118
119 Board meeting date: 6 th August 2014 Report Title: Agenda Item number: 10.7 Enclosure: 9 MHA Scrutiny Committee Chair Report Committee: Mental Health Act Scrutiny Committee Author (name & title): Dr Stuart Hill Chair of MHA Scrutiny Committee Action required from the Board Decision / Approval Gain assurance Discussion Information Key issues and risks The Mental Health Act Scrutiny Committee (MHA SC) met on the 14 th July The meeting had unfortunately been postponed from 5 th June although the Associate Lay Manager (ALM) meeting did take place on 12th June. The issues and risks considered by the meeting mainly related to the final quarter of 2013/4 and the consolidated position for the year. As such this report should be read in conjunction with the Draft Annual Report for the year which is also being considered by the Board. Key issues considered included: the IMHA service; OASIS; relationships with local emergency services; CQC; ALM recruitment and training; analysis of AMHP activity via the MHA SC dashboard; the annual report, new responsibilities in monitoring DoLs, and MHA/MCA training. 1.0 The IMHA Service The ward presence of the IMHA has now improved in Dudley but is still disappointing at Walsall. It was not clear whether the lack of presence was due to the fact that the IMHA service was not advertised widely on the wards. The meeting asked for more information to be provided on the contracts, and suggested that the Trust s EBEs could help by highlighting the service. 2.0 OASIS The Committee was advised that teams were testing new interfaces in Oasis which will go live at the end of July. However the Committee confirmed that sight of the project plan was still required by members and an update on the progress should be brought to the next Committee meeting. Page 1 of 7
120 3.0 Relationships with local emergency services 4.0 CQC This key issue was considered from a number of different perspectives. 3.1 MH Partnership Group (MHPG) Meetings The attendance by police and ambulance personnel has significantly improved, which has improved the relationship with the police who have taken practice cases back to their colleagues for discussion, as well as receiving training on the use of the Section 136 suite. The fact that MHPG Meetings will be held monthly rather than quarterly points to its relevance and the MHA SC was keen to capture the output. It was noted that very few Trusts have the opportunity to participate in this kind of forum. The meeting asked for a short quarterly report on what issues were raised, best practice, what and how have issues been addressed. 3.2 Police Training It was noted that the delivery of MH Act training to Police was already starting to pay benefits. In particular they are contacting the Crisis teams to find out if individuals are known to the Trust. If it is evident that people are likely to be under the influence of alcohol, they are sent home rather than delivered to the Section 136 Suite. As assessments cannot be made on those individuals under the influence of alcohol, the Trust contact them the next day. As a further benefit of the training, it appears that the use of Section 136 Suite in Dudley has decreased, although this will need to be monitored carefully to see if the improved trend is sustained. It was reported that the Walsall Police have noted the position in Dudley and are trying to find the funds for training. In discussion, it became apparent that this would only amount to 2k and that the cost would be recovered later, as fewer assessments would be made. It would also yield better results for service users. The MHA SC therefore asked Mrs Temple-Purcell to arrange for the MHA Training for the Walsall Police to be carried out as soon as possible, with the Trust bearing the cost. The MHA SC was informed that the 3 CQC compliance notices had been fully discharged. A follow-on action to extend best practice was outstanding - the installation of an enhanced patient alert system for individuals but these would be available by the end of the week. Managers have been reminded to ensure documentation and best interest assessments are completed and adhered to. The Director of Operations, Nursing & Estates was asked to provide a report summarising the CQC compliance actions, including progress and evidence of completion at the next MHA SC meeting. 5.0 ALM recruitment and training The MHA Manager reported that 7 new ALMs had been recruited, with some already observing hearings. The formal training will start in August, to include the legal aspects of hearings/tribunals from Mills and Reeves Solicitors. Page 2 of 7
121 6.0 Analysis of AMHP activity The MHA SC reviewed the Quarter 4 dashboard and the cumulative position for 2013/4 and agreed that the key issues had been addressed within the report. The meeting therefore focussed on trying to understand the trends behind the statistics. 6.1 Over 60s Discussion took place on the possible reasons for an increase in assessments of the over 60 s but it was agreed further investigation was needed. A deep dive was requested for the next MHA Sc meeting. 6.2 Non-admittance and informal admittance of patients As had been reported before, a large number of MHA assessments completed had resulted in non-admittance or informal admittance of patients. In order to understand this further, an audit into the patient pathways and the service interaction with Health & Social Care will be completed using a quarter s worth of data. A small working group has been set up to analyse cases in depth, for discussion at the next MHA SC meeting. 6.3 Benchmarking information from other trusts Freedom of Information requests to neighbouring local authorities had yielded some interesting benchmarking data in relation to Mental Health Act assessments for the calendar year The responses were however very patchy, as outlined below: Sandwell acknowledged receipt of request but did not reply. The request has been resubmitted. Wolverhampton replied but could not provide GP Attendance data due to the amount of time involved and will require a fee if we wish to obtain this information. Birmingham & Solihull FT provided some data, but stated they do not hold information on the number of assessments, how many were out of hours and GP attendance. Staffordshire Council stated they do not hold the information so requests were made to South Staffs and North Staffs. o South Staffs & Shropshire some data provided but information on the total number of assessments, how many were out of hours and GP attendance is not held. o North Staffs again some data provided, but as with South Staffs & Shropshire information on the number of assessments, how many were out of hours and GP attendance is not held. Additionally it should be noted that Birmingham & Solihull, North Staffs, and South Staffs & Shropshire Trusts only record MHA assessments that result in detention or informal admission Page 3 of 7
122 to hospital. Notwithstanding these limitations it can be seen in Table 1 overleaf that there are significant differences in the figures particularly when viewed on a per head of population basis. Page 4 of 7
123 Table 1 Benchmarking information from neighbouring trusts for 2013 Total no. of MHA Assessments undertaken How many of these assessments were undertaken Out of Hours Total no. of detentions under Sec.2 of the MHA Total no. of detentions under Sec.3 of the MHA Total no. of Informal Admissions Total no. of assessments where the patient s GP was in attendance Total no. of Sec. 136 assessments. (How many of these led to a detention) Total no. of CTOs Population Dudley (34) ,900 Walsall (31) 1 281,700 B ham & Solihull Information not held Information not held Information not held 707 (169) 258 1,085,400 W hampton To comply with this question would cost in excess of the 450 limit. 13 (5) 9 250,975 North Staffs Information not held Information not held Information not held 261 (21) ,000 South Staffs & Shropshire Information not held Information not held To comply with this question would cost in excess of the 450 limit. 225 (34) ,600 Sandwell Information not received from initial request resubmitted request for data. 309,000 Page 5 of 7
124 7.0 MHA SC Annual Report and Committee Effectiveness Report The latest draft of the annual report was tabled by the Chair with comments invited by the end of the week with a view to producing a final draft for this Board Meeting. Members were also invited to provide commentary on the committee effectiveness report which had been considered in outline at a previous meeting. 8.0 Extended Terms of Reference 8.1 Assurance The meeting was informed that the responsibility of monitoring the use of DoLs and giving assurance to the Board lay with the Committee. There had been recent legal changes to the application of its use, so the Trust and local authorities had to be clear on its accountabilities and responsibilities. The changes will impact on both staff and service users. The Committee s terms of reference will therefore need to be amended to incorporate the monitoring of DoLs. The Safeguarding Lead will be responsible for ensuring it was rolled out to the relevant teams, as this interfaced with her Safeguarding Lead role. The committee particularly noted the importance of assurance that compliance was incorporated into day to day practice. An update was provided on progress with new guidance, communications, and the linkage with governance reporting. It was confirmed that the Safeguarding Lead has sight of all incident reports for scrutiny. 8.2 Implementation The Committee agreed with the actions in principle and there was further discussion on the implications of DoLs on staff and the difference between the use of the MHA and DoLs. It was noted that the draft DoLs policy was expected to be ratified by the end of the week, but considered a project implementation plan will be required. The Safeguarding Lead was therefore asked to produce a DoLs implementation plan for the Committee for assurance, with progress milestones and a clear internal process with in-depth education and support for staff to ensure compliance. 8.3 Risk mitigation The Committee heard the low number of best interest assessors employed by local authorities may pose a risk to the Trust. It was imperative that a joint approach with the local authorities at the start of the process was in place. The Committee asked the Mental Health Act Manager to circulate the Cheshire West guidance document for information to members, along with the DoLs flowchart. 8.4 Next steps The Committee asked the Director of People & Corporate Development to set up a meeting with Page 6 of 7
125 a small number of Committee members to provide the following by the next Committee meeting: MCA/DOLS policy roll out plan, including effectiveness measures Training plan for MCA/DOLS Amendments to MHA SC Terms of Reference to encompass the changes 9.0 MHA & MCA Training The HR Learning & Development Manager highlighted that the MHA training compliance was at 58%. The MCA training compliance was to be confirmed. It was noted that the approach to training had been changed in order to increase compliance by delivering it in tandem with the Safeguarding training. Although some improvement was apparent the Committee felt that a risk-based approach was needed to make more progress. The HR Learning & Development Manager was therefore asked to provide a breakdown of role specific DoLs training required by service line, in order to quantify the level of risk to the organisation, for the next Committee meeting. Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees/Groups: MEXT Governance & Quality Committee Clinical Audit and Effectiveness Committee Equality and Diversity Steering Group Safeguarding Strategic Group Recommendations and requests for direction The Board is asked to accept this report for assurance. Page 7 of 7
126
127 Mental Health Act Scrutiny Committee Annual Report to the Trust Board Author: Stuart Hill (Committee Chair) Date: 26th July
128 1. SUMMARY This is the first Annual Report of the Dudley and Walsall Mental Health Partnership Trust s Mental Health Act Scrutiny Committee. It sets out the framework within which the Committee operates, provides an overview of its activities in 2013/4 and the outcomes of its deliberations, and looks ahead to developments and the changing role in 2014/5. 2. INTRODUCTION Dudley and Walsall Mental Health Partnership Trust ( the Trust ) was established in 2008 with a commitment to improving local mental health services. It has specific responsibilities in terms of the conduct, administration and application of the Mental Health Act 1983 ( MHA 1983 ), as amended by the Mental Health Act 2007 ( MHA 2007 ), more generally the Act. An important feature of the Trust s governance structure from the outset was the Mental Health Act Scrutiny Committee ( the MHA SC ) which, by contrast with some other trusts, reports directly to the Trust Board and is chaired by a Non-Executive Director. Its principal responsibilities lie in ensuring the Trust s compliance with all aspects of the Act and that significant reports, including those from the Mental Health Act Commission (until March 2009) and the Care Quality Commission, are actioned appropriately. This is the first Annual Report of the Trust s MHA SC. In particular, it: sets out the framework within which the MHA SC acts; looks back over the year 2013/14; and looks ahead to the future. 3. THE FRAMEWORK WITHIN WHICH THE MHA SC OPERATES 3.1 Membership of the MHA SC The nominal core membership of the committee is set out in the Terms of Reference (see Appendix 1). In practice organisational developments within the Trust meant a number of these roles and the individuals within them changed, so that the current de facto core membership is: Non-Executive Director (Chair) Non-Executive Director (Vice-Chair) Director of People & Corporate Development Director of Operations, Nursing & Estates Clinical Director, Acute Services Head of Acute Services Head of Older Peoples Services Head of Social Care 2
129 Approved Mental Health Professional (AMHP) Lead Learning & Development Lead Equality and Diversity Manager Information Governance Manager Mental Health Act Manager During the course of the year the Vice-Chair, Dr Robin Gutteridge, moved on to become Chair of the Trust s Governance & Quality Committee. She was replaced by another Non-Executive Director, Gill Cooper. Also during the course of the year Sue Lassetter retired from the post of Mental Health Act Manager, although she continued to provide invaluable assistance until the end of the reporting year. Nageena Bibi took over the role in August It has to be reported that early in the year, pressures on diaries meant that committee attendance was patchy. Of particular note was the need to postpone the December 2013 meeting when high priority meetings with other local NHS Trusts to plan for Winter Pressures rendered the meeting inquorate. It is pleasing to report in this context that the reconvened meeting in early February was well-attended. It is hoped that this improvement will be sustained, but it has to be recognised that pressures on diaries show no sign of abating. This, coupled with the fact that the Committee meets quarterly (so that continuity is particularly important), suggests more formal monitoring and reporting of attendance should be implemented in 2014/15. In this context it is hoped that the bedding in of the organisational changes outlined above will be helpful. 3.2 Hospital Managers The Trust provides inpatient mental health care and hence the Trust Board has a range of responsibilities relating to the detention of patients admitted under the Act. Under the terms of the Act, the Directors of the Trust are defined as the Hospital Managers 1 and have both the power to detain patients and the responsibility for seeing that the requirements of the Act are followed. This means in particular that: they must ensure that patients are detained only as the Act allows; the treatment and care of patients while detained accord fully with the provisions of the Act; & patients are fully informed of their rights, and supported in exercising them. Most of the functions and duties of the Hospital Managers may be, and are, delegated to nominated officers of the Trust in accordance with Act. However the Directors in their role as Hospital Managers may not delegate in this way their statutory responsibility to hear appeals of patients detained under the Note: this is a specific legal term and quite distinct from the day-to-day management of the Trust. 3
130 Act or to consider discharge when detention is renewed and when Community Treatment Orders ( CTOs ) 2 are extended. Associate Lay Managers undertake this role instead. 3.3 Associate Lay Managers ( ALMs ) ALMs are appointed by the Trust as volunteer lay people to carry out the Board s responsibilities under Section 23 of the MHA They have statutory powers and responsibilities to protect the rights of detained service users and are trained by the Trust to undertake specific duties as defined by the Act. ALMs therefore play an important role in ensuring that the rights of patients are upheld. They hear appeals of patients detained under the Act and consider discharge when detention is renewed and when CTOs are extended. They make judgments based upon written and oral evidence and convey these judgments to service users and/or carers. In particular they have the power to discharge patients from detention. In order to carry out this role effectively, ALMs meet as a group four times a year where they are encouraged to share best practice and suggest improvements to services, particularly in terms of training. They are accountable to the Chair of the MHA SC and who also chairs their quarterly meetings. Their performance in the role is reviewed every two years. 3.4 The role of the MHA Administration Offices The Mental Health Act administration service for the Trust is provided through two Mental Health Act Offices, one at Dorothy Pattison Hospital, Walsall and one at Bushey Fields Hospital, Dudley. The service consists of performing statutory administrative tasks in relation to the Mental Health Act including scrutinising and accepting section papers, processing appeals, facilitating Tribunals and ALM hearings and giving advice. 4. REVIEW OF 2013/14 ACTIVITIES AND PERFORMANCE The Terms of Reference of the MHA SC, as revised on 6 th included as Appendix 1 and form the basis for this review: June 2013, are 4.1 Maintain an overview of the operation and application of the Act within the Trust The Committee met 4 times during the year with scrutiny of the operation and application of the Act an overarching theme. A much improved dashboard was introduced during the year with the intention of providing the MHA SC with more complete information on the use of the Mental Health Act in Dudley & Walsall and 2 The Mental Health Act allows people in some circumstances to be put on supervised community treatment, following a period of compulsory treatment in hospital. Someone on supervised community treatment is called a 'community' patient and they are subject to a 'community treatment order' (CTO). 4
131 to facilitate the identification of trends during the year. The dashboard was initiated by the Trust s Head of Social Care based on the Trust s Accredited Mental Health Professional (AMHP) assessment activity and refined over the year as queries were raised. For example more information on in-patient Sections/Conversions is now included, along with CTOs and Hospital Manager Panel and Tribunal Hearings. The bulk of the data is analysed both by quarter and locality (Dudley and Walsall). As a consequence of these developments and the growing body of data, the dashboard became the focal point of the Committee s deliberations in: risk management, to highlight areas of risk and potential risk so that action plans can be developed to address them; benchmarking with other similar organisations, highlighting good practice and identifying where practice can be improved; & via exception reports, identifying legal breaches. 4.2 Development, review, implementation and monitoring of MHA policies and procedures to support and ensure compliance with MHA legislation During the course of the year the Committee supported the implementation of important changes in the day-to-day administration of the Act: The progress towards the standardisation of administrative practices across the Trust. Introduction of section papers scrutiny checklists across the Trust to aid senior nurses and MHA administrators in scrutinising section papers when patients are admitted. A checklist to aid medical scrutiny of section papers to ensure the medical recommendations are completed correctly. Existing policies were reviewed and/or amended, including the Section 17 Patient Leave policy and supervised community treatment policy. The MHA care plan used by nursing staff was updated, to ensure patients are informed of their rights regularly. The form T2 was updated to include recording of capacity. Updating and amending the ALM decision form to ensure a standard form is used across the trust and that there is more information on the decision forms. 4.3 The use of the MHA within the Trust and an analysis of emerging trends The following observations draw directly on the data presented in the dashboard referred to earlier. As such it has been possible to start to identify emerging trends, or suspected trends, but explanations are by the very nature of the raw data less easy to come by, and should be treated with caution. 5
132 525 MHA assessments were commenced 3 in Dudley during the year and 538 in Walsall, fairly evenly distributed quarter by quarter. In both localities the Trust itself was the predominant referral source, although there were significant variations from borough to borough. For example the Trust s Bushey Fields Hospital in Dudley referred twice as many cases as Dorothy Pattison Hospital in Walsall (150 versus 75). On the other hand the Trust s Crisis Resolution/Home Treatment (CRHT) team in Dudley referred 67 cases, whereas the equivalent team in Walsall referred 180. Police referrals were also significant in both boroughs (100 in Dudley and 57 in Walsall), as were, to a lesser extent, GPs (30 and 22 respectively) and the local acute hospitals (32 and 13). The MHA SC paid particular attention during the year to the low GP attendance at MHA assessments. In Dudley GPs attended only 10 assessments out of 524; in Walsall it was only 11 out of 537. The Head of Social Care notified commissioners of the position in Quarter 3. The main reasons stated in Dudley were Out of Hours Assessment (229), Annual Leave (69), and In Surgery/Clinic (51). No reasons were given in 66 instances. In Walsall the main reasons stated were the same: Out of Hours Assessment (232), Annual Leave (99), and In Surgery/Clinic (42). No reasons were given in 43 instances. Turning now to outcomes, in 2013/4, across the Trust as a whole 21% of the MHA assessments resulted in detentions under Sections 2 of the MHA and 12% in detentions under Section 3. Just 20% of assessments resulted in informal admissions. This then leads to striking statistic that nearly a half (47%) of MHA assessments did not lead to formal or informal admission to hospital. The MHA SC took the view as this pattern emerged during the year that it was important to understand what then happened to those clients who were not admitted and a new element was added to the dashboard. This is still very much work in progress, with a rather broad range of outcomes and some variation from borough to borough. The analysis of the incomplete assessments shows a similar picture, with the 8 inappropriate referrals out of 15 in Walsall prompting a theme to be pursued as more data is gathered in future years. The dashboard also gives a breakdown of the gender of clients assessed under the MHA, their ages and their ethnic origin. The picture with regard to gender is particularly difficult to interpret. For example in Dudley rather more males than females were assessed under the 3 24 assessments were not completed in Dudley and 42 in Walsall for various reasons. 6
133 MHA over the year (313 and 213 respectively). In Walsall the proportions were much more balance at 277 and 260. The breakdown of the ages of those assessed also shows variations between the boroughs. In Dudley the peak age range was 40-49, falling away quite sharply after, whereas in Walsall the distribution is much more even across all ages. Turning to the outcomes of the assessments across both boroughs 81 males were formally admitted, 73 were informally admitted and 121 were not admitted. A similar number of females were formally admitted (79), whereas only 41 were informally admitted 100 were not admitted. The MHA SC has for some years reviewed the distribution of ethnicity of those assessed under the MHA. However the new dashboard provides the basis for a much more detailed breakdown, not only in terms of assessments and localities but also outcomes. Dudley Ethnic Origin Population MHA Assessments (2013/4)* White 90% 79% Asian 6% 10% Mixed 2% 4% Black 2% 4% Others <1% 2% Walsall Ethnic Origin Population MHA Assessments (2013/4)* White 79% 74% Asian 15% 17% Mixed 3% 3% Black 2% 4% Others 1% 1% * Excludes not stated The tables above show that ethnic minorities are over-represented in terms of the proportion of MHA assessments versus the population as a whole, although the position is less pronounced in Walsall than in Dudley. The dashboard also provided more information about the use of the Trust s 2 Place of Safety 4 Suites ( POSS )at Dudley and Walsall. The MHA SC found particularly noteworthy the sharp fall in Dudley usage in Quarter 4; the much more even male to female ratio in Walsall (55 to 45) than Dudley (72 to 26); and the greater use of In Hours at Walsall compared with Dudley (29% to 18%). A possible explanation for the fall in Dudley usage may lie in the MHA training the 4 The term "place of safety" is used in the Mental Health Act Section 136 of the Act gives police officers the power to remove an apparently mentally disordered who is in a public place and is apparently a danger to himself or to other people, person to a "place of safety" where they may be assessed by a doctor. Section 135 of the Act gives police powers to remove a person who is not in a public place to a place of safety after the issue of a warrant by a Justice of the Peace. 7
134 Trust has provided to Police in the Borough. Anecdotal evidence suggests that, as a consequence, they are contacting the Crisis Teams at early stage to find out if individuals are known to the Trust. If it is evident that people are likely to under the influence of alcohol, they are sent home rather than delivered to the POSS. As assessments cannot be made on those individuals under the influence of alcohol, the Trust contact them the next day. Careful monitoring will be needed to see if this improved trend, which also yields better results for service users, is sustained. In the meantime the Trust is looking to extend the training to Walsall Police Returning to the statistics of the POSS, admission (either formal or informal) was even more the exception rather than the rule. 68% of assessments in Dudley led to the client not being admitted, in Walsall it was 65%. Informal admissions were the next most likely outcome (21% in Dudley and 19% in Walsall) with even fewer formal admissions under Sections 2 & 3 of the MHA (12% across both boroughs). This will be an area the MHA SC will be returning to in the future. 4.4 Reports from the Care Quality Commission (CQC) The Trust was inspected by the CQC on 26 th and 27 th February 2014 as part of its new hospital inspection programme, which was at that time still in its development phase. This was in fact one of the first inspections the CQC had carried out in this form for mental health and community trusts, and hence an overall rating was not given. The new approach was based on a site visit by a team of over 40 consisting of a chair, team leaders, doctors, nurses, allied health professionals, managers, experts by experience, CQC inspectors, analysts and planners. The team received a presentation by the Trust s Chief Executive, and carried out visits to clinical areas; staff focus groups (including junior and senior doctors and nurses); patient and public listening events; and interviews with senior managers. At the heart of the inspection were 5 key questions. Are the services provided by the Trust: Safe are people protected from abuse and avoidable harm? Effective does people s care and treatment achieve good outcomes and promote a good quality of life, and is it evidence-based where possible? Caring do staff involve and treat people with compassion, kindness, dignity and respect? Responsive are services organised so that they meet people s needs? Well-led does the leadership, management and governance of the organisation assure the delivery of high-quality patient-centred care, support learning and innovation and promote an open and fair culture? The CQC s findings were outlined to the Trust and other stakeholders at a Quality 8
135 Summit on 12 th May A number of areas of good practice were identified, but most relevant for this report is their finding that application of the Mental Health Act was good. Headline findings as they related to the application of the Act within the Trust (both positive and negative) included: People were lawfully detained under the Mental Health Act 1983 and staff were working within the Code of Practice. There were some concerns about the safety and suitability of premises at some locations (see later). Some of the hospital locations had mixed sex wards. This meant, in the older people s service, people did not always receive the care they required and their privacy and dignity was not always maintained. De facto seclusion was being practiced within the wards and staff were not adhering to the Mental Health Act Code of Practice. Mental Health Act (MHA) administrators were appointed to monitor the legality of the paperwork about detention. Audits were completed in relation to the MHA but they were basic and did not include an audit against the code of practice requirements. A number of areas for improvement were identified, including 3 Compliance Actions relating to aspects of care and environment in Holyrood Ward; Grasmere Ward as a mixed gender facility; staff training, especially in dementia and behaviours that challenge; de facto seclusion and least restrictive practice; and care plans based on assessed risk. It is recognised that the details of the Trust s response to the compliance issues will more properly fall in the 2014/5 Annual Report. Nonetheless it is perhaps worth outlining the approach given at the Quality Summit on 12 th May. The Trust reported it had: Taken immediate action following initial verbal feedback; Received and reviewed the draft inspection report, and submitted factual accuracy comments; Taken immediate action to address concerns from the report. All compliance concerns regarding patient safety and privacy and dignity had been fully addressed; Developed a comprehensive work plan to address all compliance issues, signed off by Trust Board and submitted to CQC The development of action plans to address the less pressing but still important must, could and should do recommendations was also outlined at the Quality Summit. As recognised above, these plans, and more particularly their implementation, will be reported in the 2014/5 Annual Plan. 4.5 Results of clinical audits 5 The full report is available at 9
136 The Committee regularly discusses a wide range of audits and reports in relation to the practical application of the Mental Health Act across the Trust. An audit of Mental Health Act paperwork on the wards is undertaken on a bimonthly basis. The audit results are fed back to the wards and a quarterly report is submitted to the Mental Health Act Scrutiny Committee. The audits identified a need to improve practice in relation to consent to treatment, keeping patients informed of their Section 132 rights, the completion of risk assessments prior to leave, crossing out old Section 17 leave forms and documenting if copies of the leave form have been offered to the patient. The MHA administrators continue to work with the ward managers and the consultants to improve practice in these areas. 4.6 Amendments to Mental Health Act legislation, guidance and best practice The Committee was updated during the year of any developments in Mental Health law and ensures that the systems and procedures designed to provide assurance that practice across the Trust goes above and beyond the requirements of statute, case law and the MHA Code of Practice. When required the Trust s solicitors were asked to provide advice. 4.7 The role, functioning and performance of the MHA Associate Lay Managers During the course of 2013/4 there were 14 ALMs working for the Trust: Trevor Bayley Nick Bishop Judith Cooper Alison Ford Jasvinder Hewitt Siddique Hussain Pauline McCarthy Beryl Nock Mohammed Ramzan Bryan Richens Michael Shaw Tina Virdee Geoffrey Wynne Nazia Yousaf They participated in 61 ALM hearings in the year; we would like to thank them for their continued support. Trevor Bayley and Jasvinder Hewitt resigned this year; we would like to thank them for the hard work and support. Towards the end of the year MHA SC oversaw the recruitment of a new cohort of ALMs; the committee would like to thank Michael Shaw for his help with the process. There was an excellent range of candidates and the Trust was pleased to make 7 offers: their training will be taking place in August Issues raised by the MHA Associate Lay Managers The ALMs have raised a number of important issues at the quarterly meetings which are summarised below. The failure to complete the paperwork for the extension and renewal of section in good time to allow for the hearing to take place prior to the expiry of section was 10
137 raised by the ALMs as this was not always happening with the Dudley patients. Whilst this is not illegal it is not working to best practice. This issue has been flagged up to the consultants and the medical directors, and will be monitored to ensure compliance with the MHA Code of Practice. The ALMs raised concerns that some clinicians are attending ALM meetings without adequate preparation; this has been raised with the relevant professional leads. However it should be noted that where the evidence was good, the ALMs have praised the reports and information provided by the clinical team. Whilst sitting on an ALM hearing one of the ALM recognised the fact that the interpreter attending the hearing did not speak the dialect required by the patient and the patient was struggling to understand the patient. This was raised with the Trust by an ALM. The matter was taken forward by the Trust and a complaint made to the interpreting service who dealt with the issue. 4.8 Support provided by the Mental Health Act Administration Offices 2013/4 saw an increase in workload due to the increase in the use of CTOs and hearings. With the introduction of more robust MHA administrative practices (as noted above at 4.2) to ensure compliance with the relevant legislation, this workload will continue to increase. The MHA administrators at Dudley also helped to organise and provide training for the Section 12(2) and Approved Clinician Training course in 2013/4 which was very well received. As noted earlier Sue Lassetter retired from the role of Mental Health Act Manager this year; we would like to thank her for her hard work and dedication in supporting all aspects of the Trust s MHA activities. 4.9 Review of the performance of the MHA SC in 2013/4 The Committee reviewed its performance in 2013/4 using the Self-Assessment Efficiency and Effectiveness Checklist set out in Appendix 2 at its meeting on 6 th March No major concerns were noted. However it was recognized that terms of reference and effectiveness were to be considered more broadly across all Board Committees by the Trust Board, and the outcome of these discussions would be fed into a more formal review of the effectiveness of the MHA SC at a later date. 5. A LOOK TO THE FUTURE An important development during 2013/4 was the introduction of a comprehensive dashboard, enabling the MHA SC not only to record activity under the MHA but also to highlight good practice and identify where practice could be improved. As the body of data increases, this aspect of the Committee s work will undoubtedly take on greater prominence. It will also form the basis for benchmarking with other trusts. More fundamentally, the terms of reference and scope of the MHA SC will need to be expanded to encompass monitoring and reporting on the Mental Capacity 11
138 Act (MCA) 6, DoLS 7 and de facto seclusion. Work is already underway at the time of writing this report with new policies and procedures being put in place, but the complexity of these far-reaching changes should not be under-estimated. This then leads into an aspect of the Committee s work mentioned earlier in the report the computerisation of records onto the Trust s OASIS system. Capturing and analysing data for the MHA SC is still a laborious process, notwithstanding the progress reported in the body of this document. The MHA SC has kept a keen eye on developments in this area, and will continue to do so in 2014/5, particularly in the more streamlined production of reports. As the body of MHA data increases this will be vital in discerning emerging trends and suggesting underlying factors Looking more broadly, the role of the MHA SC has already started to change from what was essentially rather passive monitoring, as exemplified by the Committee s interest and involvement in improving the links with the emergency services. Wherever these changes take the MHA SC, and many of them are very far-reaching, the Committee remains fully committed to ensuring that patients stay at the heart of the its deliberations 6 The Mental Capacity Act 2005 provides a framework to empower and protect people who may lack capacity to make some decisions for themselves. The Act makes clear who can take decisions in which situations, and how they should go about this. 7 The Mental Capacity Act Deprivation of Liberty safeguards were introduced into the Mental Capacity Act 2005 through the Mental Health Act They apply to anyone who is aged 18+ and suffers from a mental disorder or who lacks capacity to give informed consent for their care. In these circumstances, an independent assessment will be carried out and a deprivation of liberty (DoLS) may be considered to be necessary in their best interests to protect them from harm. 12
139 APPENDIX 1 MHA SC TERMS OF REFERENCE 1. Purpose 1,1 The Mental Health Act Scrutiny Committee is a sub-committee of the Board of Dudley and Walsall Mental Health Partnership NHS Trust and is responsible for discharging all requirements of the Mental Health Act ( the Act ). 2. Accountability 2.1 The Board hereby resolves to establish a Committee of the Board to be known as the Mental Health Act Scrutiny Committee ( the Committee ). The Committee is a non-executive committee of the Board and has no executive powers, other than those specifically delegated in these Terms of Reference. 2.2 The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. 3. Duties and responsibilities To maintain an overview of the operation and application of the Act within the Trust. To be responsible for the development, review, implementation and monitoring of Mental Health Act policies and procedures to support and ensure compliance with Mental Health Act legislation. To review and monitor the use of the Act within the Trust, noting and ensuring investigation of any emerging trends with respect to service, age, gender, ethnicity and cultural background. To receive and review reports from the Care Quality Commission (formerly the Mental Health Act Commission) and other relevant external bodies, ensuring that appropriate actions and responses are undertaken. Receive the results of clinical audits and other relevant reviews of the Act and oversee the development and implementation of recommendations. To review and oversee the implementation of any subsequent amendments to Mental Health Act legislation, guidance and best practice. To monitor the role, functioning and performance of the Mental Health Act Lay Managers and to liaise with them on all pertinent issues. 13
140 To support the role of the Mental Health Act Administration offices. The group will consider as a regular item pertinent issues arising from the Associate Lay Managers Peer Group. At the discretion of the Chair, the Committee will be responsible for establishing and receiving reports from working sub-groups to investigate specific issues or trends, as required. 4. Membership 4.1 The following constitutes the core membership of the Committee: Non-Executive Director (Chair) Non-Executive Director (Vice-chair) Director of People and Corporate Development Associate Director of Operations Clinical Director Acute Services Head of Acute Services Head of Older Peoples Services Head of Social Care An AMHP Lead Mental Health Act Manager Equality and Diversity Manager Learning & Development Manager 4.2 Any non-executive director may deputise for an appointed member of the Committee with the permission of the Chairman of the Board. 4.3 Core members may nominate an appropriate deputy to attend the committee on their behalf. However, it is expected that any nominated deputy will be fully briefed and have the necessary authority to participate fully in the debate and any subsequent decisions arising. 4.4 Staff from the Trust or representatives from other agencies may be invited to attend the committee for specific discussions, as required. The perspectives and contributions of Expert Service Users and Carers are recognised and valued by the Trust and therefore, they may be invited to attend the Committee, at the discretion of the Chair. 5. Quorum 5.1 The meeting will be considered to be quorate with five or more members, to include at least one Non-Executive Director and one operational lead. 5.2 It is expected that members of the Committee will attend a minimum of three Committee Meetings each year but should aim to attend all scheduled meetings. This will be monitored by the Committee Chair via the minutes and signing sheet. The attendee list will be reviewed on an annual basis and any concerns will be highlighted to the Trust Board. 14
141 6. Reporting 6.1 The Director of People and Corporate Development will make arrangements for the administration of the Committee. He or she will ensure that the minutes of the Committee meeting shall be formally recorded, the ratified minutes submitted to the private session of the Trust Board and shall provide appropriate support to the Chair and Committee members. 6.2 The Chair of the Committee will report on a regular basis to the open session of the Trust Board identifying any issues that require disclosure, or require executive action. Due to the nature of the issues considered, it may be necessary for the committee to liaise with other sub-committees, in which case specific and appropriate arrangements will be agreed. 7. Frequency of Meetings 7.1 The Committee will meet at least quarterly. 8. Review 8.1 The Committee will undertake an assessment of its overall effectiveness and compliance with these terms of reference at least annually. This review process will be in the form of a self-assessment checklist and will include the development of the following year s reporting cycle. 8.2 The terms of reference will be formally reviewed by the Committee as part of this assessment. Any proposed amendments to the terms of reference will be ratified by the Trust Board. 15
142 APPENDIX 2 SELF-ASSESSMENT EFFICIENCY AND EFFECTIVENESS CHECKLIST FOR MHA SC Efficiency Does the Committee remain abreast of legal and regulatory issues pertinent to its role? Has the Committee considered how it integrates with other relevant committees and groups? Has the Committee considered and sought assurance on the quality/ robustness of data behind reports received? Does the Committee review policies and procedures pertinent to the MHA and where relevant, recommend them for approval? Does the Committee review and monitor trends relating to the application of the MHA? Does the Committee receive and review reports from the CQC relating to MHA functions, and review resulting action plans? Does the Committee receive the results of clinical audits which pertinent to the use of the MHA, and oversee the development of recommendations? Does the Committee support the role of the MHA Manager and the MHA Administration function? Does the Committee appropriately support and liaise with the Associate Lay Managers peer group? How does the Committee assure itself of the effectiveness of the Associate Lay Manager role and function? Effectiveness Does the Committee remain abreast of legal and regulatory issues pertinent to its role? Has the Committee considered how it integrates with other relevant committees and groups? Has the Committee considered and sought assurance on the quality/robustness of data behind reports received? Does the Committee review policies and procedures pertinent to the MHA and where relevant, recommend them for approval? Does the Committee review and monitor trends relating to the application of the MHA? Does the Committee receive and review reports from the CQC relating to MHA functions, and review resulting action plans? Does the Committee receive the results of clinical audits which are pertinent to the use of the MHA, and oversee the development of recommendations? Does the Committee support the role of the MHA Manager and the MHA Administration function? Does the Committee appropriately support and liaise with the Associate Lay Managers peer group? How does the Committee assure itself of the effectiveness of the Associate Lay Manager role and function? 16
143 Board meeting date: 06 th August 2014 Agenda Item number: 10.8 Enclosure: 10 Report Title: Trust Wide Risk Register Accountable Director: Author (name & title): Wendy Pugh, Director of Operations and Nursing Neil Tong (Acting Clinical Governance Facilitator) Purpose of the report: To provide the Trust Board information on the Red Risks Held on the Trust Wide Risk Register, in line with the Trust s Risk Management Strategy Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Governance and Quality Committee Date reviewed: 9 th July 2014 All relevant risks have been reviewed by Governance and Quality Committee. Any remaining strategic risks have been reviewed by Finance & performance Committee or their appropriate director or a nominated deputy Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Please give brief details: Some of the risks held on the register have the ability to directly or indirectly impact upon the care/services offered The Trust Wide Risk Register Provides a representation of the Trusts Red Risks and the responses to managing/action planning these risks; some (due to the nature of the risk) provide a response to a short term or long term issue Some of the risks held on the Trust Wide Risk
144 Register impact upon the future viability / effectiveness of the Trusts operations. Risk FINAN 1 specifically relates to the long term outlook in relation to CIP Well-led Safe Some risks held on operational risk registers pertain to issues around service redesign and may have impacts upon leadership and staffing issues The appropriate management of risk is central to the provision of a quality, safe service. In particular CQC Outcome 16 Assessing and monitoring the quality of service provision.
145 Title Trust Wide Risk Register Introduction It is the purpose of this report to provide the Trust Board with the newly updated Trust Wide Risk Register. A number of these risks have been agreed and reviewed by the Trust s Governance and Quality Committee and Finance and Performance Committee. Governance and Quality Committee reviewed the following risks: FINAN HR002 OPS 013 PERF 09 In addition to the above risks a number of strategic risks were also reviewed (risks which do not relate to the day to day operations/quality/governance. These risks are: 226 STRAT 18 Summary of key points, issues and risks There are currently 8 risks held on Dudley and Walsall Mental Health Partnership NHS Trust s Trust Wide Risk Register. In line with the Trust s Risk Management Strategy this is an amalgamation of all the Red Risks across the organisation and those red strategic risks identified by the board. Further detail (if required) Table 1.1 and 1.2 outlined the source of the risks held on the Trust Wide Risk Register and additional further details (including their impacts on Quality/Operational issues (where appropriate). The full details of the risks are outlined in appendix 1
146 Table 1.1 Summary of Risk Risk ID Risk description Updates/additional information 202 The Better Care Fund (BCF) involves circa 1.9bn of This presents several elements of risk: NHS funding being allocated to a pooled budget to CCG commissioners are likely to have less provide integrated health and social care services. funding to invest in health services from April 2014 (average per CCG 10-15m) - this could impact directly on Trust income. Pathway redesign to create the BCF services could impact on DWMHPT pathways and services. There is no national template for creation of the BCF and plans are in the early stages of development. In some areas, planning is being led by non-finance leads which could increase financial risk inherent within service development plans / assumptions regarding cash releasing savings created by the BCF The Trusts existing block contract arrangement could put the Trust at risk if plans do not come to fruition and CCGs look to reducing the block contract to fund any gaps. The extent of activity change required to fund the BCF is large enough to cause considerable financial stress if BCF services 225 The risk of insufficient resilience and skills in leadership, which may result in poorly engaged, demotivated staff and poor service quality. 226 The Trusts ability to respond to rising demands in relation to current healthcare reforms including the Trusts FT application FINAN1 HR 002 Inability to meet CIP targets and the impact on the viability of the Trust. Reduction in Local Authority Funding for Mental Health Social Care Workforce, which may impact on service delivery and on the viability of the S75 agreements and plans do not come to full fruition Risk reviewed by Director of People and Corporate Development. Risk to remain on the Trust Wide Risk Register. No changes to risk. Risk has been added following discussions at Trust Board and the Board Development Session. Risk has been created from merger of risks STRAT 1 and FT 14 Issues Include: Costed service plans constantly in development Lack of clarity around commissioner investment plans and resulting CIP requirement from existing baselines Reduction in investment by Local Authorities Efficiency of 4 percent has been experienced for a number of years and will be experienced going forward Risk reviewed and agreed by Director of Operations and Nursing. Additional details added/reviewed by Director of People and Corporate Development Status of Risk = = = = =
147 Risk ID Risk description Updates/additional information OPS 013 A current lack of strategic direction in relation to records Risk reviewed at Directorate Risk Meeting. management leading to unacceptable practice in Changes to controls and actions within risk to be relation to record keeping within the organisation. updated and included as part of risk at next Governance and Quality Committee. Governance manager to ensure that records management (strategic direction) is included at PERF09 STRAT18 Maintaining Data Quality.. Increasingly competitive environment for Health Care providers, potentially threatening existing and future business. the next board development session Issues include Lack of external assurance on data quality since the implementation of OASIS Clinical and system processes not aligned Capacity and cultural changes within operational teams regarding the prioritisation of data quality Cultural challenges within the Performance and Informatics Teams Lack of Effective interface between Informatics and Operational Team Increasing focus on the completeness and accuracy of the MHMDS by external bodies to form a view of the organisation in the context of an imminent CQC inspection Risk reviewed by Director of People and Corporate Development. No changes proposed to risk. Status of Risk = = = Table 1.2 Number of risks on the Source of risk (how the risk has been identified) risk register Strategically identified 2 National initiative / Guidance / reforms 1 Workforce Statistics 1 Finance Projections / Data 1 Feedback from stakeholders / Partners 1 Committees actions / options appraisal 1 Departmental Priorities / Pressures 1 Recommendation It is recommended that the Trust Board approve the enclosed copy of the Trust Wide Risk Register and the details included within this report, which outlines the Red Risks to the organisation. Board action required The board is asked to approve the Trust Wide Risk Register.
148 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts 202 The B e tte r C a re Fund (BCF ) invo lves c irca 1.9bn o f NHS fund ing be ing a lloca ted to a poo led budge t to p rov ide in teg ra ted hea lth and soc ia l ca re se rv ices. T h is p resen ts seve ra l e le m en ts o f risk as fo llo w s : * CCG co m m iss ione rs a re like ly to have less fund ing to invest in hea lth se rv ices fro m A p ril 2014 (ave rage pe r CCG m ) - th is cou ld im pac t d irec tly on T rus t inco m e. * P a th w ay redes ign to c rea te the BCF se rv ices cou ld im pac t on D W M HP T pa th w ays and s e r v ices * The re is no na tiona l te m p la te fo r c rea tion o f the BCF and p lans a re in the ea rly s tages o f deve lop m en t. In so m e a reas, p lann ing is be ing led by non -finance leads w h ich cou ld inc rease financ ia l risk inhe ren t w ith in se rv ice deve lop m en t p lans / assu m p tions rega rd ing cash re leas ing sav ings c rea ted by the BCF * The T rus ts ex is ting b lock con trac t a rrange m en t cou ld pu t the T rus t a t risk if p lans do no t co m e to fru ition and CCG s look to reduc ing the N a tiona l In itia tive / G u idance 05 /03 /2014 M a rk A xce ll Trust Board 4 4 R ed 16 D irec to r o f F inance and P e rfo rm ance seek ing d irec t invo lve m en t in p lann ing fra m e w o rk to ensu re the T rus t is c lose to deve lop ing p lans and can m itiga te any risks a ris ing, e ithe r d irec tly p resen ting to the T rus t o r the w ide r hea lth econo m y. D ud ley and W a lsa ll M en ta l H ea lth P a rtne rsh ip NHS T rus t CEO is a m e m be r o f W a lsa ll's in teg ra tion boa rd, a key fo ru m to m ove fo rw a rd w ith p lans. D ra ft p lans rec ieved fro m bo th hea lth econo m ies. D of P has es tab lished co m m un ica tion channe ls w ith bo th CCG s / M B C s rega rd ing the BCF in o rde r to be tte r unde rs tand p lans and the po ten tia l im pac t on the hea lth econo m y, pa th w ays, and the T rus t R egu la r E xec leve l m ee ting es tab lished w ith D ud ley CCG w ho w ill be ho ld ing the poo led budge t in D u d l e y 4 4 R ed 16 D of P to m ee t w ith C F O a t W a lsa ll CCG to fu rthe r unde rs tand p lans E s tab lish M en ta l H ea lth o f the p lann ing fra m e w o rk fo r bo th hea lth econo m ies and con tinue a ttendance a t m ee tings, beco m ing fu lly a w a re o f p lans and s tages o f deve lop m en t and risks inhe ren t w ith in. 4 3 A m be r /07 /2014 R isk rev ie w ed a t G ove rnance and Q ua lity C o m m ittee R isk to re m a in sco red as a red r i s k.
149 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts b lock con trac t to fund any gaps * The ex ten t o f ac tiv ity change requ ired to fund the BCF is la rge enough to cause cons ide rab le financ ia l s tress if BCF se rv ices and p lans do no t co m e to fu ll fru ition. 225 The risk o f insu ffic ien t res ilience and sk ills in leade rsh ip, w h ich m ay resu lt in poo rly engaged, de m o tiva ted s ta ff and poo r se rv ice qua lity. W o r k f o r c e S t a tis tic s 09 /06 /2014 M a rsha In g ra m Chief Executive Executive Directors 4 4 R ed 16 S ta ff su rveys a re unde rtaken on a regu la r bas is. T rus t has a robus t leade rsh ip p rog ra m m e The T rus t has deve loped a nu m be r o f qua lity m e trics to m easu re se rv ice qua lity. 4 4 R ed 16 T rus t CQC ac tion p lan (cu rren tly be ing im p le m en ted ). S ta ff engage m en t w o rkp lan (cu rren tly be ing im p le m en ted ) S ta ff leade rsh ip deve lop m en t p lan (cu rren tly be ing im p le m en ted ). 4 2 A m be r 8 S ta ff S u rvey R esu lt s Q u a lit y m on ito ring m e tri c s 21 /07 /2014 R isk rev ie w ed by D irec to r o f P eop le and C o rpo ra te D eve lop m en t. R isk to re m a in on the T rus t W ide R isk R eg is te r. N o changes to risk. 226 The T rus ts ab ility to respond to ris ing de m ands in re la tion to cu rren t hea lthca re re fo rm s inc lud ing the T rus ts FT app lica tion S tr a te g ic a lly Iden tifie d 23 /06 /2014 M a rsha In g ra m Trust Board Trust Directors R ed Jacky O'Sullivan S ys te m p lans ag reed by T rus t, C lus te r and PCT s. M en ta l H ea lth P rog ra m m e B oa rd is e s ta b lished. T rus t a ttends co m m iss ione r CQR m ee ting (m e m be rsh ip expanded ) E xpe rienced FT P ro jec t M anage r FTPB and T rus t B oa rd ove rs igh t o f in te rna l p rocesses R obus t links w ith M on ito r and NHS T DA D e ta iled rev ie w o f Q ua lity and G ove rnance C o m m ittee has been c o m p le ted B oa rd s ign -o ff o f de ta iled ac tion p lans to add ress M on ito r feedback F T P rog ra m m e B oa rd is in p lace R egu la r p rog ress d iscuss ions be ing he ld w ith M on ito r assessm en t tea m. 4 4 R ed 16 N eed to F u rthe r D eve lop re la tionsh ips w ith G P s and CCG s to take th rough ou r jou rney o f ST (O ngo ing m on th ly m ee tings ) E nsu re lock in o f co m m iss ione rs, CCG s and C lus te rs to sys te m p lans (O ngo ing ) 4 2 A m be r 8 FTPB repo rts and M inu tes R egu la r repo rts to M E x T, G ove rnance and Q u a lit y C o m m ittee and T rus t B oa rd M en ta l H ea lth P rog ra m m e B oa rd SHA F T read iness assess m e n t p r ocess. S tra teg ic P a rtne rs. 01 /07 /2014 R isk has been added fo llo w ing d iscuss ions a t T rus t B oa rd and the B oa rd D eve lop m en t S ession. R isk has been c rea ted fro m m e rge r o f risks STRAT 1 and F T 14 Q G A F se lf assessm en t sco re 3.5 o r below Foundation T rus t A ssess m e n t p rocess
150 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts F INAN 1 Inab ility to m ee t C IP ta rge ts and the im pac t on the v iab ility o f the T rus t. Issues Inc lude : * C os ted se rv ice p lans cons tan tly in deve lo p m e n t * Lack o f c la rity a round co m m iss ione r investm en t p lans and resu lting C IP requ ire m en t fro m ex is ting base lines * R educ tion in investm en t by Loca l A u th o rities * E ffic iency o f 4 pe rcen t has been expe rienced fo r a nu m be r o f yea rs and w ill be expe rienced go ing fo rw a rd F inance P ro jec tions / D a t a 28 /02 /2011 M a rk A xce ll 5 4 R ed 20 D e ta iled deve lop m en t o f cos t im p rove m en t p rog ra m m e A pp roach to C IP has been ag reed a t F inance C o m m ittee P M O B oa rd es tab lished Leve l o f C IP has been co m m un ica ted to ope ra tiona l tea m s fo llo w ing LTF M re fresh (Ju ly 2013 ) M anage m en t a rrange m en ts in p lace fo r de live ry o f co rpo ra te cos t sav ings A rrange m en ts fo r m on ito ring p rog ra m m e o f C IP no w in p lace C IP ta rge ts be ing m e t th rough ag reed d ises tab lish m en t C on tinue to m anage locu m m ed ica l cos ts as ag reed th rough F&a m p ;P Q ua lity Im pac t A ssess m en t fo r a ll 2013 /14 and 2014 /15 sche m es a ll upda ted F inance tea m m e m be rs o f S e rv ice T rans fo rm a tion w o rk g roups and a lso dec is ion m ak ing P rog ra m m e B oa rd 5 3 R ed 15 W o rk requ ired to ensu re P O D s and repo rting fra m e w o rk is linked e ffec tive ly in to co m p le ted Q ua lity Im pac t A ssess m en ts (O ngo ing ). R ev ie w o f repo rt fro m rev ised P O D s and repo rting fra m e w o rk acco rd in g ly T rus t B oa rd to cons ide r ne w co m m un ica tion on C IP th rough tea m b rie f, bu ild ing on p rev ious co m m un ica tions, to ensu re tha t the m essage is w e ll unde rs tood rega rd ing the sca le o f the cha llenge 5 1 G reen 5 V a rious F inance and P e rfo rm ance repo rts inc lud ing : R epo rts to B oa rd R epo rts to F&P C o m m itt e e inc lud ing ind iv idua l ac tion p lans on p ressure a reas. R epo rts to M EXT R ev ie w s by ex te rna l assesso r s inc lud ing SHA, HDD and M on ito r In te rna l aud it repo rts a round C IP g iv ing fu rthe r assurance 09 /07 /2014 R isk deba ted by G ove rnance and Q ua lity C o m m ittee. R isk to re m a in as a red risk A c tive pa rtne r o f the M en ta l H ea lth P rog ra m m e B oa rd m a in fo ru m fo r co m m iss ione r lia ison. S ens itiv ity ana lys is bu ilt in to cu rren t p lans and fu rthe r deba te had rega rd ing m on ito r assum p tions and T rus t app roach to m itiga tion. R e m ode lled e ffic iency p lan due to changes in M on ito rs requ ire m en ts, ag reed by T rus t boa rd, F inance and P e rfo rm ance co m m ittee and M E x T S trong financ ia l pe rfo rm ance to da te in yea r R epo rting a rrange m en ts to boa rd enhanced s ince A ugus t 2013 to p rov ide m o re de ta il on sche m es as w e ll as qua lity im pac t assessm en ts M on ito ring o f bank, agency and locu m s no w fo rm s pa rt o f finance repo rt and d iscuss ion a t bo th F and P and M EXT. P lans in p lace fo r 2014 /15 and m a jo rity in p lace fo r 2015 /16
151 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts H R 002 R educ tion in Loca l A u tho rity Funding fo r M en ta l H ea lth S oc ia l C a re W o rk fo rce, w h ich m ay im pac t on se rv ice de live ry and on the v iab ility o f the S 75 ag ree m en ts Feedback F r o m S takeho lde rs / P 30 /05 /2012 W endy P ugh 4 4 R ed 16 S ec tion 75 ag ree m en ts p rov ide fo rm a l p la tfo rm as the bas is fo r any fu rthe r nego tia tions in fund ing and resou rce changes Jo in t app roach ag reed w ith W a lsa ll M B C rega rd ing im p le m en ta tion o f fund ing reduc tions. R isk A ssess m en ts on loss o f pos ts has been co m p le ted 4 4 R ed 16 D iscuss ions ongo ing a t P O G (M on th ly ) 4 2 A m be r 8 R epo rts to M EXT U pda tes to B oa rd 21 /07 /2014 R isk rev ie w ed and ag reed by D irec to r o f O pe ra tions and N u rs ing. A dd itiona l de ta ils added /rev ie w ed by D irec to r o f P eop le and C o rpo ra te D eve lop m en t R egu la r d iscuss ions be ing he ld a t P a rtne rsh ip O pe ra tions G roup. A dd itiona l sho rt te rm capac ity has been co m m iss ioned O P S 013 A cu rren t lack o f s tra teg ic d irec tion in re la tion to reco rds m anage m en t lead ing to unacceptab le p rac tice in re la tion to reco rd keep ing w ith in the o rgan isa tion. C o m m itt e e A c tions / O p tions A p 01 /04 /2011 W endy P ugh Tom Jinks 4 4 R ed 16 A n op tions app ra isa l has been co m p le ted in re la tion to the fu tu re d irec tion o f reco rds m anage m en t w ith in the o rgan isa tion. The o rgan isa tion is to e m p loy an In te rim R eco rds M anage r to add ress the issues rega rd ing reco rds m anage m en t w ith in the o rgan isa tion. W e have used the se rv ices o f a consu ltan t to ensu re the o rgan isa tion has s tra teg ic op tions as a w ay fo rw a rd. T h is w ill be w o rked up ove r the nex t 6 m on ths. Loca l aud its a re in p lace re the qua lity o f c lin ica l reco rds and these a re fed th rough to a va rie ty o f c o m m itt ees A nu m be r o f reco rds in a rch ive have been lifted fro m F M C to R eca ll w ith se rv ice be ing o ffe red a t a be tte r ra te. T ra in ing sess ions have p rov ided to s ta ff w ho m ay be requ ired to reques t reco rds fro m o f s ite s to rage. O ff s ite reco rds in a rch ive have been trans fe rred fro m F M C to R eca ll 4 4 R ed 16 K ey dec is ions to be m ade rega rd ing : o In teg ra tion o f m ed ica l and nu rs ing n o tes o R eco rds T racking P rocesses o A ccoun tab le co m m ittees o S tanda rd ised fo rm a ts o Issues a round a rch iv ing p rac tices (S o m e o f s ite reco rds in a rch ive have been T rans fe rred fro m F M C to R eca ll) o T ra in ing (T ra in ing sess ions have been p rov ided fo r s ta ff w ho m ay be requ ired to requ ire reco rds he ld o ff s ite ) (D ec is ions to be m ade based upon s tra tegy co m p le tion (due June 2013 ) Job is cu rren tly ou t to adve rt and has been banded as a band 7. R ec ru itm en t expected by Janua ry 2014 D iscuss ions cu rren tly ongo ing w ith R eca ll. The T rus t is cu rren tly exp lo ring scann ing so lu tions and the res tric tions o f no te m ove m en t. P resen ta tion by R eca ll a t the N ex t IG and R M C o m m ittee 4 1 G reen 4 R epo rts to key co m m ittees such as M e X T ou tlin ing p rog ress 23 /07 /2014 R isk rev ie w ed a t D irec to ra te R isk M ee ting. C hanges to con tro ls and ac tions w ith in risk to be upda ted and inc luded as pa rt o f risk a t nex t G ove rnance and Q ua lity C o m m itt e e. G ove rnance m anage r to ensu re tha t reco rds m anage m en t (s tra teg ic d irec tion ) is inc luded a t the nex t boa rd deve lop m en t sess ion A dd itiona l con tro ls have been im p le m en ted to res tric t the m isuse o f o ff s ite s to rage and to ensu re tha t hea lth reco rds a re des troyed in line w ith In fo rm a tion G ove rnance bes t p rac tice. T rus t is to unde rtake a re fresh in re la tion to th is issue and a re to look a t in te rna l so lu tions to m itiga te any a c tions. In te rna l aud it to be ing w o rk on A ud it o f S ys te m s and con tro ls a round
152 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts hea lthca re reco rds m anage m en t in qua rte r 3 o f 2013 /14. T h is w ill he lp in fo rm w he the r the cu rrne t s truc tu re suppo rts the requ ired gove rnance o r w he the r fu rthe r changes a re requ ired. PERF 0 9 M a in ta in ing D a ta Q ua lity Issues ; * Lack o f ex te rna l assurance on da ta qua lity s ince the im p le m en ta tion o f O A S IS * C lin ica l and sys te m p rocesses no t a ligned * C apac ity and cu ltu ra l changes w ith in ope ra tiona l tea m s rega rd ing the p rio ritisa tions o f da ta qua lity * C u ltu ra l cha llenges w ith in the P e rfo rm ance and In fo rm a tics Tea m s * Lack o f E ffec tive in te rface be tw een In fo rm a tics and O pe ra tiona l Tea m s * Inc reas ing focus on the co m p le teness and accuracy o f the M H M DS by ex te rna l bod ies to fo rm a v ie w o f the o rgan isa tion in the con tex t o f an im m inen t CQC inspec tio n. D epa rtm e n ta l P rio rities / P res 13 /07 /2012 M a rk A xce ll Chris Reynolds 2 2 G reen 4 L ive da ta qua lity im p rve m en t p lan in p lace In te rna l aud its p rog ra m m ed fo r Q 4 on D a ta Q ua lity Im p rove m en t P rog ra m D Q cu rren tly sc ru tin ized a t CAR M A dd itiona l resou rce in p lace w ith in In fo rm a tics to im p rove D a ta Q ua lity R egu la r co m m un ica tion be tw een P e rfo rm ance and In fo rm a tics tea m s and O pe ra tiona l Tea m s T ra in ing p rog ra m o f O as is and C lin ica l P rocesses is cu rren tly in p lace A live ac tion p lan dea ling w ith the co m p le teness o f the M H M DS sub m is s io n S igned o ff m e tric spec ifica tion docu m en t in p lace fo r a ll K ey P e rfo rm ance Ind ica to rs 4 4 R ed 16 E nsu re sys te m a tic p rog ra m o f oas is tra in ing and suppo rt to ensu re c lin ica l p rocesses ag reed a re then re flec ted in oas is. R o llou t o f E O A S IS to co m m un ity se rv ices. D ependen t on func tiona lity ava ilab le in p roduc t (Ju ly 2014 ) R o ll ou t O A S IS to inpa tien ts to im p rove co m p le teness o f da ta and reduce risk o f dup lica tion o r e rro r (M a rch 2014 ) R e es tab lish an e ffec tive c lin ica l p rocess g roup tha t w ill he lp to ensu re sys te m and c lin ica l p rocess a lign m en t (ope ra tion o f the g roup is c ritica l) (M a rch 2014 ) E nsu re ro ling p rog ra m o f da ta qua lity im p rove m en t (O ngo ing ) E nsu re regu la r in te rna l aud it/rev ie w (ongo ing ) E nsu re regu la r jo in t in fo rm a tics and ope ra tions m ee ting to d iscuss kno w n issues (ongo ing ) C lose m anage m en t o f the in fo rm a tics func tion to ensu re tha t ro les and responsib ilities a re re flec tive o f the needs o f the o rgan isa tion 4 2 A m be r 8 In te rna l A ud its D a ta qua lity repo rts to CAR M 01 /07 /2014 T h is risk is cu rren tly be ing rev ie w ed fo llo w ing d iscuss ions a t the F inance & P e rfo rm ance C o m m itt e e. E nsu re co m p le tion to tim escale o f ac tion p lan in re la tion to M H M DS (A p ril 2014 )
153 Risk Register R i s k R isk D esc rip tion Sou rce o f R i s k D a te P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f Fu rthe r C o m m en ts STRAT 18 In c r eas in g ly c o m p e titiv e env iron m en t fo r H ea lth C a re p rov ide rs, po ten tia lly th rea ten ing ex is ting and fu tu re bus iness. S tr a te g ic a lly Iden tifie d 01 /04 /2011 G a r y G raha m Marsha Ingram 4 4 R ed 16 M a rke t ana lys is th rough Foundation T rus t IB P. CEO and C ha ir focusing on deve lop m en t o f re la tionsh ips w ith ne w co m m iss ion ing bod ies. O ngo ing im p le m en ta tion o f S e rv ice L ine R epo rting i.e. p ro fit and loss by se rv ice line. S ta rted to cons ide r a t T rus t B oa rd the po ten tia l a reas o f g ro w th fo r the T rus t. R isk is re la ted to co m m iss ione r/g P in ten tions go ing fo rw a rd re se rv ice co m pe tition o r look ing to p lu ra lity o f p r o v id e r s. 4 4 R ed 16 F u lly e m bed bus iness deve lop m en t P M O m ode l F u lly im p le m en t se rv ice line repo rting C on tinue to cap ita lise on ex is ting m echan is m s to in fluence co m m iss ione rs (M en ta l H ea lth P rog ra m m e B oa rd ) to m a in ta in s tab ility in the hea lth econo m y (ongo ing - R ev ie w ed m on th ly ). 4 3 A m be r 12 F T P ro jec t B oa rd In teg ra ted B us iness P lan M en ta l H ea lth P rog ra m m e B oa rd B us iness D eve lo p m e n t P M O repo rt to T rus t B oa rd 01 /07 /2014 R isk rev ie w ed by D irec to r o f P eop le and C o rpo ra te D eve lo p m e n t. N o changes p roposed to r i s k. T rus t B oa rd D iscuss ions B us iness O ppo rtun ities tea m deve loped by C E E s tab lish m en t o f M a jo r P ro jec ts B oa rd to ove rsee s tra teg ic deve lo p m e n ts B o th CCG s rep resen ted on S hado w C ounc il o f G ove rno rs M a rke t in te lligence repo rting to T rus t B oa rd T rus t has rec ru ited a B id S uppo rt M anage r to suppo rt the iden tifica tion o f ne w B us iness O ppo rtun ities. The T rus t is no w p roac tive ly deve lop ing bus iness cases w ith c o m iss ione rs Funding has been secu red fo r co m m e rc ia l a w a reness tra in ing. R ec ru itm en t o f resou rces to B O T - B id M anage r w ho has se t up regu la r feeds on fo rthco m ing tende rs. B oa rd dec is ion to inc rease focus on bus iness deve lop m en t - se t up o f 'G ro w th P M O ' B us iness deve lop m en t P M O m ode l ag reed and im p le m en ted. T rus t boa rd have ag reed tha t g ro w th is a s tra teg ic p rio rity fo r the F u tu re
154
155 Board meeting date: 6 th August 2014 Agenda Item number: 10.9 Enclosure: 11 Report Title: Quality Improvement Update Report Q1 2013/15 Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie Musson Head of Nursing, Quality and Innovation Purpose of the report: The purpose of presenting this report to the Trust Board is to provide a quarterly update on: The ongoing implementation of the Trust Quality Improvement Strategy including: progress against Trust Quality Improvement Priorities 2014/15 ongoing work to embed learning from the Francis report and other key publications. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Governance and Quality Committee Date reviewed: July 2014 Sustainable progress is being made in relation to the action plan - 53% of actions completed remaining ongoing. Where slippage has occurred dates have been reviewed and new timescales set. The committee received assurance that currently no risks require escalation. A meeting has taken place with the TDA whereby it was recommended that the action plan be amalgamated into an overarching improvement plan including TIP and CQC plans. The TDA have supplied a template whose emphasis is on the measurement of impact. The Committee recommends the report to the Trust Board in August for assurance In relation to the 2014/15 QI priorities the Governance and Quality Committee are due to receive a full update in August 2014
156 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Report underpinned, by the delivery of services that people are cared for with compassion, dignity and resect Alignment of standards across service to improve responsiveness through quality improvement initiatives Promoting use of evidence based standards to improve quality of care Staff involvement/exposure to ongoing quality improvement and training in line with Trust quality improvement strategic objectives Promoting safety culture
157 Title Quality Update Report Q1 2014/15 Introduction The purpose of this report to the Trust Board is to provide a quarterly update on the ongoing implementation of the Trust Quality Improvement Strategy including: progress against Trust Quality Improvement Priorities 2014/15 ongoing work to embed learning from the Francis report and other key publications. The Trust continues to implement the Quality Improvement Strategy and promote a culture of ongoing quality improvement throughout the services delivered (appendix 1 quality improvement strategic objectives). The Trust Board has set seven quality improvement priorities for 2014/15 within the Quality Account. These priorities have been published in June 2014 in the Trust s Quality account and widely disseminated across the Trust and shared with key partners (appendix 2 Trust quality improvement priorities 2014/15). To ensure the priorities are mapped into the Trust quality governance framework, a full quarterly update is provided to the Governance and Quality Committee, detailing progress and an overview of outcomes and exceptions. This report provides the Board with an overview of progress in Q1 and also provides assurance on the ongoing delivery of the Trust s Quality Improvement Strategy. The Board is asked to note that a refresh of the Quality Strategy is currently being undertaken to ensure it reflects the revised quality governance processes since development. This is due for completion by September 2014 Furthermore there is ongoing work within the Trust to utilise the recommendations from of the Francis and Winterbourne reports to drive quality improvement. This report provides an overview of this work and progress made. A quarterly update report was presented to the Governance and Quality Committee in July 2014 for full discussion on progress. Summary of key points, issues and risks The key points of this report are: It provides assurance that the Trust s Quality Improvement Strategy continues to be embedded within the services to drive the culture of continuous improving quality care and services It provides the Board with an overview of progress towards the quality goals set within the Trust s 7 quality improvement priorities for 2014/15 and how they are being developed to be an integral part of the Trusts quality governance framework. It details the continued work to embed the recommendations of both the Francis Report and Winterbourne report, ensuring they have local high impact. Further detail Full details are set out in the attached report and Appendices.
158 Recommendation 1. That the Trust Board note the progress made in relation to commencement of the 2014/15 Quality Improvement Priorities in quarter 1 2. The Trust Board note that sustainable progress has been made in relation to the delivery of the overarching Francis Action Plan and where slippage has occurred new timescales have been supported by the Governance and Quality Committee. Board action required The Board is asked to receive the report for information and assurance.
159 1. Quality Improvement Strategy Quarter 1 Quality Update Report Work continues to drive a culture of quality improvement as described in the Trusts Quality Improvement Strategy which is underpinned by the Trusts Quality Improvement Strategic Objectives see Appendix 1. During Q1, focus has been on commencement of the new priorities and also the continuation where priorities have been rolled over from 2013/14 (Appendix 2) To ensure effective implementation each priority has a project lead and identified key milestones. Furthermore, to ensure all priorities have measurable impact each project includes measurable outcomes defined in the project plans. Impact will be measured as indicated in the individual project milestones. The Governance and Quality Committee is due to receive a full update report for discussion at its meeting in August Progress against Quality Improvement Priorities Q1 The table on the following page provides headlines of progress made in Q1. Progress has been made with all priorities within this quarter. As five of these were new priorities, the focus during quarter 1 has been predominately on the set up of the projects. 5 Page
160 Table 1 Q1 Quality Improvement Priority Progress Quality Priority 1. Providing meaningful and effective inpatient activities 2. Embedding think Family model across CAMHS and AMH services. 3. Management of Disruptive and aggressive behavior Quality Improvement Initiative Undertake a full review of inpatient activities To develop and implement Trust wide standards based on locally defined best practice Development of joint protocols and pathways between adult and child mental health service to support think family approach Undertake a review of Trust guidance against best practice and review supporting policies To incorporate the principles of restraint reduction planning Enhance training to upskill staff in deescalation techniques Q1 Progress Lead Outcome Established steering group Commenced baseline audit including staff views and patient views to establish current activity across 3 hospital sites, both therapeutic and dimensional Established steering group Commence awareness raising across Trust Named Doctor and Vulnerable Adults Children s Lead delivered awareness training to consultants Escalation process for AMH doctors implemented to facilitate greater working together for complex families Restrictive practice steering group established to oversee the Quality Priority and review supporting suite of policies relating to least restrictive practice. Draft separate MAPA policy developed (previously with Local security management policy) Reporting and governance arrangements defined and incorporated into safeguard. Violence and aggression audit revised to reflect new guidance and establish baseline for reduction target. Project Lead HOS Consultant OT QI Support Clinical Quality Improvement Manager Project Lead Vulnerable Adults and Children s Lead HOS QI Support Clinical Process Manager Project lead Lead MAPA trainer HOS (acute, older adults) QI Support Clinical Quality Improvement Manager Compliance with Trust wide, evidence based standards for delivery of activities across inpatient services to promote recovery and wellbeing. Compliance with Trust wide standards and pathways for when there is more than one family member accessing AMHS and CAMHS Compliance with locally defined best practice standards. Agreed restraint reduction plan which is least restrictive for the service user. (defined by national standards) 6 Page
161 Quality Priority 4. Focusing on dementia care 5. Health Care Assistant Development Programme Quality Improvement Initiative To undertake review of staff competency and training and introduce revised skill based training programme To ensure the inpatient environment is conducive to best practice guidance and standards To revisit local standards based on best practice for behaviors which challenge in dementia inpatient services and person centered care. To implement Health Care development programme Q1 Progress Lead Outcome Delivered e learning dementia training to inpatient staff on dementia units Complete TNA specific to dementia Environment reviewed by specialist architects and immediate actions taken ( see CQC compliance action plan) Compliance audits Pilot programme evaluated and recommendations presented to MEXT for approval. Roll out plan agreed Manager pre course training developed Redesign of mentor workbook Project Lead Inpatient Manager Learning and Development NB this is being delivered as part of the Older Adult Service review QI Lead Head of Nursing and Quality Project Lead Learning and Development QI Support Head of Nursing and Quality Compliance against best practice guidelines Staff trained in line with Training needs analysis and training plan Environment is conducive to best practice guidance for dementia Staff trained in line with Training needs analysis and training plan 7 Page
162 Quality Priority 6. My Care Plan 7. Triangle of Care (TOC) Quality Improvement Initiative Revision of CPA training on outcome focused and service user led care planning. Revision of Trust wide clinical standards for care planning Continued implementation of triangle of care model. Q1 Progress Lead Outcome Commenced review of CPA policy in line with national standards and CPAA handbook Established a steering group with EBE representation Clinical audit of inpatient and community compliance against TOC standards EBE unannounced visits to selected wards to measure TOC standards Compilation of compliance audit due for submission to TOC National Steering Group in September 2014 (compliance submission to be presented to G&QC in September 2014 prior to submission) Project Lead Clinical Process Manager QI Support Quality Improvement Facilitator Project Lead OT Consultant/Professi onal Lead QI Support Head of Nursing, Quality and Innovation Service user will receive care plans that meet Trust wide clinical standards for care planning Accreditation by Triangle of Care Clinical Staff trained in Care awareness Family and Carer Satisfaction Compliance with Carers pathway standards 2. Overarching Francis Report Update Report Q This section of the report provides the Trust Board with an update on the overarching Francis report action plan which was agreed by the Trust Board in During Q1, there has been significant amount of work undertaken across the Trust to ensure the Trust continues to give given full consideration to the Francis Report and other key publications including Winterbourne. Appendix 3 provides progress against the Trust s action plan which has been presented to the Governance and Quality Committee in July The outcome of discussions that were held by the Committee are; Sustainable progress is being made in relation to the action plan. 53% of actions completed remaining ongoing. Where slippage has occurred dates have been reviewed and new timescales set. The committee received assurance that currently no risks require escalation. A meeting has taken place with the TDA whereby it was recommended that the action plan be amalgamated into an overarching improvement plan including TIP and CQC plans. The TDA have supplied a template with emphasis on the measurement of impact. 8 Page
163 APPENDIX 1 Quality Improvement Strategic Objectives Become more efficient and productive through quality improvements Meet and where possible exceed regulatory requirements To empower and skill staff to continuously improve the quality of care Vision: Better Together - delivering flexible, high-quality, evidence-based services to enable people to achieve recovery. Deliver high quality safe services Listen to, involve and empower service users and carers resulting in continuous quality improvement Deliver services that are clinically effective and outcome focused 9 Page
164 Local Quality Improvement Priorities APPENDIX 2 Vision: Better Together delivering flexible, high-quality, evidence-based services to enable people to achieve recovery 2013/14 Rollover My Care Plan Triangle of Care New for 2014/15 Therapeutic Activities for inpatients Think Family (parental MH/domestic violence/interface between CAMHS and AMH) Inpatient pilot kindliness and awareness in practice Implementation of HCA programme Violence and Aggression Restraint reduction Planning Focussing on dementia environment/training/learning from CQC The above illustrates the local priorities for Quality Improvement which the Trust will be focussing on during 2014/15. Each area for improvement is formulated into a measurable outcome measure. The priorities are aligned to the Trust Quality Improvement Strategic Objectives. 10 Page
165 Appendix 3 Overarching Francis, Winterbourne, Cavendish, Keogh and Berwick Action Plan Overarching Themes Through considering the recommendations within the reports, the following themes have been identified for incorporation into the Trusts ongoing quality improvement programmes. Much work has been completed and underway through existing workstreams, however to ensure the reports have been given full consideration by the Trust it has been integrated in an overarching workplan. These will be monitored operationally by MEXT with the Governance and Quality Committee having overarching responsibility for reporting progress to Trust Board. This report provide the first quarterly update on progress made (March 2014) Transforming Care: Winterbourne View Hospital Improve triangulation of safeguarding trends Further develop processes to take into account views of family s and carer s Improve triangulation of trends identified through the use of the Mental Health Act Improve compliance with MCA and DOLS Training Improve incident reporting system to capture further detail regarding restraint Francis Inquiry Pledge Values in Action Increase staff engagement in quality improvement Improve communication Duty of Candor continue to develop culture of openness Nursing Strategy incorporating learning from Francis Values based recruitment Integration The Cavendish Review To introduce bespoke Healthcare Assistant development programme The Keogh Mortality Review To ensure the principles identified in the report are incorporated into the themed action plan - Values in action (individual accountability and leadership) - Duty of Candor (transparency of data) - To note the Keogh inspection framework is likely to underpin further quality inspections. Berwick Review To further review recommendations following publication of national overarching quality improvement framework To review staffing levels following publication of national work 11 Page
166 Overarching Francis, Winterbourne, Cavendish, Keogh and Berwick Action Plan Overall Theme/ Where We Can Improve Winterbourne Systems in place to identify patterns of safeguarding issues linked to services Whilst the trust has systems in place to identify patterns of safeguarding issues, it was considered that further to ensure greater triangulation of information would be beneficial. What We Have Done Safeguarding Policies and Procedures Incident Reporting Safeguarding database Monthly governance reports Patient safety co-coordinators Safeguarding lead Safeguarding Strategic Group Exception reporting the Governance and Quality Committee Training Embedding lessons What We Intend To Do To improve the triangulation of trends including incident reporting, complaints, disciplinary investigations, Positions of Trust, serious incidents. Lead Governance Manager Completion Date February 2014 Monitoring Safeguarding Group Measure of success/ impact Integration of safeguarding into the quality dashboard Update June 2014 Completed by March 2014 Safeguard module now implemented which reports into the trusts electronic risk reporting process. Safeguarding has now been incorporated into the Trusts Quality dashboard The Trust has also established a triangulation meeting, which safeguarding is an integral component. The first meeting is scheduled for March Cont d 12 Page
167 Improve embedding lessons process to ensure information is incorporated from new Trust safeguarding data base and serious case reviews Vulnerable Adults and Children s Lead January 2014 August 2014 Safeguarding Group Safeguarding incorporated into Trusts embedding lessons process All current action plans from the safeguarding perspective have been incorporated into the embedding lessons process. The Trust has also commenced triangulation meetings to enable a joined up approach to lessons learned. The Strategic Safeguarding Group which is due to meet in July where progress will be monitored for assurance. Revised completion date: August Page
168 Overall Theme/ Where We Can Improve What We Have Done What We Intend To Do Lead Completion Date Monitoring Measure of success/ impact Update June 2014 Cont d Winterbourne Systems in place to identify patterns of safeguarding issues linked to services Whilst the trust has systems in place to identify patterns of safeguarding issues, it was considered that further to ensure greater triangulation of information would be beneficial. Cont d Safeguarding Policies and Procedures Incident Reporting Safeguarding database Monthly governance reports Patient safety co-coordinators Safeguarding lead Safeguarding Strategic Group Exception reporting the Governance and Quality Committee Training Embedding lessons Safeguarding dashboard to be revised following introduction of new safeguarding data base and requirements of safeguarding boards. This will include service line reporting. Patient Safety Facilitator Vulnerable Adults and Children s lead December 2013 Safeguarding Group Governance and Quality Committee Dashboard available including data for service lines Completed by March Safeguarding dashboard has been revised and is not an integral part of the Trust Quality report. This information is available for service lines This report is also received by the Commissioners Quality review meeting for assurance The content of monthly and quarterly returns to the safeguarding boards are being finalised trough the SGB sub groups and part of the commissioner contract. 14 Page
169 Overall Theme/ Where We Can Improve Winterbourne Systems and processes in services to take into account the views of service users, their families and other visitors Carer and family engagement is currently a Trust quality improvement priority for 2013/14. It was considered that this should continue to be a priority and incorporate the learning from Winterbourne What We Have Done Triangle of Care Care Planning Process SED visibility Service User and Carer Engagement Strategy EBE service /ward visits CQUIN Friends and Family Test Community Survey Inpatient survey Advocacy Care planning processes (CPA) Ward meetings Local service user and carer groups (within services) QPRs include SE reporting and monthly stats in dashboard for each service line Patient story to Trust board New online form on the public website One in 4 member magazine features service user stories What We Intend To Do To improve real time service user feedback opportunities including use of IPADs To systematically review how we are gathering patient experience and feedback through local surveys Lead Service Experience Lead Service Experience Lead Completion Date Ongoing from Mar 14 September 2014 Complete Monitoring Governanc e and Quality Committee Governanc e and Quality Committee Measure of success/ impact Real time feedback systematically embedded in service line and pan trust performance dashboards. Rolling programme of local patient experience surveys Update June 2014 The Trust continues to utilize real time feedback Net promoter by service line established since 12/13. IPADs to replace trackers for bespoke and generic S E surveys in 13/14. EBE feedback However from March 2014 further targeted work will be commenced IPAD s are now available to use for Patient Experience feedback. Our EBE s will be using IPAD s during ward visits, surgeries, forums, workshops. Bespoke surveys have been designed, delivered and analysed within service experience, Our Experts by Experience continue to attend clinical teams on a planned and regular basis and provide real time feedback of patients comments, concerns. Revised completion date: September 2014 Completed by March Page
170 To incorporate new CQC 5 Questions into service user feedback processes To re-launch Trusts Service user and Carer forum Service Experience Lead Service Experience Lead April 14 September 2014 Complete Nov 2013 Governanc e and Quality Committee Trust Board and G & Q Generic S E surveys include CQC 5 questions Regular meetings of new Mental Health Forum held (quarterly from November 2013 Ongoing - We are working on the development of 5 core questions which will be linked to CREWS and will form the basis of our generic survey. This will be used for ongoing monitoring of the effectiveness of our action plans in response to various forms of feedback, including national surveys. Revised completion date: September 2014 Completed March 2014 To improve usage of patient stories incorporate question within clinical record to establish if service users would be interested in sharing their story Service Experience Lead April 2014 October 2014 Governanc e and Quality Committee Regular use of patient stories embedded in trusts Quality Governance processes This action is ongoing due to other data quality improvement priorities. Revised completion date: October Page
171 Overall Theme/ Where We Can Improve Winterbourne Methods in place of identifying competences required and achieved by staff in inpatient services No further actions identified however once published to review the implications of the proposed nurse revalidation process What We Have Done Safeguarding competency framework Medicines management framework HCA training programme MAPA live register and training Mandatory training Suicide prevention training Supervision and PDR process Clinical audit Medical revalidation What We Intend To Do Incorporate Nurse revalidation once published Lead Head of Nursing, Nursing and Innovation Associate Director of Learning and Development Completion Date Review June 2014 September 2014 Monitoring MExT Measure of success/ impact Nurse revalidation implemented Update June 2014 National Guidance is currently in the consultation stage, the Trust will be engaging in the consultation and will be mapping out potential implications for the Trust to support the implementation of nurse revalidation. Revised completion date: September Page
172
173 Board meeting date: 6 th August 2014 Agenda Item number: Enclosure: 12 Title Service Experience Desk Annual Report 2013/14 Accountable Director: Author (name & title): Marsha Ingram, Director of People and Corporate Development Mary Bytheway, Strategic Planning Manager Action required from the Board Decision / Approval Gain assurance Discussion Information Purpose of the report: To present the Trust s Service Experience Desk Annual report for approval. The report incorporates the Complaints Annual report. What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Governance & Quality Committee July 9 th 2014 The committee recommended that some charts be realigned and terms be explained. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources What impact or implications does this report have on the following: Caring Responsive Effective Please give brief details: Listening to, understanding acting upon feedback about our services allows us to develop meaningful improvements that impact on the experience of our service users and their families and carers. SED is a focal point for all feedback and provides a holistic and responsive approach to using feedback to drive quality
174 Well-led Safe improvements. Service experience forms a crucial part of the Trust s service line management processes and supports ongoing quality improvement. It feeds into reporting at all levels across the Trust People often contact SED crisis, or when they don t know who else to contact. It offers a route in to the Trust for otherwise vulnerable people. Triangulation of SED activity with serious incidents and safeguarding issues creates a robust approach to managing complex cases.
175 Title Service Experience Desk Annual Report 2013/14 Introduction As a provider of services, we are committed to ensuring that representatives of those people who use our services and their carers are fully integrated within our decision-making and governance structures. On a day-to-day basis, we work closely with a wide range of Service User and Carer organisations across the two boroughs, seeking their views and ensuring their participation in the planning and delivery of services. Patient knowledge and experience are essential for understanding how best to improve care. The very best user and carer involvement harnesses a passion for making things better and over the past year, we have made enormous progress with implementing and expanding our involvement strategy. Our commitment to putting service users and carers at the heart of everything we do is demonstrated by the way that service user and carer involvement is taken into consideration at the forefront of new projects, initiatives and developments. We try to focus on the things that matter the most for patients, communities and staff and emphasise a culture of genuine engagement, involvement and transparency. Summary of key points, issues and risks The contents of this report specifically meet the requirements set out for Complaints Annual Reports in section 18 of the Local Authority Social Services and National Health Service Complaints (England) Regulations The requirements state that the report should specify: the number of complaints which the responsible body received the number of complaints which the responsible body decided were well-founded the number of complaints which the responsible body has been informed have been referred to: o the Health Service Commissioner to consider under the 1993 Act; or o the Local Commissioner to consider under the Local Government Act 1974 And the report should summarise: the subject matter of complaints that the responsible body received any matters of general importance arising out of those complaints, or the way in which the complaints were handled any matters where action has been or is to be taken to improve services as a consequence of those complaints Further detail The full report is attached at Appendix 1.
176 Recommendation The SED Annual Report is recommended to the Board for information and assurance. Board action required The Board is asked to approve the report for publication.

177 Service Experience Desk Annual Report 2013/14 (Incorporating Complaints, Compliments and PALs)
178 Contents 1 CHAIR S AND CHIEF EXECUTIVE S FOREWORD ABOUT THE TRUST OUR VISION AND VALUES SERVICE EXPERIENCE DESK ACTIVITY CELEBRATING POSITIVE FEEDBACK COMPLAINTS MANAGEMENT OUTCOME OF COMPLAINTS LEARNING FROM FEEDBACK SERVICE EXPERIENCE - THE FULL PICTURE KEY ACHIEVEMENTS 2013/ PRIORITIES FOR 2014/ JARGON BUSTER...20
179 1 Chair s and Chief Executive s Foreword Welcome to the Service Experience Desk annual report from Dudley and Walsall Mental Health Partnership NHS Trust. As a provider of services, we are committed to ensuring that representatives of those people who use our services and their carers are fully integrated within our decision-making and governance structures. On a day-to-day basis, we work closely with a wide range of Service User and Carer organisations across the two boroughs, seeking their views and ensuring their participation in the planning and delivery of services. Patient knowledge and experience are essential for understanding how best to improve care. The very best user and carer involvement harnesses a passion for making things better and over the past year, we have made enormous progress with implementing and expanding our involvement strategy. Our commitment to putting service users and carers at the heart of everything we do is demonstrated by the way that service user and carer involvement is taken into consideration at the forefront of new projects, initiatives and developments. We try to focus on the things that matter the most for patients, communities and staff and emphasise a culture of genuine engagement, involvement and transparency. The contents of this report specifically meet the requirements set out for Complaints Annual Reports in section 18 of the Local Authority Social Services and National Health Service Complaints (England) Regulations The requirements state that the report should specify: the number of complaints which the responsible body received the number of complaints which the responsible body decided were well-founded the number of complaints which the responsible body has been informed have been referred to the Health Service Commissioner to consider under the 1993 Act; or the Local Commissioner to consider under the Local Government Act 1974 And the report should summarise: the subject matter of complaints that the responsible body received any matters of general importance arising out of those complaints, or the way in which the complaints were handled any matters where action has been or is to be taken to improve services as a consequence of those complaints
180 2 About the Trust Dudley and Walsall Mental Health Partnership NHS Trust was formed on 1st October 2008 and specialises in the treatment of both common and complex mental health conditions in children, adults and older people. It provides a comprehensive range of mental health and social care services, including: Community mental health services for children, adults & older people Inpatient services for adults and older people Primary Care Mental Health services (including IAPT) Mental Health Social Care Services (via local authority partnerships) Psychological Therapies Substance Misuse Services Employment, education and training support for people with mental health problems Specialist Deaf CAMHS (national hub) The Trust predominantly serves the people of the Black Country boroughs of Dudley and Walsall within the West Midlands, with a combined population of around 560,000. The Trust provides services from 28 sites (including 3 hospitals) across the two boroughs. 2.1 Our Vision and Values The Trust s vision is one of a recovery oriented service. The vision, encapsulating the concept of the benefits arising from a single mental health trust for the populations of Dudley and Walsall, is shown below. Better Together - delivering flexible, high-quality, evidence-based services to enable people to achieve recovery. The Trust s vision has been guided by national, regional and local intelligence and strategies where there is a growing emphasis on the well-being of the population and a focus on prevention and early detection and intervention. The Trust is committed to upholding the principles and values of the NHS in England (NHS Constitution, 2009). There are seven key principles that guide the NHS in all it does. They are underpinned by core values which have been derived from extensive discussions with staff, patients and the public. Recovery is not just about what services do to or for people. Rather, recovery is what people experience themselves as they become empowered to manage their lives in a manner that allows them to achieve a fulfilling, meaningful life and contributing a positive sense of belonging in their communities (NIMHE, 2005). The core values of the Trust also reflect the NHS Constitution and are significant in that they inform attitudes and therefore behaviours of staff. The Trust s core values are:

 is the central point of contact for all concerns and enquiries whether these are formal or informal, complaints,")
181 Figure 1 Trust Values Respect and dignity Compassion Working together for patients Commitment to quality of care Improving lives Everyone counts These values are realised within the Trust s everyday practice and are at the heart of the organisational development agenda. The Trust reviews and reflects upon the appropriateness of its vision, values and principles each year prior to defining the annual objectives. 3 Service Experience Desk Activity The Trust s Service Experience Desk (SED) is the central point of contact for all concerns and enquiries whether these are formal or informal, complaints, compliments or requests for information. The Trust welcomes feedback about its services and considers this a valuable source of insight into the quality of our services. Being a patient, relative or carer can be a difficult, confusing and stressful time and the Service experience Desk is there to offer advice, help and support. During the period April 2013 to March 2014, we received a total of 111 formal complaints, 192 concerns and 256 compliments. SED handled 706 new cases, which involved around 8,600 contacts. 617 of cases are attributable to Service Lines. The remaining 89 are attributable to corporate functions, trust generic or non-specific. This includes complaints, concerns, compliments, suggestions and requests for information. This feedback comes from service users, carers or their representatives and from other organisations such as commissioners or MPs. Figure 2 SED Activity by Type Case type Number Compliments 256 Informal concerns 192 Informal enquiries 120 Formal complaints 111 Suggestions 3 Table 2 above shows SED activity type for the Trust. The Trust is structured into five operational service lines as shown in figure 3: Acute, Community, Early Intervention, Older Adults and Recovery. The service line portfolios are shown below. SED activity is proportionate to the size of the service and the nature of the service users in those services, for example, the Trust finds that older adults and young people are less likely to complain than working age adults.

 Children & Adolescent Mental Health Eating Disorders Early Intervention in Psychosis Wards Day Services Community")
182 The Trust reports SED activity by Service Line and this is scrutinised at the quarterly performance Reviews alongside all other performance data. The Service Lines are shown below. Figure 3 Service Line Portfolios Service Lines Acute Services Community Services Early Intervention Services Older Adults Recovery Services Wards Crisis Resolution Home Treatment Psychiatric Liaison Electro Convulsive Therapy Medical Records Outpatients Community Recovery Service Teams (CRS) Assertive Outreach Psychology Transfer and Transition Team (TTT) Criminal Justice/Offender Liaison Primary Care Mental Health Improving Access to Psychological Therapies (Dudley) Children & Adolescent Mental Health Eating Disorders Early Intervention in Psychosis Wards Day Services Community Mental Health Teams Memory Service Outpatients Early Access service (EAS) Rehabilitation Inpatients (Walsall) Vocational services Carers service Substance Misuse Day Services Deaf Child and Family Mental Health Figure 4 SED Feedback Received 2013/14 The chart above shows the number of complaints, concerns and compliments received by quarter during the year 2013/14 for the five service lines. There are of course greater levels of feedback for our two largest service lines Acute and Early Intervention. Conversely, we received very little negative feedback about our Older Adult service line. The number of complaints received is relatively small compared to the number of patients we see and treat each year.


183 Figure 5 SED activity by type 250 of the 256 compliments received were for the care and treatment provided by our staff 3.1 Celebrating Positive Feedback Compliments are the largest category, with attitude of staff as the highest cause group within that. Over the last twelve months we are pleased to say we have also received 256 written compliments from people who have accessed our services, highlighting cases where the quality of our services has been recognised and appreciated. Care and treatment provided by staff Quality of food Information provided by services Aids/appliances/equipment/premises The Service Experience Desk (SED) shares this feedback with staff through our feature, On a Happy Note which highlights the positive comments made by service users about their care by posting a selection of experiences from service users on the Trust Intranet every month. Some examples of what people have said about our services are shown below.
184 Figure 6 Examples of compliments received by the Trust My recent experiences of the Walsall Community Psychiatric Team, has been first class. Thank you would not be enough to say how much you have helped me. Bringing me from a place where nothing or nobody mattered. Today I know what matters, it s life and what you make of it. I respect you for not giving up on me, and because of your support and care I have got my life back and my son has got his mummy back. God bless everyone that has helped. I have been very grateful to my CPN for all of her help over the last 12 months. She has assisted me to regain my confidence and feel considerably better. She is a great asset to your organisation. My wife has been admitted to Hospital and has been there now for 3 weeks due to a mental break down. I cannot thank the staff enough for all their caring. The dedication and care that they provide is second to none. The friendly atmosphere of all who work there, there is always a smile for the Carer's who visit. I wanted to say thank you for always having a smile, for remembering my name, for your time, patience and understanding. Little kindness that makes so much difference. Bloxwich Hospital should be used as a base for other hospitals to take note of how they truly work as a team from cleaners to doctors their activity staff are second to none and held in high regards by the patients. They truly do put the patients first. They need to be recognised for all of the work they do. Thank you so much for all your help. God bless you because your thoughtfulness and all the kindness that you show will always be remembered and appreciated. Thank you, may you always stay this way helping those who have lost their way. I wanted to say thank you for the support you have given me over the past few months. I now feel that I have a variety of strategies to help manage the stresses in my life. You also helped me to realise that parts of my life need to change which gave me a push to do something about it! I'm now looking forward to a brighter, less stressful future. Thank you for helping me get well. Without your help I would not be here today. I have nothing but admiration for the staff at this hospital. The whole team of nurses and doctors looked after my every need and nothing was too much trouble for any of the staff. In fact all the staff deserve medals for all that they have to endure during a working day. I have the utmost respect for everyone here who have aided my recovery over the past nine weeks. I hope that I will now continue the progress that I have made at home as I am being discharged today.
185 3.2 Complaints Management Despite our focus on quality, we recognise that sometimes people s experience of our services is not as positive as we would hope. In October 2007, the Health Service Ombudsman published Principles for Remedy as an overall good practice guide for public bodies in dealing with complaints. Our complaints policy is based around these principles which are: 1 Getting it right 2 Being customer focused 3 Being open and accountable 4 Acting fairly and proportionately 5 Putting things right 6 Seeking continuous improvement Number of Formal Complaints Received In 2013/14, the Trust received 111 formal complaints which were attributable to the five service lines. This is shown in the chart below along with the number of informal concerns and cases referred to the ombudsman. Figure /14 Complaints and Concerns Summary Informal Concerns Formal Complaints PHSO 2013/ / /14 Acute Community Early Intervention Recovery Older Adults Total Of the 111 cases in 2013/14, 59% were responded to within the timescales stipulated in our policy (45 working days) Complaints referred to the Parliamentary and Health Service Ombudsman (PHSO) The points below summarise the cases referred to the ombudsman, it should be noted that none of the notifications were from complaints received during 2013/14: 1 Notification was received from the Ombudsman during this reporting period in relation to a formal complaint that was received during 2012/13. 1 further case remains on-going with the Ombudsman, originally notified prior to this reporting period (March 13) in relation to a complaint received during July 2012.
186 3.2.3 Nature of Complaints and Concerns Received The charts below show the primary category of the complaints and concerns received by the Trust in 2013/14. Care and treatment, like within most Trusts is the highest category for formal complaints with attitude of staff the next highest. Care and treatment has been drilled down as shown in figure 9. Figure 8 Figure 9
187 The chart below shows both primary and secondary categories of complaints and concerns, received by the Trust in 2013/14. Primary category refers to the main concern raised and secondary categories include any additional concerns. The top 3 categories are care and treatment, staff attitude and communication (closely followed by appointments). Figure Outcome of Complaints Of the cases closed, 67% of complaints were upheld or partially upheld. The decision to uphold a case or not is made following a full investigation that involves the scrutiny of notes and records, interviews with staff and service users as appropriate. The table below summarises this. Figure 11 Outcome of Closed Complaints Number Not upheld 28 Upheld 12 *Partially Upheld 44 Withdrawn 3 Closed due to no response 12 *Out of time 1 On-going 11 TOTAL 111 *Partially upheld outcomes are counted as upheld for KO41 reporting purposes. *Out of time this complaint was dismissed due to the concerns being raised dating back 10 years (complaints regulations stipulate complaints have to be made within 12 months although there are exceptions to this rule).
188 3.4 Learning from Feedback The Trust takes an active approach to resolving concerns before they escalate to formal complaints. We also provide feedback to staff about what changes have been made as a result of complaints and concerns. We receive essential and valuable feedback through the function of our Service Experience Desk. Service users, carers, staff and others contact the service experience desk for advice, support and to report concerns and complaints directly to us. Over the past twelve months our 5 Expert By Experience service users (EBE s) have been directly and significantly involved in raising awareness of Trust activities as well as gaining valuable feedback from service users and carers. We have recruited a further seven Experts by Experience (EBEs), in recognition of the increased demand for the work. The team of 12 EBE s will be aligned to special areas of interest, with each EBE bringing different skills and experience to the role. Each of our EBE s has considerable knowledge and experience of using Trust services. Here are just a few of the selected actions that have been carried out as a result of feedback from those who use our services, their relatives and carers. Figure 12 Comments and Actions Taken You Said You wanted to be have a way to have your say and to ask questions about mental health It can be difficult or confusing to get help if you experience a mental health crisis You were given lots of information which could get lost My carers and I feel that we don t always experience the highest level of customer care You would like your Care Coordinator to know about other appointments within the Trust as you don t always remember to tell them Our GPs were not always clear on how to refer patients to our services You would like more information and advice about finding work, benefits and housing We Did We set up a Mental Health Forum that meets quarterly to listen and to share information and knowledge. The forum brings together, service users and carers, trust members, other statutory bodies and third sectors and community groups with an interest in mental health issues We also recruited a number of Experts by Experience who visit services to listen to you and raise your views with us We produced a crisis card for you to keep, that contains information to help you and others if you experience a mental health crisis We produced My Care Pack a folder for you to keep all the information you need about your care We organised our staff to take part in special training to help ensure that we deliver the best possible care across the Trust We changed our processes so that information about other appointments are copied to Care Coordinators We have reduced the number of ways in which people can be referred to us so that it is now much simpler. We have also produced new GP packs with clear information on how to refer patients to our various services Our Employment Services teams can support you with these issues. We have distributed leaflets and posters to raise awareness about how to be referred to them. The team gave a
189 You Said Support for families and carers could be more readily available More information about medication would be helpful Some of our sites are ageing and no longer fit for purpose The pathway from a mental health hospital to an acute hospital was unclear and distressing The outside areas were not always clean and tidy Awareness and access to the Quiet Garden at Dorothy Pattison Hospital was limited It was difficult to find the Outpatients department at Dorothy Pattison Hospital You didn t know where and how to find information about facilities and resources whilst in hospital It can be distressing if there are delays to receiving medication before going on leave Some bathrooms and consulting rooms didn t provide enough privacy It is not always easy to find refreshments out of normal working hours The experience you have in A&E, especially out of hours, can sometimes be unpleasant and distressing We Did presentation to service users and carers at the Mental Health Forum. We have distributed leaflets and posters explaining how you can get support as a Carer. We have also launched our Triangle of Care that will improve how our staff work with service users and carers We subscribed to the web resource, Choice in Medication where you can find everything you need to know about the most common medicines used in mental health. The Pharmacy team gave a presentation to service users and carers at the Mental Health Forum. We have reviewed all of our sites and have made some big changes, moved services to new or different premises where the environment is better for both service users and staff We have improved communication between Trust staff and hospital staff to ensure a smooth transition for patients We have amended our cleaning contract to include deep cleaning to some outside areas We put posters up to let you know when you can access the garden and introduced it as part of the ward activity schedule We have provided additional signage to show clearly where the outpatients department is located We are working with our Experts By Experience to refresh our hospital welcome packs to ensure they contain all the information you and your carer need We have reminded all staff to allow at least 4 hours notice when requesting medication for leave from the pharmacy at Russell s Hall We have ensured that all bathrooms now have shower curtains and the consulting room doors have obscure glass panels We are going to be providing additional vending machines and are also considering a mobile shop at Bushey Fields We have already put in place a Psychiatric Liaison service for out of hours care and we are looking into extending this to ensure that you are seen quickly and in a more therapeutic environment

190 4 Service Experience - the full picture As well as gathering feedback about our services through SED, the Trust also has a Service Experience facilitator who co-ordinates, collates and reports on other forms of service experience feedback, for example: Figure 13 Sources of Service Experience Feedback The findings of this work are triangulated with SED activity and fed into our reporting mechanisms and embedding lessons process described in section 3.2.
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016 1.00pm-3.45pm Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS PUBLIC MEETING
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016 1.00pm-3.45pm Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS PUBLIC MEETING
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017 1.00pm-3.00pm Conference Room 1, Trafalgar House, King Street, Dudley PUBLIC MEETING
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017 1.00pm-3.00pm Conference Room 1, Trafalgar House, King Street, Dudley PUBLIC MEETING
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Dudley & Walsall Mental Health Partnership NHS Trust Board
 Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
NHS East and North Hertfordshire Clinical Commissioning Group. Quality Committee. Terms of Reference Version 4.0
 NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
HERTFORDSHIRE COMMUNITY HEALTH SERVICES
 HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
Board of Directors. Approval Discussion Information Assurance
 Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Safeguarding Annual Assurance Self-assessment Tool. Sheffield Health and Social Care NHS Foundation Trust
 Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Service Guide. together. Your guide to: for Walsall GPs. Services provided Referral pathways How to contact services
 Service Guide for Walsall GPs Your guide to: Services provided Referral pathways How to contact services together Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced
Service Guide for Walsall GPs Your guide to: Services provided Referral pathways How to contact services together Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced
Special Measures Action Plan. Norfolk and Suffolk NHS Foundation Trust
 Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
How CQC monitors, inspects and regulates independent doctors and clinics providing primary care
 How CQC monitors, inspects and regulates independent doctors and clinics providing primary care October 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor independent doctors and clinics
How CQC monitors, inspects and regulates independent doctors and clinics providing primary care October 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor independent doctors and clinics
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Present: Mr B Reid OBE Chair of the Board of Directors Mr N Summers CBE Vice Chair of the Board of Directors. Mr G McEvoy Non-executive Director
 ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Sustainable & Accessible Services. Strong Partnerships X X X
 SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
BOARD PAPER - NHS ENGLAND. Title: Board Assurance Framework (incorporating the organisation s strategic risks)
") Paper NHSE121312 BOARD PAPER - NHS ENGLAND Title: Board Assurance Framework (incorporating the organisation s strategic risks) Clearance: National Director, : Bill McCarthy Purpose of paper: To update
Paper NHSE121312 BOARD PAPER - NHS ENGLAND Title: Board Assurance Framework (incorporating the organisation s strategic risks) Clearance: National Director, : Bill McCarthy Purpose of paper: To update
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC
 Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Safeguarding review to assist Walsall Healthcare NHS Trust
 [Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
[Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
Quality and Safety Strategy
 Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
TRUST BOARD 27 OCTOBER 2011 QUARTERLY CUSTOMER CARE REPORT
 TRUST BOARD 27 OCTOBER 2011 QUARTERLY CUSTOMER CARE REPORT D Summary The Trust Board at its 28 July 2011 meeting (minute TB/11/192) approved a quarterly high level customer care report be developed for
TRUST BOARD 27 OCTOBER 2011 QUARTERLY CUSTOMER CARE REPORT D Summary The Trust Board at its 28 July 2011 meeting (minute TB/11/192) approved a quarterly high level customer care report be developed for
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE
 POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Quality and Safety Committee Terms of Reference
 Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Action required: To agree the process by which Governors will meet with the inspection team.
 Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Quality and Governance Committee. Terms of Reference
 Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
Service Guide. Your guide to: for Dudley GPs. Services provided Referral pathways How to contact services
 Service Guide for Dudley GPs Your guide to: Services provided Referral pathways How to contact services Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced to help
Service Guide for Dudley GPs Your guide to: Services provided Referral pathways How to contact services Foreword Dear Colleague, Welcome to our first ever GP Service Guide, which we have produced to help
The state of health care and adult social care in England 2015/16 Care Quality Commission 13 October 2016
 The state of health care and adult social care in England 2015/16 Care Quality Commission 13 October 2016 The annual State of Care report, out today (Thursday 13 October) reports excellent examples of
The state of health care and adult social care in England 2015/16 Care Quality Commission 13 October 2016 The annual State of Care report, out today (Thursday 13 October) reports excellent examples of
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference
 CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as the Committee in
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as the Committee in
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 25th July 2016 Title: Executive Summary: Action Requested: Author: Contact Details: Resource Implications: Equality and Diversity Assessment
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 25th July 2016 Title: Executive Summary: Action Requested: Author: Contact Details: Resource Implications: Equality and Diversity Assessment
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Service Transformation Report. Resource and Performance
 SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
Delivering the transformation of children and young people s mental health services
 Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of
 An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of homicide by Sussex Partnership NHS Foundation Trust: Extended
An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of homicide by Sussex Partnership NHS Foundation Trust: Extended
DUDLEY CLINICAL COMMISSIONING GROUP BOARD
 DUDLEY CLINICAL COMMISSIONING GROUP BOARD Date of Board: 14 July 2016 Report: Sustainability and Transformation Plan (STP) Agenda item No: 7.3 TITLE OF REPORT: PURPOSE OF REPORT: AUTHOR OF REPORT: MANAGEMENT
DUDLEY CLINICAL COMMISSIONING GROUP BOARD Date of Board: 14 July 2016 Report: Sustainability and Transformation Plan (STP) Agenda item No: 7.3 TITLE OF REPORT: PURPOSE OF REPORT: AUTHOR OF REPORT: MANAGEMENT
CLINICAL GOVERNANCE AND QUALITY COMMITTEE. Final - Terms of Reference - Final
 CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
Adults and Safeguarding Committee 19 March Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy.
 Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP. Corporate Parenting Board. Date of Meeting: 23 rd Feb Agenda item: ( 7 )
") WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
PGB Joint Commissioning Board Minutes
 PGB-14-69 Joint Commissioning Board Minutes PGB-14-69 Governing Body Meeting in Public 17 June 2014 1 of 6 JOINT COMMISSIONING BOARD MINUTES Kinetic, Francis Crick House, Moulton Park, Northampton, NN3
PGB-14-69 Joint Commissioning Board Minutes PGB-14-69 Governing Body Meeting in Public 17 June 2014 1 of 6 JOINT COMMISSIONING BOARD MINUTES Kinetic, Francis Crick House, Moulton Park, Northampton, NN3
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
Debbie Edwards Interim Deputy Director of Nursing Gail Naylor- Executive Director of Nursing & Midwifery. Safety & Quality Committee
 Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement
 Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs
 Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
WOLVERHAMPTON CCG. Governing Body Meeting 9 th September 2014
 WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
Learning from Deaths - Mortality Report
 Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Review of Terms of Reference of Quality Assurance Committee
 Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
 Cornwall and Isles of Scilly draft pending formal approval master 301015 Source documents: http://www.cornwall.gov.uk/health-and-social-care/cornwall-and-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/about-cornwalland-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/?alttemplate=_standard
Cornwall and Isles of Scilly draft pending formal approval master 301015 Source documents: http://www.cornwall.gov.uk/health-and-social-care/cornwall-and-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/about-cornwalland-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/?alttemplate=_standard
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that