Presentation Objectives
|
|
|
- Jasper Barnett
- 6 years ago
- Views:
Transcription
1 At Home: Comprehensive Care of the Frail Elderly Ramiro Jervis, MD Asantewaa Poku, MPH Kristofer Smith, MD, MPP December 10, Presentation Objectives Develop, both culturally and operationally, an ondemand clinical model to respond to changes in clinical status. Utilize real-time analytics to coordinate care and identify patients in need of higher-intensity services. Leverage community paramedicine to assist with patient evaluation and triage during off-hours. Discuss the future use of advanced illness programs to manage the transition from volume to value 2 1
 Feinstein Institute for Medical Research Center for Innovation and Learning, and Patient Safety Institute NSLIJ Hofstra School of Medicine Care management")
2 3 3 At a Glance: North Shore-LIJ Health System NSLIJ Health System NSLIJ Care Solutions NSLIJ CareConnect 16 hospitals 3 SNFs 400 ambulatory physician practices Emergency Medical Services Home Care Agency Hospice Care Network (affiliated) Feinstein Institute for Medical Research Center for Innovation and Learning, and Patient Safety Institute NSLIJ Hofstra School of Medicine Care management Organization Helping NSLIJ make the switch from the illness business to the health business New entity to coordinate the resources within the Health System as we take on risk as an insurance company Focus on population management programs, such as Advanced Illness Management President Alan Murray First provider-owned plan in New York Insurance license approved July 2013 Enrolling individuals, families, and small and large business on Long Island, Queens, Staten Island, and Manhattan Available on the New York Health Benefit Exchange Emphasis on customer service and patient experience 4 2

3 Clinical Scenario 5 Clinical Imperative 6 3
 account for 50% of total costs Tier 3 Tier 3A Patients: This is who we need to target!")
4 The Clinical Imperative Care Current Source: Advanced Illness Management Strategies, Part 1, American Hospital Association, August The Financial Imperative Multiple hospitalizations, overtreatment, and care transition add up 5% (Tier 3 A) account for 50% of total costs Tier 3 Tier 3A Patients: This is who we need to target! Source: Conwell LJ, Cohen JW. Characteristics of people with high medical expenses in the U.S. civilian non-institutionalized population, Statistical Brief #73. March Agency for Healthcare Research and Quality, Rockville, MD. 8 4
5 Clinical + Financial Imperative = Opportunity CHRONIC DISEASE Case Management Medical Homes 2-20 Years Program Gap HOSPICE < 6 9 Advanced Illness Program North Shore-LIJ House Calls, Advanced Illness Management s foundational program, provides care to frail elderly patients with multiple chronic illnesses and functional impairments. Over 900 patients across Queens, Nassau and Suffolk Care team: 7 medical doctors, 3 nurse practitioners, 2 social workers, 4 medical coordinators and administrative leadership 10 5

6 Clinical Team Clinicians Establish relationship with new patients Evaluation visit and 2-week follow-up visit Regular visits at clinically appropriate intervals Urgent same- and next-day visits 24/7 telephonic response: Rotate on call coverage every night and weekend Rotate NP on call coverage in the office M-F, 9-4:30PM Remote access to EMR at all hours Social workers assist with psychosocial complexities 11 Support Team Administrative Support Intake Nurse Manages referrals and intake paperwork Medical Coordinators: Schedule appointments and optimize providers calendar Answer phone calls from patients/families and attend to administrative patient needs Transfer clinical questions to providers Biller: Answers billing questions and optimizes revenue capture 12 6


7 Patient Eligibility Homebound Prioritize referrals for patients by severity of medical necessity: Referrals from hospital or hospice Uncontrolled symptoms No relationship with a primary care provider 13 Advanced Illness Patients Demographics: Average Age: 85 yrs Gender: Female: 72.4% Male: 27.6% 65% ADL Dependency 10% 12% 13% 0 ADLs 1-2 ADLs 3-4 ADLs 5-6 ADLs Top 10 HCC Dx Condition House Calls Pts Categories (Census 11/ 2012 Dt) Diabetes 25% Protein-Calorie Malnutrition 24% Decubitus Ulcer of Skin 24% Congestive Heart Failure 17% Specified Heart Arrhythmias 17% Chronic Obstructive Pulmonary Disease 14% Renal Failure 12% Ischemic or Unspecified Stroke 12% Vascular Disease 9% Parkinson's and Huntington's Diseases 9% 14 7
8 Independence at Home Created by Affordable Care Act as part of CMMI Shared savings model Rewards based on quality and utilization Home-based primary care teams directed by physicians and nurse practitioners 15 Independence at Home Follow-up within 48 hours after hospital admission, hospital discharge, and ED visits In-home medication reconciliation within 48 hours of hospital discharge and ED visits Annual documentation of patient preferences All-cause hospital readmissions within 30 days Hospital admission rate for ambulatory care sensitive conditions ED visit rate for ambulatory care sensitive conditions 16 8
9 Independence at Home Follow-up within 48 hours after hospital admission, hospital discharge, and ED visits In-home medication reconciliation within 48 hours of hospital discharge and ED visits Annual documentation of patient preferences All-cause hospital readmissions within 30 days Hospital admission rate for ambulatory care sensitive conditions ED visit rate for ambulatory care sensitive conditions 17 Care Team Engagement Twice weekly meetings discussing significant patient events Reinforcement of shared vision and values Emphasis on return of calls same day Emphasis of reorganizing patient schedules to accommodate patient with urgent needs 18 9
10 Patient engagement Education of our on demand model Expectations that we will contact them or be contacted if they are admitted to hospital or ED 19 Clinician engagement Structured intake process with patients MOLST and health care proxy discussed at first meeting with patient Individual consent forms done by providers with patients or their health care proxies Emphasis on shared decision making from day



11 MOLST Medical orders for Life Sustaining Treatment CPR or allow natural death Treatment guidelines Mechanical ventilation Feeding tube IV fluids Antibiotics Keep at home or hospitalize 21 Community Paramedicine 22 11
12 Community Paramedicine Q integration of call center with EMS Calls from patients to our office are answered by EMS dispatch House Calls Providers credentialed as On Line Medical Control (OLMC) physicians Can provide medical orders to paramedics, and orders to treat, orders to leave the patient home Paramedics provided Geriatric Training to address the needs of the frail elderly Sensitive to patient wishes and MOLST 23 Community Paramedic Pilot Hipaa compliant video teleconference 24 12

13 Community Paramedic Pilot Initial results 21 calls Only 1/3 rd transported to the ED Average response time 25 minutes Average total time on scene 63 minutes 25 Community Paramedic Pilot Select Cases Hypertensive urgency BP 214/ 130 Improved with IV labetolol Change in mental status Symptomatic hypoglycemia Improved with IV dextrose Shortness of breath Improved with albuterol nebulizer 26 13
14 Results Care coordination Advanced Care planning LOS Admission Rate Deaths at home Patient satisfaction 27 Care Coordination Post-Admission Contact % 8679% 88% 85% 42 45% Q Q Q Q Q % 140% 120% 100% 80% 60% 40% 20% 0% Post- Discharge Med Rec Hospital Admissions Post Admissin Contact Percentage Met 28 14
15 Resuscitation Instructions Intubation & Mechanical Ventilation Treatment Guidelines Hospitalization Artificial Nutrition Antibiotics 12/10/2013 Care Coordination Post-Discharge Medication Reconciliation % 94% 81% 86% 55 63% Q Q Q Q Q % 120% 100% 80% 60% 40% 20% 0% Post- Discharge Med Rec Hospital and ED Discharges Home Percentage Met Post-Discharge Med Rec Within 48 Hrs 29 Advance Care Planning MOLST Questions Answered, Q Percentage without question answered Percentage with question answered 14% 86% 54% 54% 46% 51% 50% 46% 46% 54% 49% 50% 30 15
16 Hospital Admissions Pre- Post Hospital Admissions* 23.02% House Calls SOC 9.59% 12.95% 9.83% 13.05% 11.97% 5.33% 3.37% pre soc 7-9 pre soc 4-6 pre soc 1-3 pre soc 1-3 post soc 4-6 post soc 7-9 post soc post soc A 37% reduction in hospital admissions after coming on to the program Subset of 140 sickest patients new to program in the last year 31 Outcomes: Hospital LOS Hospital Length of Stay Hospital Admissions LOS Q Q Q Q Admissions Avg LOS (Days) Avg LOS Reduction (0.42) Excess Days Reduction (60)
17 Hospital Discharge Disposition Discharge Disposition Discharges Home Discharges to Rehab Other Discharges 6% 12% 12% 9% 14% 27% 29% 16% 36% 26% 67% 59% 71% 55% 60% Q3 2012, N=86 Q4 2012, N=118 Q1 2013, N=105 Q2 2013, N=130 Q3 2013, N= Place of Patient Death 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Patient Deaths Home Hospital Inpatient Hospice Rehab Unsure 0% 5% 7% 3% 3% 0% 1% 15% 8% 12% 2% 7% 18% 19% 28% 22% 54% 70% 67% 59% Q Q Q Q

18 Sicker Patients HCC Scores >= 3 8% 18% 23% 27% 40% 37% 28% 19% Q1 2013, N= 819 Q3 2013, N=
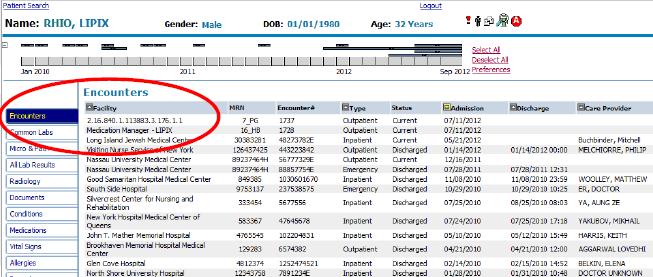
19 Leveraging Informatics to Achieve High Reliability Challenges Care Coordination Advanced Care Planning Solutions Real time notifications Provider dashboards 37 Care Coordination: Decreasing the Unknown AIM patients admitted to 21 different hospitals in 2012 Understanding the unknown Patient and provider engagement July 2012 Internal ADT Report - October 2012 Healthix Notifications- December 2012 Q % Q % Q % Q % Q % Decrease in Unknown Admissions 38 19
20 Internal ADT Alerts Real-time alerts received hourly via Includes data from 9 NSLIJ hospitals Admission, discharge and transfer data 39 External RHIO Alerts Healthix largest RHIO for NYC and Long Island Receives data feeds from 48 hospitals, 18 SNFs, provider groups and home care agencies Receives real-time registration events for ER visits and hospitalizations Able to push real time notifications to end users Requires patient consent for care coordination activies 40 20
21 Healthix notifications 41 Care Coordination 42 21
22 Care Coordination 43 Health IT Changes Old System McKesson POC EHR New System Allscripts EHR Details Advantages: e- prescribing, lab integration, reportable data fields Challenges: connectivity, new workflows, data extraction 44 22
23 Leveraging the AEHR What defines a House Calls patient in the AEHR Enrollment Order Allows us to define active patient census Differentiate our patients within the EHR 45 Leveraging the AEHR Creation of specific orders based on metrics Develop analytics reports to extract data Less manual chart review Create dashboards as a management tool 46 23
24 Care Team Engagement Share group metrics Share individual metrics 47 Advanced Illness: Taking Advantage of the Chasm 48 24
25 Reimbursement Model 12/10/2013 Payment Models Here and on the Horizon Global Market Risk Model Shared Risk Model Upside Incentive Payment Model Episode of Illness Payment Bundled Services Payment 2020 $28 Billion Fee For Services Payment 2012 $6.5 Billion Current Delivery System NSLIJ High Performance System Clinical + Financial Imperative = Opportunity CHRONIC DISEASE Case Management Medical Homes 2-20 Years Program Gap HOSPICE <
26 What is your product? What does your product cost? Insurance Company What are their biggest risks? Who is your audience? Health System/Hospital How do they make money today? What are their benefit obligations? How could they make money tomorrow? 51 What are their benefit obligations? How could they make money tomorrow? How can you help reduce their risk/meet obligations? What existing programs align with your goals? What revenue or quality opportunity does your product solve? Have they partnered with other programs already? How did it go? Who are your potential allies? Who are your potential allies? Make your pitch Make your pitch 52 26
27 Health System Case Study 53 What is your product Advanced Illness Management Complex medical management for patients with multiple chronic illnesses and functional impairment Palliative care focus High quality care transitions Admission abatement Death at home 54 27
28 Care Coordination Post-Discharge Medication Reconciliation % 94% 81% 86% 55 63% Q Q Q Q Q % 120% 100% 80% 60% 40% 20% 0% Post- Discharge Med Rec Hospital and ED Discharges Home Percentage Met Post-Discharge Med Rec Within 48 Hrs 55 Hospital Admissions Pre- Post Hospital Admissions* 23.02% House Calls SOC 9.59% 12.95% 9.83% 13.05% 11.97% 5.33% 3.37% pre soc 7-9 pre soc 4-6 pre soc 1-3 pre soc 1-3 post soc 4-6 post soc 7-9 post soc post soc A 37% reduction in hospital admissions after coming on to the program Subset of 140 sickest patients new to program in the last year 56 28
29 Place of Patient Death 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Patient Deaths Home Hospital Inpatient Hospice Rehab Unsure 0% 5% 7% 3% 3% 0% 1% 15% 8% 12% 2% 7% 18% 19% 28% 22% 54% 70% 67% 59% Q Q Q Q What does your product cost? Fixed costs Variable costs Step variable costs PMPM rate 58 29
30 Who is your audience? Health System Hospital 59 How do they make money today? Fee for Service Quality Pay for performance Full Risk Shared Risk 60 30
31 How Could They Make Money Tomorrow? Quality Pay for performance Shared Risk Full Risk Fee for service 61 What quality or revenue opportunity does your product solve? Revenue Full or partial risk P4P Hedis/Star ratings Quality Mortality Readmissions Efficiency 62 31
32 Have they partnered with other organizations? How did it go? Third party vendors Other clinical groups Other health systems 63 Who are your potential allies? Senior leadership Contracting Quality Finance Post acute services 64 32
33 Make your pitch Who is in the audience? Stay flexible Don t overpromise 65 Leveraging Informatics to Achieve High Reliability Challenges Care Coordination High risk alerts Advanced Care Planning Solutions Real time notifications Provider dashboards 66 33


34 Care Coordination: Decreasing the Unknown AIM patients admitted to 21 different hospitals in 2012 Understanding the unknown Patient and provider engagement July 2012 Internal ADT Report - October 2012 Healthix Notifications- December 2012 Q % Q % Q % Q % Q % Decrease in Unknown Admissions 67 Internal ADT Alerts Real-time alerts received hourly via Includes data from 9 NSLIJ hospitals Admission, discharge and transfer data 68 34



35 External RHIO Alerts Healthix largest RHIO for NYC and Long Island Receives data feeds from 48 hospitals, 18 SNFs, numerous provider groups and 3 home care agencies Receives real-time registration events for ER visits, hospitalizations and discharges Able to push real time notifications to end users Requires patient consent for care coordination activities 69 Healthix notifications 70 35

36 Care Coordination 71 Care Coordination 72 36

37 Health IT Changes Old System McKesson POC EHR New System Allscripts EHR Details Advantages: e- prescribing, lab integration, reportable data fields Challenges: connectivity, new workflows, data extraction 73 Leveraging the AEHR What defines an AIM patient in the AEHR Enrollment Order Allows us to label active patients 74 37



38 Leveraging the AEHR Creation of specific orders based on metrics Develop analytics reports to extract data Less manual chart review Create dashboards as a management tool 75 Care Team Engagement Share group metrics Share individual metrics 76 38

39 Reimbursement Model 12/10/2013 Advanced Illness: Taking Advantage of the Chasm 77 Payment Models Here and on the Horizon Global Market Risk Model Shared Risk Model Upside Incentive Payment Model Episode of Illness Payment Bundled Services Payment 2020 $28 Billion Fee For Services Payment 2012 $6.5 Billion Current Delivery System NSLIJ High Performance System

40 Clinical + Financial Imperative = Opportunity CHRONIC DISEASE Case Management Medical Homes 2-20 Years Program Gap HOSPICE < What is your product? What does your product cost? Insurance Company What are their biggest risks? Who is your audience? Health System/Hospital How do they make money today? What are their benefit obligations? How could they make money tomorrow? 80 40
41 What are their benefit obligations? How could they make money tomorrow? How can you help reduce their risk/meet obligations? What existing programs align with your goals? What revenue or quality opportunity does your product solve? Have they partnered with other programs already? How did it go? Who are your potential allies? Who are your potential allies? Make your pitch Make your pitch 81 Health System Case Study What is your product? 82 41
42 Care Coordination Post-Discharge Medication Reconciliation % 94% 81% 86% 55 63% Q Q Q Q Q % 120% 100% 80% 60% 40% 20% 0% Post- Discharge Med Rec Hospital and ED Discharges Home Percentage Met Post-Discharge Med Rec Within 48 Hrs 83 Hospital Admissions Pre- Post Hospital Admissions* 23.02% House Calls SOC 9.59% 12.95% 9.83% 13.05% 11.97% 5.33% 3.37% pre soc 7-9 pre soc 4-6 pre soc 1-3 pre soc 1-3 post soc 4-6 post soc 7-9 post soc post soc A 37% reduction in hospital admissions after coming on to the program Subset of 140 sickest patients new to program in the last year 84 42
43 Place of Patient Death 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Patient Deaths Home Hospital Inpatient Hospice Rehab Unsure 0% 5% 7% 3% 3% 0% 1% 15% 8% 12% 2% 7% 18% 19% 28% 22% 54% 70% 67% 59% Q Q Q Q What does your product cost? Fixed costs Variable costs Step variable costs PMPM rate 86 43
44 Who is your audience? Health System Hospital 87 How do they make money today? Fee for Service Quality Pay for performance Full Risk Shared Risk 88 44
45 How Could They Make Money Tomorrow? Quality Pay for performance Shared Risk Full Risk Fee for service 89 What quality or revenue opportunity does your product solve? Revenue Full or partial risk P4P Hedis/Star ratings Quality Mortality Readmissions Efficiency 90 45
46 Have they partnered with other organizations? How did it go? Third party vendors Other clinical groups Other health systems 91 Who are your potential allies? Senior leadership Contracting Quality Finance Post acute services 92 46
47 Make your pitch Who is in the audience? Stay flexible Don t overpromise 93 47
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Deriving Value from a Health Information Exchange. HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017
 Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
ENGAGING PHYSICIANS FOR IMPROVED OUTCOMES: CLINICAL DOCUMENTATION, FINANCIAL & PATIENT CARE
 ENGAGING PHYSICIANS FOR IMPROVED OUTCOMES: CLINICAL DOCUMENTATION, FINANCIAL & PATIENT CARE Northeast Ohio HFMA GHALI May 20, 2016 James Begley, MD, MS Physician Champion, ICD-10 & Medical Records Committee
ENGAGING PHYSICIANS FOR IMPROVED OUTCOMES: CLINICAL DOCUMENTATION, FINANCIAL & PATIENT CARE Northeast Ohio HFMA GHALI May 20, 2016 James Begley, MD, MS Physician Champion, ICD-10 & Medical Records Committee
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Staff Training. Understanding Healthix Patient Consent
 Staff Training Understanding Healthix Patient Consent Healthix Facilitates Exchange of Data Healthix Policy and Patient Consent Work Responsibilities: Training, Documenting and Preparing for Audit 1. Let
Staff Training Understanding Healthix Patient Consent Healthix Facilitates Exchange of Data Healthix Policy and Patient Consent Work Responsibilities: Training, Documenting and Preparing for Audit 1. Let
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
COLLABORATING FOR VALUE. A Winning Strategy for Health Plans and Providers in a Shared Risk Environment
 COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait
 Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Explaining the Value to Payers
 Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Explaining the Value to Payers Explaining the Value to Payers This document has been created to provide talking points for EMS agencies to explain to payers the value of EMS 3.0 services. Please review
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
UPDATE ON MEANINGFUL USE. HITECH Stimulus Act of 2009: CSC Point of View
 HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Panel Discussion: Home-Based Primary Care Led Population Management
 Panel Discussion: Home-Based Primary Care Led Population Management Moderator: Steven Merhan, MD Panelists: Barbara Sutton, MSN APRN ACHPN Terri Hobbs Christopher Day, MPH MBA Faculty Disclosures Day Kindred
Panel Discussion: Home-Based Primary Care Led Population Management Moderator: Steven Merhan, MD Panelists: Barbara Sutton, MSN APRN ACHPN Terri Hobbs Christopher Day, MPH MBA Faculty Disclosures Day Kindred
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Brave New World: The Effects of Health Reform Legislation on Hospitals. HFMA Annual National Meeting, Las Vegas, Nevada
 Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
The Park at Allens Creek Suite Allens Creek Road Rochester, NY 14618
 The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
Medical Management Program
 Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Medical Group and Hospital A Model for Clinical Integration
 Medical Group and Hospital A Model for Clinical Integration Richard Afable M.D., MPH President and CEO Hoag Memorial Hospital Presbyterian Alan Puzarne Chief Operating Officer Greater Newport Physicians
Medical Group and Hospital A Model for Clinical Integration Richard Afable M.D., MPH President and CEO Hoag Memorial Hospital Presbyterian Alan Puzarne Chief Operating Officer Greater Newport Physicians
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability
 Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability Shahla A. Mehdizadeh, Ph.D. 1 Robert A. Applebaum, Ph.D. 2 Gregg Warshaw, M.D. 3 Jane K. Straker,
Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability Shahla A. Mehdizadeh, Ph.D. 1 Robert A. Applebaum, Ph.D. 2 Gregg Warshaw, M.D. 3 Jane K. Straker,
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Mercy Virtual. Transforming Medicine and Value Through Virtual Care. Randall S Moore, MD, MBA. Orlando, FL. September, 2017
 Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1)
") Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Verdien av egengenerert helsedata. Oslo, Tor Jakob Ramsøy
 Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
HIE Data: Value Proposition for Payers and Providers
 HIE Data: Value Proposition for Payers and Providers Session #21, March 6, 2018 Laura McCrary, Executive Director, KHIN Tara Orear, Senior Ambulatory Systems Analyst, Newman Regional Health Dirk Rittenhouse,
HIE Data: Value Proposition for Payers and Providers Session #21, March 6, 2018 Laura McCrary, Executive Director, KHIN Tara Orear, Senior Ambulatory Systems Analyst, Newman Regional Health Dirk Rittenhouse,
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/28/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/28/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
PRIMARY PARTNERS, LLC. Our Journey with the State HIE
 PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
A Partnership Approach to Getting Your Patient s Status Right
 A Partnership Approach to Getting Your Patient s Status Right Karen Haesloop, RN, FNP, MSN, McBee Debra Schardt, RN, CPUR, MultiCare Health System Copyright 2017 by McBee Associates, Inc. All rights reserved.
A Partnership Approach to Getting Your Patient s Status Right Karen Haesloop, RN, FNP, MSN, McBee Debra Schardt, RN, CPUR, MultiCare Health System Copyright 2017 by McBee Associates, Inc. All rights reserved.
Section 7. Medical Management Program
 Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
HR Telehealth Enhancement Act of 2015
 HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
HIT and HIE at the Visiting Nurse Service of New York. Discussion with CHCANYS Region II Conference. Thomas Check, CIO at VNSNY.
 HIT and HIE at the Visiting Nurse Service of New York Discussion with CHCANYS Region II Conference Thomas Check, CIO at VNSNY July 13, 2009 Table of Contents Topic Slide VNSNY Overview 3 Health Information
HIT and HIE at the Visiting Nurse Service of New York Discussion with CHCANYS Region II Conference Thomas Check, CIO at VNSNY July 13, 2009 Table of Contents Topic Slide VNSNY Overview 3 Health Information
NewYork-Presbyterian/Queens PPS Clinical Integration Strategy
 NewYork-Presbyterian/Queens PPS Clinical Integration Strategy Document Title: NYP/Q PPS Clinical Integration Strategy Version 1.0 Purpose: Approving Committee: This document outlines the needs for a clinically
NewYork-Presbyterian/Queens PPS Clinical Integration Strategy Document Title: NYP/Q PPS Clinical Integration Strategy Version 1.0 Purpose: Approving Committee: This document outlines the needs for a clinically
Welcome to Rochester RHIO s GET DIRECTed! Denise DiNoto Director of Community Services March 2014
 Welcome to Rochester RHIO s GET DIRECTed! Denise DiNoto Director of Community Services March 2014 1 Agenda Introductions What is Direct? Direct Messaging Functionality Incorporating into Workflow RHIO
Welcome to Rochester RHIO s GET DIRECTed! Denise DiNoto Director of Community Services March 2014 1 Agenda Introductions What is Direct? Direct Messaging Functionality Incorporating into Workflow RHIO
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Succeeding in Value-Based Care CareConnect Journey
 Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Patient Engagement in the Population Health Management Era
 Patient Engagement in the Population Health Management Era Creagh Milford, DO, MPH President, Population Health Services A Catholic healthcare ministry serving Ohio and Kentucky Agenda Agenda I. Overview
Patient Engagement in the Population Health Management Era Creagh Milford, DO, MPH President, Population Health Services A Catholic healthcare ministry serving Ohio and Kentucky Agenda Agenda I. Overview
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Referral and Admission Models Explanation of Key Decision Points
 JUNE 2018 Referral and Admission Models Explanation of Key Decision Points This tool is designed to assist a hospice program in evaluating their referral and admission process for efficiency in operation
JUNE 2018 Referral and Admission Models Explanation of Key Decision Points This tool is designed to assist a hospice program in evaluating their referral and admission process for efficiency in operation
Care Management Framework:
 WHITE PAPER Care Management Framework: The Critical Path to Implementing a Care Management Strategy An Encore Point of View Randy Thomas, FHIMSS, Barbara Doyle, MSN, RN, January 2017 Tina Burbine, MBA,
WHITE PAPER Care Management Framework: The Critical Path to Implementing a Care Management Strategy An Encore Point of View Randy Thomas, FHIMSS, Barbara Doyle, MSN, RN, January 2017 Tina Burbine, MBA,
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Population Health Management Tools to Improve Care for Individuals and Populations of Patients
 June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
2017 State of Consumer Telehealth: Insights from Hospital Executives
 2017 State of Consumer Telehealth: Insights from Hospital Executives #BeckersHR18 May 15, 2018 1 Presenter / Agenda 1 About Teladoc 2 Survey Overview 3 Key Findings 4 Success Factors Alan Roga, MD, FACEP
2017 State of Consumer Telehealth: Insights from Hospital Executives #BeckersHR18 May 15, 2018 1 Presenter / Agenda 1 About Teladoc 2 Survey Overview 3 Key Findings 4 Success Factors Alan Roga, MD, FACEP
An Implementation Framework for Patient Safety in Ambulatory Care. To disseminate key findings from IHI s work on ambulatory safety
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care
 Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette