Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
|
|
|
- Paul Sims
- 6 years ago
- Views:
Transcription

1 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH

2

3
4
5

6 Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true Saying there is a meaningful difference between drugs when there is not Type Two Error Accepting the null hypothesis when it is false Saying there is not a meaningful difference between drugs when there is Type Three Error The unintentional error of solving the wrong problems precisely Type Four Error The intentional error of solving the wrong problems
7 Objectives Discuss policy and future trends related to hospital readmissions and their role in value-based purchasing Understand the evidence for and against readmission reduction strategies Describe care transition best practices Understand regulatory and payment support for care coordination
8 Why?
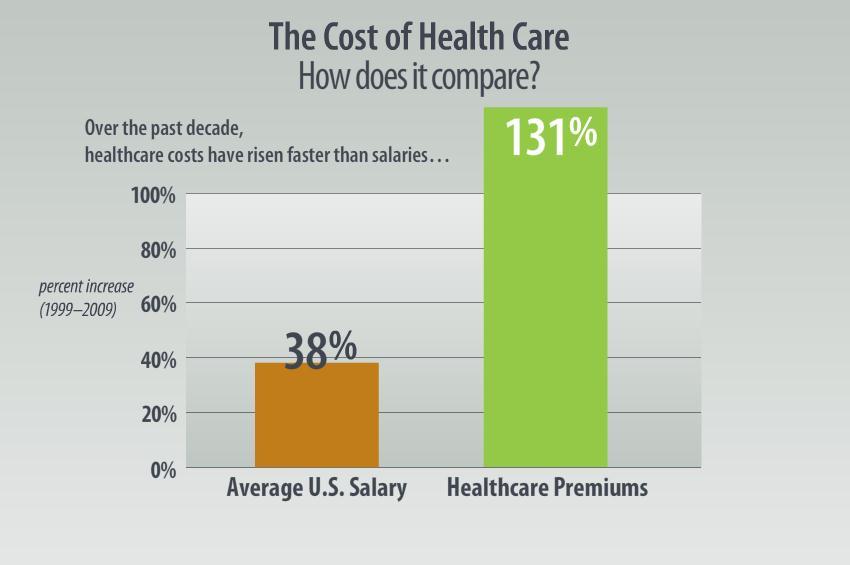
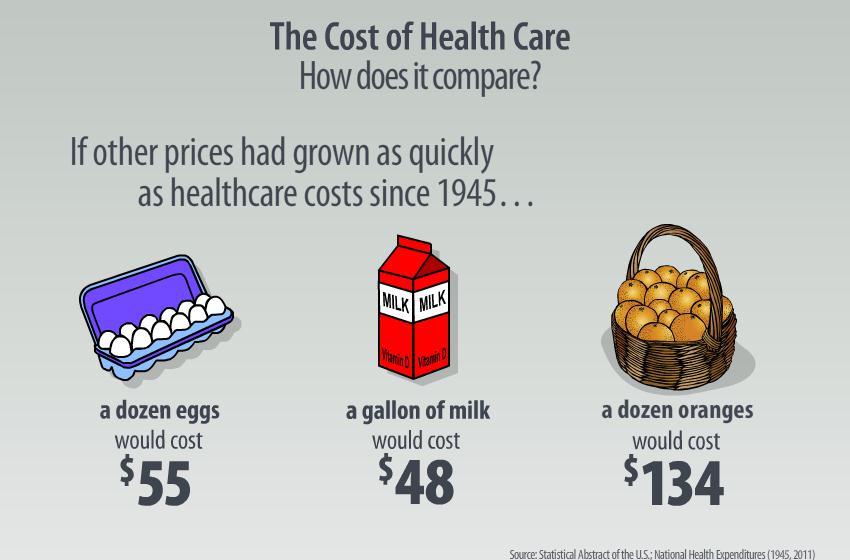
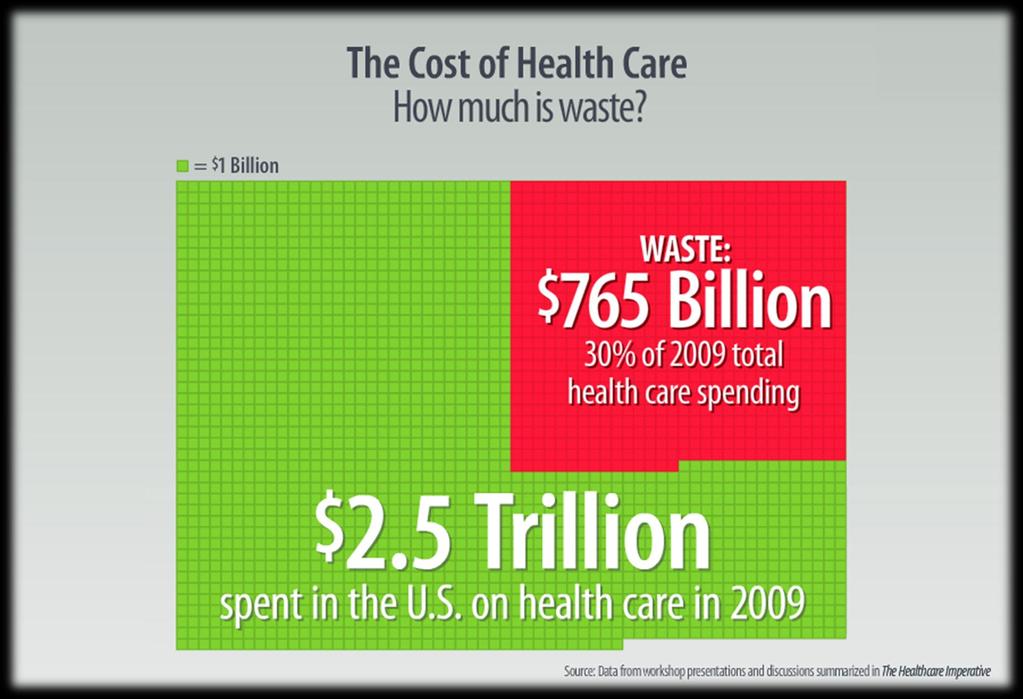
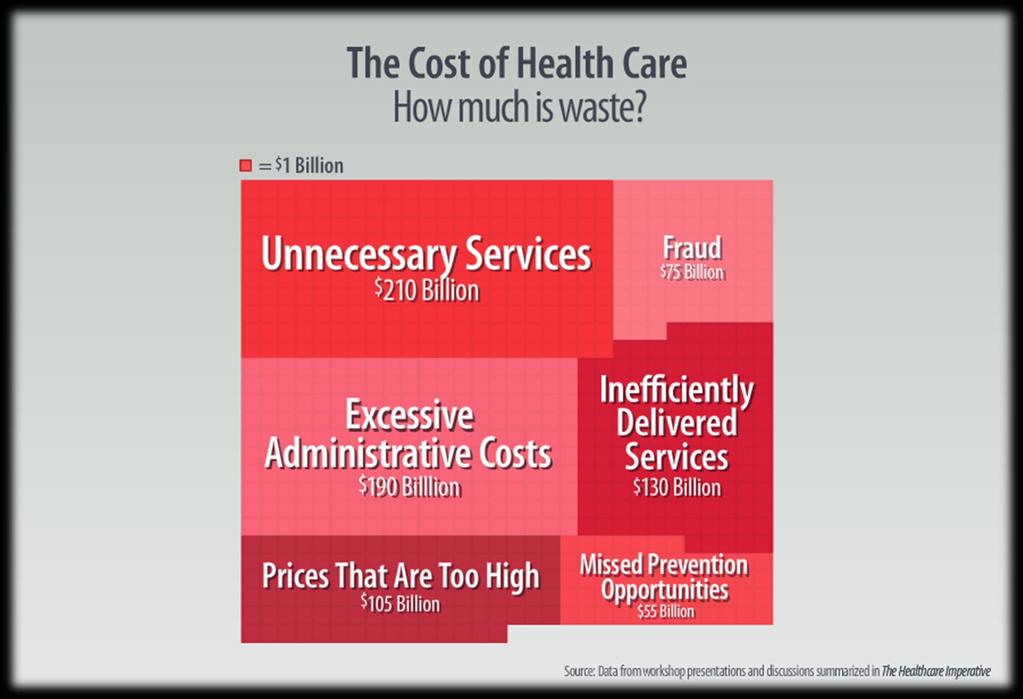
9 Cost For 31 of the past 40 years, health care costs have increased at a greater rate than the economy as a whole Health care costs constitute 18% of U.S. GDP 30% increase in personal income over the past decade effectively eliminated by a 76% increase in health care costs $765B in waste
10
11

12 Comparisons Health expenditures per capita (US$PPP)
13 Comparisons Life expectancy at birth
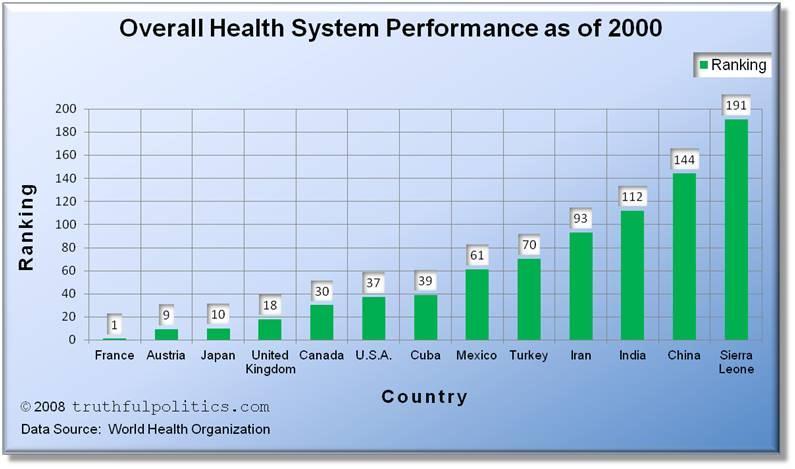
14 Comparisons

15 Missed Opportunities The U.S. Health Care System Today
16
17
18
19
20
21
22

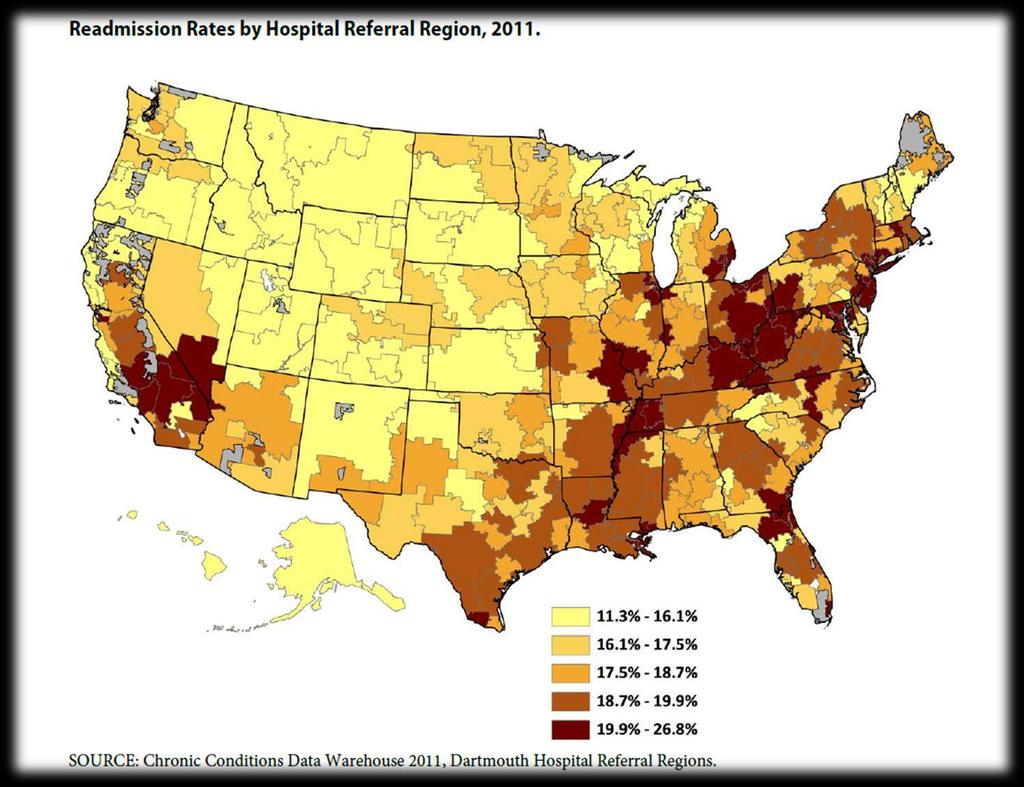
23 Challenges lead to readmissions Representative timeline of a patient s experiences in the U.S. health care system
24 Lack of coordination leads to costly care 90% of readmissions are unplanned Limited access to post-hospitalization follow-up care Usually related to poor care coordination and continuity <50% see a provider prior to the readmission Preventable transition errors (mostly medication related) Most patients are on 6+ medications at time of discharge Cost $25B annually Readmitted patients more costly with prolonged LOS Preventable readmissions could save $12B/year Heart disease and stroke lead the way, followed by diabetes
25 The situation Growing population with progressive disabilities requiring long-term services and supports 6M receive home, community or nursing home care in US Frequent changes in health Multiple transitions among providers 15% Medicare beneficiaries have chronic illness and long-term care needs 1/3 of Medicare spending Much of this spending and associated care is unnecessary
26 The response Hospital Compare Partnership for Patients Shared savings initiatives Affordable Care Act Section 3023, National Pilot Program on Payment Bundling Section 3025, Hospital Readmissions Reduction Program Section 3026, Community-Based Care Transitions Program National Quality Strategy
27 Partnership for Patients Funds hospital-level improvements 3500 hospitals 700,000 (75% of) index admissions among FFS Medicare beneficiaries Goal: 20% reduction in readmission rate by the end of 2013 through improving transitions of care
28 Section 3025 Hospital Readmissions Reduction Program Penalties for hospitals with excessive rehospitalization $280M in ,000+ hospitals penalized (1,910 less than 1%) Increase to 2% in 2013 and 3% in 2014 Targets heart failure, pneumonia and acute MI Applies to additional conditions beginning in 2015 Quality improvement programs through patient safety organizations to eligible hospitals with high severity-adjusted rehospitalization rates
29 Section 3025 Hospital Readmissions Reduction Program Motivates providers to focus on preventable rehospitalizations Provides incentives for behavior that could lead to improvements in outcomes for all beneficiaries Promising interventions have effectively reduced rehospitalizations among older chronically ill adults
30 Section 3026 Community-Based Care Transitions Program $500 million available to community-based organizations, in combination with one or more hospitals with high rehospitalization rates Provide transitional care services proven to improve outcomes and reduce costs Designed to reduce fragmentation


31 National Quality Strategy Aims and Priorities
32 Discussion
33 Getting to specifics The term transitions of care refers to a patient leaving one care setting and moving to another as their condition or healthcare needs change. The care transition often involves multiple persons including the patient, family or other caregivers An optimal transition should be well planned with the involvement of the patient and family, and adequately timed. More often, however, the communication between settings and the coordination among caregivers, patients and healthcare professionals fail to provide all the information needed for optimum quality of care

34 Care transition strategies and processes Patient Engagement Care Coordination/Communication Successful Transitions
35 Key Elements to Improving Transitions Ensure patient is the central member of the healthcare team Accuracy of information: comprehensive medication reconciliation on admission & transitions Literacy level of information given Provision of patient education with teach back Determination of patient s confidence prior to discharge Creation of comprehensive follow-up plan for those at risk Collaboration with community resources
36 Patient Engagement Activities Find safe, decent care Communicate with health professionals Organize health care Pay for health care Make good treatment decisions Participate in treatment Promote health Get preventive care Plan for end of life Seek health knowledge
37 The Patient at The Center Take patient and family preferences into account in deciding needs after discharge Diagnose patient preferences Clear concise advance directives Ensure patient has a good understanding of responsibilities for managing own health at discharge Ensure patient understands the purposes for taking medications at discharge
38 Ensuring Patient is an Active Team Member Increase physician visibility on patient units Health care team rounds at bedside Written daily care plan for patient/family Disease education with teach back Discharge instruction and medication education at discharge with teach back New medication education by pharmacy Measure and address patient s confidence at managing the medical plan Comprehensive follow-up post-discharge for high risk patients with telephone coaching and monitoring of community resources
39 Care coordination Begins in hospital before discharge Out of hospital services aligned with patient s needs Home health, rehabilitation services, outpatient ancillary follow-up with dieticians/counseling, etc. Ensure patient is an active team member The team is key to readmission reduction and patient quality of life optimization Relay of information to outside entities is key
40 Care Coordination by Patient-Centered Medical Homes Process to identify patients with hospital admissions and ED visits Process to share clinical information with hospital/ed Process to obtain patient discharge summaries Process to contact patients for follow-up care after discharge Process to exchange patient information with hospital Collaboration with patient/family to develop written care plan for transitions from pediatric to adult care Electronic exchange of key clinical information with facilities Provides electronic summary of care for more than 50% of transitions of care
41 Strategies strong evidence Re-Engineered Discharge Discharge advocate (specially trained nurse) Education throughout hospitalization Calls to reinforce discharge plan and offer problem solving Transitional Care Model Pre- and post-discharge coordination of care for high-risk, elderly patients with chronic illness by APNs Consistency of provider across entire episode of care
42 Strategies strong evidence Care transition program Medication self management Patient-centered record Follow-up with physician Knowledge of red flags and how to respond Evercare Care Model Enhanced primary care and care coordination by NPs and care managers NP care in nursing home setting Development and coordination of personalized care plans with all health providers
43 Potential Strategies Engage patients in planning quality improvements Patient education steering committee After hospital care plans Discharge planning checklists Leverage technology Enable connectivity across critical people, services, and information Active engagement with patient-generated information Web-based surveys Remote monitoring
44 More strategies Care partners support active engagement of informal caregivers (e.g., friends, family, volunteers) Embedded Case Management 400% increase in case managers embedded in primary care offices from 2011 to 2012 Top care sites for ECMs: Primary care practice (58%) Clinic (13%) Community (15%) Hospital (52%)
45 Results
46
47
48
49
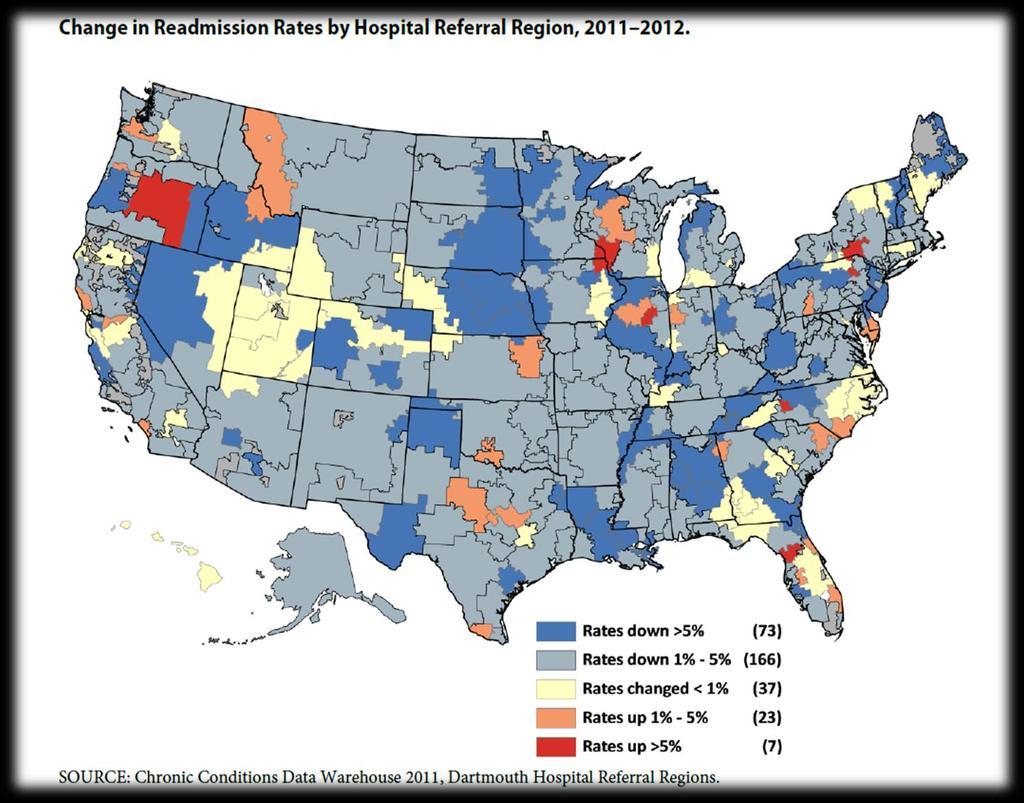
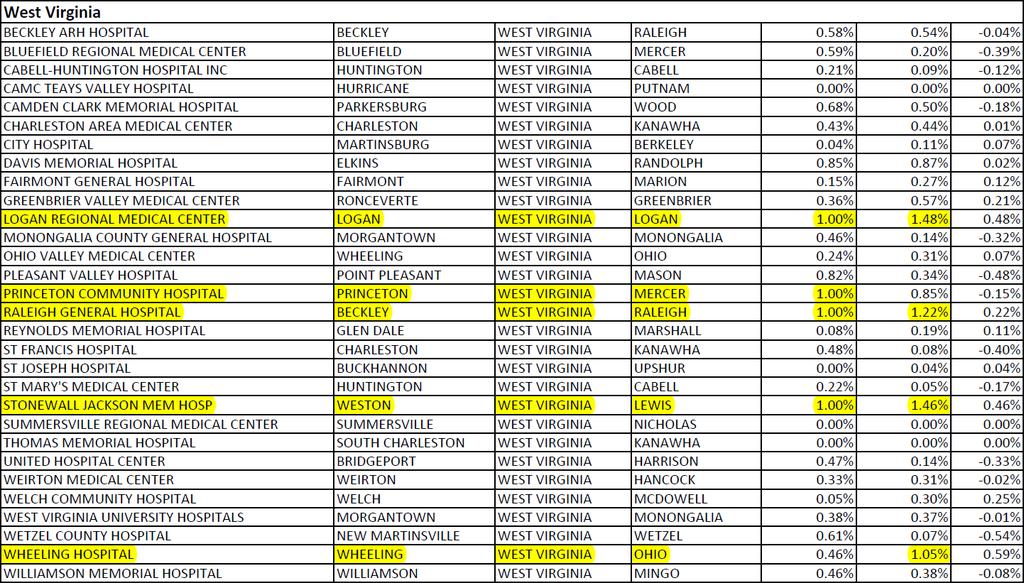
50 Hospital Readmissions Reduction Program Readmission penalities in West Virginia FY /30 hospitals had no penalty 4/30 hospitals had maximum penalty (1.00%) FY /30 hospitals had no penalty 4/30 hospitals had penalties greater than 1.00%
51
52 Unanticipated Consequences
53 Payment Bundling Incentivizes care delivery in the lowest-cost setting Creation of limited referral networks Market segmentation Withholding or denying services, shifting costs to postbundle period Excludes long-term services Little incentive to coordinate care before or beyond the episode Fails to integrate acute, postacute, and primary care services with community and institutionally based long-term services and supports
54 Section 3023 Barriers and Consequences Excludes long-term services Little incentive to coordinate care before or beyond the episode Fails to integrate acute, postacute, and primary care services with community and institutionally based long-term services and supports Incentivizes creation of limited referral networks and market segmentation Withholding or denying services, shifting costs to post-bundle period
55 Hospital Readmissions Reduction Program Barriers Many other health conditions commonly require rehospitalization (e.g., stroke, hip fracture, sepsis, UTI) Accounting for physical and cognitive deficits Chronic conditions + functional limitation = 2x cost Only high severity-adjusted rehospitalization rate hospitals eligible for QI services Excludes postacute and long-term care organizations High costs associated with preventing or reducing rehospitalization (e.g., electronic transfer of information)
56 Hospital Readmissions Reduction Program Unanticipated Consequences Ability of hospitals to offset relatively small losses from rehospitalization penalties with larger income earned from rehospitalization Penalty caps may incentivize hospitals to bear the penalties rather than the costs for prevention-related rehospitalization reduction strategies Availability of coding that could obscure or avoid measurement of some rehospitalizations (e.g. observational care)
57 Community-Based Care Transitions Program Hospitals serve as the hub of care transitions Program excludes patients not hospitalized or not living in geographic regions served by participating communitybased organizations Definition of high risk Medicare beneficiary Excludes those with low risk score but high functional impairment Not aligned with Medicaid or private payors Potential for duplication of services

58 It is not just about reimbursement
59 Or is it?
60 Financing Care Transitions
61 Getting Paid Discharge Encounter Discharge encounter Face-to-face examination Medication reconciliation Paperwork preparation/form completion Discharge summary dictation Time for completion is additive and must be documented Discharge summary Completion must be timely, even for observation services Succinct but complete Some musts Pertinent tests that were negative or positive Procedures restated with findings Medication list with medication changes from admission summarized Needed follow-up tests, office visits, or other appointments
62 Discharge care billable codes Inpatient care services (<30 minutes of time involved) (>30 minutes of time involved) Observation (outpatient) care services observation discharge (no time) admit/discharge same day Nursing home admission is separately billable even if performed on the same day
63 Getting Paid Transition Care Management Transition Care Management TCM codes mainly apply to primary care practices to help cover non face-toface services they offer Provided to patients discharged from Inpatient or observation status hospital care Skilled nursing facilities Partial hospitalization programs TCM Service: 99495/99496 Time period is 30 days (date of discharge and for next 29 days) Additional E/M visits outside of the one required are billed separately Documentation: date of d/c, date of dialogue to secure/confirm appointment, minimal content to address hospital course, subsequent correspondence, the E/M note associated with the f/u care, medication reconciliation no later than initial office visit
64 Transition Care Management (cont d) MDM of moderate complexity, face to face visit within 14 calendar days of discharge MDM of high complexity, face-to-face visit within 7 calendar days of discharge NOT to be used Unless physician or NPP accepts the care of patient post-discharge without a gap and accepts responsibility for the patient s care By surgeons in post-hospital global surgical period (90d) By hospitalists who do a one-time f/u visit By RHC and FQHCs In hospital hospital or hospital SNF transfer For TCM codes to be successfully used need partnerships: Hospital Hospital based physician Primary care physician Working as a team


65
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Declarations. Objectives. Lack of coordination leads to costly care update: Transition Care Management. Coding Today With a Look to Tomorrow:
 oding Today With a Look to Tomorrow: Transition are Management and eyond E. G. Nick Ulmer, Jr., MD P Vice President, linical Services and Medical Director of ase Management Spartanburg Regional Healthcare
oding Today With a Look to Tomorrow: Transition are Management and eyond E. G. Nick Ulmer, Jr., MD P Vice President, linical Services and Medical Director of ase Management Spartanburg Regional Healthcare
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System
 MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System STEPHANIE KENNAN, SENIOR VICE PRESIDENT 202.857.2922 skennan@mwcllc.com 2001 K Street N.W. Suite 400 Washington, DC 20006-1040
MedPAC June 2013 Report to Congress: Medicare and the Health Care Delivery System STEPHANIE KENNAN, SENIOR VICE PRESIDENT 202.857.2922 skennan@mwcllc.com 2001 K Street N.W. Suite 400 Washington, DC 20006-1040
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Submission #1. Short Description: Medicare Payment to HOPDs, Section 603 of BiBA 2015
 Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Submission #1 Medicare Payment to HOPDs, Section 603 of BiBA 2015 Within the span of a week, Section 603 of the Bipartisan Budget Act of 2015 was enacted. It included a significant policy/payment change
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes
 Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
What is Value-Based Care
 Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Transitional Care and Preventing Readmissions in San Francisco
 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Technical Overview of HCIP/CCIP
 Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings.
 Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Medicaid Managed Care Readiness For Agency Staff --
 Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Reimbursement Models of the Future A Look at Proposed Models
 Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Experience the Eide Bailly Difference Reimbursement Models of the Future A Look at Proposed Models Ralph J. Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 Introduction CAH reimbursement
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Medicaid Efficiency and Cost-Containment Strategies
 Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Transitional Care Management Services: New Codes, New Requirements
 Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR)
") Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
JOINT REPLACEMENT & OUTPATIENT BUNDLED PAYMENTS. Chris Bishop, CEO Regent Surgical Health
 JOINT REPLACEMENT & OUTPATIENT BUNDLED PAYMENTS Chris Bishop, CEO Regent Surgical Health HISTORY OF JOINTS IN THE OUTPATIENT SETTING Initial Headwinds to Change Payors Surgeons Clinical Staff Strong leadership
JOINT REPLACEMENT & OUTPATIENT BUNDLED PAYMENTS Chris Bishop, CEO Regent Surgical Health HISTORY OF JOINTS IN THE OUTPATIENT SETTING Initial Headwinds to Change Payors Surgeons Clinical Staff Strong leadership
Disclosure Statement
 2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Medicare: 2017 Model of Care Training 12/14/201 7
 Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Medicare: 2017 Model of Care Training 12/14/201 7 What is the Model of Care? The Model of Care (MOC) is Allwell s plan for delivering our integrated care management program for members with special needs.
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Assignment of Medicare Fee-for-Service Beneficiaries
 February 6, 2015 Ms. Marilyn B. Tavenner, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1461-P Room 445-G, Hubert H. Humphrey Building 200
February 6, 2015 Ms. Marilyn B. Tavenner, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1461-P Room 445-G, Hubert H. Humphrey Building 200
1. PROMOTE PATIENT SAFETY.
 SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
AGENDA. QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, /21/2014
 QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
General Background of CDI
 Clinical Documentation Improvement The Physician Champion ILHIMA 04/30/16 1 General Background of CDI 2 1 CMS Federal Register August 2008 Final Rule (CMS-1533-FC page 208) We do not believe there is anything
Clinical Documentation Improvement The Physician Champion ILHIMA 04/30/16 1 General Background of CDI 2 1 CMS Federal Register August 2008 Final Rule (CMS-1533-FC page 208) We do not believe there is anything
September 16, The Honorable Pat Tiberi. Chairman
 1201 L Street, NW, Washington, DC 20005 T: 202-842-4444 F: 202-842-3860 www.ahcancal.org September 16, 2016 The Honorable Kevin Brady The Honorable Ron Kind Chairman U.S. House of Representatives House
1201 L Street, NW, Washington, DC 20005 T: 202-842-4444 F: 202-842-3860 www.ahcancal.org September 16, 2016 The Honorable Kevin Brady The Honorable Ron Kind Chairman U.S. House of Representatives House
OUTPATIENT JOINT REPLACEMENT & BUNDLED PAYMENTS. Chris Bishop, CEO Regent Surgical Health
 OUTPATIENT JOINT REPLACEMENT & BUNDLED PAYMENTS Chris Bishop, CEO Regent Surgical Health HISTORY OF JOINTS IN THE OUTPATIENT SETTING Initial Headwinds to Change Payors Surgeons Clinical Staff Strong leadership
OUTPATIENT JOINT REPLACEMENT & BUNDLED PAYMENTS Chris Bishop, CEO Regent Surgical Health HISTORY OF JOINTS IN THE OUTPATIENT SETTING Initial Headwinds to Change Payors Surgeons Clinical Staff Strong leadership
April 26, Ms. Seema Verma, MPH Administrator Centers for Medicare & Medicaid Services. Dear Secretary Price and Administrator Verma:
 April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
Transforming Louisiana s Long Term Care Supports and Services System. Initial Program Concept
 Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
National Multiple Sclerosis Society
 National Multiple Sclerosis Society National 1 Kim, National diagnosed MS in Society 2000 > HEALTH CARE REFORM PRINCIPLES America s health care crisis prevents many people with multiple sclerosis from
National Multiple Sclerosis Society National 1 Kim, National diagnosed MS in Society 2000 > HEALTH CARE REFORM PRINCIPLES America s health care crisis prevents many people with multiple sclerosis from