NHS Forth Valley. Local Report ~ May Blood Transfusion
|
|
|
- Nicholas Curtis
- 6 years ago
- Views:
Transcription

1 NHS Forth Valley Local Report ~ May 2008 Blood Transfusion
2
3 kepcçêíüs~ääéó içå~äoééçêíúj~óommu _äçççqê~åëñìëáçå
4 içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók téü~îé~ëëéëëéçíüéééêñçêã~ååé~ëëéëëãéåíñìååíáçåñçêäáâéäóáãé~åíçåíüéëáñ Éèì~äáíóÖêçìéëÇÉÑáåÉÇÄó~ÖÉIÇáë~ÄáäáíóIÖÉåÇÉêIê~ÅÉIêÉäáÖáçåLÄÉäáÉÑ~åÇëÉñì~ä çêáéåí~íáçåkcçêíüáëéèì~äáíó~åççáîéêëáíóáãé~åí~ëëéëëãéåíiéäé~ëéëééçìêïéäëáíé EïïïKåÜëÜÉ~äíÜèì~äáíóKçêÖFKqÜÉÑìääêÉéçêíáåÉäÉÅíêçåáÅçêé~éÉêÑçêãáë~î~áä~ÄäÉçå êéèìéëíñêçãíüékepnfpbèì~äáíó~åçaáîéêëáíólññáåéêk «kepnì~äáíófãéêçîéãéåípåçíä~åçommu fp_knjuqqmqjqsmjo cáêëíéìääáëüéçj~óommu vçìå~ååçéóçêêééêççìåéíüéáåñçêã~íáçåáåíüáëççåìãéåíñçêìëéïáíüáåkeppåçíä~åç ~åçñçêéçìå~íáçå~äéìêéçëéëkvçìãìëíåçíã~âé~éêçñáíìëáåöáåñçêã~íáçåáåíüáë ÇçÅìãÉåíK`çããÉêÅá~äçêÖ~åáë~íáçåëãìëíÖÉíçìêïêáííÉåéÉêãáëëáçåÄÉÑçêÉ êééêççìåáåöíüáëççåìãéåík fåñçêã~íáçååçåí~áåéçáåíüáëêééçêíü~ëäééåëìééäáéçäókepäç~êçëlkep çêö~åáë~íáçåëiçêí~âéåñêçãåìêêéåíkepäç~êçlkepçêö~åáë~íáçåëçìêåéëiìåäéëë çíüéêïáëéëí~íéçi~åçáëäéäáéîéçíçäéêéäá~ääéçåéìääáå~íáçåk ïïïkåüëüé~äíüèì~äáíókçêö
5 `çåíéåíë N péííáåöíüéëåéåé R O pìãã~êóçññáåçáåöë S P aéí~áäéçñáåçáåöë~ö~áåëííüéëí~åç~êçë NM ^éééåçáñnódäçëë~êóçñ~ääêéîá~íáçåë ^éééåçáñoóoéîáéïéêçåéëë ^éééåçáñpóaéí~áäëçñêéîáéïîáëáí OV PM PN içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu P
6 içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu Q
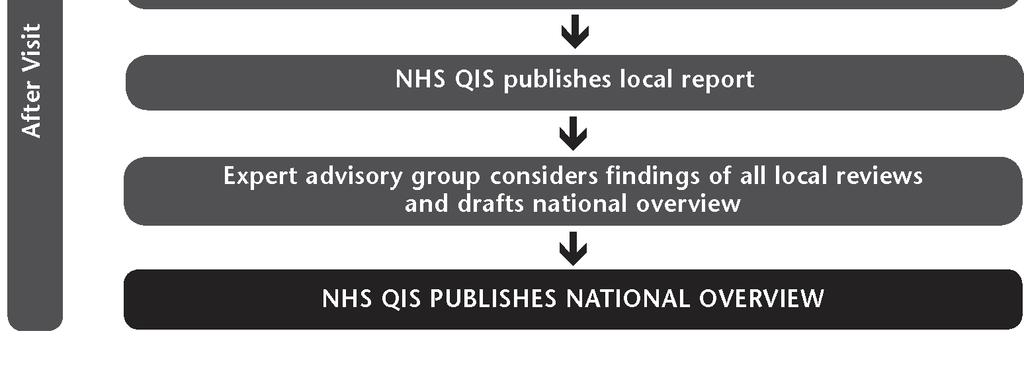
7 N péííáåöíüéëåéåé NHS Quality Improvement Scotland (NHS QIS) was set up by the Scottish Parliament in 2003 to take the lead in improving the quality of care and treatment delivered by NHSScotland. NHS QIS does this by setting standards and monitoring performance, and by providing NHSScotland with advice, guidance and support on effective clinical practice and service improvements. The Scottish National Blood Transfusion Service (SNBTS) is responsible for collecting, processing, storing and supplying all blood and blood components in Scotland and NHS boards are responsible for ordering and managing their supplies in a safe and effective manner. The Scottish Executive introduced a programme of work to improve and support transfusion practice in Scotland and, as a consequence, NHS QIS appointed a project group to develop clinical standards for blood transfusion practices. The project group developed four standards, covering: core principles; clinical management pre-transfusion; clinical management hospital transfusion laboratory; and clinical management blood and blood component collection, administration and monitoring. The Clinical Standards for Blood Transfusion were published in September These include details of the project group which set the standards and are available on request from NHS QIS or can be downloaded from the website ( About this report This report presents the findings from the peer review of NHS Forth Valley s performance against the blood transfusion standards. The review process has three key phases: preparation prior to the visit; the visit; and the report production and publication following the visit. (See flow chart in Appendix 2 for further detail.) During the visit, each multidisciplinary review team assesses performance using the categories met, not met and not met (insufficient evidence), as detailed below. Met applies where the evidence demonstrates the standard and/or criterion is being attained. Not met applies where the evidence demonstrates the standard and/or criterion is not being attained. Not met (insufficient evidence) applies where no evidence is available for the review team, or where the evidence available is insufficient to allow an assessment to be made. A final category not applicable is used where a standard and/or criterion does not apply to the NHS board under review. Each review team is led by an experienced reviewer, who is responsible for guiding the team in their work and ensuring that team members are in agreement about the assessment reached. Membership of the review team visiting NHS Forth Valley on 6 February 2008 can be found in Appendix 3. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu R
8 O pìãã~êóçññáåçáåöë OKN lîéêîáéïçñäçå~äëéêîáåééêçîáëáçå Forth Valley is situated in central Scotland and has a population of around 286, While Forth Valley comprises both urban and rural areas, the majority of the population live in urban areas, of which Falkirk and Stirling are the largest. içå~äkepëóëíéã~åçëéêîáåéë Forth Valley NHS Board is responsible for improving the health of the local population and for the delivery of the healthcare required. It provides strategic leadership and has responsibility for the efficient, effective and accountable performance of the NHS in Forth Valley. At the time of the review visit, NHS Forth Valley was a single integrated system comprising acute hospital services, and community based services which are delivered through three community health partnerships in Clackmannanshire, Falkirk and Stirling. Further information about the local NHS system can be accessed via the website of NHS Forth Valley ( The NHS Forth Valley s hospital blood bank is in the laboratory department of Stirling Royal Infirmary (SRI) and provides serology and blood issue for all areas of NHS Forth Valley. The blood bank receives blood and blood components from the West of Scotland SNBTS (Clinical Directorate) hospital transfusion laboratory (WOSBTS) based at Gartnavel Hospital, Glasgow. SRI supplies Falkirk & District Royal Infirmary (FDRI) haematology laboratory and Strathcarron Hospice, Denny, with blood and blood components, as required. The WOSBTS also supplies blood and blood components to Abbey King s Park Hospital, Stirling. In the 12 months prior to the review visit, approximately 9,300 red cell units were transfused. The NHSScotland Better Blood Transfusion Programme (BBTP) is supported by a transfusion practitioner who works across all NHS Forth Valley hospital sites. The transfusion practitioner is assisted by five other BBTP trainers. 1 General Register Office for Scotland. Mid-2006 Population Estimates Scotland: Population Estimates by Age and Sex and Administrative Area. First published on 26 April Revised 27 July Available from: içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu S
9 OKO pìãã~êóçññáåçáåöë~ö~áåëííüéëí~åç~êçë A summary of the findings from the review is presented in this section. A detailed description of performance against the standards/criteria is included in Section 3. `çêééêáååáéäéë NHS Forth Valley has an established multidisciplinary hospital transfusion committee (HTC) which meets quarterly and reports to the acute services clinical governance working group. This working group is chaired by NHS Forth Valley s chief operating officer. The HTC remit includes promotion of best practice through local blood transfusion protocols which are based on national guidelines. Whilst audit activity related to the blood transfusion standards has been taking place, this has not been multidisciplinary and there has been limited resource for the HTC to act on the audit findings. There is a highly committed operational transfusion team which promotes the targets of the NHSScotland BBTP. The team is led by the BBTP clinical lead who also sits on the HTC. The transfusion practitioner is an active member of the transfusion team and also sits on the HTC. Any laboratory-related blood transfusion incidents are investigated by the laboratory quality manager. The transfusion practitioner investigates all such clinical-related incidents and follows up with relevant staff, providing retraining as necessary. The review team encouraged the board to ensure that the HTC was more actively involved in implementing corrective and preventative change to protocols following the transfusion practitioner s investigations. NHS Forth Valley uses a bag and tag system to ensure that every unit of blood component received into the SRI laboratory can be unmistakeably traced to its recipient, or to its final fate if not transfused. There is a dedicated medical laboratory assistant with responsibility for the traceability of all units. The minimum identification data set specified to be used at every stage of the blood transfusion process in NHS Forth Valley includes full name, gender, date of birth and a unique identifier. Audit findings, however, showed that not all patients were wearing wristbands, and that not all wristbands bore the unique identifier. For patients whose identity cannot be confirmed, a minimum of gender and a unique identifier would be included on their wristband. Phlebotomists confirmed that they would not take a blood sample without the patient wearing a wristband. A risk assessed alternative to a wristband had not been agreed. This will be addressed when the NHS Forth Valley identification policy is implemented. Staff are aware that patients have an option to refuse blood transfusion and there is a system in place to alert qualified practitioners to the existence of an advance directive or special requirements. The board has a strategy for management of blood shortages. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu T
10 `äáåáå~äã~å~öéãéåíóéêéjíê~åëñìëáçå An audit of transfusion documentation has identified that the reasons for transfusion are being discussed with the patient, however, there was no evidence in the patient notes of the discussion of alternatives to transfusion or the option to refuse. A comprehensive transfusion care pathway form has been developed which includes prompts about the discussions and blood transfusion explanatory leaflets. The pathway has been piloted in FDRI and staff reported that this had significantly improved compliance with the blood transfusion standards. Where pre-transfusion discussion is not possible, for example in accident and emergency if the patient is unconscious, action would be taken to establish if the patient had an advance decision document including a search on NHSScotland s Emergency Care Summary utility if partial identity could be established. Information leaflets, explaining the risks and benefits of transfusion would be offered to such patients on their discharge. Positive patient identification at the time of blood sampling is included in all BBTP training, however, audit had identified that wristbands were not always in place and that the unique identifier was not always present on the wristbands. Prescriptions for blood units are signed by a qualified practitioner and are adequately detailed. `äáåáå~äã~å~öéãéåíóüçëéáí~äíê~åëñìëáçåä~äçê~íçêó The transfusion laboratories at FDRI and SRI are accredited by Clinical Pathology Accreditation (UK) Ltd (CPA).The SRI blood bank is preparing for an inspection by the Medicines and Healthcare products Regulatory Agency (MHRA) and has a challenging action plan in place. Competency-based training and assessment systems have been implemented and training records are maintained. NHS Forth Valley commissions services for NHS patients from Abbey King s Park Hospital and has suitable arrangements in place to ensure that the provider complies with current regulatory requirements. There are protocols in place to optimise blood use and minimise wastage although, at the time of the review visit, the laboratory was using a paper-based stock management system and could not contribute to the national transfusion epidemiology database. The review team noted that the implementation of the recently purchased Blood Track system would be a challenge for the board, but it would be a more robust system and would provide for more efficient stock management. The review team encouraged laboratory staff to participate in multidisciplinary audit. `äáåáå~äã~å~öéãéåíóääççç~åçääçççåçãéçåéåíåçääéåíáçåi ~Çãáåáëíê~íáçå~åÇãçåáíçêáåÖ The BBTP training programme, delivered by the transfusion practitioner and five other trainers, emphasises that only staff who have undertaken BBTP training appropriate to their role participate in the blood transfusion process. Positive patient identification is highlighted in the BBTP training, although audit had identified that içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu U
11 not all patients were found to be wearing a wristband and not all wristbands included the unique identifier. Protocols are in place for the monitoring of patients immediately before and during blood transfusion and any untoward events (including suspected adverse reactions) are immediately clinically managed and reported promptly to the hospital transfusion laboratory. Observational audit of transfusion episodes indicated that the protocol was not always being followed, although the new transfusion pathway form assists with this. Serious adverse events or reactions and near miss incidents are submitted to the relevant regulatory and reporting bodies. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu V
12 P aéí~áäéçñáåçáåöë~ö~áåëííüéëí~åç~êçë pí~åç~êçn~w`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüéêé~êéëóëíéãëáåéä~åéëìééçêíáåöåäáåáå~äöçîéêå~ååéíçéåëìêéë~ñéiéññéåíáîé~åç ~ééêçéêá~íéääçççíê~åëñìëáçåk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ N~KNW qüéêéáë~åéëí~ääáëüéçi~åíáîéiãìäíáçáëåáéäáå~êóüçëéáí~äíê~åëñìëáçååçããáííéé Eeq`FíÜ~íÜ~ëÇÉÑáåÉÇêÉëéçåëáÄáäáíáÉë~åÇ~ÅÅçìåí~ÄáäáíóíçíÜÉÅÜáÉÑ ÉñÉÅìíáîÉLkepÄç~êÇîá~íÜÉÅäáåáÅ~äÖçîÉêå~åÅÉëíêìÅíìêÉK pq^qrpwmet There is an established, multidisciplinary NHS Forth Valley hospital transfusion committee (HTC), with a ratified constitution and remit, which meets quarterly and follows a standing agenda. A consultant anaesthetist has been recently appointed as the committee chair, and staff reported that expanded representation from further blood user groups such as surgery and primary care, was being actively followed up. The review team noted the significant improvement in user representation on the HTC in the last year and acknowledged the challenge for the board to further broaden its membership. The head of clinical governance sits on the HTC and on the acute services clinical governance working group to which the HTC reports. This working group is chaired by NHS Forth Valley s chief operating officer and reports up to the NHS Forth Valley clinical governance committee (CGC) with which it shares membership. N~KOW qüéeq`ü~ëêçäéë~åçêéëéçåëáäáäáíáéë~ëçìíäáåéçáåjbienvvvfv~åç eaieommpfnvkqüéëéáååäìçéáåîçäîéãéåíáåãìäíájéêçñéëëáçå~ä~ìçáíiéçìå~íáçå ~åçíê~áåáåöiçéîéäçéãéåí~åçãççáñáå~íáçåçñöìáçéäáåéë~åçéêçíçåçäëi~åç áåîçäîéãéåíçñëí~âéüçäçéêëk pq^qrpwnot met NHS Forth Valley s HTC has a documented constitution and remit which includes promotion of best practice through local protocols based on national guidelines; commissioning of blood transfusion related audits; promotion of education and training and incident monitoring. The review team noted that several useful audits had been conducted, although these had been instigated by the clinical lead for blood transfusion and the transfusion practitioner. There had not been multi-professional HTC involvement in these audits and the topics had not, at the time of the review visit, been re-audited in order to içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NM
13 demonstrate improvements following retraining. With the appointment of a consultant anaesthetist, as chair of the HTC, the board anticipated more involvement of all blood user groups in audit. The transfusion practitioner provides an update on NHSScotland s Better Blood Transfusion Programme (BBTP) training at each HTC meeting, and is working towards the production of local unit BBTP training plans. The review team acknowledged the level of BBTP trained staff, in all groups, as an achievement. There was limited evidence of protocols having been changed by the HTC, as a result of audit findings, or the committee s review of incidents. Staff reported that although the HTC had no resource to prepare an action plan to address all audit findings, the clinical governance working group would support the progress of such plans. It was also reported that mechanisms were in place to cascade out changes in practice through the safe and effective care committee feeding back to general managers, service managers and individual unit clinical governance groups. The review team encouraged the board to clarify and document the remit of the HTC to ensure that the HTC could promote improvement in practice, through review and initiation of modification of local protocols in line with national guidelines. The transfusion practitioner maintains a register of all blood transfusion-related protocols and their distribution to all relevant units. The transfusion practitioner personally distributes revised protocols, and retrieves and destroys the previous version. The hospital transfusion team plan to integrate this register into an electronic quality management system (ipassport ) which is already in use in the laboratories. This system will then automatically the clinical lead for transfusion and the transfusion practitioner with prompts to review protocols at the relevant times. N~KPW qüéeq`iáååçää~äçê~íáçåïáíüíüéåäáåáå~äöçîéêå~ååéåçããáííééiáãéäéãéåíë íüékeppåçíä~åç_éííéê_äçççqê~åëñìëáçåmêçöê~ããée qmfk pq^qrpwmet The review team noted that there was a highly committed operational transfusion team in place to fulfil the objectives and aims of the HTC. This team meets every 4-6 weeks and is chaired by the BBTP clinical lead who also sits on the HTC. The transfusion practitioner is an active member of this team, as well as the HTC, NHS Forth Valley acute services safe and effective care committee, and NHS Forth Valley acute services patient safety group. This provides opportunities for the transfusion practitioner to engage with all clinical units and promote the targets of the BBTP throughout NHS Forth Valley. At the time of the review visit, the laboratory was not able to participate in the BBTP Scottish Transfusion Epidemiology Database that would inform users and providers içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NN
14 about the extent and the outcome of the use of blood. Staff reported that this is being addressed by the board. N~KQW qüéeq`êéîáéïë~ääêééçêíëçñ~çîéêëééîéåíë~åçåé~êãáëëáååáçéåíëêéä~íáåöíç ÄäççÇíê~åëÑìëáçå~åÇIáåêÉëéçåëÉIáãéäÉãÉåíëÅÜ~åÖÉëáåéê~ÅíáÅÉïÜÉêÉ åéåéëë~êók pq^qrpwnot met Blood transfusion-related incidents occurring at any blood transfusion site within NHS Forth Valley are reported to the Stirling Royal Infirmary (SRI) laboratory and transfusion practitioner by telephone and an incident record form (IR1) is completed. One copy of the IR1 is sent to the unit manager and the second is sent to the risk management department. The clinical risk management co-ordinator receives a copy of all IR1 forms that relate to clinical incidents. If the IR1 relates to blood transfusion, a copy of the form is sent to the transfusion practitioner. Laboratorybased incidents are investigated by the laboratory quality manager with input from the transfusion practitioner and appropriate corrective action taken. The transfusion practitioner investigates all clinical incidents and addresses any training needs with the individuals directly involved in the incident. All blood transfusion-related incidents are discussed by the transfusion practitioner, the clinical lead for transfusion and the laboratory quality manager, and there is further sharing of information about incidents at the transfusion team meetings where recommendations are formulated. The transfusion practitioner prepares an incident report, informs the staff involved, and their manager, and follows up on any outstanding actions or training needs identified. The hospital transfusion team reports serious blood transfusion related incidents and near miss incidents to Serious Adverse Blood Reactions and Events (SABRE) and Serious Hazards of Transfusion (SHOT). The transfusion practitioner reports on all blood transfusion-related incidents to the HTC, and all SABRE/SHOT reportable events would be discussed at the HTC and the acute services critical incident review group. The review team encouraged the HTC to be more proactive in following up the transfusion practitioner s incident reports and transfusion team recommendations, and modifying protocols to include preventative measures where appropriate. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NO
15 pí~åç~êçnäw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüékepäç~êçü~ë~ëóëíéãáåéä~åéíçéåëìêéíü~íéîéêóìåáíçñääçççåçãéçåéåí êéåéáîéçáåíçíüéüçëéáí~äíê~åëñìëáçåä~äçê~íçêóå~åäéìåãáëí~â~ääóíê~åéçíçáíë êéåáéáéåíiçêíçáíëñáå~äñ~íéáñåçííê~åëñìëéçk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêáçå NÄKNW qüéêéáë~î~äáç~íéçëóëíéãíçéåëìêéíü~íéîáçéååéçñìåãáëí~â~ääéíê~åé~äáäáíóáë ÖÉåÉê~íÉÇIëíçêÉÇ~åÇ~ÅÅÉëëáÄäÉÑçêPMóÉ~êëK pq^qrpwmet Every unit of blood component received into the SRI blood transfusion laboratory is identified with a donation number. When a component is required for a patient, a paper issue tag is printed from the laboratory computerised system which includes patient identifying information and two self-adhesive traceability labels; each label contains the donation number. The issue tag is attached to the unit of blood component until it is transfused or returned to the laboratory if unused. If transfused, one label from the tag is signed and placed in the patient s notes and the other is completed and returned to the transfusion laboratory to confirm the patient received the component. The returned labels are attached onto the back of an issue sheet with details of components supplied. When reconciled, these issue sheets are stored indefinitely in the laboratory. If a label is not returned within 1 week of issue of the component, a non-compliance letter is sent to the service manager for the area involved stating which information is missing and asking for confirmation that the units were transfused. The service manager ensures that the area clinical co-ordinator checks the patient s notes and completes the letter. If the letter is returned complete, it is filed with the issue sheet. If the letter is not returned to the laboratory or is returned incomplete, an IR1 form is completed by the medical laboratory assistant (MLA) responsible for monitoring traceability compliance. This letter is sent to the risk management department and the general manager of the area involved. It is then the general manager s responsibility to determine the fate of the units. The bag and tag system was introduced to NHS Forth Valley at the start of The transfusion practitioner prepared an instruction sheet for completion of the traceability tags and an illustrated poster on the new system. These were distributed to all relevant areas. It was noted that an action plan is in place to address the findings of a traceability audit which had been conducted by the MLA dedicated to traceability. Staff reported that compliance had improved since the audit and, at the time of the review visit, was running very close to 100%. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NP
16 pí~åç~êçnåw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüéêéáë~êçäìëíëóëíéãáåéä~åéíçéëí~ääáëüé~íáéåíáçéåíáñáå~íáçåçéí~áäë~åçã~áåí~áå íüáë~íéîéêóëí~öéçñíüéåäáåáå~äíê~åëñìëáçåéêçåéëëk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ NÅKNW qüéãáåáãìãáçéåíáñáå~íáçåç~í~ëéíeëìêå~ãéiñçêéå~ãéiëéñiç~íéçñäáêíü~åç ìåáèìéáçéåíáñáå~íáçååìãäéêiéö`çããìåáíóeé~äíüfåçéñx`efzfáëìëéç~íéîéêó ëí~öéçñíüéåäáåáå~äíê~åëñìëáçåéêçåéëëíçéçëáíáîéäóáçéåíáñóíüéé~íáéåík pq^qrpwnot met The NHS Forth Valley blood transfusion protocol states that full name, date of birth, gender and Community Health Index (CHI) or other acceptable unique identifier are used at every stage of the clinical transfusion process to positively identify the patient. A generic patient identification policy has been drafted which includes the same minimum identification data set for inclusion on patient wristbands. Observational audit of positive patient identification at pre-transfusion sampling, collection and pre-administration identified that the CHI number was not always being recorded and checked, and that gender was not always recorded on wristbands. A separate wristband audit identified that wristbands were not always in place and that the CHI number was not always present. However, phlebotomy staff reported that if a patient was not wearing a wristband, blood would not be taken and action would be taken to ensure that a wristband was prepared for the patient immediately. Positive patient identification is included in the BBTP training sessions and, following the audit findings, all materials have been updated to include reinforcement of the requirement for completeness of the data set. Further audit is planned. The review team noted that the policy for venous blood sampling did not refer to gender recording and checking, and encouraged the board to standardise this across all relevant policies. NÅKOW ^ääé~íáéåíëãìëíäéáçéåíáñá~ääé~í~ääíáãéëkfåé~íáéåíë~åçç~óé~íáéåíëãìëí ïé~ê~åáçéåíáñáå~íáçåïêáëíä~åçkfñíüéïêáëíä~åçäéåçãéëáå~ååéëëáääéñçê~åó êé~ëçåi~å~äíéêå~íáîéiêáëâj~ëëéëëéçñçêãçñáçéåíáñáå~íáçåáë~ççéíéçáããéçá~íéäók pq^qrpwnot met The blood transfusion protocol states that all inpatients must wear an identity wristband. The draft patient identification policy applies to inpatients and allows for use of wristbands for day cases. Staff confirmed that blood transfusion would only be conducted if the patient was wearing a wristband. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NQ
17 The draft identification policy is currently being circulated for comment to all interested parties. The draft policy allows for risk-assessed alternatives to be used in such circumstances. At the time of the review visit, however, a risk-assessed alternative was not in use. Staff reported that if, for example, a patient s wristband became covered by drapes in theatre, an identification band would be put on another wrist or ankle if accessible or an addressograph label would be adhered to the patient s forehead. Neither of these options has been risk assessed. Staff reported that when the identification policy was launched it was intended to issue portable blood audit release system (BARS) scanners to the phlebotomists to pilot their use for identification purposes. A request to include gender in the scanner s software for patient identification checks had been sent to the system provider. NÅKPW qüéêéáë~ëóëíéãeéöçáëíáååíáîéïêáëíä~åçëfíç~äéêíèì~äáñáéçéê~åíáíáçåéêëíç é~íáéåíëïüçü~îéëééåáñáåíê~åëñìëáçåêéèìáêéãéåíëiáååäìçáåöíüéïáëüíçåçíäé íê~åëñìëéçk pq^qrpwmet NHS Forth Valley casenotes include a printed divider at the front which has a series of alerts including the existence of an advance directive and specific transfusion requirements. A consent form to operation, investigation or treatment, which includes a section for patients to opt out of receiving a blood transfusion, was being piloted in one specialty prior to roll out across acute services. There is a comprehensive policy for the management of patients who refuse blood transfusion. The review team noted an effective flow chart for the care of women who are pregnant and who refuse the administration of blood or blood products. For elective surgical patients who refuse transfusion, an information session is arranged with the consultant anaesthetist at their pre-operative assessment. NÅKQW cçêé~íáéåíëïüçëéáçéåíáíóå~ååçíäéåçåñáêãéçeéöìååçåëåáçìëé~íáéåíëçê é~íáéåíëïáíüåçããìåáå~íáçåçáññáåìäíáéëfi~ãáåáãìãçñöéåçéê~åççåéìåáèìé áçéåíáñáéêeéö~ååáçéåí~åçéãéêöéååóåìãäéêçê`efåìãäéêfáëéëëéåíá~äñçê éçëáíáîéé~íáéåíáçéåíáñáå~íáçåk pq^qrpwmet The blood transfusion protocol states that if an unconscious patient is admitted, and their identity can not be confirmed, a wristband is prepared containing a unique identification number, generated by the accident and emergency information technology (IT) system, and marked with their gender. Staff reported that uniquely numbered identification packs are available in the accident and emergency area for use to identify mass casualties in a major incident. Specific procedures for patients with communication difficulties could not be confirmed by the review team, although it was clear that interpreting and translation facilities were available. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NR
18 pí~åç~êçnçw`çêémêáååáéäéë pí~åç~êçpí~íéãéåí qüékepäç~êçü~ë~ëíê~íéöóñçêã~å~öéãéåíçñääçççëüçêí~öéëk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêáçå NÇKNW bãéêöéååóääçççã~å~öéãéåí~êê~åöéãéåíëeb_j^f~êééëí~ääáëüéç~ëçéñáåéç áåeaieommrfork pq^qrpwmet An emergency blood stocks management group has been established and is chaired by the NHS Forth Valley medical director. The operational arm of this group is the hospital transfusion team. When the Scottish National Blood Transfusion Service (SNBTS) contacts the SRI transfusion laboratory to advise of a blood shortage, the laboratory contacts the consultant haematologist lead for transfusion who discusses the situation with the medical director. The emergency blood management arrangements (EBMA) and information cascade are activated as appropriate. The review team encouraged the board to consider including all up-to-date contact details within the EBMA flow chart. The EBMA have been linked to the major incident plan and staff reported that, at the most recent clinical governance working group meeting, it had been agreed to test the EBMA in a mock exercise. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NS
19 pí~åç~êço~w`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí qüéçéåáëáçåíçíê~åëñìëéáëã~çéñçääçïáåöåçåëáçéê~íáçåçñíüééçíéåíá~äêáëâë~åç ÄÉåÉÑáíëçÑI~åÇíÜÉ~äíÉêå~íáîÉëíçIíê~åëÑìëáçåKtÜÉêÉéçëëáÄäÉíÜáëáëÇáëÅìëëÉÇÄÉíïÉÉå íüéåäáåáåá~å~åçé~íáéåíeçêíüéáêäéö~äöì~êçá~åfáå~çî~ååéçñíê~åëñìëáçåk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ O~KNW qüéé~íáéåíûëêéåçêçëåçåí~áåéîáçéååéíü~ííüéêé~ëçåñçêíê~åëñìëáçåçñääççççê ÄäççÇÅçãéçåÉåíëÜ~ëÄÉÉåÉñéä~áåÉÇ~åÇÇáëÅìëëÉÇïáíÜíÜÉé~íáÉåíKqÜáë áååäìçéëçáëåìëëáçåçñî~äáç~äíéêå~íáîéëíçíê~åëñìëáçå~åçíüéçéíáçåíçêéñìëék pq^qrpwnot met An audit of transfusion episode documentation completeness was conducted in the programmed investigation and treatment unit (PITU) at Falkirk & District Royal Infirmary (FDRI). This audit was conducted to measure a baseline against which improvement could be demonstrated following the pilot introduction of a transfusion care pathway for outpatients and day patients in the unit. The audit identified that the reasons for transfusion were being discussed with the patients and documented in their casenotes. There was, however, no documented evidence of a discussion about alternatives to transfusion and the option to refuse. The review team encouraged the HTC to modify the transfusion protocol in line with this standard criterion. Staff reported that the use of the transfusion care pathway had greatly improved the level of documentation compliance, although this had yet to be formally measured by audit. It was reported that the care pathway had also helped document lines of responsibility for patients who had been referred to the unit by a GP. The pathway was also evaluated in the medical ambulatory care and treatment unit and will be tailored for introduction into other areas across NHS Forth Valley. The review team noted the benefits of introducing the transfusion care pathway and encouraged the board to finalise its implementation in all areas. O~KOW ié~ñäéíëéñéä~áåáåöíüéêáëâë~åçäéåéñáíëçñi~åç~äíéêå~íáîéëíçiíê~åëñìëáçå~êé êé~çáäó~î~áä~ääéñçêé~íáéåíëïüçã~óêéèìáêéíçäéiçêü~îéäééåíê~åëñìëéçk pq^qrpwmet NHS National Services Scotland produces a variety of blood transfusion-related information leaflets which are available in all relevant areas in NHS Forth Valley. These leaflets are also available in other languages. These are distributed by the transfusion practitioner who maintains records of receipt. A flow chart for contacting interpreters is available in all clinical areas and in the accident and emergency içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NT
20 department there is a phone system which can enable three-way conversation. The new transfusion care pathway contains a prompt to offer a leaflet. If a patient requests further information on alternatives to transfusion, they are referred to the transfusion practitioner. At the time of the review visit, cell salvage was only available for patients having a revision of a hip replacement. Staff reported that with orthopaedic representation on the HTC, it was anticipated that the awareness of cell salvage might increase. O~KPW tüéêééêéjíê~åëñìëáçåçáëåìëëáçåáëåçíéçëëáääéeéöáå~åéãéêöéååófíüéêéáë~ ëóëíéãiåçãé~íáääéïáíüíüéé~íáéåíûëåäáåáå~äåééçëiíçáåîéëíáö~íé~åç~åíáå ~ÅÅçêÇ~åÅÉïáíÜíÜÉé~íáÉåíÛëíêÉ~íãÉåíéêÉÑÉêÉåÅÉëKqÜáëáåÅäìÇÉëÅçãéäá~åÅÉ ïáíü~å~çî~ååéçéåáëáçåççåìãéåík pq^qrpwmet Accident and emergency staff confirmed that if an unconscious person was admitted they would search the patient for any identifying information including evidence of the existence of an advance directive. When some identifying features are found, a search on NHSScotland s Emergency Care Summary utility would be made to access further identifying information and any relevant medical details. If there is any indication of the existence of an advance directive, staff would confirm this with any accompanying family or friends before commencing a blood transfusion. These procedures are covered in the scenario induction training for new accident and emergency staff. There have been no known instances of adverse events or patient complaints arising from non-compliance with advance decision documents. O~KQW tüéåéêéjíê~åëñìëáçåçáëåìëëáçåü~ëåçíí~âéåéä~åéiíüéêé~ëçåëñçêíê~åëñìëáçå EÄ~ëÉÇçåêáëâë~åÇÄÉåÉÑáíëF~êÉÇáëÅìëëÉÇïáíÜíÜÉé~íáÉåí~åÇïêáííÉå áåñçêã~íáçåçññéêéçêéíêçëééåíáîéäók pq^qrpwnot met (insufficient evidence) Staff reported that women requiring emergency blood transfusion during childbirth would be given an information leaflet prior to discharge. A prompt for issue of an information leaflet is included on the discharge care pathway in use in the intensive care unit and the surgical high dependency unit. Staff reported that they would give the relevant leaflets to attending relatives. Completeness of the discharge care pathway had not been audited and there was no evidence available to the review team to assure it that a post-transfusion discussion was taking place and that information was being offered retrospectively. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NU
21 pí~åç~êçoäw`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí mçëáíáîéé~íáéåíáçéåíáñáå~íáçå~ííüéíáãéçñë~ãéäáåö~åçíüéìëéçñ~ãáåáãìã áçéåíáñáå~íáçåç~í~ëéíçåë~ãéäéë~åçêéèìéëíñçêãëáëéëëéåíá~äñçêéêéjíê~åëñìëáçåíéëíáåö ~åçääçççåçãéçåéåíêéèìéëíëk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêáçå OÄKNW _äçççë~ãéäéëñçêíê~åëñìëáçåéìêéçëéë~êéçäí~áåéç~åçä~äéääéçáå~ååçêç~ååé ïáíüäçå~äéêçíçåçäëiïüáåü~êéä~ëéççåå~íáçå~äöìáçéäáåéëk pq^qrpwnot met Observational audit at the time of pre-transfusion sampling identified that the CHI number was not always being recorded and checked, and that gender was not always recorded on wristbands. A separate wristband audit identified that wristbands were not always in place and that the CHI number was not always present. However, phlebotomy staff reported that if a patient was not wearing a wristband, blood would not be taken and action would be taken to ensure that a wristband was prepared for the patient immediately. Such instances would be reported to the transfusion practitioner who would follow up with the staff involved and provide additional training if necessary. It was reported that there was no single area where this error occurred more frequently than in any other. The audit also demonstrated that sample tubes were being handwritten, the majority at the patient s bedside as per local protocols. The SRI laboratory standard operating procedure for receipt and labelling of transfusion requires a check that the full name, date of birth and CHI number on the sample match those on the request form, however, a check on gender is not included. When a sample is not adequately labelled, or there is a discrepancy between the sample and the request form, a sample error log book is completed by laboratory staff. Minor amendments can be rectified and an amendment form completed and attached to the request form, otherwise a fresh sample is requested. If any one person is identified as persistently making errors then the transfusion practitioner would be informed and retraining organised. If mislabelled samples are received from GPs for patients who will be attending the PITU, these would be rejected and fresh samples requested. Staff reported that such instances are noted on the laboratory error log and staff now also complete an IR1 form. Such incidents would be reported back to the relevant community health partnership and the review team highlighted this as a strong clinical governance link. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu NV
22 pí~åç~êçoåw`äáåáå~äj~å~öéãéåíómêéjqê~åëñìëáçå pí~åç~êçpí~íéãéåí _äççç~åçääçççåçãéçåéåíéêéëåêáäáåöáëíüéêéëéçåëáäáäáíóçñ~èì~äáñáéçéê~åíáíáçåéêk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ OÅKNW ^ääéêéëåêáéíáçåëñçêääççç~åçääçççåçãéçåéåíë~êéëáöåéçäó~èì~äáñáéç éê~åíáíáçåéêk pq^qrpwmet There is space for the signature of a qualified practitioner on the intravenous fluid prescription chart which is in use throughout NHS Forth Valley. The transfusion care pathway which has been piloted has space for the prescriber s signature. The documentation audit conducted within the PITU demonstrated that all prescriptions were being signed by a qualified practitioner. OÅKOW _äççç~åçääçççåçãéçåéåíéêéëåêáéíáçåëëééåáñówääçççåçãéçåéåííçäé ~ÇãáåáëíÉêÉÇXåìãÄÉêçÑìåáíëEãáääáäáíêÉëáåé~ÉÇá~íêáÅé~íáÉåíëFíçÄÉíê~åëÑìëÉÇX Çìê~íáçåçÑíê~åëÑìëáçåX~åóëéÉÅá~äêÉèìáêÉãÉåíI~åÇ~åóëéÉÅá~äáåëíêìÅíáçåëK pq^qrpwmet Blood and blood component prescriptions specify blood component to be administered, number of units, duration of transfusion and any special requirements and instructions as per the blood transfusion protocol. There are separate transfusion guidelines for neonates and children less than 1 year old which require the prescription to specify volume of blood in millilitres. Special requirements would be entered on the laboratory computer system and would be flagged up each time a unit was requested. There is also a prompt for special requirements and instructions on the new transfusion care pathway. The documentation audit found that prescriptions complied with the requirements of this standard criterion. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OM
23 pí~åç~êçp~w`äáåáå~äj~å~öéãéåíóeçëéáí~äqê~åëñìëáçå i~äçê~íçêó pí~åç~êçpí~íéãéåí i~äçê~íçêóçééê~íáçåëåçãéäóïáíüåìêêéåíêéöìä~íçêóêéèìáêéãéåíëk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ P~KNW ^ääíê~åëñìëáçåä~äçê~íçêáéëïáíüáåíüékepäç~êç~êé~ååêéçáíéçäó`äáåáå~ä m~íüçäçöó^ååêéçáí~íáçåerhfiíçe`m^fçêéèìáî~äéåí~åç~êéåçãéäá~åíïáíüíüé jéçáåáåéë~åçeé~äíüå~êééêççìåíëoéöìä~íçêó^öéååóejeo^fêéèìáêéãéåíëk pq^qrpwnot met The departments of haematology and blood transfusion at FDRI and SRI are accredited by Clinical Pathology Accreditation (UK) Ltd (CPA) and will be reassessed in May The SRI hospital blood bank is scheduled for inspection by the Medicines and Healthcare products Regulatory Agency (MHRA) in the first quarter of A mock inspection has been carried out and a detailed action plan to address the findings is being actively followed through with appropriate resources identified. A service level agreement is in place between NHS Forth Valley and Strathcarron Hospice, Denny, to secure the provision of blood components and related services to a level that satisfies the requirements of the Blood Safety and Quality Regulations Blood and blood components are supplied to Strathcarron Hospice by the SRI blood bank on a named patient basis and the hospice follows the NHS Forth Valley protocols for blood transfusion. Hospice staff are included in the BBTP training provided by the NHS Forth Valley transfusion practitioner. NHS Forth Valley commissions services for NHS patients from Abbey King s Park Hospital, Stirling. At the time of the review visit, a service level agreement had been drafted to assure that these services are compliant with all standards of care (and subsequent updates) as set by both the Care Commission and NHS Quality Improvement Scotland (NHS QIS). The review team encouraged the board to finalise this agreement and to assure themselves that the BBTP training was ongoing in Abbey King s Park Hospital. The review team also encouraged the sharing of transfusion-related documentation including the new transfusion care pathway. The laboratory in Abbey King s Park Hospital is compliant with MHRA requirements. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu ON
24 P~KOW `çãééíéååójä~ëéçíê~áåáåö~åç~ëëéëëãéåíëóëíéãë~êéáåéä~åé~åçíê~áåáåö êéåçêçë~êéã~áåí~áåéçk pq^qrpwmet The mock MHRA inspection identified the need for the implementation of competency-based training and assessment systems and the maintenance of training records. Since the mock inspection, all biomedical scientists working in the blood transfusion laboratory had prepared and completed a competency log and personal training folders were in use. The review team acknowledged this considerable achievement. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OO
25 pí~åç~êçpäw`äáåáå~äj~å~öéãéåíóeçëéáí~äqê~åëñìëáçå i~äçê~íçêó pí~åç~êçpí~íéãéåí mêçåéçìêéë~êéáåéä~åéíççéíáãáëéääçççìëé~åçãáåáãáëéï~ëí~öék kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ PÄKNW mêçíçåçäëéåççêëéçäóíüéeq`~êéáåéä~åéiáååäìçáåöäìíåçíäáãáíéçíçwíüé ã~ñáãìãëìêöáå~äääççççêçéêáåöëåüéçìäéejp_lpfxã~ëëáîéääçççäçëëxã~àçê áååáçéåíëx~åçéãéêöéååóääçççã~å~öéãéåí~êê~åöéãéåíëk pq^qrpwmet The maximum surgical blood ordering schedule (MSBOS) followed at SRI and FDRI is included in the NHS Forth Valley blood transfusion protocol which has been endorsed by the HTC. The review team encouraged the board to consider auditing compliance with this schedule. The review team commended the protocols for massive haemorrhage in use at SRI and FDRI. Staff reported that mock exercises to test the protocols had taken place and the findings were fed back to the HTC which led to an improved protocol. The review team encouraged the board to consider incorporating the blood transfusion laboratory procedures for response to major incidents into the existing major incident protocol. The EBMA were considered satisfactory. The laboratory receives a monthly summary of blood component transactions from SNBTS which is discussed at the hospital transfusion team meetings and at the HTC. It has only recently become possible for the laboratory to track its own wastage rates to various departments, and staff reported that these wastage rates would be monitored by the HTC in the future. PÄKOW qüéêéáë~ëíçåâã~å~öéãéåíëóëíéãíçéäáãáå~íééñåéëëáåîéåíçêó~åçêéçìåé ï~ëíéiëìééçêíéçäó~åáåñçêã~íáçåíéåüåçäçöóefqfëóëíéãk pq^qrpwnot met At the time of the review visit, a paper-based blood stock management system was in use, although it was scheduled to be replaced by a more robust IT system which had already been purchased (Blood Track ). The review team noted that the implementation of the Blood Track system and the associated training programme would present a significant challenge for the board, although implementation would enable more efficient stock management and closer monitoring of blood wastage rates. This would lead to the laboratory being in a position to contribute to the BBTP Scottish Transfusion Epidemiology Database. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OP
26 Standard operating procedures are in place for the emergency issue of O RhD negative blood units and blood stock levels are monitored so that optimal blood usage is achieved and as little as possible wasted by going out of date. At the time of the review visit, there was an MLA dedicated to monitoring the traceability process for the receipt, movement and storage of blood components. PÄKPW fååçää~äçê~íáçåïáíüåäáåáå~äëééåá~äíáéëiä~äçê~íçêóëí~ññé~êíáåáé~íéáå~ìçáíçñ íê~åëñìëáçåáëëìéëk pq^qrpwnot met The board has identified that there is limited audit collaboration between laboratory staff and clinical specialties. This was highlighted by the mock MHRA inspection and has been addressed in the action plan. Traceability compliance data are collected on an ongoing basis, however, the review team encouraged the board to consider incorporating other regular audits into routine laboratory practice, in collaboration with clinical specialties. It was reported that the recently extended membership of the HTC was anticipated to encourage collaborative audit activity and that additional audit resource was being recruited into the laboratory at SRI. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OQ
27 pí~åç~êçq~w`äáåáå~äj~å~öéãéåíó_äççç~åç_äççç `çãéçåéåí`çääéåíáçåi^çãáåáëíê~íáçå~åçjçåáíçêáåö pí~åç~êçpí~íéãéåí mçëáíáîéé~íáéåíáçéåíáñáå~íáçåáëééêñçêãéç~ö~áåëííüéääçççåçãéçåéåí~åç~åó ~ÅÅçãé~åóáåÖÇçÅìãÉåí~íáçå~íÉîÉêóëí~ÖÉçÑíÜÉÅäáåáÅ~äíê~åëÑìëáçåéêçÅÉëëK kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ Q~KNW låäóëí~ññïüçü~îéåçãéäéíéçíüé qmåçåíáåìáåöéçìå~íáçåéêçöê~ããéeçê Éèìáî~äÉåíF~ééêçéêá~íÉíçíÜÉáêêçäÉÅ~åé~êíáÅáé~íÉáåíÜÉÅäáåáÅ~äíê~åëÑìëáçå éêçåéëëk pq^qrpwnot met The NHS Forth Valley blood transfusion protocol states that only medical and nursing/midwifery staff, who have completed BBTP education appropriate to their role, can take part in the transfusion process. The training has to be updated every 2 years. The transfusion practitioner maintains a database which details levels of training received by all staff involved in the clinical transfusion process and is advised when new staff join NHS Forth Valley. The transfusion practitioner delivers induction training for foundation year one (FY1) doctors, registered nurses, midwives, operating department practitioners and nursing auxiliaries. Face-to-face sessions have been conducted for all staff groups involved with the blood transfusion process including senior house officers in accident and emergency, theatre and obstetrics and gynaecology. Some consultant anaesthetists and consultants from obstetrics and gynaecology have also attended the face-to-face sessions, however, within this staff group, the percentage trained is too low to ensure that only BBTP trained staff participate in the transfusion process. Over 90% of nursing staff have received BBTP Level 1: Safe Transfusion Practice training. All phlebotomists have received training in taking a pre-transfusion blood sample. There is a porter dedicated to blood collection and other porters who might be involved have also received BBTP Level 1 training. There are five other BBTP trainers: in the surgical unit; accident and emergency; intensive care area; theatre; and in the renal unit. At the face-to-face sessions, staff are encouraged to utilise the Better Blood Transfusion Continuing Education Programme elearning materials which can be accessed through the OrasGold online recording and assessment system. OrasGold can be accessed by staff who work night shifts and FY1 doctors have to complete Level 1 and 2 training using OrasGold within their first 2 months of commencing in NHS Forth Valley. The postgraduate tutor can check if the FY1s have completed the required modules by accessing the NHSScotland Doctors Online Training System (DOTS). It was reported that retraining after 2 years was planned içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OR
28 for all staff groups. Training for some staff groups such as porters will continue to be face-to-face, although the majority will be using OrasGold. The lead clinician for blood transfusion delivers induction training to the foundation year two doctors and is promoting the completion of BBTP Level 1 training using OrasGold to all senior medical staff. The lead clinician is being assisted with this by the NHS Forth Valley medical director and a proposal to include a check that this has been completed at annual appraisal is under consideration. Participation in the SNBTS Trainers and Assessors Accreditation Programme is under way and NHS Forth Valley will participate in a pilot of a competency-based assessment tool for the collection of blood and blood components in early The percentage of BBTP trained staff, with the exception of the senior medical staff, is very high and was commended by the review team. Q~KOW qüéãáåáãìãáçéåíáñáå~íáçåç~í~ëéíáëêéåçêçéççå~ääíê~åëñìëáçåççåìãéåí~íáçå EëÉÉëí~åÇ~êÇÅêáíÉêáçåNÅKNFK pq^qrpwnot met The NHS Forth Valley blood transfusion protocol requires the minimum identification data set (full name, date of birth, gender and CHI or other acceptable unique identifier) to be used on all transfusion-related documentation. Observational audit has, however, shown that wristbands do not always include the CHI number or patient gender. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OS
29 pí~åç~êçqäw`äáåáå~äj~å~öéãéåíó_äççç~åç_äççç `çãéçåéåí`çääéåíáçåi^çãáåáëíê~íáçå~åçjçåáíçêáåö pí~åç~êçpí~íéãéåí m~íáéåíë~êéãçåáíçêéçñçê~åó~çîéêëééîéåíëçêêé~åíáçåëçìêáåö~åç~ñíéêíüé íê~åëñìëáçåéêçåéëë~ëåäáåáå~ääóáåçáå~íéçk kepcçêíüs~ääéó bëëéåíá~ä`êáíéêá~ QÄKNW m~íáéåíë~êéãçåáíçêéç~ååçêçáåöíçüçëéáí~äíê~åëñìëáçåéçäáåó~åç~åóìåíçï~êç ÉîÉåíëEáåÅäìÇáåÖëìëéÉÅíÉÇ~ÇîÉêëÉêÉ~ÅíáçåëF~êÉáããÉÇá~íÉäóÅäáåáÅ~ääó ã~å~öéç~åçéêçãéíäóêééçêíéçíçíüéeqik pq^qrpwnot met The NHS Forth Valley blood transfusion protocol states that baseline recording of temperature, pulse, respirations and blood pressure should be done before the start of transfusion of each unit. Temperature and pulse should then be measured and recorded at 15 and 30 minutes after the start of the transfusion and hourly thereafter until the end of the transfusion episode. The new transfusion pathway specifies the same baseline set of observations as the protocol, however, the pathway states that respirations must be recorded 15 and 30 minutes after the start of transfusion, in addition to temperature and pulse. Observational audit of transfusion episodes indicated that the blood transfusion protocol was not always being followed, and that temperature and pulse were not always being monitored pre-transfusion. Documentation audit also found that the monitoring observations were not always being documented in accordance with the protocol. Staff confirmed that flow charts for the management of severe acute reactions are clearly displayed in all clinical areas and include a step to promptly report these reactions to the hospital laboratory. QÄKOW péêáçìë~çîéêëééîéåíë~åçåé~êãáëëáååáçéåíë~êéêééçêíéççåíüéåäáåáå~ä áååáçéåíêééçêíáåöëóëíéãáå~ååçêç~ååéïáíüäçå~äéêçíçåçäëk pq^qrpwmet The review team noted the clarity of the posters notifying staff that serious adverse blood events and serious adverse blood reactions should be recorded on an IR1 as well as by telephone to the transfusion practitioner. There was clear documentation to support the process of reporting adverse events and near miss incidents in accordance with local protocols. The transfusion practitioner follows up investigations with individuals involved and delivers additional training if required. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OT
30 The transfusion practitioner also reports the outcome of the investigations to managers or educational supervisors. QÄKPW oééçêíëçñëéêáçìë~çîéêëééîéåíëçêêé~åíáçåë~åçåé~êãáëëáååáçéåíë~êé ëìäãáííéçíçpéêáçìë^çîéêëé_äçççoé~åíáçåë~åçbîéåíëep^_obf~åçíüépéêáçìë e~ò~êçëçñqê~åëñìëáçåepelqfáåáíá~íáîéäóíüéêéäéî~åíëí~ññk pq^qrpwmet There is an NHS Forth Valley SABRE reporting group which includes the lead clinician for transfusion, the transfusion practitioner, the blood bank manager, laboratory manager and a biomedical scientist. Each member of the group has password protected access to report to the SHOT initiative via the SABRE reporting system. içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OU
31 içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu OV ^éééåçáñnódäçëë~êóçñ~ääêéîá~íáçåë ^ÄÄêÉîá~íáçå _^op ÄäççÇ~ìÇáíêÉäÉ~ëÉëóëíÉã qm _ÉííÉê_äççÇqê~åëÑìëáçåmêçÖê~ããÉ `d` ÅäáåáÅ~äÖçîÉêå~åÅÉÅçããáííÉÉ `ef `çããìåáíóeé~äíüfåçéñ `m^ `äáåáå~äm~íüçäçöó^ååêéçáí~íáçåerhfiíç alqp açåíçêëlåäáåéqê~áåáåöpóëíéã b_j^ ÉãÉêÖÉåÅóÄäççÇã~å~ÖÉãÉåí~êê~åÖÉãÉåíë caof c~äâáêâcaáëíêáåíoçó~äfåñáêã~êó cvn ÑçìåÇ~íáçåóÉ~êçåÉ dm ÖÉåÉê~äéê~ÅíáíáçåÉê eq` Üçëéáí~äíê~åëÑìëáçåÅçããáííÉÉ fq áåñçêã~íáçåíéåüåçäçöó jeo^ jéçáåáåéë~åçeé~äíüå~êééêççìåíëoéöìä~íçêó^öéååó ji^ ãéçáå~ää~äçê~íçêó~ëëáëí~åí jp_lp ã~ñáãìãëìêöáå~äääççççêçéêáåöëåüéçìäé kepnfp kepnì~äáíófãéêçîéãéåípåçíä~åç mfqr éêçöê~ããéçáåîéëíáö~íáçå~åçíêé~íãéåíìåáí p^_ob péêáçìë^çîéêëé_äçççoé~åíáçåë pelq péêáçìëe~ò~êçëçñqê~åëñìëáçå pk_qp påçííáëük~íáçå~ä_äçççqê~åëñìëáçåpéêîáåé pof píáêäáåöoçó~äfåñáêã~êó tlp_qp téëíçñpåçíä~åç_äçççqê~åëñìëáçåpéêîáåé



32 ^éééåçáñoóoéîáéïéêçåéëë içå~äoééçêíekepcçêíüs~ääéófw_äçççqê~åëñìëáçåój~óommu PM
NHS Grampian. Local Report ~ March Blood Transfusion
 NHS Grampian Local Report ~ March 2008 Blood Transfusion kepdê~ãéá~å içå~äoééçêíúj~êåüommu _äçççqê~åëñìëáçå içå~äoééçêíekepdê~ãéá~åfw_äçççqê~åëñìëáçåój~êåüommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Grampian Local Report ~ March 2008 Blood Transfusion kepdê~ãéá~å içå~äoééçêíúj~êåüommu _äçççqê~åëñìëáçå içå~äoééçêíekepdê~ãéá~åfw_äçççqê~åëñìëáçåój~êåüommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Fife. Local Report ~ July Blood Transfusion
 NHS Fife Local Report ~ July 2008 Blood Transfusion kepcáñé içå~äoééçêíúgìäóommu _äçççqê~åëñìëáçå içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
NHS Fife Local Report ~ July 2008 Blood Transfusion kepcáñé içå~äoééçêíúgìäóommu _äçççqê~åëñìëáçå içå~äoééçêíekepcáñéfw_äçççqê~åëñìëáçåógìäóommu O kepnì~äáíófãéêçîéãéåípåçíä~åçekepnfpfáëåçããáííéçíçéèì~äáíó~åççáîéêëáíók
Blood Transfusion Policy. Version Number: 6.1 Controlled Document Sponsor: Controlled Document Lead: On: December 2014.
 Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
JOB DESCRIPTION. Specialist Practitioner of Transfusion for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:-
 JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
NHS Ayrshire & Arran. Local Report ~ July Healthcare Services for People with Learning Disabilities
 NHS Ayrshire & Arran Local Report ~ July 2009 Healthcare Services for People with Learning Disabilities kep^óêëüáêéc^êê~å içå~äoééçêíúgìäóommv eé~äíüå~êépéêîáåéëñçêméçéäé ïáíüié~êåáåöaáë~äáäáíáéë içå~äoééçêíekep^óêëüáêéc^êê~åfweé~äíüå~êépéêîáåéëñçêméçéäéïáíüié~êåáåöaáë~äáäáíáéëógìäóommv
NHS Ayrshire & Arran Local Report ~ July 2009 Healthcare Services for People with Learning Disabilities kep^óêëüáêéc^êê~å içå~äoééçêíúgìäóommv eé~äíüå~êépéêîáåéëñçêméçéäé ïáíüié~êåáåöaáë~äáäáíáéë içå~äoééçêíekep^óêëüáêéc^êê~åfweé~äíüå~êépéêîáåéëñçêméçéäéïáíüié~êåáåöaáë~äáäáíáéëógìäóommv
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Trust Policy for Blood Transfusion
 Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
REPORT OF BLOOD SAFETY REVIEW
 REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
Clinical Standards ~ September Blood Transfusion
 Clinical Standards ~ September 2006 Blood Transfusion NHS Quality Improvement Scotland 2006 ISBN 1-84404-427-0 First published September 2006 You can copy or reproduce the information in this document
Clinical Standards ~ September 2006 Blood Transfusion NHS Quality Improvement Scotland 2006 ISBN 1-84404-427-0 First published September 2006 You can copy or reproduce the information in this document
Royal Wolverhampton Hospitals NHS Trust. Job Description Haematology
 Royal Wolverhampton Hospitals NHS Trust Job Description Haematology Job Title: Grade: A4C Band 3 (Point 7) Directorate: Pathology Department: Haematology Reports to: BMS staff and section senior Professionally
Royal Wolverhampton Hospitals NHS Trust Job Description Haematology Job Title: Grade: A4C Band 3 (Point 7) Directorate: Pathology Department: Haematology Reports to: BMS staff and section senior Professionally
Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study)
") Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study) SUMMARY REPORT CEPS Project Number: 99/16 Grant-holder: Professor
Quality Improvement Programme: Safe and Effective Transfusion in Scottish Hospitals The Role of the Transfusion Nurse Specialist (SAET Study) SUMMARY REPORT CEPS Project Number: 99/16 Grant-holder: Professor
NHS Borders. Local Report ~ November Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services
 NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
Competency Framework for the Administration of all Blood Products
 Framework for the Administration of all Blood Products Ref No. Authors Others Consulted during preparation Date Created December 2006 Date reviewed March 2007 Date approved Implementation date April 2007
Framework for the Administration of all Blood Products Ref No. Authors Others Consulted during preparation Date Created December 2006 Date reviewed March 2007 Date approved Implementation date April 2007
NPSA Alert 03: Reducing the harm caused by oral Methotrexate. Implementation Progress Report July Learning and Sharing
 NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
SUBJECT: CLINICAL GOVERNANCE
 Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Blood / Blood Products Transfusion A Liquid Transplant
 Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
Policy for Patient Identification. Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead:
 CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear guidance on the use of irradiated blood products.
 Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services
 Scottish Ambulance Service Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services Scottish Ambulance Service Local Report ~ November
Scottish Ambulance Service Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services Scottish Ambulance Service Local Report ~ November
Medicines Management Strategy
 Medicines Management Strategy 2012 2014 Directorate responsible for the strategy: Medical and Governance Directorate Staff group to whom it applies: All clinical staff and Trust managers Issue date: 30/6/12
Medicines Management Strategy 2012 2014 Directorate responsible for the strategy: Medical and Governance Directorate Staff group to whom it applies: All clinical staff and Trust managers Issue date: 30/6/12
Patient Blood Management An Overview. Denise Watson Patient Blood Management Practitioner 11 th January, 2016
 Patient Blood Management An Overview Denise Watson Patient Blood Management Practitioner 11 th January, 2016 What is PBM? An evidence-based, multidisciplinary team approach to optimising the care of patients
Patient Blood Management An Overview Denise Watson Patient Blood Management Practitioner 11 th January, 2016 What is PBM? An evidence-based, multidisciplinary team approach to optimising the care of patients
Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds
 Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds Springburn Glasgow G21 3US Telephone: 0141 531 1355 Inspected
Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds Springburn Glasgow G21 3US Telephone: 0141 531 1355 Inspected
ANTI-COAGULATION MONITORING
 ANTI-COAGULATION MONITORING 2016-17 a) Purpose of Agreement This Agreement outlines the service to be provided by the Provider, called an Anti-coagulation monitoring service. b) Duration of Agreement This
ANTI-COAGULATION MONITORING 2016-17 a) Purpose of Agreement This Agreement outlines the service to be provided by the Provider, called an Anti-coagulation monitoring service. b) Duration of Agreement This
Guidance for MRC units on HTA licence applications for storage of human samples for research purposes
 Guidance for MRC units on HTA licence applications for storage of human samples for research purposes Summary In England, Wales and Northern Ireland the Human Tissue Authority (HTA) is licensing premises
Guidance for MRC units on HTA licence applications for storage of human samples for research purposes Summary In England, Wales and Northern Ireland the Human Tissue Authority (HTA) is licensing premises
A Guide To Safe Blood Transfusion Practice
 A Guide To Safe Blood Transfusion Practice Introduction To Blood Transfusion Safety Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team)
A Guide To Safe Blood Transfusion Practice Introduction To Blood Transfusion Safety Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team)
Right Patient Right Blood Monitoring Compliance Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Right Patient Right Blood Monitoring Compliance Reference Number: NHSCT/12/579 Target audience: This policy is directed to
This is an official Northern Trust policy and should not be edited in any way Right Patient Right Blood Monitoring Compliance Reference Number: NHSCT/12/579 Target audience: This policy is directed to
Changes in practice and organisation surrounding blood transfusion in NHS trusts in England
 See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
Better Blood Transfusion & anti-d Immunoglobulin
 Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
Safe Blood Transfusion
 Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
Handover of Care (Maternity) Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval
 Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval") Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
NHS Summary Care Record. Guide for GP Practice Staff
 NHS Summary Care Record Guide for GP Practice Staff NHS Summary Care Record Guide for GP Practice Staff v1.2 October 2012 Table of Contents 1 Introduction to this guide...3 2 Overview of the Summary Care
NHS Summary Care Record Guide for GP Practice Staff NHS Summary Care Record Guide for GP Practice Staff v1.2 October 2012 Table of Contents 1 Introduction to this guide...3 2 Overview of the Summary Care
Ashfield Healthcare Nurse Agency Ashfield House Resolution Road Ashby-de-la-Zouch LE65 1HW
 Ashfield Healthcare Nurse Agency Ashfield House Resolution Road Ashby-de-la-Zouch LE65 1HW Inspected by: Amanda Cross Type of inspection: Unannounced Inspection completed on: 27 May 2014 Contents Page
Ashfield Healthcare Nurse Agency Ashfield House Resolution Road Ashby-de-la-Zouch LE65 1HW Inspected by: Amanda Cross Type of inspection: Unannounced Inspection completed on: 27 May 2014 Contents Page
Laboratory Request Form Completion and Specimen Labelling Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Laboratory Request Form Completion and Specimen Labelling Reference Number: NHSCT/12/582 Target audience: This policy is directed
This is an official Northern Trust policy and should not be edited in any way Laboratory Request Form Completion and Specimen Labelling Reference Number: NHSCT/12/582 Target audience: This policy is directed
Assessment criteria for obtaining a venous blood sample
 Core blood competencies assessment framework Assessment criteria for obtaining a venous blood sample This framework is for assessing the candidates ability in obtaining a venous blood sample for transfusion.
Core blood competencies assessment framework Assessment criteria for obtaining a venous blood sample This framework is for assessing the candidates ability in obtaining a venous blood sample for transfusion.
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
European network of paediatric research (EnprEMA)
") 17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
17 February 2012 EMA/77450/2012 Human Medicines Development and Evaluation Recognition criteria for self assessment The European Medicines Agency is tasked with developing a European paediatric network
NHSLA Risk Management Standards
 NHSLA Risk Management Standards 2012-13 for NHS Trusts providing Acute Services Brighton and Sussex University Hospitals NHS Trust Level 1 October 2012 Contents Executive Summary... 3 Assessment Outcome...
NHSLA Risk Management Standards 2012-13 for NHS Trusts providing Acute Services Brighton and Sussex University Hospitals NHS Trust Level 1 October 2012 Contents Executive Summary... 3 Assessment Outcome...
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK
 PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
JOB DESCRIPTION. 2. To participate in the delivery of medicines administration depending on local need and priorities.
 JOB DESCRIPTION JOB TITLE: Clinical Pharmacy Technician PAY BAND: 5 DEPARTMENT/DIVISION: BASED AT: REPORTS TO: PHARMACY/A5 University Hospitals Birmingham Pharmacy Support Manager PROFESSIONALLY RESPONSIBLE
JOB DESCRIPTION JOB TITLE: Clinical Pharmacy Technician PAY BAND: 5 DEPARTMENT/DIVISION: BASED AT: REPORTS TO: PHARMACY/A5 University Hospitals Birmingham Pharmacy Support Manager PROFESSIONALLY RESPONSIBLE
Administration of blood components. Denise Watson Patient Blood Management Practitioner 11th January, 2016
 Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Internal Audit. Public Dental Service Accounts Receivable. December 2015
 December 2015 Report Assessment A A A A A This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
December 2015 Report Assessment A A A A A This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report. Results for July Dec 2016
 NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
Unannounced Theatre Inspection Report
 Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Electronic Blood Tracking System
 Electronic Blood Tracking System Case Study Written by Catherine McEvoy 1 P a g e Introduction Over 1,000 people receive transfusions every week in Ireland. This represents a substantial amount of blood
Electronic Blood Tracking System Case Study Written by Catherine McEvoy 1 P a g e Introduction Over 1,000 people receive transfusions every week in Ireland. This represents a substantial amount of blood
ACCESS TO HEALTH RECORDS POLICY & PROCEDURE
 ACCESS TO HEALTH RECORDS POLICY & PROCEDURE Document Number 2009/45 Version 3 Document Title Access to Health Records Policy & Procedure Author Karl Perryman Author s Job Title Head of Legal Services Department
ACCESS TO HEALTH RECORDS POLICY & PROCEDURE Document Number 2009/45 Version 3 Document Title Access to Health Records Policy & Procedure Author Karl Perryman Author s Job Title Head of Legal Services Department
Visit to Hull & East Yorkshire Hospitals NHS Trust
 Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
2015 Survey of Patient Blood Management (PBM)
") 2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
MSK AHP REFERRAL HUB (ADMIN)
") This SOP supersedes all previous versions. Review Interval: Quarterly until further notice Prepared by: Name Ruth Currie Senga Cree Job Title Acting Physiotherapy MSK Manager Head and Professional Lead
This SOP supersedes all previous versions. Review Interval: Quarterly until further notice Prepared by: Name Ruth Currie Senga Cree Job Title Acting Physiotherapy MSK Manager Head and Professional Lead
Date ratified November Review Date November This Policy supersedes the following document which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
Policy Summary. Policy Title: Policy and Procedure for Clinical Coding
 Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
Policy Title: Policy and Procedure for Clinical Coding Reference and Version No: IG7 Version 6 Author and Job Title: Caroline Griffin Clinical Coding Manager Executive Lead - Chief Information and Technology
2015 Survey of Patient Blood Management (PBM)
") 2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
2015 Survey of Patient Blood Management (PBM) This is the second national Patient Blood Management (PBM) survey. In 2013 you were invited to participate in the first PBM survey which provided valuable
Intra-operative Cell Salvage. Competency Assessment Workbook. Trainee: Hospital: Trainer/Supervisor: Date Commenced: Date Completed:
 Intra-operative Cell Salvage Competency Assessment Workbook Trainee: Hospital: Trainer/Supervisor: Commenced: Completed: Contents Introduction 1-2 Record of Assessors 4 Confirmation of Required Pre-assessment
Intra-operative Cell Salvage Competency Assessment Workbook Trainee: Hospital: Trainer/Supervisor: Commenced: Completed: Contents Introduction 1-2 Record of Assessors 4 Confirmation of Required Pre-assessment
NES Patient Safety Programme. Human Factors in Healthcare. NES Educational Developments and Resources
 NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
HAEMOVIGILANCE. Ms. Emma O Riordan Haemovigilance, CNM2 (Acting) Ms. Bríd Doyle, MSc. FAMLS. Haemovigilance Co-ordinator, (Acting)
 Ms. Bríd Doyle, MSc. FAMLS. Haemovigilance Co-ordinator, (Acting)") HAEMOVIGILANCE a set of surveillance procedures covering the whole transfusion chain from the collection of blood and its components to the follow-up of its recipients, intended to collect and assess information
HAEMOVIGILANCE a set of surveillance procedures covering the whole transfusion chain from the collection of blood and its components to the follow-up of its recipients, intended to collect and assess information
Competency Assessment for Non Medical Prescribing of Blood and Blood Components
 Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
62 days from referral with urgent suspected cancer to initiation of treatment
 Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM
 Mid-West Area Hospitals Page 1 of 5 Edition No.: 01 PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM EDITION No 01 EFFECTIVE DATE 5 th February 2013 REVIEW INTERVAL
Mid-West Area Hospitals Page 1 of 5 Edition No.: 01 PROCEDURE FOR TAKING AND LABELLING A TRANSFUSION SAMPLE AND COMPLETING THE REQUEST FORM EDITION No 01 EFFECTIVE DATE 5 th February 2013 REVIEW INTERVAL
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Job Description. TDL Laboratory Staff, Clients and Customers, Group Blood Transfusion Manager
 Job Description Job Title: Location: Reporting to: Accountable to: Liaises with: Senior Biomedical Scientist (Blood Transfusion) BMI London Independent Pathology Lead Group Laboratory Director Regional
Job Description Job Title: Location: Reporting to: Accountable to: Liaises with: Senior Biomedical Scientist (Blood Transfusion) BMI London Independent Pathology Lead Group Laboratory Director Regional
NON-MEDICAL PRESCRIBING POLICY
 NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
Highland Care Agency Ltd Nurse Agency 219 Colinton Road Edinburgh EH14 1DJ
 Highland Care Agency Ltd Nurse Agency 219 Colinton Road Edinburgh EH14 1DJ Type of inspection: Unannounced Inspection completed on: 30 April 2015 Contents Page No Summary 3 1 About the service we inspected
Highland Care Agency Ltd Nurse Agency 219 Colinton Road Edinburgh EH14 1DJ Type of inspection: Unannounced Inspection completed on: 30 April 2015 Contents Page No Summary 3 1 About the service we inspected
Report by Margaret Brown, Head of Service Planning & Donna Smith, Divisional General Manager, Patient Services, Raigmore
 Highland NHS Board 4 June 2013 Item 5.4 NHS HIGHLAND REVISED LOCAL ACCESS POLICY Report by Margaret Brown, Head of Service Planning & Donna Smith, Divisional General Manager, Patient Services, Raigmore
Highland NHS Board 4 June 2013 Item 5.4 NHS HIGHLAND REVISED LOCAL ACCESS POLICY Report by Margaret Brown, Head of Service Planning & Donna Smith, Divisional General Manager, Patient Services, Raigmore
HYWEL DDA LOCAL HEALTH BOARD. Transfusion Policy. Completed Action: Addresses all aspects of transfusion with blood and blood components
 Policy Number: 278 Supersedes: Standards For Healthcare Services No/s Version No: 1 Date Of Review: Reviewer Name: Completed Action: Approved by: Date Approved: New Review Date: Brief Summary of Document:
Policy Number: 278 Supersedes: Standards For Healthcare Services No/s Version No: 1 Date Of Review: Reviewer Name: Completed Action: Approved by: Date Approved: New Review Date: Brief Summary of Document:
Core competencies for the care of acutely ill and injured children and young people. May 2006
 Core competencies for the care of acutely ill and injured children and young people May 2006 Contents Introduction 3 How the competencies can be used 6 Core competencies : Assessment domain 7 Core competencies
Core competencies for the care of acutely ill and injured children and young people May 2006 Contents Introduction 3 How the competencies can be used 6 Core competencies : Assessment domain 7 Core competencies
Quality Manual. Folder One
 Section: Front page Bowel Screening Wales Quality Manual Folder One Version 2.0 If printed, this document is only valid for today 05 Page 1 of Section: Contents 1. Introduction... 4 2. Aim and Scope of
Section: Front page Bowel Screening Wales Quality Manual Folder One Version 2.0 If printed, this document is only valid for today 05 Page 1 of Section: Contents 1. Introduction... 4 2. Aim and Scope of
Resuscitation Training Policy
 Resuscitation Training Policy Approved by & date HMB 12 November 2003 Date of Publication February 2003 Review date February 2005 Creator & telephone details Christopher Gabel, Senior Resuscitation Officer
Resuscitation Training Policy Approved by & date HMB 12 November 2003 Date of Publication February 2003 Review date February 2005 Creator & telephone details Christopher Gabel, Senior Resuscitation Officer
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE
 POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated Click Here
 Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated 2014 Click Here Promoting Effective Immunisation Practice Published Summer 2014 NHS Education for Scotland
Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated 2014 Click Here Promoting Effective Immunisation Practice Published Summer 2014 NHS Education for Scotland
Best Practice Statement ~ March Patient Group Directions
 Best Practice Statement ~ March 2006 Patient Group Directions NHS Quality Improvement Scotland 2005 ISBN 1-84404-403-3 First published March 2006 NHS Quality Improvement Scotland (NHS QIS) consents to
Best Practice Statement ~ March 2006 Patient Group Directions NHS Quality Improvement Scotland 2005 ISBN 1-84404-403-3 First published March 2006 NHS Quality Improvement Scotland (NHS QIS) consents to
Health Department Directorate of Finance NHS HDL (2000)02
02") Health Department Directorate of Finance NHS HDL (2000)02 Dear Colleague CLINICAL NEGLIGENCE AND OTHER RISKS INDEMNITY SCHEME (CNORIS): AMENDMENT REGULATIONS AND SCHEME STANDARDS Purpose 1. This HDL provides
Health Department Directorate of Finance NHS HDL (2000)02 Dear Colleague CLINICAL NEGLIGENCE AND OTHER RISKS INDEMNITY SCHEME (CNORIS): AMENDMENT REGULATIONS AND SCHEME STANDARDS Purpose 1. This HDL provides
Patient Blood Management Certification Revisions
 Issued October 3, 07 Patient Blood Management Certification Revisions Patient Blood Management (PBM) Certification Program Assessments: Internal and External (PBMAM) Chapter Standard PBMAM. The program
Issued October 3, 07 Patient Blood Management Certification Revisions Patient Blood Management (PBM) Certification Program Assessments: Internal and External (PBMAM) Chapter Standard PBMAM. The program
Unannounced Follow-up Inspection Report: Independent Healthcare
 Unannounced Follow-up Inspection Report: Independent Healthcare St Vincent s Hospice St Vincent s Hospice Limited 28 www.healthcareimprovementscotland.org Healthcare Improvement Scotland is committed to
Unannounced Follow-up Inspection Report: Independent Healthcare St Vincent s Hospice St Vincent s Hospice Limited 28 www.healthcareimprovementscotland.org Healthcare Improvement Scotland is committed to
Serious Adverse Event Report 1 July June 2015
 Serious Adverse Event Report 1 July 2014 30 June 2015 Category Brief description Main findings There were no clear gaps in care delivery identified, but there were a Falls Unwitnessed patient fall resulting
Serious Adverse Event Report 1 July 2014 30 June 2015 Category Brief description Main findings There were no clear gaps in care delivery identified, but there were a Falls Unwitnessed patient fall resulting
Heading. Safeguarding of Children and Vulnerable Adults in Mental Health and Learning Disability Hospitals in Northern Ireland
 Place your message here. For maximum impact, use two or three sentences. Heading Safeguarding of Children and Vulnerable Adults in Mental Health and Learning Disability Hospitals in Northern Ireland Follow
Place your message here. For maximum impact, use two or three sentences. Heading Safeguarding of Children and Vulnerable Adults in Mental Health and Learning Disability Hospitals in Northern Ireland Follow
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
NHS Lanarkshire. Local Report ~ November Stroke Services: Care of the Patient in the Acute Setting
 NHS Lanarkshire Local Report ~ November 2005 Stroke Services: Care of the Patient in the Acute Setting NHSScotland Regional Breakdown 13 12 15 1 NHS Argyll & Clyde 2 NHS Ayrshire & Arran 3 NHS Borders
NHS Lanarkshire Local Report ~ November 2005 Stroke Services: Care of the Patient in the Acute Setting NHSScotland Regional Breakdown 13 12 15 1 NHS Argyll & Clyde 2 NHS Ayrshire & Arran 3 NHS Borders
abcdefghijklmnopqrstu
 Directorate of Chief Medical Officer, Public Health and Sport abcdefghijklmnopqrstu T: 0131-244 2655 F: 0131-244 2285 E: craig.gilbert@scotland.gsi.gov.uk Dear Colleague ACCREDITATION SCHEME FOR THE COLLECTION
Directorate of Chief Medical Officer, Public Health and Sport abcdefghijklmnopqrstu T: 0131-244 2655 F: 0131-244 2285 E: craig.gilbert@scotland.gsi.gov.uk Dear Colleague ACCREDITATION SCHEME FOR THE COLLECTION
Aneurin Bevan Health Board. Improving Theatre Performance
 Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
BLOOD TRANSFUSION POLICY
 Title: BLOOD TRANSFUSION POLICY Ref: 0219 Version 11 Classification: Guideline Directorate: Laboratory Medicine Due for Review: 15/12/2020 Document Control Responsible Consultant Haematologist and Transfusion
Title: BLOOD TRANSFUSION POLICY Ref: 0219 Version 11 Classification: Guideline Directorate: Laboratory Medicine Due for Review: 15/12/2020 Document Control Responsible Consultant Haematologist and Transfusion
Register No: Status: Public on ratification
 Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
COMMUNITY PHARMACY MINOR AILMENTS SERVICE
 COMMUNITY PHARMACY MINOR AILMENTS SERVICE SUPPORTING SELF-CARE OCTOBER 2010 CONTENTS Index Page No 1 Introduction 3 2 Service Specification 4 3 Consultation Procedure 7 4 Re-ordering Documentation 10 Appendices
COMMUNITY PHARMACY MINOR AILMENTS SERVICE SUPPORTING SELF-CARE OCTOBER 2010 CONTENTS Index Page No 1 Introduction 3 2 Service Specification 4 3 Consultation Procedure 7 4 Re-ordering Documentation 10 Appendices
Policy Register No: Status: Public NURSING STAFFING SHORTFALL ESCALATION POLICY. NICE Guidelines July 2014 CQC Fundamental Standards: 17
 NURSING STAFFING SHORTFALL ESCALATION POLICY Policy Register No: 09114 Status: Public Developed in response to: National Quality Board Recommendations2013 NICE Guidelines July 2014 CQC Fundamental Standards:
NURSING STAFFING SHORTFALL ESCALATION POLICY Policy Register No: 09114 Status: Public Developed in response to: National Quality Board Recommendations2013 NICE Guidelines July 2014 CQC Fundamental Standards:
Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards
 Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards Dr Steve Cross Human Reliability Dr Guro Huby University of Edinburgh Commissioned
Longer Term Impact of NHS QIS Peer Review Visits: Continuous Quality Improvement of Blood Transfusion Services in NHS Boards Dr Steve Cross Human Reliability Dr Guro Huby University of Edinburgh Commissioned
The document has been issued to:- Name Position Department Date
 VALIDATION PROTOCOL PARTICIPANTS: Validation of Traceability / Return Label VALIDATION REF # Prepared by: The document has been
VALIDATION PROTOCOL PARTICIPANTS: Validation of Traceability / Return Label VALIDATION REF # Prepared by: The document has been
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
Standard 1: Governance for Safety and Quality in Health Service Organisations
 Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
Systemic Anti-Cancer Therapy Delivery. June 2017 National External Review
 Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
NHS GREATER GLASGOW AND CLYDE POLICIES RELATING TO THE MANAGEMENT OF MEDICINES SECTION 9.1: UNLICENSED MEDICINES POLICY (ACUTE DIVISION)
") SECTION 9.1: UNLICENSED MEDICINES POLICY (ACUTE DIVISION) CONTENTS POLICY SUMMARY... 2 1. SCOPE... 4 2. AIM... 4 3. BACKGROUND... 4 4. POLICY STATEMENTS... 5 4.1. GENERAL STATEMENTS... 5 4.2 UNLICENSED
SECTION 9.1: UNLICENSED MEDICINES POLICY (ACUTE DIVISION) CONTENTS POLICY SUMMARY... 2 1. SCOPE... 4 2. AIM... 4 3. BACKGROUND... 4 4. POLICY STATEMENTS... 5 4.1. GENERAL STATEMENTS... 5 4.2 UNLICENSED
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
CAUTION: Refer to the Document Library for the most recent version of this policy. Blood Transfusion Policy. Pathology Transfusion.
 Directorate Department Year Version Number Central Index Number Endorsing Committee Date Endorsed Approval Committee Date Approved Author Name and Job Title Key Words (for search purposes) Date Published
Directorate Department Year Version Number Central Index Number Endorsing Committee Date Endorsed Approval Committee Date Approved Author Name and Job Title Key Words (for search purposes) Date Published
FIRST PATIENT SAFETY ALERT FROM NATIONAL PATIENT SAFETY AGENCY (NPSA) Preventing accidental overdose of intravenous potassium
 Preventing accidental overdose of intravenous potassium") abcdefghijklm Health Department St Andrew s House Regent Road Edinburgh EH1 3DG MESSAGE TO: 1. Medical Directors of NHS Trusts 2. Directors of Public Health 3. Specialists in Pharmaceutical Public Health
abcdefghijklm Health Department St Andrew s House Regent Road Edinburgh EH1 3DG MESSAGE TO: 1. Medical Directors of NHS Trusts 2. Directors of Public Health 3. Specialists in Pharmaceutical Public Health
Unannounced Inspection Report. Aberdeen Maternity Hospital NHS Grampian. 9 October 2013
 Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
Unannounced Inspection Report Aberdeen Maternity Hospital NHS Grampian 9 October 2013 The Healthcare Environment Inspectorate is a part of Healthcare Improvement Scotland Healthcare Improvement Scotland
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated Click Here
 Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated 2011 Click Here Promoting Effective Immunisation Practice Published Summer 2011 NHS Education for Scotland
Promoting Effective Immunisation Practice Guide for Students, Mentors and Their Employers Updated 2011 Click Here Promoting Effective Immunisation Practice Published Summer 2011 NHS Education for Scotland
Grampian University Hospitals NHS Trust. Local Report ~ February Older People in Acute Care
 Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway
Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway