Q15. Allan Frankel discloses that he is Managing Partner of Safe and Reliable Healthcare
|
|
|
- Allen Daniel
- 6 years ago
- Views:
Transcription
1 Q15 Allan Frankel discloses that he is Managing Partner of Safe and Reliable Healthcare Understanding & Improving Safety Culture Amelia Brooks, Director, Patient Safety & Europe Region, IHI Allan Frankel, Managing Partner, Safe & Reliable Healthcare Monday December 11 th :30 4:00
2 Disclosure: Safe And Reliable Care (SRH) is a cultural assessment and design group dedicated to the pursuit of perfect care through transformational change. Allan Frankel MD
3 Goals for Today: 1. How do we define safety culture, its attributes and impact? 2. How effective are your team behaviors, and what should they look like to support safety culture? What to do if professionalism or negative behaviors are eroding trust in your organization? 3. How do you create effective middle managers who can run the self-reflecting learning systems to manage change and ensure operational excellence? 4. How do we incorporate safety culture into improvement work? 5. How should senior leaders/board members engage with work settings and with the work setting managers? 6. How to embed just culture your organizations?
4 Let s get to know each other Get to know the person sitting next to you Share your names and something surprising or interesting about yourself not about work! What would you like to get from today? Take 5 mins
5 Defining Safety Culture; Attributes and Impact
6 What does a culture of safety mean to you?




7 What is Safety Culture?





8 A Culture of Safety No one is ever hesitant to voice a concern about a patient Action is taken, feedback reliably provided, changes are visible for staff and patients Skilled caregivers playing by the rules feel safe to discuss and learn from errors Concerns raised by front line caregivers are taken seriously & acted upon
9 What is Culture? How the organization behaves when no one is watching
10 Zero harm to patients and the workforce is only possible with both a robust culture of safety and an embedded organizational learning system. Leading a Culture of Safety: A Blueprint for Success
11 Exercise You are assigned responsibility to evaluate a unit in a healthcare organization. (Unit = Department, Division, Section a delineated group working together) The unit is new to you. You are to evaluate the unit for its ability to achieve safe, reliable, patient-centered operational excellence. What will you assess?

12 A Familiar Framework Personal Habits 1. Risk Factors 2. Exercise 3. Nutrition 4. Health Literacy 5. Etc Physical Exam 1. Cardiovascular 2. Pulmonary 3. Gastrointestinal 4. Musculoskeletal 5. Etc 2010 Pascal Metrics Inc.
13 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Culture Leadership Teamwork & Communication Transparency Engagement of Patients & Family Negotiation Learning System Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel

14 Teamwork and Communication Negotiation Learning System Accountability Leadership Psychological Safety Framework For Safe, Reliable and Effective Care Culture Continuous Learning Improvement and Measurement Reliability Transparency IHI and Allan Frankel
15 Framework for Safe, Reliable, Effective Care Ask Questions. Ask for Feedback. Be Respectfully Critical. Suggest Innovations. Leadership Transparency Psychological Safety Engagement of Patients & Family Accountability Teamwork & Communication Negotiation Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel
16 Framework for Safe, Reliable, Effective Care Leadership Transparency Psychological Safety Engagement of Patients & Family Accountability Teamwork & Communication Negotiation I m accountable for my actions but won t be held accountable for current system flaws. Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel
17 Framework for Safe, Reliable, Effective Care Plan forward. Leadership Psychological Safety Accountability Teamwork & Communication Reflect back. Communicate clearly. Manage risk. Transparency Engagement of Patients & Family Negotiation Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel
18 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Leadership Teamwork & Communication Collaborate grow the pie. Transparency Reliability Engagement of Patients & Family Improvement Continuous Learning Negotiation Know positions from interests. Appreciatively inquiring. & Measurement IHI and Allan Frankel
19 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Leadership Teamwork & Communication Engagement of Patients & Family Transparency Negotiation Reliability Improvement & Measurement Continuous Learning Regularly collecting and learning from defects and successes. IHI and Allan Frankel
20 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Improving work processes and patient outcomes using standard improvement tools including measurements over time. Leadershi p Transparency Reliability Engagement of Patients & Family Improvement & Measurement Teamwork & Communication Continuous Learning Negotiation IHI and Allan Frankel
21 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Applying best evidence and minimizing non-patient specific variation with the goal of failure free operation over time. Leadership Transparency Reliability Engagement of Patients & Family Improvement & Measurement Teamwork & Communication Continuous Learning Negotiation IHI and Allan Frankel
22 Framework for Safe, Reliable, Effective Care Openly sharing data and other information concerning safe, respectful and reliable care with staff and partners and families. Leadership Transparency Reliability Psychological Safety Engagement of Patients & Family Improvement & Measurement Accountability Teamwork & Communication Continuous Learning Negotiation IHI and Allan Frankel
23 Framework for Safe, Reliable, Effective Care Guardians of the Learning System. Exemplars of the Culture. Psychological Safety. Respect. Leadership Transparency Psychological Safety Engagement of Patients & Family Accountability Teamwork & Communication Negotiation Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel
24 Lessons and Behaviors from HROs In HRO interpersonal skills are equally as important as technical expertise Huddles are an opportunity for caregivers other than physicians and nurses to theorize about what is going on with their patients Professional heterogeneity is usually advantageous for collective learning, improving the range, depth and integration of information considered.

25 Balance System and Process Technical People and Culture Non-Technical

26 Legacy James Kerr "Champions do extra. They sweep the sheds. They follow the spearhead. They keep a blue head. They are good ancestors. Legacy goes deep into the heart of the world's most successful sporting team, What are the secrets of success - sustained success? 'Better people make better All Blacks'

27
28 Team Behaviors & Professionalism


29 Teamwork Climate Across Michigan ICUs No BSI = 5 months or more w/ zero No BSI 21% No BSI 31% No BSI 44% The strongest predictor of clinical excellence: caregivers feel comfortable speaking up if they perceive a problem with patient care Attribution Bryan Sexton
30 Consider places you have worked in, or that you have encountered, where: 1. The output is stellar. 2. Employees choose to stay. 3. Outsiders want to join. If you asked workers why the place is special and why they choose to stay what would they say?
31 Improvement Readiness (The Learning System) Knowing the plan - predictability Feeling safe to speak up Knowing that when you do speak up, someone cares and the team will respond appropriately Planning forward / reflecting back through debriefing to feed the Learning System
32 Effective Teamwork GENERATIVE Organization wired for safety and improvement PROACTIVE Playing offense - thinking ahead, anticipating, solving problems SYSTEMATIC Systems in place to manage hazards REACTIVE Playing defense reacting to events UNMINDFUL No awareness of safety culture Teamwork and continuous learning deeply embedded and central to our culture Teamwork methodically taught and modeled across the organization Training and tools available, partial implementation Focus on teamwork awareness / training in response to adverse events If people would just do their jobs we d have no problems
33 Culture and Teamwork team How the organization behaves when no one is watching
34 A Team A group of people working cooperatively towards a shared goal
35 NASA / UT Teamskills Briefing The effective briefing will be operationally thorough, interesting and will address coordination, planning and potential problems. Communication and Decision Reflects the extent to which free and open communication is practiced. Active participation in decisions encouraged. Team Self Feedback The extent to which a team recognises the need to give and receive feedback. Enquiry / Advocacy / Assertion Team members advocate, with appropriate persistence, the course of action they feel is best, even if it involves disagreement. Leadership / Followership / Concern for the Task The extent to which appropriate leadership and followership are practiced.. Interpersonal Relationships / Group Climate Reflects the quality of relationships among the team, the overall climate in the workplace Preparation / Planning / Vigilance Reflects the extent to which teams plan ahead, maintain situation awareness and anticipate contingencies. Workload / Distractions This is a rating of time and workload management. It reflects how the team distributes tasks, avoids overload and distractions.
36 NASA / UT Teamskills Briefing The effective briefing will be operationally thorough, interesting and will address coordination, planning and potential problems. Communication and Decision Reflects the extent to which free and open communication is practiced. Active participation in decisions encouraged. Team Self Feedback The extent to which a team recognises the need to give and receive feedback. Enquiry / Advocacy / Assertion Team members advocate, with appropriate persistence, the course of action they feel is best, even if it involves disagreement. Leadership / Followership / Concern for the Task The extent to which appropriate leadership and followership are practiced.. Interpersonal Relationships / Group Climate Reflects the quality of relationships among the team, the overall climate in the workplace Preparation / Planning / Vigilance Reflects the extent to which teams plan ahead, maintain situation awareness and anticipate contingencies. Workload / Distractions This is a rating of time and workload management. It reflects how the team distributes tasks, avoids overload and distractions.
37 Interpersonal Relationships / Group Climate Reflects the quality of relationships among the team, the overall climate in the workplace What do you do to make a positive contribution? What else could you do?
38 Personality & Behavior 38 Technical and non technical skills Personality is personal Behavior is shared

39 Hierarchy


40 The Authority Gradient Sir Cloudsley Shovell
41 Authority Gradient Pros and Cons of: Steep authority gradient Shallow gradient When each would be useful
42 Approachability Assertiveness What does it look like? What does it look like? How do you make yourself approachable? Intent / Capacity How do you do it? Licence / Capacity / Adult / Language

43 Context Busy Too many things to do Running late Short on sleep Pressure to perform Hungry Angry

44
45 Performance & Culture Demands to Think Out of Control Limit of Capacity In Control Demands to Act Amalberti
46 What Teams Do The associated behaviors: Plan Forward Brief (huddle, pause, timeout, check-in) Reflect Back Debrief Communicate Clearly Structured Communication SBAR and Repeat-Back Manage Conflict Critical Language 46


47 Team Behaviors Where do you think you are in embodying teamwork as described? Debriefing Linking teamwork and Improvement What did we do well? What did we learn so we can do it better the next time? What got in the way that needs to be fixed?
48 Behaviors that undermine a culture of safety Verbal or physical threats Intimidation Reluctance/refusal to answer questions, refusal to answer pages or calls Impatience with questions Condescending language or intonation Jo Shapiro MD, BWH
49 The Aim: Hierarchy of Responsibility No Hierarchy of Respect Jo Shapiro MD, BWH
50
51 Common responses Inadequate data Exactly who said this? Personal sabotage Dr. X is trying to discredit me Other people like me I am special and talented I do work that no one else is qualified to do This is a systems problem If this whole system functioned better Appropriate feedback Not a court of law Not an isolated incident You shouldn t have a disruptive working relationship with anyone Not a performance evaluation Yes, and you still are responsible for your behavior Jo Shapiro MD, BWH
52 Common responses Unfair process I m being singled out because Patient advocacy Others aren t responsible for patients the way I am Prove harm Give me one example Personal style I don t mean anything by it I am no worse than others I am certainly not the only one Appropriate feedback We hold everyone to the same standards Disruptive behavior is a safety risk We don t need to Impact not intent We are focusing on your issues right now Jo Shapiro MD, BWH
53 Reporting Concerns What Should Happen: Confidential discussion with Director Investigation Discussion with supervising leaders/manager Meeting with disruptor Document all interactions Jo Shapiro MD, BWH
54 Your turn: Professionalism What mechanisms exist in your organizations to ensure that professionalism and peer support are effective?
55 Leaders, Managers & Their Role in Improvement & Culture


56 Value Cultural Maturity Model GENERATIVE Safety is how we do business around here Constantly Vigilant and Transparent Tipping Point PROACTIVE Anticipating and preventing problems before they occur; Comfort speaking up REACTIVE Safety is important. We do a lot every time we have an accident SYSTEMATIC We have systems in place to manage all hazards SRH 2017 UNMINDFUL Who cares as long as we re not caught Chronically Complacent *Adapted from Safeskies 2001, Aviation Safety Culture, Patrick Hudson, Centre for Safety Science, Leiden University
57 Senior Leadership GENERATIVE Organization wired for safety and improvement PROACTIVE Playing offense - thinking ahead, anticipating, solving problems SYSTEMATIC Systems in place to manage hazards REACTIVE Playing defense reacting to events UNMINDFUL No awareness of safety culture Cyclic flow of information with feedback and organizational learning Systematic engagement with dialogue, support and learning Process for interaction between senior leaders and front line staff They re here something bad must have happened We don t know or see them
58 Local Leadership GENERATIVE Organization wired for safety and improvement PROACTIVE Playing offense - thinking ahead, anticipating, solving problems SYSTEMATIC Systems in place to manage hazards REACTIVE Playing defense reacting to events UNMINDFUL No awareness of safety culture Leaders create high degrees of psych safety and accountability. Leaders model the desired behaviors to drive culture of safety Training and support exists for building clinical leadership Episodic, completely dependent on the individual clinician Absent for the most part
59 A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System A Healthcare System
60


61 A wide variety of skills across the middle 10% 80% 10% Absent Burned Out Socially Inept Psychopathic Disinterested Source: Bohmer R, Leading Clinicians and Clinicians Leading, New Eng J Med, April 2013 Clinically excellent Well meaning Socially Adept Inadequately Trained Engaged Knowledgeable in: Organizational development Whole system change Measurement to manage Relentlessly focused on process Know culture IS a process

62 Edgar Schein Visible Attributes Espoused vs Demonstrated Values Hidden Values and Tacit Assumptions How we spend our time

63 Question Summarizing Berry: Operational excellence is dependent on volunteerism, the willingness of employees to give above and beyond what they are paid to do. What are the determinants of volunteerism?

 Safety Domain All Items The values of facility leadership are the same values that people in this")
 My suggestions about quality would be acted upon if I expressed them to management.")
 I would feel safe being treated here as a patient.")
64 The Determinants of Volunteerism Alignment of Espoused versus Actual Values Work as Imagined versus Work as Done The values of facility leadership are the same values that people in this work setting think are important. (4167) Safety Domain All Items The values of facility leadership are the same values that people in this work setting think are important. (4167) In this work setting, it is NOT difficult to discuss errors. (4187) My suggestions about quality would be acted upon if I expressed them to management. (4163) Errors are handled appropriately in this work setting (4177) I receive appropriate feedback about my performance. (4176) I would feel safe being treated here as a patient. (4157) The culture in this work setting makes it easy to learn from the errors of others. (4177) Percentage who agreed slightly or agreed strongly with each question.

65 The Determinants of Volunteerism The relationship I have with my direct Supervisor Administrator/Director Manager Supervisor Nursing Technologist Admin Support Learning Environment

66 The Determinants of Operational Excellence Do I have voice? Do my team members care about me?
67 Effective Leaders Create psychological safety Calibrate drift to minimize shortcuts and workarounds Drive effective team performance Model the values and behaviors that create value and reduce risk
? If yes, how, and if not, why? Where are they on the Cultural Maturity Model Curve?")


68 SRH 2017 Your turn: Self-Reflecting Learning Are your Managers, Directors, Chairs and Chiefs etc. consciously aware that they run learning systems (improvement readiness is their primary charge)? If yes, how, and if not, why? Where are they on the Cultural Maturity Model Curve? How culturally varied are your work settings? Learning System Value Framework for Clinical Excellence Psychological Safety Accountability Cultural Maturity Model Culture Leadership Teamwork & Communication Engagement of Patients & Transparency Family Negotiation Reliability Continuous Learning Improvement & Measurement IHI and Allan Frankel GENERATIVE Safety is how we do business around here Constantly Vigilant and Transparent PROACTIVE Tipping Point Anticipating and preventing problems before they occur; Comfort speaking up SYSTEMATIC We have systems in place to manage all hazards REACTIVE Safety is important. We do a lot every time we have an accident UNMINDFUL Who cares as long as we re not caught Chronically Complacent *Adapted from Safeskies 2001, Aviation Safety Culture, Patrick Hudson, Centre for Safety Science, Leiden University


69 A Healthcare System Joint Commission National Patient Safety Foundation (and IHI) Institute for Healthcare Improvement

70 Strategy (ALWAYS focused on Improvement Ready Work Settings.) Education and Org. Development Department Office of Clinical Excellence Office of Professionalism and Peer Support Communication and Marketing Departments IT Prioritization Office
71 Impact of Good Leadership on Survey Data Across Michigan WalkRounds feedback leads to huge improvement in cultural health across all domains of culture. n=16,797 respondents Published 2017 with DUKE: JB Sexton et al, British Medical Journal
72 Impact of Teamwork on the Ability to Improve a Process No BSI 21% No BSI 31% No BSI 44% Cultural health determines the ability to improve clinical processes, quality and outcomes. BSI = Blood Stream Infection from Central Lines NEJM 2004 Pronovost, Sexton
73 Impact of Good Leadership on SCORE Data Across Michigan What this means for an organization that wants to achieve high reliability? No BSI 21% No BSI 31% No BSI 44% WalkRounds feedback leads to huge improvement in cultural health across all domains of culture. n=16,797 respondents IN PUBLICATION with DUKE: JB Sexton et al, British Medical Journal Cultural health determines the ability to improve clinical processes, quality and outcomes. BSI = Blood Stream Infection from Central Lines NEJM 2004 Pronovost, Sexton


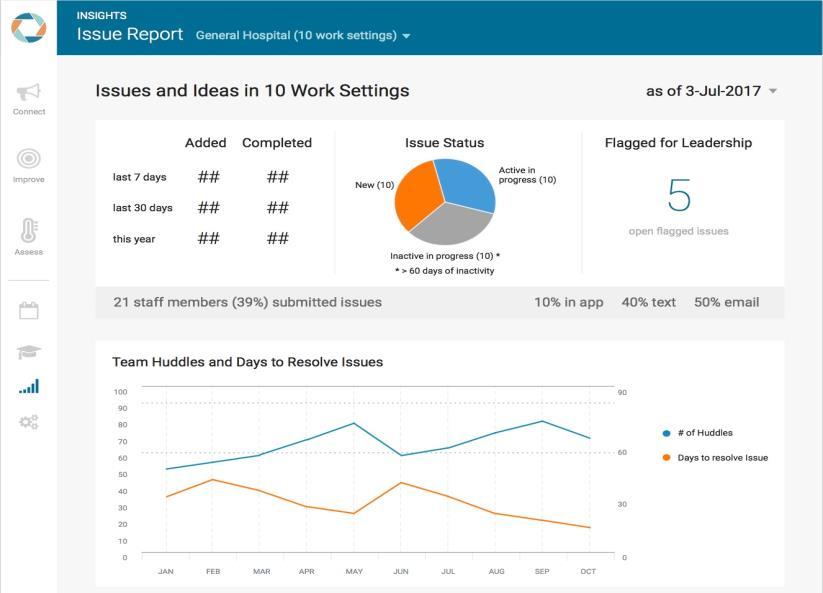
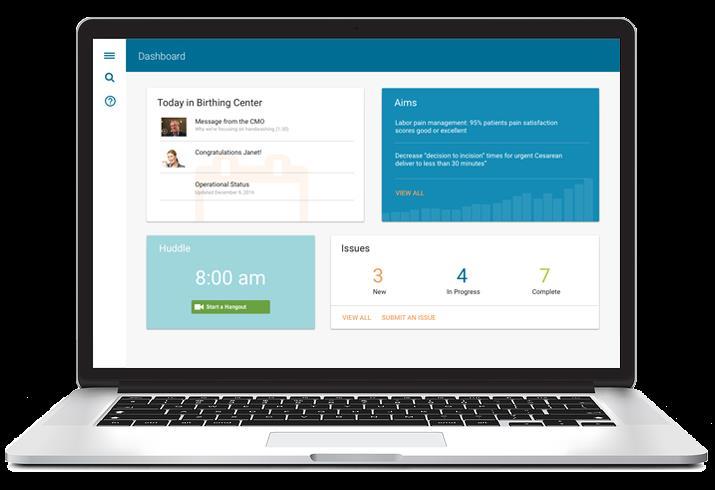
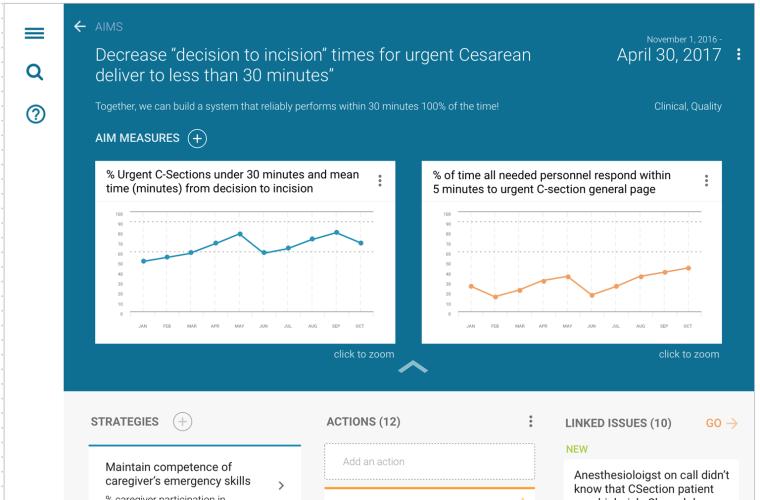
74 Learning boards capture ideas and issues from everyone ANALOG: proven results DIGITAL: available everywhere on any device.

75 Engage: Mayo/SRH TEM Model 50% Adverse Events 1.5 Length of Stay 92% Sustain Method 5yrs Later 13% Engagement Increase


76 Examples: Rounding Maine Medical Center Cincinnati Childrens Hospital

77



78




79 Technology that Enables Culture (The culture we want!)
 Education and Org.")
80 Your turn: Self-Reflecting Learning What is the true north value that drives strategy in your organization? Are you adequately configured to support your work settings as described? Strategy (ALWAYS with Improvement Ready Work Settings at the center.) Education and Org. Development Department Office of Clinical Excellence Office of Professionalism and Peer Support Communication and Marketing Departments IT Prioritization Office Explain your answer?
81 Just Culture

82 Value Cultural Maturity Model GENERATIVE Safety is how we do business around here Constantly Vigilant and Transparent Tipping Point PROACTIVE Anticipating and preventing problems before they occur; Comfort speaking up REACTIVE Safety is important. We do a lot every time we have an accident SYSTEMATIC We have systems in place to manage all hazards SRH 2017 UNMINDFUL Who cares as long as we re not caught Chronically Complacent *Adapted from Safeskies 2001, Aviation Safety Culture, Patrick Hudson, Centre for Safety Science, Leiden University
83 Organizational Fairness / Just Culture GENERATIVE Organization wired for safety and improvement PROACTIVE Playing offense - thinking ahead, anticipating, solving problems SYSTEMATIC Systems in place to manage hazards REACTIVE Playing defense reacting to events UNMINDFUL No awareness of safety culture Real events are shared by leaders, true culture of accountability and learning Clear ways to differentiate individual v. system error, safe to discuss mistakes Well understood algorithm, learning is the priority Depends who the boss is, blame and punishment are common Nothing good will come from talking about mistakes
84 Perspectives on Human Error Sidney Dekker Old View Human error is a cause of trouble You need to find people s mistakes, bad judgments and inaccurate assessments Complex systems are basically safe Unreliable, erratic humans undermine system safety Make systems safer by restricting the human contribution New View Human error is a symptom of deeper system trouble Instead, understand how their assessments and actions made sense at the time context Complex systems are basically unsafe Complex systems are tradeoffs between competing goals safety v. efficiency People must create safety through practice at all levels
85 In your Institution: How are events reported? How long does it take? Do they feel safe? What is the feedback loop? What happens in the absence of feedback?
86 LOW Individual Benefits HIGH VERY UNSAFE SPACE Drift & Risk 100% Agreement Non - acceptable Usual Space Of Action Illegal normal Real Life standards 60-90% 100% Expected safe space of action as defined by professional standards ACCIDENT Safety Reg s & good practices, accreditation standards HIGH Production Performance LOW Attribution: Dr. Rene Amalberti
87 Penetration of Just Culture What are the rules? Can you explain them in an elevator ride? If you asked 10 people in the hallway to explain just culture how would they distinguish an unsafe individual from a skilled caregiver set up to fail in a complex system how many could answer the question?
88 Inherent Human Limitations Limited memory capacity 5-7 pieces of information in short term memory Negative effects of stress error rates Tunnel vision Negative influence of fatigue and other physiological factors Limited ability to multitask cell phones and driving
89 Accountability Fair and Just Culture Clear, simple rules - one set that apply to everyone. Four questions - Was there malice involved? - Was the individual knowingly impaired? - Was there a conscious unsafe act? - Did the person(s) make a mistake that someone of similar skill and training could make under those circumstances?
90 A Systematic Approach to Safe & Reliable Care Leadership - systematic engagement, feedback, improvement, dialogue with front line caregivers discussing real cases This happened in our hospital Safety Culture unit level, broad themes across the organization; measurable, actionable items identified at a unit level Fair and Just Culture the rules are clear between individual accountability and system failures, and people feel safe to speak up and tell us. Risk Mitigation manage and reduce risk minimizing avoidable harm and its consequences keep everyone safe
91 Organizational Fairness and Professionalism Reliably excellent patient centered care is dependent on healthcare departments that are effective learning systems; they routinely identify their defects and then eliminate or ameliorate them. Individuals bring to light defects only when they trust others and feel safe about voicing their insights and concerns. Professionalism and Just Culture create trust and psychological safety and are the essential foundation for all learning systems. The job of the Safety and Reliability Committee is to safeguard Professionalism and Just Culture in order to protect and promote robust learning systems. Event or Near Event Identify Participants Review Event or Near Event. Reassign participants if evidence of: Malicious Behavior HR, Legal, Impaired Judgment - CMO, CNO, HR, EAP Unprofessional Behavior Perform Professional Behavior Evaluation RECKLESS ACTION RISKY ACTION UNINTENTIONAL The caregiver knowingly The caregiver made a The caregiver made or violated a rule and/or potentially unsafe choice. participated in an error made a dangerous or unsafe choice. The decision appears to be self serving and to have been made with little or no concern about risk. Their evaluation of relative risk appears to be erroneous. while working appropriately and in the patients' best interests individual. Step 3: IF RECKLESS: The caregiver is accountable and needs re-training. Discipline may be warranted. If the Substitution Test is positive (others would have performed similarly), then the system supports reckless action and requires fixing. The caregiver is probably less accountable for the action, and system leaders share in the accountability. If RISKY: The caregiver is accountable and should receive coaching. If the Substitution Test is positive (others would have performed similarly) the system supports risky action and requires fixing. The caregiver is probably less accountable for the action, and system leaders share in the accountability. Step 4: Promote learning and improvement The caregiver should The caregiver should participate in teaching participate in teaching others the lessons others the lessons learned. learned. Organizational Fairness and Professionalism Worksheet Step 1: Assign level of intent: Use best judgment to categorize each action as either Reckless, Risky or Unintentional. The categorization determines the general level of culpability and possible disciplinary actions, however these general categories require further analysis as below prior to making a final decision. Step 2: Evaluate systems influences Perform a Substitution Test: Ask or consider whether 3 others with similar skills or in a similar situation would behave or act similarly. Ask whether systems factors were present that would affect all individuals similarly, such as schedules leading inevitably to fatigue, unrealistic expectations regarding memory, inability to effectively follow policies or procedures, an unsafe learning environment, or distractions or interruptions? If "Yes" system influence is likely and warrants evaluation. If "No", continue evaluation of the If UNINTENTIONAL: Focus for improvement should be on system issues. Coaching and reflection on human factors and personal improvement strategies may be appropriate, especially if the Substitution Test is positive (others would have performed similarly). System leaders are accountable and should apply errorproofing improvements. The caregiver should participate in investigating why the error occurred and teach others about the results of the investigation. Complaint: Professional Behavior Evaluation and Intervention Receive Report of Concerning Behavior. Conduct confidential conversation with reporter regarding focus person (FP) behaviors. Categorize types of behaviors as well as frequency and severity. Conduct confidential interviews with others. Behavior categories include: Demeaning/angry, hypercritical, uncollegial, shirking responsibilities, misconduct, sexual harassment, patient communication concerns, boundary issues, substance abuse, blaming, and otherwise act in a manner that undermines trust and learning. Step 1: Feedback Conversation Coaching If the concern is deemed an isolated incident, the FP has not had any other issues, and the reporter feels safe to do so, provide coaching for the reporter on how to give the FP direct feedback regarding behaviors. If the situation is more complex, proceed to Step 2. Step 2: Assessing Concerns To validate the concerns and assess their frequency and severity, multisource interviews are conducted to provide comprehensive insight into and corroboration of alleged behavior. Step 3: Involving Supervisor Share findings of assessment with department chair, division chief, or supervising physician. Discuss a plan for feedback intervention (step 4) if deemed necessary. Step 4: Feedback Intervention Supervising MD and professionalism representative meet with FP to discuss/review specific disruptive behaviors FP's perspective on factors (including systems) that may be contributing to the behavior resources for facilitating behavioral changes plans for monitoring behavior unacceptability of retaliation (if applicable) potential consequences for not adhering to behavioral expectations A follow up is sent to the FP summarizing the meeting. Step 5: Monitoring and Support Inform those reporting concerns that an intervention has occurred. Inquire of them and others over time regarding subsequent behaviors. Have FP's supervisor address any systems issues discussed in Step 4. Keep process discrete and respectful to FP. Step 6: Intervention to Address Subsequent Lapses The institutional administration and legal counsel are involved. A plan of action is developed. Selected institutional administrators meet with FP to detail expected behavioral changes and consequences, including termination. Final Step: Evaluate the individual for a history of unsafe acts: Evaluate whether the individual has a history of unsafe or problematic acts. If they do, this may influence decisions about the appropriate responsibilities for the individual i.e. they may be in the wrong job. Organizations should have a reasonable and agreed upon statute of limitations for taking these actions into account. Jo Shapiro MD and Allan Frankel MD, 2015, Safe and Reliable Care Inc., Algorithm safeandreliablecare.com
92 Organizational Fairness and Professionalism - Evaluation and Intervention Worksheet The job of those entrusted to safeguard Professionalism and Just Culture is to protect and promote robust learning systems. Reliably excellent patient centered care is dependent on healthcare departments that are effective learning systems. They routinely identify their defects and then eliminate or ameliorate them. They routinely highlight good ideas and act on them. Individuals bring to light defects and ideas only when they trust others and feel safe about voicing insights and concerns. Professionalism and Just Culture create trust and psychological safety, essential foundations for all learning systems. Evaluators should consider system and human factors in their assessments of the events and actions. When possible, the caregiver should participate in the investigation and analysis of the event, and in teaching the lessons learned to others.
93 Event or Near Event Step 1: Exclude those with impaired judgment or those whose actions were malicious. - Impairment may result from legal or illegal substances, cognitive impairment, or severe psychosocial stressors. Refer to Human Resources, Risk, Senior Leaders or Professionalism Office.
94 Step 2: Characterize participant actions as either RECKLESS, RISKY or UNINTENTIONAL defined below. Consider every action independently. RECKLESS ACTION RISKY ACTION UNINTENTIONAL The caregiver knowingly violated a rule and/or made a dangerous or unsafe choice. The decision appears to be self serving and to have been made with little concern about risk. The caregiver made a potentially unsafe choice. Their evaluation of relative risk appears to be erroneous. The caregiver made or participated in an error while working appropriately and in the patients' best interest.
95 Step 3: Perform a Substitution Test to evaluate system influences: Ask 3 others with similar skills if they, in a similar situation, would have behaved or acted similarly.
96 Step 4: Evaluate whether the individual has a history of unsafe or problematic acts. Organizations should have a reasonable and agreed upon statute of - limitations for taking these actions into account.
97 Step 5: Combine the Evaluation of Individuals and System to determine next steps. A: If actions are RECKLESS: Retraining and/or disciplinary responses are warranted. RISKY: Coaching is warranted. UNINTENTIONAL: Focus on correcting systems issues to better support individual action. B: If there is a history of repeated evaluations for problem actions, consider if individual is in the wrong job. C: Finally, apply the Substitution Test. Individuals are: MORE accountable if others would not act similarly, and LESS accountable If others would act similarly. Leader accountability increases as individual accountability lessens, because the system supports reckless behavior OR risky behavior OR an environment that is not effectively supportive of personnel.
98 An Anesthesiologist, rather than reversing a muscle relaxant near the end of an operative procedure, mistakenly gives the patient more paralytic medicine causing a prolongation of the anesthetic at the end of the operative procedure. The patient emerges from the anesthetic uneventfully, but the case takes 2 1/2 hours rather than 90 minutes in the operating room. Anesthesiologist explains that the color of the vial tops had changed, so he mistakenly pulled out the wrong vial.
99 Nurse took ~2 cough syrups from pyxis for a patient. After getting meds, nurse went to dietary to get prune juice for another patient. Nurse then entered the first patient s room, sanitized hands and let patient know the reason for visit. The nurse administered the cough syrup to the first patient. When she entered the second patient s room, the patient asked for the cough syrup she had requested earlier. Upon checking the MAR, the first patient did not have cough syrup ordered and had not been coughing. The Meds were not scanned. The first patient s son complained since there was a medication allergy, and brought the medication container from the trash can. Nurse denied ever administering cough syrup to the first patient. Scanning was not done on either patient s medications that day.
100 4 year-old girl is admitted with a two-week history of viral illness. The child has not ingested fluid or food for over 24 hours, is not passing urine, covered in a rash, significantly unwell. Resident prescribes IV fluids, antibiotics and close monitoring. The Attending withdraws plan for IV fluids and antibiotics, prescribing oral fluids and regular weight monitoring. The RNs hear from Attending and Resident their differing concerns about the child. The child and mother are admitted to a private room at the end of the ward because no open beds are near the nursing station and the Charge RN chooses to not disrupt other patients to make a bed switch. When they enter the room, the RN and PCA taking care of the child see that both mother and child are sleeping and do not disturb them during the night to take vital signs. The next morning the mother cannot rouse the child, and seeks the RN for help. The RN pages a Junior doctor who goes to the room, opens the door and sees only that a child is asleep and leaves so as to not miss Rounds, planning to come back later when child wakes. The nurse goes to the room and, now concerned, calls for more help. The Attending arrives and starts resuscitation, and then leaves the resuscitation to Junior medical staff so that he can manage the remaining morning ward rounds. The group continues, but it takes extra time to get IV access, and finally an RN, over objections, calls the Rapid Response Team and the child is quickly transferred to ICU. Investigation: Independent clinical leaders partner with Risk Officer to investigate. Clinical team attends review meeting but Attending declines. All contribute but there is a sense that things aren t being said. With probing the flood gates open about extensive concerns about the Attending. No one is willing to share their concerns outside of the room for fear of being seen as criticizing a colleague. The leads inform the Medical Director who reports that he has been concerned for some time about the Attending. The Attending is taken off the acute on-call rotation pending investigation and also offered support and counseling. Further investigation indicates that the Attending tried to influence the choice of investigator (tried to ensure someone who was junior to him would lead), and contacted the family to tell them that there was no learning and nothing could have been done differently in the management of the child. The Attending is removed from the acute care rotation and reassigned to the ambulatory clinic.
101 A 65 year old male, in the ICU, has bright red rectal bleeding. He has a history of alcohol and cigarette use and has alcoholic cirrhosis and COPD. All agree that he should go to Interventional Radiology for an angiogram and embolization of the bleeding vessels. His Coags are elevated and he s ordered for, and receives, Fresh Frozen Plasma. The patient arrives in IR and the IR Nurse and Tech see the elevated Coags and voice concern because they ve had recent bad experiences in the IR area. The Fellow thinks that the still elevated Coags are from before the FFP. The RN and Tech voice their concerns to the Fellow, and the Fellow relays those concerns to the Attending - but they proceed because IR is swamped with cases and the Attending wants to get this complex add-on case done. As soon as the procedure gets underway, the patient gets a huge femoral hematoma and then rapidly deteriorates, dropping BP and becoming increasingly less responsive. The RN calls for the Rapid Response team to help resuscitate the patient. The patient s condition worsens over the next 24 hours.
102 Patient had 81 mg Aspirin, 60 mg oral Morphine, and 100 mg Metoprolol ordered for 10:00 am. RN informed student nurse that she had already given these medications. Student had already pulled medications from Pyxis with instructor and had been quizzed on medications prior to RN sharing this information. Student did not notify nursing instructor (or return meds to nursing instructor upon receiving these instructions from RN.) Student nurse administered all medications to patient. Student stated that she did scan medications in but that computer gave alert that "medication was not due at this time". Despite this alert, she still gave medications. Patient received a total of 120 mg Morphine by mouth, 162 mg Aspirin, and 200 mg of Metoprolol. Nursing instructor immediately notified nurse, clinical leader, primary care MD and cardiologist.
103 On May 27, 2017 I had a patient in room 307 who had a scheduled second troponin, the first having been within normal limits. At approximately 930 am the lab called me with a critical value of As per protocol an EKG was ordered STAT. Once I had the results I phoned Dr XXXXXX. From the very start of the phone call he was already yelling into the phone. He was yelling that he was going to cath the patient the following day and "it doesn't matter." I told him I had ordered an EKG and he yelled "you don't need an EKG!" I told him it is protocol and I tried to read him the result. He told me "I don't care, don't call me." The EKG showed non-specific ST & T wave abnormality but he would not hear me out. The third troponin came in at 217pm, and it was even more elevated at I called Dr XXXXXX again and he was livid. He cut me off during the conversation, he told me he told the other person not to call him (me, by the way). I told him as an RN I have to call him with critical results. I also told him if he didn't want any more calls then he needs to ask us to put in a provider order stating this. He told me to do it. I complied. The second call was even more stressful but it was required per hospital protocol, nursing ethics and best practice. I need to add that he was even more verbally abusive during the second call.
104 Wrap Up

105 Managing Transitions by William Bridges
106 Goals for Today: 1. How do we define safety culture, its attributes and impact? 2. How effective are your team behaviors, and what should they look like to support safety culture? What to do if professionalism or negative behaviors are eroding trust in your organization? 3. How do you create effective middle managers who can run the self-reflecting learning systems to manage change and ensure operational excellence? 4. How do we incorporate safety culture into improvement work? 5. How should senior leaders/board members engage with work settings and with the work setting managers? 6. How to embed just culture your organizations?
107 Framework for Safe, Reliable, Effective Care Psychological Safety Accountability Culture Leadership Teamwork & Communication Transparency Engagement of Patients & Family Negotiation Learning System Reliability Improvement & Measurement Continuous Learning IHI and Allan Frankel
108 Thank you! Questions? Comments?
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
4/7/2014. SocioTechnical Framework. Patient & Family Centered Care. Improving Safety Requires a Learning System
 Improving Safety Requires a Learning System Safety is a characteristic of a SocioTechnical system System level failures occur almost always because of unforeseen combinations of component failures Michael
Improving Safety Requires a Learning System Safety is a characteristic of a SocioTechnical system System level failures occur almost always because of unforeseen combinations of component failures Michael
A Comprehensive Framework for Patient Safety
 A Comprehensive Framework for Patient Safety A Framework for a System of Safety Objectives 1. Link safety to organizational strategy and resources 2. Define a culture of safety 3. Apply improvement methods
A Comprehensive Framework for Patient Safety A Framework for a System of Safety Objectives 1. Link safety to organizational strategy and resources 2. Define a culture of safety 3. Apply improvement methods
A Comprehensive Framework for Patient Safety
 These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
A Comprehensive Framework for Patient Safety, Reliability and Clinical Excellence
 14 November 2016 Oslo, Norway A Comprehensive Framework for Patient, and Clinical Excellence Frank Federico A Framework 1. Link safety and reliability to organizational strategy and resources 2. Define
14 November 2016 Oslo, Norway A Comprehensive Framework for Patient, and Clinical Excellence Frank Federico A Framework 1. Link safety and reliability to organizational strategy and resources 2. Define
A Comprehensive Framework for Patient Safety, Reliability and Clinical Excellence
 This presenter has nothing to disclose A Comprehensive Framework for Patient, and Clinical Excellence Allan Frankel, MD March 2, 2017 A Framework 1. Link safety and reliability to organizational strategy
This presenter has nothing to disclose A Comprehensive Framework for Patient, and Clinical Excellence Allan Frankel, MD March 2, 2017 A Framework 1. Link safety and reliability to organizational strategy
A Just Culture: Accountability for Patient Safety. Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012
 A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it?
 M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Frequently Asked Questions
 450 Simmons Way #700, Kaysville, UT 84037 (801) 547-9947 unar@davistech.edu www.utahcna.com Frequently Asked Questions UNAR stands for the Utah Nursing Assistant Registry, the agency in charge of the registry
450 Simmons Way #700, Kaysville, UT 84037 (801) 547-9947 unar@davistech.edu www.utahcna.com Frequently Asked Questions UNAR stands for the Utah Nursing Assistant Registry, the agency in charge of the registry
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Civility and Nursing Practice: Let s Talk About Bullying
 Civility and Nursing Practice: Let s Talk About Bullying Professional Practice Nursing Maxine Power-Murrin March 2015 A rose by any other name... Lateral violence Horizontal violence Bullying Intimidation
Civility and Nursing Practice: Let s Talk About Bullying Professional Practice Nursing Maxine Power-Murrin March 2015 A rose by any other name... Lateral violence Horizontal violence Bullying Intimidation
Participant WebEx Training. Jacob Auger Project Coordinator
 Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Disruptive Practitioner Policy
 Medical Staff Policy regarding Disruptive Practitioner Conduct MEC (9/96; 12/05, 6/06; 11/10) YH Board of Directors (10/96; 12/05; 6/06; 12/10; 1/13; 5/15 no revisions) Disruptive Practitioner Policy I.
Medical Staff Policy regarding Disruptive Practitioner Conduct MEC (9/96; 12/05, 6/06; 11/10) YH Board of Directors (10/96; 12/05; 6/06; 12/10; 1/13; 5/15 no revisions) Disruptive Practitioner Policy I.
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Human Factors Engineering in Health Care. Awatef O. Ergai, PhD Post-Doctoral Research Associate Healthcare Systems Engineering Institute
 Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
SBAR Communication Tool. Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme
 Clinical Risk Advisor, Clinical Indemnity Scheme") SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
Copyright, Joint Commission International. Tracer Methodology
 Tracer Methodology 2 What is a Tracer? JCI s key assessment method Traces a real patient s journey through the hospital, using their record as a guide Along the path, JCI observes and assesses compliance
Tracer Methodology 2 What is a Tracer? JCI s key assessment method Traces a real patient s journey through the hospital, using their record as a guide Along the path, JCI observes and assesses compliance
Entrustable Professional Activities (EPAs) for Psychiatry
 for Psychiatry") Professional Activities (EPAs) for Psychiatry These summaries describing the various EPAs can be used to formulate entrustability decisions and feedback comments on the clinic card. A student can be assessed
Professional Activities (EPAs) for Psychiatry These summaries describing the various EPAs can be used to formulate entrustability decisions and feedback comments on the clinic card. A student can be assessed
Practice Problems. Managing Registered Nurses with Significant PRACTICE GUIDELINE
 PRACTICE GUIDELINE Managing Registered Nurses with Significant Practice Problems Practice Problems May 2012 (1/17) Mission The Nurses Association of New Brunswick is a professional regulatory organization
PRACTICE GUIDELINE Managing Registered Nurses with Significant Practice Problems Practice Problems May 2012 (1/17) Mission The Nurses Association of New Brunswick is a professional regulatory organization
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
Promoting Psychological Safety for Physicians
 Doctors of BC Position Promoting Psychological Safety for Physicians Last updated: June 2017 Doctors of BC commits to working with the BC Ministry of Health, health authorities, and other stakeholders
Doctors of BC Position Promoting Psychological Safety for Physicians Last updated: June 2017 Doctors of BC commits to working with the BC Ministry of Health, health authorities, and other stakeholders
Documenting and Reporting
 Duty: Communicate Client Information to Authorized Persons Task : E.01 Report abuse of client E.02 Report client s unusual behavior E.03 Complete incident report E.05 Respond to authorized persons request
Duty: Communicate Client Information to Authorized Persons Task : E.01 Report abuse of client E.02 Report client s unusual behavior E.03 Complete incident report E.05 Respond to authorized persons request
Teaching and Assessing PBL&I and SBP On the Fly. Wisconsin Hospital Visit July 2009
 Teaching and Assessing PBL&I and SBP On the Fly Wisconsin Hospital Visit July 2009 Objectives Demonstrate how to embed the teaching and assessment of PBLI and SBP into daily activity Simple tools Benefits
Teaching and Assessing PBL&I and SBP On the Fly Wisconsin Hospital Visit July 2009 Objectives Demonstrate how to embed the teaching and assessment of PBLI and SBP into daily activity Simple tools Benefits
Welcome to LifeWorks NW.
 Welcome to LifeWorks NW. Everyone needs help at times, and we are glad to be here to provide support for you. We would like your time with us to be the best possible. Asking for help with an addiction
Welcome to LifeWorks NW. Everyone needs help at times, and we are glad to be here to provide support for you. We would like your time with us to be the best possible. Asking for help with an addiction
Returning to the Why: Patient and Caregiver Suffering and Care. Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer
 Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Toolbox Talks. Access
 Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
PERSON CENTERED CARE PLANNING HONORING CHOICE WHILE MITIGATING RISK
 PERSON CENTERED CARE PLANNING HONORING CHOICE WHILE MITIGATING RISK The purpose of the Rothschild Person-Centered Care Planning process is to support long term care communities in their efforts to honor
PERSON CENTERED CARE PLANNING HONORING CHOICE WHILE MITIGATING RISK The purpose of the Rothschild Person-Centered Care Planning process is to support long term care communities in their efforts to honor
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
5.3. Advocacy and Medical Interpreters LEARNING OBJECTIVE 5.3 SECTION. Overview. Learning Content. What is advocacy?
 Advocacy and Medical Interpreters SECTION 5.3 LEARNING OBJECTIVE 5.3 After completing this section, you will be able to: Apply a decision-making protocol for advocacy to medical interpreting. DEFINITION
Advocacy and Medical Interpreters SECTION 5.3 LEARNING OBJECTIVE 5.3 After completing this section, you will be able to: Apply a decision-making protocol for advocacy to medical interpreting. DEFINITION
Thinking Differently Acting Differently. Higher staff satisfaction = better patient outcomes & better patient experience
 Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Keeping Kids Safe TeamSTEPPS Essentials
 Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
The Intimidation Factor:
 The Intimidation Factor: Workplace intimidation and its effects on wellness, morale, and patient care Disclosure Amanda Chavez, MD, UT Health SA, UHS has no relationships with commercial companies to disclose.
The Intimidation Factor: Workplace intimidation and its effects on wellness, morale, and patient care Disclosure Amanda Chavez, MD, UT Health SA, UHS has no relationships with commercial companies to disclose.
The Milestones provide a framework for the assessment
 The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
CME Disclosure. Accreditation Statement. Designation of Credit. Disclosure Policy
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
Patient Advocate Certification Board. Competencies and Best Practices required for a Board Certified Patient Advocate (BCPA)
") Patient Advocate Certification Board Competencies and Best Practices required for a Board Certified Patient Advocate (BCPA) Attribution The Patient Advocate Certification Board (PACB) recognizes the importance
Patient Advocate Certification Board Competencies and Best Practices required for a Board Certified Patient Advocate (BCPA) Attribution The Patient Advocate Certification Board (PACB) recognizes the importance
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
Core Domain You will be able to: You will know and understand: Leadership, Management and Team Working
 DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
Preparing for the SJT. Katie Dallison Medical Careers Consultant
 Preparing for the SJT Katie Dallison Medical Careers Consultant What is SJT? In a Situational Judgement Test (SJT) applicants are presented with a set of hypothetical work relevant scenarios and asked
Preparing for the SJT Katie Dallison Medical Careers Consultant What is SJT? In a Situational Judgement Test (SJT) applicants are presented with a set of hypothetical work relevant scenarios and asked
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots
 HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
WORKPLACE BULLYING: RESPONDING TO THE EPIDEMIC
 WHY TOPIC IS IMPORTANT FOR PEDIATRIC HEALTH CARE PROFESSIONALS? Childhood is where bullying starts Little bullies grow up to be big bullies If bullying is not addressed early on, it continues/worsens WORKPLACE
WHY TOPIC IS IMPORTANT FOR PEDIATRIC HEALTH CARE PROFESSIONALS? Childhood is where bullying starts Little bullies grow up to be big bullies If bullying is not addressed early on, it continues/worsens WORKPLACE
MEDICAL STAFF BYLAWS APPENDIX C
 P a g e 1 MEDICAL STAFF BYLAWS APPENDIX C HOSPITAL POLICY REGARDING BEHAVIOR THAT UNDERMINES A CULTURE OF SAFETY For purposes of this policy, "behavior that undermines a culture of safety" is any conduct
P a g e 1 MEDICAL STAFF BYLAWS APPENDIX C HOSPITAL POLICY REGARDING BEHAVIOR THAT UNDERMINES A CULTURE OF SAFETY For purposes of this policy, "behavior that undermines a culture of safety" is any conduct
CASE MANAGEMENT POLICY
 CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
After Hours Support for Continuity of Care
 After Hours Support for Continuity of Care A few good ideas for meeting the Standard of Care A. INTRODUCTION In June 2015, the College of Physicians & Surgeons of Alberta (CPSA) released an updated Standard
After Hours Support for Continuity of Care A few good ideas for meeting the Standard of Care A. INTRODUCTION In June 2015, the College of Physicians & Surgeons of Alberta (CPSA) released an updated Standard
Radis Community Care (Nottingham)
") G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
Building a Just Culture
 Approved by: Building a Just Culture President and Chief Executive Officer Corporate Policy & Procedures Manual Policy No. III-35 Date Approved September 13, 2011 Next Review October 2014 Purpose The purpose
Approved by: Building a Just Culture President and Chief Executive Officer Corporate Policy & Procedures Manual Policy No. III-35 Date Approved September 13, 2011 Next Review October 2014 Purpose The purpose
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
PERSONAL CARE ATTENDANT COMPETENCY DEVELOPMENT GUIDE
 PERSONAL CARE ATTENDANT COMPETENCY DEVELOPMENT GUIDE Introduction and Overview A highly competent personal care attendant workforce is critical to the well-being and safety of individuals who need support
PERSONAL CARE ATTENDANT COMPETENCY DEVELOPMENT GUIDE Introduction and Overview A highly competent personal care attendant workforce is critical to the well-being and safety of individuals who need support
RALF Behavior Management Rules IDAPA
 RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
A26/B26: Goal Zero: South Carolina s Commitment to Safety
 A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
PREVENTION OF VIOLENCE IN THE WORKPLACE
 POLICY STATEMENT: PREVENTION OF VIOLENCE IN THE WORKPLACE The Canadian Red Cross Society (Society) is committed to providing a safe work environment and recognizes that workplace violence is a health and
POLICY STATEMENT: PREVENTION OF VIOLENCE IN THE WORKPLACE The Canadian Red Cross Society (Society) is committed to providing a safe work environment and recognizes that workplace violence is a health and
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
Workplace Violence & Harassment Policy Final Draft August 3, 2016 Date Approved October 1, 2016
 Workplace Violence & Harassment Policy Final Draft August 3, 2016 Date Approved October 1, 2016 Purpose To ensure that volunteers engage with Volunteer Toronto in an environment that is free from violence
Workplace Violence & Harassment Policy Final Draft August 3, 2016 Date Approved October 1, 2016 Purpose To ensure that volunteers engage with Volunteer Toronto in an environment that is free from violence
This matter was initiated by a letter from the complainant received on March 20, A response from Dr. Justin Clark was received on May 11, 2017.
 COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of
 Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
Reducing Stress. Changing Health Behaviors for the Better. Reducing Stress. What You ll Learn. What Exactly is Stress?
 Reducing Stress Changing Health Behaviors for the Better 1 What You ll Learn Why managing stress is important. The consequences of not managing stress. The benefits of reducing stress. The barriers preventing
Reducing Stress Changing Health Behaviors for the Better 1 What You ll Learn Why managing stress is important. The consequences of not managing stress. The benefits of reducing stress. The barriers preventing
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
https://www.new-innov.com/evaluationforms/evaluationformshost.aspx?data=ilai7qy...
 Page 1 of 6 Ambulatory Assessment of Resident [Subject Name] [Subject Status] [Evaluation Dates] [Subject Rotation] Evaluator [Evaluator Name] [Evaluator Status] 1) Was a feedback session held with the
Page 1 of 6 Ambulatory Assessment of Resident [Subject Name] [Subject Status] [Evaluation Dates] [Subject Rotation] Evaluator [Evaluator Name] [Evaluator Status] 1) Was a feedback session held with the
Skill 2: Client will identify triggers that have the greatest impact on his or her medical regimen
 OUTCOME AND SKILLS Outcome 1: Client will identify information sources regarding health and treatment Outcome 2: Client will identify factors that influence adherence to a medical regimen Skill 1: Client
OUTCOME AND SKILLS Outcome 1: Client will identify information sources regarding health and treatment Outcome 2: Client will identify factors that influence adherence to a medical regimen Skill 1: Client
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention
 Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention Maryland Nurses Association October, 2016 Pamela Shumate, DNP, RN, CCRN, CNE University of Maryland School of Nursing
Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention Maryland Nurses Association October, 2016 Pamela Shumate, DNP, RN, CCRN, CNE University of Maryland School of Nursing
Protect Your Patient, Protect Yourself: Know Your Nursing Practice Act
 Protect Your Patient, Protect Yourself: Know Your Nursing Practice Act Presenters: Judy Ho MSN, RN, ACNS- BC, CPHQ Geraldine Jones MS, RN-BC April 2010 Objectives List the primary types of Nursing Peer
Protect Your Patient, Protect Yourself: Know Your Nursing Practice Act Presenters: Judy Ho MSN, RN, ACNS- BC, CPHQ Geraldine Jones MS, RN-BC April 2010 Objectives List the primary types of Nursing Peer
Moorleigh Residential Care Home Limited
 Moorleigh Residential Care Home Limited Moorleigh Residential Care Home Inspection report Lummaton Cross, Barton, Torquay. TQ2 8ET Tel: 01803 326978 Website: Date of inspection visit: 14 April 2015 Date
Moorleigh Residential Care Home Limited Moorleigh Residential Care Home Inspection report Lummaton Cross, Barton, Torquay. TQ2 8ET Tel: 01803 326978 Website: Date of inspection visit: 14 April 2015 Date
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
Legal Issues facing Healthcare Employees. Medical Therapeutics Gibson County High School
 Legal Issues facing Healthcare Employees Medical Therapeutics Gibson County High School Learning Objectives for Standard 2 Compare and contrast the specific laws and ethical issues that impact relationships
Legal Issues facing Healthcare Employees Medical Therapeutics Gibson County High School Learning Objectives for Standard 2 Compare and contrast the specific laws and ethical issues that impact relationships
Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England
 Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England As a Healthcare Support Worker
Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England As a Healthcare Support Worker
Overview SKASS2. Control the movement of spectators and deal with crowd issues at an event
 issues at an Overview This standard is about keeping a careful watch over spectators including their entry to and exit from the venue. It also covers dealing with crowd issues such as unexpected movements,
issues at an Overview This standard is about keeping a careful watch over spectators including their entry to and exit from the venue. It also covers dealing with crowd issues such as unexpected movements,
Resource Library Banque de ressources
 Resource Library Banque de ressources SAMPLE POLICY: STAFF SAFETY Sample Community and Health Services Keywords: high risk, safety, home visits, staff safety, client safety, disruptive behavior, refusal
Resource Library Banque de ressources SAMPLE POLICY: STAFF SAFETY Sample Community and Health Services Keywords: high risk, safety, home visits, staff safety, client safety, disruptive behavior, refusal
Practice Guideline Duty to Report
 The College of Licensed Practical Nurses of Nova Scotia (CLPNNS) is the regulatory body for the Licensed Practical Nurses (LPN) of Nova Scotia. Its mandate is to protect the public by promoting the provision
The College of Licensed Practical Nurses of Nova Scotia (CLPNNS) is the regulatory body for the Licensed Practical Nurses (LPN) of Nova Scotia. Its mandate is to protect the public by promoting the provision
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Assessing Non-Technical Skills. A Guide to the NOTSS Tool Adapted for the Labour Ward
 Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Clinical Nurse Director
 Date: March 2018 Job Title : Clinical Nurse Director Department : Acute and Emergency Medicine Division and Specialty Medicine & Health of Older People Division Location : North Shore Hospital, Waitakere
Date: March 2018 Job Title : Clinical Nurse Director Department : Acute and Emergency Medicine Division and Specialty Medicine & Health of Older People Division Location : North Shore Hospital, Waitakere
Legally. Copyright 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
 Legally speaking 40 January 2011 Nursing Management When can staff say No? Accepting responsibilities that are beyond the scope of your license or skill level can have serious consequences for you, your
Legally speaking 40 January 2011 Nursing Management When can staff say No? Accepting responsibilities that are beyond the scope of your license or skill level can have serious consequences for you, your
Delivering Great Care with High Reliability The Orlando Health Journey
 FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
Psychologically Safe Leader Assessment
 Psychologically Safe Leader Assessment Psychologically Safe Leader Assessment (PSLA) By completing the Psychologically Safe Leader Assessment: Employee Feedback (PSLA-E), you are contributing to your leader
Psychologically Safe Leader Assessment Psychologically Safe Leader Assessment (PSLA) By completing the Psychologically Safe Leader Assessment: Employee Feedback (PSLA-E), you are contributing to your leader
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance