Using MEDMARX for Reporting and Benchmarking. Anne Skinner, RHIA Katherine Jones, PhD, PT
|
|
|
- Maria Miller
- 6 years ago
- Views:
Transcription
1 Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT
2 Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify and analyze system sources of error Compare current medication use system to best practices and prioritize change Conduct root cause analysis, failure mode and effect analysis Implement and maintain organizational change
. To Err is Human: Building a Safer Health System.")
3 Why Are We Here? The problem is not bad people; the problem is that the system needs to be made safer. Institute of Medicine. (2000). To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press, p. 49.

4 Errors in Our Health Care System 44,000 98,000 deaths per year due to medical errors 8 th cause of death One jet airplane crash per day 2.9% - 3.7% of hospital admissions result in adverse events Cost $17 - $29 billion/yr Adults get 55% of recommended care

5 Humans work in CAHs, too Drugs given despite allergy IV antibiotics not infused Concentrated sodium chloride given to patient in error
6 Role of MEDMARX in the Project Provides standardized terminology for data collection and analysis A critical tool TELL A STORY WITH YOUR DATA Source of benchmarks Overcomes rural barriers to QI Small numbers Limited information management resources Limited human resources
7 Medication Safety Model (USP, 2004) Culture Data Collection Data Analysis Plan Change MEDMARX Implement Change Assess Impact of Change
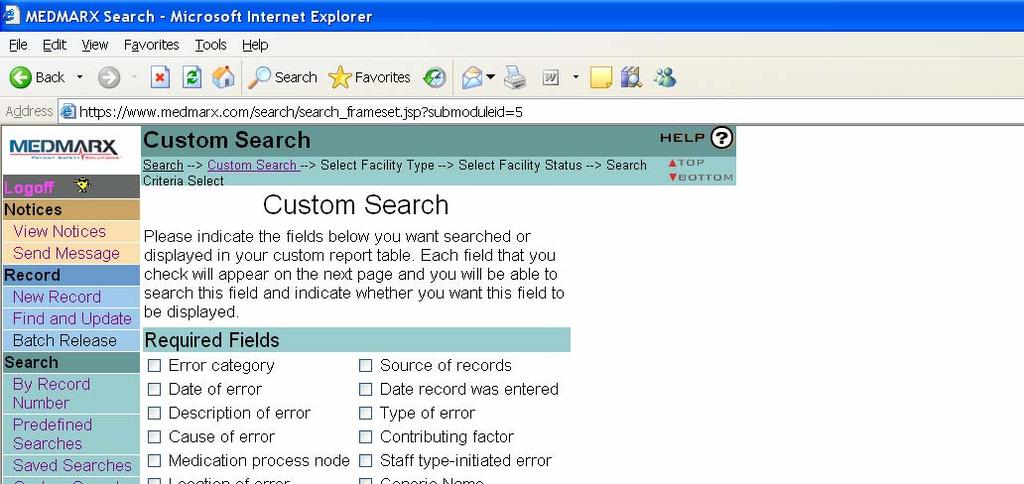
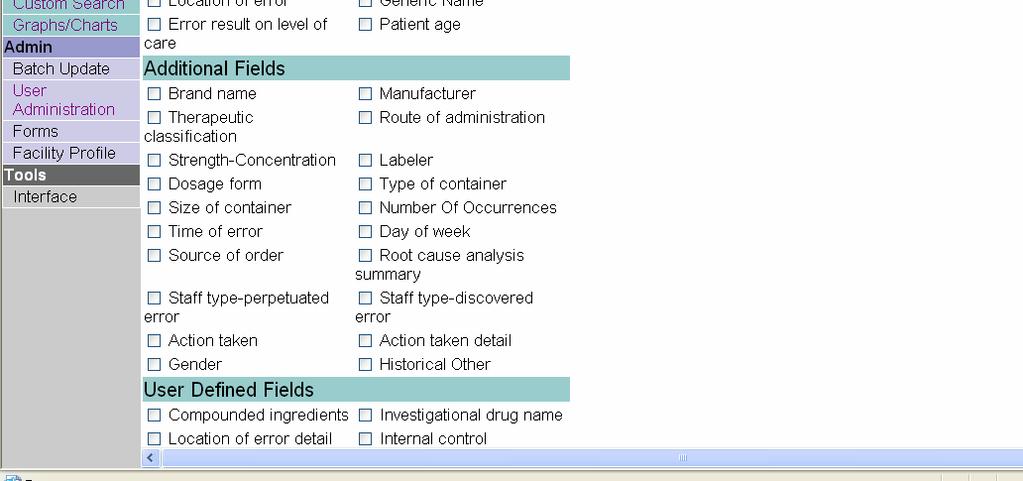
8 MEDMARX Menu Notices Public/Private Notices Messages from UNMC Send Message to USP Record New Find and Update/Delete Search By Record Number Predefined, Saved, Custom, Graphs/Charts
9 MEDMARX Menu Admin User Administration Enter, Search, Update, Hold/Release & Admin Records Online Forms not user friendly Facility Profile Update at least annually when subscription renewed Location of error detail specified
10 Brief review of record entry Continuous approach to data entry Review of field lists A vs B why such a big deal? From the patient s perspective A means no error B means error occurred but was intercepted a measure of success
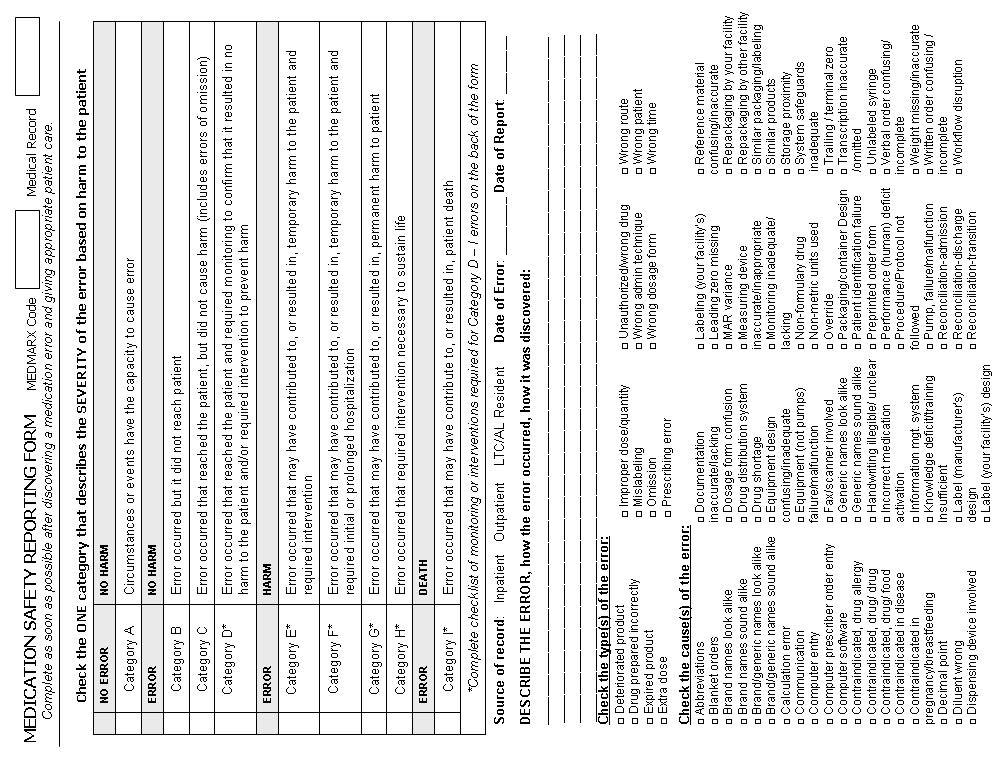
11
12
13 Category A Example Patient admitted from ER. Admitting nurse made a new Med list from patient s info and med bottles, but did not compare it to the med list in the clinic file. The meds missed from the clinic list included Calcium w/vitamin D, Mobic and Effexor. Omission was picked up the next day by the 7-3 nurse comparing all the lists. Physician was notified, Effexor was the only one ordered, and was covered before the daily dose was due. Reporting nurse also noted to write out the home med list in layperson s language, not abbreviations, and to omit unapproved abbreviations e.g. qd as every day.
14 Category B Example Xopenex and Atrovent Neb treatment ordered q 6hr without dose/strength of Xopenex indicated. Root cause analysis summary: Physicians often let Pulmonary services complete the dose they want, but this leaves open the possibility that pharmacy might enter a different dose/strength in the computer. If Pulmonary doesn t clarify order the order remains incomplete and can delay treatment. Action taken details: Informed staff who made the initial error (Physician)
15
16 Brief Review of Record Entry Source of Record Description Who (level of staff) Did what When Where Specific consequences
17 Brief review of record entry Causes Mar Variance MAR differs from order Performance/human deficit Reconciliation Contributing Factors No 24 hour pharmacy Nodes Procurement ordering of inventory
18 Brief review of record entry Location of initial error Consistent with Source of Record Products Enter information you will use Add additional product(s) Location of error detail Required for data to be included in graphs Additional fields use what is relevant WORKING DOCUMENT for 60 days
19 Summary Entering Records Select Error Category Enter Required Fields Enter Product Information Enter Additional Fields Administration Holding/Releasing Records Locating/Updating/Deleting Held Records
20 Enter Reports Problems Challenges Frustrations
21 Bolster Your Reporting Educate staff Use video to remind staff Purpose of project Culture of safety Completing forms Description most important Review definitions of fields Policy Statement
22 Policy Statement Nonpunitive culture Definitions Data Entry Continuous approach best Feedback on accuracy ed monthly Use Find and Update to make corrections QI Process
23 Next Steps Conference Call Fall 05 Prioritize change using data from MEDMARX Use best practices check list Workshop Spring 06 Implement and maintain change RCA basics
24 MEDMARX Searches and Reports
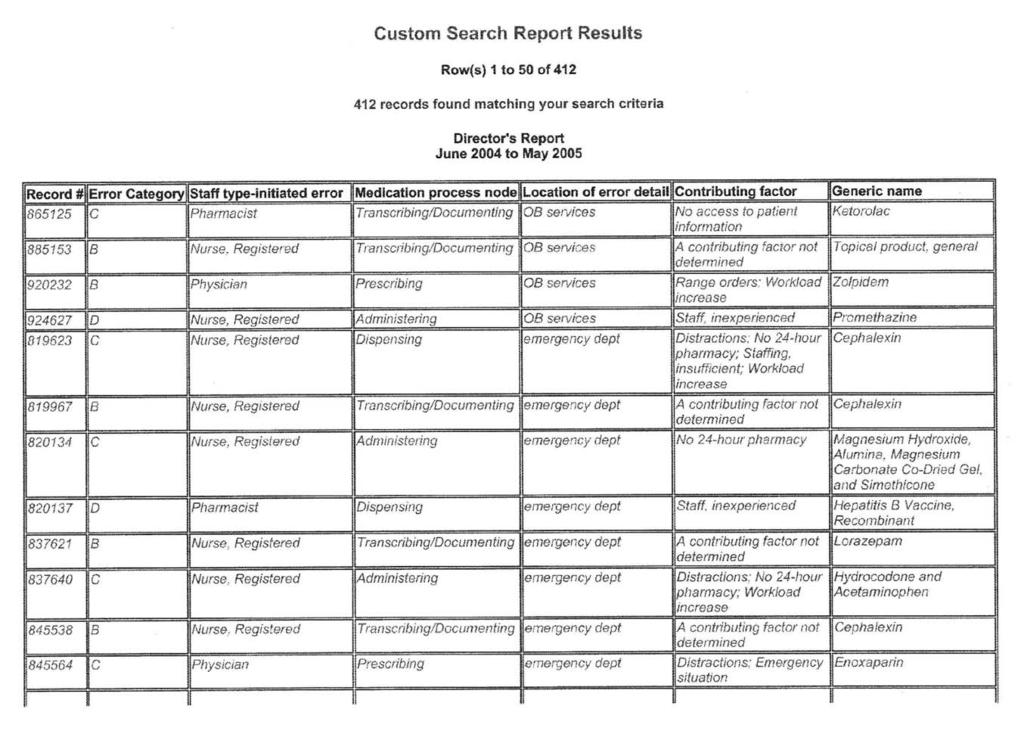
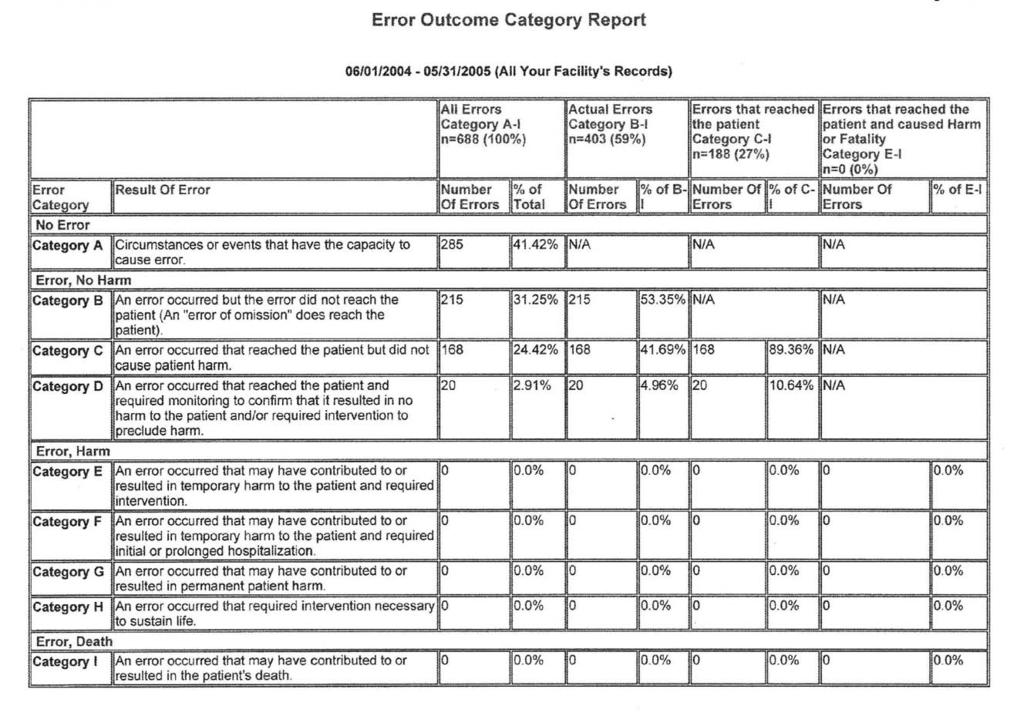
25 Searches By Record Number Predefined Searches Director s Report Spreadsheet for trending level of staff making Error Outcome Category (demo) Spreadsheet shows number and %age of errors by severity Product Summary Report (demo) Spreadsheet shows products involved in errors during specified time
26
27
28
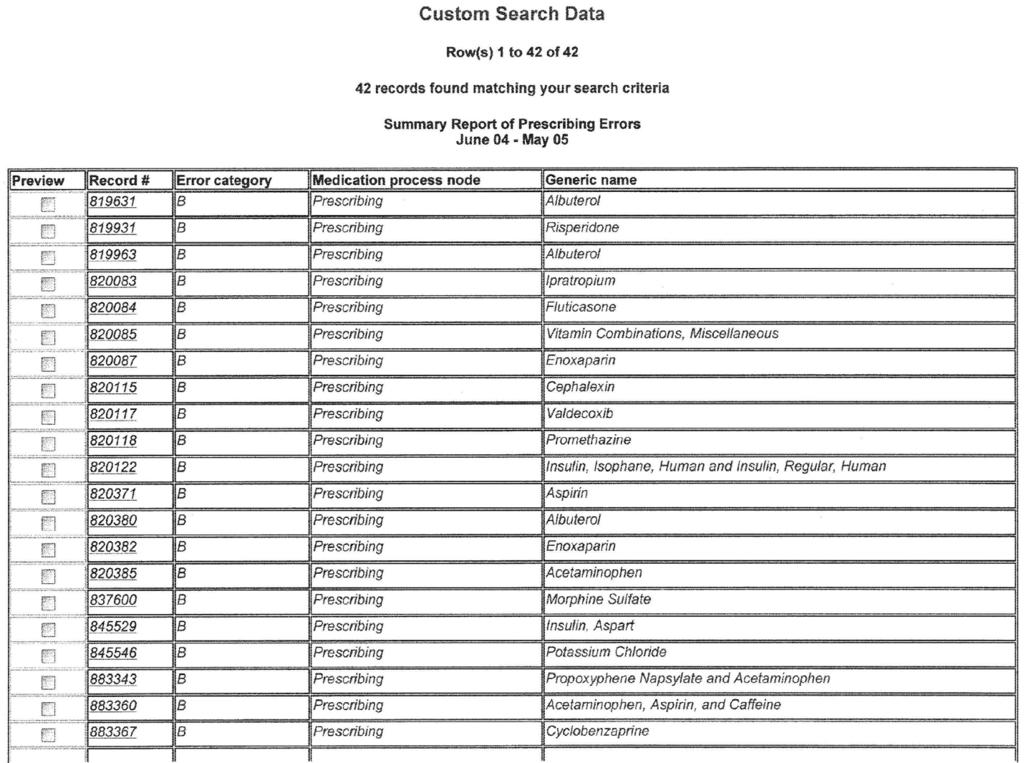
29 Searches Predefined Searches Summary Report Spreadsheet shows severity, node, location of errors during specified time Top Five Types of Error Drill Down (demo) Spreadsheet shows top five error types and their top three causes, contributing factors, level of staff making error, and products involved during specified time Top Five Generic Names Drill Down Spreadsheet shows top five generic names and their top three causes, contributing factors, level of staff making error, and products involved during specified time
30
31
32 Predefined Graphs Top Generic Names Top Therapeutic Classes Top Types of Error Top Causes of Error
33 Your Facility Top Therapeutic Class of Errors that Reached the Patient from 6/1/2004 to 5/31/ Blood Coagulation Modifiers Opioid Analgesics Beta-Lactam Antimicrobials Non-Opioid Analgesics Oral Antidiabetic Agents Vaccines Electrolytes/Minerals Antiulcer Agents Laxatives/Antidiarrheal Agents Amino Acids/Proteins/ Parenteral # of Errors
34 Your Facility Top Error Cause All Error Categories from 6/1/2004 to 5/31/ Computer entry Procedure/protocol not followed Transcription inaccurate/omitted Communication Written order Knowledge deficit Blanket orders Reconciliation-admission Performance (human) deficit Documentation # of Errors
35 Graphic Trending useless Improper Dose Quantity Error Reports from 6/1/2004 to 5/31/2005 (your facility) No Error Error, No Harm # oferrors Qtr Qtr Qtr Qtr Qtr Quarter
36 Predefined Spreadsheet Totals Spreadsheet Tally by Month, Quarter, Year Date of Error Error Category Desired Field (Type, Cause, Node, Location) Total Number of Reports over time
37
38
39 Suggested Quarterly Graphs Track Your Shared Organizational Goal: Maximize Reporting of Potential & Near Miss Errors (A & B Error Reports) Error Severity by Month Severity Pie Chart Process Node Pie Chart
40 Error Severity Over Time Facility X Error Severity by Month June May 2005 A B C D # oferrors Jun 04 Jul 04 Aug 04 Sep 04 Oct 04 Nov 04 Dec 04 Jan 05 Feb 05 Mar 05 Apr 05 May 05 Month
41 Severity Pie Chart Error Severity from 6/1/2004 to 5/31/2005 (your facility) D, 17, 3% C, 148, 24% A, 265, 42% B, 190, 31%
42 Node Pie Chart Medication Process Node from 6/1/2004 to 5/31/2005 (your facility) Dispensing, 31, 8% Monitoring, 2, 0% Prescribing, 42, 10% Transcribing/Docum enting, 189, 48% Administering, 139, 34%
43 Suggested Quarterly Graphs: Stacked columns to slice your data by severity Nodes by Severity Types by Severity Causes by Severity Location by Severity
44 Nodes by Severity Medication Nodes by Severity from 6/1/2004 to 5/31/2005 B C D # oferrors Administering Dispensing Monitoring Prescribing Transcribing/Documenting
45 Type By Severity Type of Error by Severity from 6/1/2004 to 5/31/2005 (your facility) A B C D # oferrors Drug prepared incorrectly Extra dose Improper dose/quantit y Mislabeling Omission error Prescribing error D C B A Unauthorize d/wrong drug Wrong Wrong Wrong administrati dosage Wrong route Wrong time patient on form
46 Benchmarks definition?? Error Severity by size Reporting by phase Harmful error types How common is my error? What did others do about it? In hospitals my size reporting to MEDMARX In all hospitals reporting to MEDMARX
47 Severity Benchmark 1-10 Beds Aggregate Error Severity of 19 Critical Access Hospitals (Average Occupancy 1-10 Beds) 2004 D, 64, 3% E, 11, 1% F, 5, 0% I, 1, 0% A, 510, 25% C, 1194, 58% B, 263, 13%
48 Severity Benchmark Beds Aggregate Error Severity of 13 Critical Access Hospitals (Average Occupancy Beds) Reporting to Medmarx in 2004 E, 12, 1% F, 6, 0% D, 80, 4% A, 537, 28% C, 749, 38% B, 562, 29%
49 Cause Benchmark CAHs Aggregate Causes of Error in 32 Critical Access Hospitals Reporting to Medmarx in 2004 Abbreviations 2% Computer entry 3% Written order 3% Knowledge deficit 4% Other 14% Performance (human) deficit 26% Communication 4% Transcription inaccurate/omitted 11% Procedure/protoco l not followed 16% Documentation 17%
50 Detective Work Are we really different? Severity Phase Types Has this error happened elsewhere? How often? In which size hospital? What level of staff was involved? What did they do about it?
51 Questions Katherine Jones Anne Skinner
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Medication Safety Dashboard
 How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
EMR Adoption: Benefits Realization
 EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
A Million Little Pieces: Developing a Controlled Substance Diversion Program. Tanya Y. Barnhart, PharmD, BCPS
 A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Improving Safety Practices Anticoagulation Therapy
 Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Introduction. Medication Errors. Objectives. Objectives. January What is a Medication Error? Define medication errors/variances
 Medication Errors Earlene Spence, Pharm.D., Miami VA Healthcare System Neena John, Pharm.D., Miami VA Healthcare System Eva Moreira, Pharm.D., Miami VA Healthcare System Chantal Chan, Pharm.D., Miami VA
Medication Errors Earlene Spence, Pharm.D., Miami VA Healthcare System Neena John, Pharm.D., Miami VA Healthcare System Eva Moreira, Pharm.D., Miami VA Healthcare System Chantal Chan, Pharm.D., Miami VA
Patient Safety in Ambulatory Care: Why Reporting Counts. August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH
 Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Drug Events. Adverse R EDUCING MEDICATION ERRORS. Survey Adapted from Information Developed by HealthInsight, 2000.
 Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Background and Methodology
 Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
UHF Quality Institute. Patient-Reported Outcomes in Primary Care New York PROPC-NY. Module 2 Webinar
 UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Nursing Home Medication Error Quality Initiative
 Nursing Home Medication Error Quality Initiative MEQI Report: Year Five October 1, 2007 to September 30, 2008 MEQI A report on the fifth year of mandatory reporting of medication errors for all state licensed
Nursing Home Medication Error Quality Initiative MEQI Report: Year Five October 1, 2007 to September 30, 2008 MEQI A report on the fifth year of mandatory reporting of medication errors for all state licensed
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L
 Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Drug Distribution Services for Long Term Care Facilities. Susan L. Lakey, PharmD 1/11/06
 Drug Distribution Services for Long Term Care Facilities Susan L. Lakey, PharmD 1/11/06 Drug distribution The process: Receipt / transcription of order Interpretation / evaluation of order Filling and
Drug Distribution Services for Long Term Care Facilities Susan L. Lakey, PharmD 1/11/06 Drug distribution The process: Receipt / transcription of order Interpretation / evaluation of order Filling and
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
MEDICATION USE EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014
 TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
National Homecare KPI performance March 2017
 National Homecare KPI performance March 2017 Foreword We are pleased to publish our latest KPI report, continuing our commitment to the transparency of the service we provide to our patients and customers,
National Homecare KPI performance March 2017 Foreword We are pleased to publish our latest KPI report, continuing our commitment to the transparency of the service we provide to our patients and customers,
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now!
 Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
University of Wisconsin Hospital and Clinics Medication Reconciliation Education Packet
 Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Information Technology Report to Medical Executive Committee
 July 10, 20 Information Technology Report to Medical Executive Committee Contents 1 Medicare Meaningful Use 1 Drug/Drug Interaction Alert 2 Leapfrog Group 2 My Apps Icon/Shortcut 2 NHIQM Project 3 mpages
July 10, 20 Information Technology Report to Medical Executive Committee Contents 1 Medicare Meaningful Use 1 Drug/Drug Interaction Alert 2 Leapfrog Group 2 My Apps Icon/Shortcut 2 NHIQM Project 3 mpages
5. returning the medication container to proper secured storage; and
 111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Importance of Clinical Leadership in Pharmacy
 Importance of Clinical Leadership in Pharmacy Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center, Los Angeles Assistant Dean, Clinical Pharmacy UCSF School of Pharmacy
Importance of Clinical Leadership in Pharmacy Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center, Los Angeles Assistant Dean, Clinical Pharmacy UCSF School of Pharmacy
Ontario Shores Journey to EMRAM Stage 7. October 21, 2015
 Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events
 Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Enlisted Professional Military Education FY 18 Academic Calendar. Table of Contents COLLEGE OF DISTANCE EDUCATION AND TRAINING (CDET):
:") Enlisted Professional Military Education FY 18 Academic Calendar Table of Contents STAFF NON-COMMISSIONED OFFICER ACADEMIES: SNCO Academy Quantico SNCO Academy Camp Pendleton SNCO Academy Camp Lejeune
Enlisted Professional Military Education FY 18 Academic Calendar Table of Contents STAFF NON-COMMISSIONED OFFICER ACADEMIES: SNCO Academy Quantico SNCO Academy Camp Pendleton SNCO Academy Camp Lejeune
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016
 COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
Storyboard Submission NHS Wales Awards Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated INRs
 Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
CHC-A Continuity Dashboard. All Sites Continuity - Asthma. 2nd Qtr-03. 2nd Qtr-04. 2nd Qtr-06. 4th Qtr-03. 4th Qtr-06. 3rd Qtr-04.
 PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Using Data to Inform Quality Improvement
 20 15 10 5 0 Using Data to Inform Quality Improvement Ethan Kuperman, MD FHM Aparna Kamath, MD MS Justin Glasgow, MD PhD Disclosures None of the presenters today have relevant personal or financial conflicts
20 15 10 5 0 Using Data to Inform Quality Improvement Ethan Kuperman, MD FHM Aparna Kamath, MD MS Justin Glasgow, MD PhD Disclosures None of the presenters today have relevant personal or financial conflicts
Licensed Pharmacy Technicians Scope of Practice
 Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Northern Health - Acute Services. Evidence Based Practice Venous Thromboembolism Prevention
 Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
Andrew Kirby Director, Healthcare Solutions Microsoft Services
 Andrew Kirby Director, Healthcare Solutions Microsoft Services Microsoft in Health Patient Safety Challenges The Patient Safety Principles Driving MSCUI Delivery Roadmap Review Examples of MSCUI in Use
Andrew Kirby Director, Healthcare Solutions Microsoft Services Microsoft in Health Patient Safety Challenges The Patient Safety Principles Driving MSCUI Delivery Roadmap Review Examples of MSCUI in Use
Medication Reconciliation with Pharmacy Technicians
 Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY
 REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016
 Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Prohibited. Implementation & Results. Karen Horon, Director, Professional Practice. use space to insert photo or graphics
 Prohibited Abbreviations i Implementation & Results use space to insert photo or graphics Karen Horon, Director, Professional Practice Objectives To learn how focused education and communication, rather
Prohibited Abbreviations i Implementation & Results use space to insert photo or graphics Karen Horon, Director, Professional Practice Objectives To learn how focused education and communication, rather
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Medication Reconciliation
 Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Quality and Safe Respiratory Care: Does it Work in a Productivity Model?
 Quality and Safe Respiratory Care: Does it Work in a Productivity Model? Timothy R. Myers MBA, RRT-NPS, FAARC Associate Executive Director, Brands Management American Association for Respiratory Care Adjunct
Quality and Safe Respiratory Care: Does it Work in a Productivity Model? Timothy R. Myers MBA, RRT-NPS, FAARC Associate Executive Director, Brands Management American Association for Respiratory Care Adjunct
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY
 Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
Leapfrog Group Report on CPOE Evaluation Tool Results June 2008 to January 2010
 Leapfrog Group Report on CPOE Evaluation Tool Results June 2008 to January 2010 Executive Summary Using The Leapfrog Group s web based simulation tool, 214 hospitals tested their computerized physician
Leapfrog Group Report on CPOE Evaluation Tool Results June 2008 to January 2010 Executive Summary Using The Leapfrog Group s web based simulation tool, 214 hospitals tested their computerized physician
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Running head: MEDICATION ERRORS 1. Medications Errors and Their Impact on Nurses. Kristi R. Rittenhouse. Kent State University College of Nursing
 Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
In-Patient Medication Order Entry System - contribution of pharmacy informatics
 In-Patient Medication Order Entry System - contribution of pharmacy informatics Ms S C Chiang BPharm, MRPS, MHA, FACHSE, FHKCHSE, FCPP Senior Pharmacist Chief Pharmacist s Office In-Patient Medication
In-Patient Medication Order Entry System - contribution of pharmacy informatics Ms S C Chiang BPharm, MRPS, MHA, FACHSE, FHKCHSE, FCPP Senior Pharmacist Chief Pharmacist s Office In-Patient Medication
MEDICINES RECONCILIATION GUIDELINE Document Reference
 MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology
 Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Grant Reporting for Faculty Grant Expense Detail
 Grant Reporting for Faculty Grant Expense Detail This report provides line item detail expenses for a user-specified Sponsored Program. The report allows faculty and department administrators to more easily
Grant Reporting for Faculty Grant Expense Detail This report provides line item detail expenses for a user-specified Sponsored Program. The report allows faculty and department administrators to more easily
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Utilizing FPPE and OPPE Effectively OPPE & FPPE. Joint Commission FAQs. Utilizing FPPE and OPPE Effectively. Susan Mellott PhD, RN.
 Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Pharmaceutical Services Instructor s Guide CFR , (a)(b)(1) F425
(b)(1) F425") Centers for Medicare & Medicaid Services (CMS) Pharmaceutical Services Instructor s Guide CFR 483.60, 483.60(a)(b)(1) F425 2006 Prepared by: American Institutes for Research 1000 Thomas Jefferson St, NW
Centers for Medicare & Medicaid Services (CMS) Pharmaceutical Services Instructor s Guide CFR 483.60, 483.60(a)(b)(1) F425 2006 Prepared by: American Institutes for Research 1000 Thomas Jefferson St, NW
HOW TO DO POST-HOC RESPONSE REVIEWS
 HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
St. Michael s Hospital Medication Reconciliation Learning Package
 St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Nurse Orientation. Medication Management
 Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
MEDMARX ADVERSE DRUG EVENT REPORTING
 MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
Case Study BACKGROUND. Recovering Ambulance Linen. Larry J Haddad, CLLM Textile Management Consultant. Midwest Region
 Title: Facility: Author: Recovering Ambulance Linen Midwest Region Larry J Haddad, CLLM Textile Management Consultant Midwest Region BACKGROUND A 294-bed, not-for-profit community hospital in the Midwest
Title: Facility: Author: Recovering Ambulance Linen Midwest Region Larry J Haddad, CLLM Textile Management Consultant Midwest Region BACKGROUND A 294-bed, not-for-profit community hospital in the Midwest
About us USING MEDICATION RECONCILIATION TO RECONCILE THE TEAM. St Luke Community Healthcare 3/6/2015
 USING MEDICATION RECONCILIATION TO RECONCILE THE TEAM St Luke Community Healthcare About us Community owned & operated; heart of healthcare in the Mission Valley Nestled between Flathead Lake, Mission
USING MEDICATION RECONCILIATION TO RECONCILE THE TEAM St Luke Community Healthcare About us Community owned & operated; heart of healthcare in the Mission Valley Nestled between Flathead Lake, Mission
Achieving HIMSS Level 7 Implications for HIM. Children s Health System of Texas
 Achieving HIMSS Level 7 Implications for HIM Children s Health System of Texas Katherine Lusk, MHSM, RHIA Chief Health Information Management & Exchange Officer Children s Health SM Four Campuses, 562
Achieving HIMSS Level 7 Implications for HIM Children s Health System of Texas Katherine Lusk, MHSM, RHIA Chief Health Information Management & Exchange Officer Children s Health SM Four Campuses, 562
Go! Guide: Medication Administration
 Go! Guide: Medication Administration Introduction Medication administration is one of the most important aspects of safe patient care. The EHR assists health care professionals with safety by providing
Go! Guide: Medication Administration Introduction Medication administration is one of the most important aspects of safe patient care. The EHR assists health care professionals with safety by providing
Royal Cornwall s implementation plan: A Chief Pharmacist s perspective
 Royal Cornwall s implementation plan: A Chief Pharmacist s perspective Iain Davidson, Chief Clinical Information Officer and Chief Pharmacist, Royal Cornwall Hospitals NHS Trust 13 April 2016 GS1 at The
Royal Cornwall s implementation plan: A Chief Pharmacist s perspective Iain Davidson, Chief Clinical Information Officer and Chief Pharmacist, Royal Cornwall Hospitals NHS Trust 13 April 2016 GS1 at The
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Administration of Oral Prescription Medication Procedure Page 1 of 6
 Page 1 of 6 RATIONALE: Hamilton-Wentworth District School Board is committed to ensuring the provision of plans, programs, and/or services that will enable students with health or medical needs to attend
Page 1 of 6 RATIONALE: Hamilton-Wentworth District School Board is committed to ensuring the provision of plans, programs, and/or services that will enable students with health or medical needs to attend
Presentation Outline
 Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
Case Study: Cass Regional Medical Center
 Case Study: Cass Regional Medical Center CASS REGIONAL MEDICAL CENTER, A COUNTY HOSPITAL SERVING BOTH SUBURBAN AND RURAL COMMUNITIES, PURCHASED A NEW NURSE CALL PLATFORM TO SUPPORT THEIR GOALS TO IMPROVE
Case Study: Cass Regional Medical Center CASS REGIONAL MEDICAL CENTER, A COUNTY HOSPITAL SERVING BOTH SUBURBAN AND RURAL COMMUNITIES, PURCHASED A NEW NURSE CALL PLATFORM TO SUPPORT THEIR GOALS TO IMPROVE
Reducing Medication Errors: National Update
 Reducing Medication Errors: National Update Ahmed Ameer Medication Safety Officer Ahmed.Ameer@NHS.net Safer Medication Practice & Medical Devices Team 27 th January 2015 Agenda 1. Development of the National
Reducing Medication Errors: National Update Ahmed Ameer Medication Safety Officer Ahmed.Ameer@NHS.net Safer Medication Practice & Medical Devices Team 27 th January 2015 Agenda 1. Development of the National
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Adverse Drug Events in Wyoming
 Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop