Importance of Clinical Leadership in Pharmacy
|
|
|
- Deborah Flowers
- 5 years ago
- Views:
Transcription
1 Importance of Clinical Leadership in Pharmacy Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center, Los Angeles Assistant Dean, Clinical Pharmacy UCSF School of Pharmacy

2 Objectives Describe why clinical leadership in pharmacy is essential to advance pharmacy practice Describe the characteristics and priorities of clinical leaders Recognize the clinical elements of the medication use process Provide examples demonstrating the clinical value of pharmacists
3 Why clinical leadership is essential Key global challenges in healthcare and pharmacy are clinical ones: reducing drug costs and improving the quality and safety of medication use in our patients We must resolve issues of medication safety, such as medication use across the continuum of care and the reconciliation of medications for specific patient populations. The pharmacy director or manager must serve as a clinical leader adapted from William Gouveia. Clinical Leadership Am J Health-Syst Pharm. 2005; 62:805.
4 Why clinical leadership is essential? 2015 Revised FIP Basel Statements on the Future of Hospital Pharmacy The overarching goal of hospital pharmacists is to optimize patient outcomes through collaborative, inter-professional, responsible use of medicines and medical devices. Hospital pharmacists should serve as a resource regarding all aspects of medicines use and be accessible as a point of contact for patients and health care providers.
5 Characteristics of Clinical Leaders Context: Maintains understanding of current healthcare priorities and needs of patients Recognizes implications of priorities for pharmacy profession Relevance: Develops programs and services which meet needs of patients (pts) and healthcare system

6 Leadership Context Health Care Health- System Pharmac y
7 Characteristics of Clinical Leaders Places patients at the center of decision-making Interprets and translates healthcare priorities into pharmacy strategic initiatives Committed to lifelong learning Creates expectations Communicates effectively to decision-makers, clinicians and staff Possesses team skills Passion accessed 10/13/16


8 Clinical Leadership Physician Pharmacist Nurse

9 Characteristics of Clinical Leaders Sees problems as opportunities
10 Why Pharmacy Leadership is a Clinical Role Financial Management Multidisciplinary Collaboration Clinical Mind Medication Use Process Human Resources Management Safety and Quality


11 Financial Management Managing and Justifying Pharmacy Expenses Drugs Costly new drugs Exponential increase in generic drug prices People Drug Distribution Clinical Services Automation Robots, automated dispensing machines
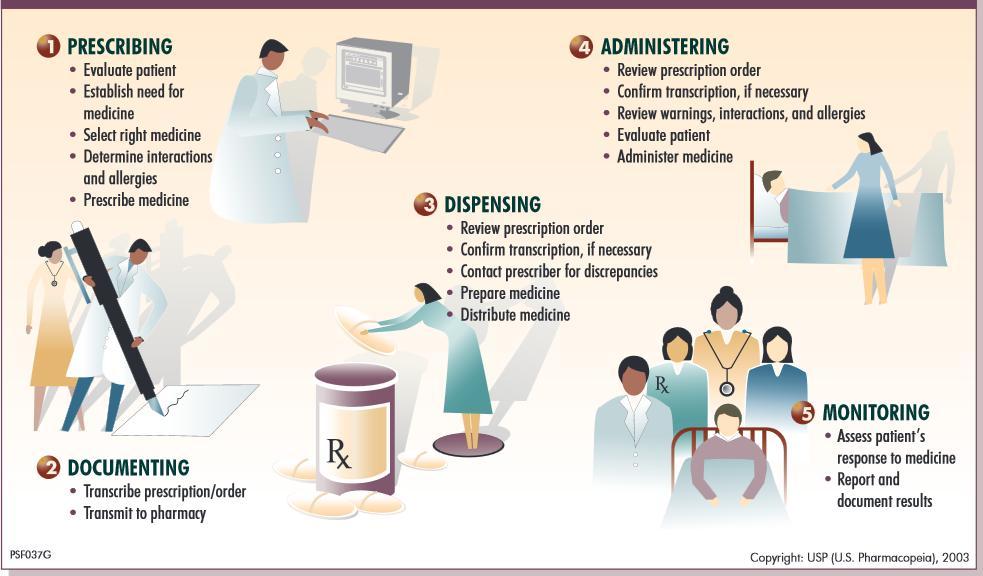
12 Responsibility for the Medication Use Process









13 Medication Use Process PHYSICIANS PHARMACY STAFF Prescriber Order Entry Pharmacist Evaluation and Verification Pharmacy Robot Unit dose packager Liquid packager Infusion Pump Automated Cabinets Med Cart Sterile Compounding Carousel E-MAR Documentation NURSES BCMA
14 Medication Use Process What are the risks at each step? Selection & Procurement Wrong concentration sent by wholesaler-kcl 40meq/15 cc received Preparing & Dispensing Immediate release dispensed instead of sustained release Storage Heparin 10,000 units /ml stocked instead of 100 units/ml Administering Morphine and Hydromorphone -Look alike/sound alike Chlorpromazine given as IV Push Ordering & Transcribing Omitted chemotherapy medication Enoxaprin ordered in pt with renal failure Monitoring Patient on antibiotics; culture and sentiviities show resistance

15 Quality and Safety Underuse Overuse Misuse Healthcare Problems


16 Preventing Medication Errors: $21 Billion Opportunity 1 Average pt >65 is on 15 medications Up to 20% of readmissions are medication-related 700,000 ED visits and 120,000 hospitalizations are due to medications $3.5 billion in annual health care costs to treat adverse drugs events
17 Priorities for Patient-Centered Medication Management Patient care services for all patients Review of lab values to identify drug-related problems Medication reconciliation when pts transfer to a different level of care Daily review of medication profile Patient care services for high risk patients/therapies Pharmacist-managed dosing services Antimicrobial stewardship Focus on critical care, pediatric, oncology, etc.


18 Objectives Priorities for Patient-Centered Medication Management CSMC Clinical Service Plan Ensure consistent approach to clinical services Defines the elements of the initial review and daily review Defines the minimum level of clinical services each patient receives each day Describes the clinical role of pharmacists to Executive Management 18
19 Clinical Service Plan Evaluation of New Orders and Daily Review Drug allergies Review of prior to admission vs current medication list for discrepancies, potential errors Evaluate drug-drug interactions, duplicates, relevant lab orders.. Appropriateness of the drug, dose, frequency, dosage form, route of administration and duration Evaluate drugs with safety warnings Evaluate anticoagulation therapy Target drugs
20 Clinical Service Plan Participate on the Code Blue Team, Code Brain, Participate in rounds (ICUs, Oncology, Pediatrics, Progression of Care etc.) Provide patient education (e.g. CHF, warfarin, antiplatelets) Antimicrobial Stewardship Frail patient evaluation Pharmacist dosing protocols Participate in transitions of care activities 20
21 Human Resources Anything is possible with great people Clinical pharmacy=one individual at a time Knowledge and skills Intellectually curious Committed to learning Passion Professionalism Ensuring competency
22 Ensuring Consistency: Inpatient Competencies Basic life support Code Blue Drug Therapy Stroke and tpa kit Antimicrobials Pharmacokinetics (aminoglycosides/ vancomycin) Medication Safety Anticoagulation Transplant Congestive Heart Failure Assessing renal function Oncology Transitions of Care Pediatrics
23 Supporting Growth Career Ladders to advance patient care and individual growth Pharmacists Technicians Teaching opportunities Setting stretch goals

24 Multidisciplinary Collaboration Every encounter is an opportunity
25 DEMONSTRATING VALUE: Measuring Impact Of Pharmacists Clinical Contributions
26 Pharmacist Evaluation Process for Medication Orders Pharmacist evaluation of medication orders: Prior to Admit Medication List Drug Indication Dose Route Frequency Dosage form Duration Rate Pt Demographics Age (peds/ geriatrics) Gender Ht Wt Allergies Renal/Hepatic Function Current labs Previous admissions Current Medication List Drug-drug interactions Drug-disease interactions Duplicate therapy Contraindications, ADRs, BBW Medications needed but not prescribed Optimize medication therapies Monitoring requirements Prioritization based on: High risk patients or therapies such as: Chemotherapy Pediatrics ICU Anticoagulation Dosing per pharmacy protocol Antimicrobials Medication Dispensed -
27 Categories of Errors Prevented ADR Detected Allergy Drug-Drug Interaction Duplicate Therapy Incompatibility Incomplete Order Omission of Medication on Transfer Recommended Initiation Medication Wrong Rate Wrong Route Wrong Concentration Wrong Dosage Form Wrong Dose Wrong Duration Wrong Frequency Wrong Medication Ordered Wrong Patient

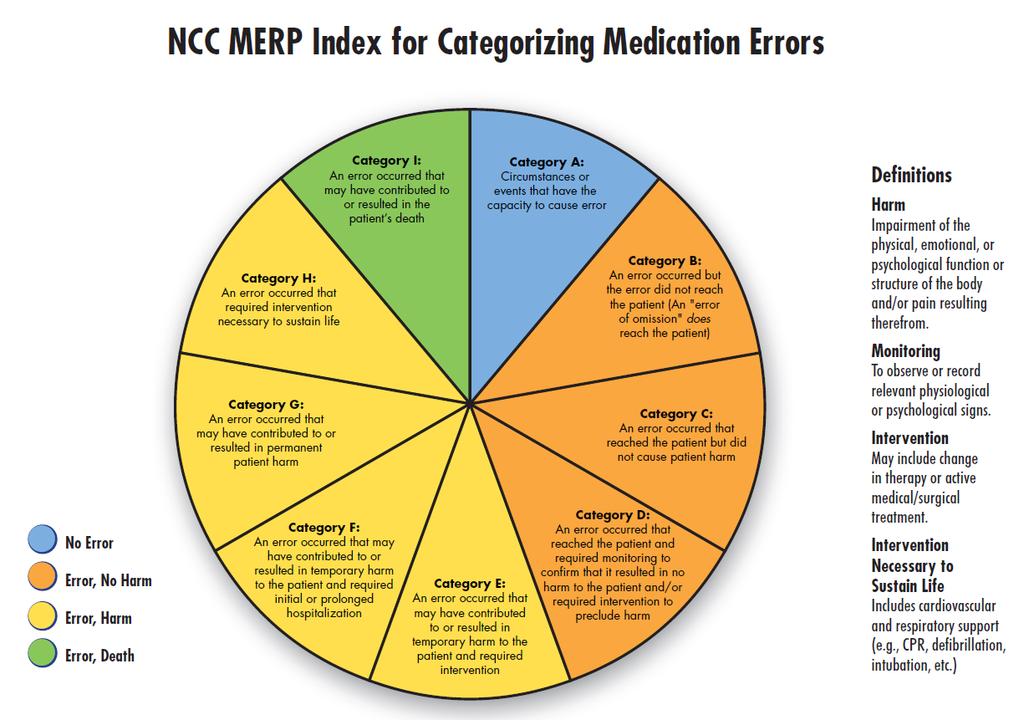
28 Methodology Life Threatening Low Capacity for Harm Serious/Significant 28*
29 Severity of Prescribing Errors Life Threatening Intercepted Based on NCCMERP Category G: The identified and intercepted error may have contributed to or resulted in permanent patient harm Category H: The identified and intercepted error may have required intervention necessary to sustain life Category I: The identified and intercepted error may have contributed to or resulted in the patient s death Serious/Significant Category D: The identified and intercepted error could have reached the patient and would have required monitoring to confirm that it resulted in no harm to the patient and/or required intervention to preclude harm
30 Prescribing Errors Intercepted 2000 Jan'15 - Feb' Life Threatening Serious/Significant Low Capacity for Harm Jan feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb 30
31 Prescribing Errors Prevented Order Ordered clopidogrel 600mg daily MD ordered insulin infusion at a rate of 4.5 units/kg/hr (408 units/hr) Precedex infusion ordered based on weight of 150kg when patient s actual weight was 43kg Drug Related Problem (DRP) Identified & Pharmacist Actions Loading dose ordered as maintenance dose Recommended 600mg x 1, followed by 75mg daily MD meant to order 4.5 units/hr Dose corrected Incorrect patient weight entered in medical record Confirmed actual patient weight and modified Precedex dose Avoided Outcome Potential increased risk of bleeding Potential increased risk of hypoglycemia Potential Precedex overdose and bradycardia 31

32 Ensuring Safe Transitions of Care Patient-Centered Reduce Preventable Admissions Prevent Adverse Drug Events Reduce Length of Stay Medworxx.com, accessed 7/2/14
33 Medication History Errors Lead to Errors During Admission Up to 67% of patients on medications have a medication history error or discrepancy on their medication list 39% of these have the potential to cause moderate to severe harm Evaluation of hospitalized patients demonstrated that >30% had errors in medication orders of which 85% originated from the medication history Shane R. Why Universal Precautions are needed for medication lists. BMJ Qual Saf doi: /bmjqs
34 Medication Errors at Discharge 14-80% of patients experienced at least 1 medication discrepancy or error post-discharge 19% of patients experienced an adverse event within 3 weeks of hospital discharge, 67% were attributed to medications and 12% of the adverse drug events were preventable

++ MedAL: medication adherence and literacy *High")

35 Safe Medication Transitions Methodology Patient meets high risk criteria* Pharmacy staff performs medication reconciliation and assesses MedAL score^ Patients with MedAL score < 6, pharmacist follow up within 72h post discharge Drug-related problems identified are resolved with prescribing MD(s) and/or pt Pharmacists identify pts with significant DRPs that may result in 30d readmission (MACEs)++ MedAL: medication adherence and literacy *High risk criteria: > 10 chronic meds, on anticoagulant, diagnosis of CHF w/ EF< 40%, pneumonia ^MedAL score: CSMC algorithm to assess patient s medication adherence and medication literacy ++Physician validation of likelihood of readmission


36 Post-Discharge Follow Up Results Jan-May 2016 Jan 16 Feb 16 Mar 16 Apr 16 May 16 Number of patients evaluated % significant/lifethreatening Drug- Related Problems 69.6% 72.7% 81.4% 71.0% 73.9% (DRPs)/DRPs total DRPs/pt % readmissions prevented validated by 80.0% 79.4% 85.2% 76.7% 82.6% MDs
 Bradycardia: metoprolol increased to 50mg BID but medication history states 25mg BID.. Pt also started on digoxin. Family reports HR in the 40s.")
37 Examples of Post Discharge (Drug-Related Problems) DRPs Identified and Resolved Case DRPs Identified and Pharmacist s Actions Avoidable MACE CC: 91 yo F w/ PMH of CVA, afib on rivaroxaban, aortic stenosis, seizure, presenting w/ UTI 1) Bradycardia: metoprolol increased to 50mg BID but medication history states 25mg BID.. Pt also started on digoxin. Family reports HR in the 40s. 2) Pt on levofloxacin for 5-day based on dirty UA. Denies symptoms; culture results suggests colonization. 3) Pt prescribed rivaroxaban 20 mg daily. Recommended dose for pt w/ CrCL 29ml/min is 15 mg. Readmission due to bradycardia, bleeding 77 yo F w/ PMH of DM2, CAD, HTN, presenting with w/ hyperglycemia (BG 649 on admission) Recommendations: 1) Recommend hold metoprolol, and D/C digoxin or check level. 2) Recommend D/C levofloxacin 3) Recommend rivaroxaban dose change to 15mg daily. 1) Pt was not using insulin glargine 10 units or checking BG after discharge. Pt reports no insulin or supplies at home. 2) Pt not taking simvastatin Recommendations: 1) Found the most affordable insulin. Educated pt about compliance. 2) Called in prescription for simvastatin, test strips and lancets. Readmission with hyperglycemia due to med non-compliance
38 Safe Medication Transitions Results 7.4 medication history errors/high risk pt on admission Pts with low and intermediate adherence have a 2.54-fold higher odds of readmission compared those with high adherence (p=0.05). 4.3 drug-related problems/patient post-discharge Approximately 50% of problems are pt. related and 50% are prescriber-related High likelihood of readmissions without pharmacist follow up (based on physician validation)

39 Patient-Centered Clinical Leadership Each problem represents an opportunity Committed to Lifelong Learning Creates expectations Team- Focused Demonstrates passion

40
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Background and Methodology
 Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Presentation Outline
 Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016
 Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Hospital Self Assessment Worksheet
 DESCRIPTION AND INSTRUCTIONS This worksheet consists of 106 questions assessing adoption of the Hospital Self- Assessment recommendations at the hospital level. These recommendations were based on the
DESCRIPTION AND INSTRUCTIONS This worksheet consists of 106 questions assessing adoption of the Hospital Self- Assessment recommendations at the hospital level. These recommendations were based on the
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration
 One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Licensed Pharmacy Technicians Scope of Practice
 Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
EMR Adoption: Benefits Realization
 EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
PGY-1 Pharmacy Practice
 Lutheran Health Network PGY-1 Pharmacy Practice Residency Program LHN Pharmacy Residency Program Mission Statement The mission of the LHN Pharmacy Residency Program is to empower pharmacy residents to
Lutheran Health Network PGY-1 Pharmacy Practice Residency Program LHN Pharmacy Residency Program Mission Statement The mission of the LHN Pharmacy Residency Program is to empower pharmacy residents to
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
Nurse Orientation. Medication Management
 Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
MEDICATION USE EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014
 TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
Using MEDMARX for Reporting and Benchmarking. Anne Skinner, RHIA Katherine Jones, PhD, PT
 Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
PGY1 Oncology 2 Advanced Learning Experience
 PGY1 Oncology 2 Advanced Learning Experience Potential Preceptor: Kendra VanHandel, Rani Scranton Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description
PGY1 Oncology 2 Advanced Learning Experience Potential Preceptor: Kendra VanHandel, Rani Scranton Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Medication Safety Dashboard
 How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
IMPACT OF TECHNOLOGY ON MEDICATION SAFETY
 Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
The Joint Commission Medication Management Update for 2010
 The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
Improving Safety Practices Anticoagulation Therapy
 Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
PHARMACY PRACTICE. Residency Program
 PHARMACY PRACTICE Residency Program PGY-1 Pharmacy Practice RESIDENCY OVERVIEW The Pharmacy Practice Residency Program is a comprehensive post-graduate training program that provides unique learning opportunities
PHARMACY PRACTICE Residency Program PGY-1 Pharmacy Practice RESIDENCY OVERVIEW The Pharmacy Practice Residency Program is a comprehensive post-graduate training program that provides unique learning opportunities
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS
 APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
Medication Control and Distribution. Minor/technical revision of existing policy. ± Major revision of existing policy Reaffirmation of existing policy
 Name of Policy: Policy Number: 3364-133-17 Department: Pharmacy Approvingofficer: Chief Executive Officer THE unrversity OF TOLEDO MEDICAL CERITER Responsible Agent: Scope: Director of Pharmacy University
Name of Policy: Policy Number: 3364-133-17 Department: Pharmacy Approvingofficer: Chief Executive Officer THE unrversity OF TOLEDO MEDICAL CERITER Responsible Agent: Scope: Director of Pharmacy University
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Strategies for Successful Medication Reconciliation and Management. Steve Kennedy, PharmD Paula Zelle, PharmD, FASHP
 Strategies for Successful Medication Reconciliation and Management Steve Kennedy, PharmD Paula Zelle, PharmD, FASHP Disclosures The speakers declare no conflicts of interest or financial interest in any
Strategies for Successful Medication Reconciliation and Management Steve Kennedy, PharmD Paula Zelle, PharmD, FASHP Disclosures The speakers declare no conflicts of interest or financial interest in any
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Medication Reconciliation
 Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Strategies for Successful Medication Reconciliation and Management
 Strategies for Successful Medication Reconciliation and Management Steve Kennedy, PharmD Paula Zelle, PharmD, FASHP Disclosures The speakers declare no conflicts of interest or financial interest in any
Strategies for Successful Medication Reconciliation and Management Steve Kennedy, PharmD Paula Zelle, PharmD, FASHP Disclosures The speakers declare no conflicts of interest or financial interest in any
Drug Distribution Services for Long Term Care Facilities. Susan L. Lakey, PharmD 1/11/06
 Drug Distribution Services for Long Term Care Facilities Susan L. Lakey, PharmD 1/11/06 Drug distribution The process: Receipt / transcription of order Interpretation / evaluation of order Filling and
Drug Distribution Services for Long Term Care Facilities Susan L. Lakey, PharmD 1/11/06 Drug distribution The process: Receipt / transcription of order Interpretation / evaluation of order Filling and
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Safety Technology The Good, the Bad and the Unintended Consequences
 Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
PHCY 471 Community IPPE. Student Name. Supervising Preceptor Name(s)
") PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Practice Tools for Safe Drug Therapy
 Practice Tools for Safe Drug Therapy Practice Tools for Safe Drug Therapy Pharmacists and pharmacy technicians make sure the right person gets the right dose of the right drug at the right time and takes
Practice Tools for Safe Drug Therapy Practice Tools for Safe Drug Therapy Pharmacists and pharmacy technicians make sure the right person gets the right dose of the right drug at the right time and takes
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Medication Reconciliation. Peggy Choye, Pharm.D., BCPS
 Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Electronic Prescribing of Chemotherapy-It s Not a Video Game!
 Faculty Disclosures Electronic Prescribing of Chemotherapy-It s Not a Video Game! Mary Mably has no disclosures Mary S. Mably, RPh, BCOP Pharmacy Oncology Coordinator, University of Wisconsin Hospital
Faculty Disclosures Electronic Prescribing of Chemotherapy-It s Not a Video Game! Mary Mably has no disclosures Mary S. Mably, RPh, BCOP Pharmacy Oncology Coordinator, University of Wisconsin Hospital
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology
University of Wisconsin Hospital and Clinics Medication Reconciliation Education Packet
 Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE
 Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP,
Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP,
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Practice Spotlight. Children's Hospital Central California Madera, California
 Practice Spotlight Children's Hospital Central California Madera, California http://www.childrenscentralcal.org Richard I. Sakai, Pharm.D., FASHP, FCSHP Director of Pharmacy Services IN YOUR VIEW, HOW
Practice Spotlight Children's Hospital Central California Madera, California http://www.childrenscentralcal.org Richard I. Sakai, Pharm.D., FASHP, FCSHP Director of Pharmacy Services IN YOUR VIEW, HOW
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Welcome to the New England QIN-QIO Medication Safety Webinar!
 Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
Improving the Patient Experience Through Pharmacy
 Rick Burnett Chief Operating Officer Kenneth Maxik Director, Patient Safety & Pharmacy Compliance Improving the Patient Experience Through Pharmacy August 19, 2015 Speakers Rick Burnett, PharmD, FACHE
Rick Burnett Chief Operating Officer Kenneth Maxik Director, Patient Safety & Pharmacy Compliance Improving the Patient Experience Through Pharmacy August 19, 2015 Speakers Rick Burnett, PharmD, FACHE
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
Preventing Adverse Drug Events and Harm
 Preventing Adverse Drug Events and Harm Frank Federico, RPh, IHI Executive Director Steve Meisel, PharmD, IHI Faculty March 27th,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH, Institute
Preventing Adverse Drug Events and Harm Frank Federico, RPh, IHI Executive Director Steve Meisel, PharmD, IHI Faculty March 27th,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH, Institute
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
MEDCOM Medication Management Discussion
 MEDCOM Medication Management Discussion 2009 MEDCOM-TJC Conference Manager, Army Patient Safety Program Quality Management Office HQ, US Army Medical Command Fort Sam Houston, TX 19 Nov 2009 BRIEFING OUTLINE
MEDCOM Medication Management Discussion 2009 MEDCOM-TJC Conference Manager, Army Patient Safety Program Quality Management Office HQ, US Army Medical Command Fort Sam Houston, TX 19 Nov 2009 BRIEFING OUTLINE
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY
 REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
A Million Little Pieces: Developing a Controlled Substance Diversion Program. Tanya Y. Barnhart, PharmD, BCPS
 A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
Medical Intensive Care Unit Rotation EUHM
 PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
Penn Specialty Pharmacy Program mypennpharmacy bringing the Pharmacy to Patients
 Penn Specialty Pharmacy Program mypennpharmacy bringing the Pharmacy to Patients Richard F Demers, MS, RPh, FASHP Chief Administrative Officer Ambulatory Pharmacy Services University of Pennsylvania Health
Penn Specialty Pharmacy Program mypennpharmacy bringing the Pharmacy to Patients Richard F Demers, MS, RPh, FASHP Chief Administrative Officer Ambulatory Pharmacy Services University of Pennsylvania Health
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
End-to-end infusion safety. Safely manage infusions from order to administration
 End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess.
 - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess.") Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess. Number Outcome SBA SBA-1 SBA-1.1 SBA-1.2 SBA-1.3 SBA-1.4 SBA-1.5 SBA-1.6 SBA-1.7
Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess. Number Outcome SBA SBA-1 SBA-1.1 SBA-1.2 SBA-1.3 SBA-1.4 SBA-1.5 SBA-1.6 SBA-1.7
Medication Management: Is It in Your Toolbox?
 Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Patient Safety and Quality Measures for CRRT: The UAB Experience. Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012
 Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
High Alert Medications: Reducing Patient Harm
 High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Neurocritical Care Rotation - EUH
 Preceptor: Bill Asbury, B.S., Pharm.D. Office: EUH- EG35 Hours: ~ 8:00am-4:30pm Desk: 404-712-7491 Pager: 404-686-5500 pic 14028 ICU cell phone: 404-326-8256 PGY-2 Residency Training Program Neurocritical
Preceptor: Bill Asbury, B.S., Pharm.D. Office: EUH- EG35 Hours: ~ 8:00am-4:30pm Desk: 404-712-7491 Pager: 404-686-5500 pic 14028 ICU cell phone: 404-326-8256 PGY-2 Residency Training Program Neurocritical
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Management and Use. Anadolu Medical Center. August, Departman Tarih
 Medication Management and Use Anadolu Medical Center August, 2014 Departman Tarih Medication Management and Use standards (MMU) Organization and Management 1. Medication use in the hospital is organized
Medication Management and Use Anadolu Medical Center August, 2014 Departman Tarih Medication Management and Use standards (MMU) Organization and Management 1. Medication use in the hospital is organized
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L
 Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Medication Safety & Electrolyte Administration. Objectives. High Alert Medications. *Med Safety Electrolyte Administration
 Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Objective Competency Competency Measure To Do List
 2016 University of Washington School of Pharmacy Institutional IPPE Checklist Institutional IPPE Team Contact Info: Kelsey Brantner e-mail: ippe@uw.edu phone: 206-543-9427; Jennifer Danielson, PharmD e-mail:
2016 University of Washington School of Pharmacy Institutional IPPE Checklist Institutional IPPE Team Contact Info: Kelsey Brantner e-mail: ippe@uw.edu phone: 206-543-9427; Jennifer Danielson, PharmD e-mail:
Adapting Practice to Keep Pace with Changes in Health Care. Change in Health Care. Professional Responsibilities?
 Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Session Objectives. Medication Errors in Adults and Children. Dennis Quaid American Society of Health- System Pharmacists (ASHP) Meeting December 2009
 Meeting December 2009") Medication Errors in Adults and Children Carly C. Feldott, PharmD Medication Safety Program Director, VUMC Amy L. Potts, PharmD, BCPS Assistant Director, Monroe Carell, Jr. Children s Hospital at Vanderbilt
Medication Errors in Adults and Children Carly C. Feldott, PharmD Medication Safety Program Director, VUMC Amy L. Potts, PharmD, BCPS Assistant Director, Monroe Carell, Jr. Children s Hospital at Vanderbilt
Introduction to Pharmacy Practice
 Introduction to Pharmacy Practice Learning Outcomes Compare & contrast technician & pharmacist roles Understand licensing, certification, registration terms Describe advantages of formal training for technicians
Introduction to Pharmacy Practice Learning Outcomes Compare & contrast technician & pharmacist roles Understand licensing, certification, registration terms Describe advantages of formal training for technicians
Pharmacy Services in the Emergency Department
 Pharmacy Services in the Emergency Department Targeting the Highest Risk Patients Kunal Gohil Specialist Clinical Pharmacist Emergency Department Nottingham University Hospitals NHS Trust When all else
Pharmacy Services in the Emergency Department Targeting the Highest Risk Patients Kunal Gohil Specialist Clinical Pharmacist Emergency Department Nottingham University Hospitals NHS Trust When all else