The Power of One: Impacting Patient Outcomes by Returning to the Basics
|
|
|
- Kerry Patrick
- 5 years ago
- Views:
Transcription



1 The Power of One: Impacting Patient Outcomes by Returning to the Basics Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net Northville Michigan ADVANCING NURSING LLC 2017


2 Disclosures for Kathleen Vollman Consultant-Michigan Hospital Association Keystone Center Consultant/Faculty for CUSP for MVP AHRQ funded national study Subject matter expert for CAUTI and CLABSI for CMS/HEN 1.0 & 2.0 Consultant and speaker bureau for Sage Products LLC Consultant and speaker bureau for Hill-Rom Inc Consultant and speaker bureau for Eloquest Healthcare
3 Session Objectives Create the link of patient advocacy to the basic nursing care Define key fundamental evidence based nursing care practices that reduce non-vent HAP and Safely improve in-bed and out of bed mobility for the patient and caregiver Discuss strategies to overcome barriers
4 Notes on Hospitals: 1859 It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sick no harm. Florence Nightingale Advocacy = Safety


5 PROTECT THE PATIENT FROM BAD THINGS HAPPENING ON YOUR WATCH
6 Interventional Patient Hygiene Hygiene the science and practice of the establishment and maintenance of health Interventional Patient Hygiene.nursing action plan directly focused on fortifying the patients host defense through proactive use of evidence based hygiene care strategies Incontinence Associated Dermatitis Prevention Program
7 INTERVENTIONAL PATIENT HYGIENE(IPH) VAP/HAP Oral Care/ Mobility HAND Patient HYGIENE Catheter Care Skin Care/ Bathing/Mobility CA-UTI CA-BSI SSI Falls HASI Vollman KM. Intensive Crit Care Nurs, 2013;22(4):
8 Achieving the Use of the Evidence Factors Impacting the ability to Achieve Quality Nursing Outcomes at the Point of Care Vollman KM. Australian Crit Care, 2009;22(4): Value Attitude & Accountability NSO
9 Building Resiliency Into Interventions Forcing functions and constraints Automation and computerization Strongest Standardization and protocols Checklists and independent check systems STRENGTH OF INTERVENTION Rules and policies Education and information 9 Weakest Vague warnings Be more careful!
10 Why HAI's? Protecting Patients From Harm Estimates: 183 Hospitals in 10 States HAI: 722,000/year HAI-related deaths: 75,000/year Hospitalized patients develop infection: 1 out of 25 (4%) Death due to sepsis/septic shock: 700/day Money spent: $45 billion/year Increase risk of 27days vs. 59 days readmission: Magill SS, et al. New England Journal of Med, 2014;370:
11 Health Care Associated Infection Data Measurement NHSN Acute Care Hospitals HAP/per 1000 patient days Estimated # of Infections *157,500 (21.8%) VAP/per 1000 vent days Range of pooled means 0.2 (Ped CVICU) -4.4 (Burn ICU) *49,900 CLA-BSI/per 1000 cath days MBI-LCBI excluded CA-UTI/per 1000 cath days Range of pooled means 0.0 (Prenatal )-2.9 (Burn ICU) Step-down 0.6 (Adult)-1.4 (Peds) Range of pooled means 0.0 (Peds Surgical)-4.8 (Burns) Stepdown 0.8 (Peds) 1.7 (Adults) Dudek MA, et al Am J Infect Control,2015;43: *Magill SS, et al. New England Journal of Med, 2014;370: *15,600 *35,600
12 Economic Burden of HAI s: Build The Business Case Zimlichman E, et al. JAMA Intern Med, 2013; 173: Generated point estimates for attributable cost & LOS 5 Major Infections=9.8 billion SSI s, CLABSI s, VAP/VAE, CAUTI s, C-Diff SSI s (33.7%) 50% VAP (31.6%) HAI s CLA-BSI (18.9%) Preventable C-Diff (15.4%) CA-UTI <1% Per Case Basis SSI CLABSI VAP CAUTI C-Diff $20,785 $45,814 $40,144 $896 $11,285
13 Missed Nursing Care Any aspect of required patient care that is omitted (either in part or whole) or significantly delayed. A predictor of patient outcomes Measures the process of nursing care
 Am Jour Med Quality, 26(4), 291-299.")
14 Hospital Variation in Missed Nursing Care Kalish, R. et al. (2012) Am Jour Med Quality, 26(4),
. TJC Jour Qual Patient Safety,38(4), 161-167.")
15 Patient Perceptions of Missed Nursing Care Kalisch, B et al. (2012). TJC Jour Qual Patient Safety,38(4),
16 Source Control: The Oral Cavity as a Risk Factor in NV-HAP and VAP
17 Build the Will: NV-HAP? HAP 1st most common HAI in U.S. Increased morbidity 50% are not discharged back home Increased mortality 18%-29% Extended LOS 4-9 days Increased Cost $28K to $109K 2x likely for readmission <30 day Slide courtesy of Barb Quinn Kollef, M.H. et.al. (2005). Chest. 128, ATS, (2005). AmJ Respir Crit Care Med. 171, Lynch (2001) Chest. 119, 373S-384S. Pennsylvania Dept. of Public Health (2010).
18 Compelling Incidence Data Study Incidence Mortality +LOS Cost J. Davis (2012) Pennsylvania HCUP National database (P) 5,600 /3 yrs 18.9% Not queried $28,000 2/100 pts 14.5% 4 days $36,400 CDC (2014) 13% of all HAIs 19%-50% 4-9 days $40,000 Slide courtesy of Barb Quinn Davis, Pt Safety Authority (3). Giuliano,K. et al. (2016) APIC Podium 2016 Magill, S.S. et.al. (2014) NEJM. 370(13), p
19 Hospital-Acquired Pneumonia: Non-Ventilated versus Ventilated Patients in Pennsylvania Purpose: Compare VAP and NV-HAP incidence, outcomes Methods: Pennsylvania Database queried All nosocomial pneumonia data sets ( ) Retrieved on 4/24/13 from

20 Results: Mortality Incidence Total deaths Total cost Wide spread Retrieved on 4/24/13 from
21 Incidence, Prevalence of NV-HAP: A Local Study (2010) Purpose: Determine incidence and clinical factors of NV-HAP Method: Descriptive, quasi-experimental study using retrospective data Inclusion criteria: All adult discharges ICD-9 codes of pneumonia not POA AND met CDC definition of HAP Quinn, B., Baker, D., et. al. (2013). Journal of Nursing Scholarship.


22 NV HAP SMCS Research Findings: ,482 patients and 94,247 patient days Incidence: 115 adults 62% non-icu 50% surgical Average age 66 Common comorbidities: CAD, COPD, DM, GERD Common Risk Factors: Dependent for ADLs (80%) CNS depressant meds (79%) Cost: $4.6 million 23 deaths Mean Extended LOS 9 days 1035 extra days Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19
23 Impact of NV-HAP in the ICU HAPPI-2 Preliminary Data 23 hospitals in U.S.; 2014 data; 1306 total cases 28% occurred in ICU 26% occurred on Med/Surg units and were transferred to ICU 54% of all NV-HAP cases spend some time in the ICU 33% transferred to ICU died 42% transferred to ICU survived but were discharged to a higher level of care; 25% home Impact of NV-HAP on one year mortality: Any length of time spent in an ICU increases mortality of elderly patients who survive to discharge Slide courtesy of Barb Quinn Quinn & Baker (2016) pend. Pub. Vivek et al. (2016) CC Med,
24 Methods: ICU-Acquired pneumonia: VAP vs. NV-HAP Prospective study of 135 consecutive episodes over 3 years of adults with ICU-acquired pneumonia Compared clinical and microbiological characteristics of VAP and NV- HAP Results for VAP & NV-HAP were not statistically different: Pathogens Comorbid conditions, Severity parameters, Mortality, and Hospital length of stay Among NV-HAP patients, 79 (52%) needed subsequent intubation Slide courtesy of Barb Quinn Esperatti et al (2010) Am J Respir Crit Care Med. Vol 182, p
25 Where is the Highest Risk for NV-HAP? 2.5 Rate of Nonventilator Hospital- Acquired Pneumonia Vent Med/Surg NV-ICU 0 Vent Med/Surg NV-ICU NV-HAP per 1000 patient days Slide courtesy of Barb Quinn
26 Preventing NV-HAP Through Evidence Based Fundamental Nursing Care Strategies



27 Pathogenesis Prevention Germs in Mouth Dental plaque provides microhabitat Bacteria replicate 5X/24 hrs Aspirated into Lungs Most common route 50% of healthy adults micro-aspirate in sleep Weak Defenses Poor cough Immunosuppressed Multiple co-morbidities Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19
28 Micro Aspiration During Sleep in Healthy Subjects Prospective duplicate full-night studies 10 normal male s yrs of age Methods: Radioactive 99 mtc tracer inserted into the nasopharynx Lung scans conducted immediately following final awakening No difference in sleep efficacy btwn 2 study nights Results: 50% of subjects had tracer in the pulmonary parenchyma upon final awakening No difference in age, time spent in bed, efficacy of sleep, apnea-hyponea index, arousal plus awakening index or % sleep in the supine position between subjects that aspirated and those that did not. Gleeson K, et al. Chest. 1997;111:

29

30 AACN Procedural Manual-6 th ed Procedure 4: Endotracheal Tube Care and Oral Care Authors: Kathleen M Vollman Mary Lou Sole Barbara Quinn
31 Risk Factors for Oral Bacteria in the Hospital Poor oral health in the U.S. (CDC, 2011) Increased bacteria counts Plaque, gingivitis, tooth decay Reduced salivary flow hours for HAP pathogens in mouth If aspirated =100,000,000 bacteria/ml saliva into lungs Scannapieco FA, Stewart EM, Mylotte JM. Colonization of dental plaque by respiratory pathogens in medical intensive care patients. Crit Care Med. 1992;20: Langmore, S. et.al. (1998). Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. 13,

32 Oral Cavity & VAP 89 critically ill patients Examined microbial colonization of the oropharynx through out ICU stay Used pulse field gel electrophoresis to compare chromosomal DNA Results: Diagnosed 31 VAPs 28 of 31 VAP s the causative organism was identical via DNA analysis Garrouste-Orgeas et. al. Am J Respir Crit Care Med. 1997;156: elderly nursing home residents admitted to the hospital Examined baseline dental plaque scores & microorganism within dental plaque Used pulse field gel electrophoresis to compare chromosomal DNA Results 14/49 adults developed pneumonia 10 of 14 pneumonias, the causative organism was identical via DNA analysis El-Solh AA. Chest. 2004;126:

33 Formation of Biofilm Over 13 Hours Loesche, W. 2012
34 Impact of Oral Care on HAP Kaneoka A, et al Infect. Control Hosp. Epidemiol, 2015;36(8):
35 Current Evidence for Oral Care Procedure Method: Review of 7 RCTs and 1 meta-analysis Results: Toothbrushing removes dental plaque; swabs do not. Chlorhexidine reduces oropharyngeal colonization Chlorhexidine interventions reduce rate of VAP Optimal frequency of basic oral care unknown Slide courtesy of Barb Quinn Halm, A. Amer J Crit Care ,
36 SMCS HAP Prevention Plan Phase 1: Oral Care Formation of new quality team: Hospital-Acquired Pneumonia Prevention Initiative (HAPPI) New oral care protocol to include non-ventilated patients New oral care products and equipment for all patients Staff education and in-services on products Ongoing monitoring and measurement Monthly audits Quinn B, et al. J of Nursing Scholarship, 2014, 46(1):11-19
37 Gap Analysis Best Practice Our Gaps Action To Take Comprehensive oral care for all (CDC, SHEA) Oral CHG (0.12%) periop adult CV surgery and vent pts. (CDC, ATS, IHI). ICU vent patients only Not using CHG on these patients. Develop inclusive oral care protocol Added to preprinted orders, and to protocol Therapeutic oral care tools (ADA) Poor quality oral care tools. Absence of denture care supplies. New tools and supplies. Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19
 Package instructions 4 X / day Dependent / Vent ICU Suction toothbrush kit (6) Package instructions 6 X / day Dentures Tools + Cleanser Adhesive Remove dentures & soak Brush gums,")
38 Protocol Plain & Simple Patient Type Tools Procedure Frequency Self Care / Assist Brush, paste, rinse, moisturizer Provide tools Brush 1-2 minutes Rinse 4 X / day Dependent / Aspiration Risk Suction toothbrush kit (4) Package instructions 4 X / day Dependent / Vent ICU Suction toothbrush kit (6) Package instructions 6 X / day Dentures Tools + Cleanser Adhesive Remove dentures & soak Brush gums, mouth Rinse 4X / day Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19
39 Provide Meaningful Data 4.0 SGH Ortho - Association of Mean Oral Care to HAP Frequency Number HAP Cases Mean Oral Care 3 Ortho Unit had ZERO HAP cases in the last 4 months of 2013!! Great WORK!! 2 HAP Cases Mean Oral Care Remember, the goal is to provide and document oral care after each meal and before bedtime. Used with permission from Barbara Quinn
40 JAN 2010 FEB 2010 MAR 2010 APR 2010 MAY 2010 JUN 2010 JUL 2010 AUG 2010 SEP 2010 OCT 2010 NOV 2010 DEC 2010 MAY 2012 JUN 2012 JUL 2012 AUG 2012 SEP 2012 OCT 2012 NOV 2012 DEC 2012 JAN 2013 FEB 2013 MAR 2013 APR 2013 MAY 2013 JUN 2013 JUL 2013 AUG 2013 SEP 2013 Number of non-ventilator HAP cases OCT 2013 NOV 2013 DEC 2013 NV-HAP Incidence 50 % Decrease from Baseline Baseline Control chart for NV-HAP January 2010 to December 2013 Oral Care Month/Year Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19 UCL Average LCL


41 Open Heart Surgery Patients: NV HAP Reduced 75% Oral chlorhexidine periop started Used with permission from Barbara Quinn
42 Return on Investment 60 NV-HAP avoided Jan 1 Dec $2,400,000 cost avoided - 117,600 cost increase for supplies $2,282,400 return on investment 8 lives saved Quinn, B. et al. Journal of Nursing Scholarship, (1):11-19
43 Patient Early Mobility
44 Immobility Risk Skin Risk Factors Mobility, Skin & Fall Prevention Strategies Care Giver Risk Moisture Clean & Protect Repetitive motion, Lifting Pressure Shear Friction Deconditioni ng Falls Delirium ICU and H it llos Reduce Pressure & Shear Safe Handling Inbed Exercise & Out of Bed Mobility Repetitive motion, Lifting & Limb holding Repetitive motion, Dragging, patient weight
 or medical (22%) with a median of 16 beds (12 24) 34% dedicated PT or OT for the ICU Performed a median of 6 days, 52% began on admission Factors associated Factors Associated with with EMP:")
45 Environmental Scan of EM Practices 687 randomly selected ICU s stratified by regional density & size responded (73% response rate) Demographics: 51% academic affiliation, mixed medical/surgical (58%) or medical (22%) with a median of 16 beds (12 24) 34% dedicated PT or OT for the ICU Performed a median of 6 days, 52% began on admission Factors associated Factors Associated with with EMP: EMP: Dedicated PT/OT PT/OT Written sedation protocol Daily MDR MDR Daily Written Goals Daily written goals Bakhru RN, et al. Crit Care Med 2015; 43:

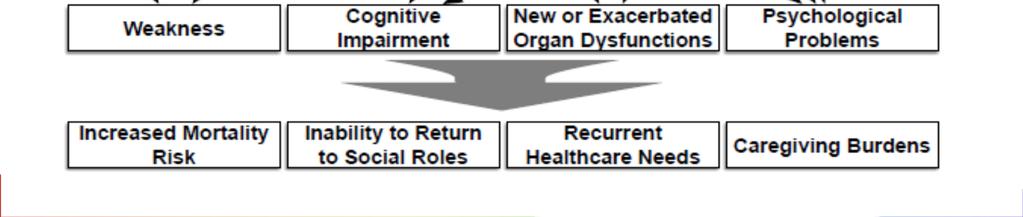
46 Consequences of Acute Illness and Immobility Consequences of Acute Illness and Immobility Courtesy of Jack Iwashya

47 Oh, My Aching Back! Back Pain Incidence in Nursing: 8 out of 10 nurses work despite experiencing musculoskeletal pain 1 62% of nurses report concern developing a disabling musculoskeletal injury 1 56% of nurses report musculoskeletal pain is made worse by their job 1 Nursing assistants had the 2 nd highest and RNs had the 6 th highest number of musculoskeletal disorders in the U.S American Nurses Association. (2013). ANA Health and Safety Survey. Retrieved from HealthSafetySurvey.html 2. U.S. Department of Labor, Bureau of Labor Statistics. (2014). Table 16. Number, incidence rate, and median days away from work for nonfatal occupational injuries and illnesses involving days away from work and musculoskeletal disorders by selected worker occupation and ownership, Retrieved from
48 What is the Incidence & Cost? Body Part Incidence Cost Back 51.3% $8700 Avg Shoulder 20.1% $13,400 Avg Wrist 6.7% Arm 4.2% $8500 Avg Knee 4.0% $11,300 Avg Neck $12,700 Avg
49 Hospital Acquired Skin Injury HAPU are the 4 th leading preventable medical error in the US 2.5 million patients are treated annually in Acute Care NDNQI data base: critical care: 7% med-surg: 1-3.3% Acute care: 0-12%, critical care: 3.3% to 53.4% (International Guidelines) Most severe pressure injury: sacrum (44.8%) or the heels (24.2%) 60,000 persons die from pressure injury complications each yr. National health care cost $11 billion annually Dorner, B., Posthauer, M.E., Thomas, D. (2009), Whittington K, Briones R. Advances in Skin & Wound Care. 2004;17: Reddy, M,et al. JAMA, 2006; 296(8): Vanderwee KM, et al., Eval Clin Pract 13(2): National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention & treatment of pressure ulcers :clinical practice guideline. Emily Haesler (Ed) Cambridge Media: Osborne Park: Western Austrlia;2014.
50 START HERE Includes complex, intubated, hemodynamically unstable and stable intubated patients; may include non-intubated Progressive Mobility Continuum Includes intubated, non intubated hemodynamically stable/stabilizing, no contraindications Perform Initial mobility screen w/in 8 hours of ICU admission Reassess mobility level at least every 24 hours (Recommended at shift Δ) Refer to the following criteria to assist in determining mobility level o PaO2/FiO2 > 250 o Peep <10 o O2 Sat > 90% o RR o No new onset cardiac arrythmias or ischemia o HR >60 <120 o MAP >55 <140 o SBP >90 <180 o No new or increasing vasopressor infusion o RASS > 3 NO Start at level I* YES Start at level II and progress* LEVEL I LEVEL II LEVEL III LEVEL IV LEVEL V RASS -5 to - 3 RASS -3 & up RASS -1 & up Goal: clinical stability; passive ROM ACTIVITY: HOB > 30º *Passive ROM 2X/d performed by RN, or UAP CLRT/Pronation initiated if patient meets criteria based on institutional practice OR Q 2 hr turning Tolerates Level I Activities Goal: upright sitting; increased strength and moves arm against gravity PT consultation prn OT consultation prn ACTIVITY: Q 2 hr turning *Passive /Active ROM 3x/d 1. HOB 45º X 15 min. 2. HOB 45º,Legs in dependant position X 15 min. 3. HOB 65º,Legs in dependant position X 15 min. 4. Step (3) & full chair mode X20 min. 3X/d Or Full assist into cardiac chair 2X/day Tolerates Level II Activities Goal: Increased trunk strength, moves leg against gravity and readiness to weight bear PT: Active Resistance Once a day, strength exercises OT consultation prn ACTIVITY: Self or assisted Q 2 hr turning 1.Sitting on edge of bed w/rn, PT, RT assist X 15 min. 2.Progressive bed sitting Position Min.20 min. 3X/d Or Pivot to chair position 2X/d Tolerates Level III Activities RASS 0 & up Goal: stands w/ min. to mod. assist, able to march in place, weight bear and transfer to chair PT x 2 daily OT consult for ADL s ACTIVITY: Self or assisted Q 2 hr turning 1.Bed sitting Position Min.20 min. 3X/d; 2.Sitting on edge of bed; stand w/ RN, PT, RT assist 3.Active Transfer to Chair (OOB) w/ RN/PT/RT assist Min. 3X/d Tolerates Level IV Activities RASS 0 & up Goal: Increase distance in ambulation & ability to perform some ADLs PT x 2 daily & OT x1 daily ACTIVITY: Self or assisted Q 2 hr turning 1.Chair (OOB) w/ RN/PT/RT assist Min. 3X/day 2.Meals consumed while dangling on edge of bed or in chair Ambulate progressively longer distances with less assistance x2 or x3/day with RN/PT/RT/UAP For each position/activity change allow 5-10 minutes for equilibration before determining the patient is intolerant ***If the patient is intolerant of current mobility level activities, reassess and place in appropriate mobility level*** *Mobility is the responsibility of the RN, with the assistance from the RT s Unlicensed Assistive Personnel and PT/ OT. PT and OT may assist the team with placement to the appropriate mobility level of activity, always prioritizing patient and provider safety. Placement is based on clinical judgment.
 2012 Apr;28(2):88-97 Needham DM, et al. Arch PhStaudinger t, et al. Crit Care Med, 2010;38.")
:1874-82. Thomsen GE, et al. CCM 2008;36;1119-1124 Winkelman C et al, CCN,2010;30:36-60 Azuh O, et al. The American Journal of Medicine, 2016, doi:10.")
51 Outcomes of Early Mobility Programs incidence of VAP time on the ventilator days of sedation incidence of skin injury delirium ambulatory distance Improved function in hospital readmissions Bassett RD, et al.intensive Crit Care Nurs (2012) 2012 Apr;28(2):88-97 Needham DM, et al. Arch PhStaudinger t, et al. Crit Care Med, 2010;38. Abroung F, et al. Critical Care, 2011;15:R6 Morris PE, et al. Crit Care Med, 2008;36: Pohlman MC, et al. Crit Care Med, 2010;38: Schweickert WD, et al. Lancet, 373(9678): Thomsen GE, et al. CCM 2008;36; Winkelman C et al, CCN,2010;30:36-60 Azuh O, et al. The American Journal of Medicine, 2016, doi:10.106/jmjmed
52 Systematic Review of Early Systematic Review of Early Rehabilitation in the IC Rehabilitation in the ICU 14 studies/1753 patients 880 patients in intervention group 873 patient in control group Varying methodologies Results No difference in short or long term mortality Tipping CJ, et al. ICM, 2017;43:
53 Systematic Review of Early Rehabilitation in the ICU Systematic Review of Early Rehabilitation in the ICU Results of Active Rehab muscle mass at ICU d/c probability of walking without assistance at hospital d/c more days alive and out of hospital 180 days Limitations Variation in dosage, small sample sizes of individual studies Tipping CJ, et al. ICM, 2017;43:

:35-8, 40-7 http://www.iculiberation.")
54 A ASSESS, PREVENT & MANAGE PAIN B BOTH/SAT & SBT C CHOICE OF ANALGESIA & SEDATION D DELIRIUM E F EARLY MOBILITY FAMILY ENGAGEMENT & EMPOWERMENT Balas MC, et al. Crit Care Nurse Apr;32(2):35-8,

55 ABCDEF Bundle: Improving Survival & Reducing Brain Dysfunction ABCDEF Bundle: Improving Survival & Reducing Brain Dysfunction Ventilated and non-ventilated medical and surgical ICU patients enrolled between January 1, 2014 and December 31, 2014 Determine association between ABCDEF bundle compliance/total & partial & outcomes of hospital survival and deliriumfree and coma-free days/ adjusting for age, severity of illness, and presence of mechanical ventilation Patients experienced more days alive and free of delirium and coma with both total bundle compliance (incident rate ratio, 1.02; 95% CI, ; p = 0.004) and partial bundle compliance (incident rate ratio, 1.15; 95% CI, ; p < 0.001). 10% in total bundle compliance, patients had a 7% higher odds of hospital survival Barnes-Daly, MA, et. al. Crit Care Med, 2017;45:



56 It Takes a Village for Sustainability It Takes a Village For Sustainability 1. Necessary Components for Early Rehab Buy-in Multiple disciplines Team communication Opinion leader Individual discipline champion Dedicated rehab personnel Equipment Sedation practice Administrative funding 2. Implementation Strategies Team center approach Staff education Strength & quality of evidence 3. Perceived Barriers Increased workload Safety concerns 4. Positive Outcomes Improved patient outcomes Staff satisfaction Changed culture Financial savings Eakin MN, et al. J of Crit Care, 2015;30:
57 Early Mobility + Skin Prevention & Safe Patient Handling In-Bed Mobility & Out of Bed Mobility
58 Achieving the Use of the Evidence For In-Bed Mobility Factors Impacting the ability to Achieve Quality Nursing Outcomes at the Point of Care Resource & System Breathable glide sheet/stays Foam Wedges Microclimate control Reduce layers of linen Wick away moisture body pad Protects the caregiver Value Attitude & Accountability Vollman KM. Intensive Care Nurse.2013;29(5):250-5


59 Comparative Study of Two Methods of Turning & Positioning Non randomized comparison design 59 neuro/trauma ICU mechanically ventilated patients Compared SOC: pillows/draw sheet vs turn and position system (breathable glide sheet/foam wedges/wick away pad) Measured PU incidence, turning effectiveness & nursing resources Demographic Comparison Powers J, J Wound Ostomy Continence Nur, 2016;43(1):46-50
60 Comparative Study of Two Methods of Turning & Positioning Results: Nurse satisfaction 87% versus 34% 30 turn achieved versus 15.4 in SOC/7.12 degree difference at 1hr (p<.0001) SOC PPS P PU development 6 1 a.04 # of times patients pulled up in bed # of staff required to turn patient < a PU development with 24hrs of admission Powers J, J Wound Ostomy Continence Nur, 2016;43(1):46-50
61 Impact of a Turn & Position Device on PI & Staff Time Prospective, QI study (1 SICU & 1MICU) 2 phases SOC: pillows, underpads, standard low airloss bed and additional staff if required Interventional: turn and position system, a large wicking pad (part of the product) Inclusion criteria: newly admitted, non-ambulatory, required 2 or more to assist with turning/repositioning Turning procedures were timed/admitting till ICU discharge Results No difference in sociodemographic and clinical data between the groups Phase 1: 14 patients (28%) Stage II sacral PI Phase 2: zero sacral PI (p<.0001) Timing: Phase 1: mins (range 4-60min) SD= Phase 2: 3.58 mins (range ) SD = 2.31 (p=0.0006) Hall KD, et al. Ostomy Wound Management, Nov 2016:40-44
")

62 Reducing HAPI & Patient Handling Injuries Compared pre-implementation turning practice: pillows/draw sheet vs turn and position system (breathable glide sheet/foam wedges/wick away pad) Baseline: November August 2012 Implementation period: November 2012 to August patients Compared HAPI rates, patent handling injuries and cost 74% reduction Way H, Am JSPHM, 2016;6(4):
63 Evidence Based Strategies for Safe Patient Handling Salsbury S. Presented at AACN s National Teaching Institute, May 16 th -19 th, New Orleans, LA.





64 In-Bed Technology

65 Current Seating Positioning Challenges Airway & Epiglottis compressed Body Alignment Shear/Friction Sacral Pressure Frequent repositioning & potential caregiver injury Potential risk of sliding from chair


66 Repositioning Patients in Chairs: An Improved Method (SPS) Study the exertion required for 3 methods of repositioning patients in chairs 31 care giver volunteers Each one trial of all 3 reposition methods Reported perceived exertion using the Borg tool, a validated scale. Method 1: 2 care givers using old method of repositioning 246% greater exertion than SPS Method 2: 2 caregivers with SPS Method 3: 1 caregiver with SPS 52% greater exertion than method 2 Fragala G, et al. Workplace Health & Safety;61:

67 Early Mobility: Can We Do It? Is it Safe?
68 Safety > 1 % adverse events during 1449 sitting, standing and walking sessions with patients on ventilators. Underwent daily sedation interruption followed by PT & OT daily until achieving physical function independence Safety events occurred in 16% of all sessions Loss of 1 arterial line, 1 nasogastric tube, 1 rectal tube Therapy was stopped on 4% of all sessions for vent asynchrony, agitation, or both Delirium present 53% of the time during therapy sessions Bailey P, et al. Crit care Med, 2007;35: Pohlman MC, et al. Crit Care Med, 2010;38:
 Hemodynamic")
")

69 Challenges to Mobilizing Critically Ill Patients Potentially Modifiable Barriers Patient related barriers (50%) Hemodynamic instability, ICU devices, physical & neuropysch Structural (18%) Human or Technological Resources ICU culture (18%) Knowledge/Priority/Habits Process related (14%) Service delivery/lack of coordination Clinician function Dubb R, et al, Annual ATS, 2016 in press
70 Hemodynamic Instability??? Is it a Barrier to Positioning? 50% reported in studies as the # 1 patient barrier
71 The Role of Hemodynamic Instability in Positioning 1,2 Lateral turn results in a 3%-9% decrease in SVO 2, which takes 5-10 minutes to return to baseline Appears the act of turning has the greatest impact on any instability seen Minimize factors that contribute to imbalances in oxygen supply and demand Factors that put patients at risk for intolerance to positioning: 3 Elderly Diabetes with neuropathy Prolonged bed rest Low hemoglobin and cardiovascular reserve Prolonged gravitational equilibrium 1.Winslow EH, et al. Heart Lung. 1990;19: Price P. Dynamics. 2006;17: Vollman KM. Crit Care Nurs Q. 2013;36:17-27
72 Decision-Making Tree for Patients Who Are Hemodynamically Unstable With Movement 1,2 Screen for mobility readiness within 8 hrs of admission to ICU & daily initiate in-bed mobility strategies as soon as possible Is the patient hemodynamically unstable with manual turning? O 2 saturation < 90% New onset cardiac arrhythmias or ischemia HR < 60 <120 MAP < 55 >140 SPB < 90 >180 New or increasing vasopressor infusion Yes Is the patient still hemodynamically unstable after allowing 5-10 minutes adaption post-position change before determining tolerance? Yes Screen for mobility readiness within 8 hrs of admission to ICU & daily initiate inbed mobility strategies as soon as possible Yes Has the manual position turn or HOB elevation been performed slowly? Yes Initiate continuous lateral rotation therapy via a protocol to train the patient to tolerate turning No No No No Begin in-bed mobility techniques and progress out-of-bed mobility as the patient tolerates Begin in-bed mobility techniques and progress out-of-bed mobility as the patient tolerates Allow the patient a minimum of 10 minutes of rest between activities, then try again to determine tolerance Try the position turn or HOB maneuver slowly to allow adaption of cardiovascular response to the inner ear position change HOB=head of bed; HR=heart rate; MAP=mean arterial pressure; SPB=systolic blood pressure. Vollman KM. Crit Care Nurse. 2012;32: Vollman KM. Crit Care Nurs Q. 2013;36:17-27.
73 Evidence Based Strategies to Overcome Barriers Patient related Inclusion, exclusion criteria, protocols, research on specific equipment for safety (CCRT, etc.) Structural Development and implementation of protocols, increase staffing & purchase of equipment ICU culture Education, training, coaching, video s, improve coordination between professionals Process related Interprofessional meetings and rounds, sharing clinical responsibility, collaboration with champions, remove default orders Dubb R, et al, Annual ATS, 2016 in press


74 Cultural Adaptation to Increase Sustainability Vollman KM, Bassett R. Transforming the Culture: The Key to Hardwiring Early Mobility & Safe Patient Handling. Amer Nurse Today, 2014, September

75 It is not enough to do your best; you must know what to do, and THEN do your best. ~ W. Edwards Deming
76 Driving Change Gap analysis Build the Will Protocol Development Structure Make it Prescriptive Overcoming barriers Daily Integration Process Outcomes
77 Targeting to Zero!!!!
78 Be Courageous We all are responsible for the safety of our patients Own the Issues If not this, then what?? If not now, then when? If not me, then who??
Nurse-Driven Safe Patient Early Mobility: Making it Happen In Your ICU
 Nurse-Driven Safe Patient Early Mobility: Making it Happen In Your ICU Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net
Nurse-Driven Safe Patient Early Mobility: Making it Happen In Your ICU Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net
Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions
 Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator /
Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator /
The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia
 The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
Do No Harm: Mitigating Risk Factors for Ventiltor and Non Ventilator Pneumonia
 Do No Harm: Mitigating Risk Factors for Ventiltor and Non Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
Do No Harm: Mitigating Risk Factors for Ventiltor and Non Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Objectives 10/3/16. Transforming Collegial Relationships in Critical Care. Disclosures
 Transforming Collegial Relationships in Critical Care Kathleen M Vollman, MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Consultant ADVANCING NURSING LLC kvollman@comcast.net www.vollman.com ADVANCING
Transforming Collegial Relationships in Critical Care Kathleen M Vollman, MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Consultant ADVANCING NURSING LLC kvollman@comcast.net www.vollman.com ADVANCING
Do No Harm: Evidence Based Basic Nursing Care Strategies to Impact Patient Outcomes. Disclosures
 Do No Harm: Evidence Based Basic Nursing Care Strategies to Impact Patient Outcomes Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING kvollman@comcast.net
Do No Harm: Evidence Based Basic Nursing Care Strategies to Impact Patient Outcomes Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING kvollman@comcast.net
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Intact Skin is In: Bundling Evidence Based Strategies to Reduce Hospital Acquired Skin Injury while Protecting the Caregiver
 Intact Skin is In: Bundling Evidence Based Strategies to Reduce Hospital Acquired Skin Injury while Protecting the Caregiver Kathleen M Vollman, MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Consultant
Intact Skin is In: Bundling Evidence Based Strategies to Reduce Hospital Acquired Skin Injury while Protecting the Caregiver Kathleen M Vollman, MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Consultant
2/20/2017. Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator
 Barbara Quinn, RN, ANCS-BC Sutter Medical Center, Sacramento, CA Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator The story of May and how we began this
Barbara Quinn, RN, ANCS-BC Sutter Medical Center, Sacramento, CA Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator The story of May and how we began this
Can nurses Compliance to Ventilator Care Bundle Help to Prevent Ventilator Associated Pneumonia in ICU? Mok Chi Man, RN (SP) ICU, PYNEH, HKEC
 ICU, PYNEH, HKEC") Can nurses Compliance to Ventilator Care Bundle Help to Prevent Ventilator Associated Pneumonia in ICU? Mok Chi Man, RN (SP) ICU, PYNEH, HKEC 1 Introduction Ventilator-associated pneumonia (VAP): Lung
Can nurses Compliance to Ventilator Care Bundle Help to Prevent Ventilator Associated Pneumonia in ICU? Mok Chi Man, RN (SP) ICU, PYNEH, HKEC 1 Introduction Ventilator-associated pneumonia (VAP): Lung
Raise your game: The UP Campaign. Bruce Spurlock, M.D. Cynosure Health
 Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Champion the Skin and Win:
 Champion the Skin and Win: Eliminating Pressure, Shear and Moisture Risk Factors to Eliminate Hospital Acquired Skin Injuries Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant
Champion the Skin and Win: Eliminating Pressure, Shear and Moisture Risk Factors to Eliminate Hospital Acquired Skin Injuries Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Get UP to Drive Harm Down. ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health
 Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Back to the Basics: Good Nursing Care Saves Lives
 Back to the Basics: Good Nursing Care Saves Lives Kathleen M. Vollman MSN, RN, CCNS, FCCM Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net www.vollman.com Northville,
Back to the Basics: Good Nursing Care Saves Lives Kathleen M. Vollman MSN, RN, CCNS, FCCM Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING LLC kvollman@comcast.net www.vollman.com Northville,
THE INTERVENTIONAL PATIENT HYGIENE COMPANY
 THE INTERVENTIONAL PATIENT HYGIENE COMPANY Born from a core belief in prevention, Interventional Patient Hygiene is a nursing action plan focused on fortifying patients host defenses with evidence-based
THE INTERVENTIONAL PATIENT HYGIENE COMPANY Born from a core belief in prevention, Interventional Patient Hygiene is a nursing action plan focused on fortifying patients host defenses with evidence-based
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Conflict of Interest Disclaimer. The Affordable Care Act. The Affordable Care Act. Caring for the Critically Ill. The Affordable Care Act
 Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
Conflict of Interest Disclaimer Reducing Risks of Harmful Events in the Critically Ill I have no financial interests or conflicts of interest related to this talk Alfred F. Connors, Jr., MD Chief Medical
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Alaina Tellson, PhD, RN-BC, NE-BC
 Alaina Tellson, PhD, RN-BC, NE-BC Localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure or pressure in combination with shear and/or friction tional
Alaina Tellson, PhD, RN-BC, NE-BC Localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure or pressure in combination with shear and/or friction tional
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Preventing ICU Complications. Lee-lynn Chen, MD Assistant Clinical Professor UCSF Department of Anesthesia and Perioperative Care
 Preventing ICU Complications Lee-lynn Chen, MD Assistant Clinical Professor UCSF Department of Anesthesia and Perioperative Care Overview Catheter related bloodstream infection Ventilator associated pneumonia
Preventing ICU Complications Lee-lynn Chen, MD Assistant Clinical Professor UCSF Department of Anesthesia and Perioperative Care Overview Catheter related bloodstream infection Ventilator associated pneumonia
Early Progressive Mobility- Letting Go of Bedrest
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs. June 13, 2018
 Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs June 13, 2018 1 Agenda Morning Welcome Get UP as a cross cutting strategy to reduce harm 12:00-12:30
Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs June 13, 2018 1 Agenda Morning Welcome Get UP as a cross cutting strategy to reduce harm 12:00-12:30
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Reducing Ventilator Associated Pneumonia (V.A.P) System and Patient Tracer
 System and Patient Tracer") Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Beyond the Bundle. Improving Ventilator Related Outcomes through Multidisciplinary Collaboration
 Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
Use of TeleMedicine to Improve Clinical and Financial Outcomes
 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning
 MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning Presented by: Nika Carlson, MSN, RN, Director of Clinical and Quality Improvement Jennifer Castro, MSN,
MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning Presented by: Nika Carlson, MSN, RN, Director of Clinical and Quality Improvement Jennifer Castro, MSN,
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
The impact of nighttime intensivists on medical intensive care unit infection-related indicators
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Interventional Patient Hygiene: Impacting Patient Outcomes By
 Interventional Patient Hygiene: Impacting Patient Outcomes By Returning to the Basics Disclosures Sage Products Speaker Bureau & Consultant Hill-Rom Inc Speaker Bureau & Consultant Merck Speaker Bureau
Interventional Patient Hygiene: Impacting Patient Outcomes By Returning to the Basics Disclosures Sage Products Speaker Bureau & Consultant Hill-Rom Inc Speaker Bureau & Consultant Merck Speaker Bureau
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation
 Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
PRESSURE ULCER PREVENTION
 PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
Missed Nursing Care: Errors of Omission
 Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
The Use of Patient Audits and Nurse Feedback to Decrease Postoperative Pulmonary Complications
 The Use of Patient Audits and Nurse Feedback to Decrease Postoperative Pulmonary Complications Christine M. Schleider, RN, BSN Adam P. Johnson, MD, MPH Kathleen M. Shindle, RN, BSN Scott W. Cowan, MD,
The Use of Patient Audits and Nurse Feedback to Decrease Postoperative Pulmonary Complications Christine M. Schleider, RN, BSN Adam P. Johnson, MD, MPH Kathleen M. Shindle, RN, BSN Scott W. Cowan, MD,
Reducing Hospital Acquired Pressure Ulcers in the ICU
 Reducing Hospital Acquired Pressure Ulcers in the ICU Joanne Matukaitis, MSN, RN, NE-BC Christiana Care Health System Newark, Delaware 1 Christiana Care Health System 2 Title goes here 1 Opportunity for
Reducing Hospital Acquired Pressure Ulcers in the ICU Joanne Matukaitis, MSN, RN, NE-BC Christiana Care Health System Newark, Delaware 1 Christiana Care Health System 2 Title goes here 1 Opportunity for
Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU)
") Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU) Nihar Bhatia Head Quality Assurance & Fortis Operating System and Prateem Tamboli, Facility Director, Fortis Escorts Hospital
Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU) Nihar Bhatia Head Quality Assurance & Fortis Operating System and Prateem Tamboli, Facility Director, Fortis Escorts Hospital
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Subject: Skilled Nursing Facilities (Page 1 of 6)
") Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Key Steps in Creating & Sustaining Excellence
 Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Columbus Regional Hospital Pressure Ulcer Prevention
 Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study
 Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Progressive Mobility at AUMC
 Progressive Mobility at AUMC Why do we need Progressive Mobility Program? National Data shows that Mobility Programs: Reduces hospital LOS/reduces ICU LOS Reduces Ventilator days Reduces Pneumonia/VAP
Progressive Mobility at AUMC Why do we need Progressive Mobility Program? National Data shows that Mobility Programs: Reduces hospital LOS/reduces ICU LOS Reduces Ventilator days Reduces Pneumonia/VAP
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION
 EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
Prone Positioning Protocol
 Prone Positioning Protocol Objectives To illustrate patient criteria for prone positioning as an adjunct therapy in the treatment of Acute Respiratory Distress Syndrome (ARDS) To review the exclusion and
Prone Positioning Protocol Objectives To illustrate patient criteria for prone positioning as an adjunct therapy in the treatment of Acute Respiratory Distress Syndrome (ARDS) To review the exclusion and
Helen Kenedi, M.S., CCC-SLP Jenny Reynolds, M.S., CCC-SLP JoBeth Vance, M.S., CCC-SLP
 Helen Kenedi, M.S., CCC-SLP Jenny Reynolds, M.S., CCC-SLP JoBeth Vance, M.S., CCC-SLP Disclosure Helen Kenedi, Jenny Reynolds, and JoBeth Vance have no financial or nonfinancial disclosures and do not
Helen Kenedi, M.S., CCC-SLP Jenny Reynolds, M.S., CCC-SLP JoBeth Vance, M.S., CCC-SLP Disclosure Helen Kenedi, Jenny Reynolds, and JoBeth Vance have no financial or nonfinancial disclosures and do not
Pay-for-Performance: Approaches of Professional Societies
 Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
Pay-for-Performance: Approaches of Professional Societies CCCF 2011 Damon Scales MD PhD University of Toronto Disclosures 1.I currently hold a New Investigator Award from the Canadian Institutes for Health
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Marianne Chulay is a critical care nursing/clinical research consultant in Chapel Hill, NC. The author has no financial relationships to disclose.
 VAP is a common and potentially fatal complication of ventilator care. Following the latest CDC recommendations is the best defense you can offer your patients. Marianne Chulay, RN, DNSC, FAAN Marianne
VAP is a common and potentially fatal complication of ventilator care. Following the latest CDC recommendations is the best defense you can offer your patients. Marianne Chulay, RN, DNSC, FAAN Marianne
19th Annual. Challenges. in Critical Care
 19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU. Dr David Ng Paediatric Medical Officer Sarawak General Hospital
 Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Best Practices for Prevention of Ventilator Associated Pneumonia. Marti Shaver, RN, CIC Derreck Wallace, RRT Ruth Sidor, MSN APRN
 Best Practices for Prevention of Ventilator Associated Pneumonia Marti Shaver, RN, CIC Derreck Wallace, RRT Ruth Sidor, MSN APRN North Decatur Hillandale Downtown Decatur DeKalb Regional Health System
Best Practices for Prevention of Ventilator Associated Pneumonia Marti Shaver, RN, CIC Derreck Wallace, RRT Ruth Sidor, MSN APRN North Decatur Hillandale Downtown Decatur DeKalb Regional Health System
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Safe Patient Handling:
 Safe Patient Handling: The Hazards of Immobility Prepared by : Learning Objectives Discuss the opportunity for quality improvement using SPHM practices Discuss expected positive patient outcomes using
Safe Patient Handling: The Hazards of Immobility Prepared by : Learning Objectives Discuss the opportunity for quality improvement using SPHM practices Discuss expected positive patient outcomes using
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Case: Comparing Two Scenarios
 The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
Key prevention strategies for MRSA bacteraemia: a case study. Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta
 Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
Exemplary Professional Practice: Patient Care Delivery Model(s)
") Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Harm Across the Board Reporting: How your Hospital Can Get There
 Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Selecting Measures. Presented by: Rebecca Lash, PhD, RN Collaborative Outcomes Council July 2016
 Selecting Measures Presented by: Rebecca Lash, PhD, RN Collaborative Outcomes Council July 2016 Content adapted from Robert Martin, PsyD, Performance Excellence & Dr. Moira Inkelas Methods for Improvement
Selecting Measures Presented by: Rebecca Lash, PhD, RN Collaborative Outcomes Council July 2016 Content adapted from Robert Martin, PsyD, Performance Excellence & Dr. Moira Inkelas Methods for Improvement
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY
 MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
Jennifer A. Meddings, MD, MSc
 CAUTI progress reports: How was this data collected? Jennifer A. Meddings, MD, MSc University of Michigan Medical School Disclosures: Research Grant Funding: AHRQ, BCBSFM Honorariums: SHEA, RAND, CSCR
CAUTI progress reports: How was this data collected? Jennifer A. Meddings, MD, MSc University of Michigan Medical School Disclosures: Research Grant Funding: AHRQ, BCBSFM Honorariums: SHEA, RAND, CSCR
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
ROTOPRONE THERAPY SYSTEM. with people in mind.
 ROTOPRONE THERAPY SYSTEM with people in mind www.arjohuntleigh.com THE CLINICAL CHALLENGE: MINIMIZING MORTALITY AND POTENTIAL COMPLICATIONS IN ARDS PATIENTS WHILE MAKING IT EASIER TO DELIVER PRONE THERAPY
ROTOPRONE THERAPY SYSTEM with people in mind www.arjohuntleigh.com THE CLINICAL CHALLENGE: MINIMIZING MORTALITY AND POTENTIAL COMPLICATIONS IN ARDS PATIENTS WHILE MAKING IT EASIER TO DELIVER PRONE THERAPY
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage