Operational Policy. Peninsula Major Trauma Network. Authors
|
|
|
- Randolph Warner
- 5 years ago
- Views:
Transcription

1 Peninsula Major Trauma Network Operational Policy Authors Mark Jadav Michele Ahearne Date approved 25 th October 2016 Date circulated Review date August 2017 August 2016 V6 1
2 Contents Introduction 3 Philosophy of Care 5 Principal Network Stakeholders 6 Network Governance Arrangements 7 Patient Profile 9 Pre-hospital Provision 10 Pre-Hospital Enhanced Care 13 Network Admission and Operational Policy 14 Network Transfer Policy 17 Trauma Nurse Co-ordinators 19 Network Massive Transfusion Policy 20 Network Spinal Policy 20 Adult and Paediatric Imaging Guidelines 20 Tele-radiology 21 Discharge/Repatriation Policy 22 Access to Rehabilitation Services 23 Trauma Network Director of Rehabilitation 23 MTC Rehabilitation Lead 23 TU Rehabilitation Lead 23 Rehabilitation Co-ordinator 23 Directory of Rehabilitation Services 23 Rehabilitation Services 24 Rehabilitation Referral Process 25 Rehabilitation Prescription 26 Paediatrics 27 Network Documentation 28 Audit and Research 29 TARN 30 Service, Evaluation and Feedback 33 Staff Support, Training and Development 34 Emergency Planning 35 Network Communications 36 Appendix 1 (PTN Clinical Policies) 39 Appendix 2 (NICE Guidance) 40 Appendix 3 (MTC Dashboards Measures) 41 Appendix 4 (Major Trauma Network Leads) 42 Appendix 5 (PTN Group Membership) 44 Glossary 45 Useful Websites 46 2

3 Introduction The Peninsula Trauma Network is a largely rural region (see map in appendix 1) with very few centres with a large urban population. The cities of Plymouth and Exeter are the largest two centres and their populations are only 258,000 and 123,400 respectively. Although there are relatively few sizeable urban areas there are quite a few pockets of severe deprivation in Plymouth, Torquay and South West Cornwall. The overall population of the region is approximately 1.67million. This can increase by an extra 1 million people in the peak holiday season. 30% of the total population are over 60 years of age and 2014/15 TARN data showed that 63% of major trauma have a fall under 2m as their mechanism of injury. There are currently substantial areas of expansion and development at Cranbrook near Exeter which should generate 6,550 homes by 2026 and Sherford near Plymouth which should generate 5,500 homes by Geographically, the Peninsula is varied, encompassing an area of 3,970 square miles including Dartmoor, Exmoor, and Bodmin moor, as well as the Isles of Scilly, Guernsey and Lundy. The Peninsula is approximately 134 miles from east to west and 70 miles from north to south. The length of coastline for both counties is one of the longest in England at 743 miles. There are 12,542 miles of road within the Peninsula and with the exception of a 22 mile section of the M5 between Exeter and the Devon/Somerset border, these are all A, B or unclassified Roads, (Figure 2 shows the 60 minute isochrones for the Peninsula). The Peninsula Trauma Network is built around the hub-and-spoke model shown in Figure 1. The Peninsula Trauma Centre at Derriford Hospital, Plymouth and the Paediatric Major Trauma Centre at Bristol Children s Hospital provide Major Trauma Centre (MTC) services. Trauma Units are situated at the Royal Devon & Exeter Hospital, Torbay Hospital, North Devon District Hospital in Barnstaple and Royal Cornwall Hospital in Truro (see appendix 3 for network configuration). Figure 1 Major Trauma Networks configuration for NHS South 3

4 There are no other emergency departments within the region. There are, however, minor injury units, walk in centres and urgent care centres which whilst not included within the Trauma Network are part of the new Urgent Care Network. Figure 2 60 minute road travel isochrone for PTC The topology of the Peninsula contributes to some sizeable travel times from scene to MTC. For example, from Porthcurno in Cornwall to the MTC in Plymouth, a distance of 88 miles, takes 2hrs 17 mins by road, or from East Prawle in the South Hams to the MTC in Plymouth, 29.5 miles, takes 1hr 09 mins. As can be seen from Figure 2 a significant percentage of the network is outside of the 60 min bypass timeframe from the MTC. Figure 2 clearly demonstrates how much of the region is dependent on the Trauma Units and even though the bypass time has changed to 60 mins from the original 45 mins this does not change the Networks reliance on the TU s. It is also worth noting that an area in North Cornwall and Northwest Devon is outside of the 60min bypass time for either a TU or the MTC. Rehabilitation services across the peninsula include one Level 2a and two Level 2b neurorehabilitation units. There are several community hospitals providing generic rehabilitation and many community teams providing a variety of rehabilitation services. There is a currently a Peninsula Rehabilitation, Reablement & Recovery Project that is being run by the Southwest Strategic Clinical Network of which there a number of representatives from the Peninsula on the group including Dr Rachel Botell (PHNT) and Jude Fewings (PTN). There is currently a bed audit ongoing for the South West Peninsula. 4
5 Philosophy of Care The Peninsula Trauma Network, through its constituent members, seeks to uphold the 7 Guiding Principles of the NHS for major trauma patients: 1. The Network will provide a comprehensive major trauma service available to all. We will take responsibility for influencing the services that you access at the point of injury, through reception in hospital, to definitive care and rehabilitation. 2. Access is based on clinical need alone. We will strive to ensure that wherever you are, and whoever you are, you will be able to access the trauma services you require. 3. The Network aspires to the highest standards of excellence and professionalism. We will support and encourage our providers in developing their services to match the best available standards nationally and internationally. In return our providers will be held accountable by us for the standard of service and care they provide. 4. The Network aspires to put patients at the heart of everything it does. We will aim to develop our services around the needs of the patients, not around the needs or structures of the provider organisations. We will engage patients in our Network, from patient representation in advisory groups for governance, service planning and development, to ensuring regular feedback from patients about their experiences. 5. The Network works across organisational boundaries, in partnership with other organisations in the interests of patients, local communities and the wider population. We recognise the multiplicity of services and providers, both funded and voluntary, stateowned and private, which are involved in providing major trauma care. We will work with all necessary providers to ensure the interests of patients are met. 6. The Network is committed to providing best value for money and the most effective, fair and sustainable use of finite resources. We recognise that trauma care comes at a price. We will work with national and regional structures to develop cost-effective solutions to the challenges facing us. 7. The Network is accountable to the public, communities and patients that it serves. We will maintain transparency through public access to TARN summaries, peer review reports and Freedom of Information requests. We will demonstrate accountability through the PTN Executive Board and the Operational Delivery Network framework via the Regional Operational Delivery Network Oversight Group. 5
6 Principal Network Stakeholders The Network is made up of a range of local health providers including pre-hospital, acute and community based services. The following are the main members of the Network: Pre-hospital South Western Ambulance Service NHS Foundation Trust (SWASFT) Devon Air Ambulance Trust Cornwall Air Ambulance Trust Bristows Search and Rescue Service HM Coastguard Devon & Cornwall BASICS Acute Hospitals Plymouth Hospitals NHS Trust (Adult MTC) Peninsula Trauma Centre Bristol Royal Hospital for Children (Paediatric MTC) Northern Devon Healthcare NHS Trust (TU) Royal Cornwall Hospitals NHS Trust (TU) Royal Devon and Exeter NHS Foundation Trust (TU) Torbay & South Devon Healthcare NHS Foundation Trust (TU) Community Northern Devon Healthcare NHS Trust Peninsula Community Health - Cornwall Live well (Southwest) - Plymouth Torbay & South Devon Healthcare NHS Foundation Trust Rehabilitation Plym Neurological Rehab Unit (Level 2a) Mardon Neuro-Rehabilitation Centre (Level 2b) Marie Therese House Neuro-rehabilitation unit ( Level 2b) All other Rehabilitation facilities are included in the Networks Directory of Rehabilitation Services 6
7 Network Governance Arrangements The Peninsula Network Reports to its host Trust (Plymouth Hospitals NHS Trust) as per national policy. The Network Governance Pathway can be viewed as figure 3. The Network itself has the following boards/groups: Executive Board Clinical Advisory Group Rehabilitation Group The Trauma Network Executive Board has a membership that is composed of a senior executive from the MTC and each of the Trauma units, principle Pre-hospital services and local commissioning CCG s. The chair of the Executive Board will normally be a senior executive from outwith the Network management team or that of the MTC. Clinical Governance occurs regularly at all levels throughout the system There are weekly clinical governance meetings in the MTC and all TUs for hot case review and longitudinal audit of key performance indicators. and the minutes of the MTC Weekly case reviews are circulated, for information, through the Network using the same mailing list as for the PTN Governance Teleconference. Each trust lead to cascade this information within their TU. Every MTC trauma death is reviewed at the monthly Major Trauma Centre Management Committee meeting by a multi-disciplinary group. Issues in clinical care or process are identified and rectified. There is a well-established monthly PTN teleconference at which cases from each TU are discussed in detail from point of injury through to discharge. SWASFT hosts regular pre-hospital trauma governance meetings at which cases identified as requiring review are discussed. Individual air ambulance organisations host monthly internal governance meetings. The MTC holds trust-wide clinical governance meetings 6-monthly at which clinical problems are highlighted and discussed. An invite to this has been extended across the Network. The PTN also hosts 6-monthly governance meetings at which cases of ISS >15 not transferred and deaths are reviewed. Minutes and distillation of lessons learned from these meetings are distributed. A recent addition to the governance process has been paediatric governance, with Bristol Children s Hospital MTC. In addition to the BCH monthly case-discussion meetings there will soon be regular case review teleconferences. Twice a year a cross network M & M meeting is held to discuss cases from both PTN and STN. Representatives from the Paeds MTC and network participate in PTN monthly teleconferences, as required, when an injured child is discussed. In 2015 a SouthWest Operational Delivery Networks Oversight Board was established by NHS England South to work alongside and actively engage with stakeholder groups and organisations including; NHS England, Major Trauma Clinical Reference Group (CRG), 7

8 National Major Trauma Peer Review team and other areas where there is the opportunity to develop a national profile regarding the impact and benefit for patients of Critical Care & Major Trauma ODNs. The Peninsula Trauma Network will be one of the 6 Networks represented. Network Member Governance Figure 3 Network member organisations should have a full governance process that will incorporate: Morbidity and Mortality Risk management Case review Issue/incident investigation All reviews or investigations must be recorded or logged, via the PTN office, to ensure clarity. Any Serious Untoward Incidents (SUI) should be investigated using the usual process for the organisation involved. The Network Governance Lead must be kept advised of the investigation at the appropriate points. A copy of the final report should be sent to the Network office. Figure 3 shows the Peninsula Trauma Network Governance framework. All Network member organisations should work within the network policies and NICE Guidance as listed in Appendix 1 and 2. 8
9 Patient Profile The overall population of the region is approximately 1.57 million, increasing by up to an extra 1 million people during the peak holiday season. This population is steadily growing and with the development of 2 new towns in Devon (Cranbrook, Nr Exeter and Sherford, Nr Plymouth) is set to grow even further. Population, over 60 years for Peninsula Trauma Network 30% of the total network population are over 60s years of age with 12% of them being over the age of % of the overall population are under the age of 10. Figure 4 gives a breakdown, by Unitary Authority, of the Network population: Peninsula Area Total Under 10yrs Cornwall 541,300 56, ,800 16,400 Devon 773,100 79, ,700 27,500 Plymouth 261,546 30,365 59,126 5,942 Torbay 133,000 14,100 42,800 5,100 Total 1,708, , ,426 59,942 The average wage across the Peninsula is below the national average. There are only a few industrial complexes in the region, most of which are based in or around the large conurbations. Most of the region s employment is based around tourism, healthcare, farming and the armed forces. There are areas of deprivation within the Peninsula, with high unemployment and increased mortality: West Cornwall (Redruth/Cambourne) Plymouth Torbay Figure 4 Pre-hospital Provision Ambulance Services within the Peninsula Trauma Network are solely provided by Southwest Ambulance Service NHS Foundation Trust. SWASFT work closely with the air ambulance charities to provide paramedics on rotary-wing aircraft within the region. They also work in close conjunction with Bristow s, the current Search and Rescue provider, to support their operations and utilise their resources to optimise rescue and transfer capabilities within the region. The Peninsula Trauma Network is very fortunate to have extremely good provision of rotary wing air services. The current services are described below: Service Base Type of Helicopter No on 9
10 (From 2016) Cornwall Air Ambulance Trust Devon Air Ambulance Trust Bristow s Search & Rescue Service Bristow s Search & Rescue Service Devon and Cornwall Police Force Newquay International Airport Eaglescott Air Field, N. Devon. Exeter International Airport RAF St Athan, South Wales Newquay International Airport Exeter International Airport Site MD902 Explorer 2 Eurocopter EC135s Eurocopter EC135s Agusta Westland AW189 Sikorsky S Sikorsky S-92 2 Eurocopter EC145 1 Helicopter Services The Devon Air Ambulance was first established in By March 2014 they had flown over 20,600 missions with their two helicopters which are based at Exeter International Airport and Eaglescott Airbase in North Devon. The service is currently provided by Paramedics, although there are a small minority of shifts that include Doctors who fly with them on a voluntary basis. They have expanded their flying time, up to 14 hours per day, in the summer from 2012 and there are plans to expand into night operating within the next 2-3 years. The Cornwall Air Ambulance was established in in 1987 and was the first of its kind in the UK. Since then they have flown over 24,000 missions with their helicopter which is based at Newquay airport. They are able to reach the majority of Cornwall within 20 minutes and the Isles of Scilly within 30 minutes. Their service is also currently provided by Paramedics although again there are a small minority of shifts that include Doctors who fly with them on a voluntary basis, but it is also not a HEMS model. The charity has just taken delivery of two new helicopters that are capable of night flying and as a first step towards a 24/7 service they have extended their operating hours to 12 hours plus per day in the summer of The primary role of the Search & Rescue service is to provide a maritime search and rescue service that covers a 200 mile radius from their base, including the Western Approaches of the Atlantic, the Southerly portion of the Irish Sea and the Western end of the English Channel. As well as this they also provide this Search & Rescue service to the population of Devon, Cornwall, Somerset, Dorset and South Wales. The Devon and Cornwall Police Helicopter provides a service primarily at night when currently the air ambulances do not, as yet, fly. This is purely from the scene of an incident to the nearest TU or MTC. Helicopter Control centres Both Air Ambulances are controlled through a Helicopter Emergency Medical Service s (HEMS) Dispatch Desk, based at the SWASFT control room in Exeter, and which is manned 10
11 by a dedicated dispatcher, whose sole task is to deploy the Air Ambulances for Devon, Cornwall, Dorset & Somerset, Wiltshire and the Great Western Air Ambulance. This HEMS desk became operational in 2007 and while hosted by SWASFT the costs are shared between the Air Ambulance charitable trusts. The Search and Rescue teams from Bristows that are based at Newquay international Airport in Cornwall and RAF St Athan in South Wales are tasked via the UK Aeronautical Rescue Coordination Centre (UKARCC) at RAF Kinloss in Scotland. It is planned that this service will move to the UK Coastguard base in Southampton during As well as primary rescue and retrieval they can offer aeronautical transfer for NHS patients from TU to MTC within the Southwest or to specialist centres outside of the region. This service is chargeable back to the appropriate patients CCG via SWASFT and as such this should no bearing on whether to use the service or not. Patients will also, occasionally, be received from the east of the region, via the Coastguard/Bristows helicopter stationed at Lee-on-Solent in Hampshire. This helicopter is also tasked by the UKARCC. Hospital Helipads All of the Hospitals within the Peninsula Trauma Network have helipads. The type and availability is variable: Hospital Helipad 24/7 Weather Station Derriford Hospital Yes (SAR & AA) Yes Yes North Devon District Hospital Yes (SAR & AA) 24/7 + transfer No Royal Cornwall Yes (1 x SAR) Pad 1-24/7 + transfer Hospital Yes (1 x AA) Pad 2 - Daylight only Yes Royal Devon & Exeter Hospital Yes (1 x AA) Daylight only No Torbay Hospital Daylight only + Yes (1 x AA) transfer No Air Transfers Currently both of the air ambulance trusts and the search and rescue team helicopters will undertake transfers from the TU s to the MTC. In addition to this, where necessary, they will also undertake transfers out of area. Primarily out of area transfers will be either to Morriston Hospital, Swansea (Regional Burns Centre) or Bristol Royal Hospital for Children. Morriston Hospital (Burns Centre) There is a specific process to follow for helicopter transfers to Morriston Hospital, Swansea, South Wales. It is very important that the following telephone number is used to communicate with the Emergency Department staff by the TU/MTC to advise them of the transfer: Telephone Number:
12 The Emergency Department staff will then make contact with the on-site portering/security services to facilitate the patients arrival. The helicopter landing site will need an ambulance to transfer a patient from the helipad to the hospital. This needs to be arranged by the transferring trust through their Clinical Contact Centre: Telephone Number: Bristol Royal Hospital for Children (BRHC) There is a helipad on the roof of the Bristol Royal Infirmary which is the adjoining building and there is a dedicated lift that will take the patient to the courtyard opposite the BRHC ED entrance. This helipad is only rated for air ambulance size helicopters and nothing larger. If a transfer is undertaken using a larger aircraft i.e. a Sea King or Bristows helicopter, then the flight must go to the helipad at Southmead Hospital (MTC), Bristol where a road transfer of approximately 20 minutes will then be required. Transfer charges The air ambulance charities do not charge for the transfer of trauma patients to an out of area hospital as it is part of their mandate. However the Bristows search and rescue service does charge for out of area transfers. This charge is covered by the patients CCG. Discussions are ongoing between the Network and Bristow s S&R service to clarify and finalise service level details. Pre-Hospital Enhanced Care (T16-2A-103) There is currently a limited Pre-hospital enhanced care provision within this Network. This consists of: BASICS - BASICS South West was formed in March 2010 as an umbrella group for the immediate care schemes working with SWASFT. BASICS provides a network of volunteer doctors across the region with training in the emergency management of trauma and medical conditions outside hospital. They respond to incidents at the request of ambulance control. The doctors are available on-call 24 hours a day, seven days a week and perform this role in addition to their "day jobs" which are predominantly in general practice, anaesthetics and emergency medicine (A&E). This purely a voluntary role and is not part of the Doctors job plans. Currently 29 Drs make up this group. 12
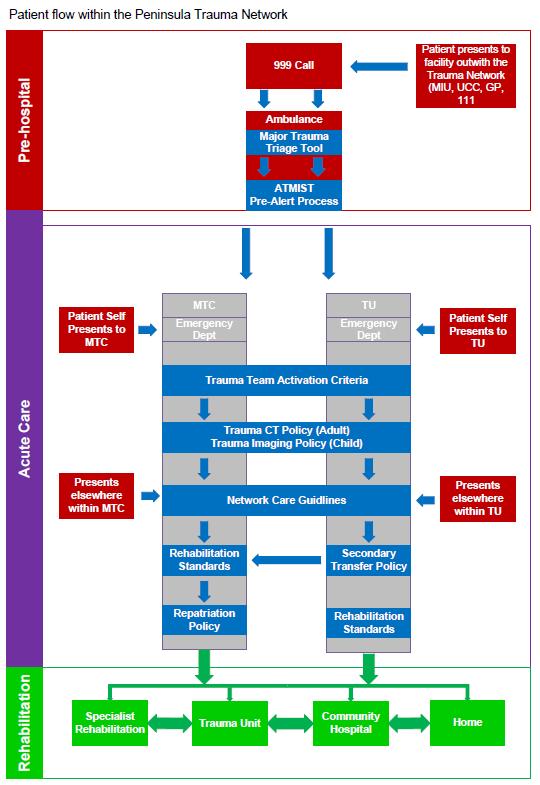
13 Clinical Governance for BASICS Southwest is comes under the SWASFT processes. HEMS Paramedics on the 3 air ambulances in the Peninsula. These are frontline paramedics with extended roles but are not yet Critical Care Paramedics (CCP). The CCP level of training is not, as yet, available within the Peninsula Region. HEMS Physicians Currently the level of service provide is quite variable: Great Western Air Ambulance provides a physician-staffed air ambulance with 85% daytime critical care physician cover. This service can provide cross-cover to the North Devon region Dorset and Somerset Air Ambulance provides 45% daytime critical care physician cover. This service can provide cross-cover to the East Devon region Cornwall and Devon Air Ambulances provide some HEMS cover on an as and when basis. The significant problem/difficulty with all of the HEMS physician services is that they are all provided on a voluntary basis. To ensure a quality service, a fully commissioned service is required and at the current time there is a large amount of work ongoing between SWASFT, the air ambulance providers and both the Peninsula and Severn Trauma Networks (this issue remains on the PTN risk register). This subject is also being raised with commissioners. Search and Rescue The winchmen for Bristow s Search and Rescue Service are dual trained as Paramedics and as such the helicopters are able to take to the patient to the most appropriate destination. It has been agreed with Bristows that when appropriate they will take patients direct to the MTC rather than the nearest hospital. However there is currently no formal guideline/policy for this. Network Admission and Operational Policy Figure 5 (Page 17) demonstrates the flow of patients within the Network and how the Network Policies (in blue) relate to them. The Peninsula Trauma Network accepts major trauma patients from all routes of entry into the healthcare system. Predominantly, but not exclusively, the entry is through 999 call to the ambulance service. Patients also self-present to the Emergency Departments, Minor Injury Units and General Practitioners, and some patients sustain major trauma whilst residing as inpatients within the community or acute hospitals. Patients may also present with apparently unrelated problems which are found on investigation to be complications of recent trauma. Presentation via the ambulance service following trauma will trigger a Major Trauma Triage Tool (appendix 1) assessment using the Major Trauma Triage Tool Checklist (appendix 2). 13
14 Patients found to meet criteria for Primary Bypass under the Major Trauma Triage Tool (attachment 1) will be transferred directly to the MTC as long as they also meet the criteria within the Automatic Acceptance policy (appendix 3). Other patients with a major mechanism of injury will be taken to their nearest TU for further assessment. At both the MTC and TU, the Trauma Team Activation Criteria (appendix 4) are in place to offer the most seriously injured patient s consultant-led multidisciplinary trauma assessment and resuscitation and will be activated as appropriate. A patient meeting SWASFT Pre-alert Criteria (appendix 5) should trigger a telephone call to the receiving ED in the ATMIST (appendix 6) format. Occasionally patients without a major mechanism of injury will be taken (or self-present) to the closest Minor Injury Unit or Urgent Care Centre. These units are not part of the Trauma Network: when the injuries are found to exceed the capabilities of these units, a 999 call to the ambulance service should be placed and a Major Trauma Triage Tool (appendix 1) assessment is triggered. Patients self-presenting to an Emergency Department and fulfilling Trauma Team Activation Criteria (appendix 4) are moved to the Resuscitation Room for Trauma Team assessment. Within the ED, imaging is carried out according to the Trauma CT policy (adult) (appendix 7) and Trauma Imaging Policy (paediatric) (appendix 8). The Peninsula Trauma Network policy for Adult and Paediatric imaging, is that it is carried out in accordance with the Royal College of Radiology, Standards of Practice and Guidance for Trauma Radiology in Severely Injured Patients (appendix 9) and Paediatric Trauma Protocols (attachment 10). Best care for individual injuries follows the local implementation of Network Care Guidelines as per Appendix II: Where a patient is at a TU and the patient s injuries exceed the capability of the Unit to provide the necessary care, or where the ISS is likely to be greater than 15 and transfer for care at the MTC is in the patient s best interests, the patient is transferred to the MTC as per the Automatic Acceptance and Secondary Transfer Policy (appendix 3) or the Paediatric Policy (appendix 22). Patients too unwell to travel may initially be treated at the TU until stable enough to transfer. Patients remaining at the TU are admitted under a named consultant who accepts responsibility for coordination of care. The patient s rehabilitation needs should be met and a rehabilitation prescription given to the patient as per T16-2D-106. When onward transfer 14
15 to the MTC for tertiary non-time-critical care is required, this should occur within 48 hours of acceptance. Patients at the MTC will be admitted under a named consultant and supported by Major Trauma Centre Coordinators (MTCC s) who accept responsibility for coordination of care. The MTCC s ensures that a rehabilitation prescription is commenced as per the Rehabilitation Standards (appendix 23). When the patient is referred back to their local Trauma Unit, community hospital or rehabilitation facility, this transfer should occur within 48hours of referral as per the Repatriation Policy (appendix 24). All patients with an ISS of 15+ that receive their definitive care in a TU must be audited to determine if this was the correct course of action. This group of patients will be reviewed through the Network governance processes. 15
16 16
17 Network Transfer Policy (T16-1C-104) Primary Transfers from scene of incident to MTC are indicated by the Major Trauma Triage Tool (appendix 52). A transfer time limit of 60 minutes is used to allow primary transfer to MTC when a closer TU is available ( Primary Bypass ). The number of primary bypass journeys is audited annually by SWASFT. Devon Air Ambulance, Cornwall Air Ambulance and Bristow s Search and Rescue Helicopter service work closely with South West Ambulance Service to provide Primary Transfer from remote locations Secondary Transfer from Trauma Unit to MTC follows the Secondary Transfer Policy (attachment 3) and the Paediatric Major Trauma Policy (appendix 22). The choice of land or air transport is determined by factors of availability, time, weather conditions, distance and personnel, as well as patient factors such as stability. SWASFT has agreed that they will treat time-critical secondary transfers as a priority and will aim to provide an ambulance with the national 8 min response time. In reality, most TUs will be able to give up to an hour s notice of a transfer. Non-time critical Secondary or tertiary Transfers should be effected within 48 hours of acceptance as per D15a (Major Trauma Service Specification), see the Secondary Transfer Policy (appendix 3) for details. The Safe Transfer of Critically Injured Patients Policy (appendix 22) covers transfers within and between hospitals. Paediatric Transfers Due to the geography of the PTN it has been agreed with Bristol Royal Hospital for Children (BRHC) that for time critical transfers the referring hospital (TU or adult MTC) will undertake the transfer and not the Western Acute Transport for Children Team (WATCh). This is a pragmatic decision based on time; not having to wait for WATCh can save up to 4 hours on a road transfer from the Royal Cornwall Hospital (Truro). Non Time-critical transfers to BRHC will be retrieved by the Western Acute Transport for Children Team (WATCh). Further information on can be found in the PTN/STN Paediatric Major Trauma Policy (appendix 22) Once the BRHC have completed their joint working agreement with the Coventry Paediatric Air Ambulance it is envisaged that local air ambulances will still be used for any critical transfers. Air Transfers to BRHC can be by Air Ambulances or search and rescue helicopters, however only Air Ambulances can land at BRHC as the helipad is on the hospital roof and 17
18 only rated for that size of vehicle. Transfers by larger SAR helicopters must go to Southmead hospital (Adult MTC) and then be transferred to BRHC by road. The Paediatric policy was compiled jointly between the PTN, STN, WATCh and the BRHC s Major Trauma Team. Transfer Documentation A Critical Care Transfer form (appendix 43) is used to document inter-hospital critical care transfers. There is a pre-transfer checklist on the rear of this document. Currently copies of this form are sent to the Southwest Critical Care Network office in Torbay for collation prior to audit by the Critical Care Network. The form is suitable for use with both Paediatric and Adult transfers. The PTN are liaising with them and with SWASFT to design a suitable electronic format for the future. It is hoped that this will be part of the ambulance service s (SWASFT) new electronic Patient Care Record. Regular audit of all patients with ISS >15 who are not transferred to an MTC is required by the PTN. These cases are discussed at the Network Governance meetings to ensure the Network Secondary Transfer Policy is appropriately enacted. Secondary Transfer has been shown to add a significant delay to arrival at definitive care for patients with head injury when compared to patients with a Primary Transfer to the MTC. The PTN is currently looking at ways of shortening Secondary Transfer times as well as facilitating Primary Bypass from more remote locations. 18
19 Trauma Nurse Co-ordinators (TNC) (T16-2C-103) & (T16-2C-303) Trauma Nurse Co-ordinators are experienced nurses that provide a service at both the MTC and the TU s, to co-ordinate the care of all major trauma patients and to provide a single point of contact for a patients relatives and next of kin. The service provided must fit the national criterion but at the same time it is acceptable for the service in the trauma units to be, if necessary, integrated with an existing role. Currently only 2 TU s provide this service (see figure 5). Major Trauma Centre At the MTC the service must be provided 7 days a week and must therefore be resourced appropriately. Each patient/family should be provided with the contact details for the service as soon as possible after admission. The MTC provides the following posts in this service: Lead Major Trauma Centre Co-ordinator (MTCC) X 1 Major Trauma Centre Co-ordinators X 3 Major Trauma Centre Co-ordinator/Occupational Therapist X 1 Major Trauma Centre Co-ordinator/ Physiotherapist X 1 Administrative Assistants X 2 For further details on the MTC service please see the MTCC service SOP. Trauma Units For the TU s the service should be provided Monday to Friday. Each patient/family should be provided with the contact details for the service as soon as possible after admission. It is considered good practice for each TNC service to have a messaging service attached to the contact telephone number. Furthermore consideration should be given to providing the TNC s with a pager and possibly a mobile phone of some type to minimise the time spent retrieving messages and calling people back. It is quite appropriate for the TNC role to integrate with the role of the Rehabilitation Coordinator. The services are as follows: NDDH 1 wte Clinical Site Manager (nurse) with cover by the rest of the Site Services team for leave etc. RCHT No service as of 01/02/2016 RD&E No service as of 01/02/2016 SDHFT Integrated into role of existing Orthopaedic Trauma Co-ordinators plus a falls Specialist Nurse from ED. 19 Figure 5
20 Network Massive Transfusion Policy The Peninsula Trauma Network is composed of 5 large acute NHS Trusts and as such each has a range of services that is different from the others. Early on, it was agreed by the Network Clinical Advisory Group that each acute trust would retain their own Massive Transfusion Policy (MTP) as part of their Trust Transfusion Policy. The Network has developed an overarching Massive Transfusion Policy that stipulates what each Trust should include in their policy. Please see appendix 27 for a copy of the Peninsula Trauma Network Massive Transfusion Policy. Network Spinal Injury Policy T16-1C-109 The Peninsula Trauma Network has two Spinal Centres: Plymouth Hospitals NHS Trust, a combined Orthopaedic and Neurosurgical Spinal Service Royal Devon and Exeter NHS Foundation Trust, which is an Orthopaedic Spinal Service. The Peninsula Trauma Network Spinal Policy (appendix 39) aims to ensure that a patient with Spinal Cord or Column Injuries gets to the most appropriate centre for their treatment. A pathway and careplan has been developed which includes their immediate ED care, initial inpatient treatment and rehabilitation and transfer to a specialist Spinal unit as appropriate. The regional Spinal Injuries Centre for the Peninsula Trauma Network is: Duke of Cornwall Spinal Treatment Salisbury District Hospital Salisbury Wiltshire SP2 8BJ ext
21 Adult and Paediatric Imaging Guidelines T16-1C-107 The Peninsula Trauma Network Policies for Adult and Paediatric Imaging (attachment 7 & 8), are that imaging is carried out in accordance with the Royal College of Radiology, Standards of Practice and Guidance for Trauma Radiology in Severely Injured Patients (attachment 9) and Paediatric Trauma Policy (attachment 10). The paediatric policy is consistent with those of the Regional Paediatric MTC in Bristol. Teleradiology T16-1C-105 When the previous GE PACS imaging system was installed in the Peninsula the ability to share images was not a function. In 2013 when the Insignia PACS was procured, by all 5 acute trusts in the Southwest, a key requirement was the ability to share images between NHS Trusts within the region. Since implementation in 2013 the PACS teams and colleagues at each of the Trusts have had to manually share images by pushing images electronically to each Trust, or continue to use Image Exchange Portal and bbrad systems. In the summer of 2014 each of the Trusts took an upgrade of Insignia PACS which enabled sharing of images from within the PACS. While the new image sharing facility provides sharing capability a number of issues are evident and a resolution to these is still being sought. A link to Bristol Children s Hospital to enable visibility of paediatric images, has recently enabled, which is currently in testing. Insignia are due to release the next version of image sharing soon after April Image sharing depends on the using the patients NHS number as the unique identifier. Within normal working hours the data quality team can provide this and then the PACS teams are able to push/pull the images. However out of hours the image transfer is stalled without the patients NHS number. Images can still be viewed on the system at the MTC but manipulation of the images is limited. As an interim safety backup the Network is arranging with the Trauma Units and the Major Trauma Centre that access to their PACS system will be supplied to each Trauma Team Leader at BRHC. A statement from each TU and the MTC on tele-radiology is available as attachments
22 MTC Update In March 2015 we enabled image sharing across selected users at Plymouth NHS Trust as a function within Insignia PACS. This enabled users at Plymouth to retrieve images from Torbay, Exeter, Barnstaple and Truro PACS from within the Plymouth PACS. During 2015 we also enabled links to Bristol from within Insignia PACS for our Imaging IT Team. During 2015 the image sharing functionality was migrated out to key users in stages designed to ensure that there was no adverse impact upon the underlying IT networks. As contingency, users retained individual logins to remote sites. In 2016 we anticipate improvements in terms of sharing system reliability, enhanced features for dealing with Trauma patients and those without an NHS Number Identifier (currently a key element to sharing). With these enhancements from Insignia we hope to be able to expand the sharing facility to a wider cohort of users. Image sharing still depends on the using the patients NHS number as the unique identifier. Within normal working hours the data quality team can provide this and then the PACS teams are able to push/pull the images. However out of hours the image transfer is subject to Images being pushed to the remote site, this process is reliant upon human intervention and knowledge at both the sending and receiving locations. T Llewellin, July 2016 Discharge/Repatriation Policy The Repatriation Policy (see appendix 24) covers repatriation of patients from the MTC to local providers. Through this Policy, Trauma Units agree to accept patients within 48 hours of referral. The Policy details the escalation procedure to be followed when repatriation is not achieved within the expected timeframe. Instances of breaches of this Policy are reported by the MTC, recorded at Network level and audited regularly. A request for the regionally-devised Trauma Unit Service Specification to be included in the Trauma Units commissioning round for 2016/17 has been made to aid with the delayed repatriations problems. Commissioning groups have expressed a desire to undertake this piece of work and also to develop a mechanism to incentivise compliance with the repatriation part of the Service Specification. When a trust has not taken a patient back from the MTC within the agreed 48 hour timeframe then the MTCC S will raise a governance issue form which they will then forward to the Network Governance Lead for investigation. An will also be sent to the MTC Head of Operations so that a higher level conversation can be held to resolve the issue if required. A repatriation dashboard has been developed so that there is oversight of all delays with repatriations. The Repatriation Policy will be revised during
23 Access to Rehabilitation Services Trauma Network Rehabilitation Director (T16-1C-111) The PTN Rehabilitation Director, Jude Fewings, is a Band 8a Therapist and undertakes this role as a part-time position. The post holder works under the guidance of the Network Director but is otherwise an autonomous role. Major Trauma Centre Rehabilitation Lead (T16-2D-101) There should be a named lead clinician for major trauma rehabilitation at the MTC, who should be a consultant in rehabilitation medicine, and have an agreed list of responsibilities and a minimum of 1 PA allocated for the role. Trauma Unit Rehabilitation Lead Each Trauma Unit should have a single nominated lead therapist as the clinician responsible for all of the Major Trauma therapy services, including: Physiotherapy Occupational Therapy Speech and Language Therapy Dietetics Psychology/Neuropsychology Although this is not a nationally required role this person will be the principle point of contact for all therapy related matters, will attend the PTN Rehabilitation Group and will be able to speak on behalf of the trust on rehabilitation matters. Rehabilitation Co-ordinators (T16-2D-103 & T16-2D-312) These are nurses or allied health professionals (Physiotherapist, Occupational Therapist, Dietician, Speech & Language Therapist or Psychologist) who are responsible for the coordination and communication of the patients current and future rehabilitation needs. For the MTC the co-ordinator must be available 7 days a week. For the TU s the co-ordinator should be individual who is responsible for the co-ordination and communication of the patients current and future rehabilitation needs.. The Rehabilitation Co-ordinator should be a nurse or allied health professional with experience in rehabilitation. It is not inappropriate for this role to be integrated with the role of the MTCC/TNC. Directory of Rehabilitation Services The current version is in a paper format due to the recent failure of a programme of work with another Network to further develop their e-directory. Currently it is proposed that the Network investigates whether it is appropriate to utilise the ORION Directory of services platform. 23
24 Rehabilitation Services At present there is one Level 2a neuro-rehabilitation unit, based in Plymouth. The Plym Unit has 15 beds (2 tracheostomy) and accepts patients from across the peninsula. The full dataset is submitted to UKROC. Occasionally patients are referred to the Frenchay Brain Injury Centre, Bristol, which is a Level 1 unit. There are two other neuro-rehabilitation units (Exeter and Hayle, Cornwall) who are able to manage less complex patients (level 2b) and have some input from Rehabilitation Medicine Consultants. The Brain Injury Rehabilitation Trust also has a centre in Cullompton, which patients are referred to for slow stream rehabilitation after brain injury. All Spinal Cord Injured patients are referred to the Duke of Cornwall SCI Centre in Salisbury. Not all patients will choose to go there, often due to the distance from their home address. There are level 3 rehabilitation services within the community hospitals across the Peninsula. Furtjher details are available in the network Directory of Services. There is a wide range of community rehabilitation services across the peninsula. There are no paediatric in-patient rehabilitation beds within the peninsula, complex paediatric trauma cases are managed at Bristol Royal Hospital for Children. This issue is recognised in the PTN Risk Register. There are two prosthetic services for the peninsula. Plymouth prosthetic rehabilitation service covers the whole of Cornwall, Isles of Scilly, Plymouth and south west Devon (although patients from North and South Devon may also choose to attend this service). It is a Rehabilitation Medicine consultant led service with a weekly outreach clinic at Camborne Redruth Community Hospital. Exeter Mobility Centre covers South, East and North Devon. There is no Rehabilitation Medicine Consultant in this service. At the present time most patients who experience musculoskeletal injuries after major trauma receive much of their rehabilitation within the acute hospital. Many of these are able to go home with a list of exercises and referral to community rehabilitation teams. Those (often the elderly) who require a longer period of less intense rehabilitation are transferred to community hospitals for generic rehabilitation. Rehabilitation Referral process Trauma patients are reviewed by the multidisciplinary team at the MTC, which includes limited input from the existing RM Consultant and Consultant Therapist. This team makes a clinical decision based on assessment regarding onward referral for rehabilitation. All complex (category A and B) patients are discussed on a weekly basis with the Plym MDT. 24

25 Spinal cord injury patients are discussed with the SCI Centre in line with the PTN Spinal Policy. There are service specific referral forms for some of the rehabilitation services and others accept telephone or letter referral. There is a Major Trauma Rehabilitation Standards document (attachment 23) in place within the Network. This document provides direction and guidance for key individuals and organisations and intends to improve the patient pathway and quality of rehabilitation for major trauma patients. The referral pathway at figure 6 describes the process: Figure 6 Rehabilitation Referral Pathway 25
26 Rehabilitation Prescription MTC Paper Rehabilitation Prescriptions (RP) have been used in the Adult MTC since April The RP is a 2-part document to accommodate the differences between those patients with more and less complex rehabilitation needs. At present the RP is completed by the ward therapy teams with input from a RM Consultant or Consultant Therapist for the more complex patients. The current paper system has many limitations and consideration is being given to an electronic prescription through the ORION/IRMA pilot. When the additional RM Consultant is in post the erp will form a key part of the multidisciplinary rehabilitation process within the MTC. For details on the processes involved please refer to the MTC Operational Policy. Trauma Units It has been agreed, by the PTN Rehabilitation Group, that the Trauma Units within the Peninsula Trauma Network are free to develop their own Rehabilitation Prescription as long as it contains the same core elements as that of the MTC. It is quite acceptable to integrate this document with an existing one, of a similar type, to help prevent the spread of an unacceptable number of documents for staff to have to become familiar with and use. Key Rehabilitation issues See Annual Report and Appendix to Annual Report for a full description of current key issues in rehabilitation after major trauma in the Peninsula. All risks form part of the PTN Risk Register and work plan. 26
27 Paediatrics Trauma Network Paediatric Lead The Peninsula Network has a paediatric major trauma Lead, Dr Peter Davis, based at BRHC, that is a shared role across Peninsula and Severn Major Trauma Networks. It is a 1PA post that is split between the 2 networks. The funding for the post is also apportioned in the same way. Transfer The MTC for the Peninsula Trauma Network is not a paediatric MTC and as such is only able to treat children up to the same level as a Trauma Unit. All children with major trauma must be discussed with Paediatric Trauma Team Leader at the BRHC: Tel: The decision whether or not to transfer a patient to the PMTC ultimately rests with the Paediatric TTL. All children with time-critical injuries who are to transferred to BRHC will be transferred by the referring TU, who will be responsible for arranging the transfer vehicle and transferring Clinician. Children with non-time-critical can be transferred by the referring TU or can be retrieved by the Bristol WATCh Retrieval Team or the Coventry Paediatric Air Ambulance. Either of the retrieval methods must be organised by the PTTL at the BRHC. Repatriation Children will receive their care at the BRHC for as long as is appropriate for the individual child, this also includes rehabilitation. When they no longer require the level of care provided by the PMTC and are ready for repatriation back to their nearest home hospital then the Paediatric Repatriation policy requires that they are treated in the same manner as adults i.e. that a bed is identified within 48 hours. Time Critical Neurosurgical or Cardiothoracic Surgery If, within the Peninsula Trauma Network region, a child with Cardiothoracic or Neurological injuries is considered too unstable for transfer or unlikely to survive a transfer without prior treatment. The respective surgical teams have agreed that in those circumstances they will undertake life-saving surgery, in liaison with their respective colleagues at the PMTC, at the adult Major Trauma Centre at Derriford Hospital prior to transfer. Audit A twice yearly, cross network, stakeholder meeting is held which alternates between Exeter and Taunton. This event covers general topics including research and new developments and includes a half day Morbidity & Mortality meeting, with case studies as appropriate. Each network funds & organises their local event. 27
28 Trauma Documentation The Trauma Network endeavours to strike a balance between asking Network Trusts to use Network designed documentation and allowing them either use their existing trust documents or their own internally designed documentation. There are currently the following documents that the network designs and requests that the MTC and TU s use: Trauma booklet (A4) ATMIST sticker (A5) Governance form (A4) Morbidity and Mortality form (Attachment 42) Rehabilitation Prescription All Major Trauma Centre s and Trauma Units are required to issue appropriate patients with a rehabilitation prescription as per the national major trauma quality Indicators. Each organisation is encouraged to develop their own Rehabilitation Prescription to minimise the amount duplication of effort. For example one Trauma Unit has integrated their Rehabilitation Prescription with their Stroke Discharge document, as they are very similar. This ensures that the appropriate clinicians and therapists have only one document to complete and that therefore this aims to ensure that the completing clinicians do not have too much additional documentation to complete. Inter-Hospital Transfer form Currently the network requires that the Major Trauma Centre and Trauma Units all use the, long established, South West Critical Care Transfer form (attachment 26). The duplicate copies of these forms are sent to the Critical Care Network where they have a database that they log all of the relevant details. All duplicate copies of the form should be sent to The Critical Care Network Manager/Lead Nurse in the attached envelope. As the Critical transfer form is a large A3 form that no longer optimally meets the needs of the end users, there is a proposal that this form becomes part of the SWASFT new electronic patient record system. This system is currently in the development and integration phase and so representatives from the Peninsula Trauma and South West Critical Care Networks will meet with them in due course to develop the e-version of the transfer form. This has been added to the PTN workplan. 28
Severn & Peninsula Major Trauma Networks
 Severn & Peninsula Major Trauma Networks Paediatric Major Trauma Centre Acceptance Policy May 2014, V3 REVIEW DISTRIBUTION APPROVAL/ADOPTED 6 months after formal approval and then annually Severn major
Severn & Peninsula Major Trauma Networks Paediatric Major Trauma Centre Acceptance Policy May 2014, V3 REVIEW DISTRIBUTION APPROVAL/ADOPTED 6 months after formal approval and then annually Severn major
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
Sample Template Operational Policy
 Operational Delivery s Sample Template Operational Policy October 2014 Document MTN-OP-03-10-14 Classification: General Organisation Document Purpose Title Author Operational Delivery s Guidance Sample
Operational Delivery s Sample Template Operational Policy October 2014 Document MTN-OP-03-10-14 Classification: General Organisation Document Purpose Title Author Operational Delivery s Guidance Sample
Clinical Guideline Trauma Care: Accessing Trauma Services
 Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
Clinical Guideline Trauma Care: Accessing Trauma Services Guideline ID CG24 Version 1.2 Title Approved by Trauma Care: Accessing Trauma Services Clinical Effectiveness Group Date Issued 17/03/2017 Review
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation
 Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Major Trauma Review Implications
 Meeting: NoSPG Date: 19 th February 2014 Item: 09/14 (a) NORTH OF SCOTLAND PLANNING GROUP Major Trauma Review Implications Introduction The National Planning Forum Major Trauma Sub Group developed a quality
Meeting: NoSPG Date: 19 th February 2014 Item: 09/14 (a) NORTH OF SCOTLAND PLANNING GROUP Major Trauma Review Implications Introduction The National Planning Forum Major Trauma Sub Group developed a quality
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and
 Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
Trauma Care Network News. West Midlands Major Trauma Clinical Lead appointed. Inside Issue 3. Issue 3
 Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation
 Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals
 A Guide for Healthcare Professionals") Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
NHS Emergency Planning Guidance
 NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives
 NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
Wales Critical Care & Trauma Network (North)
") Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
62 days from referral with urgent suspected cancer to initiation of treatment
 Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
Appendix-2012-87 Borders NHS Board PATIENT ACCESS POLICY Aim In preparation for the introduction of the Patients Rights (Scotland) Act 2011, NHS Borders has produced a Patient Access Policy governing the
Intensive Psychiatric Care Units
 NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
NHS England South Escalation Framework
 NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
Scottish Ambulance Service. Our Future Strategy. Discussion with partners
 Discussion with partners Our values Glossary of terms We will: put the patient at the heart of everything we do. treat each and every person well, with respect and dignity. always be open, honest and fair.
Discussion with partners Our values Glossary of terms We will: put the patient at the heart of everything we do. treat each and every person well, with respect and dignity. always be open, honest and fair.
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Intensive Psychiatric Care Units
 NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
Greater Manchester Neuro-Rehabilitation Services information for patients and carers
 THIS BOOKLET IS BEING TRIALLED Greater Manchester Neuro-Rehabilitation Services information for patients and carers Greater Manchester Neuro-Rehabilitation Services gmnrodn@srft.nhs.uk All Rights Reserved
THIS BOOKLET IS BEING TRIALLED Greater Manchester Neuro-Rehabilitation Services information for patients and carers Greater Manchester Neuro-Rehabilitation Services gmnrodn@srft.nhs.uk All Rights Reserved
Intensive Psychiatric Care Units
 NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
Grampian University Hospitals NHS Trust. Local Report ~ February Older People in Acute Care
 Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway
Grampian University Hospitals NHS Trust Local Report ~ February 2004 Older People in Acute Care NHSScotland Board Areas 13 12 15 1 Argyll & Clyde 2 Ayrshire & Arran 3 Borders 9 7 4 Dumfries & Galloway
NHS Borders. Intensive Psychiatric Care Units
 NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Rehab V Vita Square Operational Guideline
 Southern Adelaide Local Health Network Rehab V Vita Square Operational Guideline Consultation Paper Version 2.2 January 2018 Purpose The purpose of this document is to provide an overview of operational
Southern Adelaide Local Health Network Rehab V Vita Square Operational Guideline Consultation Paper Version 2.2 January 2018 Purpose The purpose of this document is to provide an overview of operational
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT)
") TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT) Introduction The National Institute for Clinical Excellence has developed Guidance on Supportive and Palliative Care for patients with cancer. The standards
TOPIC 9 - THE SPECIALIST PALLIATIVE CARE TEAM (MDT) Introduction The National Institute for Clinical Excellence has developed Guidance on Supportive and Palliative Care for patients with cancer. The standards
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
SCHEDULE 2 THE SERVICES. A. Service Specifications. E07/S/c Paediatric Long Term Ventilation
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Briefing on Shaping Our Future urgent care work stream progress
 Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
8.1 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS. Date of the meeting 18/05/2016
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74
 Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK.
 Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK. Created: 13.9.16 Created by: Becca Robinson - Service Improvement Lead Bristol CCG Version: Draft v0.5 Last Review: Next Reviewed
Front Door Streaming to Primary Care Hub Pilot DRAFT GOVERNANCE FRAMEWORK. Created: 13.9.16 Created by: Becca Robinson - Service Improvement Lead Bristol CCG Version: Draft v0.5 Last Review: Next Reviewed
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification
 E07/S/c 2013/14 NHS STANDARD CONTRACT PAEDIATRIC LONG TERM VENTILATION PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner Lead Provider Lead Period
E07/S/c 2013/14 NHS STANDARD CONTRACT PAEDIATRIC LONG TERM VENTILATION PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner Lead Provider Lead Period
AMP Health and Social Care Professional Implementation Group Update
 AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster.
 Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
SERVICE SPECIFICATION
 SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
SERVICE SPECIFICATION Service Rotherham Hospice Lead Gail Palmer Provider Lead Paula Hill / Mike Wilkerson Period 21 st July 2010 20 th July 2013 1. Purpose This specification describes the services which
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Introducing a 7-day service: the benefits of increased consultant presence
 Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
SOUTH CENTRAL AMBULANCE SERVICE NHS FOUNDATION TRUST
 SOUTH CENTRAL AMBULANCE SERVICE NHS FOUNDATION TRUST CLINICAL SERVICES POLICY & PROCEDURE (CSPP No. 19) STROKE CARE POLICY AND PROCEDURES September 2016 DOCUMENT INFORMATION Author: Dave Sherwood Assistant
SOUTH CENTRAL AMBULANCE SERVICE NHS FOUNDATION TRUST CLINICAL SERVICES POLICY & PROCEDURE (CSPP No. 19) STROKE CARE POLICY AND PROCEDURES September 2016 DOCUMENT INFORMATION Author: Dave Sherwood Assistant
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Paper 5.0 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE.
 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
From April 2017 NHS Kernow aims to have in place a new NHS funded transport policy which will clearly outline:
 About the consultation From October 2018 NHS Kernow will commission one universal non-emergency patient transport service for patients in Cornwall and the Isles of Scilly. This will make it easier to make
About the consultation From October 2018 NHS Kernow will commission one universal non-emergency patient transport service for patients in Cornwall and the Isles of Scilly. This will make it easier to make
Requesting A&E Ambulance Transport A Guide for Healthcare Professionals
 Requesting A&E Ambulance Transport A Guide for Healthcare Professionals Contents Page No. Introduction... 3 What patients should travel with A&E ambulance transport?... 4 Procedure for calling an ambulance...
Requesting A&E Ambulance Transport A Guide for Healthcare Professionals Contents Page No. Introduction... 3 What patients should travel with A&E ambulance transport?... 4 Procedure for calling an ambulance...
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
Briefing on the first stage of the Acute Services Review the clinical recommendations
 Briefing on the first stage of the Acute Services Review the clinical recommendations Introduction Over 100 clinicians from our four main hospitals, GPs, NHS managers and patient representatives have been
Briefing on the first stage of the Acute Services Review the clinical recommendations Introduction Over 100 clinicians from our four main hospitals, GPs, NHS managers and patient representatives have been
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Headline consensus statement
 Consensus Statement on Saving Lives and Improving Health and Wellbeing between the Association of Ambulance Chief Executives (AACE) and the Chief Fire Officers Association (CFOA) 17 th March 2016 1. This
Consensus Statement on Saving Lives and Improving Health and Wellbeing between the Association of Ambulance Chief Executives (AACE) and the Chief Fire Officers Association (CFOA) 17 th March 2016 1. This
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
ROLE DESCRIPTION NATIONAL CLINICAL LEAD INTEGRATED CARE PROGRAMME FOR PATIENT FLOW
 ROLE DESCRIPTION NATIONAL CLINICAL LEAD INTEGRATED CARE PROGRAMME FOR PATIENT FLOW CLINICAL STRATEGY AND PROGRAMMMES DIVISION The HSE's Clinical Strategy and Programmes Division (CSPD) is leading a large-scale
ROLE DESCRIPTION NATIONAL CLINICAL LEAD INTEGRATED CARE PROGRAMME FOR PATIENT FLOW CLINICAL STRATEGY AND PROGRAMMMES DIVISION The HSE's Clinical Strategy and Programmes Division (CSPD) is leading a large-scale
Standard Operating Procedure INTER-HOSPITAL TRANSFERS
 Standard Operating Procedure INTER-HOSPITAL TRANSFERS DATE APPROVED: September 2010 APPROVED BY: Air Operations Manager IMPLEMENTATION DATE: November 2014 REVIEW DATE: November 2015 LEAD DIRECTOR: IMPACT
Standard Operating Procedure INTER-HOSPITAL TRANSFERS DATE APPROVED: September 2010 APPROVED BY: Air Operations Manager IMPLEMENTATION DATE: November 2014 REVIEW DATE: November 2015 LEAD DIRECTOR: IMPACT
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Job Description. Job title: Uro-Oncology Clinical Nurse Specialist Band: 7
 Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES
 Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
Effective discharge from hospital: the role of communication of home circumstances February 2017
 Effective discharge from hospital: the role of communication of home circumstances February 2017 Page 1 of 10 1. Introduction 1.1 Healthwatch Coventry is the independent champion for health and social
Effective discharge from hospital: the role of communication of home circumstances February 2017 Page 1 of 10 1. Introduction 1.1 Healthwatch Coventry is the independent champion for health and social
Intensive Psychiatric Care Units
 NHS Greater Glasgow and Clyde Leverndale Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality
NHS Greater Glasgow and Clyde Leverndale Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality
Monthly Delayed Transfer of Care Situation Reports. Definitions and Guidance
 Monthly Delayed Transfer of Care Situation Reports Definitions and Guidance Version Date issued 1.00 18 December 2006 1.01 31 March 2008 1.02 18 January 2010 Changes made Indicator of response to pressures
Monthly Delayed Transfer of Care Situation Reports Definitions and Guidance Version Date issued 1.00 18 December 2006 1.01 31 March 2008 1.02 18 January 2010 Changes made Indicator of response to pressures
Review of Stroke (Acute Phase) & TIA Services
 & TIA Services") West Midlands Partnership of Cardiac and Stroke Networks Review of Stroke (Acute Phase) & TIA Services Report Date: June 2011 Visit Dates: May to November 2010 Images courtesy of The Stroke Association,
West Midlands Partnership of Cardiac and Stroke Networks Review of Stroke (Acute Phase) & TIA Services Report Date: June 2011 Visit Dates: May to November 2010 Images courtesy of The Stroke Association,
LymeForward Health and Wellbeing Group
 LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Expansion of Individual Placement and Support (IPS) services Proposal Guidance for Wave 1 Funding
 services Proposal Guidance for Wave 1 Funding") Expansion of Individual Placement and Support (IPS) services Proposal Guidance for Wave 1 Funding Expansion of Individual Placement and Support (IPS) services proposal guidance for Wave 1 funding Version
Expansion of Individual Placement and Support (IPS) services Proposal Guidance for Wave 1 Funding Expansion of Individual Placement and Support (IPS) services proposal guidance for Wave 1 funding Version
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Responding to a risk or priority in an area 1. London Borough of Sutton
 Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Adult Therapy Services. Community Services. Roundshaw Health Centre. Team Lead / Service Manager. Service Manager / Clinical Director
 THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
Sentinel Stroke National Audit Programme (SSNAP)
") Sentinel Stroke National Audit Programme (SSNAP) Acute organisational audit proforma 2016 Clinical Standards, Royal College of Physicians, London. On behalf of the Intercollegiate Stroke Working Party.
Sentinel Stroke National Audit Programme (SSNAP) Acute organisational audit proforma 2016 Clinical Standards, Royal College of Physicians, London. On behalf of the Intercollegiate Stroke Working Party.
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
DRAFT - NHS CHC and Complex Care Commissioning Policy.
 DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Improving Access to Therapeutic Apheresis Services in the South West of England: The Development of a Web-based Roadmap to Outline Referral Pathways
 South West Regional Transfusion Committee Improving Access to Therapeutic Apheresis Services in the South West of England: The Development of a Web-based Roadmap to Outline Referral Pathways Executive
South West Regional Transfusion Committee Improving Access to Therapeutic Apheresis Services in the South West of England: The Development of a Web-based Roadmap to Outline Referral Pathways Executive
NHS Highland Plan for rebalancing of Primary Care Dental Services
 Highland NHS Board 3 February 2015 Item 4.3 NHS Highland Plan for rebalancing of Primary Care Dental Services 2015-2020 Report by Dr Ken Proctor Associate Medical Director, Executive Director for Primary
Highland NHS Board 3 February 2015 Item 4.3 NHS Highland Plan for rebalancing of Primary Care Dental Services 2015-2020 Report by Dr Ken Proctor Associate Medical Director, Executive Director for Primary
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
Efficiency Review of The Welsh Ambulance Services NHS Trust
 Efficiency Review of The Welsh Ambulance Services NHS Trust Undertaken by Lightfoot Solutions in association with Lis Nixon Associates And Baker Tilly on behalf of Health Commission Wales and The Welsh
Efficiency Review of The Welsh Ambulance Services NHS Trust Undertaken by Lightfoot Solutions in association with Lis Nixon Associates And Baker Tilly on behalf of Health Commission Wales and The Welsh