Improving Processes Using Lean We Got This! Becky Dodge, RN, MBA, CSSBB UNC Medical Center Rehab Services
|
|
|
- Alisha Stephens
- 5 years ago
- Views:
Transcription

1 Improving Processes Using Lean We Got This! Becky Dodge, RN, MBA, CSSBB UNC Medical Center Rehab Services


2 Benefits of Lean Six Sigma Provides a comprehensive tool set to solve problems and to increase the speed and effectiveness of any process Provides a consistent lens and vocabulary for all staff Increases efficiency Increases revenue Reduces costs Increases employee and customer satisfaction Develops effective people

3 Lean Six Sigma Purple Belt Lean Toyota Production System

4 Flow = The Goal of a Lean Hospital

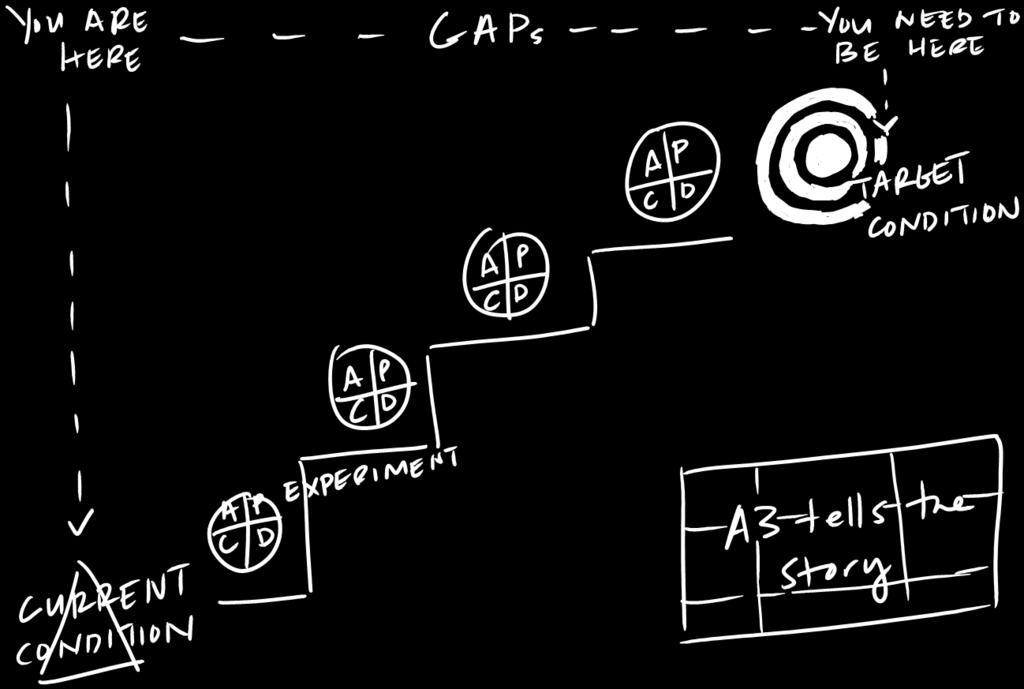
5 What is A3 Thinking?


6 A3 Thinking: Problem Solving Process
7 Value Added Activities For a process step to be considered value add, it must meet the following three criteria: 1. The customer has to care about the step 2. The thing going through the process changes 3. The process step is done right the first time
8 The 8 wastes (DOWNTIME) are: Defects Overproduction Waiting Non-utilized Talent Transportation Inventory Motion Extra Processing

9 Leadership
10

11 Team Composition Who should be on a Kaizen team? Home team: members closest to the process Visiting team: those who can provide outside eyes on the process Team leader: helps manage the team, keep them on track, positive influence Sponsor: provides management oversight and support, is responsible for the success of the team and helps prepare for the Kaizen.

12 Falls A3 Project
13 Box 1. Problem Statement In calendar year 2014 the falls rate index (# falls/1000 patient days) on the UNC Inpatient Rehab Unit ranged from for an average of The National Database of Nursing Quality Indicators (NDNQI) national benchmark for Rehab units is 5.29 (based on the 50th percentile). Clearly we wanted to do better!






14 Falls Protocol Pre A3 Use of Red/Yellow/Green signs Bed Alarms on (?) Hourly rounding Yellow arm bands, gripper socks Post fall huddle (?)

15 A3 Training Team met for a total of 3 days (1 month in between) Team works through the A3 over the course of several months Why a month apart? Gives them an opportunity to do the work in between training days Gives them time to absorb the information



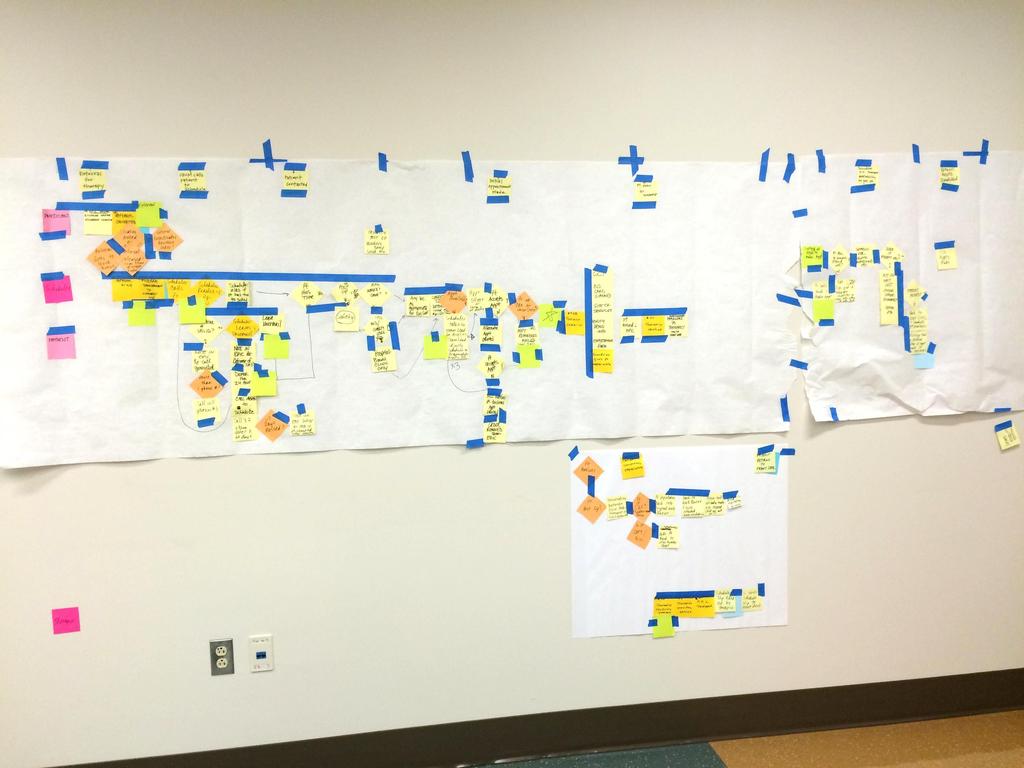
16 Box 2. Current State Words / Pictures Unsafe, poor patient satisfaction, lack of ownership in culture, complacency, lack of standardization / consistency, complex
17 Variables (41) Collected on Falls Patients (FY2014) N = 63 Room number Phone in reach? Time of fall Falls band on? Age of patient Urinal in reach? Sex of patient Bed/chair alarm activated? Diagnosis Gripping socks on? Isolation precautions? Environmental clutter a reported factor? Day of fall Patient taking diuretics? Previous fall in last 3 months? Patient taking sedatives? Pre fall Morse scale score Patient follows directions? Post fall Morse scale score Patient confused/cognitively impaired? Level of injury post fall Last comprehensive FIM score prior to fall Activity at time of fall Patient neutropenic? How fall occurred, ie, from bed, w/c, toilet, etc. Orthopedic diagnosis? Where fall occurred, ie, in room, bathroom, etc. Patient tethered to something? Did patient call for assistance? Patient reaching for something? Bed table in reach? Staff present? Bed low and locked? Family present? Call bell in reach? NA's fully staffed? Caution signs in place? RN's fully staffed? Light on? Number of patients RN had on day of fall Number of patients NA had on day of fall


18 Current State What does the data say?

19


20 What else did the data reveal? 75% of the patients were not repeat falls 52% of falls occurred while transferring or sitting 75% of falls occurred in the patient s room 66% of patients did not call for assistance 52% of the time the call bell was in reach 59% of time bed was low and locked 10% of time call bell not in reach 56% of patients followed directions 56% of patients were confused The majority of falls occurred around 4P
21 Who is with the patient?

22 We need help! Or do we?
23 What other information did we gather? Call bell response time AM and PM How often Care Board updated by PT and OT Room inventory chair placement, #w/c s, commode placement, assistive devices, IV poles, etc. Survey of nurse s comfort with transfers PT shadowing nursing



24 Box 3. Target State Where did we want to be? Reduction in falls, standard process, teamwork, commitment, communication, blame free environment, accountability, cognition and Morse scale, Staff and family education
25 Importance of VOC Members of our Patient and Family Advisory Board were invaluable both in terms of providing feedback on their hospital stay (both had fallen while on Rehab) and in offering suggestions for how to improve. The frankness/honesty of their answers was incredibly helpful. Things you wouldn t think of: What is mechanical soft? I didn t use the call bell because I couldn t speak and I was also embarrassed by the fact that I couldn t respond. This helped turn the team members who weren t convinced we needed a new process. As a result of what they shared, one of the team members suggested we go to another unit that was using symbols on their care boards for toileting and take a look at them. This idea was incorporated into our solutions.

26 Box 4. Gap Analysis Getting to the Root Causes! What are the steps? 1. Brainstorm potential root causes 2. Organize (affinitize) into like groups 3. Put header cards on each section 4. Perform the 5 Whys 5. If necessary, multivote to determine focused number of causes to address 6. Perform the 5 Whys for each potential root cause
27 Results of the Gap Analysis # Gaps Root Cause 1 Incomplete Documentation re: fall event Lack of ownership of process 2 Inaccurate signage No accountablity 3 Lack of clarity/criteria for putting on bed alarm No accountablity 4 Lack of gait belt use Lack specific location and education re: gait belt 5 Care boards incomplete and hard to understand No accountablity 6 No cognitive assessments & action plans Lack of education 7 Lack of communication between nurses/therapy Lack process and operational definitions 8 Don't know when a fall occurs No process to communicate fall (nursing to therapy) 9 Lack of visual aides Never thought of it 10 No toileting schedule; rounding Inconsistent application of process
28 Box 5. Solution Approach # Solution (if we) Outcome (then we) Gap No. 1 Have a process for the purpose and use of the care boards Improve universal communication with staff, patients and families 2, 5, 7, 8, 9 2 Supplement rounding schedules to accommodate high risk falls patients/times Improved patient safety and satisfaction 10, 3 3 Create a process for interviewing patients and staff post fall Have more complete information to guide prevention strategies 8 4 Develop visual aides for the patient rooms Improve communication and increase patient safety 3, 7, 9 5 Document fall(s) in the sticky notes Therapy and other staff will be aware of when a fall occurred 8, 1
29 Box 6. Rapid Experiments # Experiment Anticipated Effect Actual Effect Follow-up Action SA No. 1 Standard Work for Use of the Care Boards Therapy staff will update Care Boards Daily Standard work created during Kaizen Implement standard work 1 2 Identify High Risk Patients with LEAF Identification of High Risk Pts > Dec Falls Standard work created during Kaizen for LEAF pts Implement standard work 2 3 Supplemental Rounding on High Risk Patients Decreased Falls Standard work created during Kaizen for LEAF pts Implement standard work 2 4 Document date/time of fall in the Sticky Notes Therapy staff aware of occurrence of a fall Standard work created during Kaizen for LEAF pts Implement standard work 5 5 Interview patients/family and staff post fall Improve data collection re why fall has occurred Standard work created during Kaizen for LEAF pts Implement standard work 3 6 Develop visual aids for the patient rooms/care boards Improve communication with patients, family and staff In Process 4


30 Identification of High Risk Patients LEAF (Phase I) This symbol is placed outside the door of LEAF patients, and a smaller LEAF magnet is placed on the Care Board for easy identification while either inside or outside the room. LEAF patients are rounded on every half hour.


31 Enhancing Communication (Phase I) A checklist was developed to improve communication between nursing and therapy staff; though taking care of the same patient there may be minimal contact between the disciplines during a shift. This laminated sheet hung in the room allowed for more frequent updates that all could be aware of at any given time.
32 Post Fall Interview Patient (Phase I)
33 Post Fall Interview - Staff (Phase I)


34 Post Fall Survey (Phase I)
35 Box 7. Completion Plan # Action Owner Due Status 1 Care Board Pilot - 5 rooms Tim In Process 2 Staff Education/Inservice Start: In Process 3 Falls notebooks on both A and B sides 09/09/15 4 LEAF Pilot Lia 09/10/15 5 Staff Education Start: 09/09/15 6 Document Fall in Sticky Notes Lia 09/09/15 7 Supplemental Rounding Krishna 09/10/15 8 Education on New Process for Falls Lia 09/09/15 9 Sean 09/09/15 10 Process for auditing Care Boards Sean 09/09/15 11 Gait Belts Carty In Process

36 # Metric Unit Current Target Kaizen 30-Day 60-Day 90-Day Staff educated on new falls process Sticky Note in chart % % Staff/Patient Interview done % % % Supp. Rounding Completed % % N/A N/A LEAF outside room for LEAF pts % Magnet Up in Room for LEAF pts % % Intervention sheets updated % Falls Rate (Goal = 5.29)



37 Box 9. Insights

38
. In January of 2016, therapy staff began inservicing nursing staff on the use of the gait belts.")
39 Gait Belts (Phase II) In the fall of 2015 a grant was written to our Volunteer Services department to obtain a grant for funds to purchase washable gait belts for all 30 beds. Belts were spray painted with UNC Rehab and the room number (labor intensive). In January of 2016, therapy staff began inservicing nursing staff on the use of the gait belts. This should assist in the transferring of patients to/from the bed (identified as the chief reason for falls).

40 Standard Work

41 Care Board Changes (Phase III)
42 Sustaining the Change The Falls Prevention Team was formed to meet monthly and review any/all falls, identify root causes and consider any opportunities for improvement. Members include PT, PTA, RN, CNA, Health Unit Coordinator and former HUC, and coach. Recent changes include the development of an algorithm for deciding when to take a patient off of LEAF. Staff are collecting data from recent falls and analyzing it to determine if any new root causes are evident.
43 Thinking about Discontinuing LEAF Protocol? Has patient been alert and oriented x3 with no cognitive deficits for at least 24 hours? NO YES Does patient use call bell appropriately without activating bed alarm? NO YES Continue LEAF protocol for an additional 24 hours (minimum), then reassess YES Has patient exhibited impulsivity within the last 24 hours? NO Additional Notes: Once LEAF protocol is discontinued, leave bed alarm on for 24 hours RN will assess Q shift and communicate LEAF status in report Communicate LEAF status daily with primary therapist Put LEAF status in "sticky notes" (ex: Date & time of fall, assisted/unassisted fall, LEAF status) Orange "Falls Intervention Checklist" Write the Date & Time LEAF protocol was discontinued Discontinue LEAF protocol [ ] Remove LEAF from assignment considerations in E-Kardex [ ] Remove LEAF from the patient s room door and care board


44 EPIC Changes
45 So What does the data say? Average monthly falls rate index: Oct 2015 Dec 2016 = 4.84 (Range ) Jan 2017 Jan 2018 = 5.8 (Range ) Our original goal was to be < 5.29 (50 th percentile NDNQI) We have reduced our falls by over 50%! Gait belt expenditures dropped (from over $3000/year to $386.35/1.5 years!)


46 Helpful Tips Team selection is critical ensure everyone involved in the process is included Involve patients and their representatives- their point of view is invaluable! Carefully decide the plan of action/implementation Measure sustainment to ensure success Continue to improve!

47 Improving Care Access in Outpatient Therapy Clinics
 staff in the Outpatient Therapy clinics were frustrated; it was difficult to get patients in for appointments, but")
48 Box 1. Problem Statement Therapy and ORCM (front desk) staff in the Outpatient Therapy clinics were frustrated; it was difficult to get patients in for appointments, but there were also a significant number of no shows, so utilization rates were lower than expected. Use of the wait list was variable, and communication was fragmented.

49 Scheduling Status Pre A3 Patients are contacted and scheduled (ideally) within 48 hours of a physician referral and, once the patient is seen, getting return appointments scheduled in a timely manner. Work queues averaged from a low of 80 to 250, the wait list was used inconsistently, and processes varied depending on provider. Rehab Services and ORCM need to work collaboratively to provide appointments in a timely manner. Utilization rates were approximately 65%, compared to the expectation of 75%.

50 Box 2. Current State Words / Pictures
51 Voice of the Customer Patients overall were satisfied other than some dissatisfaction with being able to see the same therapist. Staff were dissatisfied with the timeliness of care and patients being scheduled properly. Front desk staff and therapy staff lacked unity.
52 What other information did we gather?
53
54
55 Box 3. Target State Where did we want to be?

56 What were we aiming for?
57 Box 4. Gap Analysis Getting to the Root Causes! What are the steps? 1. Brainstorm potential root causes 2. Organize (affinitize) into like groups 3. Put header cards on each section 4. Perform the 5 Whys 5. If necessary, multivote to determine focused number of causes to address 6. Perform the 5 Whys for each potential root cause

58


59 Results of the Gap Analysis
60 Box 5. Solution Approach

61 Box 6. Rapid Experiments Creating Standard Work

62 The new process map is much more efficient: a decrease of 5 non-value added steps, 6 decision points and 4 rework loops to schedule an evaluation!

63 Before After
 ORCM 07/29/15 2 Office staff education (MM,")

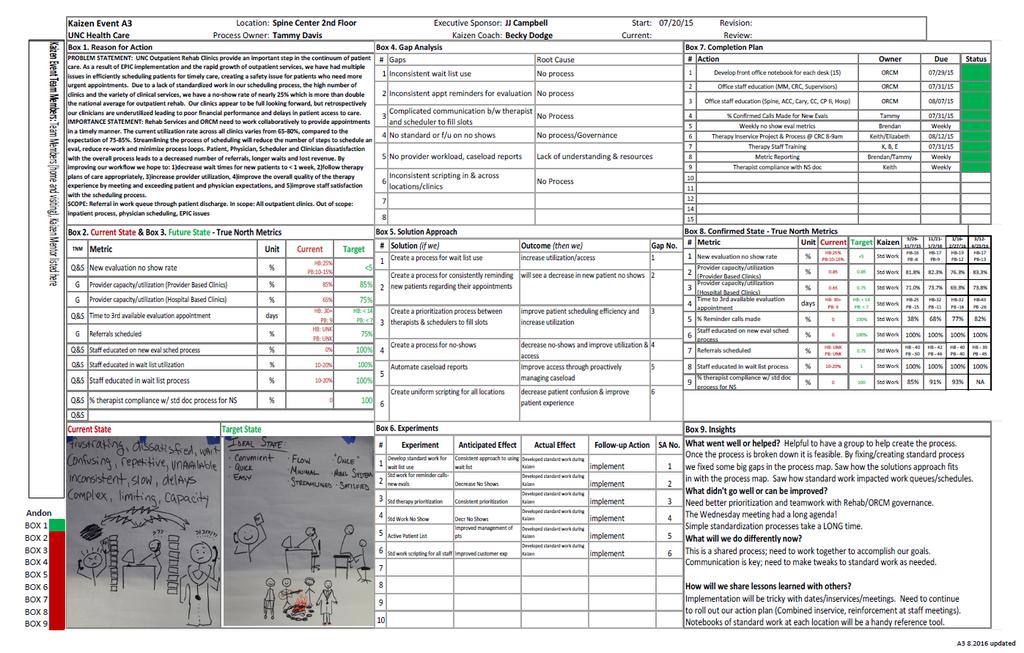
64 Box 7. Completion Plan # Action Owner Due Status 1 Develop front office notebook for each desk (15) ORCM 07/29/15 2 Office staff education (MM, CRC, Supervisors) ORCM 07/31/15 3 Office staff education (Spine, ACC, Cary, CC, CP II, Hosp) ORCM 08/07/15 4 % Confirmed Calls Made for New Evals Tammy 07/31/15 5 Weekly no show eval metrics Brendan Weekly 6 Therapy Inservice Project & CRC 8-9am Keith/Elizabeth 08/12/15 7 Therapy Staff Training K, B, E 07/31/15 8 Metric Reporting Brendan/Tammy Weekly 9 Therapist compliance with NS doc Keith Weekly
65 Box 8. Confirmed State # Metric Unit Current Target Kaizen 9 / / 7/ 1 1 New evaluation no show rate % Provider capacity/utilization (Provider Based Clinics) Provider capacity/utilization (Hospital Based Clinics) Time to 3rd available evaluation appointment HB:25% PB:10-15% <5 % % day s HB: 30+ PB: 9 HB: < 14 PB: < 7 5 % Reminder calls made % 0 100% 6 Staff educated on new eval sched process 7 Referrals scheduled % 8 9 True North Metrics Staff educated in wait list process % therapist compliance w/ std doc process for NS % 0 100% HB: UNK PB: UNK 0.75 % 10-20% 1 % Std Work Std Work Std Work Std Work Std Work Std Work Std Work Std Work Std Work HB-16 PB -8 11/ 2 1-1/ 2 / 1 HB-17 PB-9 1/ 16-2 / 2 7/ HB-19 PB-12 3 / 12-4 / 2 3 / HB-17 PB % 82.3% 76.3% 83.3% 71.0% 73.7% 69.3% 73.8% HB-25 PB -15 HB-32 PB -11 HB-32 PB -16 HB-43 PB % 68% 77% 82% 100% 100% 100% 100% HB - 40 PB - 50 HB - 42 PB - 46 HB - 40 PB - 40 HB - 39 PB % 100% 100% 100% 85% 91% 93% NA

66 Box 9. Insights

67 War Room
68


69 Sustaining the Change Audits were done to determine understanding/compliance with standard work Therapy and ORCM Leadership met weekly for 2 years to review data and continuously improve processes, now meet bi-weekly Therapy and ORCM staff now meet quarterly in a joint meeting Morale is UP! Repeat repeat repeat


70 So What does the data say?


71 Post Kaizen To-do List: Where do we begin? Standard Work review and updates Education of clinical and non-clinical staff Voice of customer/ feedback Metric definitions/identification Best way to collect/ obtain data Project out of scope list! (huge )


72 Standard Work New Evaluation Scheduling New Evaluation Reminder Calls Check in and out procedures Standardized scheduling slip Use of waitlist No show policy enforcement No show documentation Dismissing the non-compliant patient

73 Standard Work - Example Standardized use of scheduling slip with complexity to indicate priority for wait list


74 Standard Work These three aspects of standard work and education proved very important to the goal of decreasing our noshow rates: No show policy enforcement No show documentation Dismissing the non-compliant patient

75 Staff Education Each area of standard work was rolled out to the clinical and non-clinical staff in a variety of ways Lots of updates, revisions and re-education needed Small team meetings Larger staff meetings updates Kaizen Newsletter Standard work notebooks


76 Importance of VOC The action plan was implemented, but Feedback from staff indicated there was a lack of understanding of the standard work Further education to clinical staff of standard work of front desk staff (Who is taking care of what?)


77 Importance of VOC Restart of Implementation Audits of processes revealed inconsistencies Not everyone understood or was following the script Notebooks were not in color and important aspects were not clear/ highlighted Updates to standard work were not getting replaced in the notebooks

78 Metrics: What data was important to track? % No shows % No show New Evaluations % schedule utilization Time to 3 rd next New Evaluation slot Referral Work queue Totals % Therapist No show documentation Collections

79 Metric definitions: Work Queue Total The number of referrals waiting in the Epic work queue to get scheduled. This is a general indicator of access. Larger work queue volumes indicate longer lines of patients waiting to be seen, which leads to longer wait times to get patients in for an evaluation.

80 Metric definitions: % Therapist Use of No-show Documentation How many times the no-show documentation is completed in the chart compared to the overall number of no-shows. This helps track that physicians are being notified of patient noncompliance, and helps therapists spot patterns of noncompliance in the medical record. This also helps track need for dismissal from therapy and improved access for more compliant patients.

81 Initial Metric Tracking Display Each clinic had a display updated weekly for all staff to see real time results Eventually transitioned to an electronic version with periodic updates sent to staff.



82 Current Data Collection The Epic Appointment statistic report is run weekly for the previous week. The total visits, new and return appointments, no shows are filled into an Excel spreadsheet Time worked is added Formulas compute schedule utilization and no show percentages.


83 Current Data Collection WQ totals and time to 3 rd are also collected Each therapist data sheet is linked into a clinic roll- up Each clinic is linked to an on-going dashboard Working with programmers for an automated report and eventually an automated clinic dashboard

84 Data Collection- Sample Dashboard


85 Additional Problem Areas Tackled Referral Inconsistencies Single flow vs batching Inappropriate referrals or insufficient info Back and forth to correct and delay in care



86 Additional Problem Areas to Tackle Clinic Information Accurate clinic information needed for automated calls and printed appointments Easily accessible clinic information with maps and directions for patients Website overhaul for easily accessible, accurate and valuable information

87 Where are we now?



88 More Than The Numbers! Patient access, improved schedule utilization and reduced no-shows were the main initial drivers of this project Additional bonuses: Greatly improved relationship between clinical and nonclinical staff Greatly improved communication Better understanding of each area of responsibility and challenges Improved staff and patient satisfaction

89 I went through some helpless experiences trying to make an appointment at UNC Healthcare, including being on hold for literally hours with the Spine Center. When I finally reached them, their first opening was for two months later. However, after the first of this year things became much better and I am grateful that both of you were able to help me. Please tell whomever was responsible for fixing things, that his/her efforts have worked and I am extremely grateful for them. -Spine Center Patient The wait list function has been working exceptionally well and has been critical to maintaining a high utilization rate...the reminder calls for new evaluations have also been well received - post-project feedback from therapist staff member

90 Lessons Learned Our process was inconsistent and undefined Consistency is the key We have good people working hard to help patients get in for care but the process needed to support them Voice of the customer! Don t stop after the initial rollout: keep re-introducing and refining the process Better access = satisfied patients and staff Project and follow up was hard work but well worth it!
91 What is 5S? Sort Red tagging, eliminating supplies/ stuff Set Organize remaining items Shine Clean and maintain Standardize Standard work (labeling, pictures, videos, flowcharts, etc.) Sustain Audits and accountability

92 5S Wakebrook Before

93 5S Wakebrook After

94 Wakebrook Before




95 Wakebrook After

96 OT Psych Red Tag

97 OT Psych Before

98 OT Psych After

99 OT Psych Before

100 OT Psych After



101 OT Psych Additional Features

102 Equipment Room Before

103 Equipment Room After

104 Standard Work / Visual Management
105 Start small Build buy in Have successes Helpful Hints Proceed to larger projects Build leadership in your staff Create pull (vs push) how much change at one time? Drive quality through local area councils and Keep improving! You got this!

106
107 Thank you for the privilege of your time!
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Using Lean Principles to Decrease Outpatient Registration Wait Times. It s a Journey not a Destination
 Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Fall Prevention Protocol
 Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Engaging Frontline Staff in Real-Time Improvement
 Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Home Health Timely Care Value Stream Mapping Event
 1 Home Health Timely Care Value Stream Mapping Event Proactive Strategies for Fall Prevention November 7 & 8, 2012 Laura McNicholl, MS, RN-BC, CNS-BC; Mary Gibbons, MSN, RN, NE-BC Patient Falls-IFOH A
1 Home Health Timely Care Value Stream Mapping Event Proactive Strategies for Fall Prevention November 7 & 8, 2012 Laura McNicholl, MS, RN-BC, CNS-BC; Mary Gibbons, MSN, RN, NE-BC Patient Falls-IFOH A
Fall Prevention Program. St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer
 Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Fall Prevention Program St. Catherine Hospital East Chicago, Indiana Paula Swenson Chief Nursing Officer St. Catherine Hospital 189 bed community hospital, located in East Chicago Indiana Member of Community
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
Julie Bantle, MA, OT/L, Chief Operating Officer Deirdre Huneke, PT, Therapy Supervisor/FIM Coordinator
 Julie Bantle, MA, OT/L, Chief Operating Officer Deirdre Huneke, PT, Therapy Supervisor/FIM Coordinator Mercy Rehabilitation Hospital, St. Louis, Missouri A Partnership Between Kindred Healthcare and Mercy
Julie Bantle, MA, OT/L, Chief Operating Officer Deirdre Huneke, PT, Therapy Supervisor/FIM Coordinator Mercy Rehabilitation Hospital, St. Louis, Missouri A Partnership Between Kindred Healthcare and Mercy
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Laguna Honda Lean Transformation. Laguna Honda Strategic Performance Management November 2017
 Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Purpose and Objectives
 Fall Prevention Purpose and Objectives Purpose: Review the UC Health Fall Prevention Program. Objectives: 1. Present evidence about patient safety and falls. 2. Review the UC Health Fall Prevention Policy
Fall Prevention Purpose and Objectives Purpose: Review the UC Health Fall Prevention Program. Objectives: 1. Present evidence about patient safety and falls. 2. Review the UC Health Fall Prevention Policy
PFAC as Consultant to Hospital Initiatives
 4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
4th Annual Patient and Family Advisory Council Conference Strengthening Patient and Family Engagement in Massachusetts Hospitals PFAC as Consultant to Hospital Initiatives Lois Erhartic, Colleen McCauley,
When going Lean, Waste is the Enemy
 When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Reaching the Core of Quality
 Reaching the Core of Quality 7 th Annual American Nurses Association Nursing Quality Conference February 2013 Session 211: Engaging the Bedside Nurse in Quality Improvement Presented by: Holli Roberts,
Reaching the Core of Quality 7 th Annual American Nurses Association Nursing Quality Conference February 2013 Session 211: Engaging the Bedside Nurse in Quality Improvement Presented by: Holli Roberts,
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN
 NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN Robertson County is located approximately 30 miles north of Nashville. Robertson county sits between Cheatham, Davidson and Sumner counties and
NorthCrest Medical Center Amanda Costello RN, BSN, CMSRN Robertson County is located approximately 30 miles north of Nashville. Robertson county sits between Cheatham, Davidson and Sumner counties and
Fall Prevention at SMH
 Fall Prevention at SMH All hospitalized patients are at Risk to fall. The Fall risk assessment, located on the Nursing assessment flow sheet, helps to identify who is most at risk for falling. The fall
Fall Prevention at SMH All hospitalized patients are at Risk to fall. The Fall risk assessment, located on the Nursing assessment flow sheet, helps to identify who is most at risk for falling. The fall
Patient-Centered Case Management Assessment & Patient Interview Techniques
 Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
System redesign in Primary Care
 System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
Lynn Ives, MSN, RN-BC; Jessie Reich, MSN, RN, ANP-BC, CMSRN. Disclosure. Learning Objectives. The speakers have no conflicts of interest to disclose
 Reducing Falls with Injury on an Inpatient Geriatric Psychiatry Unit through Elevation of Nursing Support Staff: An Interprofessional Approach Lynn Ives, MSN, RN-BC Kathryn Farrell, MSN, RN John Brennan,
Reducing Falls with Injury on an Inpatient Geriatric Psychiatry Unit through Elevation of Nursing Support Staff: An Interprofessional Approach Lynn Ives, MSN, RN-BC Kathryn Farrell, MSN, RN John Brennan,
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 EFFECTIVE DATE: January January 2013 NPP600-E-6
 KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Inpatient Cerner Navigation and Documentation For Nursing Students
 Inpatient Cerner Navigation and Documentation For Nursing Students Audience Note: Purpose: Objectives: Cerner PowerChart training is for all students in the following inpatient areas Med/Surg, OSN, Oncology,
Inpatient Cerner Navigation and Documentation For Nursing Students Audience Note: Purpose: Objectives: Cerner PowerChart training is for all students in the following inpatient areas Med/Surg, OSN, Oncology,
Discharge Before Noon DH32
 Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
IHI Expedition: Smart Use of Resources: Nurses' Time. IHI Support Staff
 IHI Expedition: Smart Use of Resources: Nurses' Time Session 6 June 28, 2012 Content: Designing new care delivery models IHI Support Staff Tracy Jacobs Director Kayla DeVincentis Project Coordinator 2
IHI Expedition: Smart Use of Resources: Nurses' Time Session 6 June 28, 2012 Content: Designing new care delivery models IHI Support Staff Tracy Jacobs Director Kayla DeVincentis Project Coordinator 2
Patient Fall Prevention Orientation Module. Wheaton Franciscan Healthcare
 Patient Fall Prevention Orientation Module Wheaton Franciscan Healthcare Learning Objectives Define the goals of fall prevention Define a fall Identify patients at risk for falls Identify factors that
Patient Fall Prevention Orientation Module Wheaton Franciscan Healthcare Learning Objectives Define the goals of fall prevention Define a fall Identify patients at risk for falls Identify factors that
HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016
 HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016 Objectives: 1. Gain an in-depth understanding of four Core Leadership Competencies 2. Apply practical insights to developing
HIGH-IMPACT LEADERSHIP: DEVELOPING CORE LEADERS M12 Monday, December 5, 2016 Objectives: 1. Gain an in-depth understanding of four Core Leadership Competencies 2. Apply practical insights to developing
Falls Prevention In Rehabilitation
 Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
ATTENTION ALL C.N.A S
 ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Executive Summary Leapfrog Hospital Survey and Evidence for 2014 Standards: Nursing Staff Services and Nursing Leadership
 TO: FROM: Joint Committee on Quality Care Cindy Boily, MSN, RN, NEA-BC Senior VP & CNO DATE: May 5, 2015 SUBJECT: Executive Summary Leapfrog Hospital Survey and Evidence for 2014 Standards: Nursing Staff
TO: FROM: Joint Committee on Quality Care Cindy Boily, MSN, RN, NEA-BC Senior VP & CNO DATE: May 5, 2015 SUBJECT: Executive Summary Leapfrog Hospital Survey and Evidence for 2014 Standards: Nursing Staff
Fall Prevention. Falls 1
 Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
An academic medical center is practicing wasteology to pare time, expense,
 Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Solution Title: Sustaining Fall Prevention Over Time, Is It Possible?
 Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan
 Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan Stacey Willis Jr. MBA Emily Teesdale MSN RN 2 Spectrum
Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan Stacey Willis Jr. MBA Emily Teesdale MSN RN 2 Spectrum
Quality Improvement Medication Reconciliation Tools, Techniques and Tales
 Quality Improvement Medication Reconciliation Tools, Techniques and Tales Presented by: Marsha Nicholson, Steve Scott, City of Toronto Long-Term Care Homes and Services Division January 10, 2012 Outline
Quality Improvement Medication Reconciliation Tools, Techniques and Tales Presented by: Marsha Nicholson, Steve Scott, City of Toronto Long-Term Care Homes and Services Division January 10, 2012 Outline
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL!
 THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL! Multi-Disciplinary Team Peggy Benenati Risk Management Beverly Campbell Nursing Kim Cerri Quality Roberta Farley Physical Therapy Kelli Farnell
THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL! Multi-Disciplinary Team Peggy Benenati Risk Management Beverly Campbell Nursing Kim Cerri Quality Roberta Farley Physical Therapy Kelli Farnell
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Rapid Recovery Therapy Program. GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen
 Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Building a Lean healthcare machine
 Building a Lean healthcare machine PULSE Summer 2016 We re using Lean as a cultural transformation. We want to empower every member of our organization, particularly those at the frontlines and the bedside,
Building a Lean healthcare machine PULSE Summer 2016 We re using Lean as a cultural transformation. We want to empower every member of our organization, particularly those at the frontlines and the bedside,
Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses
 Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
Fall Protection and Prevention Program. Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare
 Fall Protection and Prevention Program Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare Objectives & About Us St. Elizabeth is a multi-facility Health Care System in Northern Kentucky hospitals,
Fall Protection and Prevention Program Wendy Bauer, MSN, NHA, NEA-BC St. Elizabeth Healthcare Objectives & About Us St. Elizabeth is a multi-facility Health Care System in Northern Kentucky hospitals,
Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach
 Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach INTRODUCTION Target Audience This toolkit is geared toward health care teams who have a basis of quality improvement
Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach INTRODUCTION Target Audience This toolkit is geared toward health care teams who have a basis of quality improvement
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
Innovative Methods to Manage the Investigatory Caseload. Angie Matthes Manager of Investigations
 Innovative Methods to Manage the Investigatory Caseload Angie Matthes Manager of Investigations Initial Intake/ Inquiry Phase Incoming/pending complaints High priority complaints Tracking case assignment
Innovative Methods to Manage the Investigatory Caseload Angie Matthes Manager of Investigations Initial Intake/ Inquiry Phase Incoming/pending complaints High priority complaints Tracking case assignment
SFGH. Management System. Components. SFGH Management System. Improvement. Time. Strategic Planning True North. Value Streams: Rapid Improvement Events
 SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Laguna Honda Hospital and Rehabilitation Center Value Stream #1 Admissions Kaizen Workshop #3 Room Readiness Report out.
 Laguna Honda Hospital and Rehabilitation Center Value Stream #1 Admissions Kaizen Workshop #3 Room Readiness Report out June 12 16, 2017 Value Stream Future Map Nov 2016 This is how the value stream mapping
Laguna Honda Hospital and Rehabilitation Center Value Stream #1 Admissions Kaizen Workshop #3 Room Readiness Report out June 12 16, 2017 Value Stream Future Map Nov 2016 This is how the value stream mapping
5 S Your Spring Cleaning with Lean Tools. Building Leaders Transforming Hospitals Improving Care
 5 S Your Spring Cleaning with Lean Tools Building Leaders Transforming Hospitals Improving Care Who We Are Our Company Formerly known as Brim Healthcare we have a 45 year track record of delivering superior
5 S Your Spring Cleaning with Lean Tools Building Leaders Transforming Hospitals Improving Care Who We Are Our Company Formerly known as Brim Healthcare we have a 45 year track record of delivering superior
Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project
 Pilot Project") Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project Dana Tschannen, PhD, RN Michelle Aebersold, PhD, RN University of Michigan, School of Nursing June 3, 2010 Presentation
Improving Student Critical Thinking Skills through a Root Cause Analysis (RCA) Pilot Project Dana Tschannen, PhD, RN Michelle Aebersold, PhD, RN University of Michigan, School of Nursing June 3, 2010 Presentation
2/5/2014. Patient Satisfaction. Objectives. Topics of discussion. Quality for the non-quality Manager Session 3 of 4
 Patient Satisfaction Quality for the non-quality Manager Session 3 of 4 Presented by Paul E. Frigoli, Ph.D.(c), R.N., C.P.H.Q., C.S.S.B.B. Certified Lean Six Sigma Master Black Belt Objectives At the end
Patient Satisfaction Quality for the non-quality Manager Session 3 of 4 Presented by Paul E. Frigoli, Ph.D.(c), R.N., C.P.H.Q., C.S.S.B.B. Certified Lean Six Sigma Master Black Belt Objectives At the end
Tehama County Health Services Agency Mental Health Division Quality Improvement Program
 Tehama County Health Services Agency Mental Health Division Quality Improvement Program The Mental Health Plan (MHP) shall have a written Quality Improvement (QI) Program Description in which structure
Tehama County Health Services Agency Mental Health Division Quality Improvement Program The Mental Health Plan (MHP) shall have a written Quality Improvement (QI) Program Description in which structure
Leadership. David Dalton Chief Executive
 Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Outpatient Services Improvement September 2010
 Service Improvement Team Outpatient Services Improvement September 2010 SUMMARY The purpose of this report is to give an update on the service improvement project within the outpatient department. BACKGROUND
Service Improvement Team Outpatient Services Improvement September 2010 SUMMARY The purpose of this report is to give an update on the service improvement project within the outpatient department. BACKGROUND
4/12/2016. High Reliability and Microsystem Stress. We have no financial, professional or personal conflict of interest to disclose.
 High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
3. Does the institution have a dedicated hospital-wide committee geared towards the improvement of laboratory test stewardship? a. Yes b.
 Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
The Quality Journey of
 The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
The University of Michigan Health System. Geriatrics Clinic Flow Analysis Final Report
 The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
Operational Assessments: Utilizing Productivity Standards
 Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
The Patient Experience at Florida Hospital Learning Module for Students
 The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
LEAN Community Care Coordination
 LEAN Community Care Coordination May 2013 to December 2013 Waterloo Wellington CCAC Lynda van Dreumel, Project Manager Dana Khan, Director Client Services Patricia DiRuzza, Manager Client Services Why
LEAN Community Care Coordination May 2013 to December 2013 Waterloo Wellington CCAC Lynda van Dreumel, Project Manager Dana Khan, Director Client Services Patricia DiRuzza, Manager Client Services Why
Building a Sustainable Telemonitoring Program from the Ground UP
 Building a Sustainable Telemonitoring Program from the Ground UP Kathy Duckett RN, BSN Director of Clinical Programs Partners Home Care kduckett@partners.org 781-290-4058 Objectives Upon completion the
Building a Sustainable Telemonitoring Program from the Ground UP Kathy Duckett RN, BSN Director of Clinical Programs Partners Home Care kduckett@partners.org 781-290-4058 Objectives Upon completion the
Lab Quality Confab Process Improvement Institute. New Orleans, LA. John Waugh 11/3/2015
 Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
CAH Quality Improvement and Care Transitions Collaborative
 CAH Quality Improvement and Care Transitions Collaborative Lean Concepts and TeamSTEPPS Tools Working Together to Improve Quality Outcomes July 14, 2016 How to Participate in the Session If you have called
CAH Quality Improvement and Care Transitions Collaborative Lean Concepts and TeamSTEPPS Tools Working Together to Improve Quality Outcomes July 14, 2016 How to Participate in the Session If you have called
Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology
 Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Checklists for Preventing and Controlling
 Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey -
 Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Alberta First Nations Continuing Care Needs Assessment p. 1 Alberta First Nations Continuing Care Needs Assessment - Health and Home Care Program Staff Survey - Definition of Terms Continuing Care: As
Falls Program on an Acute Psychiatric Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-15-2016 Falls
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-15-2016 Falls
Patient Centric Model (PCM)
") Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Observations for all areas: What type of supervision is provided to the resident and by whom? How are care-planned interventions implemented?
 Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Introductions. Learning Objectives. Financial Disclosure FORGING NEW MODELS: THE IN DEPTH INTERDISCIPLINARY TEAM (IDT) CARE COORDINATION MEETING
 CARE COORDINATION MEETING") FORGING NEW MODELS: THE IN DEPTH INTERDISCIPLINARY TEAM (IDT) CARE COORDINATION MEETING Introductions Presenters Suzanne Cast, MSW, LCSW Social Worker Lisa Kish Pittman, MSW, LCSW Social Worker Ana Jacobsen,
FORGING NEW MODELS: THE IN DEPTH INTERDISCIPLINARY TEAM (IDT) CARE COORDINATION MEETING Introductions Presenters Suzanne Cast, MSW, LCSW Social Worker Lisa Kish Pittman, MSW, LCSW Social Worker Ana Jacobsen,
Newport Hospital Interdisciplinary Falls Team (IFT) Summary; July 2010
 Summary; July 2010") Newport Hospital Interdisciplinary Falls Team (IFT) Summary; July 2010 The IFT is comprised of 26 representatives, 6 representatives being leadership mentors and the other 20 all direct care and support
Newport Hospital Interdisciplinary Falls Team (IFT) Summary; July 2010 The IFT is comprised of 26 representatives, 6 representatives being leadership mentors and the other 20 all direct care and support
Interprofessional Model of Care Redesign
 Interprofessional Model of Care Redesign Betty Anne Whelan, RN, MSN Project Manager Interprofessional Model of Care redesign Model of Care Review 2013 Summary of Findings( Completed by Professional Practice)
Interprofessional Model of Care Redesign Betty Anne Whelan, RN, MSN Project Manager Interprofessional Model of Care redesign Model of Care Review 2013 Summary of Findings( Completed by Professional Practice)
Our Journey Towards CAUTI Freedom. Johnson City Medical Center
 Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
Our Journey Towards CAUTI Freedom Johnson City Medical Center Objectives List two of the HICPAC appropriate indications for indwelling urinary catheters List two obstacles we encountered that prevented
Measurement Strategy Overview
 Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome