Session #:RO1. Advanced Strategies to Re-hospitalizations
|
|
|
- Aileen Horn
- 5 years ago
- Views:
Transcription


1 Session #:RO1 Advanced Strategies to Re-hospitalizations
2 Marsha Moxley RN, BSN, MA, CPHQ, FNAHQ
3 Objectives: Identify the various process measures involved in Re-hospitalizations Discuss ways to conduct Root Cause Analysis on Re-hospitalizations Identify strategies to avoid Re-hospitalizations Discuss innovative ideas experienced from participants (Lessons Learned)to reduce Rehospitalizations
4 WHY? WHY? WHY? Medicare Payment Advisory Commission estimates 75% of Re-hospitalizations are avoidable Estimated total hospital costs up to $44 billion annually More than 20% Re-hospitalizations within 30 days 90% are unplanned Re-hospitalizations rates vary from less than 10% to greater than 40%
5 FY2015 CMS is finalizing the expansion of the applicable conditions for FY2015 to include: Patients admitted for an acute exacerbation of chronic obstructive pulmonary disease (COPD) Patients admitted for elective total hip arthroplasty (THA) and total knee arthroplasty (TKA)
6 Effective Interventions to Reduce Re-hospitalizations (IHI study) Enhanced care and support at transitions Improved discharge processes, nurse education about disease management, remote monitoring, improved communication with hospital Improved patient education and self-management support Multidisciplinary team management Co-management between Ortho and Geriatric services early DC planning transmission of detailed DC instructions to the receiving facility Patient-centered planning at the end of life Referral to Hospice
7 No single intervention was regularly associated with reduced risk of 30-day Re-hospitalization. Hansen LO, Young RS, Hinami K, Leung A, Williams MV.Interventions to Reduce 30-Day Readmission: A systematic Review. Annuals of Internal Medicine; 2011 October: 155(8)
8 Some Process Drivers for Readmissions Staffing challenges Poor communication with transition of care Physician services minimal PCP involvement with transition planning Identity of high-risk residents Lack of education to disease management Hospital relations Use of Stop and Watch Use of SBAR Advance planning for end-of-life Lack of team approach
9 Some Strategies to Improve Processes Prior to Admission Conducting RCA and address causal factors Work with hospital(s) to review obstacles and what interventions could be put into place Engage residents and family in DC planning Meet with hospital staff prior to admitting meds reconciliation equipment needs lab results
10 Some Strategies to Improve Processes After Admission Use of Stop and Watch, SBAR and Huddles Staffing challenges addressed PCP engagement Education of staff and competencies to disease management and early detection of signs and symptoms Identify high-risk residents Resident and family education/re-education
11 Group Activity: What are some of Yours? Form into groups Discuss/list what challenges you are experiencing with your readmissions process Select a person to present to the audience

12 Group Activity Each group discuss your experiences with rehospitalizations and what worked well Select a scribe to capture these Lessons Learned Select a person to present to the audience Have some fun!

13 What did you Learn?




14 Root-Cause Analysis Basics Symptom of problem: THE WEED Above the surface Obvious Underlying causes: THE ROOT Below the surface Not obvious
15 Purpose of Root-Cause Analysis Continued To understand variation in process by exploring potential reasons or causal factors To identify opportunities that need to be changed in process

16 Root-Cause Analysis The ability and desire to continually make improvements can happen by asking: Why? Why? Why? Why? Why? Why? Is there a better way to do this?
17 Definitions Root-Cause Analysis (RCA) The process for identifying basic reasons or causal factors that underlie a variation in performance A method of problem solving that tries to identify root causes of faults or problems Wikipedia
18 Root-Cause Analysis (RCA) Root-Cause Analysis is a method of problem solving that tries to identify root causes of faults or problems. Wikipedia Root-Cause Analysis is not a single, sharply defined methodology; there are many different tools, processes and philosophies for performing RCA.

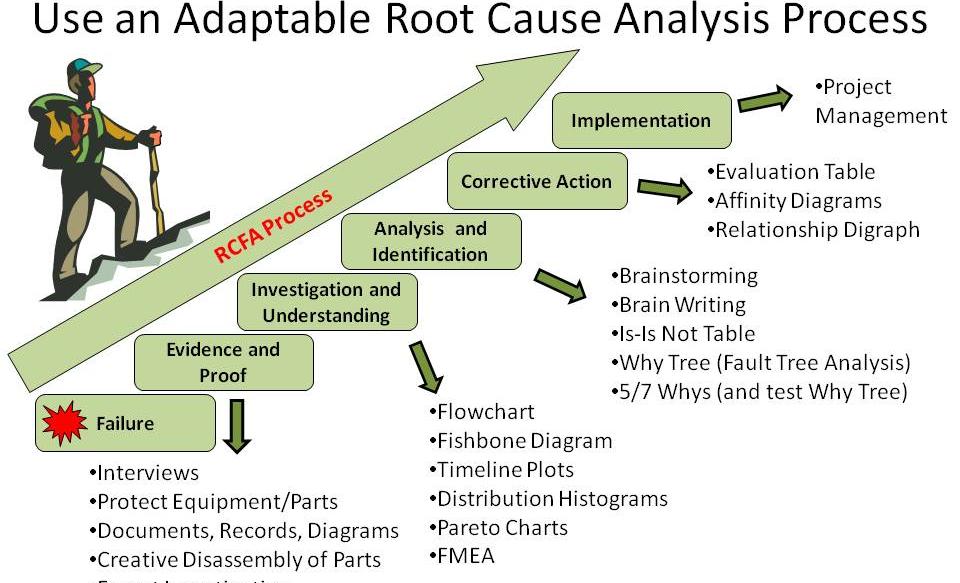
19 Various RCA Tools
20 Must Have s for Root-Cause Analysis Credibility Why? Is the RCA repeatedly digging deeper by asking why 5 times? Is there participation by leaders and associates that are closely involved with work in the process/system with the RCA? Does the RCA include considerations of any relevant literature (evidence-based practice)?

21 Symptom Root Cause
22 Keep Asking Why? What happened? Why did it happen? What can be done to prevent it from happening again? Where (location) is it happening most? What time of day? What day of the week? What shift? What unit?


23 If you don t involve the user you will develop the wrong system system. Brian Joiner

24 Group Activity Each group discuss your challenges with rehospitalizations and perform RCA Develop a list of ways to improve process/challenges Select a person to present to the audience Have some fun!
25 Case Study Group One Mrs. M Black was admitted to the facility on August 13, 2013 and is an 85 year old morbidly obese female and her medical diagnoses include: osteoarthritis, lumbago, diabetes without complications, chronic obstruction pulmonary disease, unspecified essential hypertension, atrial fibrillation, chronic kidney disease, esophageal reflux, history of venous thrombosis embolism. She was admitted to the hospital on 08/08/2013 with complaints of severe abdominal pain associated with alternating bouts of diarrhea and constipation. Resident (M. Black) is alert and oriented with intermittent confusion. She requires total assistance with transfers and bed mobility and rides a scooter throughout the facility. On August 29 th, 2014, Mrs. Black complained with chest and right arm pain, but stated she did not need to go to the hospital as the pain was not that severe. Vital signs were taken and were as follows; temperature 98.6, heart rate 94, respirations 26, blood pressure 130/68 and oxygen saturation of 96% on room air. Further assessment revealed increased anxiety, a hacky nonproductive cough and complaints of heartburn. MD notified and orders received to administer doxycycline 100mg by mouth twice daily for 7 days and Mucinex 600mg by mouth twice daily for 7 days. Orders processed, faxed to the pharmacy and implemented within 3 hours of receiving the orders. Documentation related to the change in condition continued throughout every shift with coughing continuing but slight improvement noted. Resident did not show signs and/or symptoms of adverse reactions related to antibiotic therapy and denied pain to chest and/or arm. On September 1, 2014 at 10:30 am, resident complained with chest pain and requested to go to the emergency room. Vital signs were 99.4, 60, 24, 120/60 and 02 saturation 93% on room air. Lung sounds were clear and there was no obvious shortness of breath noted. MD notified and orders received to send resident to the emergency room. September 1, 2014 at 5:00 pm, the hospital called to state resident was ready to return to the facility. She returned to the facility with the following diagnosis, COPD exacerbation and urinary tract infection. Resident received albuterol nebulizer treatments, Tylenol, Solumedrol and Macrobid while at the hospital. She returned to the facility with orders for Albuterol nebulizer treatments, prednisone 20mg tab, 2 tablets by mouth daily for 10 days and Macrobid 100mg daily for 10 days.
26 Case Study Two Resident #1 is an 82 year old white male who was admitted to the facility on 10/08/2014 with diagnoses of: CVA w/ Wallenberg syndrome, migraines, GERD, prostate CA, right posterior subarachnoid subdural bleed, C3 vertebral fracture, fall history, and DVT risk among others. He spent approximately 5 weeks in a Rehab facility prior to coming to Sunny USA. He was on a puree diet with Honey thick liquids on admission and had a PEG tube in place that was not in use. He showed no s/s of aspiration on admission. Nurses notes reflected no distress, compliant with his meals and use of thickened liquids. He was receiving ST, OT and PT. He was making good progress here in the facility. He was receiving no narcotics or psychoactive medications. His pain was managed with Salon pas patches. His DVT prevention was ASA. He had baseline labs on 10/09/2014 that showed his WBC within normal limits at 8.9. He did have an incident on 10/25 where he was stung by a bee sitting out on the front porch with his family. (He had no allergy to bee stings). First aid was provided immediately. MD was notified with an antihistamine prn order received. No respiratory distress noted, only site reaction to sting and itching. Benadryl was given by the nurse. The resident showed no s/s until evening of 10/27/2014 at approximately 8pm. The resident c/o of chills with a temperature of O2 saturation on room air was 92%, and a pulse 90 which was extremely high for him (he is normally in range). Resident had some coughing and increasing congestion. MD was called with orders received for a stat CXR and a urinalysis and C&S was ordered. The resident was medicated for elevated temp. Orders received for nebulizer as well. At 10:00 PM. The resident s O2 saturation was 73-80% while receiving O2 at 2L/minute. Nebulizer treatments were given as ordered. The resident s temperature was up to Pulse and respirations were increased. The resident began vomiting. Orders received for Zofran and Tylenol which were given. Respiratory distress continued and resident was sent out via 911 at 11 PM. Pertinent information: Labs routine at 14 days post admission showed WBC while still WNLs was increasing. (8.9 increased to 10.3). Potential indicator of infection brewing. PA was provided with report and made no changes in his plan. He was placed on the dashboard at the time of the bee sting and monitored x 72hrs with no unusual symptoms. Nurses notes well written to doc same. Stat CXR on 10/27 was negative and UA showed WBCs TNTC. This resident s returned to the facility on November 5, The resident s hospital admission diagnosis upon returning to the facility was sepsis, respiratory failure with aspiration and severe dysphagia. He had a UTI. His CXR in the ER was neg. He was treated with ABTs. He is also currently NPO and receives nutrition via PEG.
27 Some New Strategies to Improve Processes After Admission Disease management for infections, pneumonia, CHF, falls with fractures Medication Reconciliation-check Beers criteria Incorporate therapists and therapy Coordination of care with multidisciplinary team (PCP, Nursing, Therapy, Dietary, Social Services) Lab, Imaging, Cardiac monitoring, Telemedicine
28 Questions and Answers



29 Thank you! Marsha Moxley RN, BSN, MA, CPHQ, FNAHQ Vice President Clinical Quality 600 College Street P.O. Box 1547 Albertville, AL office cell Need Help? [Toll Free] Team TSI Corporation
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Final Report. January 12, Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek
 Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Recognizing and Reporting Acute Change of Condition
 Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Recognizing and Reporting Acute Change of Condition Welcome to the Elizabeth McGowan Training Institute Cell Phones and Pagers Please turn your cell phones off or turn the ringer down during the session.
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease This booklet has been written to answer questions that many patients and family members ask about their care during their hospital stay. It will explain the experiences
Chronic Obstructive Pulmonary Disease This booklet has been written to answer questions that many patients and family members ask about their care during their hospital stay. It will explain the experiences
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Essentials for Clinical Documentation Integrity 2017
 Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
New Models in Payment: Joint Replacements. Sharon Eloranta, MD February 18, 2016
 New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
EarlySense InSight. Integrating Acute and Community Care
 EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
Comprehensive Aspiration Risk Management Plan (CARMP) Individual s Name: Case Manager: Date of CARMP: DOB:
 Individual s Name: Case Manager: Date of CARMP: DOB:") Individual s Name: Case Manager: Date of CARMP: DOB: Case Management Agency: NOTE: Individuals at moderate risk for aspiration due to Risky Eating Behaviors (REB) identified as the only Aspiration Risk
Individual s Name: Case Manager: Date of CARMP: DOB: Case Management Agency: NOTE: Individuals at moderate risk for aspiration due to Risky Eating Behaviors (REB) identified as the only Aspiration Risk
Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC. Month Day Year / / Month Day Year
 / / UHHC. Month Day Year / / Month Day Year") Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
ACE PROGRAM Dysphagia Management
 ACE PROGRAM Dysphagia Management Purpose: The purpose of this program is to address dysphagia in the clients we serve. Dysphagia has far-reaching consequences to the overall health, medical condition,
ACE PROGRAM Dysphagia Management Purpose: The purpose of this program is to address dysphagia in the clients we serve. Dysphagia has far-reaching consequences to the overall health, medical condition,
CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENT PATHWAY
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATHWAY PROCESS OUTCOMES ADMISSION This will help you understand what will happen to you during your stay at the hospital. If you do not understand, please feel free
CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATHWAY PROCESS OUTCOMES ADMISSION This will help you understand what will happen to you during your stay at the hospital. If you do not understand, please feel free
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Role of Clinical Pharmacist in Primary Care Clinic HYOJIN SUNG, PHARM.D SALEM HEALTH MEDICAL GROUP OSMA ANNUAL CONFERENCE APRIL 14, 2018
 Role of Clinical Pharmacist in Primary Care Clinic HYOJIN SUNG, PHARM.D SALEM HEALTH MEDICAL GROUP OSMA ANNUAL CONFERENCE APRIL 14, 2018 Objectives Understand the scope of practice for pharmacist and role
Role of Clinical Pharmacist in Primary Care Clinic HYOJIN SUNG, PHARM.D SALEM HEALTH MEDICAL GROUP OSMA ANNUAL CONFERENCE APRIL 14, 2018 Objectives Understand the scope of practice for pharmacist and role
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Effective Tools to Prevent and Manage Adverse Events
 Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
REFERRAL GUIDELINES: Werribee Health Independence Program (HIP)
") All clients referred to the Werribee HIP are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
All clients referred to the Werribee HIP are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
Factors that Impact Readmission for Medicare and Medicaid HMO Inpatients
 The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population
 Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population Unified Quality Improvement Symposium March 31, 2017 Background Venous thromboembolism (VTE) is a
Raising Awareness: Venous Thromboembolism Prevention and Reduction in the Orthopedic Patient Population Unified Quality Improvement Symposium March 31, 2017 Background Venous thromboembolism (VTE) is a
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE
 DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE Speakers for this conference have disclosed that they do not have significant relationships or affiliations with any commercial organization that could
DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE Speakers for this conference have disclosed that they do not have significant relationships or affiliations with any commercial organization that could
Stage 2 GP longitudinal placement learning outcomes
 Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Snohomish County Case Management Nursing Services
 Snohomish County Case Management Nursing Services Carolyn Hundley, RN /Supervisor Denice Ulowetz, RN Kirstie Clinko, RN Sue Lee, RN Joy Maine, RN Amy Robertson, RN Overview New Changes in Nursing Services
Snohomish County Case Management Nursing Services Carolyn Hundley, RN /Supervisor Denice Ulowetz, RN Kirstie Clinko, RN Sue Lee, RN Joy Maine, RN Amy Robertson, RN Overview New Changes in Nursing Services
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Keeping Seniors at Home: An Emergency Department Link
 Keeping Seniors at Home: An Emergency Department Link Grey Matters 2012: Creating Age- Friendly Communities September 13, 2012 Presented by: Naeema Hudda, RN, BScN, Covenant Health & Jamie Davenport, MHSA,
Keeping Seniors at Home: An Emergency Department Link Grey Matters 2012: Creating Age- Friendly Communities September 13, 2012 Presented by: Naeema Hudda, RN, BScN, Covenant Health & Jamie Davenport, MHSA,
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
NM DDSD Intensive Medical Living Services Eligibility Parameter Tool A. MEDICATION ADMINISTRATION SEVERE 4 SIGNIFICANT 3 MODERATE 2 LOW 1 NONE - 0
 FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Quality Standards. Patient Reference Guide. Chronic Obstructive Pulmonary Disease Care in the Community for Adults. November 2017
 Quality Standards Patient Reference Guide Chronic Obstructive Pulmonary Disease Care in the Community for Adults November 2017 Quality standards outline what high-quality care looks like. They focus on
Quality Standards Patient Reference Guide Chronic Obstructive Pulmonary Disease Care in the Community for Adults November 2017 Quality standards outline what high-quality care looks like. They focus on
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence
 Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
OUTPATIENT ASSESSMENT SMMC: Page 1 of 5 Adopted Date: Revised Date: 10/02; 6/04; 11/04 Reviewed Date: Name Birthdate Phone Number:
 Name Birthdate Phone Number: Dear Patient and Family, Please answer the following questions. Your answers will help your health care team plan and give care to you or your significant other. A nurse will
Name Birthdate Phone Number: Dear Patient and Family, Please answer the following questions. Your answers will help your health care team plan and give care to you or your significant other. A nurse will
Preventing Avoidable Readmissions Together: Improving Discharge Summaries. R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC
 Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
Example 1 G202 Home Health Aide Services
 Example 1 G202 Home Health Aide Services NAME OF PROVIDER OR SUPPLIER: (X4) ID PREFIX TAG SUMMARY STATEMENT OF DEFICIENCIES (EACH DEFICIENCY MUST BE PRECEDED BY FULL REGULATORY OR LSC IDENTIFYING INFORMATION)
Example 1 G202 Home Health Aide Services NAME OF PROVIDER OR SUPPLIER: (X4) ID PREFIX TAG SUMMARY STATEMENT OF DEFICIENCIES (EACH DEFICIENCY MUST BE PRECEDED BY FULL REGULATORY OR LSC IDENTIFYING INFORMATION)
Skilled Nursing Facility Admission Orders
 Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
Medication Reconciliation
 Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
Tube Feeding Status Critical Element Pathway
 Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Return to independent living Self manage breathing techniques, secretion clearance Recognize early symptoms of COPD exacerbation
 CLINICAL PATHWAY Chronic Obstructive Pulmonary Disease Exacerbation (COPD-E) Civic General Clinical Frailty Scale (At baseline, at least 2 weeks before hospitalization) Init. Diagram Frailty Scale Description
CLINICAL PATHWAY Chronic Obstructive Pulmonary Disease Exacerbation (COPD-E) Civic General Clinical Frailty Scale (At baseline, at least 2 weeks before hospitalization) Init. Diagram Frailty Scale Description
4/24/2012. Cake Walk for a Successful National Government Services Medical Review Process. Today s Presenter. Disclaimer. Sally Rosiello, BSN
 Cake Walk for a Successful National Government Services Medical Review Process 2012 Today s Presenter Sally Rosiello, BSN 2 Disclaimer has produced this material as an informational reference for providers
Cake Walk for a Successful National Government Services Medical Review Process 2012 Today s Presenter Sally Rosiello, BSN 2 Disclaimer has produced this material as an informational reference for providers
The POLST Conversation POLST Script
 The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
Outpatient/Community Health Nursing
 2043_Ch08_125-144.qxd 9/25/08 3:37 PM Page 125 8 Outpatient/Community Health Nursing Intuition will tell the thinking mind where to look next. Jonas Salk ABBREVIATION LIST ACE AHA BP D5W ECG GERD HCP H&H
2043_Ch08_125-144.qxd 9/25/08 3:37 PM Page 125 8 Outpatient/Community Health Nursing Intuition will tell the thinking mind where to look next. Jonas Salk ABBREVIATION LIST ACE AHA BP D5W ECG GERD HCP H&H
MARATHON HEALTH CENTER a benefit of CHG Health and Wellness
 Health & Wellness MARATHON HEALTH CENTER a benefit of CHG Health and Wellness WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE PEOPLE TO LEAD HEALTHIER LIVES. CHG Healthcare Services
Health & Wellness MARATHON HEALTH CENTER a benefit of CHG Health and Wellness WE ARE A DIFFERENT KIND OF HEALTHCARE COMPANY. OUR MISSION IS TO INSPIRE PEOPLE TO LEAD HEALTHIER LIVES. CHG Healthcare Services
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
Partnering with the Care Management Department. Medical Staff and Allied Health Practitioner Orientation
 Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
Partnering with the Care Management Department Medical Staff and Allied Health Practitioner Orientation 10/2015 Department of Care Management Medical Directors of Care Coordination Inpatient Case Managers
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
CONSULTANT PHARMACIST LICENSING PROGRAM SELF-ASSESSMENT EXAMINATION **** 2014 ANSWER SHEET ****
 CONSULTANT PHARMACIST LICENSING PROGRAM SELF-ASSESSMENT EXAMINATION **** 2014 ANSWER SHEET **** (Mark all correct answers, may be more than one answer per question) 1. Pharmaceutical Services in the Long
CONSULTANT PHARMACIST LICENSING PROGRAM SELF-ASSESSMENT EXAMINATION **** 2014 ANSWER SHEET **** (Mark all correct answers, may be more than one answer per question) 1. Pharmaceutical Services in the Long
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES. By Maureen Kroning EdD, RN
 A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Community Health Needs Assessment Mercy Hospital Ardmore 2012
 Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Appropriate Care Pathway
 Appropriate Care Pathway Karen Titchener MSc NMP RGN Deputy Head Nursing Guys and St Thomas NHS Foundation Trust Jaqualine Lindridge MA, PG Cert, MCPara Consultant Paramedic London Ambulance Service NHS
Appropriate Care Pathway Karen Titchener MSc NMP RGN Deputy Head Nursing Guys and St Thomas NHS Foundation Trust Jaqualine Lindridge MA, PG Cert, MCPara Consultant Paramedic London Ambulance Service NHS
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL