MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story
|
|
|
- Joella McCoy
- 5 years ago
- Views:
Transcription
1 SHN MedRec National Teleconference MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story Medication Management Support Services (MMSS) Speakers: Mary Burello-Cordovado Lisa Sever 1
2 Medication Management Support Services (MMSS) The MMSS program has been recognized provincially and nationally. They were short-listed for the Ontario Ministry of Health s - Health Achieve, Patient Safety in Nov Won the Commitment to Care s Overall Patient Care Award in Nov was also the 2010 Innovation Award finalist at the Innovations In Health Care Expo related to Medication Management Support Services and keeping seniors healthy and safe.
3 Mary Burello-Cordovado, RN, BSCN Mary is an experienced Senior Manager with and has been the Project Manager for Medication Management Support Services since its inception in She has successfully implemented this service and received the Individual Care Award with the Ontario CCAC s in June 2011 for implementing this program.

4 Lisa Sever RPh, ACPR, BSc Phm Lisa graduated from the University of Toronto in 1992 and completed her residency at St. Joseph s Hospital, Hamilton, ON in She has held positions at St. Joseph s and York Central Hospital focusing on the ambulatory care populations. Her experience with the Dialysis population allowed her to witness the medication complications that arise when patients cross the continuum of care home to hospital and back. Lisa joined the Medication Management Support Services at a Kaizen event in August 2008 and immediately saw how pharmacists in the home care setting could benefit patient care. She joined the team as the Lead Pharmacist in December Lisa won the OPA s Award of Merit for her role in MMSS in June
5 Medication Management Support Services (MMSS) June 5, 2012 Presenters: Mary Burello-Cordovado, Senior Manager, Client Services Central Community Care Access Centre Lisa Sever, MMSS Pharmacy Lead, York Central Hospital Outstanding care every person, every day 5
6 Objectives Background Opportunity for Improvement MMSS process / Meds Check process MMSS database Results and Benefits Next Steps 6
7 Central Community Care Access Centre () One of 14 CCACs in Ontario Provincial agency funded by the Ministry of Health and Long-Term Care through the Central LHIN Provide in-home care to children and adults Determine eligibility and facilitate access to long-term care homes Approximately 23,000 clients on service every day 700 staff and 35 service provider agencies providing a range of services: nursing, physiotherapy, occupational therapy, Speech Language Pathology, Dietician, social work and personal support service 7
8 What is the problem? Clients returning home from hospital at risk for falls, ER visits and hospital readmits due to medication related adverse events No standardized approach to medication management Clients being asked for the same information by multiple care providers Information not shared between various care and service providers, e.g. Meds Check 8
9 The Need Required a standardized process for medication management in the community Sustainable process that generates quality data to track changes / improvements in clients outcomes Accountable to the Central Local Health Integration Network (funders of the project) Develop an easy-to-use system Internally align with organization s strategy to provide quality care = safety, science, service 9
10 Background MMSS established processes, with LEAN value-stream analysis, between June 2008 and December 2008 Implemented in December 2008 with nurses Implemented in January 2009 with pharmacists Collaborative approach with partners: York Central Hospital Southlake Regional Health Centre VHA Rehab Solutions ISMP Canada 10
11 What is the Eligibility Criteria? Adults Taking three (3) or more prescription medications Have one (1) or more chronic diseases Valid OHIP; eligible for CCAC services Resident of One or more risks as identified in eligibility criteria (falls, frequent visits to ER/hospitalizations, uncontrolled pain) 11
12 Method CCAC Case Manager assesses client using RAI-CA or RAI-HC CCAC Case Manager determines that client would benefit from medication review Outcomes from RAI-HC/RAI-CA Client meets eligibility criteria Case Managers make referral based on criteria: Meds Check (Community Pharmacist service) OR Medication Management Support Services (CCAC service) 12
13 Criteria for Meds Check Patient does not understand medication regimen Physical limitations with taking medication Medicine cabinet clean up May benefit from increased medication adherence via provision of medication schedule, compliance package or dosette setup Concern regarding interactions of medications with prescription, over the counter (OTC) or natural products Requiring updated medication listing 3 months prior to admission to Long Term Care 13
14 Criteria for MMSS Community pharmacy unable to provide Meds Check Transitioning from hospital to home Concern re: taking high alert medications Client s active unresolved medication management issues Cognitive limitations Pain (uncontrolled) History of falling possibly related to medication Symptoms of adverse drug events Service may offset the need for hospital admission and/or ED visit 14
15 Meds Check Method Case Manager confirms community pharmacy of choice with client/caregiver Contacts community pharmacy to inform of request Completes and faxes Meds Check referral form Waits for medication list from community pharmacy Timeframe requested: 14 days 15
16 Meds Check referral form To be Completed by REASON FOR REFERRAL MedsCheck MedsCheck at Home Specify limitation: physical cognitive accessibility safety knowledge storage and organization Other: MEDICAL INFORMATION Main Concern(s) Medical History Medications Script attached Client is pending admission to LTC home 16
17 Meds Check referral form cont d The above named client/substitute Decision Maker has consented to proceed with a MedsCheck referral. Please complete MedsCheck within 14 days and fax back this form and a MedsCheck list to at the number provided below. Please indicate the outcome below: MedsCheck completed. Medication list is attached. Issues resolved. MedsCheck completed. Medication list and issues are attached. Issues need further investigation to resolve. Please refer to MMSS*. To be Completed by Community Pharmacist: Unable to perform a MedsCheck within 14 days. Please refer to MMSS*. Family Physician (please print clearly): *Medication Management Support Services (MMSS) is a service to provide pharmacy consultation for Case complicated Manager: clients. If your assessment reveals the client has Phone too #: many ( ) issues to resolve within your timeframe / expertise, please refer them back to CCAC for an assessment by our (MMSS) program. Pharmacy Name and Fax#: Pharmacist Name (please print): Date: Pharmacist Signature: 17
18 MMSS Method Case Manager sends MMSS referral based on criteria Client Health Related Information System (CHRIS) set up with pharmacy consultation Sends referral via Health Partner Gateway (secure method of transmitting Personal Health Information electronically) Authorize 2 visits over a 60-day period 70% of referrals require 2 visits 30% of referrals require 1 visit only 18
19 What is the opportunity? MMSS implemented to support clients in the community and those returning home from hospital who are at risk for falls, ER visits and hospital readmits due to medication adverse events Phase 1: paper capture - variation in data quality depending upon the provider; helped to refine the data capture Phase 2: Identify how to capture, share, and report via a secure, web-based database 19
20 MMSS Database Secure, web-based, automated solution for Central CCAC s Medication Management Support Services (MMSS) application Process improvement ability to exchange secure information Reduction in workload for CCAC staff Better Accessibility and Transparency of MMSS information Broader range of information available to Improved Data Quality 20
21 21
22 22
23
24 24
25 25
26 MMSS PHARMACY HOME VISIT 26
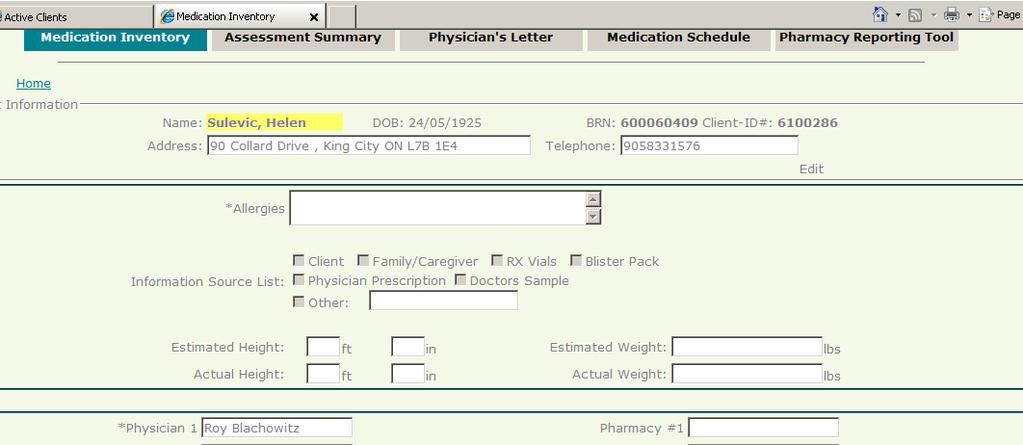
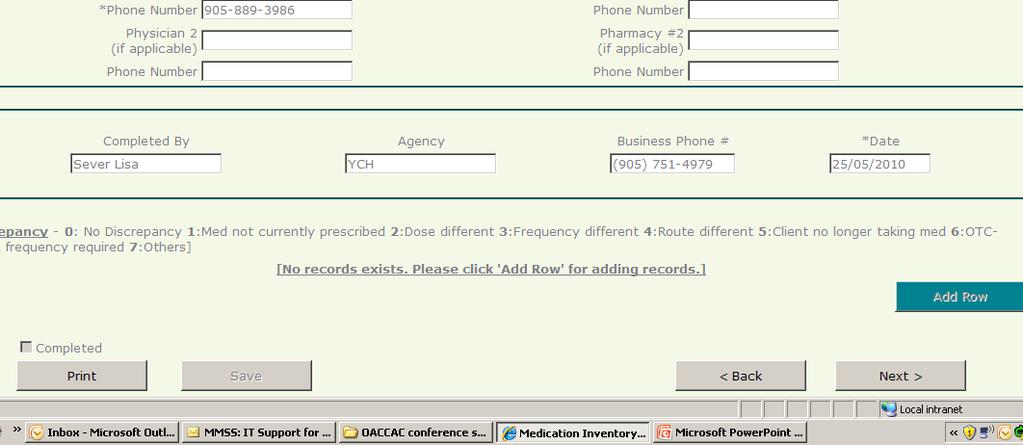
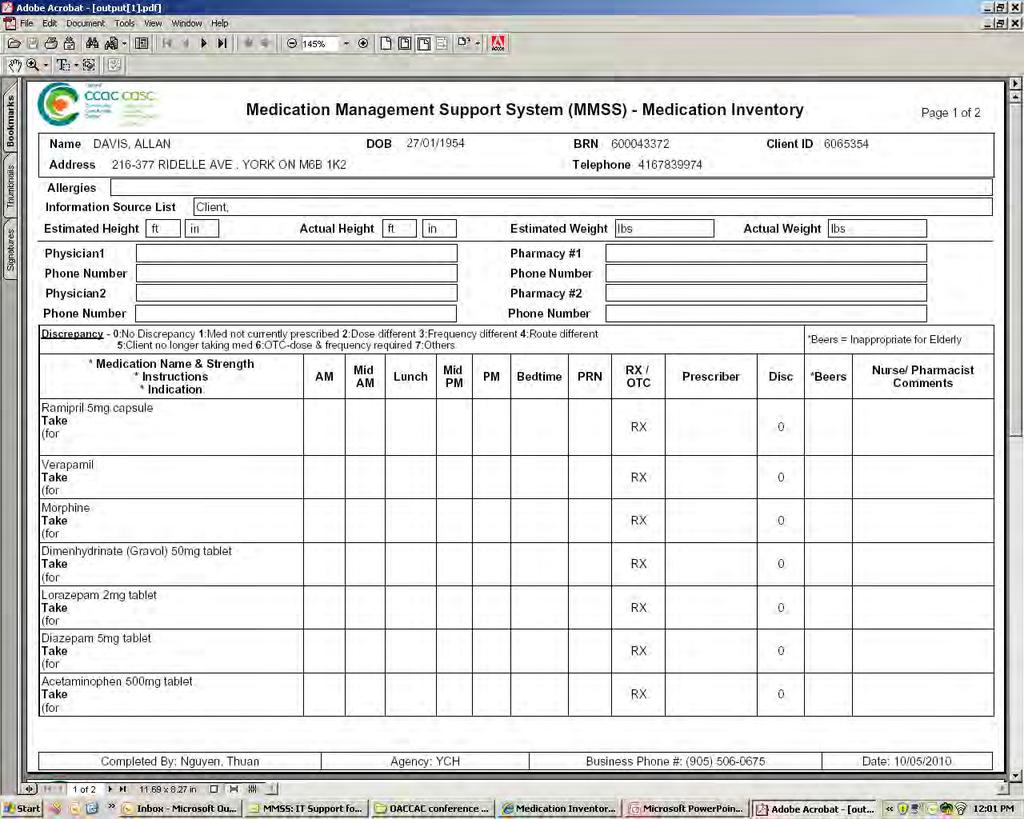
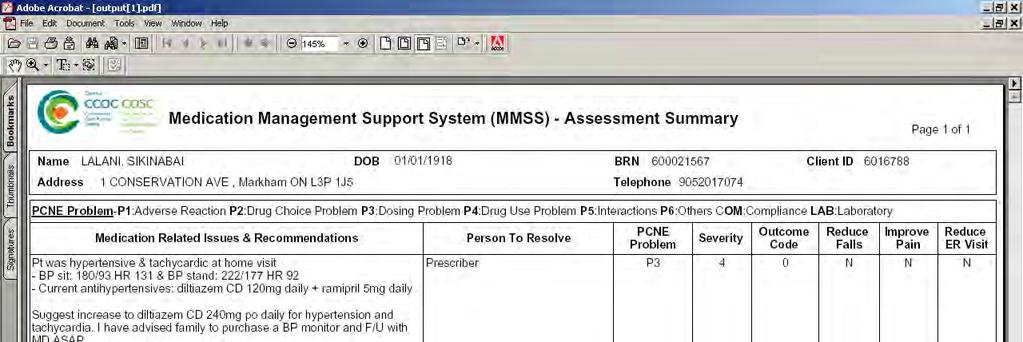
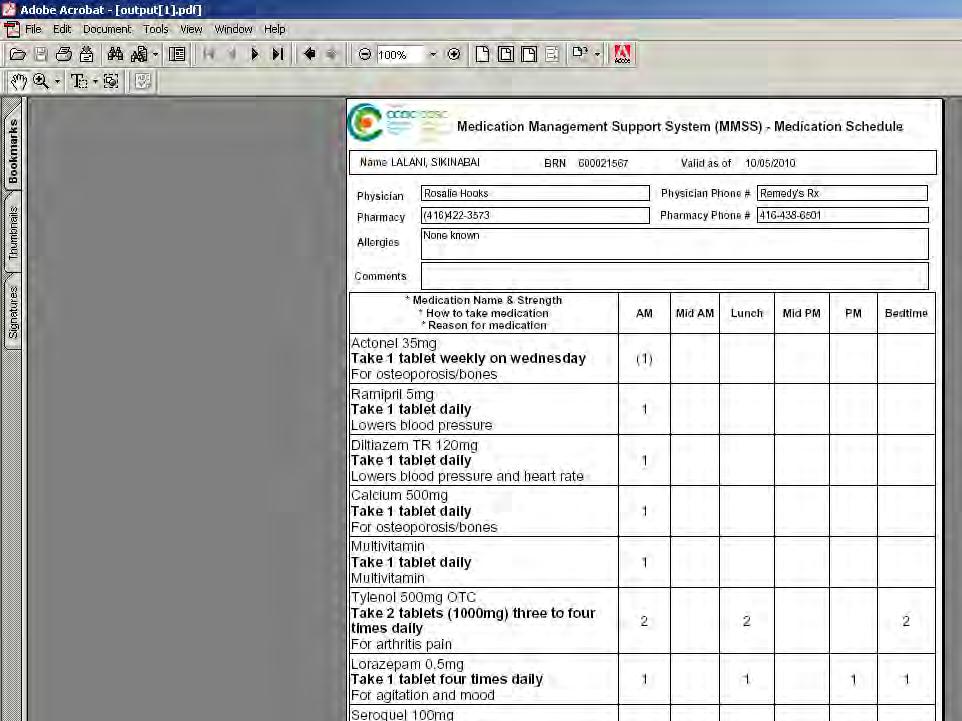
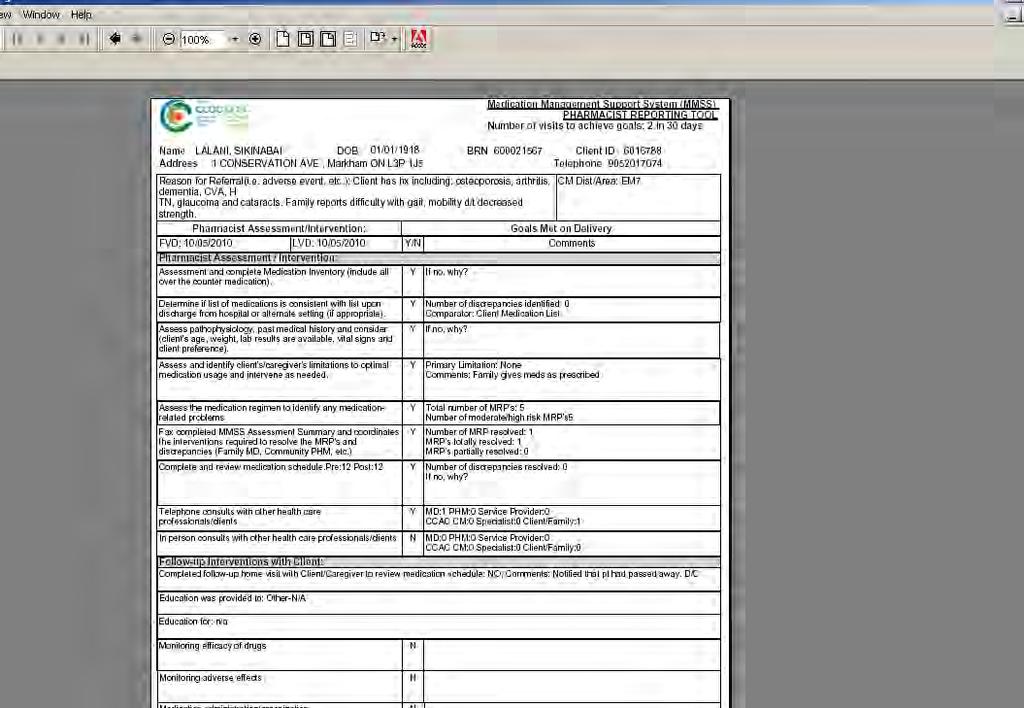
27 What can the client/caregiver expect? First visit: The pharmacist completes a medication inventory Best Possible Medication History (BPMH) Makes recommendations to client/caregiver or Case Manager Preventive medicine is used and prescribed appropriately (e.g., Vitamin D, EC ASA) Blister pack or dosette system, visual reminders Increased PSW hours for reminders, OT assessment, referral to a community support agency Link with community pharmacy Summary completed identifying discrepancies and recommendations; pharmacist sends letter(s) to client s physicians 27
28 What can the client/caregiver expect? Second visit: Incorporate physician response into medication plan Link with community pharmacy Provide education to client/caregiver Administration techniques as appropriate Provide client/caregiver with medication schedule CCAC forwards copy of medication schedule to family physician and service providers 28


29 Assessing limitations that lead to discrepancies or MRP s Physical Cognitive Accessibility Adherence Safety Knowledge Storage 29
30 Role of Pharmacist Create an accurate inventory of all medications Prescriptions, over-the-counter, herbal Assess for safety, simplicity and correctness Compare current regimen with prescribed medications Identify any discrepancies or medication related problems Bring to attention of prescribing physician 90% response rate from physicians Resolve issues and follow-up to ensure client success 30
31 Benefits to Clients/Caregivers Better ways to organize and schedule medications Learn to take medications safely and avoid serious drug interactions Avoid visits to the hospital or Emergency Room caused by medication-related problems Better understanding of why they are taking their medications Improved health because medications are working better for them 31
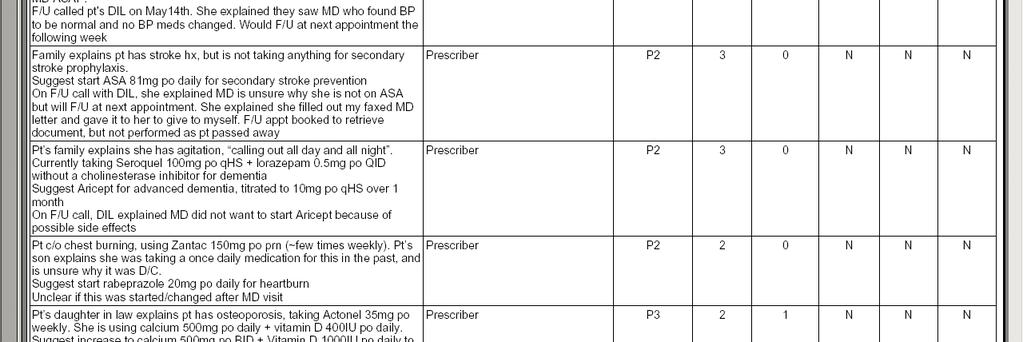
32 Let s consider these cases What could possibly go wrong? 32
33 Communication glitches Client B.W. living at a retirement home, medication administered by nursing MMSS Pharmacist reviews Medication Administration Record and compares to hospital discharge Rx Notes three discrepancies - No Nitroglycerin spray, Aranesp or dutaseride Finding/Resolution: Page 3 of the discharge Rx was lost in transmission Discrepancies resolved and client was able to receive these medications 33
34 Discharge instructions No one told me to change anything Medication reviewed with son and client Client used to be independent with his medications but now requires assistance from son Client s main complaint is dizzy a lot Standing BP 97/59 Client s medications: Amlodipine 5 mg daily Metoprolol 50 mg bid HCTZ 25 mg daily Were these the discharge instructions? 34
35 Lack of Knowledge Cost was an issue too! Admitted for a GI bleed (diagnosed as duodenal ulcer) Computerized discharge prescription given to patient including a PPI (the main drug!) PPI not covered by provincial drug plan Client was unaware of importance of medication, so decided not to pick up prescription due of cost Community pharmacist unaware of why Rx had been prescribed has many GI uses Client had NSAIDs in his home for arthritis pain (contraindicated in a fresh GI bleed) 35

36 New Care Provider the wife Appointment made with client s wife who reluctantly agrees to a pharmacist visit Hospital and community pharmacist reviewed medication schedule in detail with wife prior to client s discharge What did the MMSS pharmacist find? 36
37 Hospital orders not implemented once home Admission for nausea and vomiting, postural hypotension Many medications were adjusted in hospital Client was given a discharge medication schedule and new prescriptions Visiting pharmacist came 1 week after discharge and found patient had reverted to her preadmission medication regimen! 37
38 Risky business Lack of medication monitoring Discharged home on warfarin Unable to get to lab due to physical exhaustion / weakness Unaware of risks associated with too much or discontinuation of warfarin stopped taking after 6 days In home INR testing had not been set-up at discharge Family MD was advised, accepted responsibility for dosage/monitoring in home lab arranged until patient was able to go to outside lab 38
39 Until you look for medication problems You have no idea what you are missing!! 39
40 Outcomes Have we made a difference? 40

41 MMSS Summary 2011/12 Information taken from MMSS Tracker 41

42 Indicator List 2011/12 42

43 Community & Hospital Referrals Information taken from MMSS Tracker 43

44 Discrepancies & MRP s Information taken from MMSS Database 44

45 Pre & Post Medications Information taken from MMSS Database 45

46 Follow up services required Information taken from MMSS database 46

47 Average wait time Information taken from MMSS tracker 47

48 Self-Reported Survey Results 48

49 Annual Cost Savings 49

50 Results 50


51 Home First Clients Discharged from Hospital Success Stories Caregiver was given a handwritten list with new medications only Caregiver assumed this list was complete and did not resume previous meds Pharmacist had to clarify if the old meds need to be restarted (e.g. ASA for a fresh stroke) Educate caregiver that previous meds need to be administered as well 50-year-old male requiring total care Spouse checks blood sugar many times during the day MMSS pharmacist identified that spouse purchased own test strips; Rx was not received to allow billing under ODB MMSS pharmacist obtained Rx for test strips to be covered under ODB and provided necessary education re: blood sugar monitoring to alleviate spouse s anxiety Patient discharged from Hospital and no oral meds sent home MMSS pharmacist contacted hospital and obtained a Rx with necessary meds Client was discharged on April 3; Home visit was on April 9 (within 7 days timeframe) and order received on April 10 Client taking 7-8 medications and ½ of the medication regimen had a discrepancy Client taking wrong dose; blood pressure was low and fluctuated when sitting and standing Daughter not aware that medications changed on discharge MMSS pharmacist called GP on discharge and referral made to CCAC for nurse to administer medication and check blood pressure Caregiver received a more simplified medication regimen and associated education 51
52 ImagineNation Challenge Next Steps engaged in expanding medication reconciliation electronically via the MMSS database Community pharmacy Rapid Response Nurses Contracted Nursing Providers within Engage other CCACs interested in MMSS database 52
53 Discussion & Questions 53
54 Upcoming MedRec National Webinars ET Sept 1, 2012: Accreditation Canada, speaker Greg Kennedy Nov 13, 2012: Date to be confirmed January 8, 2013: topic to be determined March 5, 2013: topic to be determined
55 We encourage you to report medication incidents Practitioner Reporting Consumer Reporting
Making a PDiF-ference Results of the PDiF Quality Improvement Initiative
 Making a PDiF-ference Results of the PDiF Quality Improvement Initiative March 2014 www.saferhealthcarenow.ca Bienvenue! Welcome also to our francophone attendees Bienvenue à nos participants francophones
Making a PDiF-ference Results of the PDiF Quality Improvement Initiative March 2014 www.saferhealthcarenow.ca Bienvenue! Welcome also to our francophone attendees Bienvenue à nos participants francophones
Making a case for medication reconciliation in primary care
 Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool
 Tool") How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Long Term Care Pharmacy
 Long Term Care Pharmacy Medication Reconciliation in The Electronic Age Courtney Doherty Oland R.Ph, MBA President The LTC setting is currently under enormous transformation silver tsunami - greater demand/
Long Term Care Pharmacy Medication Reconciliation in The Electronic Age Courtney Doherty Oland R.Ph, MBA President The LTC setting is currently under enormous transformation silver tsunami - greater demand/
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
IHA Regional Pharmacy Best Possible Medication History Practice Standard
 IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
Medication Reconciliation
 Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Hospital Pharmacy. Tutorial Series. Title slide without an image. Tutorial series learning objectives. Tutorial overview Learning outcomes
 Hospital Pharmacy Title slide without an image Tutorial Series Tutorial series learning objectives To understand the roles of hospital pharmacists, including in the continuum of patient care. To recognise
Hospital Pharmacy Title slide without an image Tutorial Series Tutorial series learning objectives To understand the roles of hospital pharmacists, including in the continuum of patient care. To recognise
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016
 COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
Medicine Management Policy
 INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
DRUG COVERAGE PEARLS FOR THE HOSPITAL PHARMACIST. Souzi Badr BScPhm, PharmD, ACPR
 DRUG COVERAGE PEARLS FOR THE HOSPITAL PHARMACIST Souzi Badr BScPhm, PharmD, ACPR Disclosures Presenter Disclosure I have no current or past relationships with commercial entities I have received no speaker
DRUG COVERAGE PEARLS FOR THE HOSPITAL PHARMACIST Souzi Badr BScPhm, PharmD, ACPR Disclosures Presenter Disclosure I have no current or past relationships with commercial entities I have received no speaker
Medication Reconciliation
 Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Mental Health Pharmacist Education. Medication Reconciliation Patient Safety Initiative
 Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population
 Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Medication Management: Therapy Scope Versus Comfort Level
 Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Medication Reconciliation. Peggy Choye, Pharm.D., BCPS
 Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Health Advocacy Tips for Family Caregivers and Care Recipients. An Educational Program of the
 Health Advocacy Tips for Family Caregivers and Care Recipients An Educational Program of the National Family Caregivers ers Association Today s program is designed to better prepare you and your loved
Health Advocacy Tips for Family Caregivers and Care Recipients An Educational Program of the National Family Caregivers ers Association Today s program is designed to better prepare you and your loved
JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge
 JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge Donna L. Poole, Juliane N. Chainakul, Mary Pearson, LeAnn Graham Keywords: Discharge, Information technology, Medication
JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge Donna L. Poole, Juliane N. Chainakul, Mary Pearson, LeAnn Graham Keywords: Discharge, Information technology, Medication
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
Safe & Sound: How to Prevent Medication Mishaps. A Family Caregiver Healthcare Education Program. A Who What Where Why When Tool Kit
 Safe & Sound: How to Prevent Medication Mishaps A Family Caregiver Healthcare Education Program A Who What Where Why When Tool Kit National Family Caregivers Association www.thefamilycaregiver.org 800/896-3650
Safe & Sound: How to Prevent Medication Mishaps A Family Caregiver Healthcare Education Program A Who What Where Why When Tool Kit National Family Caregivers Association www.thefamilycaregiver.org 800/896-3650
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care
 Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
ISMP Canada Progress Report. to the. Ontario Ministry of Health and Long-Term Care. and the. Ontario Pharmacy Council. June 2009
 ISMP Canada Progress Report to the Ontario Ministry of Health and Long-Term Care and the Ontario Pharmacy Council June 2009 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire
ISMP Canada Progress Report to the Ontario Ministry of Health and Long-Term Care and the Ontario Pharmacy Council June 2009 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
YOUR DISCHARGE IS SOMEONE S ADMISSION
 YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
LEVELS OF CARE FRAMEWORK
 LEVELS OF CARE FRAMEWORK DISCUSSION PAPER July 2016 INTRODUCTION In Patients First: A Roadmap to Strengthen Home and Community Care, May 2015, the Ontario Ministry of Health and Long-Term Care stated its
LEVELS OF CARE FRAMEWORK DISCUSSION PAPER July 2016 INTRODUCTION In Patients First: A Roadmap to Strengthen Home and Community Care, May 2015, the Ontario Ministry of Health and Long-Term Care stated its
University of Wisconsin Hospital and Clinics Medication Reconciliation Education Packet
 Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Patient Safety Initiatives
 Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
OSCE demo Oral Structured Clinical Examination
 OSCE demo Oral Structured Clinical Examination Patient interview. ü Aim: Identify incorrect medications in medication list Physician discussion. ü Aim: Implement correct medication list Tommy Eriksson
OSCE demo Oral Structured Clinical Examination Patient interview. ü Aim: Identify incorrect medications in medication list Physician discussion. ü Aim: Implement correct medication list Tommy Eriksson
Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project
 1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
Prescribing Standards for Nurse Practitioners (NPs)
") Standards Prescribing Standards for Nurse Practitioners (NPs) Month Year PRESCRIBING FOR NURSE PRACTITIONERS MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Standards Prescribing Standards for Nurse Practitioners (NPs) Month Year PRESCRIBING FOR NURSE PRACTITIONERS MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta () Provincial
St. Michael s Hospital Medication Reconciliation Learning Package
 St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Getting Started with Medication Reconciliation in Long Term Care. SHN! MedRec Teleconference September 14, EST
 Getting Started with Medication Reconciliation in Long Term Care SHN! MedRec Teleconference September 14, 2010 1200-1300 EST 1 Welcome! By the end of this teleconference, participants will: Understand
Getting Started with Medication Reconciliation in Long Term Care SHN! MedRec Teleconference September 14, 2010 1200-1300 EST 1 Welcome! By the end of this teleconference, participants will: Understand
Information shared between healthcare providers when a patient moves between sectors is often incomplete and not shared in timely enough fashion.
 THE DISCHARGE MEDICINES REVIEW SERVICE Introduction During a stay in hospital a patient s medicines may be changed. Studies show that many patients may experience an error or problem with their medicines
THE DISCHARGE MEDICINES REVIEW SERVICE Introduction During a stay in hospital a patient s medicines may be changed. Studies show that many patients may experience an error or problem with their medicines
Who s s on What? Latest Experience with the Framework Challenges and Successes. November 29, Margaret Colquhoun Project Leader ISMP Canada
 Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Penticton & District Community Resources Society. Child Care & Support Services. Medication Control and Monitoring Handbook
 Penticton & District Community Resources Society Child Care & Support Services Medication Control and Monitoring Handbook Revised Mar 2012 Table of Contents Table of Contents MEDICATION CONTROL AND MONITORING...
Penticton & District Community Resources Society Child Care & Support Services Medication Control and Monitoring Handbook Revised Mar 2012 Table of Contents Table of Contents MEDICATION CONTROL AND MONITORING...
Lewisham Integrated Medicines Optimisation Service
 Lewisham Integrated Medicines Optimisation Service By Kath Howes (CCG) & Kay Fahy (University Hospital Lewisham) Katherine.howes@nhs.net LIMOS: 02030493228 Seen this before??- Hoarding & Wastage The Story
Lewisham Integrated Medicines Optimisation Service By Kath Howes (CCG) & Kay Fahy (University Hospital Lewisham) Katherine.howes@nhs.net LIMOS: 02030493228 Seen this before??- Hoarding & Wastage The Story
Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors
 Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors January 2011 (as updated September 2012) Ministry of Health and
Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors January 2011 (as updated September 2012) Ministry of Health and
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
POLICY AND PROCEDURE: MEDICATION
 POLICY AND PROCEDURE: MEDICATION Cheshire does not administer medication. However, front line staff provide physical assistance with medication at the consumer/client s direction. (Exception: Cheshire
POLICY AND PROCEDURE: MEDICATION Cheshire does not administer medication. However, front line staff provide physical assistance with medication at the consumer/client s direction. (Exception: Cheshire
NP Discharge & Admission: Legislative Authority
 The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
Harrison Memorial Hospital Cynthiana, KY. Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018
 Harrison Memorial Hospital Cynthiana, KY Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018 About Us HMH is a regional healthcare facility licensed to operate 61 beds 20
Harrison Memorial Hospital Cynthiana, KY Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018 About Us HMH is a regional healthcare facility licensed to operate 61 beds 20
All Wales Multidisciplinary Medicines Reconciliation Policy
 All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
ehealth Report for Ed Clark November 10, 2016 My Background and Context:
 ehealth Report for Ed Clark November 10, 2016 My Background and Context: I worked for a number of years for OHIP at the Ministry of Health in Kingston. Several major project initiative involved converting
ehealth Report for Ed Clark November 10, 2016 My Background and Context: I worked for a number of years for OHIP at the Ministry of Health in Kingston. Several major project initiative involved converting
Getting Started Kit MEDICATION RECONCILIATION IN HOME CARE. Version 2. Reducing Harm Improving Healthcare Protecting Canadians
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN HOME CARE Getting Started Kit Version 2 March 2015 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN HOME CARE Getting Started Kit Version 2 March 2015 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to
Medication Adherence. Office Staff Training
 Medication Adherence Office Staff Training 2018. All rights Learning Objectives The participant will be able to: Describe the lifestyle of seniors. Identify the challenges of medication adherence. Utilize
Medication Adherence Office Staff Training 2018. All rights Learning Objectives The participant will be able to: Describe the lifestyle of seniors. Identify the challenges of medication adherence. Utilize
Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP
 Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP 1.Review What a Consultant Pharmacist Does and the Role of Pharmacy for Long Term Care Facilities 2.Identify Key Components of a Medication
Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP 1.Review What a Consultant Pharmacist Does and the Role of Pharmacy for Long Term Care Facilities 2.Identify Key Components of a Medication
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS
 BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Inpatient Anticoagulation Management Services to Improve Transitions of Care
 Inpatient Anticoagulation Management Services to Improve Transitions of Care Andrea Resseguie PharmD, RPh, CACP Advanced Practice Clinical Specialist Anticoagulation Management Service Learning Objectives
Inpatient Anticoagulation Management Services to Improve Transitions of Care Andrea Resseguie PharmD, RPh, CACP Advanced Practice Clinical Specialist Anticoagulation Management Service Learning Objectives
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Medication Adherence
 Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Medication Adherence. Pharmacy and Pharmaceutical Sciences
 Pharmacy and Pharmaceutical Sciences Medication Adherence Sabrina Anne Jacob B.Pharm(Hons.), MPharm, PhD(Clinical Pharmacy) Lecturer School of Pharmacy Monash University Malaysia Adherence is the extent
Pharmacy and Pharmaceutical Sciences Medication Adherence Sabrina Anne Jacob B.Pharm(Hons.), MPharm, PhD(Clinical Pharmacy) Lecturer School of Pharmacy Monash University Malaysia Adherence is the extent
PHCY 471 Community IPPE. Student Name. Supervising Preceptor Name(s)
") PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
Rapid Recovery Therapy Program. GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen
 Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Pharmacy Medication Reconciliation Workflow Emergency Department
 Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Form CMS (5/2017) Page 1
 Page 1") Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Tackling the challenge of non-adherence
 Tackling the challenge of non-adherence 2 How is adherence defined? WHO definition: the extent to which a person s behaviour taking medication, following a diet and/or executing lifestyle changes corresponds
Tackling the challenge of non-adherence 2 How is adherence defined? WHO definition: the extent to which a person s behaviour taking medication, following a diet and/or executing lifestyle changes corresponds
STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists. Issued by: Contact:
 STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists Standing Order used for the Community Pharmacy Anticoagulant Management (CPAM) Service
STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists Standing Order used for the Community Pharmacy Anticoagulant Management (CPAM) Service
Coordinated Care Planning
 Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
Coordinated Care Planning What is a Coordinated Care Plan? A plan for your care that is created with you and your family (as per your direction) and involves all the members of your health care team. What
Getting Started Kit MEDICATION RECONCILIATION IN LONG-TERM CARE. Reducing Harm Improving Healthcare Protecting Canadians
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit March 2012 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to join
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit March 2012 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to join
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ
 Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Looking Back and Looking Forward. A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs)
") Looking Back and Looking Forward A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs) DANYAL MARTIN LAURIE DUNN NOVEMBER 20, 2017 Learning Objectives Share learnings from the 2017/18
Looking Back and Looking Forward A Sneak Peek for the 2018/19 Home Care quality improvement plans (QIPs) DANYAL MARTIN LAURIE DUNN NOVEMBER 20, 2017 Learning Objectives Share learnings from the 2017/18
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Medication Reconciliation as a Patient Safety Practice During Transitions of Care
 Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
Workflow Best Practices. Ashley Branham, PharmD, BCACP Bri Morris, PharmD
 Workflow Best Practices Ashley Branham, PharmD, BCACP Bri Morris, PharmD Disclosures Ashley Branham is receiving an honorarium for this program. The conflict of interest was resolved by peer review of
Workflow Best Practices Ashley Branham, PharmD, BCACP Bri Morris, PharmD Disclosures Ashley Branham is receiving an honorarium for this program. The conflict of interest was resolved by peer review of
Getting Started Kit MEDICATION RECONCILIATION IN LONG-TERM CARE. Version 3. Reducing Harm Improving Healthcare Protecting Canadians.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit Version 3 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit Version 3 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting
 Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Learner Manual. Document Best Possible Medication History (BPMH)
") Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
Medication Reconciliation for Older Adults Transitioning from. Long-Term Care to Home. Allison (Leverett) Kackman
 Kackman") Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
A Discussion of Medication Error Reduction Strategies
 A Discussion of Medication Error Reduction Strategies By: Donald L. Sullivan, R.Ph., Ph.D. Program Number: 071067-011-01-H05 C.E.U.s: 0.1 Contact Hours: 1 hour Release Date: 4/1/11 Expiration Date: 4/1/14
A Discussion of Medication Error Reduction Strategies By: Donald L. Sullivan, R.Ph., Ph.D. Program Number: 071067-011-01-H05 C.E.U.s: 0.1 Contact Hours: 1 hour Release Date: 4/1/11 Expiration Date: 4/1/14
COMMITTEE REPORTS TO THE BOARD
 Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Quality, Risk and Patient Safety Report Fiscal Year , Third Quarter Submitted to: Board of Directors March 3, 2017
 Quality, Risk and Patient Safety Report Fiscal Year 20, Third Quarter Submitted to: Board of Directors March 3, 2017 Analysis and Ideas for Improvement Contributed by Staff of the North East CCAC Date
Quality, Risk and Patient Safety Report Fiscal Year 20, Third Quarter Submitted to: Board of Directors March 3, 2017 Analysis and Ideas for Improvement Contributed by Staff of the North East CCAC Date
Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin
 Protocol Number: 7 Protocol Title: Ambulatory Initiation and Management of Warfarin for Adults Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin Target Patient
Protocol Number: 7 Protocol Title: Ambulatory Initiation and Management of Warfarin for Adults Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin Target Patient
C O M M U N I T Y H E A L T H C E N T E R S 1
 C O M M U N I T Y H E A L T H C E N T E R S 1 Medical/Dental Home? A Patient Centered Medical/Dental Home is called a "home" because we would like it to be the first place you think of for all your healthcare
C O M M U N I T Y H E A L T H C E N T E R S 1 Medical/Dental Home? A Patient Centered Medical/Dental Home is called a "home" because we would like it to be the first place you think of for all your healthcare
FACILITATOR GUIDE. inotice Professional Development Program and Resources
 inotice Professional Development Program and Resources FACILITATOR GUIDE Heightened awareness of safe medication management for aged care community workers Contents BACKGROUND... 3 INTRODUCTION... 4 FACILITATION...
inotice Professional Development Program and Resources FACILITATOR GUIDE Heightened awareness of safe medication management for aged care community workers Contents BACKGROUND... 3 INTRODUCTION... 4 FACILITATION...
Pharm2Pharm Standard Operating Procedures. University of Hawai i at Hilo The Daniel K. Inouye College of Pharmacy Center for Rural Health Science
 Pharm2Pharm Standard Operating Procedures University of Hawai i at Hilo The Center for Rural Health Science INTRODUCTION PURPOSE: The purpose of the Pharm2Pharm Standard Operating Procedures (SOPs) is:
Pharm2Pharm Standard Operating Procedures University of Hawai i at Hilo The Center for Rural Health Science INTRODUCTION PURPOSE: The purpose of the Pharm2Pharm Standard Operating Procedures (SOPs) is:
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Primary care patient experience survey April 2016
 Primary care patient experience survey April 2016 Survey overview 1. This version of the survey does not show the logic that skips people to appropriate questions based on their answers. Not all people
Primary care patient experience survey April 2016 Survey overview 1. This version of the survey does not show the logic that skips people to appropriate questions based on their answers. Not all people
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Objectives. Institutional Pharmacy Practice. Medicare, Medicaid, What s the difference? Medicare Modernization Act
 Objectives Institutional Pharmacy Practice Donald H. Williams, RPh, FASHP Affiliate Professor University of Washington To discuss the regulation of institutional pharmacy practice in Washington To differentiate
Objectives Institutional Pharmacy Practice Donald H. Williams, RPh, FASHP Affiliate Professor University of Washington To discuss the regulation of institutional pharmacy practice in Washington To differentiate
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Objectives. Medication Therapy Management: The Important Role of the Pharmacy Technician. Medication Therapy Management (MTM)
") Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
IMPROVING MEDICATION RECONCILIATION WITH STANDARDS
 Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital