Making a PDiF-ference Results of the PDiF Quality Improvement Initiative
|
|
|
- Christiana Moore
- 6 years ago
- Views:
Transcription

1 Making a PDiF-ference Results of the PDiF Quality Improvement Initiative March

2 Bienvenue! Welcome also to our francophone attendees Bienvenue à nos participants francophones Hélène Riverin Conseillère en sécurité et en amélioration Safety Improvement Advisor
3 Objectives of today s call Colleen Cameron: Describe the PDiF initiative, its outcomes and key lessons learned. A few practical challenges to consider. Marg Colquhoun: The MedRec Journey from 2005 and onwards. 3
4 Please input your Questions All questions will be addressed at the end of the webinar Ask questions or send feedback via the chat box Select All participants Type message Click Send All Participants


5 Where to find our webinars
6 Please complete our poll 6
7 Making a PDiF-ference Results of the PDiF Quality Improvement Initiative Colleen Cameron, RPh, Pharm.D. PDiF Coordinator, Grand River Hospital ISMP Canada/Safer Healthcare Now! April 8, 2014
8 Objectives Describe the PDiF initiative, its outcomes and key lessons learned. A few practical challenges to consider.
9 Guelph General Hospital Grand River Hospital St. Mary s General Hospital Groves Memorial Hospital WW LHIN (775,000 people) Cambridge Memorial Hospital St. Joseph s Health Centre North Wellington Health Care




10 PDiF = Pharmacy Discharge Facilitator
 Perindopril Bisoprolol Clopidogrel Lantus")
11 Two stories - 63 year old male - 3 rd cardiac event. - Discharged post-stent insertion. $$$ $$$ $$$ PRE Metformin ASA Atorvastatin Ramipril Bisoprolol POST Metformin ASA Lipitor (Brand) Perindopril Bisoprolol Clopidogrel Lantus Rapid Ezetimibe Esomeprazole Docusate Senokot Nitro Patch
12 Two stories Losartan 100mg Irbesartan 300mg


13 Two stories Losartan 100mg 200 Irbesartan 300mg

14 The most unpredictable variables in the entire equation
15 Pharmacy Discharge Facilitator Project What is it? Quality Improvement Initiative Uniquely included 2 local CEOs in its development Possibly helped to keep the project s profile and momentum January-September 2013 Facilitate medication discharge for high-risk medicine patients with a goal of improving care and outcomes PDiF team = pharmacist + University of Waterloo pharmacy co-op student
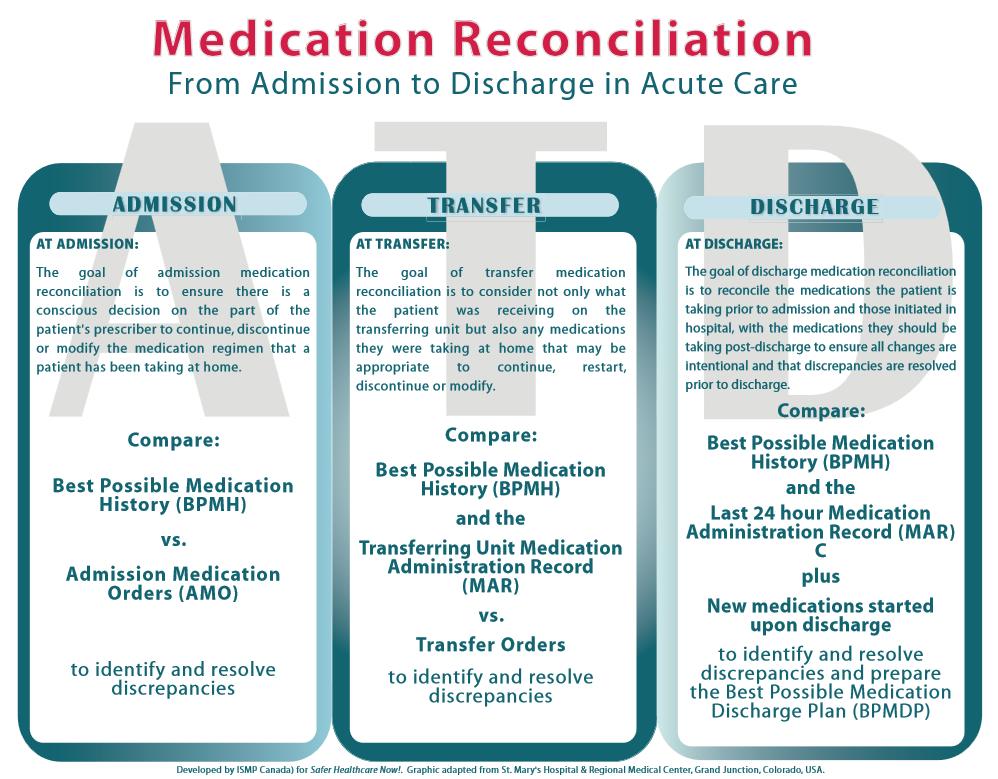
16 Medication Care Map in Hospital Patient Pharmacy MD Discharge Pt Admitted To Hospital Discharge preparation and coordination BPMH Completed / AMR (Best Possible Medication History/ Admission Med Red) Medication Therapy In Hospital
17 Components of PDiF Patient Pharmacy MD Discharge Pt Admitted To Hospital PDiF 1 On admission Identify High-Risk Patients Discharge preparation and coordination BPMH Completed (Best Possible Medication History) Medication Therapy In Hospital
18 Components of PDiF Patient Pharmacy MD Discharge Pt Admitted To Hospital PDiF 2 During hospital stay Modify medications that will be practical and make sense for discharge Discharge preparation and coordination BPMH Completed (Best Possible Medication History) Medication Therapy In Hospital
19 Components of PDiF PDiF 3 At time of MD Patient Discharge preparation and coordination Discharge Pharmacy Pt Admitted To Hospital BPMH Completed (Best Possible Medication History) discharge 1. Communicate with involved health care providers about medication changes and rationale for those changes. 2. Talk to patient/ caregiver to ensure they understand directions. Medication Therapy In Hospital
20 Components of PDiF Patient Pharmacy MD Discharge Pt Admitted To Hospital PDiF 4 Post-discharge - Call patient hours postdischarge to see if they are able to follow the instructions we gave them. Discharge preparation and coordination BPMH Completed (Best Possible Medication History) Medication Therapy In Hospital
21 Outcomes Qualitative Patient / caregiver satisfaction Primary Care Provider satisfaction Community Pharmacist satisfaction Hospitalist satisfaction Quantitative 7, 30 and 90 day ER visits 7, 30 and 90 day readmissions Conservable Bed Days unexpected
22 Demographics # of patients seen 148 (+) Average age 74.2 years 7 patients died during index hospital admission % Age Ranges 79%
23 Age Range % of Patients % (N=5) % (N=26) % (N=52) % (N=65) Heart Failure (# of pts) Diabetes (# of pts) Warfarin (# of pts) Total 148 pts 26% 43% 51%
24 Qualitative Outcomes Did we achieve Patient / Caregiver satisfaction? Did we achieve Primary Care Provider satisfaction? Did we achieve Community Pharmacist satisfaction? Did we achieve Hospitalist satisfaction?

25 Quantitative Outcomes (#, $) ER/Readmission Rates 7, 30 and 90 day ER visits 7, 30 and 90 day hospital readmission rates Data disclaimer Historical = All comers young patients, DKA, pneumonias, acute ingestions, dialysis PDiF patients
26 GRH Readmission Rates - Historical CIHI 13.3% % FY FY FY FY day 30 day 90 day
27 GRH Readmission Rates CIHI 13.3% % FY FY FY FY PDiF 0 7 day 30 day 90 day
28 ER Visit Rates - Baseline % FY FY FY FY day 30 day 90 day
29 ER Visit Rates % FY FY FY FY PDiF 0 7 day 30 day 90 day


30 What do these numbers have the statistical power to prove? Anything? probably not Causality? certainly not Benchmarking? - maybe Is that the only information that matters? What if patients subsequently go elsewhere for care?

31 Quantitative Outcomes (#, $) Hospital Readmissions and ED Visits At first glance, our PDiF numbers look great


32 Quantitative Outcomes (#, $) Hospital Readmissions and ED Visits At first glance, our PDiF numbers look great BUT

33 This is bigger than GRH
34 Quantitative Outcomes (#, $) Conservable Bed Days Definition relevance Over 9 months, PDiF realized 8 weeks of conservable bed days Medications involved Warfarin, Methadone Unexpected, but fascinating Consequently have started targeting patients on medications that are more likely to delay discharge Warfarin / NOACs Insulin
35 Top 5 lessons learned 1. Dare to look at your patients experience post-discharge. Are they seeing their family doctor postdischarge? Are they getting their prescriptions filled as expected? Are they going to other local hospitals for subsequent visits? Follow-up phone calls are quick, and incredibly valuable!
36 Top 5 lessons learned 2. Drugs delay discharge Warfarin, LMWHs, insulins, methadone We now assess 100% of patients on warfarin for timely and safe discharge from Medicine program Assist with LMWH coordination post-discharge Educate injection technique while in hospital Phone call follow ups Anticoagulation summary of INRs & warfarin doses, Ensure patient has appt with PCP as well as plans to go to lab
37 Top 5 lessons learned 2 ½. Where there is warfarin (or NOACs) there are other medication misadventures looming Warfarin and NOACs are predictors of other highrisk medications (insulin, digoxin, spironolactone, amiodarone etc) Most computer systems can search for certain medications. This is the best place to start!


38 Top 5 lessons learned 3. Use the hospital admission to optimize chronic medications Clinical inertia Look for adherence issues!!! ODB DPV has picked up on MANY misadventures Incorporate practical medication discharge assessment upstream
39 Top 5 lessons learned 4. Medication knowledge transfer contributes to efficient and safe patient care GRH has an electronic discharge prescription but. PCPs and Community Pharmacists need information about medications, including rationale and plans of care. What is your ehealth system? Fusion software (transcription software) Clinical Connect (LHIN EHR) Medication-Focused Discharge Summaries

40 Medication-Focused Discharge Summary One of the most valuable interventions from the PDiF project!
41 Medication-Focused Discharge Summaries Standardized document including Date of Admission/Discharge Adherence Issues Identified** Drug Cost Issues Identified Numerical List of medications comment if same, increased, decreased or new Medications discontinued or held Additional information Commentary including plan of care, monitoring plans, concerns My name and telephone extension
42 Top 5 lessons learned 5. Discharge medication reconciliation is time consuming! Track outcomes/stories to strengthen your argument for more funding Go to your program director with proposal Develop a business case? Dr. Schnipper s data Be creative in staffing Pharmacist : patient ratio Pharmacy students Pharmacy Technicians Financially: 1 pharmacist 2 technicians 4 co-op students
43 Summary Was the PDiF project successful? Did we improve outcomes? Unequivocally Are there simple strategies every hospital can implement to help these patients? Absolutely Medication misadventures We don t even know the magnitude of the problem yet





44
45 The MedRec Journey Margaret Colquhoun, B.Sc.Phm., FCSHP, R.Ph., Project Lead, ISMP Canada Institute for Safe Medication Practices Canada (ISMP Canada)
46 Objectives To talk about the MedRec from Highlight SHN tools and resources Highlight your accomplishments To announce changes in Institute for Safe Medication Practices Canada (ISMP Canada)


47 Thanks to Canadian Patient Safety Institute 2005 MedRec Intervention 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

48 MedRec 2005 Unknown did not know what we did not know Systems not in place Measures not in place Studies not driving practice change
49 Things I am Proud of!!! Creation of new language and knowledge Being used around the world Whole country worked together and learned together as a team Tools and Resources Webinars, kits, questions Unbelievable sharing though our network of MedRec teams across Canada 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

50 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

51 Action for Safer Medical Care Medication Reconciliation, CMPA/ACPM, Institute for Safe Medication Practices Canada (ISMP Canada)

52 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

53 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

54 2014 Institute for Safe Medication Practices Canada (ISMP Canada)



55 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

56 2014 Institute for Safe Medication Practices Canada (ISMP Canada)


57 Institute for Safe Medication Practices Canada (ISMP Canada)



58 Institute for Safe Medication Practices Canada (ISMP Canada)

59 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
60 National Team Sharing through Webinars lines for each webinar Showcase the Success of our Teams Well received by attendees Relevant and Timely 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
61 The Stepping Stones to MedRec Success London Health Sciences Centre describes: The challenging elements of MedRec implementation in one of Canada's largest, acute care teaching hospitals 1. How LHSC overcame these challenges by focusing on interdisciplinary collaboration 2. How LHSC is evaluating and sustaining the process 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
62 Square Peg in a Round Hole: MedRec in Ambulatory Clinics Requires a Different Model Vancouver Health Authority and University Health Network, Toronto Describe how ambulatory clinic patients require a different system to enable medication reconciliation & review. Understand the longitudinal team approach to improve accuracy & error reduction through regular review. Describe two approaches to medication reconciliation in the ambulatory clinic setting. Identify opportunities of a patient registry as it relates to patient care (medication reconciliation), the organization (drug usage review) and outcomes research. To share the findings of medication discrepancies and drug therapy problems identified in a post discharge medication reconciliation pilot study Institute for Safe Medication Practices Canada (ISMP Canada)
63 Different Strokes: Engaging Pharmacy Technicians in MedRec The Moncton Hospital, The Ottawa Hospital, Trillium Health Centre, Peterborough Regional Health Centre Describe the medication reconciliation model developed for pharmacy technicians Review the training process involved for pharmacy technicians in medication reconciliation Highlight the role of the pharmacy technician in the Emergency Department and/or the pre-admission clinic 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
64 Got Med Wreck? Targeted Repairs from the Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) Dr. Jeffrey Schnipper Results of a funded research study into what works and what is the impact of MedRec All past and future webinars available from: SHN website: ISMP Canada website: (Education & Training) 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

65 Slide Courtesy of Dr.Jeff Schnipper Safer Healthcare Now! Webinar Jan, Institute for Safe Medication Practices Canada (ISMP Canada)

66 MedRec Webinars Available online All past and future webinars available from: SHN website: ISMP Canada website: (under Education & Training) 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

67 2010- National MedRec Summit To accelerate a system-wide strategy to implement medication reconciliation (MedRec) Healthcare CEOs, senior leaders, representatives from national organizations, provincial quality councils, physicians, nurses and pharmacists identified themes that would accelerate and optimize MedRec across the continuum of care 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

68 Senior leadership commitment is critical to ensuring MedRec is implemented successfully across an organization. Accountability must rest with the CEO with clear reporting expectations at the board level. REF: Optimizing Medication Safety at Care Transitions: A National Challenge, Institute for Safe Medication Practices Canada (ISMP Canada)

69 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

 2014")

70 Consumer Awareness and Tools PR Campaign from North Bay Regional Health Centre (ON) 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

71 Interactive Map Relatively few self-identified MedRec All-Stars who have MedRec in place across admission, transfer and discharge 2014 Institute for Safe Medication Practices Canada (ISMP Canada)

72 Paper to Electronic Tools/Checklists Organizational Readiness Steps to support the safe transition to emedrec Ideal features of emedrec, Evaluation of emedrec 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
73 October 2013 was National MedRec Quality Audit Month 103 Organizations 2340 patients 29% (acute care) 55% (Long Term Care) 1906 Acute Care 329 Long Term Care Met all 5 quality criteria Met all 5 quality criteria 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
74 National Quality Audit Results Summary Comments MUST critically evaluate admission to ensure quality at discharge Canadian audit tool results demonstrate need for ongoing and specific improvements People believe they are doing MedRec but they may not be doing it well The foundation of the process the BPMH needs work 2014 Institute for Safe Medication Practices Canada (ISMP Canada)



75 In 2014 we have NOT reliably implemented MedRec!!! 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
76 Outstanding Issues in MedRec! Getting to where we want to be Leadership Measuring and Monitoring Quality Role and use of technology Embedding roles and processes into system Consumer Engagement Primary care 2014 Institute for Safe Medication Practices Canada (ISMP Canada)
77 Light. at the end of a lot of hard work The tipping point is that magic moment when an idea, trend, or social behavior crosses a threshold, tips, and spreads like wildfire Institute for Safe Medication Practices Canada (ISMP Canada)
78 Changes in Institute for Safe Medication Practices Canada (ISMP Canada)

79 2014 Institute for Safe Medication Practices Canada (ISMP Canada)


80 Questions 80


81 Questions 1. Raise your hand and we may be able to open your phone line 2. Send feedback via the chat box Select All participants Type message Click Send All Participants

82 Please complete our poll 82
83 Upcoming MedRec Webinars Thank you for attending Join us on May 6, 2014 at 12 noon ET for our next MedRec webinar Safety, Sleuthing and Students: A Novel Collaborative MedRec Event at the University of British Columbia 83

84 We encourage you to report medication incidents Practitioner Reporting Consumer Reporting
(2006) free")



")



85 Medication Safety Self-Assessment Hospitals (acute care)(2006) free for Ontario* Long-term care (2012) free for Ontario* Complex Continuing Care and Rehabilitation (2008) free for Ontario* Community and Ambulatory Pharmacy (2007) free for Ontario* Operating Room Medication Safety Checklist (2009) free for Ontario* Oncology (2012) Anticoagulant Safety (VTE) free for Ontario* HYDROmorphone Safety Self-Assessment (2014) - $50 * Supported by the Ontario MOHLTC For more information visit or mssa@ismp-canada.org
86 Thank you for attending
YOUR DISCHARGE IS SOMEONE S ADMISSION
 YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
Making a case for medication reconciliation in primary care
 Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story
 SHN MedRec National Teleconference MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story Medication Management Support Services (MMSS) Speakers: Mary
SHN MedRec National Teleconference MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story Medication Management Support Services (MMSS) Speakers: Mary
Mental Health Pharmacist Education. Medication Reconciliation Patient Safety Initiative
 Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Partnering with Patients in Medication Safety
 Partnering with Patients in Medication Safety February 6 th, 2018 PPC 2018 Alice Watt, RPh. B.Sc (Pharm) ISMP Canada ISMP Canada 1 Presenter Disclosure Presenter s Name: Alice Watt I have no current or
Partnering with Patients in Medication Safety February 6 th, 2018 PPC 2018 Alice Watt, RPh. B.Sc (Pharm) ISMP Canada ISMP Canada 1 Presenter Disclosure Presenter s Name: Alice Watt I have no current or
Getting Started with Medication Reconciliation in Long Term Care. SHN! MedRec Teleconference September 14, EST
 Getting Started with Medication Reconciliation in Long Term Care SHN! MedRec Teleconference September 14, 2010 1200-1300 EST 1 Welcome! By the end of this teleconference, participants will: Understand
Getting Started with Medication Reconciliation in Long Term Care SHN! MedRec Teleconference September 14, 2010 1200-1300 EST 1 Welcome! By the end of this teleconference, participants will: Understand
Who s s on What? Latest Experience with the Framework Challenges and Successes. November 29, Margaret Colquhoun Project Leader ISMP Canada
 Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Involving Patients and Families to Improve Care Transitions
 Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Medication Reconciliation
 Medication Reconciliation ISMP Canada Annual Report to CPSI Safer Healthcare Now! Medication Reconciliation Intervention April 2010 to March 2011 Safer Healthcare Now! Medication Reconciliation Intervention
Medication Reconciliation ISMP Canada Annual Report to CPSI Safer Healthcare Now! Medication Reconciliation Intervention April 2010 to March 2011 Safer Healthcare Now! Medication Reconciliation Intervention
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP
: Progress Report for 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP Positive Patient Experience Overall, how would you rate the care and services you received at the hospital? (inpatient), add the number
Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP Positive Patient Experience Overall, how would you rate the care and services you received at the hospital? (inpatient), add the number
A MEDICATION SAFETY ACTION PLAN. Produced September 2014
 We are not, as a country, doing enough to ensure the safe use of medications. Medicine, in all its forms, is the most common treatment in health care and it works miracles every day when it s used appropriately.
We are not, as a country, doing enough to ensure the safe use of medications. Medicine, in all its forms, is the most common treatment in health care and it works miracles every day when it s used appropriately.
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population
 Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Sub-region Geography Data Analysis
 Guelph-Puslinch Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 Guelph 128,573 Puslinch 7399 # Seniors (65+) 18,669 Guelph 17,205 Puslinch 1,464 % Seniors (65+) 13.7%
Guelph-Puslinch Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 Guelph 128,573 Puslinch 7399 # Seniors (65+) 18,669 Guelph 17,205 Puslinch 1,464 % Seniors (65+) 13.7%
Sub-region Geography Data Analysis
 Region Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 128,573 Puslinch 7399 # Seniors (65+) 18,669 17,205 Puslinch 1,464 % Seniors (65+) 13.7% 13.4% Puslinch 19.8% %
Region Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 135,972 128,573 Puslinch 7399 # Seniors (65+) 18,669 17,205 Puslinch 1,464 % Seniors (65+) 13.7% 13.4% Puslinch 19.8% %
Medication Reconciliation Bundle of Care. Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013
 Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
From Clinician. to Cabinet: The Use of Health Information Across the Continuum
 From Clinician to Cabinet: The Use of Health Information Across the Continuum Better care. Improved quality and safety. More effective allocation of resources. Organizations in Canada that deliver mental
From Clinician to Cabinet: The Use of Health Information Across the Continuum Better care. Improved quality and safety. More effective allocation of resources. Organizations in Canada that deliver mental
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for the 2015/16 QIP
: Progress Report for the 2015/16 QIP") Excellent Care for All Quality Improvement Plans (QIP): Progress Report for the 2015/16 QIP ID Measure/Indicator from 2015/16 1 Overall, how would you rate the care and services you received at the hospital?
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for the 2015/16 QIP ID Measure/Indicator from 2015/16 1 Overall, how would you rate the care and services you received at the hospital?
ClinicalConnect Base Funding Allocation
 Meeting Date: March 01, 2012 Action: Topic Decision ClinicalConnect Base Funding Allocation Purpose: To provide the Waterloo Wellington Local Health Integration Network s Board of Directors with the information
Meeting Date: March 01, 2012 Action: Topic Decision ClinicalConnect Base Funding Allocation Purpose: To provide the Waterloo Wellington Local Health Integration Network s Board of Directors with the information
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool
 Tool") How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY. April 2009 September 2012
 MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist
 Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 2015-2016 3/31/2015 This document is intended to provide health care organizations in Ontario with guidance as to how they
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 2015-2016 3/31/2015 This document is intended to provide health care organizations in Ontario with guidance as to how they
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
CKHA Quality Improvement Plan (QIP) Scorecard
 Scorecard") CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
ISMP Canada Progress Report. to the. Ontario Ministry of Health and Long-Term Care. and the. Ontario Pharmacy Council. June 2009
 ISMP Canada Progress Report to the Ontario Ministry of Health and Long-Term Care and the Ontario Pharmacy Council June 2009 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire
ISMP Canada Progress Report to the Ontario Ministry of Health and Long-Term Care and the Ontario Pharmacy Council June 2009 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire
Health Sciences North Horizon Santé-Nord (QIP) Quality Improvement Plan
 Quality Improvement Plan") Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Sub-region Geography Data Analysis
 Kitchener-Waterloo-Wilmot-Wellesley-Woolwich (KW4) Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 391,521 Kitchener 231,482 Waterloo 104,165 Wilmot 20,240 Wellesley 11,216 Woolwich
Kitchener-Waterloo-Wilmot-Wellesley-Woolwich (KW4) Sub-region Geography Data Analysis 1 DEMOGRAPHICS Total Population (2013) 391,521 Kitchener 231,482 Waterloo 104,165 Wilmot 20,240 Wellesley 11,216 Woolwich
Why is Critical Incident Reporting and Shared Learning Important for Patient Safety?
 Why is Critical Incident Reporting and Shared Learning Important for Patient Safety? Reporting on Critical Incidents Related to Medication / IV Fluid Ontario Hospital Association Video and Webcast Toronto,
Why is Critical Incident Reporting and Shared Learning Important for Patient Safety? Reporting on Critical Incidents Related to Medication / IV Fluid Ontario Hospital Association Video and Webcast Toronto,
Insights into Quality Improvement. Key Observations Quality Improvement Plans Hospitals
 Insights into Quality Improvement Key Observations 2014-15 Quality Improvement Plans Hospitals Introduction Ontario has now had close to four years of experience with Quality Improvement Plans (QIPs),
Insights into Quality Improvement Key Observations 2014-15 Quality Improvement Plans Hospitals Introduction Ontario has now had close to four years of experience with Quality Improvement Plans (QIPs),
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Waterloo Wellington Community Care Access Centre. Community Needs Assessment
 Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Welcome to the New England QIN-QIO Medication Safety Webinar!
 Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
Welcome to the New England QIN-QIO Medication Safety Webinar! Thank you for joining. Our presentation will begin shortly. If you haven t already, please dial in to the audio line: 888-895-6448 Passcode:
THE JCPP PHARMACISTS PATIENT CARE PROCESS: TIME TO REINVENT THE WHEEL?
 Alexa Carlson, RPh, PharmD, BCPS a.carlson@northeastern.edu Margarita DiVall, RPh, PharmD, MEd, BCPS m.divall@northeastern.edu THE JCPP PHARMACISTS PATIENT CARE PROCESS: TIME TO REINVENT THE WHEEL? Objectives
Alexa Carlson, RPh, PharmD, BCPS a.carlson@northeastern.edu Margarita DiVall, RPh, PharmD, MEd, BCPS m.divall@northeastern.edu THE JCPP PHARMACISTS PATIENT CARE PROCESS: TIME TO REINVENT THE WHEEL? Objectives
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Storyboard Submission NHS Wales Awards Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated INRs
 Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
Storyboard Submission 1. Title Improving Patient Safety How ABHB Ward Pharmacists Monitor Elevated 2. Brief Outline of Context As part of the 1000 Lives Plus initiative, ward pharmacists throughout ABHB
IHA Regional Pharmacy Best Possible Medication History Practice Standard
 IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Toronto Central LHIN 2016/2017 QIP Snapshot Report. Health Quality Ontario The provincial advisor on the quality of health care in Ontario
 Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Waterloo Wellington Local Health Integration Network. Board of Directors MINUTES. Thursday, May 22, 2008
 Waterloo Wellington Local Health Integration Network Board of Directors MINUTES Thursday, The following are the minutes of the Regular Meeting held at 7:00 p.m. on Thursday, May 22, 2008 at Marden Community
Waterloo Wellington Local Health Integration Network Board of Directors MINUTES Thursday, The following are the minutes of the Regular Meeting held at 7:00 p.m. on Thursday, May 22, 2008 at Marden Community
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM
 Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report. October 2011 to December 2012
 Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report October 2011 to December 2012 Submitted to the Ontario Ministry of Health and Long-Term Care and Health Quality Ontario
Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report October 2011 to December 2012 Submitted to the Ontario Ministry of Health and Long-Term Care and Health Quality Ontario
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
ENGAGING PATIENTS IN TRANSITIONS OF CARE:
 1 ENGAGING PATIENTS IN TRANSITIONS OF CARE: Laura Kreofsky, MHA, MBA Susan Woods, MD, MPH Nan Robertson, RPh 2 Presenters Laura Kreofsky, MHA, MBA Principal and leader of Impact Advisors Discovery and
1 ENGAGING PATIENTS IN TRANSITIONS OF CARE: Laura Kreofsky, MHA, MBA Susan Woods, MD, MPH Nan Robertson, RPh 2 Presenters Laura Kreofsky, MHA, MBA Principal and leader of Impact Advisors Discovery and
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care
 Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Venous Thromboembolism (VTE) Audit Day
 Audit Day") Venous Thromboembolism (VTE) Audit Day Questions If you have any questions or require clarification, please contact Artemis Diamantouros. Email: artemis.diamantouros@sunnybrook.ca Welcome to the Canadian
Venous Thromboembolism (VTE) Audit Day Questions If you have any questions or require clarification, please contact Artemis Diamantouros. Email: artemis.diamantouros@sunnybrook.ca Welcome to the Canadian
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure.
 Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Understanding and Identifying Target Populations for Integrated Care
 Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
Understanding and Identifying Target Populations for Integrated Care W.Wodchis, X.Camacho, I. Dhalla, A. Guttman, B.Lin, G.Anderson Leveraging the Culture of Performance Excellence in Ontario s Health
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Unintentional Medication Discrepancies Technical Assistance Webinar October 16 17, 2017
 Unintentional Medication Discrepancies Technical Assistance Webinar October 16 17, 2017 Jeffrey L. Schnipper, MD, MPH, FHM Director of Clinical Research, BWH Hospitalist Service Associate Physician, Division
Unintentional Medication Discrepancies Technical Assistance Webinar October 16 17, 2017 Jeffrey L. Schnipper, MD, MPH, FHM Director of Clinical Research, BWH Hospitalist Service Associate Physician, Division
High Alert Medications: Reducing Patient Harm
 High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
SPSP Medicines October 2016 WebEx NHS Orkney and NHS Shetland Reducing medicines harm across transitions
 SPSP Medicines October 2016 WebEx NHS Orkney and NHS Shetland Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation
SPSP Medicines October 2016 WebEx NHS Orkney and NHS Shetland Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Looking Back and Looking Forward. A sneak peek for the 2018/19 hospital quality improvement plans (QIPs)
") Looking Back and Looking Forward A sneak peek for the 2018/19 hospital quality improvement plans (QIPs) KAREN SEQUEIRA, DANYAL MARTIN, SUDHA KUTTY SEPTEMBER 26, 2017 Learning Objectives Share learnings
Looking Back and Looking Forward A sneak peek for the 2018/19 hospital quality improvement plans (QIPs) KAREN SEQUEIRA, DANYAL MARTIN, SUDHA KUTTY SEPTEMBER 26, 2017 Learning Objectives Share learnings
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Patient Safety Initiatives
 Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
St. Michael s Hospital Medication Reconciliation Learning Package
 St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013
 NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Report on the. Results of the Medication Safety Self- Assessment for Long Term Care. Ontario s Long-Term Care Homes
 Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Canadian Consensus on Clinical Pharmacy Key Performance Indicators: Quick Reference Guide
 Canadian Consensus on Clinical Pharmacy Key Performance Indicators: Quick Reference Guide MAKE IT COUNT! Advancing practice to improve patient outcomes AUTHORS Olavo Fernandes Kent Toombs Taciana Pereira
Canadian Consensus on Clinical Pharmacy Key Performance Indicators: Quick Reference Guide MAKE IT COUNT! Advancing practice to improve patient outcomes AUTHORS Olavo Fernandes Kent Toombs Taciana Pereira
Benefits Evaluation Experiences at Canada Health Infoway
 Benefits Evaluation Experiences at Canada Health Infoway May 30, 2009 Simon Hagens Director, Benefits Realization & Quality Improvement shagens@infoway-inforoute.ca Presentation to the Office of the Auditor
Benefits Evaluation Experiences at Canada Health Infoway May 30, 2009 Simon Hagens Director, Benefits Realization & Quality Improvement shagens@infoway-inforoute.ca Presentation to the Office of the Auditor
2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA CONFERENCE AT A GLANCE HOSTED BY
 2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA www.canadianinterrai.org CONFERENCE AT A GLANCE HOSTED BY 2018 CANADIAN interrai CONFERENCE MONDAY, MAY 14 8:30 am - 11:30 am Site Visits
2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA www.canadianinterrai.org CONFERENCE AT A GLANCE HOSTED BY 2018 CANADIAN interrai CONFERENCE MONDAY, MAY 14 8:30 am - 11:30 am Site Visits
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan
 BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Module 14: Medication Reconciliation
 Module 14: Medication Reconciliation Emanuel LL, Taylor L, Hain A, Combes JR, Hatlie MJ, Karsh B, Lau DT, Shalowitz J, Shaw T, Walton M, eds. The Patient Safety Education Program Canada (PSEP Canada) Curriculum.
Module 14: Medication Reconciliation Emanuel LL, Taylor L, Hain A, Combes JR, Hatlie MJ, Karsh B, Lau DT, Shalowitz J, Shaw T, Walton M, eds. The Patient Safety Education Program Canada (PSEP Canada) Curriculum.
Planning to Improve the Health of a Diverse Population
 Planning to Improve the Health of a Diverse Population The Role of Information Technology Dr. Mary-Lyn Fyfe Chief Medical Information Officer Island Health June 2015 Objectives Discuss One Approach to
Planning to Improve the Health of a Diverse Population The Role of Information Technology Dr. Mary-Lyn Fyfe Chief Medical Information Officer Island Health June 2015 Objectives Discuss One Approach to
Optimizing Patient Care Transitions
 Optimizing Patient Care Transitions Leveraging ereferral Technology in a Time of System Change In this time of unprecedented change, health care leaders are challenged to improve the quality, access and
Optimizing Patient Care Transitions Leveraging ereferral Technology in a Time of System Change In this time of unprecedented change, health care leaders are challenged to improve the quality, access and
2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA CONFERENCE AT A GLANCE HOSTED BY
 2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA www.canadianinterrai.org CONFERENCE AT A GLANCE HOSTED BY 2018 CANADIAN interrai CONFERENCE MONDAY, MAY 14 8:30 am - 11:30 am Site Visits
2018 Canadian interrai Conference May 14 17, 2018 CALGARY, ALBERTA www.canadianinterrai.org CONFERENCE AT A GLANCE HOSTED BY 2018 CANADIAN interrai CONFERENCE MONDAY, MAY 14 8:30 am - 11:30 am Site Visits
Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP. Target as stated on QIP 2016/
: Progress Report for 2016/17 QIP. Target as stated on QIP 2016/") Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP ID Measure/Indicator from 2016/17 1 % of patients who have delirium recorded in their health record (
Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP ID Measure/Indicator from 2016/17 1 % of patients who have delirium recorded in their health record (
transitions in care what we heard
 transitions in care what we heard Early in 2018, Health Quality Ontario asked Ontarians a simple question: what affected your transition from hospital to home? Good and bad. Big and small. We wanted to
transitions in care what we heard Early in 2018, Health Quality Ontario asked Ontarians a simple question: what affected your transition from hospital to home? Good and bad. Big and small. We wanted to
Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project
 1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
The South West Regional Wound Care Program (SWRWCP): A Collaborative Approach to Wound Care
: A Collaborative Approach to Wound Care") The South West Regional Wound Care Program (SWRWCP): A Collaborative Approach to Wound Care 2017 OACCAC Conference June 15, 2017 #OACON17 I @OACCAC I @SWRWCP Disclosures None Objectives By the conclusion
The South West Regional Wound Care Program (SWRWCP): A Collaborative Approach to Wound Care 2017 OACCAC Conference June 15, 2017 #OACON17 I @OACCAC I @SWRWCP Disclosures None Objectives By the conclusion
Getting Started Kit MEDICATION RECONCILIATION IN ACUTE CARE. Version 4. Reducing Harm Improving Healthcare Protecting Canadians.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN ACUTE CARE Getting Started Kit Version 4 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has been
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN ACUTE CARE Getting Started Kit Version 4 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has been
Current Performance as stated on QIP2016/17
 Excellent Care for All Quality Improvement Plans (): Progress Report for The Progress Report is a tool that will help organizations make linkages between change ideas and improvement, and gain insight
Excellent Care for All Quality Improvement Plans (): Progress Report for The Progress Report is a tool that will help organizations make linkages between change ideas and improvement, and gain insight
EXECUTIVE COMPENSATION PROGRAM
 EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases
EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases