2018 Practice Improvement Program (PIP) Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
|
|
|
- Frederica Carter
- 6 years ago
- Views:
Transcription
1 2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
 Leadership")




2 Practice Improvement Program (PIP) Leadership Team James Glauber, Chief Medical Officer Adam Sharma Director, Health Outcomes Improvement Vanessa Pratt Manager, Population Health Kanelle Barreiro Program Manager, Pay for Performance Katherine Quen Specialist, Population Health
3 Agenda TIME ITEM 8:30 Welcome Review Agenda and Meeting Objectives 8:40 Program Overview 8:50 Review Changes in 2018 PIP Clinical Quality Domain Data Quality Domain Patient Experience Domain Systems Improvement Domain 9:40 Break 9:50 Review all other measures with no changes in 2018 Small group activity 10:25 Review 2018 Enrollment 10:45 Closing & Evaluation Distribution

4 Housekeeping Webinar will be recorded Slides will be sent out after Please mute phone lines, *6 Don t put phone lines on hold Ask questions throughout and at Q&A No question is silly
5 Objectives General overview of program Review changes and new measures Answer questions that will help you be successful

6 What is PIP? Incentive program for SFHP Medi-Cal clinics and medical groups to achieve improvements in system and health outcomes.
7 PIP Guiding Principles Comprehensive Collaborative Standardized Incentivizing Technical Assistance

8 The History of PIP 2011 Program launch Reporting only to incentivize building capacity for reporting data 2014 Strength in Numbers P4P measures rolled into CQ domain, all participants held accountable for data quality measures Fewer measures, simpler deliverables, specialty care access measures New measures were added to the Systems Improvement domain to support appropriate utilization of primary care visits and expansion of the palliative care Medi-Cal benefit Stronger commitment to quality-established clinical thresholds, incentivized outreach to higher risk populations 2015 Improving access, narrowing the number of measures to focus improvement on lowest performing Newer measures were added to the Clinical Quality domain to increase alignment with external entities.

")


9 Standardized PIP Participant Types Academic Medical Center (1) Individually Contracted Specialty (1) Community Clinic (7) IPA (3) Clinic-Based RBO (1)
10 PIP Incentives incentivizing Maximum quarterly payments are allocated based on capitation and actual member months accrued during each month of the quarter. 18.5% of Medi-Cal capitation 5% of Healthy Kids HMO capitation
11 Quadruple Aim comprehensive Patient Experience Domain Patient Experience Domain Improving Patient Experience Improving Staff Satisfaction All Domains Reducing the Per Capita Cost of Health Care Improving Population Health Clinical Quality Domain Data Quality Domain
12 collaborative PIP Measure Development PIP Participants, SFHP stakeholders, NCQA, HEDIS, QMED, Meaningful Use, DMHC, DHCS SFHP Subject Matter Experts Advisory Committee
13 PIP Reporting Timeline Quarter Quarter End Date Materials Due to SFHP Reporting Period Enrollment Friday, January 19, 2018* For all measures, the quarter s end date serves as 1 March 31, 2018 Monday, April 30, 2018 the last day of the reporting 2 June 30, 2018 Tuesday, July 31, 2018 period. Please see each 3 September 30, 2018 Wednesday, October 31, 2018 measure s specifications for the first day of the 4 December 30, 2018 Thursday, January 31, 2019 reporting period. *Late baseline data submissions jeopardize the PIP database setup. We thank you in advance for your timeliness with your baseline data!
14 Clinical Quality Scoring collaborative Deliverable For each of the Priority Five measures: Achieving 90 th percentile HEDIS or 75 th internal PIP percentiles or 15% or more relative improvement Achieving 75 th percentile HEDIS or 60 th internal PIP percentiles or 10-14% relative improvement Achieving 5-9% relative improvement over baseline Self-reporting data quarterly Maintaining performance relative to baseline* For each of the non-priority Five measures: Quarterly Scoring (Self-Reported Data) 1.25 points 1.0 point 0.75 point 0.25 point 0.25 point
15 PIP Payment Methodology % of points = 100% of payment 80 89% of points = 90% of payment 70 79% of points = 80% of payment 60 69% of points = 70% of payment 50 59% of points = 60% of payment 40 49% of points= 50% of payment 30 39% of points= 40% of payment 20 29% of points = 30% of payment Less than 20% of points = no payment

16 Scorecard Review
17 PIP Website Technical Assistance All 2018 measure resources will be listed here
18 Program Guide 2018 Changes

19 All-Participant Program Guide At the top of each page, each measure specification lists which participants have measure assigned in their measure set.
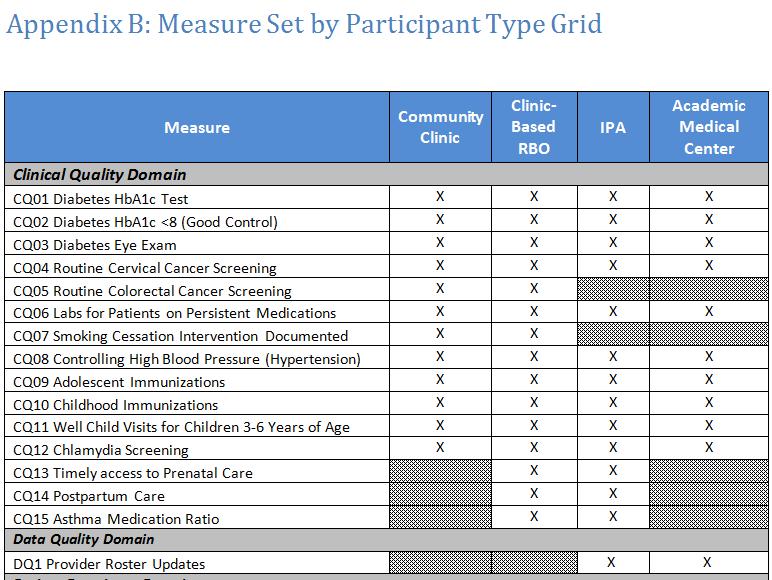
20 All-Participant Program Guide
21 Clinical Quality Domain: 2018 Changes
22 SFHP option discontinued Overall, this decision will benefit our provider network in various ways: o Fewer charts will be requested from providers during the SFHP HEDIS pursuit o Fewer SFHP dollars will be spent on the administration of the HEDIS pursuit o Further development of PIP self-reporting capacities
23 CQ 06: Labs for Patients on Persistent Medications HEDIS Changes from 2017 Digoxin has been removed from the reporting requirements for EAS and NCQA. As such, PIP participants have the option of removing digoxin from their 2018 PIP reporting. Measure CQ 06: Labs for Patients on Persistent Medications Numerator/Denominator Numerator: Number of patients in denominator population who received, in the last year: At least one serum potassium, AND A serum creatinine within the measurement year OPTIONAL: AND (for members on digoxin) A serum digoxin (applies only to members on digoxin) Denominator: Number of active patients 18 years and older, on ACE inhibitor, ARBs, digoxin or diuretics for 180 days or more in the last year
24 CQ09: Adolescent Immunizations Changes from 2017 In alignment with clinical guidelines that recommend the inclusion of HPV in the vaccination schedule for adolescents, CQ9 Adolescent Immunizations was replaced by CQ12 Adolescent Immunizations (with HPV). Measure CQ09: Adolescent Immunizations Numerator/Denominator Numerator: Number of patients in the denominator population who received one meningococcal vaccine on or between the member s 11th and 13th birthday and one (Tdap) or (Td) vaccine on or between the member s 10th and 13th birthdays, and two HPV vaccines between the member s 9 th and 13 th birthday. Denominator: Number of active patients who turned 13 years old during the last year
25 CQ09: Adolescent Immunizations Measures without comparable NCQA HEDIS thresholds, a PIP network threshold will be used based on prior year s PIP participant data: Measure CQ09 Adolescent Immunizations 75 th percentile 60 th percentile 73.00% 50.40%
26 CQ12: Chlamydia Screening HEDIS Changes from 2017 This measure will be scored as a non-priority Five measure, earning points maintaining baseline. Measure Numerator/Denominator Numerator: Number of patients in the denominator population with at least one test for chlamydia in the last year CQ14: Chlamydia Screening Denominator: Number of active patients who meet all of the following criteria: are sexually active have the ability to become pregnant between the ages of years old
27 CQ13-CQ14: Perinatal Care Changes from 2017 This measure will be scored as a non-priority Five measure, earning points maintaining baseline. HEDIS Measure Numerator CQ15: Timely Access to Prenatal Care CQ16: Postpartum Care Numerator: Number of patients in the denominator population who received a prenatal in the first trimester of their pregnancy or within 42 days of enrollment into Medi-Cal, whichever is later. Numerator: Number of patients in the denominator population who had a postpartum visit between days after delivery. Denominator: Number of active patients who had a live birth in the last year.
28 CQ15: Asthma Medication Ratio Changes from 2017 This measure will be scored as a non-priority Five measure, earning points maintaining baseline. HEDIS Measure Numerator/Denominator Numerator: Number of patients in the denominator population who have a ratio of 0.5 or greater of controller asthma medications to total asthma medications in the measurement year. CQ17: Asthma Medication Ratio Denominator: Number of active patients between the ages 5-64 with persistent asthma as defined as one or more of the following in the past two years: At least one ED visit with a primary diagnosis of asthma At least one inpatient encounter with a primary diagnosis of asthma At least four outpatient visits with a diagnosis of asthma and at least two asthma medication dispensing events At least four asthma medication dispensing events If the patient was only dispensed short acting medications (leukotriene modifier or antibody inhibitor) they should also have a diagnosis of asthma in any setting

29 Data Quality Domain 2018 Changes
30 DQ1: Provider Roster Updates Changes from 2017 Measure applies only to IPA & Academic Medical Center participants Reporting frequency changed from quarterly to biannually. Deliverable Due Dates Scoring If there are no changes that need to be made to the current quarter s provider roster, please submit the Provider Roster Attestation. If changes do need to be made to the current quarter s provider roster, please submit the supporting information in one of the two approved ways. Deductions will be made in these cases: o 0.10 point deduction (up to a maximum of 0.50 point) for each piece of missing information noted in Measure Description. o 0.25 point deduction (up to a maximum of 1.0 point): Discrepancy between Medical Staff Office (MSO)/Profiles/Change Reports/Credentialing Packet and Provider Roster. Discrepancies that will affect scoring are: Providers in one source and not the other. Additions/terminations reported via PIP that should have been reported via entity s contractual method > 1 month prior Quarter 2 Quarter points
31 Patient Experience Domain 2018 Changes
32 PE8: Expanding Access to Services Changes from 2017 There are two new options for 2018: Option Three: Patient-centered scheduling practices Option Four: Improvements in transgender health are new in 2018 The option to offer primary care services by staff other than PCPs was retired to create opportunity for new improvement projects. Option Five was modified to include a range of access improvement projects. Option One: Best Practices in Hepatitis C Screening & Treatment Option Two: Improvements in Opioid Safety Option Three: Patient-Centered scheduling Practices Option Four: Improvements in Transgender Health Option Five: Access Improvement Project
33 PE8: Expanding Access to Services Deliverables Due Dates Scoring Deliverable A: Submit service expansion plan using required template Quarter points for completed template Deliverable B: Submit example materials from service expansion Quarter points for example materials Deliverable C: Attestation service expansion has occurred, signed by Medical Director or equivalent Quarter points for signed attestation
34 Systems Improvement Domain 2018 Changes
35 SI1: Depression Screening and Follow-up Changes from 2017 The Depression Screening Rate will become pay-for-performance in Q Follow-up to a positive screen was added as a qualitative component of this measure. PART A: Rate of patients receiving depression screening Depression Screening Rate = Numerator: Total number of patients in the denominator with a depression screening in the measurement year. Denominator: Total number of active patients at least 12 years of age during the measurement year. Numerator Measurement Option #2: Measure depression screening using other registry methods. Participants choosing this option must report their methodology for measuring depression screening.
36 SI1: Depression Screening and Follow-up PART B: Create a system/clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen. Appropriate Follow-up on or within 30 days of positive screen 1. Additional evaluation for depression Follow-up with a case manager, with documented assessment of depression symptoms. Telephone visit with diagnosis of depression or other behavioral health condition. Assessment on the same-day as the positive screen, including additional depression assessment indicating no depression or no symptoms that require follow-up. 2. Referral to a practitioner who is qualified to diagnose and treat depression Follow-up behavioral health encounter, including assessment, therapy, collaborative care, medication management, acute care, and telehealth encounters. Follow-up outpatient visit, with a diagnosis of depression or other behavioral health condition. 3. Pharmacological Intervention Dispensed anti-depressant medication
37 SI1: Depression Screening and Follow-up Deliverable Due Dates PIP Network Threshold Quarterly Scoring Deliverable A: Self-report the numerator and denominator as noted in the Measure Description. Quarter 1 & Quarter 2 (reporting only) N/A 1.0 point Deliverable B: Documentation of system/clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen, submitted via Wufoo. Quarter 3 & Quarter 4 (pay-for-performance) Percentile TBD 1.0 point Percentile 0.5 point TBD Quarter 3 N/A 4.0 points IPA participants only: Provide an attestation signed by Medical Director, or equivalent, verifying at least three sites have developed a clinic-wide protocol with pathways for each of the four appropriate follow-ups to a positive screen described in the table below.
38 SI2: Follow-Up After Hospital Discharge Changes from 2017 Numerator definition was updated to support clinical best practice that a follow-up visit post discharge should not occur on the same-day as discharge. Quarterly Office Visit Follow-Up After Hospital Discharge Rate = Numerator: Total number of discharges in the denominator with an eligible follow-up visit 1-7 calendar days post discharge Denominator: Total number of inpatient discharges during the quarter Deliverable Due Date Threshold Scoring Submit quarterly numerator and denominator as noted above via quantitative data template. Quarter 1 Quarter 2 Quarter 3 Quarter 4 50% 1.0 point 40% 0.5 point
39 SI5: Percent of Members with a Primary Care Visit Quarterly Primary Care Visit Rate = Numerator: Number of SFHP members in the denominator population with at least one PCP visit in the last year Denominator: Total number of continuously enrolled SFHP Medi- Cal members assigned to your organization during the quarter. Deliverable Due Date Scoring SFHP to provide in Quarter 1, Quarter 2, Quarter 3, and Quarter 4 Deliverable A: Receive PCP visit rate. To be scored Q points for achieving 5% or more absolute improvement over baseline* or achieving SFHP average PCP visit rate. 1.5 points for achieving 3% absolute improvement over baseline.* 1.0 points for achieving 1% absolute improvement over baseline.* Deliverable B: Submit improvement plan template (for participants not meeting SFHP average PC visit rate in Q1 2018) Quarter points *Baseline will be determined by Q PCP visit rate
40 SI6: Palliative Care Part A (IPA, Clinic-Based RBO, and Academic Medical Center participants only): Complete an assessment of the palliative care resources available within your network. Part B (All Participants): Identify patients who may be eligible for referral to palliative care services by completing the following: Identify patients with COPD or CHF who are potentially eligible for palliative care by using an SFHP list of members who are potentially eligible for palliative care, or creating your own list of potentially eligible patients. For potentially eligible members with COPD or CHF, perform chart review to determine eligibility for referral to palliative care services. Attestation signed by medical director (or equivalent) verifying chart review of members eligible for palliative care and appropriate referrals were made.
41 SI6: Palliative Care Deliverable Due Date Scoring Deliverable A (for IPA, Clinic-Based RBO, and Academic Medical Center participants only): Submit template outlining the palliative care services and/or resources available within your network. Quarter points Deliverable B (All Participants) : Submit attestation signed by a medical director (or equivalent), verifying that chart review was performed for members with COPD potentially eligible for palliative care and appropriate referrals were made. Quarter points
42 Questions?
43 BREAK!

44 Review All Remaining Measures
45 Clinical Quality Domain
46 Clinical Quality Scoring collaborative Deliverable Quarterly Scoring (Self-Report) For each of the Priority Five measures: Achieving 90 th percentile HEDIS or 75 th internal PIP percentiles or 15% or more relative improvement Achieving 75 th percentile HEDIS or 60 th internal PIP percentiles or 10-14% relative improvement Achieving 5-9% relative improvement over baseline Self-reporting data quarterly Maintaining performance relative to baseline* For each of the non-priority Five measures: 1.25 points 1.0 point 0.75 point 0.25 point 0.25 point

47 CQ01-CQ03: Diabetes (All Participants) HEDIS Measure CQ 01: Diabetes HbA1c Test CQ 02: Diabetes HbA1c <8 (Good Control) CQ 03: Diabetes Eye Exam Numerator Numerator: Number of patients in denominator population who received at least one HbA1c test within the last 12 months Numerator: Number of patients in denominator whose most recent HbA1c level is < 8.0 in the last 12 months Numerator: Number of patients in denominator population with retinal exam or dilated eye exam performed by an eye care professional in the past 12 months OR a negative retinal or dilated eye exam performed by an eye care professional in last 24 months Denominator: Number of active patients with diabetes ages years old
48 CQ04: Cervical Cancer Screening (All Participants) HEDIS Measure CQ04: Routine Cervical Cancer Screening Numerator/Denominator Numerator: Number of patients with cervices ages who received one or more Pap tests during the past 3 years OR patients with cervices ages who received cervical cytology and HPV co-testing during the past 5 years Denominator: Number of active patients with cervices ages years old
49 CQ05: Colorectal Cancer Screening (Community Clinics & Clinic Based RBO s only) Measure Numerator/Denominator Numerator: Number of patients in denominator population who received a FOBT or FIT test during the past year, OR CQ05: Routine Colorectal Cancer Screening Number of patients in denominator population who received a sigmoidoscopy during the past 5 years, OR Number of patients in denominator population who received a screening colonoscopy during the past 10 years Denominator: Number of active patients ages years old
50 CQ 07: Smoking Cessation Intervention (Community Clinics & Clinic Based RBO s only) Measure Numerator/Denominator Numerator: Number of patients in denominator population with a documented smoking cessation counseling intervention in the EHR or registry in the last 2 years CQ 07: Smoking Cessation Intervention Denominator: Number of active patients who are (must meet all of the following): a) 18 years or older b) Have a documented history of tobacco use in the past 2 years c) Seen for at least one outpatient visit within the past 2 years
51 CQ08: Controlling High Blood Pressure (All Participants) HEDIS Measure Numerator/Denominator Numerator: Number of patients in the denominator population in which the most recent BP reading in an outpatient visit within the reporting period was documented as follows: years of age whose BP was <140/90 mm Hg; CQ08: Controlling High Blood Pressure years of age with a diagnosis of diabetes whose BP was <140/90 mm Hg; years of age without a diagnosis of diabetes whose BP was <150/90 mm Hg. Denominator: Number of active patients with hypertension ages years old
52 CQ10: Childhood Immunizations (All Participants) HEDIS Measure Numerator/Denominator Numerator: Number of patients in the denominator population who received all of the following vaccines by their second birthday: four diphtheria, tetanus and acellular pertussis (DTaP); three polio (IPV); one measles, mumps and rubella (MMR); CQ10: Childhood Immunizations three haemophilus influenza type B (HiB); three hepatitis B (HepB), one chicken pox (VZV); and four pneumococcal conjugate (PCV) Denominator: Number of active patients who turned 2 years old during the last year
53 CQ11: Well Child Visits for Children 3-6 Years of Age (All Participants) HEDIS Measure Numerator/Denominator CQ10: Childhood Immunizations Numerator: Number of patients in the denominator population who had at least one well-child visit with a PCP during the past year. Denominator: Number of active patients 3-6 years old
54 Patient Experience Domain
55 PE1: Third Next Available Appointment (Community Clinics & Clinic Based RBO s only) Deliverable Due Dates # of Days Reduced Threshold Scoring Submit the median established patient followup visit TNAA for each of the final 5 full weeks of the reporting period. Note: SFHP will determine median of five pieces of data and use it to score performance. Quarter 1 Quarter 2 Quarter 3 Quarter 4 n/a > 10 days 14 calendar days or less calendar days or less 2.0 points 1.5 points 5-9 days n/a 1.0 point
56 PE2: Show Rate (Community Clinics, Clinic-based RBOs, & Academic Medical Centers only) Monthly Show Rate = Numerator: Of the total appointments in the denominator, the number of appointments which patients kept. Denominator: Total number of pre-scheduled appointments for a PCP/PCP team visit during any given calendar month. Deliverable Submit monthly data each quarter via the quantitative template. Note: SFHP will determine quarterly show rate by combining numerators and denominators for each month in the quarter, and using it to determine performance. Due Dates Quarter 1 (Timeframe: Jan, Feb, Mar) Quarter 2 (Timeframe: Apr, May, Jun) Quarter 3 (Timeframe: Jul, Aug, Sept) Quarter 4 (Timeframe: Oct, Nov, Dec) Relative Improvement Threshold Quarterly Scoring n/a 85% or 1.0 point more 10% 80-84% 0.75 point 5-9% n/a 0.5 point
57 PE3: Office Visit Cycle Time (Community Clinics, Clinic-based RBOs, & Academic Medical Centers only) Deliverable Due Dates # Minutes Reduced Self-report the median cycle time for each month in the quarter. Quarter 1 (Data Collection Period: Jan, Feb, Mar) Quarter 2 (Data Collection Period: Apr, May, Jun) Quarter 3 (Data Collection Period: Jul, Aug, Sept) Quarter 4 (Data Collection Period: Oct, Nov, Dec) 10 or more minutes reduced 5-9 minutes reduced PIP Network Threshold 75 th percentile 64 minutes or less 60 th percentile minutes Quarterly Scoring 1.0 point 0.5 point
58 PE4: Staff Satisfaction Improvement Strategies (All Participants) Deliverables Due Dates Scoring Deliverable A: Submit template with the following included: Baseline score of a staff satisfaction survey o If survey has multiple questions, only one score may be chosen. rate met. For participants using Net Promoter survey, chosen question must be How likely are you to recommend organization as a place to work? Survey type (Gallup, Net Promoter, etc.) Survey date (completed October 1, 2015-January 15, 2016) Survey question Response rate (numerator/denominator) 1-2 priority areas identified for improvement Deliverable B: Submit template with a report of activities implemented specifically to address priority areas identified for improvement Deliverable C: Submit template with the following included: Survey type (must be same as baseline) Survey date (completed August 1, 2016-October 15, 2016) Survey question (must be same as baseline) Response rate (numerator/denominator) Deliverable D: Improvement on staff satisfaction survey score, submitted via the Quantitative Data Template. o Score must represent question chosen for baseline. Quarter point for completed template, if required response 0 point if required response rate not met. Quarter point for completed template Quarter point for completed template, if required response rate met. 0 point if required response rate not met. Quarter 3 If required response rate met: 1.0 point for > 4.0% relative improvement 1.0 point for 2.0% - 3.9% relative improvement If required response rate not met: 0 point
59 PE5: Improvement in Patient Experience of Primary Care Access (All Participants) Patient Experience Survey Tool Criteria Criteria 1. Conducted and analyzed by or audited by third party 1. Surveyed population is a random sample of all Medi-Cal patients 1. Survey conducted at least twenty-four hours after visit concludes Rationale Supports consistent and unbiased survey methodology Results can be generalized across the population Surveys conducted during or immediately after a visit can offer a limited view of the patient s full experience, including follow-up services needed post visit 1. Tool has been validated Validation ensures that the tool is reliable; meaning, that it yields results that reflect patient perception of the health care system 1. Includes access-related questions Access to care represents the biggest opportunity for improvement for San Francisco s Medi-Cal population, as it is the lowest ranking area on member surveys 1. Sampling methodology ensures that each question obtains at least thirty responses Results can be considered statistically meaningful
60 PE5: Improvement in Patient Experience of Primary Care Access Deliverables Due Dates Scoring Deliverable A: Submit template with: CG-CAHPS or equivalent baseline data A description of the qualitative data collection methodology (sampling methodology, questions asked, and number of patients participating) An analysis of themes found in qualitative data Plan to improve results, based on qualitative data Deliverable B: Submit template with report of activities implemented Deliverable C: Submit re-measurement score for CG- CAHPS or equivalent survey on Quantitative Data Template Deliverable D: Submit template with re-measurement data collection methodology. Quarter 2 Quarter 3 Quarter 4 Quarter points for completed template 1.0 point for completed template 2.0 points for >3% absolute improvement 1.0 point for % absolute improvement 0.0 points for <2% absolute improvement 0.5 points
61 PE6: Primary Care Access as Measured by Appointment Availability Survey Compliance (Academic Medical Centers & IPAs) Primary Care Appointment Availability = Numerator: Total number of primary care providers in compliance with DMHC Appointment Availability standards listed in the measure specification (must be compliant in both categories) Denominator: Total number of primary care providers that respond to the Appointment Availability Survey Deliverable Due Date Scoring Quarter 4. No submission due from participants. Participate in provider appointment availability survey (via phone, online, or fax) 8.0 points for achieving a 80% compliance rate
62 PE7: Improvement in Specialty Access as Measured by HP-CAHPS (Clinic-Based RBOs & IPAs) Deliverable Due Date Scoring Deliverable A: Receive re-measurement score Deliverable B: Submit template with Score for HP-CAHPS specialist access question as reported by SFHP An analysis of themes found in qualitative data Plan to improve results, based on qualitative data SFHP to provide in August 2018 Quarter 4 To be scored Q points for achieving 4% or more absolute improvement over baseline score on the specialist access question 3.0 points for achieving % absolute improvement 2.0 points for achieving % absolute improvement 2.0 points for completed template
63 Systems Improvement Domain
64 SI3: Opioid Safety (Community Clinics, Clinic-based RBOs & Academic Medical Centers) Quarterly Opioid Safety Rate = Numerator: Total number of opioid registry patients who meet the opioid safety requirements: all of the following must be documented in the last 12 months: one drug urine screen (does not have to be random) a signed opioid treatment agreement CURES report reviewed Denominator: Total number of patients in Opioid Registry on the last day of the Quarter Deliverable Due Date Quarterly Scoring Deliverable A: Self-report the numerator and Quarter point for > 60% denominator as noted in the Measure Quarter point for 50-59% Description Quarter 3 0 points for 49% or less Quarter 4 Part B: Submit template with the names of 5 SFHP members with opioid safety risk reviewed during the months of the quarter by the Controlled Substance Review Committee. Include brief documentation of committee recommendations and attestation that CURES report reviewed. CURES must be run no more than one month prior to review. Quarter 1 Quarter 2 Quarter 3 Quarter point/member, up to 0.5 point, will be awarded for submitting (via secure ) the completed template listing the 5 SFHP members reviewed by the Controlled Substance Review Committee to PainManagement@sfhp.org.
65 SI4: Providers Open to New Members (IPAs only) Quarterly Rate of Providers Open to New Members = Numerator: PCPs in the denominator open to new members and to auto-assigned members. Auto-assigned members are new members who do not choose a Primary Care Provider on enrollment with SFHP. Denominator: Total number of PCPs affiliated with SFHP as of the last week of the Quarter. Deliverable Due Date Relative Improvement No deliverables Quarter 1 required for this Quarter 2 measure. Quarter 3 Quarter 4 Threshold Quarterly Scoring > 15% > 80% 2.0 points 10-14% 70-79% 1.5 points 5-9% 60-69% 1.0 point
66 PIP Enrollment Process Two steps: 1. Wufoo form 2. Enrollment Attestation: Data Sharing Consent form 2017 Q4 data will be used for 2018 baseline
67 Wufoo Form
68 Wufoo Form Section 1: General Information & Participant Contact Information
69 Wufoo Form Section 2: PIP Alignment Survey
70 Wufoo Form Section 3: Clinical Quality Domain Reporting
71 Wufoo Form Section 4: Patient Experience & Systems Improvement Domain Measure Questions
72 Wufoo Form Section 5: Attestations & Comments/Questions
73 Questions?
74 Evaluation We appreciate your honest feedback on the evaluation!
75 Questions? Contact information: Kanelle Barreiro Program Manager, Pay for Performance (415) Katherine Quen Specialist, Population Health (415) Website:
Practice Improvement Program 2017 Program Guide Primary Care
 Practice Improvement Program 2017 Program Guide Primary Care Community Clinic Enrollment Deadline: January 20, 2017 Last updated: June 23, 2017 Contacts: Kanelle Barreiro, Program Manager, Pay for Performance
Practice Improvement Program 2017 Program Guide Primary Care Community Clinic Enrollment Deadline: January 20, 2017 Last updated: June 23, 2017 Contacts: Kanelle Barreiro, Program Manager, Pay for Performance
Practice Improvement Program 2014 Program Guide
 Practice Improvement Program 2014 Program Guide Measure Set for NEMS & CCHCA Application due: January 31, 2014 Contacts: Lauren Baehner, Project Manager, Practice Improvement Program 415 615 4284 Lbaehner@sfhp.org
Practice Improvement Program 2014 Program Guide Measure Set for NEMS & CCHCA Application due: January 31, 2014 Contacts: Lauren Baehner, Project Manager, Practice Improvement Program 415 615 4284 Lbaehner@sfhp.org
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
HEDIS TOOLKIT FOR PROVIDER OFFICES. A Guide to Understanding Medicaid Measure Compliance
 HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives. Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018
 Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Federally Qualified Health Centers Rural Health Clinics. February Interim. Pay for. Quality
 Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
Quality Improvement Program (QIP) Measurement Specifications
 Measurement Specifications") Quality Improvement Program (QIP) 2014 2015 Measurement Specifications Developed by: Marya Choudhry Contributors include: Robert Moore Jess Liu Jennifer Dionisio Carolyn Stewart Melanie Lam Jessica Thatcher
Quality Improvement Program (QIP) 2014 2015 Measurement Specifications Developed by: Marya Choudhry Contributors include: Robert Moore Jess Liu Jennifer Dionisio Carolyn Stewart Melanie Lam Jessica Thatcher
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary
 2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
HEDIS Updates to quality ratings, measures & reporting. Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation
 HEDIS 2018 Updates to quality ratings, measures & reporting Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation Agenda HEDIS Overview HEDIS 2018 Changes to Existing Measures HEDIS 2018
HEDIS 2018 Updates to quality ratings, measures & reporting Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation Agenda HEDIS Overview HEDIS 2018 Changes to Existing Measures HEDIS 2018
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
HEDIS Measures and the Family Physician Office. Pablo J Calzada DO, MPH, FAAFP, FACOFP
 HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
HEDIS 101 for Providers 2018
 HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
Quality Measures for HMO s: Understanding HEDIS
 Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
10/6/2017. FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction. Agenda. Incentives in PPS: what does excludable mean?
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting. November 3, 2016
 Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting November 3, 2016 Agenda Welcome & Introductions Core Measure Set MY 2017 EAS Measure Set Update Benchmarks Core Measure Set Adoption
Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting November 3, 2016 Agenda Welcome & Introductions Core Measure Set MY 2017 EAS Measure Set Update Benchmarks Core Measure Set Adoption
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be faxed back.
 Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Value Based P4P Program Updates MY 2017 & MY 2018
 Value Based P4P Program Updates MY 2017 & MY 2018 January 31, 2018 Lindsay Erickson, Director Ginamarie Gianandrea, Senior Program Coordinator Thien Nguyen, Project Manager Brandi Melville, Health Care
Value Based P4P Program Updates MY 2017 & MY 2018 January 31, 2018 Lindsay Erickson, Director Ginamarie Gianandrea, Senior Program Coordinator Thien Nguyen, Project Manager Brandi Melville, Health Care
QUALITY IMPROVEMENT. Articles of Importance to Read: Quality Improvement Program. Winter Pages 1, 2, 3, 4 and 5 Quality Improvement
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
For more information on any of the topics covered, please visit our provider self-service website at
 Quality improvement summary The results are in We d like to share with you our annual quality improvement summary of clinical performance and service satisfaction. Throughout the year, we evaluate data
Quality improvement summary The results are in We d like to share with you our annual quality improvement summary of clinical performance and service satisfaction. Throughout the year, we evaluate data
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Florida Medicaid: Performance Measures (HEDIS)
") Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Payment Transformation 2018 Measure Changes and Updates. April 4, 2018
 Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications
 Issue Brief No. 13 January 2015 Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications Ann Hardesty, Project Manager Jill Yegian, Senior Vice President,
Issue Brief No. 13 January 2015 Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications Ann Hardesty, Project Manager Jill Yegian, Senior Vice President,
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Molina Healthcare of Ohio Marketplace Plans
 Section 4. Benefits and Covered Services Molina Healthcare covers the services described in the Summary of Benefits and Evidence of Coverage (EOC) documentation for each Molina Marketplace plan type. If
Section 4. Benefits and Covered Services Molina Healthcare covers the services described in the Summary of Benefits and Evidence of Coverage (EOC) documentation for each Molina Marketplace plan type. If
Chapter 7. Unit 2: Quality Performance Measures
 Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
Medical Record Review Tool Standards with Definitions
 WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Driving Quality Improvement in Managed Care. Toby Douglas, Director California Department of Health Care Services
 1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
1 Driving Quality Improvement in Managed Care Toby Douglas, Director 2 Presentation Overview 1. Background on California s Medicaid Program (Medi-Cal) 2. California s Quality Improvement Focuses 3. Challenges
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Quality Improvement Program Evaluation
 Denver Health Medical Plan, Inc. Quality Improvement Program Evaluation 2013 Commercial and Exchange Products 1 Page Table of Contents I. Executive Summary...3 II. Quality Improvement Program Evaluation
Denver Health Medical Plan, Inc. Quality Improvement Program Evaluation 2013 Commercial and Exchange Products 1 Page Table of Contents I. Executive Summary...3 II. Quality Improvement Program Evaluation
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Provider Training Quality Enhancement 2016
 Provider Training Quality Enhancement 2016 1 What s Ahead? Why Are We Here? 3 NCQA Accreditation & HEDIS 4-6 Medicare Start Rating & HEDIS 7 Provider s Role and Expectation 8-11 Staying Healthy During
Provider Training Quality Enhancement 2016 1 What s Ahead? Why Are We Here? 3 NCQA Accreditation & HEDIS 4-6 Medicare Start Rating & HEDIS 7 Provider s Role and Expectation 8-11 Staying Healthy During
June Thank you for attending today s Webinar. We will begin shortly. June Brian Clark. Diana Charlton. Debbie Barkley Aetna Inc.
 June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
Anthem Blue Cross and Blue Shield
 Anthem Blue Cross and Blue Shield 2016 Quality-In-Sights Primary Care Quality Incentive Program Part of the Anthem Quality Insights suite of innovative, quality recognition and health improvement programs
Anthem Blue Cross and Blue Shield 2016 Quality-In-Sights Primary Care Quality Incentive Program Part of the Anthem Quality Insights suite of innovative, quality recognition and health improvement programs
2016 Quality Management Annual Evaluation Executive Summary
 2016 Quality Management Annual Evaluation Executive Summary July 2017 Mission and Vision The purpose of the 2016 Annual Evaluation is to assess IEHP s Quality Program. This assessment reviews the quality
2016 Quality Management Annual Evaluation Executive Summary July 2017 Mission and Vision The purpose of the 2016 Annual Evaluation is to assess IEHP s Quality Program. This assessment reviews the quality
Instructions for Accessing the Secure Portal and the Verification Process
 Instructions for Accessing the Secure Portal and the Verification Process Community Checkup report: www.wacommunitycheckup.org More about the Alliance: www.wahealthalliance.org 1 Contents Overview... 3
Instructions for Accessing the Secure Portal and the Verification Process Community Checkup report: www.wacommunitycheckup.org More about the Alliance: www.wahealthalliance.org 1 Contents Overview... 3
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Technical Specifications Community Checkup Measures About the technical specifications Measures sourced from the Washington Health Alliance Database
 Technical Specifications Community Checkup Measures September 2017 About the technical specifications The 2017 Community Checkup relies on three categories of data to produce results: The Alliance (the
Technical Specifications Community Checkup Measures September 2017 About the technical specifications The 2017 Community Checkup relies on three categories of data to produce results: The Alliance (the
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Created for Sample ABC, Inc
 Created for Report Date: NOV-05-2013 Demographics Subscribers 4,895 - Members 12,746 - Membership 13,461 - Age (subscribers) 41.0 41.0 Age (members) 28.5 33.3 Gender (% female, all members) 45% 51% Contract
Created for Report Date: NOV-05-2013 Demographics Subscribers 4,895 - Members 12,746 - Membership 13,461 - Age (subscribers) 41.0 41.0 Age (members) 28.5 33.3 Gender (% female, all members) 45% 51% Contract
A. Encounter Data Submission Requirements
 A. Encounter Data Submission Requirements APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY: A. As of October 1, 2015, IEHP has transitioned to ICD-10 diagnosis and procedure coding
A. Encounter Data Submission Requirements APPLIES TO: A. This policy applies to all IEHP Medi-Cal Providers. POLICY: A. As of October 1, 2015, IEHP has transitioned to ICD-10 diagnosis and procedure coding
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM
 IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
Tennessee Health Care Innovation Initiative
 March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
McLaren Health Plan Quality Improvement Update 2014
 McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
2017 Quality Rewards Program
 2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Anthem Blue Cross. CCHCA Physician Handbook (7 th Edition) Updated 3/15
 Updated 3/15") Part II Section B Anthem Blue Cross Introduction 1 Verifying Member Eligibility and Benefits 1 Sample Anthem Blue Cross Member ID Card 2 Anthem Blue Cross Managed Medi-Cal Program 4 CCHCA Physician Handbook
Part II Section B Anthem Blue Cross Introduction 1 Verifying Member Eligibility and Benefits 1 Sample Anthem Blue Cross Member ID Card 2 Anthem Blue Cross Managed Medi-Cal Program 4 CCHCA Physician Handbook
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
In This Issue. Issue: 8. Codes Utilization FAQs Harry s Health Highlights. Who s Harry? HEDIS News
 Issue: 8 Who s Harry? Born from the mists of success, and integrated into the core of our measures; Harry forges forward in an undying quest to bring H knowledge to Cenpatico s provider network. In This
Issue: 8 Who s Harry? Born from the mists of success, and integrated into the core of our measures; Harry forges forward in an undying quest to bring H knowledge to Cenpatico s provider network. In This
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
Medical Records Review & Retrieval
 Healthcare Effectiveness Data Information Set (HEDIS) Medical Records Review & Retrieval Measuring quality of care and services provided to our members! Date: November 16, 2016 Partnership HealthPlan Presenter:
Healthcare Effectiveness Data Information Set (HEDIS) Medical Records Review & Retrieval Measuring quality of care and services provided to our members! Date: November 16, 2016 Partnership HealthPlan Presenter:
Medicare Advantage Star Ratings
 Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Oregon's Health System Transformation
 Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
ZIP CODE. Other Zip Codes Unknown Residence
 ZIP CODE Zip Code Other Zip Codes Unknown Residence TOTAL Patients Note: This is a representation of the form; however the actual on line input process will look significantly different, as may the printed
ZIP CODE Zip Code Other Zip Codes Unknown Residence TOTAL Patients Note: This is a representation of the form; however the actual on line input process will look significantly different, as may the printed
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Medicare & Medicaid. William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA
 Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
2018 Hospital Pay For Performance (P4P) Program Guide. Contact:
 Program Guide. Contact:") 2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Please stand by. There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1
 Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Meaningful Use and PCC EHR
 Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
PATIENT CENTERED. Medical Home. Attestation. Facility Compliance
 2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Inside This Issue: * Introductory Letter to Premier Blue Providers. * Credentialing. * Office Site Assessments * HEDIS. * Office Medical Record Review
 PB-1-99 March 10, 1999 Sent to: PB PCPs, RSs Inside This Issue: * Introductory Letter to Premier Blue Providers * Credentialing * Office Site Assessments * HEDIS * Office Medical Record Review * Member
PB-1-99 March 10, 1999 Sent to: PB PCPs, RSs Inside This Issue: * Introductory Letter to Premier Blue Providers * Credentialing * Office Site Assessments * HEDIS * Office Medical Record Review * Member
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Pediatrics How-to Guide for TRICARE Beneficiaries. Readiness Better Care Trusted Care, Anywhere Best Value Better Health
 Pediatrics How-to Guide for TRICARE Beneficiaries Pediatric Clinic Operations How to Set Up an Appointment Appointment Line 722-1802 (0700-1630) Call early for same day appointment! 1. The Appointment
Pediatrics How-to Guide for TRICARE Beneficiaries Pediatric Clinic Operations How to Set Up an Appointment Appointment Line 722-1802 (0700-1630) Call early for same day appointment! 1. The Appointment
Table of Contents. ii 2016 New Jersey HMO & PPO Performance Report
 Table of Contents Commissioner s Letter... 1 Introduction... 2 Quality Matters... 3 Staying Healthy... 4 Breast Cancer Screening... 5 Cervical Cancer Screening... 6 Colorectal Cancer Screening... 7 Childhood
Table of Contents Commissioner s Letter... 1 Introduction... 2 Quality Matters... 3 Staying Healthy... 4 Breast Cancer Screening... 5 Cervical Cancer Screening... 6 Colorectal Cancer Screening... 7 Childhood
Assistance. Improving. Consumer Health. Strategies for
 Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
HEDIS. Provider Manual. McLarenHealthPlan.org
 HEDIS Provider Manual McLarenHealthPlan.org TABLE OF CONTENTS Welcome... 2 How to Use this Manual... 3 Section 1: Partnering with McLaren Health Plan to Measure Quality Pay for Performance (P4P) Program
HEDIS Provider Manual McLarenHealthPlan.org TABLE OF CONTENTS Welcome... 2 How to Use this Manual... 3 Section 1: Partnering with McLaren Health Plan to Measure Quality Pay for Performance (P4P) Program
Meaningful Use Stage 1 Guide for 2013
 Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
2016 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
DENVER HEALTH MEDICAL PLAN, INC. & DENVER HEALTH MEDICAID CHOICE Medicaid Choice & CHP+ Quality Improvement Work Plan
 *2016-2017 QI Program Description-Scope The QI Program Description is reviewed annually and updated according to national and state standards and guidelines. The QI program scope, goals, objectives and
*2016-2017 QI Program Description-Scope The QI Program Description is reviewed annually and updated according to national and state standards and guidelines. The QI program scope, goals, objectives and
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
2017 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
Meaningful Use of an EHR System
 Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program
 + Welcome Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program March 6, 2012 We will begin promptly @ 1 PM EST Event
+ Welcome Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program March 6, 2012 We will begin promptly @ 1 PM EST Event
FEE FOR SERVICE MEASURES
 FEE FOR SERVICE MEASURES Fee for Service (FFS) Measures provide a single payment incentive to PCP sites in exchange for performing a service or activity. All 2018 measures require providers to submit a
FEE FOR SERVICE MEASURES Fee for Service (FFS) Measures provide a single payment incentive to PCP sites in exchange for performing a service or activity. All 2018 measures require providers to submit a
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
HEDIS Provider Guide & Toolkit
 HEDIS Provider Guide & Toolkit MolinaHealthcare.com HEDIS 2016 Contents Welcome...1 How to Use this Guide...2 Section 1: Molina Healthcare Resources What can we do for you?...3 Contact Information...4
HEDIS Provider Guide & Toolkit MolinaHealthcare.com HEDIS 2016 Contents Welcome...1 How to Use this Guide...2 Section 1: Molina Healthcare Resources What can we do for you?...3 Contact Information...4