TRANSITION PREPARATION
|
|
|
- Godwin Brown
- 5 years ago
- Views:
Transcription

1 Health Care Transition & Title V Care Coordination Initiatives: Webinar Series Webinar # 2 March 28, 2018 TRANSITION PREPARATION Michelle Jiggetts, MD, MS, MBA Program Administrator Complex Care Program and Parent Navigator Program Children s National Health System s Goldberg Center Patience White, MD, MA Co-Director, Got Transition The National Alliance to Advance Adolescent Health
2 Disclosures and Funding Source Michelle Jiggetts and Patience White have no financial disclosures or conflicts of interest. Got Transition, a program of The National Alliance to Advance Adolescent Health, is funded by the Maternal and Child Health Bureau, Health Resources and Services Administration, DHHS. 2
3 Support state Title V implementation and measurement of health care transition (HCT) in care coordination programs Got Transition s Webinar Series Goals Guide care coordination improvements by sequentially building on the evidence-informed Six Core Elements Share promising practices from state Title V-supported care coordination programs (CC) 5-session webinar series on HCT and care coordination The webinars and handouts will be available following each session at 3
4 At the conclusion of Webinar 2, attendees will be able to Webinar #2 Objectives Identify key components of HCT policy for CC programs that families/youth want to know Customize transition readiness assessment (RA) for CC programs Pilot and disseminate HCT policy and RA Incorporate RA skill needs into plan of care and educate youth and families on needed skills Prepare medical summary and emergency care plan with youth and families and their providers 4
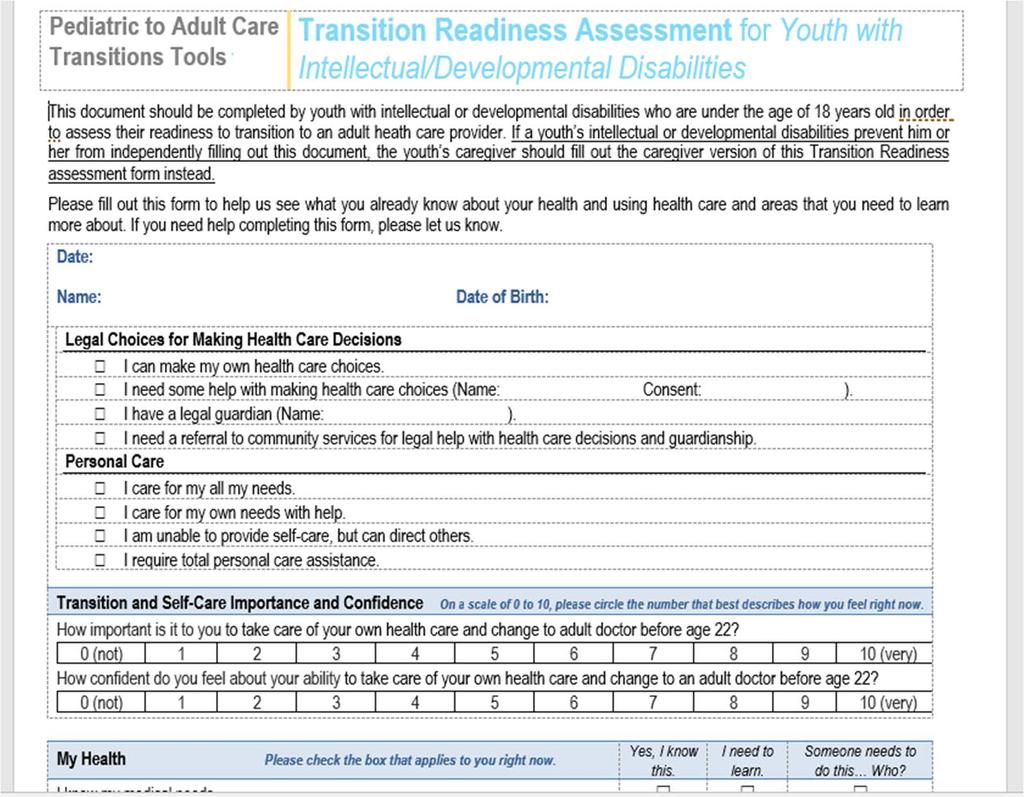
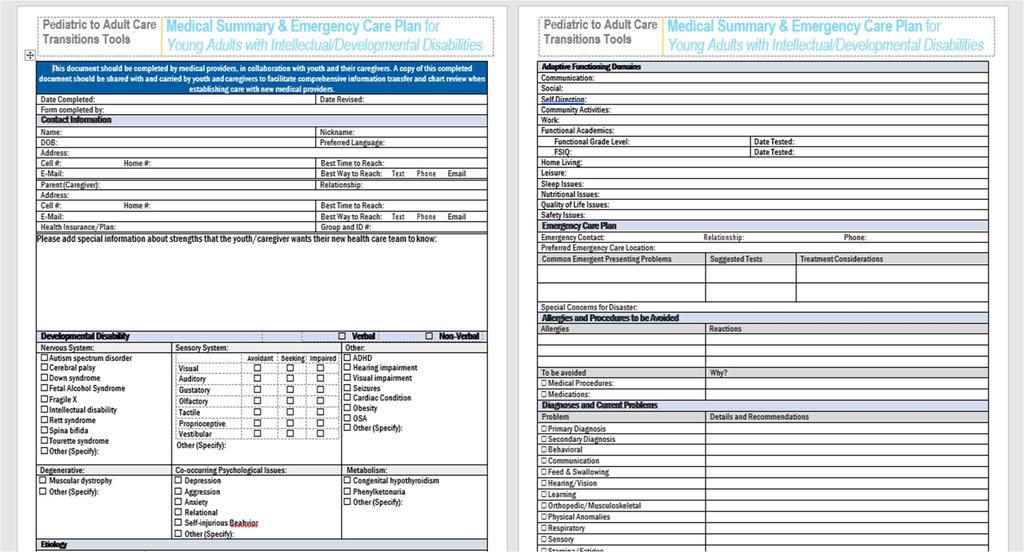
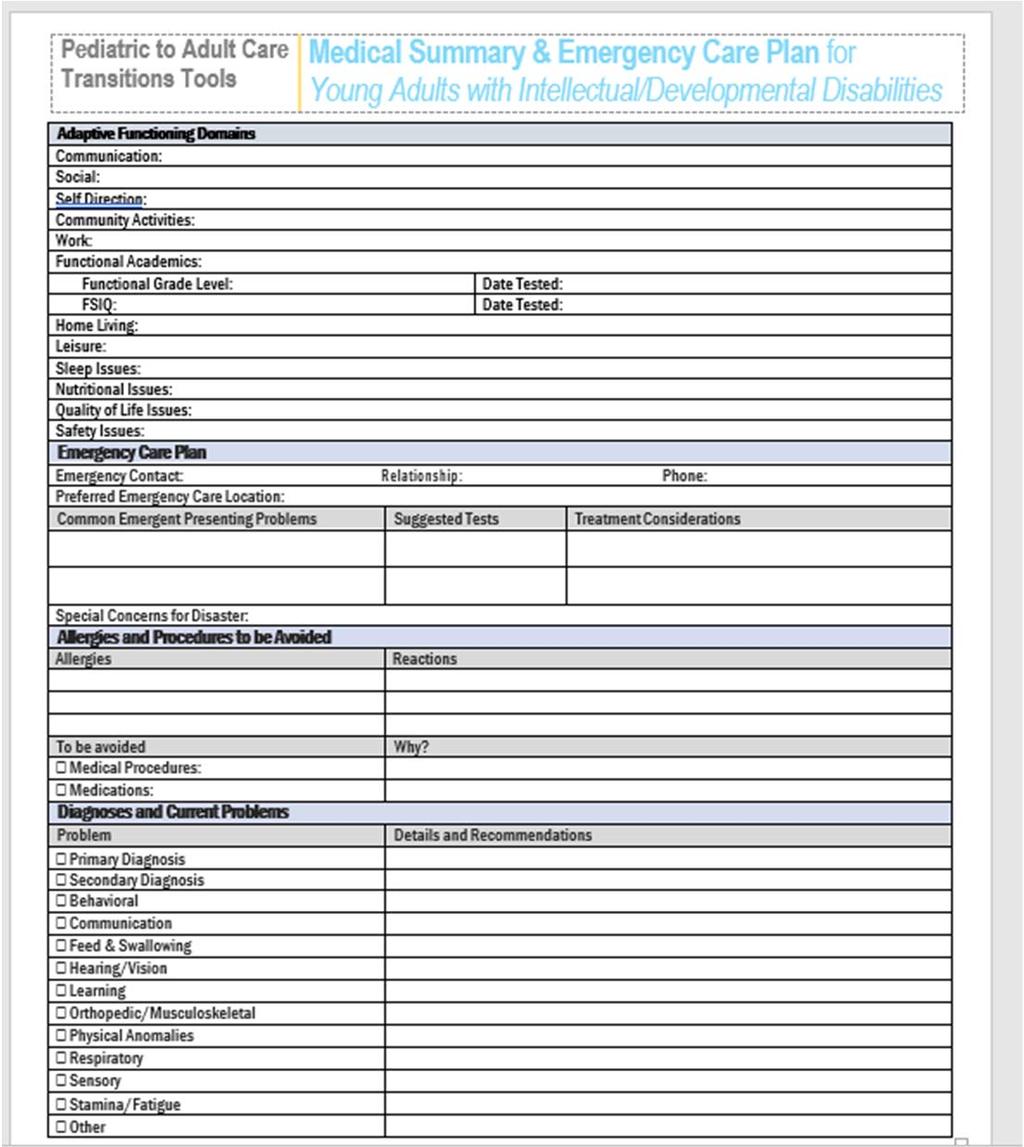
5 Webinar #2 Handouts 1. Webinar #2 Slideshow 2. iphone and Android Info sheets 3. Got Transition RA 4. Youth with ID/DD and parent readiness assessments 5. Medical Summary for youth with ID/DD 5
6 Webinar #1 REVIEW HCT Clinical Foundations HCT Performance Measurement Title V Baseline Assessment Starting a HCT Pilot using Quality Improvement and the Core Element Processes 6


7 HCT Clinical Foundations Six Core Elements of HCT: Transitioning Youth to an Adult Clinician 7










8 Sample Forms and Templates Discuss transition policy AGE AGES Track progress Assess skills AGES AGES Develop transition plan Transfer documents AGE months after transfer Confirm completion

9
10 Core Element #1: POLICY Purpose: Formalize CC program s approach, reduce care coordinators variability and offer a transparent approach to youth and families Content: Define program approach and recommended ages for transition preparation for adult-focused care, transfer, and integration into adult care Clarify adult approach to care and legal changes at age 18 Reading level should be appropriate Post: Communicate it to all involved early in the process 10
11 Transition Policy Challenges How to establish a written HCT policy? What topics should be included in a policy? How best to get youth and family/caregiver involvement and feedback? How and with whom should the policy be shared?

12
13 Purpose: Facilitate systematic data collection to improve quality at individual and population levels Core Element #2: TRANSITION TRACKING & MONITORING Content: Demographic and diagnostic/complexity data Date of receipt of each core element (e.g., policy shared, readiness assessment administered, etc.) Format: paper checklist, excel spreadsheet, EHR 13
14 Transition Tracking & Monitoring Challenges What information should be tracked e.g., name, date of birth, case mix complexity, diagnosis, date of receipt of each core element? What options are available to track and trigger use of core elements within CC programs?

15
16
17 Purpose: Assess the youth s skills to manage their health/health care in the adult approach to care. Core Element #3: TRANSITION READINESS Content: Ranks importance of changing to adult provider before age 22 Ranks confidence about ability of changing to adult provider Assesses self-care skills related to own health and using health care services Use: Completed several times during the transition process Used as a discussion tool to plan skillbuilding education Does not predict transition success Customized to meet the needs of the practice s population 17
18 Assessment indicators of importance and confidence added to the readiness assessment tool (post testing) Transition Readiness or Self-Care Assessment Drawn from decision making & motivational interviewing content Includes questions with rating scale: 1. Importance: How do you feel at this moment about Moving to a doctor who cares for adults? How important is it to you personally to manage your own health care? (If 0 was not important and 10 was very important, what number would you give your self?) 2. Confidence: If you decided right now to transfer to an adult provider, how confident do you feel about succeeding with this? (If 0 is not confident and 10 is very confident, what number would you give yourself?) Clinician action: If importance rating is low, focus on this first; If ratings are roughly equal, start with importance

19 Smart Phone Majority of youth/young adults have a cell phone Strategies for Youth Uptake of Key Health Information Knowledge Add health information to their phone e.g. diagnosis, allergies, medications, who to contact in an emergency Accessible without a passcode for access (EMS, others) Facilitates their ability to communicate/keep track of key health information Example: Health Apps for iphones 19
: o o o o General Medicine (SGIM, SAHM, HCTN, ACP, AAP, AAFP, AOA, Med-Ped Program")
20 ACP Council on Subspecialties Transition Initiative Partnership with Got Transition in 2016 Customized Six Core Elements transition readiness assessment, self-care assessment, and medical summary for selected conditions (teams included representatives from pediatric and adult professional and patient groups): o o o o General Medicine (SGIM, SAHM, HCTN, ACP, AAP, AAFP, AOA, Med-Ped Program Directors) ID/DD Physical disabilities Hematology (Hemophilia, Sickle Cell Disease), Cardiology (CHD), Endocrine Society (Diabetes), Gastroenterology (IBD), Neurology (Epilepsy), Nephrology (ESRD), Rheumatology (JIA, SLE) Available at under News and Announcements or ACP website
21
22 Transition Readiness Challenges What skills about health and health care are important for CC clients to know? How can youth and family/caregiver involvement and feedback on the RA be obtained? When should transition readiness be assessed? Will youth and parents complete the RA on their own or will the CC administer the RA?

23
24 Purpose: Establish agreement between youth and CC and/or clinician about set of actions to address priorities and access current medical information Core Element #4: TRANSITION PLANNING Content: Identify what matters most to youth in becoming adult beyond health goals Define how learning about health and health care supports youth s over all goals (add readiness assessment skill needs to the plan) ACP project developed POC templates for ID, physical disabilities along with some subspecialty diseases (see Also complete portable medical summary and emergency care plan with special information non medical for adult provider 24
25
26 How to incorporate HCT into plan of care? Transition Planning Challenges How can youth and family/ caregiver involvement and feedback on HCT plan of Care be obtained? How can CC programs enable HCP to complete medical summary and emergency care plan? Who will provide needed self care education?

27 What to do? Where to start? 27
28 Introductory Remarks Djinge Lindsay, MD, MPH Deputy Director for Policy and Programs Community Health Administration (CHA) 28

29 Parent Navigators: Making the Transition Connection in DC Got Transition Webinar Health Care Transition & Title V Care Coordination Transition Planning Michelle Jiggetts, MD, MS, MBA March 28, 2018
30 Objectives Discuss History of Parent Navigator Program Discuss role of Parent Navigators Discuss Transition integration into the Medical Home setting using the Six Core Elements Next Steps
 employed by the hospital to provide peer support to other families of CSHCN Currently have 6 full time PN s Available to families of CYSHCN")
31 Parent Navigator Program: Our Story Program established in 2008 Based in Goldberg Center for Community Pediatric Health Children s National COE Support from DC DOH and Maryland DHMH Composed of parents of children with special health care needs (CSHCN) employed by the hospital to provide peer support to other families of CSHCN Currently have 6 full time PN s Available to families of CYSHCN receiving primary care and complex care services at Children s National

32 Parent Navigator: A Key Member of the Medical Healthcare Team Insurance Case Manager Primary Care Medical Home School Nurse Community Therapists Specialty Physicians Private Duty Nurse Inpatient Care Team Parent Navigator
33 Roles and Responsibilities Based on Pediatricians and Family Needs Provide Peer-to-Peer support Coach families how to advocate for their child Help families to communicate more effectively with health care professionals Coach families how to navigate services throughout the hospital and in the community Link families to community and educational resources Work with families to understand their educational rights and responsibilities (e.g. IFSP, IEP, 504) Provide follow-up with families to ensure needs are met Prepare families for transitioning to adult health services
34 Integrating Transition Formulated a Transition team Program Administrator, Navigators, Physicians from both primary and adolescent departments Facilitate bi-weekly transition meetings Reviewed Six Core Element toolkit Performed a Self-Evaluation Designed Transition Integration according to the Six Core Elements


35 Self Evaluation Reviewed Got Transition National Standards

36 Putting the Six Core Element Pieces Together Transfer Completion Transfer of Care Transition Planning Transition Readiness Transition Tracking & Monitoring Transition Policy

37 1 Transition Policy Six Core Element National Standard Develop a transition policy/statement with input from youth and families that describe the practice s approach to transition, including privacy and consent information Educate all staff about the practice s approach to transition, the policy/statement, the Six Core Elements, and distinct roles of the youth, family, and pediatric and adult health care team in the transition process, taking into account cultural preferences. Post policy and share/discuss with youth and families, beginning at age 12 to 14, and regularly review as part of ongoing care. Navigator s Role A Transition policy/statement has been developed, uploaded to our intranet. Educated management staff and Adolescent providers on the particulars of the policy Policy is discussed with youth and families, beginning at age 14 when the Readiness Assessment is completed.

38 2 Transition Tracking & Monitoring Six Core Element National Standard Establish criteria and process for identifying transitioning youth and enter their data into a registry. Utilize individual flow sheet or registry to track youth s transition progress with the Six Core Elements. Incorporate the Six Core Elements into clinical care process, using HER if possible Navigator s Role Established criteria and process for identifying transitioning youth and enter their data into a registry. o All children between years with complex medical needs, autism and developmental delay o Receive a list every week of eligible teens that have upcoming appointments o List is divided up among navigators according to alphabet Created a registry to track youth s transition planning
39 PN Transition Registry Excel Registry Components of the Transition Registry Name Patient Residence Service location Insurance Attempts Made(1 st, 2 nd, 3 rd ) Date RA Obtained Goals Discussed Adult Provider Name Date of Appt. Feedback

40 3 Transition Readiness Six Core Element National Standard Conduct regular transition readiness assessments, beginning at age 14, to identify and discuss with youth and parent/caregiver their needs and goals in self-care Jointly develop goals and prioritized actions with youth and parent/caregiver and document regularly in a plan of care Navigator s Role Conduct regular transition readiness assessments, beginning at age Verification of cognitive level and age of patient to determine if the child or the parent should complete the Readiness Assessment (RA) Generate weekly calls to families Meet family at the visit Discuss goals and prioritize actions with youth and parent/caregiver. Utilize registry to track youth s transition o RA documented in EMR o Telephone Encounter sent to provider seeing pt. to notify them of Administer the RA
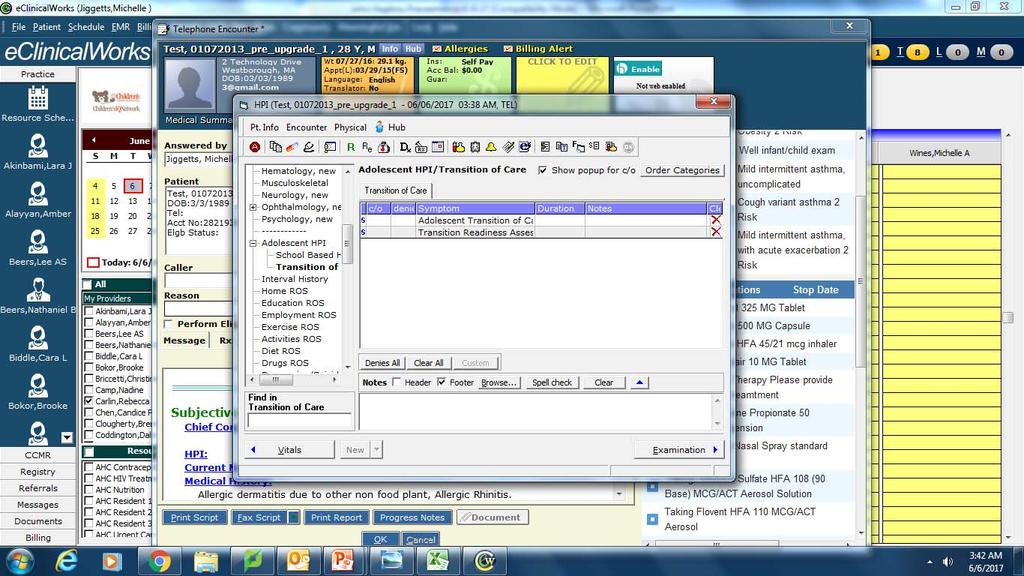
41 Documentation of RA

42 Goals Discussed

43 4 Transition Planning Six Core Element National Standard Including readiness assessment findings, goals and prioritized actions, medical summary and emergency care plan, and if needed, a condition fact sheet and legal documents. Prepare youth and parent/caregiver for adult approach to care at age 18, including legal changes in decisionmaking and privacy and consent, self-advocacy and access to information. Determine level of need for decision-making supports for youth with intellectual challenges and make referrals to legal resources. Plan with youth/parent/caregiver for optimal timing of transfer. If both primary and subspecialty care are involved, discuss optimal timing for each. Assist youth in identifying an adult provider and communicate with selected provided about pending transfer of care. Provide linages to insurances resources, self-care management information and culturally appropriate community supports. Navigator s Role Prepare youth and parent/caregiver for adult approach to care at age 18. Start the discussion around Power of Attorney versus Guardianship Determine level of need for decision-making supports for youth with intellectual challenges and make referrals to legal resources. Dissemination of guardian decision making and guardianship brochure. Assist youth in identifying an adult provider and communicate with selected provided about pending transfer of care. o PN provides family an adult provider list Provide linkages to insurances resources, self-care management information and culturally appropriate community resources.

44 5 Transfer of Care Six Core Element National Standard Confirm date of first adult provider appointment. Transfer young adults when his/her condition is stable Complete transfer package, including final transition readiness assessment, plan of care with transition goals and pending actions, medical summary and emergency care plan, and it needed, legal documents, condition fact sheet, and additional provider records. Prepare letter with transfer package, send to adult practice and confirm adult practice s receipt of transfer package. Confirm with adult provider the pediatric provider s responsibility for care until young adult is seen in adult setting. Navigator s Role Navigator assists family with scheduling the initial adult primary care visit. Assists family with getting a copy of the medical visit summary and an immunization record.

45 6 Transfer Completion Six Core Element National Standard Contact young adult and parent/caregiver 3 to 6 months after last pediatric visit to confirm transfer of responsibilities to adult practice and elicit feedback on experience with transition process. Communicate with adult practice confirming completion of transfer and offer consultation assistance, as needed. Build ongoing and collaborative partnerships with adult primary and specialty care providers. Navigator s Role Navigators contacts families approximately 2 wks. after the appt. to verify attendance.
46 Reasons for continuing to do this Parent Comments I never really thought about guardianship, happy that you re doing it. Don t know what my child is able to do. I can start working on goals with my her. Wish I started this process earlier. Why are you starting at 14 years of age.
47 Next Steps Develop Training workshops for families Develop Training workshops for providers Collaborate with hospital staff to strategize on making this a hospital-wide effort 19
48 Questions? About writing HCT Policy with staff, youth and family and sharing it with them? About customizing the RA? About creating a plan of care with HCT components such as with RA skill needs? About how DC s Parent Navigator Program implements the 6 Core Element Process? 29
49 Transfer to Adult Care April 26, 3-4 pm ET Upcoming Title V Care Coordination Webinars Integration into Adult Care May 31, 3-4 pm ET Youth, Young Adult, & Parent Engagement June 28, 3-4 pm ET To register, please visit Got Transition s website under Webinars (
50 Thank You! WEBSITE See link to new transition news and articles and download the Six Core Elements 2.0 packages to start making HCT quality improvements in your practice FACEBOOK PAGE HealthCareTransition 31

51 EXTRA SLIDES
52
Clinician Information Packet: Transition from Pediatric to Adult Care
 Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Youth Health Transition Quality Improvement Grant Guidance Wisconsin Children and Youth with Special Health Care Needs
 Youth Health Transition Quality Improvement Grant Guidance Wisconsin Children and Youth with Special Health Care Needs Thank you for your interest in the Wisconsin Youth Health Transition Quality Improvement
Youth Health Transition Quality Improvement Grant Guidance Wisconsin Children and Youth with Special Health Care Needs Thank you for your interest in the Wisconsin Youth Health Transition Quality Improvement
CHRISTOPHER PEZZULLO, DO, CHIEF HEALTH OFFICER, DHHS
 SUPPORTING HEALTH CARE TRANSITION FROM ADOLESCENCE TO ADULTHOOD CHRISTOPHER PEZZULLO, DO, CHIEF HEALTH OFFICER, DHHS NANCY CRONIN, MA EXECUTIVE DIRECTOR, MAINE DEVELOPMENTAL DISABILITIES COUNCIL APRIL
SUPPORTING HEALTH CARE TRANSITION FROM ADOLESCENCE TO ADULTHOOD CHRISTOPHER PEZZULLO, DO, CHIEF HEALTH OFFICER, DHHS NANCY CRONIN, MA EXECUTIVE DIRECTOR, MAINE DEVELOPMENTAL DISABILITIES COUNCIL APRIL
Medical Transition of Youth with Special Health Care Needs
 Tuesday, 1:00 2:30, B3 Medical Transition of Youth with Special Health Care Needs Tisa M Johnson-Hooper MD Objectives: Identify effective methods for the practical application of concepts related to improving
Tuesday, 1:00 2:30, B3 Medical Transition of Youth with Special Health Care Needs Tisa M Johnson-Hooper MD Objectives: Identify effective methods for the practical application of concepts related to improving
Baseline Assessment of Health Care Transition Implementation in Title V Care Coordination Programs
 R EPORT NO.4 OCTOBER 2 0 1 7 Baseline Assessment of Health Care Transition Implementation in Title V Care Coordination Programs Margaret McManus, MHS Samhita Ilango, BA Daniel Beck, MA Patience White,
R EPORT NO.4 OCTOBER 2 0 1 7 Baseline Assessment of Health Care Transition Implementation in Title V Care Coordination Programs Margaret McManus, MHS Samhita Ilango, BA Daniel Beck, MA Patience White,
Health Care Transition. A Parent, Family and Caregiver s Guide
 Health Care Transition A Parent, Family and Caregiver s Guide Health Care Transition A Parent, Family and Caregiver s Guide The N.C. Family to Family Health Information Center A project of The Exceptional
Health Care Transition A Parent, Family and Caregiver s Guide Health Care Transition A Parent, Family and Caregiver s Guide The N.C. Family to Family Health Information Center A project of The Exceptional
New Directions in Health Care Transition Improvement
 New Directions in Health Care Transition Improvement CAAI Webinar: Autism Spectrum Disorder and Transition April 30, 2014 Patience White, MD. MA Got Transition/Center for Health Care Transition Improvement
New Directions in Health Care Transition Improvement CAAI Webinar: Autism Spectrum Disorder and Transition April 30, 2014 Patience White, MD. MA Got Transition/Center for Health Care Transition Improvement
Health Care Transition for Youth with Special Health Care Needs (YSHCN)
") Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
Health Care Transition for Youth with Special Health Care Needs (YSHCN) Stephanie Lawrence, MD Assistant Professor Division of General Internal Medicine Department of Internal Medicine and Pediatrics The
State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions
 REPORT No.1 F E B R U A R Y 2 0 1 6 State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions Prepared by Margaret McManus, MHS; Daniel Beck, MA; and
REPORT No.1 F E B R U A R Y 2 0 1 6 State Title V Health Care Transition Performance Objectives and Strategies: Current Snapshot and Suggestions Prepared by Margaret McManus, MHS; Daniel Beck, MA; and
TRANSFER TO ADULT CARE
 Health Care Transition & Title V Care Coordination Initiatives: Webinar Series Webinar # 3 April 26, 2018 TRANSFER TO ADULT CARE Karen Rundall, RN, MSN, CCM Lee Gordon, MPA Kentucky Commission for Children
Health Care Transition & Title V Care Coordination Initiatives: Webinar Series Webinar # 3 April 26, 2018 TRANSFER TO ADULT CARE Karen Rundall, RN, MSN, CCM Lee Gordon, MPA Kentucky Commission for Children
Clinical Report Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home
 Guidance for the Clinician in Rendering Pediatric Care Clinical Report Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home abstract Optimal health care is achieved when
Guidance for the Clinician in Rendering Pediatric Care Clinical Report Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home abstract Optimal health care is achieved when
Transition, Families, and Youth-Essentials in the Medical Home Neighborhood
 Transition, Families, and Youth-Essentials in the Medical Home Neighborhood A statewide quality improvement initiative for children and youth with special health care needs Lizanne Welding Mills, MS, MBA
Transition, Families, and Youth-Essentials in the Medical Home Neighborhood A statewide quality improvement initiative for children and youth with special health care needs Lizanne Welding Mills, MS, MBA
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group
 Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Approaches to Transitioning Youth and Young Adults from Pediatric to Adult Health Care Systems
 Approaches to Transitioning Youth and Young Adults from Pediatric to Adult Health Care Systems Sponsored by the Health and Disability Special Interest Group (SIG) In collaboration with ITAC 1 Indiana University
Approaches to Transitioning Youth and Young Adults from Pediatric to Adult Health Care Systems Sponsored by the Health and Disability Special Interest Group (SIG) In collaboration with ITAC 1 Indiana University
Health Care Transition
 Health Care Transition Florida Association of Children s Hospitals David Wood, MD, MPH October 3, 2013 www.jaxhats.ufl.edu First the good news 90% of Seriously Ill Children become adults The bad news:
Health Care Transition Florida Association of Children s Hospitals David Wood, MD, MPH October 3, 2013 www.jaxhats.ufl.edu First the good news 90% of Seriously Ill Children become adults The bad news:
Health Literacy, Communication, & Self-Management: Critical Pathways to Adulthood
 Health Literacy, Communication, & Self-Management: Critical Pathways to Adulthood 1 Presenter Janet Hess, DrPH, MPH USF College of Medicine Department of Pediatrics, Adolescent Medicine Project Director,
Health Literacy, Communication, & Self-Management: Critical Pathways to Adulthood 1 Presenter Janet Hess, DrPH, MPH USF College of Medicine Department of Pediatrics, Adolescent Medicine Project Director,
Health Care Transition Training for Health Care Professionals
 Health Care Transition Training for Health Care Professionals Presenters 2 Janet Hess, DrPH University of South Florida Assistant Professor FloridaHATS Project Director (813) 259-8604 jhess@health.usf.edu
Health Care Transition Training for Health Care Professionals Presenters 2 Janet Hess, DrPH University of South Florida Assistant Professor FloridaHATS Project Director (813) 259-8604 jhess@health.usf.edu
2016 Complex Case Management Program Description. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Description Our mission is to improve the health and quality of life of our members Complex Case Management Program Description I. Purpose To improve the health status
2016 Complex Case Management Program Description Our mission is to improve the health and quality of life of our members Complex Case Management Program Description I. Purpose To improve the health status
Marsh and McLennan Companies 2018 Overview: Best Doctors, Health Advocate, Cigna and MSK Direct October 12, 2017
 Marsh and McLennan Companies 2018 Overview: Best Doctors, Health Advocate, Cigna and MSK Direct October 12, 2017 Agenda 1 Welcome 2 Best Doctors 3 Health Advocate 4 Cigna EAP 5 MSK Direct 1 Best Doctors
Marsh and McLennan Companies 2018 Overview: Best Doctors, Health Advocate, Cigna and MSK Direct October 12, 2017 Agenda 1 Welcome 2 Best Doctors 3 Health Advocate 4 Cigna EAP 5 MSK Direct 1 Best Doctors
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013
 National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
National Health Policy Forum Richard C. Antonelli, MD, MS Boston Children s Hospital Harvard Medical School November 08, 2013 Understand the potential strengths of family- and patient-centered Medical
Improving Transitions from Child to Adult Care
 Improving Transitions from Child to Adult Care October 19, 2016 @cfhi_fcass Please introduce yourself and your organization name 4 Let s Tweet Together: Join the conversation on Twitter! @CFHI_FCASS @CAPHC
Improving Transitions from Child to Adult Care October 19, 2016 @cfhi_fcass Please introduce yourself and your organization name 4 Let s Tweet Together: Join the conversation on Twitter! @CFHI_FCASS @CAPHC
Consents. Youth s strengths and concerns on transfer (to be completed by youth, parent/family and/or health care team)
") Youth/ Family Family Practitioner Adult Specialist ON TRAC TRANSITION CLINICAL PATHWAY (COMPLEX) DATE INITIATED / / DD MM YYYY DATE LAST CLINIC VISIT / / DD MM YYYY Preferred Name Date of Birth PHN# Initiating
Youth/ Family Family Practitioner Adult Specialist ON TRAC TRANSITION CLINICAL PATHWAY (COMPLEX) DATE INITIATED / / DD MM YYYY DATE LAST CLINIC VISIT / / DD MM YYYY Preferred Name Date of Birth PHN# Initiating
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Advocacy for Adults with Intellectual and Developmental Disabilities Assisting in the Transition from Pediatric to Adult Medical Services
 Advocacy for Adults with Intellectual and Developmental Disabilities Assisting in the Transition from Pediatric to Adult Medical Services November 12, 2016 Richard McChane, M.D. rick.mcchane@twc.com Objectives
Advocacy for Adults with Intellectual and Developmental Disabilities Assisting in the Transition from Pediatric to Adult Medical Services November 12, 2016 Richard McChane, M.D. rick.mcchane@twc.com Objectives
interchange Provider Important Message
 HUSKY Health Primary Care Increased Payments Policy In accordance with Provider Bulletin PB14-75, certain primary care providers are eligible to receive increased Medicaid payments for primary care services
HUSKY Health Primary Care Increased Payments Policy In accordance with Provider Bulletin PB14-75, certain primary care providers are eligible to receive increased Medicaid payments for primary care services
How Confident Are You in This Estimate? (Scale 1-10; 10 high): (low) (high) How Confident Are You in This Estimate?
: (low) (high) How Confident Are You in This Estimate?") On-Site Medical Home Practice/Clinic Assessment Checklist Illinois Medical Home Project (IMHP), Phase II, IL Chapter of the American Academy of Pediatrics (focusing on Children with Special Health Care
On-Site Medical Home Practice/Clinic Assessment Checklist Illinois Medical Home Project (IMHP), Phase II, IL Chapter of the American Academy of Pediatrics (focusing on Children with Special Health Care
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM
 Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM 1 Co-Presenters Ray Hanbury, Ph.D., A.B.P.P. Chief Psychologist, Dept. of Psychiatry
Mental / Behavioral Health Screening in Pediatric Primary Care OVERVIEW OF THE PEDIATRIC PSYCHIATRY COLLABORATIVE PROGRAM 1 Co-Presenters Ray Hanbury, Ph.D., A.B.P.P. Chief Psychologist, Dept. of Psychiatry
Health Smart: Teens with Sickle Cell Disease Moving from Pediatric Care to Adult Care
 Health Smart: Teens with Sickle Cell Disease Moving from Pediatric Care to Adult Care Produced by St. Jude Children s Research Hospital, Departments of Hematology, Patient Education, and Biomedical Communications.
Health Smart: Teens with Sickle Cell Disease Moving from Pediatric Care to Adult Care Produced by St. Jude Children s Research Hospital, Departments of Hematology, Patient Education, and Biomedical Communications.
Personalized Primary Care Annual Meeting. Care Management Catherine Hamilton, BSN, MS, MBA
 Personalized Primary Care Annual Meeting Care Management Catherine Hamilton, BSN, MS, MBA Care Manager Assessments 75% of care managers assessed Observed processes Evaluated against NCQA 2014 Medical Home
Personalized Primary Care Annual Meeting Care Management Catherine Hamilton, BSN, MS, MBA Care Manager Assessments 75% of care managers assessed Observed processes Evaluated against NCQA 2014 Medical Home
Beyond Implementation: Capturing the Value of Care Coordination
 2015 Webinar Series Pediatric Care Coordination: Beyond Policy, Practice, and Implementation A webinar series brought to you by the National Center for Medical Home Implementation Beyond Implementation:
2015 Webinar Series Pediatric Care Coordination: Beyond Policy, Practice, and Implementation A webinar series brought to you by the National Center for Medical Home Implementation Beyond Implementation:
Wisconsin State Plan to Serve More Children and Youth within Medical Homes
 Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Internship Opportunities
 Internship Opportunities Mission Statement The Harrisonburg-Rockingham Community Services Board provides services that promote dignity, recovery, and the highest possible level of participation in work,
Internship Opportunities Mission Statement The Harrisonburg-Rockingham Community Services Board provides services that promote dignity, recovery, and the highest possible level of participation in work,
Louisiana Department of Health and Hospitals Bureau of Health Services Financing
 Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised April
Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised April
ecw Integration PIX, XACML, CCD with Basic Clinical Event Notifications Project Scope Definition
 ecw Integration PIX, XACML, CCD with Basic Clinical Event otifications Project Scope Definition April 27, 2017 I. Key Contacts: Healthix Project Manager and Contact Information: Healthix Business Development
ecw Integration PIX, XACML, CCD with Basic Clinical Event otifications Project Scope Definition April 27, 2017 I. Key Contacts: Healthix Project Manager and Contact Information: Healthix Business Development
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Louisiana Department of Health and Hospitals Bureau of Health Services Financing
 Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised March
Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised March
EXHIBIT AAA (3) Northeast Zone PROVIDER NETWORK COMPOSITION/SERVICE ACCESS
 Northeast Zone PROVIDER NETWORK COMPOSITION/SERVICE ACCESS") EXHIBIT AAA (3) Northeast Zone PROVIDER NETWORK COMPOSITION/SERVICE ACCESS 1. Network Composition The PH-MCO must consider the following in establishing and maintaining its Provider Network: The anticipated
EXHIBIT AAA (3) Northeast Zone PROVIDER NETWORK COMPOSITION/SERVICE ACCESS 1. Network Composition The PH-MCO must consider the following in establishing and maintaining its Provider Network: The anticipated
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Adolescent Champion Model
 Adolescent Champion Model Vision: Transform the healthcare landscape to optimize adolescent and young adult health and well-being Mission: To advance innovative adolescentcentered healthcare through practice
Adolescent Champion Model Vision: Transform the healthcare landscape to optimize adolescent and young adult health and well-being Mission: To advance innovative adolescentcentered healthcare through practice
INFANTS & TODDLERS PROGRAM IFSP SERVICE COORDINATION MEDICAID BILLING MANUAL
 Prince George's County Public Schools INFANTS & TODDLERS PROGRAM IFSP SERVICE COORDINATION MEDICAID BILLING MANUAL 2016-2017 Prince George's County Public Schools Medicaid Office 14201 School Lane, Temp
Prince George's County Public Schools INFANTS & TODDLERS PROGRAM IFSP SERVICE COORDINATION MEDICAID BILLING MANUAL 2016-2017 Prince George's County Public Schools Medicaid Office 14201 School Lane, Temp
Preventative Guidelines
 Preventative Guidelines Well Care Services-determined by age and gender Services paid at 100 percent, meaning- at no cost to you. Ages: Newborn-18 years of age Adults: 19 years and up Diagnostic Checkups
Preventative Guidelines Well Care Services-determined by age and gender Services paid at 100 percent, meaning- at no cost to you. Ages: Newborn-18 years of age Adults: 19 years and up Diagnostic Checkups
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Enhancing the Medical Home for Children with Special Health Care Needs: A Quantitative Approach
 Enhancing the Medical Home for Children with Special Health Care Needs: A Quantitative Approach The Quality Colloquium August 20, 2008 Angelo P. Giardino, MD, PhD, MPH Renee M. Turchi, MD, MPH Overview
Enhancing the Medical Home for Children with Special Health Care Needs: A Quantitative Approach The Quality Colloquium August 20, 2008 Angelo P. Giardino, MD, PhD, MPH Renee M. Turchi, MD, MPH Overview
TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN
 TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN January 21, 2015. Children s Policy Council 1 http://www.amchp.org/aboutamchp/newsletters/member-briefs/documents/standards%20charts%20final.pdf
TX Action Learning Collaborative: National Standards for Systems of Care for CYSHCN January 21, 2015. Children s Policy Council 1 http://www.amchp.org/aboutamchp/newsletters/member-briefs/documents/standards%20charts%20final.pdf
Emergencies in Medically Complex Children: Tip & Tools
 Emergencies in Medically Complex Children: Tip & Tools ANGIE CUNNINGHAM, BSN, RN, CCRN-K, C-NPT TRANSPORT OUTREACH AND EMS RELATIONS COORDINATOR CHILDREN S MERCY CRITICAL CARE TRANSPORT KANSAS CITY, MO
Emergencies in Medically Complex Children: Tip & Tools ANGIE CUNNINGHAM, BSN, RN, CCRN-K, C-NPT TRANSPORT OUTREACH AND EMS RELATIONS COORDINATOR CHILDREN S MERCY CRITICAL CARE TRANSPORT KANSAS CITY, MO
Toolkit to Support Effective Collaboration within an Integrated Care Team
 Toolkit to Support Effective Collaboration within an Integrated Care Team January 2015 1 P a g e PCMCH Toolkit to Support Integrated Care Team Members The Provincial Council for Maternal and Child Health
Toolkit to Support Effective Collaboration within an Integrated Care Team January 2015 1 P a g e PCMCH Toolkit to Support Integrated Care Team Members The Provincial Council for Maternal and Child Health
A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation
 A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation Müge Chavdar, MPH and Joan Jeung, MD, MPH, FAAP This publication of the National Center
A Collection of Strategies Used to Support Innovative and Promising Practices in Pediatric Medical Home Implementation Müge Chavdar, MPH and Joan Jeung, MD, MPH, FAAP This publication of the National Center
Speare Memorial Hospital myspeare Patient Portal User Guide
 Speare Memorial Hospital myspeare Patient Portal User Guide pg. 1 myspeare Patient Portal User Guide Table of Contents Topic Page # Homepage..3 Proxy Access. 4 Contact Us.. 5 What s New.. 6 Profile...7
Speare Memorial Hospital myspeare Patient Portal User Guide pg. 1 myspeare Patient Portal User Guide Table of Contents Topic Page # Homepage..3 Proxy Access. 4 Contact Us.. 5 What s New.. 6 Profile...7
A Transition Protocol at Children s Hospital of Pittsburgh of UPMC
 A Transition Protocol at Children s Hospital of Pittsburgh of UPMC Unoma Akamagwuna MD, Rachel Young CRNP-BC, Amy Houtrow MD, Brad Dicianno MD Pediatric Rehabilitation Medicine University of Pittsburgh
A Transition Protocol at Children s Hospital of Pittsburgh of UPMC Unoma Akamagwuna MD, Rachel Young CRNP-BC, Amy Houtrow MD, Brad Dicianno MD Pediatric Rehabilitation Medicine University of Pittsburgh
EPAs, Competencies and Milestones: Putting it all Together
 EPAs, Competencies and Milestones: Putting it all Together 2014 Fall APPD Meeting Robert Englander, MD,MPH Carol Carraccio, MD, MA Disclosures We have no financial or other Conflicts of Interest to disclose
EPAs, Competencies and Milestones: Putting it all Together 2014 Fall APPD Meeting Robert Englander, MD,MPH Carol Carraccio, MD, MA Disclosures We have no financial or other Conflicts of Interest to disclose
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Welcome to the Webinar!
 Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
AMCHP 2017 Annual Conference Saturday, March 4, :30-4:30PM
 The National Standards for Systems of Care for Children and Youth with Special Health Care Needs: New Frontiers in Implementation for Title V and Partners AMCHP 2017 Annual Conference Saturday, March 4,
The National Standards for Systems of Care for Children and Youth with Special Health Care Needs: New Frontiers in Implementation for Title V and Partners AMCHP 2017 Annual Conference Saturday, March 4,
Multidisciplinary Intervention Navigation Team (MINT) for Pediatric to Adult Healthcare Transitions
 for Pediatric to Adult Healthcare Transitions") Multidisciplinary Intervention Navigation Team (MINT) for Pediatric to Adult Healthcare Transitions North Texas Transitional Care Sophia Jan, MD, MSHP Feb 16, 2017 @PolicyLabCHOP GOAL To increase safety
Multidisciplinary Intervention Navigation Team (MINT) for Pediatric to Adult Healthcare Transitions North Texas Transitional Care Sophia Jan, MD, MSHP Feb 16, 2017 @PolicyLabCHOP GOAL To increase safety
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18
 Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs
 Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs Presenter: Richard Antonelli, MD, Medical Director, Integrated Care
Walking before Running: Developing Care Coordination Capacity to Achieve High Value Outcomes for Patients with Behavioral Health Needs Presenter: Richard Antonelli, MD, Medical Director, Integrated Care
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Uses a standard template but may have errors of omission
 Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
Louisiana Department of Health and Hospitals Bureau of Health Services Financing
 Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised June
Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised June
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Louisiana Department of Health and Hospitals Bureau of Health Services Financing
 Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised November
Louisiana Department of Health and Hospitals Bureau of Health Services Financing Affordable Care Act Enhanced Reimbursement of Primary Care Services Informational Bulletin December 19, 2012 Revised November
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Memorandum of Understanding NAME OF AUTISM IDENTIFICATION TEAM
 Among Name of Medical Practice Name of County Health Department Name of County Health Department Name of Educational Service District or School District For the Provision of Services and Referrals Related
Among Name of Medical Practice Name of County Health Department Name of County Health Department Name of Educational Service District or School District For the Provision of Services and Referrals Related
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Challenging Behaviour Program Manual
 Challenging Behaviour Program Manual Continuing Care Branch Table of Contents 1.0 Introduction... 2 2.0 Purpose... 2 3.0 Vision... 2 4.0 Mission... 3 5.0 Guiding Principles... 3 6.0 Challenging Behaviour
Challenging Behaviour Program Manual Continuing Care Branch Table of Contents 1.0 Introduction... 2 2.0 Purpose... 2 3.0 Vision... 2 4.0 Mission... 3 5.0 Guiding Principles... 3 6.0 Challenging Behaviour
Children s Hospital Association Summary of Final Regulation. November 9, 2012
 Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Comprehensive Community Services (CCS) File Review Checklist Comprehensive
 File Review Checklist Comprehensive") This is a sample form developed by the "CCS Statewide QA/QI Work Group", and is available to CCS sites as a sample for consideration of use, modification, and customization. There is no implicit or explicit
This is a sample form developed by the "CCS Statewide QA/QI Work Group", and is available to CCS sites as a sample for consideration of use, modification, and customization. There is no implicit or explicit
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
So You Want to Start a Down Syndrome Clinic?
 So You Want to Start a Down Syndrome Clinic? Lessons Learned and Pitfalls to Avoid: Our 20 year Experience running a Down Syndrome Clinic in Ottawa, Canada Dr Mary Pothos, Dr Asha Nair, Dr Rob Laberge
So You Want to Start a Down Syndrome Clinic? Lessons Learned and Pitfalls to Avoid: Our 20 year Experience running a Down Syndrome Clinic in Ottawa, Canada Dr Mary Pothos, Dr Asha Nair, Dr Rob Laberge
Launching Rx for CalFresh in San Diego County
 Launching Rx for CalFresh in San Diego County Integrating Food Security into Healthcare Settings Amanda Schultz Brochu, MPH CalFresh Outreach Director San Diego Hunger Coalition www.sdhunger.org SDHC Mission
Launching Rx for CalFresh in San Diego County Integrating Food Security into Healthcare Settings Amanda Schultz Brochu, MPH CalFresh Outreach Director San Diego Hunger Coalition www.sdhunger.org SDHC Mission
HOME HEALTH VALUE BASED PURCHASING FREQUENTLY ASKED QUESTIONS Updates in Red
 1. What is the contact information of the Home Health Value-Based Purchasing (HHVBP) Helpdesk? General HHVBP The HHVBP Helpdesk can be reached by email at HHVBPquestions@cms.hhs.gov). The Helpdesk number
1. What is the contact information of the Home Health Value-Based Purchasing (HHVBP) Helpdesk? General HHVBP The HHVBP Helpdesk can be reached by email at HHVBPquestions@cms.hhs.gov). The Helpdesk number
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Maternal and Child Health Services Title V Block Grant for New Mexico. Executive Summary. Application for Annual Report for 2015
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Assuring Better Child Health and Development Initiative (ABCD)
") Assuring Better Child Health and Development Initiative (ABCD) Presented by Jennifer May National Academy for State Health Policy Act Early Region X Summit Feb 4-5, 2010 Seattle, Washingon Supported by
Assuring Better Child Health and Development Initiative (ABCD) Presented by Jennifer May National Academy for State Health Policy Act Early Region X Summit Feb 4-5, 2010 Seattle, Washingon Supported by
Minnesota Chapter of the American Academy of Pediatrics Foster Care Health Learning Collaborative
 Minnesota Chapter of the American Academy of Pediatrics Foster Care Health Learning Collaborative Comments on Minnesota s services for children in foster care as outlined in the Minnesota Annual Progress
Minnesota Chapter of the American Academy of Pediatrics Foster Care Health Learning Collaborative Comments on Minnesota s services for children in foster care as outlined in the Minnesota Annual Progress
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Please return your completed materials to: Duke University Medical Center Box 3417 Durham, NC 27710
 Thank you for your interest in the with the Child and Adolescent Life Program. Our internship program is offered two times a year: Fall (September-December) and Spring (January April) To be qualified for
Thank you for your interest in the with the Child and Adolescent Life Program. Our internship program is offered two times a year: Fall (September-December) and Spring (January April) To be qualified for
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Improving Outcomes in Sickle Cell Anemia: The Role of a Transition Program
 Improving Outcomes in Sickle Cell Anemia: The Role of a Transition Program Mailman Center for Child Development May 27, 2016 Ofelia Alvarez, MD Director University of Miami Sickle Cell Center University
Improving Outcomes in Sickle Cell Anemia: The Role of a Transition Program Mailman Center for Child Development May 27, 2016 Ofelia Alvarez, MD Director University of Miami Sickle Cell Center University
Resident Dyads Providing Transition Care to Adolescents and Young Adults With Chronic Illnesses and Neurodevelopmental Disabilities
 Resident Dyads Providing Transition Care to Adolescents and Young Adults With Chronic Illnesses and Neurodevelopmental Disabilities Richard J. Chung, MD Joan Jasien, MD Gary R. Maslow, MD, MPH ABSTRACT
Resident Dyads Providing Transition Care to Adolescents and Young Adults With Chronic Illnesses and Neurodevelopmental Disabilities Richard J. Chung, MD Joan Jasien, MD Gary R. Maslow, MD, MPH ABSTRACT
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Captivate Wednesday, April 23, 2014
 Slide 1 PATIENT CARE INQUIRY (PCI) ACCESSING PATIENT'S MEDICAL RECORDS IN MEDITECH Content provided by: Melinda Mauk-Templeton, IT Clinical Systems Analyst Development by: Deb Rodman, IT Training Analyst
Slide 1 PATIENT CARE INQUIRY (PCI) ACCESSING PATIENT'S MEDICAL RECORDS IN MEDITECH Content provided by: Melinda Mauk-Templeton, IT Clinical Systems Analyst Development by: Deb Rodman, IT Training Analyst
PMA Cenpatico Integrated Care. Guidance Document. [Special Assistance] Developed by. Cenpatico Integrated Care
![PMA Cenpatico Integrated Care. Guidance Document. [Special Assistance] Developed by. Cenpatico Integrated Care](/thumbs/75/72141872.jpg "PMA Cenpatico Integrated Care. Guidance Document. [Special Assistance] Developed by. Cenpatico Integrated Care") PMA 3.11.1 Cenpatico Integrated Care Guidance Document [Special Assistance] Developed by Cenpatico Integrated Care Effective Date: [November 2016] 1 TITLE [Special Assistance Guidance Document] GOAL/WHAT
PMA 3.11.1 Cenpatico Integrated Care Guidance Document [Special Assistance] Developed by Cenpatico Integrated Care Effective Date: [November 2016] 1 TITLE [Special Assistance Guidance Document] GOAL/WHAT
Intellectual Disability Waiver Transition Plan Regarding Compliance with the HCBS Final Rule Elements July 30, 2014
 Intellectual Disability Waiver Transition Plan Regarding Compliance with the HCBS Final Rule Elements July 30, 2014 Assessment of Waiver and Service Definitions Virginia is currently in the process of
Intellectual Disability Waiver Transition Plan Regarding Compliance with the HCBS Final Rule Elements July 30, 2014 Assessment of Waiver and Service Definitions Virginia is currently in the process of
Provider Orientation to Magellan s Outpatient Behavioral Health Model
 Provider Orientation to Magellan s Outpatient Behavioral Health Model July 2017 Big-picture objectives Magellan Healthcare s outpatient care management model: Reduces provider administrative tasks Expedites
Provider Orientation to Magellan s Outpatient Behavioral Health Model July 2017 Big-picture objectives Magellan Healthcare s outpatient care management model: Reduces provider administrative tasks Expedites
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
State of California Health and Human Services Agency Department of Health Care Services
 State of California Health and Human Services Agency Department of Health Care Services JENNIFER KENT DIRECTOR EDMUND G. BROWN JR. GOVERNOR DATE: December 3, 2015 ALL PLAN LETTER 15-025 (SUPERSEDES ALL
State of California Health and Human Services Agency Department of Health Care Services JENNIFER KENT DIRECTOR EDMUND G. BROWN JR. GOVERNOR DATE: December 3, 2015 ALL PLAN LETTER 15-025 (SUPERSEDES ALL