Renee Coughlin PT, DPT, MHS Steven Pamer PT, MPA, CGS
|
|
|
- Lynn O’Brien’
- 5 years ago
- Views:
Transcription
 - Ability to cope with the medical costs of our aging")
1 Improving Chronic Care Renee Coughlin PT, DPT, MHS Steven Pamer PT, MPA, CGS The Financial Imperative United States Economy - Cost $1 trillion annually and could reach $6 trillion by 2050 Failure to contain the containable undermines: - Potential of extending health care coverage (the ACA) - Ability to cope with the medical costs of our aging population 1


2 United States Volumes United States Cost Burden 2


3 Economic Impact: The Alternative Path Impact on GDP in
4 Impact on Healthcare Spending Chronic conditions are widespread Primary consumers of health care - Drive most health care spending Account for 75% of all: - Hospital Days - Physician Office Visits - Home Health Care - Prescription Drugs Human Costs Leading cause of death & disability in the U.S. (7 out of 10 deaths) - Heart disease, cancer & stroke account for 50% of all deaths - About 25% have 1 ADL limitation(s) - Arthritis is most common cause of disability (19 million Americans) - DM is leading cause of kidney failure, non-traumatic LE amputations and blindness among adults 4




5 Whoever said If you always do what you ve always done, you will always get what you ve always got. 5
6 How do we identify the appropriate patient? RISK STRATIFICATION - A tool used to identify those at low risk, moderate risk and high risk Software written by our IT Sits over the top of our EMR Tools are only as good as the education to the staff Risk Stratification Report Patient Code Zip Code M30 SOC M0032 ReSu M66 DOB Gender Diagnosis x 13 Falls M1000 Inpatient Facility M1032 Risk for Hospitalization M1034 Overall Status 6
7 Risk Stratification Report PHQ-2 M1740 Cog Behavioral M1400 SOB M1410 Resp. Treatments M1302 Risk of Wound M1340 Surgical Incision M1100 Patient Living Situation Risk Stratification Report M1910 Multi Factorial Fall Assess. M2100 Caregiver Management M2020 Oral Meds M2013 Injectable Meds Discipline at SOC 7
8 Cost Associated with HF 2008 study published in Health Services Research 1,435 hospitalizations of patients 60 years of age Median cost: $10,454 Titler MG et al. Cost of hospital care for older adults with heart failure: Medical, pharmaceutical, and nursing costs. Health Serv Res Apr, 43(2): Our Hospital Has a Patient Five admissions through the ED between 5/9/2014 and 8/29/ $10,454 X 5 = $52,270 - $13, 060 x 5 = $65,300 Time for something different 8
9 Cross-Continuum Collaboration Cardiologist Visiting Physician Practice - PCP and NP Visiting Palliative Medicine Physicians Home Health RN, PT and OT - All came together to pilot a hospital at home concept Mr. J. 81 years old and living in the community in his own home - Chronic combined systolic and diastolic HF (NYHA Class III) - Cardiac Amyloidosis - Chronic hyponatremia - Oxygen 2LPM continuous - 9 additional comorbid conditions - DC home with PICC line in place 9
10 New York Heart Association Classifications Class I Class II Class III Patients experience no limitations; ordinary physical activity does not cause undue fatigue, dyspnea or palpitations Patients experience slight limitation of physical activity; patients are comfortable at rest; ordinary physical activity results in fatigue, palpitations, dyspnea or angina Patients experience marked limitation of physical activity. Although patients are comfortable at rest, less than ordinary activity leads to fatigue, dyspnea, palpitations or angina Class IV Symptoms of HF are present at rest; discomfort increases with any physical activity Pilot: Hospital at Home Hospital DC 9/6/2014 Home Health SOC 9/7/2014 RN visits : 24 PT Visits : 16 OT Visits: 6 NP Visits: 9 MD Visits: 3 10


11 11/2/

12 Home Health Costs Fully loaded cost of 46 skilled home visits: $ Reimbursement: $ Net: $37.88 Mr. J. passed away in March at home with the care of his siblings, children and Hospice services 12
13 Positive Outcomes The patient was able to remain out of acute care and in his home for the last 6 months of his life The patient s family met their goal of keeping him home and participating in caring for him Home Care Value Proposition Assuming the rate of 5 admissions per 4 months, the hospital saved 7.5 acute admissions, or: 7.5 X $10,454 = $78, x $13,060= $97,950 13
14 Business-as-Usual Assumes the current baseline projections for 2003 to 2023 hold relative to: - The aging population - Behavioral risk factors and other demographic influences - Improvement in early detection and medical innovation - Health-care cost changes Alternative Path Assumes a range of reasonable improvements in prevention, behavioral patterns, and treatment: - Reduction in Obesity - Continued reduction in smoking - Decline in alcohol consumption - Increase in physical activity - Percentage of people with high cholesterol stabilizes at 2000 levels 14

15 Two Paths, Two Choices True Patient-Centered Care Paradigm shift in interaction with patients Validated partnership-based approaches (e.g. Motivational Interviewing) are superior for uncovering and addressing ambivalence and key motivational barriers to change 15
16 Partnership Model of Care Practitioners are the experts on disease; patients are the experts on their own lives Shared caregiving and responsibility for outcomes Patients identify the problems their diseases cause, e.g. limited mobility; practitioners help clarify Partnership Model Patients set their goals and practitioners help them make informed choices Change is motivated internally; patient self-efficacy is key 16
17 Self-Care Support Focus on solving the problems that the medical condition causes through good care, self-care information and behavior change support (in contrast to patient education) Mr. P. 84 year old former Marine - Comorbidities: CHF, Anxiety/ Depression, DM, Ca, frequent UTIs - First admission with CCAH was 3/2014, 3 additional admissions through 12/ (of 42) rehab visits by 6 different clinicians 17
18 Health Literacy The degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions 18
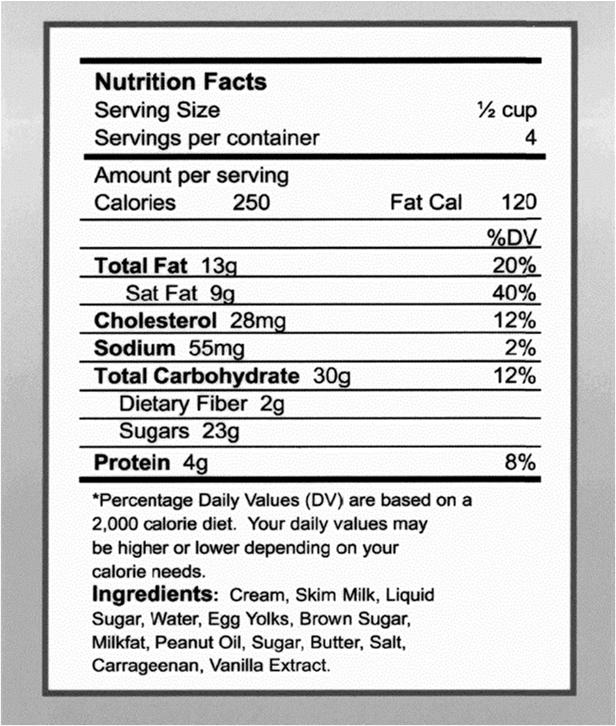
19 Risk for Limited Health Literacy Increases in individuals with: - Lower education or socioeconomic level - Older adults with vision, hearing or memory disorders - Limited English proficiency (when the providers speak only English) Assessing Health Literacy The Newest Vital Sign (Pfizer/Weiss et al., 2005) - Uses a nutrition label to assess an individual s ability to follow physician instructions regarding health 19
20 20


21 Patient Activation Found to be strongly related to a broad range of health-related outcomes Patients are an untapped resource in the effort to improve health care quality - Benefit to themselves, health care delivery systems and our nation 21
22 Patient Activation Assessment Eric Coleman, MD, MPH Tracks patient progress in skill transfer and activation along the Four Pillars during participation in the Care Transitions Intervention - Medication Management - Red Flags - Medical Care Follow Up - Personal Health Record Time Points for Completion First home visit (baseline) After each contact At discharge Evaluations are tracked on the Patient Activation Assessment form 22

23 Medication Management Patient Activation Assessment Level of Performance (Please rate: 1 point each) Red Flags Medical Care Follow Up Personal Health Record (PHR) Comments Demonstrates effective use of Medication Management System (medication organizer, flow chart, etc.) For each medication, understands the purpose, when and how to take, and possible side effects Demonstrates ability to accurately update medication list Agrees to confirm medication list with PCP and/or Specialist Demonstrates understanding of Red Flags, or warning signs that condition may be worsening Reacts appropriately to Red Flags per education given (or understands how to react appropriately) Can schedule and follow through on appointment(s). Writes a list of questions for PCP and/or specialist and brings to appointment Understands the purpose of PHR and the importance of updating PHR Agrees to bring PHR to every health encounter Sum: /4 Sum: /2 Sum: /2 Sum: /2 Total Score: /10 Copyright The Care Transitions Program, Eric A. Coleman, MD, MPH WISE Model 23
24 WISE Model of Chronic Conditions Better engage patients Facilitate better health care Facilitate health behavior changes Puts the spotlight on the patient, not the disease Bring barriers to health improvement to the surface Helps clinicians leverage their expertise Focus on The Big Five Coronary Artery Disease (CAD) Heart Failure (HF) Diabetes Chronic Obstructive Pulmonary Disease (COPD) Asthma 24
25 Why The Big Five? Because they are: a) Prevalent b) Costly c) Associated with standards of care d) Have a significant impact on health HF: Self-Care Steps Follow CAD Self-Care Recommendations Monitor Weight Daily Most HF patients can benefit from general CAD self-care recommendations for diet, weight management, stress management, and coping. Patients with HF should obtain a physical activity prescription that specifies the activity type, intensity, and duration according to their HF severity level and functional status. Weight monitoring helps quickly identify fluid retention. Patients should weight themselves upon rising, after they have urinated, but before eating breakfast. They should also notify their physician immediately if they experience a daily weight gain of more than 2-3 pounds. Manage Sodium Intake Sodium intake should be limited to 2,000 milligrams per day. Patients should be particularly careful of hidden sodium in many packaged and prepared foods. 25
26 HF: Self-Care Steps, continued Manage Fluid Intake Some physicians may also recommend restrictions of daily fluid intake. Manage Alcohol Intake Avoid alcohol or consume no more than two to three alcoholic drinks per week. Adjust Sleeping Position Sleep with head propped at a 45 degree angle if experiencing shortness of breath. Other Self-Care Considerations Lifestyle Management - Diet and Nutrition - Hydration - Weight Management - Physical Activity - Stress Management - Tobacco Cessation 26
27 Health Coaching Ideal Approach - Appropriate for across continuum - Well to seriously ill - Younger to older - Less or more educated or verbal - Practical in any patient encounter - Any member of health care team, clinical and non-clinical Ideal Approach continued Validated steps for teaching and proficiency Supported by standardized, validated tools Patient-centered, but flexible for practitioners to apply clinical expertise and address priorities Proven to deliver better patient-level outcomes 27
28 Motivational Interviewing (MI) Currently the only approach that meets the Ideal Approach criteria The patient, rather than the practitioner, voices the arguments for the behavior change Outperforms traditional advice-giving in the treatment of a broad range of behavioral problems and diseases Patient Talk Three Types Change Talk: Statements in favor of change Sustain Talk: Statements that represent ambivalence about change Discord: Statements that represent an interpersonal tension between the patient and practitioner 28
29 Practitioner Behaviors MI-consistent (MIC) - Ask for permission - Validate patient s position, barriers to change, challenging situation - Support patient control/autonomy - Provide affirmations that address strengths or patient activation MI-inconsistent Behaviors (MIIN) More consistent with the traditional patient education model Confronting, directing, providing information or advice without permission Higher levels of MIIN are associated with higher levels of resistance Lower levels of MIIN, with greater patient engagement 29
30 Comparison of Approaches Traditional Medical Model Expert Authoritarian Judgmental Confrontational or pushy Based on premise that information changes behavior Objective is to direct and tell what to do Emphasis on gathering and sharing information Goal is treatment adherence and positive clinical outcome MI-Based Model Collaborative Evocative Empathetic Supportive of autonomy and choice Based on evidence-based behavior change science Objective is to activate and empower Emphasis on encouraging selfcare Goal is treatment adherence Basic Skills in MI Open Questions Affirmations Reflections Summaries 30
31 Challenges Non-adherence Patients who are stuck Passive patients Cultural differences Low health literacy Older patients with cognitive issues Multiple chronic conditions Mental illness Move from Volume to Value - 90% of all Medicare spending has a link to quality by % of all Medicare payments tied to quality or value through alternative payment models by 2018 ACOs Bundled Payment for Care PCMH/Medicaid Health Homes 31
32 Home Health Value-Based Purchasing (HHVBP) Proposed Implementation 1/1/16-5 years 2016 to 2022 Basis for HHVBP - Tie quality to payment to improve outcomes - Payment adjustments that reward/penalize will incent providers - ACA requires HHS to develop plan for HHVBP under Medicare 6 HHVBP Domains 29 Metrics Clinical Quality of Care Communication and Care Coordination Efficiency and Cost Reduction Patient Safety Patient and Caregiver Centered Experience (CAHPS) Population/Community Health 32
33 33
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings
 Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
Oxford Condition Management Programs:
 Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment
 Toolkit Questionnaires for use in a comprehensive needs assessment") Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment This resource is a guide to conducting a comprehensive needs assessment for the Coordinated Veterans Care
Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment This resource is a guide to conducting a comprehensive needs assessment for the Coordinated Veterans Care
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
COPD National Action Plan. COPD.nih.gov
 COPD National Action Plan COPD.nih.gov Kyle Mahan, MSM, RRT Vice President of KSRC DCE for Jefferson Community and Technical College RCP 14-ish Years AZ native. I am not from Kentucky, but I got here as
COPD National Action Plan COPD.nih.gov Kyle Mahan, MSM, RRT Vice President of KSRC DCE for Jefferson Community and Technical College RCP 14-ish Years AZ native. I am not from Kentucky, but I got here as
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
EVOLENT HEALTH, LLC. Asthma Program Description 2018
 EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Maternity Management. The best part? These are available to you at no additional cost. Intro
 Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN ( )
") MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN (2016-2019) An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for each hospital within the Central Community: * Hospital
MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN (2016-2019) An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for each hospital within the Central Community: * Hospital
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
INTEGRATED CARE SERVICE AND OUTCOMES
 DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Ambulatory Care Management An Enhanced Care Coordination Program
 Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
Thinking Differently about Hospital Readmissions
 Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
arizona health net a better decision sm Putting you at the center of everything we do.
 arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have
arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have
PROVIDER NEWSLETTER. Illinois 2016 Issue II DISEASE MANAGEMENT IMPROVING MEMBERS HEALTH IN THIS ISSUE
 Illinois 2016 Issue II PROVIDER NEWSLETTER DISEASE MANAGEMENT IMPROVING MEMBERS HEALTH Disease Management is a no-cost, voluntary program to assist members with specific chronic conditions. A member is
Illinois 2016 Issue II PROVIDER NEWSLETTER DISEASE MANAGEMENT IMPROVING MEMBERS HEALTH Disease Management is a no-cost, voluntary program to assist members with specific chronic conditions. A member is
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Blending Behavioral Health and Primary Care. Applying the Model. Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist
 Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
EVOLENT HEALTH, LLC. Asthma Program Description 2017
 EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Outline 11/17/2014. Overview of the Issue Program Overview Program Components Program Implementation
 Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Module 7. Tips for Family and Friends
 Module 7 Tips for Family and Friends The Heart Failure Society of America (HFSA) is a non-profit organization of health care professionals and researchers who are dedicated to enhancing quality and duration
Module 7 Tips for Family and Friends The Heart Failure Society of America (HFSA) is a non-profit organization of health care professionals and researchers who are dedicated to enhancing quality and duration
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation. by Christina Rock, BSN, RN Supervisor, Clinical Education
 Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
SURVEY Being Patient. Accessibility, Primary Health and Emergency Rooms
 SURVEY 2017 Being Patient Accessibility, Primary Health and Emergency Rooms Being Patient: Accessibility, Primary Health and Emergency Rooms New Brunswick Health Council Who we are New Brunswickers have
SURVEY 2017 Being Patient Accessibility, Primary Health and Emergency Rooms Being Patient: Accessibility, Primary Health and Emergency Rooms New Brunswick Health Council Who we are New Brunswickers have
For fully insured groups of 100 or more eligible employees. HealthyOutcomes. A fully-integrated health management solution that works for you
 For fully insured groups of 100 or more eligible employees HealthyOutcomes wellness case management condition care maternity A fully-integrated health management solution that works for you HealthyOutcomes
For fully insured groups of 100 or more eligible employees HealthyOutcomes wellness case management condition care maternity A fully-integrated health management solution that works for you HealthyOutcomes
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
New Options in Chronic Care Management
 New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Quality Measurement at the Interface of Health Care and Population Health
 1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans
 Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans A Report of the Iowa Chronic Care Consortium February 2003 Background The Iowa Chronic Care Consortium
Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans A Report of the Iowa Chronic Care Consortium February 2003 Background The Iowa Chronic Care Consortium
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Programs and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance Program
 s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
The Camden Coalition of Healthcare. Management
 Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
NATIONAL ACADEMY OF CERTIFIED CARE MANAGERS
 NATIONAL ACADEMY OF CERTIFIED CARE MANAGERS Content Domains and Care Manager Tasks The Care Manager Certification examination questions contain content from the following domains. The approximate percentage
NATIONAL ACADEMY OF CERTIFIED CARE MANAGERS Content Domains and Care Manager Tasks The Care Manager Certification examination questions contain content from the following domains. The approximate percentage
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
IMPROVES HEALTH RELATED QUALITY OF LIFE (HRQOL)
") Objectives Chronic Disease Self Management Dr. Shah MD, MPH, FAAFM What are Chronic Diseases/illness/conditions How common are Chronic Diseases/illness/conditions Silent Killer Secrets Hospitals Won t
Objectives Chronic Disease Self Management Dr. Shah MD, MPH, FAAFM What are Chronic Diseases/illness/conditions How common are Chronic Diseases/illness/conditions Silent Killer Secrets Hospitals Won t
Heart Failure Education Consider Health Literacy
 Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease This booklet has been written to answer questions that many patients and family members ask about their care during their hospital stay. It will explain the experiences
Chronic Obstructive Pulmonary Disease This booklet has been written to answer questions that many patients and family members ask about their care during their hospital stay. It will explain the experiences
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
A20, B20. This presenter has nothing to disclose
 A20, B20 This presenter has nothing to disclose What Matters to You? Using Co-design to Revolutionize Patient Experience Christina Gunther-Murphy, MBA, The Institute for Healthcare Improvement Beth Hennessey,
A20, B20 This presenter has nothing to disclose What Matters to You? Using Co-design to Revolutionize Patient Experience Christina Gunther-Murphy, MBA, The Institute for Healthcare Improvement Beth Hennessey,
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination.
 NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
E-nabling Disease Management through IT The Next Generation of DM services
 E-nabling Disease Management through IT The Next Generation of DM services The Disease Management Colloquium Jefferson Medical College, Philadelphia, PA June 27-30, 2004 Thomas G. Lundquist, MD, MMM Executive
E-nabling Disease Management through IT The Next Generation of DM services The Disease Management Colloquium Jefferson Medical College, Philadelphia, PA June 27-30, 2004 Thomas G. Lundquist, MD, MMM Executive
Michigan Newsletter Summer 2010
 What s New Michigan Newsletter Summer 2010 Provider Demographic Changes Effective September 1, 2010 Molina Healthcare will allow Providers to submit their demographic changes either via e-mail, regular
What s New Michigan Newsletter Summer 2010 Provider Demographic Changes Effective September 1, 2010 Molina Healthcare will allow Providers to submit their demographic changes either via e-mail, regular
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Primary Care Development in Hong Kong: Future Directions
 Primary Care Development in Hong Kong: Future Directions HA Convention 2014 8 May 2014 Professor Sophia CHAN PhD, MPH, MEd, RN, RSCN, FAAN, FFPH, JP Under Secretary for Food and Health, Government of the
Primary Care Development in Hong Kong: Future Directions HA Convention 2014 8 May 2014 Professor Sophia CHAN PhD, MPH, MEd, RN, RSCN, FAAN, FFPH, JP Under Secretary for Food and Health, Government of the
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Effective Care Coordination
 Effective Care Coordination Coordinating Care for Adults with Multiple Chronic Illnesses: Searching for the Holy Grail National Health Policy Forum March 27, 2009 Randall Brown, Ph.D. Goals of Presentation
Effective Care Coordination Coordinating Care for Adults with Multiple Chronic Illnesses: Searching for the Holy Grail National Health Policy Forum March 27, 2009 Randall Brown, Ph.D. Goals of Presentation