AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE
|
|
|
- Darrell Lang
- 5 years ago
- Views:
Transcription
1 AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE 1
2 Road map What is DSRIP (Delivery System Reform Incentive Payments) Integrating the mission of DSRIP & End the Epidemic Building community based collaborative leadership REACH Collaborative Creating a cross-agency team of community health navigation, peer support and coordination Bringing care out into the community through DSRIP waivers Using information systems as essential tools to support access, integration and care coordination Improving access to clinical care and care coordination through practice transformation
3 What is DSRIP? In 2014, Governor Andrew Cuomo announced that New York State and CMS finalized agreement on the Medicaid Redesign Team Waiver Amendment. $6.42 Billion for Delivery System Reform Incentive Payments (DSRIP) Specific Goals 1. Reduce avoidable hospitalizations and emergency department visits by 25% over 5 years 2. Transform the Medicaid delivery system to be value-based 3. Achieve Triple Aim (improved health, improved quality, lower costs) 3

 Cure Hepatitis C")

4 What are we trying to accomplish? End the AIDS Epidemic (PEP, PrEP & TasP) Cure Hepatitis C Projected HCV related deaths without treatment People living with HIV w/ Medicaid are not in care 4
 C Pharmacy")
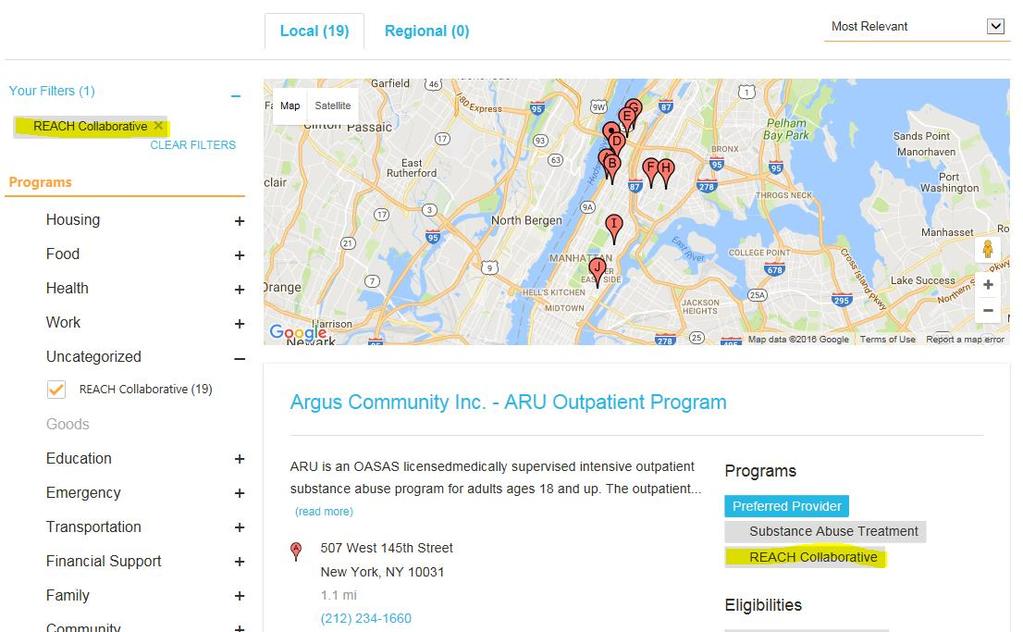
5 REACH Collaborative Ready to End AIDS & Transitions of Care Medical Delivery Health Case On-site System Management Home Reform Incentive Cure Hepatitis Case HIV Hepatitis Management Program Testing C Services (DSRIP) C Pharmacy Services 5

6 Care Coordination through IT integration Health Exchange Resource Mapping Care Coordination 6
7 Care Coordination through IT integration 7
8 8
9 9
10 Stimulating Transformation of Technology and Team structure to Reach People Living with HIV A Special Projects of National Significance Project Supported by HRSA
11 Practice Transformation - Susan Olender, MD, MS September 8, 2016 AIDS Institute Quality of Care Clinical Advisory Meeting
12 Objectives Healthcare delivery changes and impact on practice model Support for change CHP Practice transformation Model Quality and Practice Transformation 12

13
 Delivery System Reform Incentive Payment (DSRIP) ACO Practice Transformation Model (PTM)")
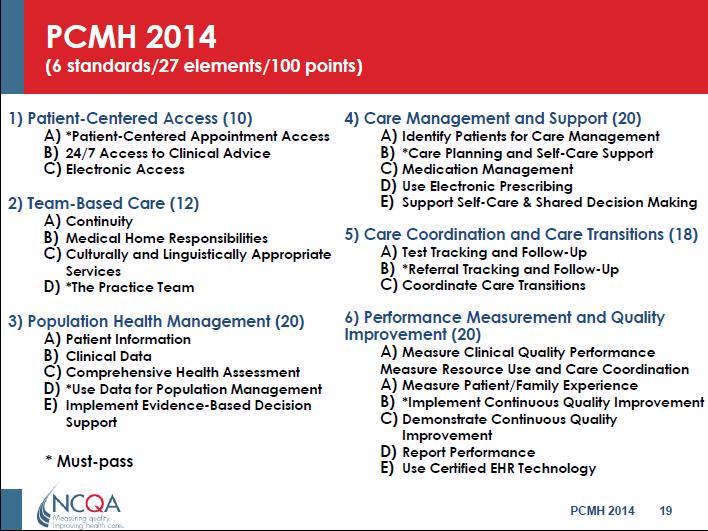
14 Alphabet Soup of Delivery System Change Affordable Care Act (ACA) Patient Centered Medical Homes (PCMH) Health Homes (HH) Accountable Care Organization (ACO) Delivery System Reform Incentive Payment (DSRIP) ACO Practice Transformation Model (PTM) 14
15 HRSA Recognizes Need for Capacity Building and Creates a SPNS Initiative Trends affecting HIV care: Growing population Aging population with complex medical and psychosocial comorbidities Improved access to care First generation of HIV providers nearing retirement Ongoing changes to the health care system and funding as a result of ACA Lack of full integration of care, silos Outcome: Demand for services is eventually expected to exceed capacity 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
16 SPNS: System-level Workforce Capacity Building for Integrating HIV Primary Care in Community Healthcare Settings Goal: To identify successful practice transformative models (PTMs) Efficiencies in structural workforce systems that optimize human resources and improve health outcomes PTMs tackle workforce challenges in multiple ways 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
17 HRSA SPNS Workforce Initiative Project Title: Workforce Capacity Building Initiative 4-Year HRSA-Special Project of National Significance Grant Funded to design, implement, evaluate, and disseminate the intervention Multi-site: 15 demonstration sites across the country Practice Transformation Models or PTMs System level staffing changes Heavily based on Patient Centered Medical Home (PCMH) Improves capacity to care for people living with HIV, valuing efficiency and sustainability Optimizes resources in changing landscape Improves linkage, engagement, retention in care, and suppression rates Cross-site Evaluation UCSF s Evaluation and Technical Assistance Center (ETAC) 17


18 Comprehensive Health Program (CHP) Academic medical center in Upper Manhattan Level II PCMH Provides outpatient & inpatient care to people living with or at-risk for HIV 2200 ambulatory patients and 20 bed inpatient unit Multidisciplinary clinical care Providers, nurses, social workers, care coordinators, nutritionist, psychiatrists, patient navigators, medical and nursing assistants 18
19 Why Practice Transformation at CHP? Changing healthcare landscape HIV primary care workforce shortages Increasing demand for access to quality HIV, HCV and Prevention services More than 100 staff operating in a variety of settings Inpatient Outpatient Community Home Visits Growing attention to at-risk population through expansion of: Sexual health services (PrEP, PEP, STIs) Hepatitis C care and treatment 19

20 Planning the Practice Transformation: PRECEDE PROCEDE Framework 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
 Targeting Members of Clinical")
21 Pre-Implementation Activities HIV Surveillance & Ryan White Program Data (Publicly Available) HIV Care Continuum Indicators Clinic Observation Activities Focus Groups with Clinic Staff STaR Pre-Launch Survey (ie: Teams, Flow, Function, IT) Targeting Members of Clinical Care Teams 21
22 CHP Program Impact Pathway (Logic Model) Inputs Funding & Resources Facilities & Equipment Evidence-Base Policies, Protocols & Guidelines Training & Technical Assistance CHP & NYP Strategic Plans Health Information Technology Monitoring and Evaluation (M&E) Systems Community Partners Activities Clinical & Non-Clinical Services Patient Flow Redesign Expanded Walk-In Capacity & Targeted Coordination of Same Day Services Population Health Management by Clinical Care Teams (CCT) Integrated Clinical & Non-Clinical Care Coordination via CCTs RN & Non-RN Care Coordinator Support of Care Transitions Referrals & Linkages to Community-Based Services Community-Based Outreach & Engagement Consumer Education Consumer Advocacy Outputs Prevention, Care & Support, and Treatment Services Provided Workflow Changes & Quality Improvements Implemented Increase Capacity in Team-Based Care Coordination & Population Health Management Successful Outreach & Engagement of High- Risk Populations and Linkage to Treatment, Care, and Supportive Services Patients Self-Efficacy, Satisfaction & Engagement in Program Development Outcomes (Intermediate Effects) Improvements in Service Delivery: Access Coverage Quality Cost-Effectiveness Staff- & Team-Level Changes in: Knowledge Attitudes Practices Increase Proportion of Patients: Retained in Care & Achieved Viral Suppression Impact (Distal Effects) Psychosocial wellbeing improved among HIV-positive individuals HIV prevalence decreased in the community HIV incidence decreased in the community HIV morbidity & mortality decreased among HIV-positive individuals CHP Quality Improvement, Monitoring & Evaluation of Program 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
23 Stimulating Transformation: Needs Assessment Care Coordination Inefficiencies in identifying who to follow-up Separate programs for adherence, care coordination, nursing care, medical care Communication Complex communication patterns Multiple staff members in various settings with variable communication Untapped opportunities for efficiencies through HIT 23
24 Stimulating Transformation: Needs Assessment Accessibility Need for strengthening patient access to same-day walk-in care Many providers are not on-site full time (fellows, researchers, etc.) No-shows High no-show rates resulting in lost capacity Staff working at the top of their license Primary Care Nursing 24
25
26 26
27 Percentage Number and Proportion of Persons with HIV in New York City Engaged in Selected Stages of the Continuum of Care at the End of % 133, % 114,926 80% 60% 40% 20% 0% Estimated HIVinfected 86% of infected Ever HIVdiagnosed 97,940 73% of infected 85% of diagnosed Ever linked to HIV care 72,918 55% of infected 74% of linked to care Retained in HIV care in 2012 Engagement in HIV care 67,624 51% of infected 93% of retained in care Presumed ever started on ART 55,453 41% of infected 82% of started on ART Suppressed viral load ( 200 copies/ml) in 2012 Of all persons estimated to be infected with HIV in NYC, 41% have a suppressed viral load. As reported to the New York City Department of Health and Mental Hygiene by June 30, For definitions of the stages of the continuum of care, see Appendix 2.
28 28

29 Community Outreach
30 Stimulating Transformation of Technology and Team structure to Reach People Living with HIV

31 STaR Practice Transformation Model: Providing More Care Through Harmonious Redesign (without sacrificing quality) Enhanced Communication Efficient Use of Clinical Space - Patient flow redesign Integrating Health Information Technology for Population Health Management - Designing IT dashboard to summarize key indicators for each team LTFU, High Acuity, etc. Panel-Based Clinical Care Team - Organizing staff into dedicated teams for specific groups of patients - Engaging Teams in Quality Coordinated Care Across Settings - Developing the role of the RN Clinical Care Coordinator to provide support transitions, facilitate CCTs and support navigators 31
32 STaR Practice Transformation Activities Practice Operations and Systems Practice Staff Consumers Pre- Implementation Implementation Evaluation 32
33 Panel-Based Care
34 Building the Clinical Care Teams 600 Provider (PCP)-Social Worker (SW) Team Alignment 300 Social Worker Distribution by Team A Provider PCP Team A PCP Team B PCP Team C PCP Team D PCP Team E 0 No SW Assigned SW Team E SW Team D SW Team C SW Team B SW Team A Salcedo Rojas Pudil Hidalgo Cruz Cella- Shackelford Cabrera Cabreja Campos 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT




35 Panel-Based Clinical Care Teams & Coordinated Care Across Settings CCT A STaR Clinical Care Coordinator at the Comprehensive Health Program CCT B CCT C CCT D STaR Clinical Care Coordinator: Provides CCT structure and training Supports Navigators, Community Health Workers and Peer Educators Crosses settings and program boundaries Social Worker(s) Registered Nurse Clinicians Care Coordinators Patient Navigators Social Worker Registered Nurse Clinicians Care Coordinators Patient Navigators Social Worker Registered Nurse Clinicians Care Coordinators Patient Navigators Social Worker(s) Registered Nurse Clinicians Care Coordinators Patient Navigators Adherence Supervisor, Community Health Worker, Peer Educator, Nutritionist, Psychiatrist, Patient Financial Advisors, & Other Staff Care Enhancements: Better communication Social Worker co-lead Clinical Care Teams Medication adherence through Primary Care RN Integration of HIV Prevention Coordinated Services for People with Complex Co-Morbidities Integration of Behavioral Health 35
 Theme-based discussion calendar Review of Dashboard indicators 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE &")
36 Coordinating Weekly Care Team Meetings RN Care Coordinators send out daily reminders Pre-meeting planning between RN Care Coordinators and Social Worker (Team Co-Captains) Theme-based discussion calendar Review of Dashboard indicators 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

37 Patient Discussion Structure 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
38 Population Health Through HIT
39 Accesible Health Information Technology Improve registry functions Search for patients based on key indicators Uncontrolled HIV? Recent hopsitalizations? Recent visit? Lost to follow-up Accessible access to data summaries 39
40 Integration of Health Information Technology (HIT) for Population Health Management Updates to HIT to support team discussions (population health) and create efficiencies Collaboration with RDE Systems Dashboard design Adding additional key clinical indicators 40

41 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
42

43 CCT New Clients 43

44 Clinical Care Teams from the Patient Perspective

45 Patient Clinical Care Team Sheet Improving Communication with Clients Clinical Care Team Provider names Photos Accurate contact information
46 How does this transformation occur in the clinic and how can stakeholders drive the process? 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
47 Quality
48 Practice Transformation and Quality Improvement If we want safer, higher-quality care, we will need to have redesigned systems of care, including the use of information technology to support clinical and administrative processes. Committee on the Quality of Health Care in America (Institute of Medicine, Crossing the Quality Chasm, 2001) 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
49 NYP QPS Goals and Metrics Nursing QPS CHP Goals and Metrics ACN QPS CHP Quality Program Implementing Practice Transformation through a Quality Framework QI (or Patient Care Improvement ) Teams PDSAs STaR Work Groups Program Monitoring Monthly Review of Program Performance Quality Assurance & Regulatory Compliance Outcome Measures Review (CHP/State/Regional) Program Outcomes Evaluation Staff Surveys & Focus Groups Patient Surveys 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

50 Integrating Quality Improvement into Clinical Care Team Include all practice members Support development of PDSA cycles Provide data and administrative support to develop ideas Place Clinical Care Teams at the center so that team members explore shared goals and shared solutions 50

51 Care Teams QI Projects Timeline 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
52 TEAM A Project
53 Facilitating Transformation: Updating the Treatment Adherence Program Jumpstart Adherence Program defunded Pre-poured pillboxes paired with education are essential adherence support intervention for patients Opportunities to use Nursing expertise in medications and patient education Prevention of Medication errors Nurses as an integral part of the Clinical Care Teams 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

54 CCT Dashboard: Primary Care Nursing 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

55 STaR Working Group on Medication Distribution & Adherence Support Working Group consisted of representatives from each of the stakeholder groups with interest: Registered Nurses Nurse Administrator Clinicians Adherence Supervisor Operations Manager STaR Team facilitated the creation of the Working Group and participated in the meetings 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

56 Building on a Strength and Engaging Stakeholders for Transformation 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
57 Planning Implementation of New Treatment Adherence Program Review the old process and policies with the following goals: Identify issues Medical errors Reconciliation issues Large number of patients pick-up medication (~200 patients) Identify opportunities for transformation Nursing expertise in medication and education Nursing now committed to dedicated Clinical Care Team (CCT) Solutions Shrink pick-up list Move medication reconciliation and adherence pick-up under Nursing Nursing will be able to guide CCT meetings with up to date knowledge 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT



58 Pre-Implementation Activities: Pilot & Evaluation Practice Transformation Interest Group Meeting September 58

59 Updating Protocol & Workflows 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT


60 Changes to the Medication Distribution & Adherence Program Workflow First Work Group Meeting on Medication Distribution, Reconciliation, & Adherence 2 Week Pilot New Medication Distribution via RNs April 2015 August 2015 September 2015 Clinical Care Teams Review Program Enrollment & Proposes Graduation from Program Medication Distribution Shifts to RNs, Updates to Adherence Program Policy and Workflow Finalized 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
 STaR Project Director /Quality Manager 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE &")
61 Treatment Adherence Program QI Team Clinical Care Team A Treatment Adherence Supervisor All RNs (4) STaR Project Director /Quality Manager 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
62 QI Project AIM Increase, over a period of three months initially, the proportion of patients outreached, re-engaged and/or referred to other internal resources (e.g., Treatment adherence educator, Medical Case Management, or peer education) by those directly involved in implementing adherence support for CHP clients out of those patients enrolled in the program and who are failing to pick-up their medication or need additional adherence support NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
63 Intermediate AIMS Regulatory Decrease number of medications returned to Pharmacy. Intervention Monitoring Achieve real-time monitoring of missed medication pick-ups Improve care coordination among those involved in treatment adherence monitoring and support Care Teams at Clinic, Community Partner Staff, Nursing Team 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
64 Number of Patients CHP Adherence Program Population (February 2016): Viral Suppression (<200copies/mL) Rates by Teams N=150 47% 32% 32% 15% 12% 5% A B C D Clinical Care Teams Unsuppressed Overall, 64% viral suppression rate. Suppressed 6% 1% 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
65 CHP Adherence Program Population (February 2016): Last Viral Load > 6 month N=23 Unsuppressed Suppressed 17% 83% 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
 Develop med pick-up tracking system Develop medication pick-up patient list and")

 referral to MCM, 4) need to be outreached and scheduled for PC visit.")
66 PDSA Work Plan Action Step Details When Who 1) Develop and maintain Adherence Program population report through ecompas Get an updated list from AHF of patients picking-up at CHP; and Enroll patients in the Program in ecompas and maintain list so it is up-to-date Ongoing STaR Data Coordinator 2) Develop med pick-up tracking system Develop medication pick-up patient list and tables for monitoring missed medication pick-ups End of May Treatment Adherence Supervisor (TAS) 3) Medication pick-up weekly afternoon huddle Implement Friday afternoon huddle with RN and TAS to further refine weekly reports of missed medication pick-ups and protocol; identify patients to be outreached and discussed at CCT meetings Beginning of July RNs, TAS, and other team members as needed 4) Identify patients for CCT meeting discussion Patient discussion might result in an intervention including but not limited to: 1) referral to peer program, 2) referral to TAS, 3) referral to MCM, 4) need to be outreached and scheduled for PC visit. Beginning of July RNs, TAS, and other team members as needed 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
67 TAS often excluded from day-to-day patient encounters and pick-ups Peer referrals dropped off Nurses with many responsibilities and less time for intensive cases TAS able to attend team meetings RN variable team meeting attendance TAS not aware of who is picking up/not (prev based on individual patient interactions) Team QI PDSA (Where we lost ground) 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
68 Changes to the Medication Distribution & Adherence Program Workflow Primary Care Nursing Panels in CCT Dashboard Updated December 2015 March 2016 July 2016 Start of QI Discussions at CCTs Meetings, and Team A Proposes PDSA Nursing Panel Reviews at CCT Weekly Meeting Start PDSA Implementation Starts: Weekly Friday Afternoon Huddles, Meds put on Hold, and Targeted Patient Outreach 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

69 Team QI PDSA Progress (What We Have Accomplished) Coordinated with Pharmacy - accurate master list of patients picking up med Reviewed Master Medication Delivery logs for teams Conducted four afternoon Adherence QI huddles in July with RNs, TAS, and Quality Manager Patient tracking list TAS coordinating with pharmacy to reduce med returns Weekly Huddles assure improved RN- TAS communication proper med returns Identified and reached out to patients who need more support referred for peer, MCM, TAS support via Team structure 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT


70 Meds Missed Pick-up & Viral Load Suppression Tracking Tool Tables

71 Creating Efficiencies Adherence Program Indicators in the CCT Dashboard Adherence Program 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT

72
73

74 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT


75 Secure Data Transfer 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
76 Summary Involving stakeholders in all the stages of process improvement and transformation Building trust Using HIT solutions to achieve efficiencies and enhance communication Employing QI approaches or tools allow for systematic assessment of changes Leveraging Clinical Care Team to support continuous quality improvement 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT



77 Examination of organizations that have achieved and sustained substantial performance improvements reveals that lasting transformation requires the relentless hard work of local operational redesign. 77

78 STaR Team Susan Olender - PI Mila Gonzalez - Project Director Audrey Perez - Clinical Care Coordinator Marilena Lekas - Evaluator James Beltran - Data Manager Jesse Thomas - HIT Consultant, RDE Anusha Dayananda - HIT Consultant, RDE Peter Gordon Medical Director 78

79 Questions 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
80 Efficient Use of Clinical Space

81 Current CHP Patient Flow Model Reg & DC Meds NA Waiting Room RN PCP 81
82 82


83 HP6 Proposed Patient Flow Model Patient Arrives Pt checks in at front desk Pt Presents insurance card Patient is Registered PFA Arrives Patient in Eagle and updates Pt Status in XA. PFA verifies pts insurance PFA updates demographic information PFA prints label and room assignment on encounter form. PFA updates Pt Status to read r for vitals, SW, JS, CASAC, RD, etc. Vital Signs Conducted NA takes pt to exam room assigned (on encounter form) NA conducts vital signs NA updates pt status list r for PCP. In exam room PCP sees Patient PCP informed pt is ready via pt status column. PCP sees pt; updates pt status; completes documentation including orders; updates pt status: r for RN, r for D/C, DC by MD PCP exits exam room and visits next pt. RN sees Patient RN notified to see pt via pt status and by monitoring doctors orders RN gets pt; updates status w/ RN, sees pt; when finished, updates status r for D/C. Patient Checks Out Pt exits exam room (either after PCP or RN) and proceeds to front desk. PFA completes any PCP orders PFA discharges patient OR Patient uses mynyp.org and checks on appts from home. CRD 2/08/11
Approaches to practice transformation to improve outcomes along the HIV Care Continuum Panel Session
 Approaches to practice transformation to improve outcomes along the HIV Care Continuum Panel Session Integrating Quality Improvement and Population Health Approaches into Panel-based Care through Practice
Approaches to practice transformation to improve outcomes along the HIV Care Continuum Panel Session Integrating Quality Improvement and Population Health Approaches into Panel-based Care through Practice
Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources
 Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources About the Primary Care Development Corporation (PCDC) Founded in 1993, PCDC s mission is to catalyze excellence in primary care through
Paying for HIV Prevention: Reimbursement & Sustainable Payer Sources About the Primary Care Development Corporation (PCDC) Founded in 1993, PCDC s mission is to catalyze excellence in primary care through
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Meeting Title. Facilitator. Conference Line
 DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
New York Presbyterian s HIV Care Cascade: Methodology & Next Steps. Pete Gordon, MD Sam Merrick, MD
 New York Presbyterian s HIV Care Cascade: Methodology & Next Steps Pete Gordon, MD Sam Merrick, MD 1 Cascade Reporting Requirements Open versus Active caseloads - Open: any services at NYP - Active: any
New York Presbyterian s HIV Care Cascade: Methodology & Next Steps Pete Gordon, MD Sam Merrick, MD 1 Cascade Reporting Requirements Open versus Active caseloads - Open: any services at NYP - Active: any
Health System Transformation Overview of Health Systems Transformation in New York State. July 23, 2015
 Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
Working together to improve HIV/AIDS services in Nevada and the Las Vegas TGA
 Ryan White Part A, B, C, D, F and Prevention Cross Part Collaborative Clinical Plan State of Nevada and the Las Vegas TGA Grant Year 2014-2015 Working together to improve HIV/AIDS services in Nevada and
Ryan White Part A, B, C, D, F and Prevention Cross Part Collaborative Clinical Plan State of Nevada and the Las Vegas TGA Grant Year 2014-2015 Working together to improve HIV/AIDS services in Nevada and
Ryan White Part A. Quality Management
 Quality Management Medical Case Management 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part
Quality Management Medical Case Management 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part
Community Health Workers: ACA and Redesign Funding Opportunities
 Community Health Workers: ACA and Redesign Funding Opportunities What are the Goals of the Affordable Care Act and Redesign? Increased Coverage Better Population Health Higher Quality, More-Patient Centered
Community Health Workers: ACA and Redesign Funding Opportunities What are the Goals of the Affordable Care Act and Redesign? Increased Coverage Better Population Health Higher Quality, More-Patient Centered
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Welcome and Orientation Webinar
 Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
AGENDA. 1. Latest Developments in the NYP PPS. 4. NYC Primary Care Information Program (Anname Phann)
") NYP PPS - Project Advisory Committee [PAC] meeting 107 East 70 th Street, (btw Park/Lexington Avenues) VNSNY Auditorium, 1 st Floor Dial-in 212-305-9039 Monday, March 9, 2015 9:30 a.m.-11:30 a.m. AGENDA
NYP PPS - Project Advisory Committee [PAC] meeting 107 East 70 th Street, (btw Park/Lexington Avenues) VNSNY Auditorium, 1 st Floor Dial-in 212-305-9039 Monday, March 9, 2015 9:30 a.m.-11:30 a.m. AGENDA
Indianapolis Transitional Grant Area Quality Management Plan (Revised)
") Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
PROJECT INSPIRE NYC. NASTAD Hepatitis Technical Assistance Meeting November 30, :00a 10:15am
 1 PROJECT INSPIRE NYC NASTAD Hepatitis Technical Assistance Meeting November 30, 2017 9:00a 10:15am 2 Credit and Disclaimer The project described was supported by Grant Number 1C1CMS331330-01-00 from the
1 PROJECT INSPIRE NYC NASTAD Hepatitis Technical Assistance Meeting November 30, 2017 9:00a 10:15am 2 Credit and Disclaimer The project described was supported by Grant Number 1C1CMS331330-01-00 from the
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA)
") NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE
 Data Decisions Delivery Directing Comprehensive TA: From Systems to Sustainability ADVANCING HIV PREVENTION THROUGH HEALTH DEPARTMENTS HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE HIV PREVENTION EDUCATIONAL
Data Decisions Delivery Directing Comprehensive TA: From Systems to Sustainability ADVANCING HIV PREVENTION THROUGH HEALTH DEPARTMENTS HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE HIV PREVENTION EDUCATIONAL
Center for Community Health Navigation at NewYork-Presbyterian Hospital
 Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard
 April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Medicaid and the. Bus Pass Problem
 Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
Medicaid and the Bus Pass Problem PRESENTED BY: Cardinal Innovations Healthcare Richard F. Topping, Chief Executive Officer Leesa Bain, Vice President, Care Coordination & Quality Management September
I. Coordinating Quality Strategies Across Managed Care Plans
 Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
4/22/2018. Redesign and Reimage Long Term Care for the Future. Health Care Landscape Change. Disclosure of Commercial Interests
 Redesign and Reimage Long Term Care for the Future Lisa Thomson Chief Strategy and Marketing Officer www.pathwayhealth.com Disclosure of Commercial Interests We consult for the following organization:
Redesign and Reimage Long Term Care for the Future Lisa Thomson Chief Strategy and Marketing Officer www.pathwayhealth.com Disclosure of Commercial Interests We consult for the following organization:
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
The Improvement Journey; From Beginning to Continued Improvement
 The Improvement Journey; From Beginning to Continued Improvement Clemens Steinbock and Lori DeLorenzo National Quality Center Together, we can make a difference in the lives of people with HIV. NQC provides
The Improvement Journey; From Beginning to Continued Improvement Clemens Steinbock and Lori DeLorenzo National Quality Center Together, we can make a difference in the lives of people with HIV. NQC provides
Design Principles for Learning and Caring in Patient-Centered Primary Care Homes
 The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Discussion of Care Integration Best Practices & Challenges
 Discussion of Care Integration Best Practices & Challenges Alicia Downes, LMSW Snr Program Manager-AIDS United Peter Coronado, Jr-Valley AIDS Council Director of Linkage to Continuum of Care South Central
Discussion of Care Integration Best Practices & Challenges Alicia Downes, LMSW Snr Program Manager-AIDS United Peter Coronado, Jr-Valley AIDS Council Director of Linkage to Continuum of Care South Central
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN
 ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified in this
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified in this
Delivery System Reform Incentive Payment (DSRIP)
") Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S
 ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
ACADEMIC GROUP PRACTICE AND THE LEADERSHIP OF APRN S Margaret Head, Chief Operating Officer/Chief Nursing Officer Susan Moseley Gent, Administrative Director Vanderbilt Medical Group March 10, 2012 With
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
The evolution and future of the NY health home program
 The evolution and future of the NY health home program Authors: Catherine Castillo, Senior Consultant, Tony Shi, Intern, Evan King, Executive Vice President Background In 2010, the Affordable Care Act
The evolution and future of the NY health home program Authors: Catherine Castillo, Senior Consultant, Tony Shi, Intern, Evan King, Executive Vice President Background In 2010, the Affordable Care Act
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, :00 5:00 PM
 ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
Meeting Title. Facilitator. Conference Line. Corporation)
") DSRIP Meeting Agenda 10/23/15 NYP PPS Clinical Operations Date and Time Meeting Title Committee Location Heart Center Room 4 Facilitator Dr. Emilio Carrillo, Angela Go to Meeting https://global.gotomeeting.com/
DSRIP Meeting Agenda 10/23/15 NYP PPS Clinical Operations Date and Time Meeting Title Committee Location Heart Center Room 4 Facilitator Dr. Emilio Carrillo, Angela Go to Meeting https://global.gotomeeting.com/
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Behavioral Health Integration in the Primary Care Setting
 Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations
 Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations Nicole Downey, MBA, RD, CDE Program Director Diabetes Services The Polyclinic Seattle,
Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations Nicole Downey, MBA, RD, CDE Program Director Diabetes Services The Polyclinic Seattle,
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET
 PHSSR Research in Progress Webinar Series Speaker Biographies Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET Presenters
PHSSR Research in Progress Webinar Series Speaker Biographies Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET Presenters
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network
 Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act
 Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Medical Case Management
 Definition: services (including treatment adherence) is the provision of a range of consumer-centered consumer activities focused on improving health outcomes in support of the HIV Care Continuum. Consumer
Definition: services (including treatment adherence) is the provision of a range of consumer-centered consumer activities focused on improving health outcomes in support of the HIV Care Continuum. Consumer
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
USING PSYCKES TO SUPPORT CARE COORDINATION IN NEW YORK STATE
 USING PSYCKES TO SUPPORT CARE COORDINATION IN NEW YORK STATE NYS Office of Mental Health Edith Kealey, PhD Deputy Director, PSYCKES OVERVIEW Introduction to PSYCKES: The Psychiatric Services and Clinical
USING PSYCKES TO SUPPORT CARE COORDINATION IN NEW YORK STATE NYS Office of Mental Health Edith Kealey, PhD Deputy Director, PSYCKES OVERVIEW Introduction to PSYCKES: The Psychiatric Services and Clinical
New Opportunities in Long Term Services and Supports
 Profiles of State Innovation: Long -Term Supports and Services CHCS Webinar November 22, 1010 New Opportunities in Long Term Services and Supports Mary Sowers Director, Division of Community and Institutional
Profiles of State Innovation: Long -Term Supports and Services CHCS Webinar November 22, 1010 New Opportunities in Long Term Services and Supports Mary Sowers Director, Division of Community and Institutional
What is Mental Health Integration?
 What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Introduction to the Malnutrition Quality Improvement Initiative (MQii)
") Introduction to the Malnutrition Quality Improvement Initiative (MQii) Presentation Outline Business Case for the Malnutrition Quality Improvement Initiative (MQii) Background on the MQii and Learning
Introduction to the Malnutrition Quality Improvement Initiative (MQii) Presentation Outline Business Case for the Malnutrition Quality Improvement Initiative (MQii) Background on the MQii and Learning
o Recipients must coordinate these testing services with other HIV prevention and testing programs to avoid duplication of efforts.
 E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
10/31/2016. Primary Care Plan. DY2 - Revised
 10/31/2016 Primary Care Plan DY2 - Revised Table of Contents CONTENTS Executive Summary... 2 Fundamental 1: Assessment of current primary care capacity, performance and needs, and a plan for addressing
10/31/2016 Primary Care Plan DY2 - Revised Table of Contents CONTENTS Executive Summary... 2 Fundamental 1: Assessment of current primary care capacity, performance and needs, and a plan for addressing
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
An Implementation Framework for Patient Safety in Ambulatory Care. To disseminate key findings from IHI s work on ambulatory safety
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Building a Better Home: Transformation to a Patient Centered Health Home. Anna M. Gard, FNP-BC Association of Clinicians for the Underserved
 Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Residency PCMH Longitudinal Curriculum Competency Based Goals and Objectives
 PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
PCMH Ambulatory Care Curriculum Goals and Objectives The PCMH Ambulatory Care Curricular Competency Based Goals are: Access to Care Quality Improvement Population Management Team Based Care Integrated
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11
 Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Payer Perspectives On Value-based Contracting
 Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
Payer Perspectives On Value-based Contracting Miles Snowden, MD, MPH, CEBS Chief Medical Officer 1 A simple goal Making the health system work better for everyone 2 Optum serves 60,000,000+ individuals
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional