Improving Episode Management and Patient Engagement with Telehealth Programs
|
|
|
- Moses Byrd
- 5 years ago
- Views:
Transcription


1 Improving Episode Management and Patient Engagement with Telehealth Programs Aurora at Home Amy Shockley MSN RN GCNS-BC Melissa Jordan BSN RN Aurora Health Care at a Glance Private, not-for-profit integrated health care provider 31 counties, 90 communities 16 hospitals 159 clinic sites 70 retail pharmacies 30,000 caregivers including 1,600 employed physicians Largest homecare organization in Wisconsin More than 1.2 million patient encounters $4.1 billion in annual revenue 2 1


2 Our mission is to help you live well by bringing the future of health care to you, in the place you call home. Presentation Objectives Discuss remote patient monitoring strategies implemented at Aurora Explain the program scope and roles of the home care team Demonstrate program outcomes 2
3 Telehealth Program Educated health care providers to recognize program scope and care impact Culture change Transition program as a self-awareness monitoring tool Allows patients to identify trends Not intended an emergency response device Establish Focus Reinforce Action Plan Share Information Develop Action Plan Developed Shared Goals Predictions The prevalence of chronic disease is projected to increase; over 157 million Americans are expected to be living with one or more chronic diseases by According to Center for Medicaid and Medicare (2012), 1 out of every 5 older adults age 65 and older are admitted to the hospital is readmitted within 30 days. More than 50% of patients hospitalized for heart failure are readmitted to the hospital within 6 months after their most recent hospital discharge. COPD is also a highly prevalent condition that is expected to be the third cause of death worldwide by 2020 and is also associated with risk of disability and high use of health care resources. 3



4 Management Disease management programs typically involve a multidisciplinary, integrated approach to care for patients with a chronic illness or multiple chronic conditions. Telehealth is becoming increasingly utilized within the community setting and is a form of promoting chronic disease self-management. Interventions such as patient education, health programs, pharmacological strategies and Telehealth can be utilized Detect worsening health status Assist in implementing timely interventions Health care expense Health care expenditures increase with the number of chronic conditions with nearly 80% of Medicare expenditures for individuals with at least four chronic medical conditions. Hospital readmissions for patients within 30 days of their last hospital stay are burdening, and costs the health care system over 5 billion dollars annually. Healthcare organizations have a responsibility to attempt to reduce adverse outcomes such as hospital readmission rates and increase patient self-efficacy and quality of life to improve patient care and patient outcomes. 4







5 Prevalence of chronic conditions Older adults with multiple chronic conditions endure functional decline and loss of independence placing them at high risk for hospitalization. Often times the burden of accessing healthcare is placed on individual patients. Telehealth programs are being implemented due to enhancements with patient self management. Aurora at Home Telehealth Combines technology and disease management to enhance and extend case management techniques Facilitates and improves the health of designated population Provides care coordination and support for patients with chronic conditions to avoid unnecessary hospitalizations Self-awareness program with monitoring tools for patients to identify trends while providing transitional care support in the home 5


6 Program Enhancements Wireless medical devices Option to manually enter vital signs Multiple choice responses, not limited to yes/no Customize-able clinical content and questionnaires Daily and weekly disease management surveys Risk assessments Transmits over analog, VOIP, cellular Our summary dashboard allows us to quickly identify patients that are out of range with either vitals or survey responses 6


7 Multidisciplinary Team approach to care Registered Nurses, Therapists, Advanced Practice Nursing, Registered Dietitians, Medical Social Workers, Hospital Liaisons, and Leadership Utilization of workflows to track high-risk patients follow-up Interventions may include Follow-up phone calls Tuck-in calls Increased monitoring frequency or RN home visit Frequent collaboration with the RN Case Manager MD collaboration Self-Management Promotion Model Enhanced patient education and support through structured teach back interactions Individualized Action Plan Medication management Disease specific education Transition to own equipment To be sure that I have explained myself clearly, can you please repeat back to me in your own words how you will take your daily weight 7

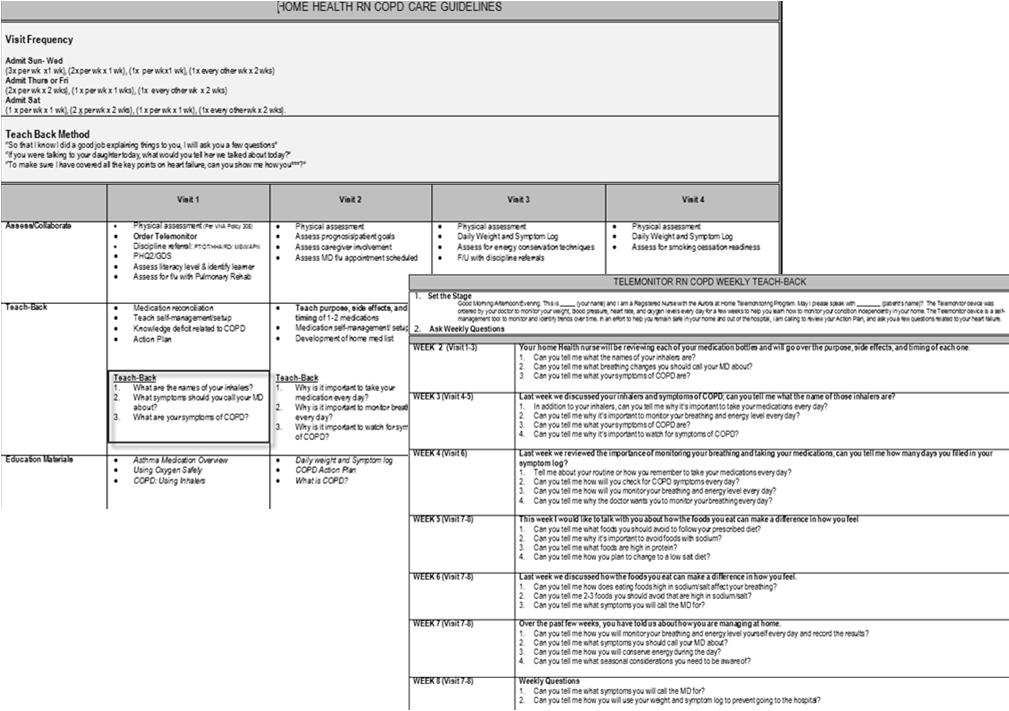
8 Education tools Structuring the episode 8
.")
9 Episode Management Plan Nursing support when not making a home visit Provides structure to care and discharge planning Risk Stratification with LACE LACE Model Screening Tool Screening method to identify patients who are at high-risk for hospital readmission within 30 days of their last hospital discharge. Length of Stay Less than 1 day (0). 1 day(1), 2 days(2), 3 days(3), 4 6 days (4), 7 13 days(5), 14 + days(6) Acute Admission Inpatient(3), Observation(0) Comorbidity (0) No history (1)DM no complications, Cerebrovascular disease, Hx of MI, PVD, PUD (2)Mild liver disease, DM with end organ damage, CHF, COPD, Cancer, Leukemia, Lymphoma, Tumor, Mod severe renal disease (3)Dementia or connective tissue disorder (4)Mod severe liver disease or HIV (6)Metastatic cancer ED utilization visits (0), 1 visit (1), 2 visits (2), 3 visits (3), 4 or more visits (4) 9

10 Validated Screening Tools Patient Health Questionnaire Assesses for Depression Orientation Memory Concentration Test Assesses for Cognitive Impairment Patient Activation Measure Extent in which individuals are able to manage their own healthcare and encompasses a range of elements important in self-management that extend beyond any single health behavior Older adults with chronic disease may lack the ability and willingness to manage aspects of their health and health care. This lack of activation by the patient is associated with a higher use of acute care services and rehospitalization shortly after discharge. PAM 13-Item Questionnaire 10
")
11 Patient Activation Model Strategy review Developed episode management plan Structured sequential patient education Visit set for in-home RN and Telehealth RN Identified workflow needs based on risk stratification LACE High-Risk Screening Tool Integrated validated screening tools Patient Activation Measure Orientation Memory Concentration Test Patient Health Questionnaire (PHQ-9) 11

12 Scope and Roles The patient and their home health team Self-management goals Patients with chronic illness require a balance between medical care, patient participation, and cooperation with self-management abilities Evaluate the Response Recognize Change in Condition Implement a Treatment Evaluate the Change Decide to Take Action 12


 At Risk for Falls Age 80 or older 2 or more Hospitalizations/ED visits in the past 6")
13 Aurora at Home Telehealth is considered to be a vital component of transitional care coordination for patients Telehealth can coordinate and support the care of vulnerable patient populations with chronic conditions, and avoid unnecessary hospitalizations. Right Patient Right Program Right Time Inclusion Criteria Chronic Condition (CHF, COPD, DM, MI, HTN, Depression etc.) At Risk for Falls Age 80 or older 2 or more Hospitalizations/ED visits in the past 6 mo Taking 5 or more medications At Risk for re hospitalization 13
14 Exclusion Criteria Physically or cognitively unable to use the equipment safely and has no caregiver available. Residence not conducive/safe for monitoring (i.e. power, extreme clutter/infestation). Patients with low functional vision, unless there is a competent caregiver Patient unwilling to agree to terms as stated on installation ereferrals 14

15 Clinical Collaboration Installation Process Admitted to Home Health Care or Home Palliative Services Internal or External Referral Admitting RN sends referral to Telemonitor Program RN send referral Smart Text documentation template to our Team Assistant Risk Stratification Assessment Welcome Call placed to patient Trapollo notified of new referral Connect with patient and ship out equipment via UPS Monitor is installed via remote support Telemonitor RN collaborates with patient, MD, and Field RN Monitor is sent back to Trapollo via UPS upon program completion 15

16 Virtual connections Disease specific surveys individualized to the patient s TeleStation Assists with early identification of warning signs Guides intervention/notification of subtle changes Promotes self-management and monitoring their condition Aurora at Home STEP Pilot Study Determine whether a telehealth program with a sequential education plan compared to standard telehealth positively impacts patient self-management through patient activation, patient satisfaction, and decreases 30 day readmission. There is support for use of telehealth in the home health setting to assist in promoting increased patient knowledge and adherence, and preventing rehospitalizations. The use of telemonitoring along with remote patient education provided by a registered nurse has been studied with varied results. There is a need for additional research to identify strategies to improve patient self-management that may impact clinical outcomes. 16
17 Episode Management Experimental Pilot The Aurora at Home Sequential Telemonitor Education Pilot (STEP) study examined if there was a difference in patient activation, patient satisfaction and 30-day readmission rates between patients with CHF or COPD who received standard telemonitor home health care versus telemonitoring with a sequential education plan. A secondary analysis was also conducted using data from the Sequential Telemonitor Education Pilot study to examine the relationship between older adults depression and their level of patient activation. Outcomes Measures Patient Activation Measure Patient Experience 30-Day Hospital Readmission rates Reduction of Skilled Nursing Home Visits Outcomes Clinical Operations Patient 30 day readmits Utilization Growth Visits Activation Participation 17
18 Statistics January September 2015 Total Initial Enrollment* 1224 New Participants 901 Average Days Monitored 36.5 Onsite Appointments 11 Removals 807 Time from enrollment to on service December 14 February 15 Longest: 32 Days Shortest: 3 Days Average: 9Days March 15 May 15 Longest: 24 Days Shortest: 3 Days Average: 6Days June 15 August 15* Longest: 15 Days Shortest: 1 Day Average: 5Days 18


19 Primary diagnosis and Length of service installs average Program Participate by team location 19
20 Inventory turns Dec 14 Jan 15 Feb 15 Mar 15 Apr 15 May 15 Jun 15 Jul 15 Aug 15 Sep 15 Monitored Census in Jan 15 Feb 15 Mar 15 Apr 15 May 15 Jun 15 Jul 15 Aug 15 Sep 15 20




21 Lessons learned Clinical leadership, oversight and support Transitions are overwhelming for patients, plan the timing of equipment arrival Front-load clinical visits and then taper back. Use Plain Language (Plug-in and turn on versus Install) Avoid survey fatigue Partnerships Thank you! Aurora at Home 21
22 References Asua, J., Orruno, E., & Gagnon, P. (2012). Healthcare professional acceptance of telemonitoring for chronic care patients in primary care..medical Informatics and Decision Making, 12 (139), Blum, K., & Gottlieb, S. S. (2014). The effect of a randomized trial of home telemonitoring on medical costs, 30-day readmissions, mortality, and health-related quality of life in a cohort of community-dwelling heart failure patients. Journal Of Cardiac Failure, 20(7), doi: /j.cardfail Bowles, K. H., Dykes, P., & Demiris, G. (2015). The Use of Health Information Technology to Improve Care and Outcomes for Older Adults. Research In Gerontological Nursing, 8(1), doi: / Boyne, J. J., Vrijhoef, H. J., Spreeuwenberg, M., De Weerd, G., Kragten, J., & Gorgels, A. P. (2014). Effects of tailored telemonitoring on heart failure patients knowledge, selfcare, self-efficacy and adherence: A randomized controlled trial. European Journal Of Cardiovascular Nursing, 13(3), doi: / Damiani, G., Salvatori, E., Silvestrini, G., Ivanova, L., Bojovic, L., Iodice, L., & Ricciardi, W. (2015). Influence of socioeconomic factors on hospital readmissions for health failure and acute myocardial infarction in patients 65 years and older: Evidence from a systematic review. Clinical Interventions in Aging, 10 (1), Hibbard, J., Stockard, J., Mahoney, E., & Tusler, M. (2004). Development of the Patient Activation Measure (PAM): Conceptualizing and Measuring Activation in Patients and Consumers. Health Services Research, 34(4), Katzman R, Brown T, Fuld P, et al. (1983). Validation of a short orientation-memory-concentration test of cognitive impairment. American Medical Journal Psychiatry, 140(6), Kroenke, K., Spitzer, R., & Williams, J. (2001). The PHQ9. Journal of General Internal Medicine. 16(9), Madigan, E., Schmotzer, B. J., Struk, C. J., DiCarlo, C. M., Kikano, G., Piña, I. L., & Boxer, R. S. (2013). Home health care with telemonitoring improves health status for older adults with heart failure. Home Health Care Services Quarterly, 32(1), doi: / Pedone, C., Chiurco, D., Scarlata, S., & Incalzi, A. (2013). Efficacy of multiparametric telemonitoring on respiratory outcomes in elderly people with COPD: A randomized controlled trial. BMC Health Services Research, 13 (82) 3-7. Ryan, P., & Sawin, K. (2009). The Individual and Family Self-Management Theory: Background and perspectives on context, process, and outcomes. Nursing Outlook, (57), Takahashi, P., Pecina, J., Upatising, B., Chaudhry, R., Shah, N., Van Houten, H., &... Hanson, G. (2012). A randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visits. Archives Of Internal Medicine, 172(10), Wade, M. J., Desai, A. S., Spettell, C. M., Snyder, A. D., McGowan-Stackewicz, V., Kummer, P. J., & Krakauer, R. S. (2011). Telemonitoring with Case management for seniors with heart failure. American Journal Of Managed Care, 17(3), e
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Saint Agnes Hospital. Pharmacist utilization of the LACE tool to prevent hospital readmissions. Program/Project Description, including Goals:
 Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Running head: SMART APPS TO DECREASE CHF READMISSION RATES 1
 Running head: SMART APPS TO DECREASE CHF READMISSION RATES 1 Use of Smartphone Applications in the Reduction of Hospital Readmissions of Heart Failure Patients in Short Term Acute Care Facilities Eleanor
Running head: SMART APPS TO DECREASE CHF READMISSION RATES 1 Use of Smartphone Applications in the Reduction of Hospital Readmissions of Heart Failure Patients in Short Term Acute Care Facilities Eleanor
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
PERFORMANCE MEASURE DATE / RESULTS / ANALYSIS FOLLOW-UP / ACTION PLAN
 Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Combining Nursing Power and Quality Metrics to Influence Policy Development
 Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Advancing Popula/on Health and Consumerism
 Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Northumberland Frail Elderly Pathway. Dr David Shovlin Fiona Brown
 Northumberland Frail Elderly Pathway Dr David Shovlin Fiona Brown What s special about the Frail Elderly Pathway Patient centered joint working across the entire health and social care system for over
Northumberland Frail Elderly Pathway Dr David Shovlin Fiona Brown What s special about the Frail Elderly Pathway Patient centered joint working across the entire health and social care system for over
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
EVOLENT HEALTH, LLC. Asthma Program Description 2018
 EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries
 Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries IOM 9/22/11 Kathy Duckett RN, BSN Director of Clinical Programs Partners Healthcare at Home
Innovations in Expanding Primary Care Capacity: Moving Away from Visit Based Care for Medicare Beneficiaries IOM 9/22/11 Kathy Duckett RN, BSN Director of Clinical Programs Partners Healthcare at Home
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Better Health and Lower Costs for Patients With Complex Needs
 Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage
 Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2)
") Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010)
") Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
Medicaid HCBS/FE Home Telehealth Pilot Final Report for Study Years 1-3 (September 2007 June 2010) Completed November 30, 2010 Ryan Spaulding, PhD Director Gordon Alloway Research Associate Center for
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Appendix: Assessments from Coping with Cancer
 Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation: